High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 1 of 31
High Dose Antipsychotic Treatment
(HDAT) Guideline In-patient and Community Patient
Lead Author: Lesley Dewar
Endorsing Body: NHSL Mental & Learning Disabilities Drug & Therapeutic Committee
Governance or Assurance Committee
NHSL Mental & Learning Disabilities Clinical Governance
Implementation Date: April 2018
Version Number: 1.0
Review Date: 28th March 2021
Responsible Person Lesley Dewar
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 2 of 31
CONTENTS
Section Content
1 Consultation and Distribution Record
2 Change Record
3 Introduction
4 Aim and purpose
5 Prescribing HDAT
5.1 RCPsych Consensus
5.2 General Recommendations
5.3 Risks associated with HDAT
5.4 Management of QTc prolongation
6 Information about Tool Kit
7 HDAT Review
8 Responsibilities
9 Tool Kit Tool 1 HDAT Monitoring Form Tool 2 HDAT Monitoring Guide Tool 3 HDAT Dose Calculation Tools Tool 4 HDAT Interacting Medicines Tool 5 HDAT Consent Form Tool 6 HDAT Side Effect Rating Scales Tool 7 HDAT GP Information Letter
Appendix 1 Good Practise Flow Chart for Monitoring Antipsychotics
Appendix 2 General Guidance for Monitoring Antipsychotics
Appendix 3 Royal College of Psychiatrists Consensus Statement on high dose antipsychotic medication (CR190)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 3 of 31
1. Consultation and Distribution
CONSULTATION AND DISTRIBUTION RECORD
Contributing Author / Authors
Lesley Dewar
Consultation Process / Stakeholders:
Louise Bradley
Gillian, Brown
Jennifer Byant
Laura Cameron
Venkat Chekuri
Linda Findlay
Mary Gilfillan
Billy Lang
Memo Langa
Gillian Laughlan
Ana Lopez
Irene McCormick,
Margaret McGreevy ,
Stewart Marshall
Jacqueline Mitchell,
Sheila Moug,
Janice Murphy,
Khalid Nawab
Margaret Serrels,
Vijay Sonthalia
Tryra Smyth
Suzanne Urquhart
Distribution: Dissemination to all MH&LD, OAP & CAMHS Medical & Nursing & Pharmacy Staff, Wards and Community teams
First Port
Staff briefing
Medicine Matters and/or MH&LD D&T Newsletter
Prescribing News
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 4 of 31
2. Change Record
CHANGE RECORD
Date Author Change Version No.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 5 of 31
3. Introduction This guidance has been developed to promote the appropriate and safe use of high dose antipsychotics in both the hospital and community setting. It replaces and extends previous NHSL High Dose Antipsychotic Treatment (HDAT) Guidance. The decision to prescribe, continue to prescribe or recommend the use of high dose antipsychotics should be undertaken with consideration to the RCPsych consensus statement (November 2014) (see Appendix 3) 4. Aim The purpose of this guidance is to promote and facilitate the safety of patients who are prescribed High Dose Antipsychotic Treatment in both in-patient and community settings in Lanarkshire. 5. Prescribing High Dose Antipsychotics 5.1 RCPsych consensus Consideration should be given the RCPsych Consensus Statement published in November 2014. The key points from the consensus statement are summarised in the appendix 3. The full statement can be found at http://www.rcpsych.ac.uk/usefulresources/publications/collegereports/cr/cr190.aspx 5.2 General recommendations of prescribing or recommending the use of HDAT
The use of HDAT should be an exceptional clinical practice and generally only employed when an adequate trial of standard treatments, including clozapine have failed.
Documentation of target symptoms, response and side effects should be standard practice so there is on-going consideration of risk-benefit ratio.
Failure of previous therapy due to non-compliance should be ruled out
The decision to use HDAT should be made by a senior psychiatrist, involving the MDT and be done, where possible, with patient consent.
The decision to prescribe the ongoing clinical assessment and the decision to continue should be documented.
Contra-indications should be ruled out and other risks minimised where possible.
Common sense approach should be taken with the elderly or frail individuals who may be more sensitive to the side effects of antipsychotics and require monitoring equivalent to that of HDAT at lower doses.
Prescribing for children and adolescents with antipsychotics should be undertaken cautiously and increased monitoring may be required at licensed doses.
Prescribing antipsychotics off label for children and adolescents should always be considered HDAT.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 6 of 31
5.3 Risks associated with HDAT 5.3.1 General increase of side effects Most side effects of antipsychotics are dose dependant and so the likelihood of a patient experiencing side effects to medication, increases with HDAT. In addition, the additive side effects of 2 or more antipsychotics may be particularly troublesome for some patients. This may also be compounded e.g. the use of antimuscarinics to counteract EPSE’s may cause cummulative dry mouth or constipation side effects. For this reason subjective side effects should be monitored using a patient self rating scale such as GASS (see Tool 6). 5.3.2 Cognitive side effects of antipsychotics Cognition should be regularly monitored for patients on HDAT’s. Cognitive function may be impaired with increasing dose and the cummulative effects of 2 or more antipsychotics. This may be particularly problematic where antimuscarinic side effects predominate especially if additional antimuscarinics are used for EPSE’s. 5.3.3 QT interval prolongation Case control studies have suggested that the use of most antipsychotics is associated with an increase in the rate of sudden cardiac death. Specifically, some antipsychotics block potassium channels and this affects the duration of cardiac repolarization. Cardiac repolarization is measured by the QT interval, i.e. time from onset of ventricular depolarisation to complete repolarisation. This is subject to a number of influences, including heart rate. Consequently QTc (QT interval corrected for heart rate) is considered the most appropriate measure to use when monitoring the effect of antipsychotics on ventricular repolarization. Prolonged QTc interval is considered a risk factor for arrhythmias, including Torsades de Pointes, the life-threatening polymorphic ventricular arrhythmia. Evidence suggests the risk of arrhythmia is exponentially related to extent of prolongation beyond normal limits. Although this evidence is limited, there is strong evidence that a QTc of greater than 500msec is a major risk for arrhythmia and Torsades de Pointes (TdP). As the overall risk would appear to be dose related, it follows that risks of QTc prolongation and arrhythmias are higher when patients are treated with high dose antipsychotics. 5.3.4 Risk factors for QTc prolongation with antipsychotics
High Dose Antipsychotics Treatment
Congenital long QT syndrome
Previous episodes of TdP
Pre-existing cardiac disease e.g. left ventricular dysfunction/hypertrophy
Extremes of age
Bradycardia or presence of extrasystoles (and any associated condition)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 7 of 31
Electrolyte abnormalities, particularly hypokalaemia, hypocalcaemia & hypomagnesaemia (including co-administration of drugs which may cause this if uncorrected)
Malnorishment/alcoholism due to associated liver disease
Female (longer QT interval on average than males)
Possibly restraint in some patients
Co –administration of other drugs which prolong QTc
Any factor which may increase plasma levels of an antipsychotic e.g. co-administration of drugs which inhibit metabolising enzyme or in patients who are slow metabolisers
Early in treatment or soon after plasma increases (dose increase/ addition of interacting drug)
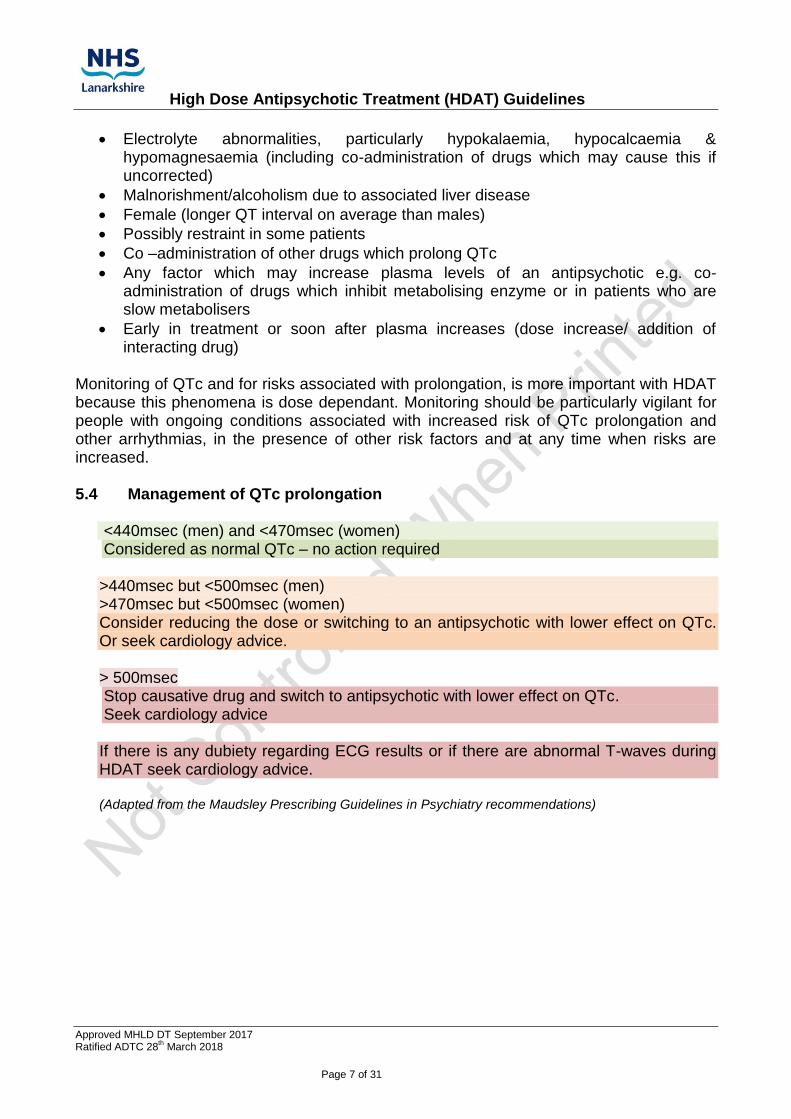
Monitoring of QTc and for risks associated with prolongation, is more important with HDAT because this phenomena is dose dependant. Monitoring should be particularly vigilant for people with ongoing conditions associated with increased risk of QTc prolongation and other arrhythmias, in the presence of other risk factors and at any time when risks are increased. 5.4 Management of QTc prolongation
<440msec (men) and <470msec (women) Considered as normal QTc – no action required
>440msec but <500msec (men) >470msec but <500msec (women) Consider reducing the dose or switching to an antipsychotic with lower effect on QTc. Or seek cardiology advice.
