
4/17/2017
1
Illinois Chapter of the AAP Autism, Behavior, and Complex
Medical Needs – Downstate Conference
Erica D. Wiebe, MD 4/28/2017
I declare that neither I, or my immediate family, have a financial interest or other relationship with any manufacturer/s of a commercial product/s or service/s which may be discussed at the conference.
Understand the importance of medical, legal, educational and social transition for youth with special healthcare needs
Appreciate the current state of healthcare transition for special needs patients in the US
Recognize the various parent, patient, and provider perspectives surrounding transition

4/17/2017
2
Acknowledge the components of the transition process
Consider potential process improvements or future directions for current transition models
“You grow up the day you have your first real laugh -- at yourself.”
― Ethel Barrymore
Transition is the deliberate process of moving seamlessly from child-oriented healthcare to adult-oriented healthcare.
Components
Endowment of Self-Determination
Preparation for Adult Health Care
Provisions for Work/Independence
Inclusion in Community Life

4/17/2017
3
Good Preparation
Person-Centered Planning
Flexible Timing
Efficient Care Coordination
Joint Transition Efforts
An estimated 4.5 million or 18.4 % of United States youth age 12-18 have special healthcare needs
Prevalence is double that of young children age 0-5
More than 33 % of those youth have an emotional, behavioral, or developmental condition
More than ¼ with those conditions experience persistent and significant impact on their activities as a result of their condition
Fewer than ½ of youth with special needs have a designated medical home
Youth with special healthcare needs (YSHCN) are at greater risk of unmet medical needs
Limited access to mental health services
Rates of risky behaviors (alcohol and tobacco use, drug use, and unprotected sexual activity) are similar to or greater than their peers in the general population
Medical needs shift with evolution into adulthood

