
Kiren Mitruka, MD, MPH
Medical Officer- care and treatment
Division of Viral Hepatitis
Centers for Disease Control and Prevention
Hepatitis B and C Prevention Strategies,
United States
1st International Meeting on Hepatitis Cure and Eradication
November 6, 2014
Division of Viral Hepatitis
National Center for HIV/AIDS, Viral Hepatitis, STD & TB Prevention

Persons Living With Viral Hepatitis B and C, United States
Virus
Prevalence % Unaware of
infection
Deaths (2006)
Hepatitis B 800,000 – 1.4
million ~ 65% 3,000
Hepatitis C 3-4 million 50-75% 15,000
2

Mortality associated with Hepatitis B, Hepatitis C, and HIV United States,
1999–2010
K Ly et al, Ann Intern Med 2012; 156:271-8
0
1
2
3
4
5
6
7
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rat
e p
er
10
0,0
00
Pe
rso
ns
Year
Hepatitis B
Hepatitis C
HIV

United States Viral Hepatitis Action Plan, 2011 (updated 2014) : Priority Areas
Educate providers and communities
to reduce health disparities
Improve testing, care and treatment
Strengthen surveillance
Eliminate transmission of vaccine-
preventable hepatitis
Reduce viral hepatitis caused by drug-use
behaviors
Protect patients and workers from healthcare-
associated hepatitis

Overview of Hepatitis B Virus Prevention and Control
Vaccination
All infants, beginning at birth
All children and adolescents (through age 18)
Adults in high-risk groups (e.g., STD, MSM, IDU, HIV-infected)
Reducing perinatal transmission Screening for HBsAg* in pregnancy and post exposure prophylaxis of newborn
Screening for infection
High risk groups
Foreign-born persons from countries with prevalence ≥2%
Education and raising awareness
Testing and linkage to care programs
* Hepatitis B surface antigen

Hepatitis B Vaccine Policy and Rates of
Acute Hepatitis B, United States,1980–2011
6
0
2
4
6
8
10
12
14
Cas
es/
10
0,0
00
po
pu
lati
on
Year
All US infants,
1991
Ages 0-18 years, 1999
Adults <60 years with Diabetes
Birth dose, 2006
High-risk groups,*
1982
Infants of HBsAg-positive women, 1984
*Health care providers, MSM, IDU, hemodialysis patients, household & sexual partners of persons with chronic HBV,
persons in certain institutional settings, e.g., inmates of long-term correctional facilities.
Source: National Notifiable Disease Surveillance System (NNDSS)
Universal maternal
HBsAg testing 1988

Estimated Number of Births to HBsAg-Positive Pregnant Women
U.S., 1993-2009
0
10000
20000
30000
Nu
mb
er
of
liv
e b
irth
s
Year
Smith, E.A., et al., The national Perinatal Hepatitis B Prevention Program, 1994-2008. Pediatrics, 2012. 129(4): p. 609-16. 7
19,048
24,804

U.S. Perinatal Hepatitis B Prevention Program
Created in 1990 to assist in elimination of
perinatal hepatitis B transmission
Programs in 64 public health jurisdictions
50 states, 6 cities, 8 territories and freely associated
island nations
Fosters collaboration with healthcare providers, laboratories,
hospitals, nursery staff, and families
8
http://www.cdc.gov/hepatitis/HBV/PerinatalXmtn.htm

Perinatal Hepatitis B Prevention
Screen all pregnant women
First prenatal visit and retest at or prior to
delivery if at risk
Link to care and treatment if infected
Post-exposure prophylaxis to newborn
HBIG and single antigen Hepatitis B vaccine
within 12 hours of birth
Timely completion of HBV vaccine series
Post-vaccination serologic testing 1-2 months
after completion of vaccine series, not before
9 months of age
Revaccinate if not protected
• HBsAg-negative and antibody to
hepatitis B surface antigen (≥10mlU/mL)
9
MMWR Dec 2005

Percentage of Infants of HBsAg*-Positive
Mothers Completing Case Management,
CDC Perinatal Program, 1993–2009
* Hepatitis B surface Antigen.
Data Source: National Center for Immunization and Respiratory Disease, CDC, as of 8/2013
0
20
40
60
80
100
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
Pe
rce
nt
infa
nts
Year
Vaccine/HBIG at birth
3 doses by 6-8 months
Post-vaccination testing
95%
73%
58%

CDC and USPSTF* Recommendations
for Hepatitis B Testing
Populations with >2% prevalence1,2
Foreign born
US-born to parents born in high
prevalence regions (>8%)
Other: MSM, IDU, HIV + persons, household contacts or sexual partners of
HBV+
Candidates for immunosuppression therapy
Screening and treatment cost effective
$29,230/QALY 3
* US Preventive Services Task Force 1 MMWR 2008; 57 (No. RR-8):1-20; 2 LeFevre Screening for Hepatitis B Virus Infection in Nonpregnant Adolescents and Adults: U.S.
Preventive Services Task Force Recommendation Statement, May 2014 3Eckman, MH, CID 2011:52 11