> 500msec Stop causative drug and switch to antipsychotic with lower effect on QTc. Seek cardiology advice
If there is any dubiety regarding ECG results or if there are abnormal T-waves during HDAT seek cardiology advice.
(Adapted from the Maudsley Prescribing Guidelines in Psychiatry recommendations)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 8 of 31
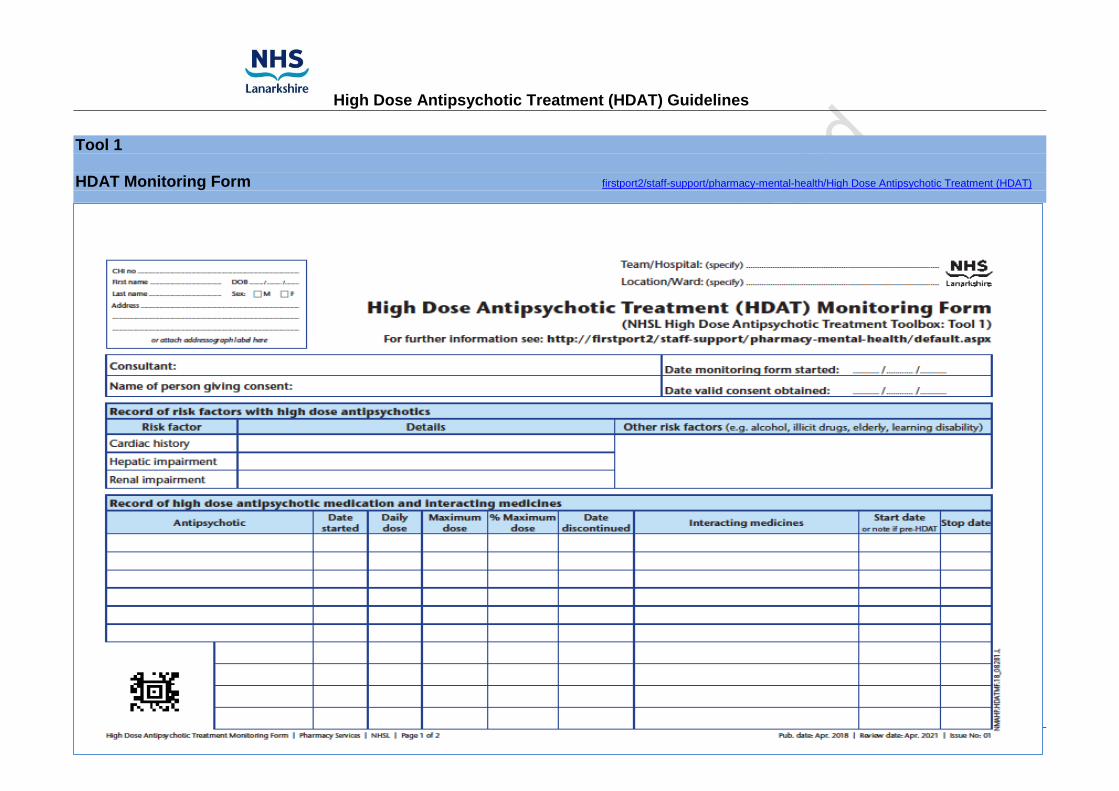
6 HDAT Tool Kit A High Dose Antipsychotic Treatment Tool Kit has been compiled to help deliver best practise when considering and using high dose antipsychotics. In addition to the Toolbox, appendix 1 and appendix 2 give guidance on the general monitoring of antipsychotics, and when additional monitoring should be carried out. 6.1 Tool 1 HDAT Monitoring Form Additional monitoring should be carried out when the use of antipsychotics in a patient falls into the high dose range. These parameters should be recorded on the NHSL High Dose Antipsychotic Monitoring Form (Tool 1). These parameters are in addition to standard monitoring for antipsychotics or any additional monitoring required by the manufacturers of individual antipsychotics. Baseline recording should be made before patients are prescribed in the high dose range and at regular intervals during high dose treatment. The monitoring form should be retained in the patient’s notes and a copy transferred when patient moves between inpatient and outpatient settings. 6.2 Tool 2 HDAT Monitoring Guide The HDAT Monitoring Guide (Tool2) provides a guide to the use of Tool 1 (HDAT Monitoring Form) on the parameters to be monitored and the frequency this should be carried out. 6.3 Tool 3 HDAT Calculation tools High Dose Antipsychotics can occur from two scenarios
1. A single antipsychotic is prescribed at a dose higher than the maximum licensed daily dose for the age and clinical condition of the patient.
2. The cumulative % daily dose of two or more antipsychotics is more than 100% (using the percentage method*)
*the percentage method Convert the dose of each drug into the percentage of the maximum licensed dose for the patients age and clinical condition and add these together. A cumulative dose of more than 100% is HDAT. Tool 3 provides advice on how to check if a patient is in the high dose range. NB if the dose of any antipsychotic exceeds the maximum dose for that drug, it is an off-label use and local unlicensed use protocols should be followed in addition to HDAT guidance. Situations where an antipsychotic is being used for children or adolescents, out with it’s the licensed indication, should be treated as HDAT. Off-label use and local unlicensed use protocols should also be followed.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 9 of 31
6.4 Tool 4 HDAT Guide to Interacting Medicines Tool 4 is a guide to interacting medicines which may increase the risks associated with the use of high dose antipsychotics. It provides links to resources to check for such interactions. 6.5 Tool 5 HDAT Consent Form Valid patient consent should be obtained when prescribing or recommending antipsychotics in the high dose range. A consent form for this purpose is available as Tool 5. 6.8 Tool 6 HDAT Side Effects Rating Scales Regular monitoring of side effects, using recognised rating scales, is strongly recommended. Tool 6 guides on the availability of these, with links to GASS, GASS for clozapine, easy read versions of these and tools to assess side effects in people with communication problems that are unable to use these. 6.9 Tool 9 GP HDAT Information Letter The GP should be notified of the patient’s high dose status and the implications this has. Tool 9 can be used to inform the GP of the reasons for HDAT and the need to be aware of additional changes to the patient’s medicines in general, that may increase the risks associated with HDAT. 7. Medication Review The key recommendation of the RCPsych Consensus Statement is that any prescription of high-dose antipsychotic medication should be seen as an explicit, time-limited individual trial with a distinct treatment target. Doses should be increased slowly and not more than once weekly. There should be a clear plan for regular clinical review including safety monitoring. The high-dose regimen should only be continued if the trial shows evidence of benefit that is not outweighed by tolerability or safety problems. For this reason, the benefit and the outcome should be documented in the patient’s notes. There is a tick box on the monitoring form to document when this is done. It is recommended that if there is no improvement after 3 months doses should be reduced to standard doses.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 10 of 31
8. Responsibilities 8.1 In patients 8.1.1 Consultant / SAS Psychiatrist Responsibilities
To be ultimately responsible for the use of HDAT and to retain this responsibility when the patient is discharged from hospital.