4/17/2017
4
Failure to successfully transition contributes to significant gaps in healthcare
Negative health outcomes associated with risky behaviors
Increases in hospital admissions secondary to
Infection
Equipment failure
Poor medication compliance
Higher clinic “no show” rates
Increased healthcare costs
Increased life expectancy < 1/3 of patients with spina bifida survived beyond age
20 in 1970 vs >80% current survival rates
Rise in rates of many ND disorders
1 in 9 pregnancies results in preterm birth
Autism Spectrum Disorder currently affects 1 in 68 children
2010 survey of the Association of American Medical Colleges Except for neonatology, every pediatric specialty has
inadequate numbers of physicians to meet patient needs
Successful
Transition
Patient
Adult
Provider
Parents/
Caregivers
Pediatric
Provider
4/17/2017
5
Self Reported Priorities
Career development
Independent living skills
Finding quality medical care
Emergency preparedness
Legal rights and transitions
Self protection
Financing for education
Self Reported Concerns Lack of understanding of their medical condition by
adult providers
Health insurance continuation into adulthood
Dealing with emotional attachments Their own
Their parents
The pediatric provider
Feel surrounded by support now but aren’t aware of what’s available in the future
The vast majority do not feel “listened to”
Many express worries similar to their general population peers
Adult romantic relationships
Adult friendships
Findings jobs
Fitting in at the community level
Wanting resources so they don’t always have to turn to their parents for help
Avoiding future planning
4/17/2017
6
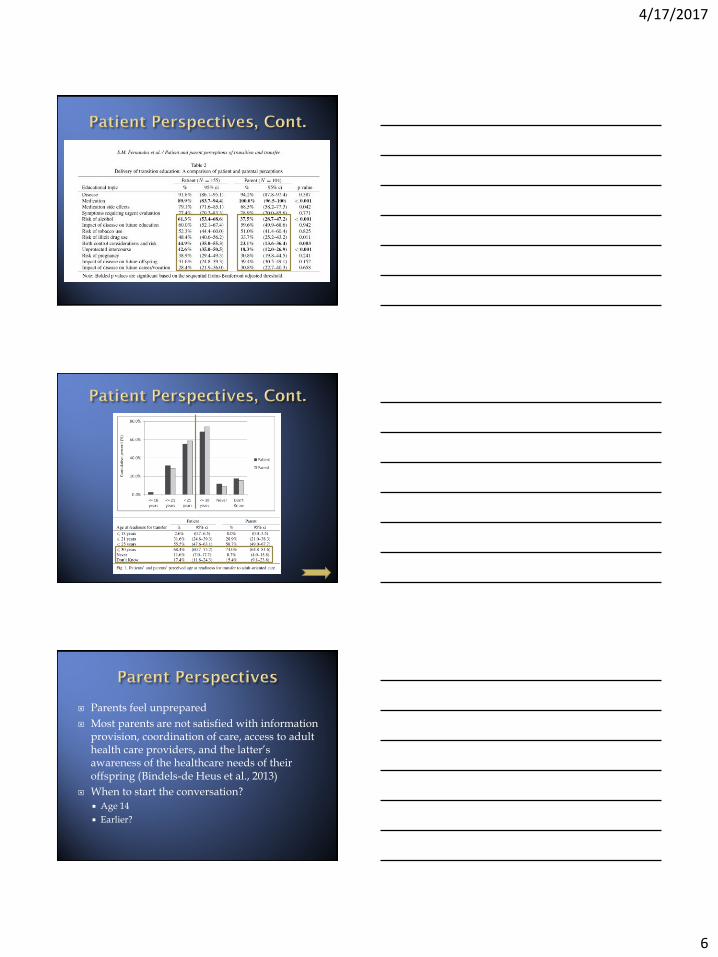
Parents feel unprepared
Most parents are not satisfied with information provision, coordination of care, access to adult health care providers, and the latter’s awareness of the healthcare needs of their offspring (Bindels-de Heus et al., 2013)
When to start the conversation?
Age 14
Earlier?
4/17/2017
7
Most report needing help with the emotional and cognitive shift from parent directed care to patient directed care or, as needed, parent supported care
Do adult providers want/need their perspective?
Transition should be structured yet allow room for flexibility as patient conditions change, treatments evolve, and family dynamics fluctuate
5 parent recommendations
Give more information to parents about the options and make clear why transfer is necessary
Make transition a gradual process
Organize a joint consultation between the pediatrician and the new specialist
Give parents a copy of the medical history and referral letter
Consider ALL aspects of transition (health, community life, work, education, legal issues)
While the majority of providers report they provide patients and families with adequate transition education, most fail to implement a standardized approach (Fernandez et al., 2014)
Most report initiating conversations but feel they lack knowledge surrounding resources available in the community
An overwhelming majority struggle to document the transition process
4/17/2017
8
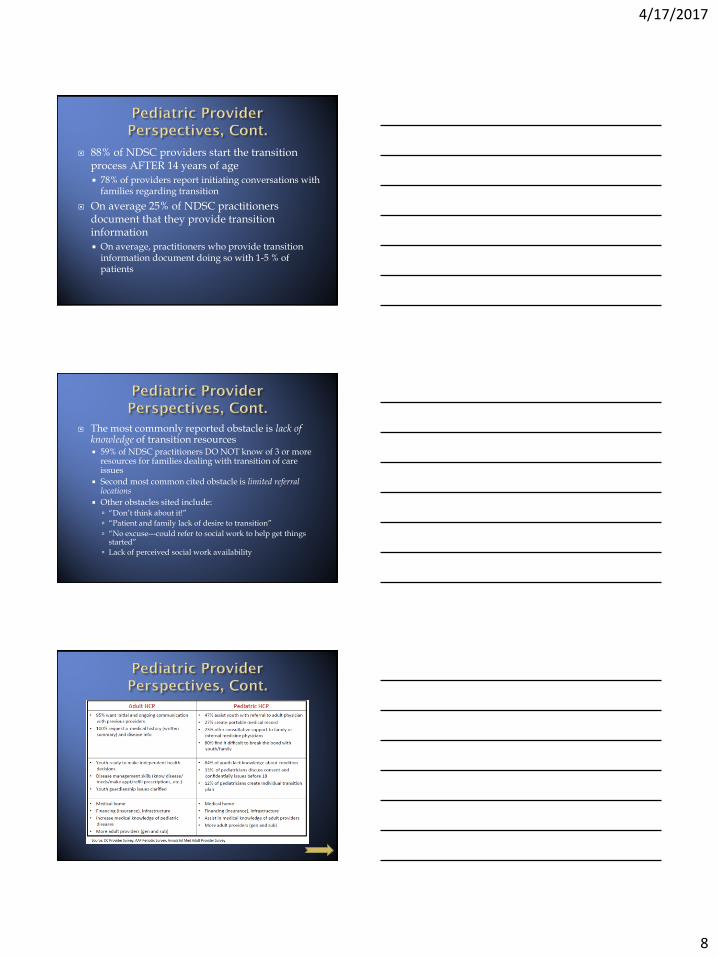
88% of NDSC providers start the transition process AFTER 14 years of age
78% of providers report initiating conversations with families regarding transition
On average 25% of NDSC practitioners document that they provide transition information
On average, practitioners who provide transition information document doing so with 1-5 % of patients
The most commonly reported obstacle is lack of knowledge of transition resources 59% of NDSC practitioners DO NOT know of 3 or more
resources for families dealing with transition of care issues
Second most common cited obstacle is limited referral locations
Other obstacles sited include: “Don’t think about it!”
“Patient and family lack of desire to transition”
“No excuse---could refer to social work to help get things started”
Lack of perceived social work availability