Raising Awareness
http://www.cdc.gov/knowhepatitisb/materials.htm 12
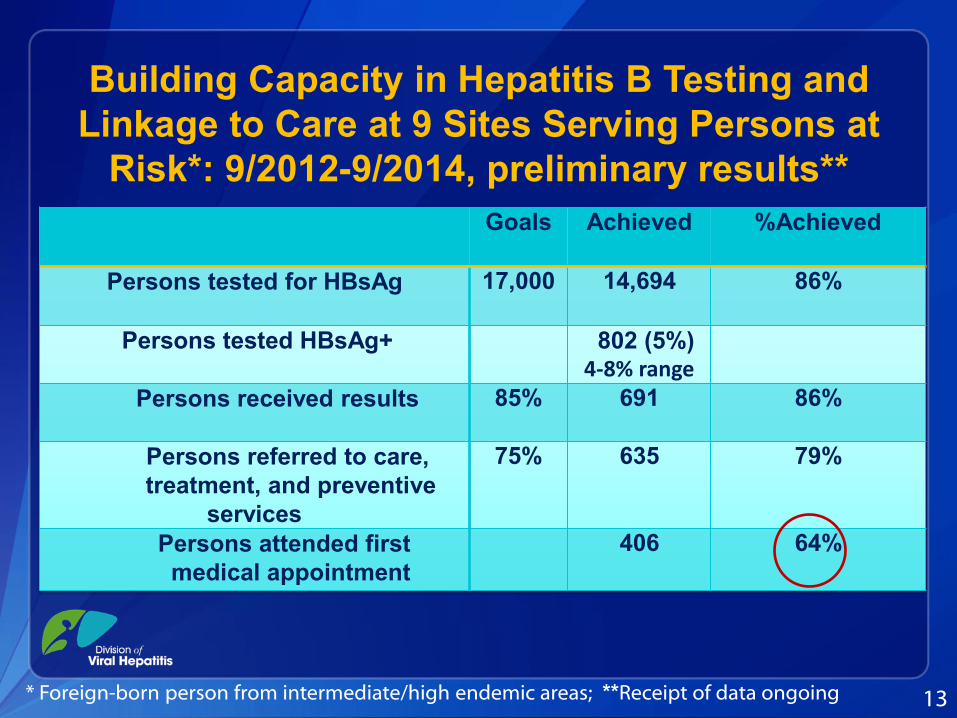
Building Capacity in Hepatitis B Testing and
Linkage to Care at 9 Sites Serving Persons at
Risk*: 9/2012-9/2014, preliminary results**
Goals Achieved %Achieved
Persons tested for HBsAg
17,000 14,694 86%
Persons tested HBsAg+
802 (5%) 4-8% range
Persons received results
85% 691 86%
Persons referred to care,
treatment, and preventive
services
75% 635 79%
Persons attended first
medical appointment
406 64%
13 * Foreign-born person from intermediate/high endemic areas; **Receipt of data ongoing

Community-Based Hepatitis B Programs 10/2014–9/2016
Goal: To improve the capacity of healthcare
providers to identify and link foreign-born
individuals with chronic hepatitis B to care
14
Number of awards 3
Eligibility Established coalition of public
health, academic centers, and
primary care providers (PCP)
One year award amount $300,000
Project period 2 years
Total project period funding $1.8 million
CDC RFA- PS 14-1414

Hepatitis C Virus: Prevention and Control
Primary Prevention (prevent infection)
Screen blood supply
Ensure safe therapeutic injection practices
Practice universal precautions in medical practices
Counsel infected person to reduce transmission risk behavior
Reduce illicit drug use and ensure safety (e.g., needle exchange)
Secondary prevention (prevent disease)
Test to detect active infection
Counsel to avoid alcohol intake
Vaccinate for hepatitis A and B
Treat with antivirals
Adapted from Thomas D. Nature Medicine July 2013 : ( 19) 850-859

Impact of Prevention Measures
on Hepatitis C Virus (HCV) Infection in United States
Alter MJ JAMA 1990; Jagger J, J infect Dis Pub Health 2008; CDC.gov/hepatitis;
0
2
4
6
8
10
12
14
16
18
20
Anti-HCV test licensed
1992
1986 Indirect blood screening for HCV
and HIV prevention measures
Needle stick Safety
and Prevention Act
2001
Year
Discovery
of HCV
1989
22,000 new acute HCV cases reported in 2012

Recent Increases in HCV Infection
17
Between 2007 and 2012 50% increase in case reporting
200% increase in 17 states
Risk factors • ~ 70% persons who inject drugs
• Previous oral prescription
narcotic use
• Equally male to female
• Young, ages 18 to 29 years
• White
• Rural and suburban
Zibbell J, et al. AJPH 2014; Suryprasad AG, et al. CID 2014