To ensure reason for high-dose use is documented in patient notes.
To ensure patient consent has been obtained. The Patient Consent Form is available as Tool 5. This should be ticked as having been done on the HDAT Monitoring Form (Tool 1).
To ensure appropriate monitoring is in place and is documented according to these guidelines regardless of the patient’s inpatient/outpatient status.
To ensure clinical progress is regularly monitored and documented in patient notes regardless of the patient’s in-patient/out-patient status. Tick on the monitoring form that this has been done.
To be aware that the use of PRN antipsychotics may tip the patient into the high dose range. Base line monitoring should be done if this is a possibility.
For patients with incapacity who are not complying with HDAT monitoring, ensure this is documented on the HDAT Monitoring Form, in the case notes and that Alternative Heath Checks are carried out.
To complete an Inpatient Unlicensed Use Form if a single antipsychotic is above the maximum licensed dose or the antipsychotic is being used off licence. https://www.medednhsl.com/sites/drugs & prescribing/medicines approval
On discharge, to liaise with GP around the use of HDAT and any unlicensed use.
To be aware that HDAT monitoring is not the routine responsibility of the GP, however they should consider the risks of initiating interacting medicines in patients on HDAT and carrying out additional monitoring if this is deemed necessary.
To use the template GP information letter (Tool 7) to inform GP of high dose use on discharge and the unlicensed use request form if any antipsychotic is being used off-license http://firstport2/staff-support/pharmacy-mental-health/Documents/General Mental Health Prescribing/NHSL Unlicensed Use Prescribing Request to GP and Patient Consent Form.pdf
To send a copy of the patient consent form (Tool 5) with the GP information letter (Tool 7) on discharge
To seek pharmacy advice if necessary. 8.1.2 Junior Doctor Responsibilities
To be aware when a patient is on high-dose antipsychotics and attach HDAT alert sticker to prescription chart.
To be aware of consultant responsibilities.
To check that HDAT Monitoring Form (Tool 1) is being completed.
To complete patient details on high dose antipsychotic therapy (HDAT) sheet
To check high dose antipsychotic therapy (HDAT) is mentioned on consent to treatment or second opinion form, if applicable.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 11 of 31
To ensure Patient Consent Form (Tool 5) has been completed and documented in notes.
To complete Risk Factors section.
To complete interacting medicines section.
To complete high-dose details and write % of maximum antipsychotic dose being prescribed. (Tool 3).
To ensure an inpatient unlicensed use form is completed if the dose of a single antipsychotic is above the maximum licensed dose. MedEd Prescribing form C
To order ECGs and document results on monitoring form (Tool 1).
To check U&Es and document results on monitoring form (Tool 1).
To check LFTs and document results on monitoring form (Tool 1).
To ensure on patients’ discharge that GP and other relevant community mental health personnel are informed of HDAT status (see consultant responsibilities).
As an integral part of discharge planning, collaborate with nursing staff to ensure a system is in place to facilitate continuation of HDAT ‘monitoring & review’ within the community setting.
To undertake pharmacy responsibilities where there is no pharmacy cover.
Seek pharmacy advice if necessary.
* If no junior doctor cover these responsibilities should be undertaken by the consultant. ** In some areas, ANP’s may be able to carry out U&E’s & LFT’s, however medical staff retain the responsibility of checking and recording these results.
8.1.3 Nursing Staff Responsibilities
To document “high dose” status in the nursing care plan (in MiDIS where available).
To check patient temperature and document on Monitoring Form (Tool 1) and NEWS.
To check blood pressure and document on Monitoring Form (Tool 1) and NEWS.
To check that parameters are being entered in the HDAT Monitoring Form (Tool1).
To check HDAT sticker is attached to the prescription chart (or HDAT stamp is used).
To check warning sticker is attached to prescription chart if ‘PRN’ medication will result in HDAT.
To ensure that high-dose status is discussed at review.
As an integral part of discharge planning, collaborate with medical staff, to ensure a system is in place to facilitate continuation of HDAT ‘monitoring & review’ within the community setting.
Seek pharmacy advice if necessary.
** In some areas, ANP’s may be able to carry out U&E’s & LFT’s, however medical staff retain the responsibility of checking and recording these results. 8.1.4. Pharmacist Responsibilities*
To assist with identification of patients on high-dose antipsychotics
To ensure patient details are entered on HDAT Monitoring Form (Tool 1) and parameters are being recorded
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 12 of 31
To verify high-dose details are correct
To verify interacting medicines section is accurate and kept up to date
To ensure HDAT sticker has been fixed to chart when appropriate
To provide advice to medical and nursing staff when necessary *If no pharmacist cover, these responsibilities should be undertaken by a Clinician 8.2 Community Patients 8.2.1 Consultant /SAS Psychiatrist Responsibilities
To be ultimately responsible for the use of HDAT and to retain this responsibility when the patient is discharged from hospital.
To ensure local arrangements are put in place to maintain appropriate and regular monitoring of patients on HDAT according to these guidelines.
To be aware that the logistics of how monitoring is carried out should make best use of the resources within the patient’s locality or community team with consideration to the needs of the patient.
To be aware that HDAT monitoring is not the routine responsibility of the GP, however they should consider the risks of initiating interacting medicines in patients on HDAT and carrying out additional monitoring if this is deemed necessary.
To liaise with GP around the use of HDAT and any unlicensed use. Use the template GP information letter (Tool 7) to inform GP of high dose use on discharge.
To ensure reason for high-dose is documented in case notes.
To ensure patient consent has been obtained. The Patient Consent Form is available as Tool 5. This should be ticked as having been done on the HDAT Monitoring Form (Tool 1)
To send a copy of the patient consent form (Tool 5) with the GP information letter (Tool 7).
To ensure the HDAT Monitoring Form (Tool 1) is completed each time a parameter is monitored, and a decision made, and noted on form, as to when that parameter next needs monitored.
To ensure clinical progress is regularly monitored and documented in patient notes. Tick on the monitoring form that this has been done.
To retain the HDAT Monitoring Form (Tool 1) within the patient’s notes and ensure a copy is sent to the MH ward should the patient be admitted.
To be aware that the use of PRN antipsychotics may tip the patient into the high dose range. Base line monitoring should be done if this is a possibility.
For patients with incapacity who are not complying with HDAT monitoring, ensure this is documented on HDAT Monitoring Form, in the case notes and that Alternative Heath Checks are carried out.
To seek pharmacy advice if necessary. 8.2.2 Community nurse Responsibilities
To be aware of the NHSL HDAT Guideline and it’s implications.
To be aware when a patient is on HDAT (see Tool 3 HDAT calculation).
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 13 of 31
To be aware of the additional monitoring necessary during HDAT (see Tool 2 HDAT monitoring Guide).
To liaise with psychiatrist if there are any concerns regarding ongoing monitoring, patient’s physical condition or mental health.
To carry out BP and temperature monitoring when local arrangements indicate this is the best use of local resources.
To assess for side effects using Antipsychotic Side Effect Rating Scales (Tool 6) when local arrangements indicate this is the best use of local resources.
To record when BP, temperature and side effect assessment have been carried out in patient’s notes or MiDIS. This should also be recorded on NEWS.
To either record BP, temperature and that side effect assessment has been done on the HDAT Monitoring Form (Tool 1) or contact psychiatrist to notify them of the information for this to be recorded.
Highlight any abnormalities to psychiatrist and/or GP.
8.2.3 General Practitioner Responsibilities
To be aware of the patients high dose antipsychotic status when notified by psychiatrist and the implications on this on patient health.
To consider the risks of initiating or stopping interacting medicines in patients who have a HDAT status. (Tool 4 – HDAT Guide to Interacting Medicines)
To carry out additional monitoring if this is deemed necessary when starting or stopping interacting medications
To be aware that for patients on more than one antipsychotic, increasing the dose of one these, may result in a high dose antipsychotic status. This can occur even if drugs are within the licensed maximum dose. (Tool 3 – HDAT calculation Tools).
To ensure any antipsychotics prescribed are included in repeat prescription list to trigger drug interactions on the prescribing system (Vision, Emas).
To use appropriate warning system on prescribing system to highlight to prescribers in GP practise that patient is on HDAT e.g. n Vision free form text in the yellow pop up box should be used.
To be aware that for patients for patients already on antipsychotics, commencing another antipsychotic result in a high dose antipsychotic status. This can occur even if drugs are within the licensed maximum dose. (Tool 3 – HDAT calculation Tools).
To liaise with psychiatrist or mental health team around the use of HDAT when necessary.
8.2.4 Footnote in relation to responsibilities It is acknowledged that HDAT monitoring is not covered by the GP contract. However in exceptional circumstances it may be in the patient’s best interests to attend the GP surgery for phlebotomy in relation to this. Any such requests should not be made without prior discussion and agreement with the patient’s GP. The additional information box in Tool 7 may be used to confirm any agreed arrangements.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 14 of 31
9 References
Royal College of Psychiatrists consensus Statement on High Dose Antipsychotic Treatment 2014 (CR190)
The Maudsley Prescribing Guidelines in Psychiatry 12th edition
British National Formulary Edition 70
Thanks to Nicola Barrie for proof reading this guideline
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018 Page 15 of 31
Tool 1 HDAT Monitoring Form firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018 Page 16 of 31
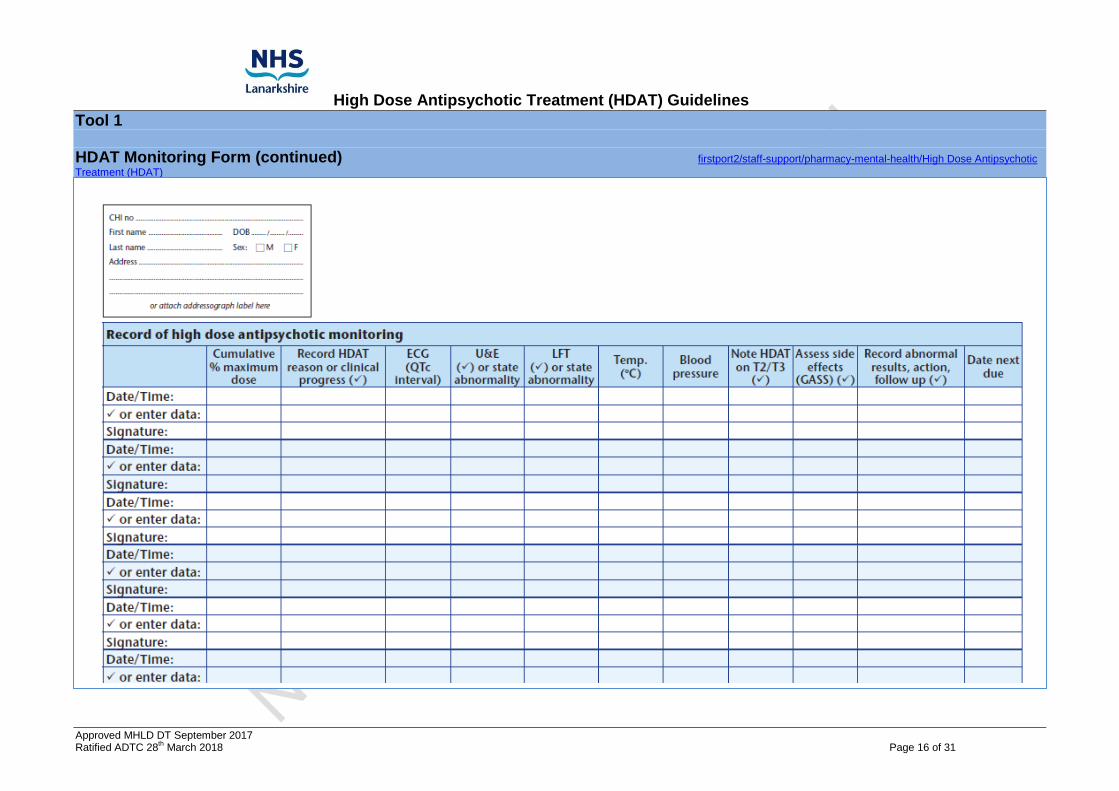
Tool 1 HDAT Monitoring Form (continued) firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic
Treatment (HDAT)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 17 of 31
Tool 2 HDAT Monitoring Form Guide firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
Consent Ensure consent is obtained from patient or welfare guardian. Consent form is available in Tool 5.
Risk Factors (see section 5.3.4 of HDAT guideline)
Long QT syndrome, and cardiac disease e.g. bradycardia, ischaemic heart disease, myocarditis, myocardial infarction, and left ventricular hypertrophy.
Hypokalaemia, hypomagnesaemia increase the risk of QTc prolongation and should be monitored and corrected before and during HDAT.
Renal and hepatic impairment may increase plasma levels of antipsychotics and should be monitored before and during HDAT.
The elderly, children, people who are malnourished, have learning disabilities or genetic syndromes that predispose to arrhythmia, may be at higher risk of QTc prolongation.
People who abuse alcohol or illicit drugs may be at higher risk of QTc prolongation.
Co-prescription of interacting medicines (see Tool 4).
Dose Details of antipsychotic dose should be entered when high dose monitoring is initiated and each time dose is changed.
Interacting Medicines Details of interacting medicines should be stated when HDAT monitoring is initiated, if a new interacting medicine is started or if the interacting medicine is discontinued/dose changed. See Tool 4 for examples of interacting medicines. Monitoring
Current cumulative dose should be entered each time a parameter is measured.
Clinical progress should be reviewed and documented; reason for HDAT or reason for dose change should be documented; continuation of HDAT justified.
Date that each parameter is monitored should be stated, and results followed up and recorded on form - state values or tick if normal; plan and record follow up if abnormal. Date parameter should next be monitored should be considered and recorded on form. Clinician entering data should sign form.
Additional monitoring for patients falling into the high dose range
ECG
LFTs
U&Es
Temperature
Blood Pressure
Side effects (GASS, Easy-Read GASS or LAPSAC- see Tool 6)
Clinical progress including cognitive function (particularly if also on anticholinergics)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 18 of 31
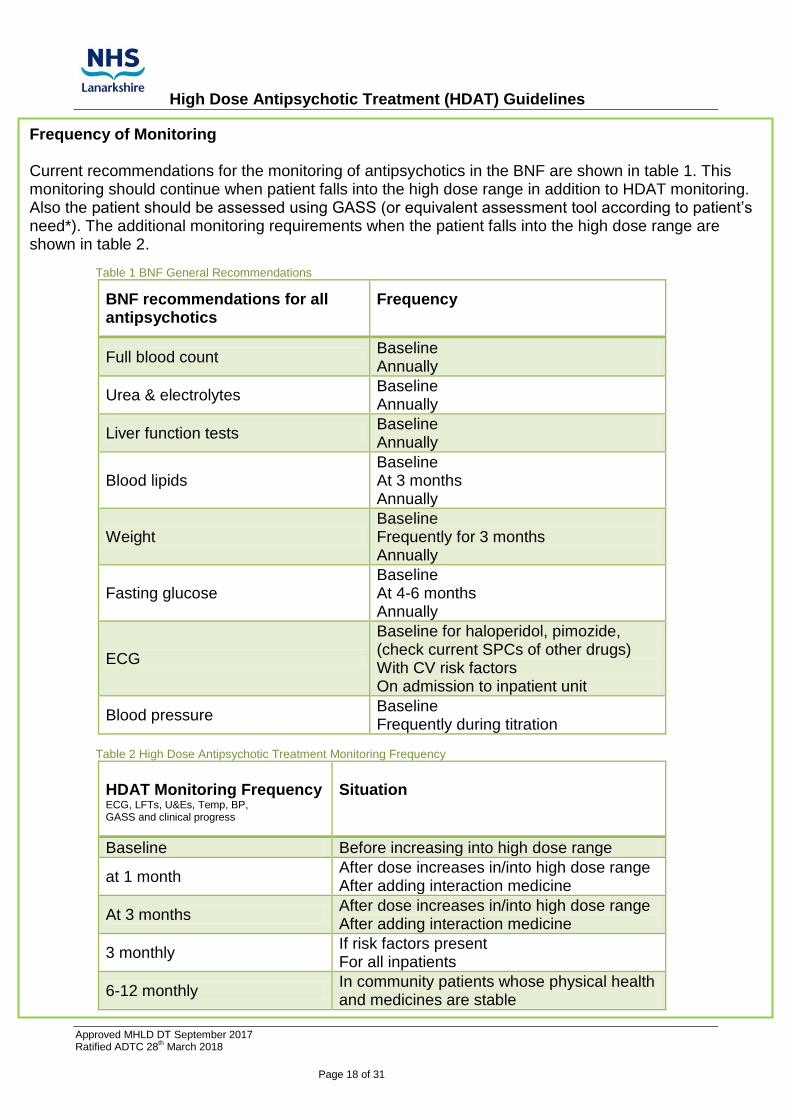
Frequency of Monitoring Current recommendations for the monitoring of antipsychotics in the BNF are shown in table 1. This monitoring should continue when patient falls into the high dose range in addition to HDAT monitoring. Also the patient should be assessed using GASS (or equivalent assessment tool according to patient’s need*). The additional monitoring requirements when the patient falls into the high dose range are shown in table 2.