Broader HCV Testing Recommendation in 2012 One time Test for Persons Born 1945 –1965
Birth cohort represent
81% of adult chronic infections
73% HCV deaths
Prevalence ~6 times higher (3.29%
vs 0.55% other ages)
No reported risk factors: 44%
Benefit of treatment, with SVR
reducing
Liver cancer risk: 70%
All-cause mortality: 50%
MMWR August 17, 2012 / 61(RR04);1-18 ; Armstrong, et al. Ann Int Med. 2006.; Kramer, Et al., Hepatology 2011; Backus LI, Clin Gastroenterol Hepatol. 2011; Morgan RLAnn Intern Med. 2013

USPSTF* and CDC Recommendations for HCV Testing
One time screening test for persons born 1945-1965
without ascertainment of risk (USPSTF Grade B)
Major risk
Past or present injection drug use
Other risks
Received blood/organs prior to June 1992
Received blood products made prior to 1987
Ever on chronic hemodialysis
Infants born to HCV infected mothers
Intranasal drug use
Unregulated tattoo
History of incarceration
Medical
Persistently elevated ALT
HIV
* US Preventive Services Task Force . Updated recommendation for screening June 2013
MMWR Aug 2012.; Moyer VA, Ann Int Med 2013. *

Health Impact of Birth Cohort Recommendations
Outcome Birth Cohort Testing with Therapy
PegIFN-Riba + Telapravir
Additional identified cases 809,000
Cirrhosis cases averted 203,000
Decompensated cirrhosis
cases averted 74,000
Hepatocellular carcinoma
cases averted 47,000
Transplants averted 15,000
Deaths from hepatitis C virus
averted 121,000
Medical costs averted $2.5B
Cost/QALY gained $35,700
Rein DB, Annals of Internal Medicine. 2011.

Know More Hepatitis Campaign Strategies
National Educational Campaign
News/Media Advocacy
Opinion Leader Outreach
Professional Education
Partnership
Engagement
Social
Media
Broadcast
(Radio/ TV Public Service
Advertising)
Digital Media

Educating Communities
22
Airport Diorama
Highway Billboard

Treatment as Prevention Strategy to reduce HCV Prevalence
Martin NK et al . Hepatology 2013
23

Cure and Prevention (CaP): Models for Persons Who Inject Drugs (PWID)
Model under development to estimate the impact of targeted
treatment on incidence and prevalence associated with
prevention strategies*
Targeted treatment to active injectors within social networks
Assess reductions in morbidity & mortality and reinfection rates
Use existing datasets to model case-studies for U.S. settings
Rural versus urban
New treatment and associated costs
Develop estimates of cost, and cost-effectiveness to achieve
desired health outcomes
24 * Includes concurrent evidence-based interventions needles exchange and opioid agonist treatment

Building Capacity in Hepatitis C Testing and
Linkage to Care at 22 Sites Serving Persons
at Risk*: 9/2012–9/2014, preliminary results*
Continuum of care Goals Achieved %Achieved
Persons tested for HCV Antibody
and HCV RNA
47,400 43,768 92%
Persons tested anti-HCV + 5,796 (13%)
Range 3-51%
Persons received RNA test 85% 3,557 61%
Persons received RNA
results
85% 2,189 83%
Persons referred to care,
treatment, and preventive
services
75% 2,078 79%
Persons began treatment 15% 70 3%
25 *Receipt of data ongoing

Community-based Programs to Test and Cure Hepatitis C: 9/2014 –9/2018
Goal: develop package of services to improve
healthcare capacity to test and cure
26
Number of awards 3
Eligibility Established coalition of
public health, academic
centers, and primary care
Average one year award amount $1.5 million
Project period 4 years
Total project period funding $20 million
CDC RFA- PS 14-1413

Community-based Programs to Test and Cure
Hepatitis C: Outcomes
Initial targets
An annual increase in testing, diagnosis, and cure by of ≥ 50%, with at least
• 10,000 persons tested
• 2000 persons diagnosed
• 2500 cured
Targets to be revisited during project period

Community-based Programs to Test and Cure
Hepatitis C: Package of Services
Identify and educate target population
Incorporate HCV testing among in primary care practices
Implement regular consultation of primary care provider with
HCV specialists
Case management
Monitor outcome and community impact via data system
Leverage Affordable Care Act: insurance enrollment, free
testing, and improve quality of care through use of EMR

American Medical Association Performance Measures Updated (2013)
Screening
One-time screening: patients at risk (injection drug use ever, blood
transfused prior to 1992, or born during 1945–1965)
Annual HCV screening: patients who are active injection Drug Users
Care and treatment
Referral to treatment for patients identified with HCV Infection
Sustained Virologic Response (SVR)
Confirmation of Hepatitis C viremia
Hepatitis C RNA and genotype testing before initiating treatment
HCV RNA testing between 4-12 weeks after treatment start
Discontinuation of antiviral therapy if inadequate response
Additional performance measures on prevention (vaccination, alcohol
consumption counseling, HCC screening)
29

Viral Hepatitis Prevention in the United States
Improve primary prevention: reduce transmission
Strengthen the continuum of HBV and HCV testing,
care, and treatment
Enhance surveillance to detect and interrupt
transmission
Build evidence base for policy development and to
guide interventions
30