Table 1 BNF General Recommendations
BNF recommendations for all antipsychotics
Frequency
Full blood count Baseline Annually
Urea & electrolytes Baseline Annually
Liver function tests Baseline Annually
Blood lipids Baseline At 3 months Annually
Weight Baseline Frequently for 3 months Annually
Fasting glucose Baseline At 4-6 months Annually
ECG
Baseline for haloperidol, pimozide, (check current SPCs of other drugs) With CV risk factors On admission to inpatient unit
Blood pressure Baseline Frequently during titration
Table 2 High Dose Antipsychotic Treatment Monitoring Frequency
HDAT Monitoring Frequency ECG, LFTs, U&Es, Temp, BP, GASS and clinical progress
Situation
Baseline Before increasing into high dose range
at 1 month After dose increases in/into high dose range After adding interaction medicine
At 3 months After dose increases in/into high dose range After adding interaction medicine
3 monthly If risk factors present For all inpatients
6-12 monthly In community patients whose physical health and medicines are stable
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 19 of 31
Tool 3
HDAT Calculation tools firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
High Dose Antipsychotics can occur from two scenarios
1. A single antipsychotic is prescribed at a dose higher than the maximum licensed daily dose for the age and clinical condition of the patient.
2. The cumulative % daily dose of two or more antipsychotics is more than 100% (using the percentage method*).
*the percentage method Convert the dose of each drug into the percentage of the maximum licensed dose for the patient’s age and clinical condition and add these together. A cumulative dose of more than 100% is HDAT. NB if the dose of any antipsychotic exceeds the maximum dose for that drug, it is an off-label use and local unlicensed use protocols should be followed. Situations where an antipsychotic is being used for children or adolescents, out with it’s the licensed indication, should be treated as HDAT. Off-label use and local unlicensed use protocols should also be followed. NHSL HDAT calculator For convenience the NHSL online High Dose Antipsychotic Calculator can be found via the following link. firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
SPC & BNF The maximum licensed dose of an antipsychotic can be found in the current BNF or SPC. BNF link https://www.medicinescomplete.com/mc/bnf/current/
SPC link http://www.medicines.org.uk/emc/
POMH-UK At the time of writing NHSL does not have access to the POMH-UK Ready Reckoner. If copies of these are used, the user must ensure they are accessing the most up to date version.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 20 of 31
Tool 4
HDAT Guide to Interacting Medicines
firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT) This appendix is intended to provide a guide to concomitant medicines which may increase the risks associated with HDAT and are therefore contraindicated, should be used with caution or require additional or more frequent monitoring. These medicines fall into 4 main categories
1. Concomitant drugs which prolong QTc interval e.g. methadone, tricyclic antidepressants, citalopram, domperidone, erythromycin, ketoconazole, clarithromycin
2. Drugs which increase plasma levels of antipsychotics by inhibition of CYP enzymes e.g. fluoxetine, fluvoxamine, paroxetine, valproate
3. Drugs which increase risk factors predisposing to QTc prolongation
- drugs causing bradycardia - drugs effecting electrolyte balance particularly K, Mg & Ca (check & correct low levels)
4. Stopping drugs which induce CYP enzymes (subsequent increase in plasma levels)
e.g. stopping smoking (increases clozapine, olanzapine), stopping/reducing carbamazepine/phenytoin
The following resources are available to check interactions for individual medication regimens. Consideration should be given to the risks associated with interacting medicines with regards frequency and timing of monitoring. Drug interaction resource links Stockley’s Drug Interactions knowledge network/medicinescomplete.com/stockey's drug interactions
BNF knowledge network/medicinescomplete/bnf/current/interactions
Summary of Product Characteristics www.medicines.org.uk/emc/
Credible meds website https://www.crediblemeds.org/new-drug-list/
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 21 of 31
HDAT Tool 5
Patient Consent to High Dose Antipsychotic Treatment
firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 22 of 31
HDAT Tool 6
Side Effect rating Scales
firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
Patient subjective side effect rating scales should be used to monitor for additional side effects and the effect these have on the patient’s quality of life. Monitoring side effects and addressing intolerances to medication can not only improve the patient’s physical health but can also help facilitate adherence to the medication. The preferred rating scale is the Glasgow Antipsychotic Side Effect Rating Scale (GASS). http://firstport2/staff-support/pharmacy-mental-health/Documents/Psychosis/GASS.pdf
GASS for clozapine provides a clozapine specific version of GASS. http://firstport2/staff-support/pharmacy-mental-health/Documents/Psychosis/GASSforClozapine.pdf
There is also an easy read version of GASS and GASS for clozapine which may be more suitable for some patients including those with learning disabilities, learning difficulties, and those whose first language is not English. Easy Read GASS http://firstport2/staff-support/pharmacy-mental-health/Documents/Psychosis/PILGASS.pdf
Easy Read GASS for Clozapine http://firstport2/staff-support/pharmacy-mental-health/Documents/Psychosis/PIL GASS for clozapine.pdf
For people who have severe communication problems and cannot use the easy read GASS, LAPSAC (Lanarkshire Antipsychotic Side Effect Assessment in Communication Difficulties) may be used. This is a side effect assessment tool, that is based on LUNSERS, and can be used as a prompt when discussing side effects with carers. As this is a reflection on the carers observations, it may not identify all side effects experienced by the patient. However it may help the mental health clinician identify some of the more subjective side effects patients with more severe communication difficulties may be experiencing. http://firstport2/staff-support/pharmacy-mental-health/Documents/Psychosis/LAPSAC.pdf If there is difficulty for an Adult with Incapacity, being treated with HDAT, in complying with monitoring, this should be documented in the patient’s notes each time. Alternative health recordings should be made as detailed in the document found at link below. firstport2/staff-support/pharmacy-mental-health/HighDoseAntipsychoticTreatment(HDAT)
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 23 of 31
HDAT Tool 7
GP Information Letter
firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
Dear Regarding I recommend that the following antipsychotic treatment be prescribed for this patient.
Name of antipsychotic Daily dose % of maximum dose Cumulative % max
The above dose(s) fall into the High Dose Antipsychotic range either because the maximum licence dose has been exceeded or the cumulative % of the maximum licence dose of two or more antipsychotic drugs is greater than 100%. Please refer to the NHSL High Dose Antipsychotic Treatment (HDAT) Guidance, on the clinical guidelines website, for more information. I have obtained consent from the patient or his/her legal representative and the patient is being monitored according to the NHSL HDAT guidance. A copy of the consent form is attached. MHLD DT suggest that GP’s use a warning box in the patients e-notes on the GP prescribing system, e.g. the yellow free-text pop up box on vision, to highlight the patient’s high dose antipsychotic status. HDAT increases the risks of side effects including QTc prolongation. Consideration has been given to the current medicines that I am aware of, but please be aware that additional changes to the patient’s general medicines may have an impact on the risks associated with HDAT. Tool 4 in the NHSL HDAT Guidance Toolbox provides information and links to help identify this. The GP prescribing systems will highlight interactions if the antipsychotic is on the repeat list. Consideration should be given to U&E and/or ECG monitoring soon after initiating an interacting medicine to minimise risk to patient’s physical health. Please liaise with the mental health team to communicate the results of any additional monitoring. firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
Thank you Yours Faithfully
Name of GP
Name of patient
CHI number
Signature of consultant/SAS
Print name of consultant/SAS Date
Additional information if relevant
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 24 of 31
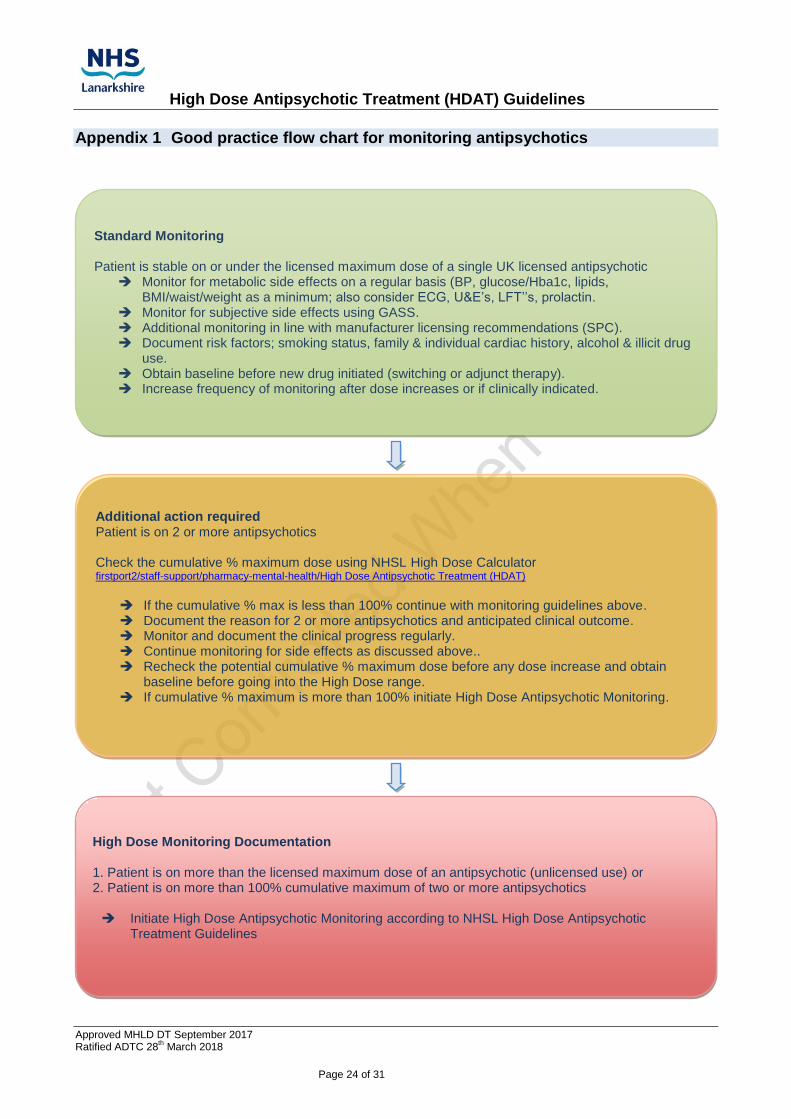
Appendix 1 Good practice flow chart for monitoring antipsychotics
High Dose Monitoring Documentation 1. Patient is on more than the licensed maximum dose of an antipsychotic (unlicensed use) or 2. Patient is on more than 100% cumulative maximum of two or more antipsychotics Initiate High Dose Antipsychotic Monitoring according to NHSL High Dose Antipsychotic
Treatment Guidelines
Additional action required Patient is on 2 or more antipsychotics Check the cumulative % maximum dose using NHSL High Dose Calculator firstport2/staff-support/pharmacy-mental-health/High Dose Antipsychotic Treatment (HDAT)
If the cumulative % max is less than 100% continue with monitoring guidelines above. Document the reason for 2 or more antipsychotics and anticipated clinical outcome. Monitor and document the clinical progress regularly. Continue monitoring for side effects as discussed above.. Recheck the potential cumulative % maximum dose before any dose increase and obtain
baseline before going into the High Dose range. If cumulative % maximum is more than 100% initiate High Dose Antipsychotic Monitoring.
Standard Monitoring Patient is stable on or under the licensed maximum dose of a single UK licensed antipsychotic
Monitor for metabolic side effects on a regular basis (BP, glucose/Hba1c, lipids, BMI/waist/weight as a minimum; also consider ECG, U&E’s, LFT’’s, prolactin.
Monitor for subjective side effects using GASS. Additional monitoring in line with manufacturer licensing recommendations (SPC). Document risk factors; smoking status, family & individual cardiac history, alcohol & illicit drug
use. Obtain baseline before new drug initiated (switching or adjunct therapy). Increase frequency of monitoring after dose increases or if clinically indicated.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 25 of 31
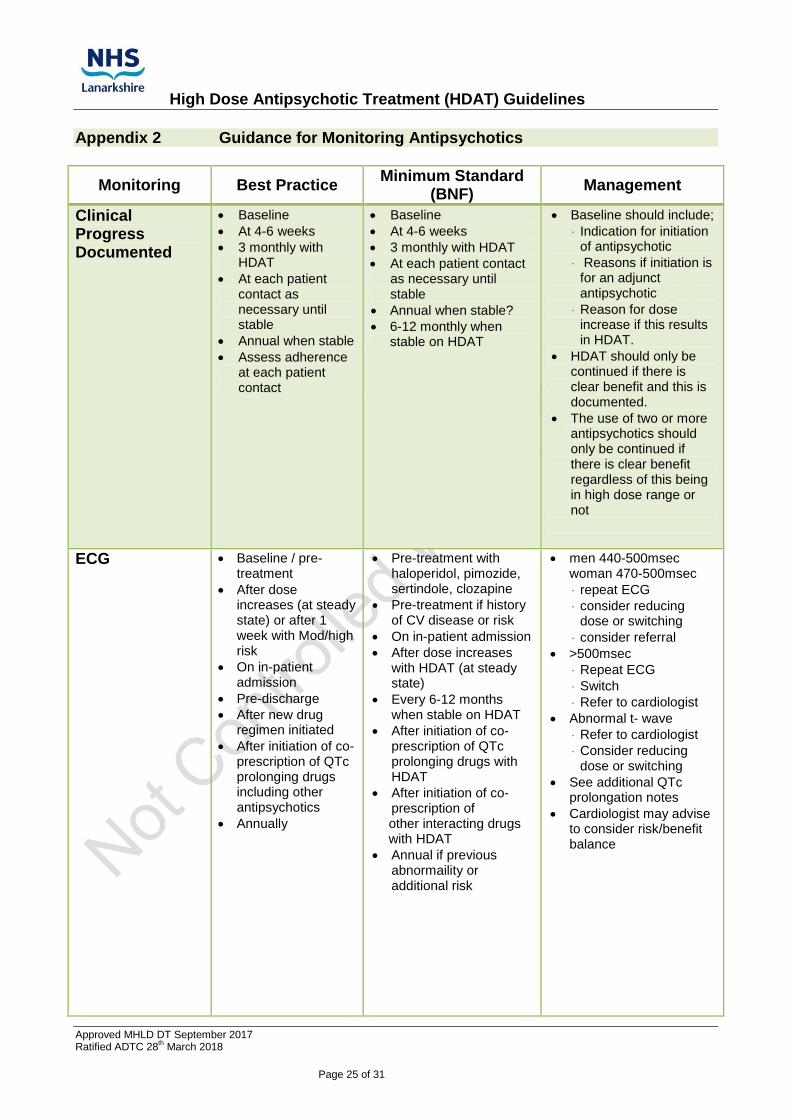
Appendix 2 Guidance for Monitoring Antipsychotics
Monitoring Best Practice Minimum Standard
(BNF) Management
Clinical Progress Documented
Baseline
At 4-6 weeks
3 monthly with HDAT
At each patient contact as necessary until stable
Annual when stable
Assess adherence at each patient contact
Baseline
At 4-6 weeks
3 monthly with HDAT
At each patient contact as necessary until stable
Annual when stable?
6-12 monthly when stable on HDAT
Baseline should include;
Indication for initiation of antipsychotic
Reasons if initiation is for an adjunct antipsychotic
Reason for dose increase if this results in HDAT.
HDAT should only be continued if there is clear benefit and this is documented.
The use of two or more antipsychotics should only be continued if there is clear benefit regardless of this being in high dose range or not
ECG Baseline / pre-treatment
After dose increases (at steady state) or after 1 week with Mod/high risk
On in-patient admission
Pre-discharge
After new drug regimen initiated
After initiation of co-prescription of QTc prolonging drugs including other antipsychotics
Annually
Pre-treatment with haloperidol, pimozide, sertindole, clozapine
Pre-treatment if history of CV disease or risk
On in-patient admission
After dose increases with HDAT (at steady state)
Every 6-12 months when stable on HDAT
After initiation of co-prescription of QTc prolonging drugs with HDAT
After initiation of co-prescription of other interacting drugs with HDAT
Annual if previous abnormaility or additional risk
men 440-500msec woman 470-500msec
repeat ECG
consider reducing dose or switching
consider referral
>500msec
Repeat ECG
Switch
Refer to cardiologist
Abnormal t- wave
Refer to cardiologist
Consider reducing dose or switching
See additional QTc prolongation notes
Cardiologist may advise to consider risk/benefit balance
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 26 of 31
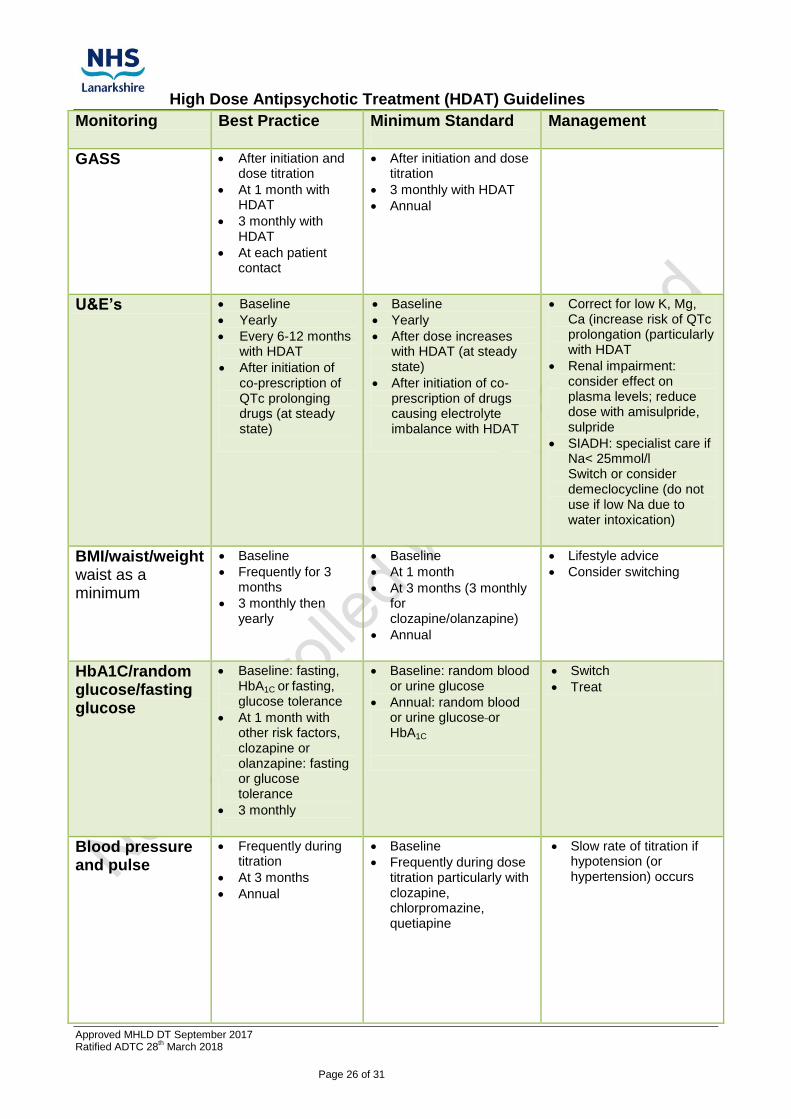
Monitoring Best Practice Minimum Standard
Management
GASS
After initiation and dose titration
At 1 month with HDAT
3 monthly with HDAT
At each patient contact
After initiation and dose titration
3 monthly with HDAT
Annual
U&E’s Baseline
Yearly
Every 6-12 months with HDAT
After initiation of co-prescription of QTc prolonging drugs (at steady state)
Baseline
Yearly
After dose increases with HDAT (at steady state)
After initiation of co-prescription of drugs causing electrolyte imbalance with HDAT
Correct for low K, Mg, Ca (increase risk of QTc prolongation (particularly with HDAT
Renal impairment: consider effect on plasma levels; reduce dose with amisulpride, sulpride
SIADH: specialist care if Na< 25mmol/l Switch or consider demeclocycline (do not use if low Na due to water intoxication)
BMI/waist/weight waist as a minimum
Baseline
Frequently for 3 months
3 monthly then yearly
Baseline
At 1 month
At 3 months (3 monthly for clozapine/olanzapine)
Annual
Lifestyle advice
Consider switching
HbA1C/random glucose/fasting glucose
Baseline: fasting, HbA1C or fasting, glucose tolerance
At 1 month with other risk factors, clozapine or olanzapine: fasting or glucose tolerance
3 monthly
Baseline: random blood or urine glucose
Annual: random blood or urine glucose or HbA1C
Switch
Treat
Blood pressure and pulse
Frequently during titration
At 3 months
Annual
Baseline
Frequently during dose titration particularly with clozapine, chlorpromazine, quetiapine
Slow rate of titration if hypotension (or hypertension) occurs
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 27 of 31
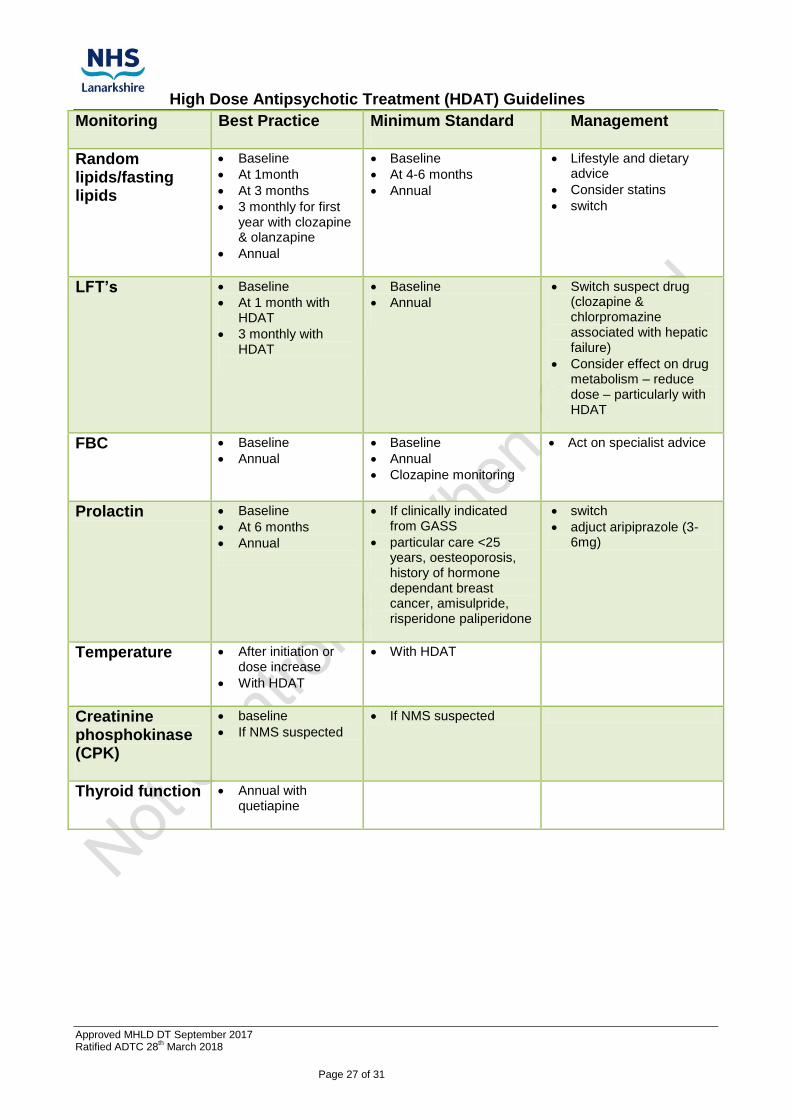
Monitoring Best Practice Minimum Standard
Management
Random lipids/fasting lipids
Baseline
At 1month
At 3 months
3 monthly for first year with clozapine & olanzapine
Annual
Baseline
At 4-6 months
Annual
Lifestyle and dietary advice
Consider statins
switch
LFT’s Baseline
At 1 month with HDAT
3 monthly with HDAT
Baseline
Annual
Switch suspect drug (clozapine & chlorpromazine associated with hepatic failure)
Consider effect on drug metabolism – reduce dose – particularly with HDAT
FBC Baseline
Annual
Baseline
Annual
Clozapine monitoring
Act on specialist advice
Prolactin Baseline
At 6 months
Annual
If clinically indicated from GASS
particular care <25 years, oesteoporosis, history of hormone dependant breast cancer, amisulpride, risperidone paliperidone
switch
adjuct aripiprazole (3-6mg)
Temperature After initiation or dose increase
With HDAT
With HDAT
Creatinine phosphokinase (CPK)
baseline
If NMS suspected
If NMS suspected
Thyroid function Annual with quetiapine
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 28 of 31
Appendix 3 Royal College of Psychiatrists Consensus Statement on high dose antipsychotic medication (CR190) Outlined below are the key points relating to the RCPsych Consensus Statement that was published in November 2014. The full consensus statement can be found at http://www.rcpsych.ac.uk/usefulresources/publications/collegereports/cr/cr190.aspx Summary While there is little convincing evidence that off-label prescription of doses of antipsychotic medication above the licensed dosage range has any therapeutic advantage in any clinical setting, there is clear evidence for a greater side-effect burden and the need for appropriate safety monitoring. The key recommendation is that any prescription of high-dose antipsychotic medication should be seen as an explicit, time-limited individual trial with a distinct treatment target. There should be a clear plan for regular clinical review including safety monitoring. The high-dose regimen should only be continued if the trial shows evidence of benefit that is not outweighed by tolerability or safety problems. High Dose Definition A total daily dose of a single antipsychotic which exceeds the upper limit stated in the SPC or BNF with respect to the age of the patient and the indication being treated, and a total daily dose of two or more antipsychotics which exceeds the SPC or BNF maximum using the percentage method* *For percentage method- covert the dose of each drug into a percentage of the maximum licensed dose and add these together. A cumulative dose of more than 100% is high dose Rational for high dose antipsychotic treatment The only rational for high dose antipsychotics is in a small number of patients in whom pharmacokinetic differences mean there are low plasma levels and insufficient receptor blockade of D2 receptors at standard doses. However routine drug plasma level monitoring is not yet routine practise and so the effectiveness of this in predicting who may benefit from HDAT has not been established. 5.4 First episode - evidence and clinical implications
There is no evidence that high-dose antipsychotic use is beneficial for patients with first-episode psychosis and such use should be avoided.
Antipsychotic polypharmacy should be avoided. ‘Top up’ oral antipsychotic doses for patients on depot/long-acting injection medication should be used only as a short term measure.
Where antipsychotic response is poor, switching medication should be the preferred course of action, rather than increasing doses above BNF limits.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 29 of 31
Short-term benzodiazepine prescription has been suggested as preferable for the sedation of patients with aggression at this early stage of the illness.
Clozapine should be considered in patients with first-episode psychosis who fail to show complete remission following adequate trials of two different antipsychotics.
Acute psychotic Episode - evidence and clinical implications
For the majority of people with acute psychotic illness, the target dose for effective treatment is likely to be below the licensed maximum.
The local implementation of current national guidelines (see above) should include clear protocols for the management and treatment of acute psychotic episodes. Adherence to such protocols should minimise the use of high-dose antipsychotic medication.
Initiation of antipsychotic drug treatment in the first episode or in a subsequent untreated episode after a drug-free period should not involve starting more than one antipsychotic at the same time.
Relapse prevention - evidence and clinical implications
There does not seem to be any justification in the published literature for the use of highdose antipsychotic medication for relapse prevention in schizophrenia.
There is no convincing evidence that incremental increase of antipsychotic dose at times of psychotic relapse, with subsequent continuation of the new, higher dose, provides better relapse prevention in the long term
Acute violence and emergency tranquillisation - evidence and clinical implications
Rapid tranquillisation should only be used when careful clinical judgement is that the associated risks are less than the risks of not using rapid tranquillisation or employing non pharmacological methods alone to manage disturbance (Coburn & Myck, 2009; Rossi & Swan, 2010). Lack of previous exposure to antipsychotic medication must be considered as well as possible illicit substance use. Another risk factor to be taken into account is a family history of sudden cardiac death (NICE, 2013).
The aim of rapid tranquillisation is not to induce sleep or unconsciousness; the patient should be sedated but still able to respond to communication throughout and to participate in further assessment and treatment and (Battaglia et al, 2003; Citrome, 2004). The choice of medication and dosage should be individually tailored to the patient.
The patient must be informed that medication is going to be administered and given the opportunity to accept oral medication voluntarily at all stages.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 30 of 31
Given the lack of evidence for use of highdose medication and the proven associated risks, the lowest dose compatible with effective treatment should be used and BNF maximum doses (over a 24-hour period) only exceeded in rare circumstances and with caution, increased monitoring, and the advice of a consultant psychiatrist.
The indication for which any p.r.n. medication is prescribed should be explicit and clearly documented and all p.r.n. medications should be reviewed on a regular basis.
Oral and intramuscular medication should be prescribed separately.
As few medicines as possible should be used.
The use of combinations from the same class of medicine should be avoided wherever possible.
Patients should be regularly monitored for clinical benefit and side effects from administered medication
Persistent aggression - evidence and clinical implications
The goal of long-term treatment is to decrease the frequency and intensity of future episodes of agitation or aggression.
The perceived clinical driver for the aggressive behaviour (such as being delusionally driven or related to impulsivity or co-morbid personality disorder) might dictate which medication is chosen in the first instance.
It is important to address the multi-factorial aetiology of violent behaviour, including any co-morbid issues and environmental factors that contribute to increased risk.
There is no justification in the published literature for high-dose antipsychotics in the treatment of persistent aggression. Regular and frequent review of treatment plans in relevant clinical settings might allow for the safe and appropriate use of antipsychotic medication without any increase in violence (Herlihy & Smith, 2010; Choong et al, 2011).
When prescribing medication to target the medium- or long-term risk of violence, the clinician should bear in mind the limited evidence and only prescribe medication after a thorough multidisciplinary assessment, risk– benefit evaluation and careful review of effects and side-effects.
Continuing adherence to prescribed medication is especially important in the long-term reduction of aggressive behaviour (Swanson et al, 2004, 2008; Arango et al, 2006)
Of the available antipsychotic medications, clozapine has the best evidence base for reducing the risk of violence in people with schizophrenia in the long term. This treatment might have a specific effect on symptoms related to aggression.
High Dose Antipsychotic Treatment (HDAT) Guidelines
Approved MHLD DT September 2017 Ratified ADTC 28
th March 2018
Page 31 of 31
Schizophrenia failing to respond to standard antipsychotic regimens - evidence and clinical implications
Treatment-resistant schizophrenia is usually defined as illness that has shown an insufficient response to adequate trials, in terms of dose, duration and adherence, of at least two different antipsychotic medications. NICE (2009) guidelines indicate that at least one of the drugs should be a non-clozapine, second-generation antipsychotic.
There is no convincing evidence that antipsychotic dosage higher than the maximum licensed dose is more effective than standard dosage for treatment-resistant schizophrenia.
Before resorting to high dosage, evidence based strategies for treatment-resistant illness should be exhausted, including optimised use of clozapine.
If a clinician initiates a high-dose antipsychotic treatment regimen, this should be as a limited therapeutic trial, with dosage returned to conventional levels after a 3-month period unless the clinical benefits evidently outweigh the risks.
The potential side-effects of high-dose antipsychotic regimens should be monitored
appropriately, by systematic enquiry, physical examination, ECG and appropriate haematological investigations