4/17/2017
9
Many young adults transitioned from pediatric to adult services are unprepared upon arrival Identification of patients who are actually ready?
Guardianship issues often not completed or clarified leading to various legal ramifications for adult providers
Providers remain concerned that families will not remain actively involved in the care of young adults with special needs
The parent/provider relationship is also different
Internists polled reported greater willingness to accept adult patients with conditions such as Down syndrome and CF compared to those with Autism and Spinal Muscular Atrophy
Site knowledge regarding various childhood onset disease processes
Trouble with care coordination
Technology dependence for communication and activities of daily living
Need assistance handling potential death early in the adult patient/adult provider relationship
Desire for additional training
Transition process
Child onset chronic diseases and congenital disorders
Meeting the unique psychosocial needs of this population
Specialists concerned that pediatric providers are “not letting go”

4/17/2017
10
“You need not be sorry for her. She was one of the kind that likes to grow up. In the end she grew up of her own free will a day quicker than the other girls.”
― J.M. Barrie, Peter Pan
Increased focus on transition planning since the early 1990’s
Since 2001, the Department of Health and Human Services’ Maternal and Child Health Bureau (MCHB) has been collecting data on 6 core performance outcomes necessary to “create a comprehensive system of services for all children”
One of these outcomes is specific to transition
MCHB has partnered every 4-5 years with the National Center for Statistics to conduct the National Survey for Children with Special Healthcare Needs
Survey conducted 2005-2006 and again 2009-2010
A total of 17,114 interviews were completed for youth with special healthcare needs (YSHCN) between the ages of 12 and 18
4/17/2017
11
Outcome #6:
“Youth with special healthcare needs who receive the necessary services to make appropriate transitions to adult healthcare, work, and independence”
Composite measure calculated by using responses to 4 component measures and their follow-up questions

4/17/2017
12
4/17/2017
13
“Kids think with their brains cracked wide open; becoming an adult, I've decided, is only a slow sewing shut.”
― Jodi Picoult, My Sister's Keeper
4/17/2017
14
1. Assess for transition readiness
- Patient and Parent Transition Readiness Assessments
2. Plan a dynamic and longitudinal process for accomplishing realistic goals
- Institutional Transition Policy
- Privacy and Consent Policy
- Transition Flow Sheet
3. Implementation of the plan through education of all involved parties and empowerment of the patient in the areas of self care
- Provide a Portable Medical Summary
- Transfer Packets and Transfer Checklists
- Remain an available consultant to Adult Healthcare Providers
4. Document Progress
- Maintain a database of patients
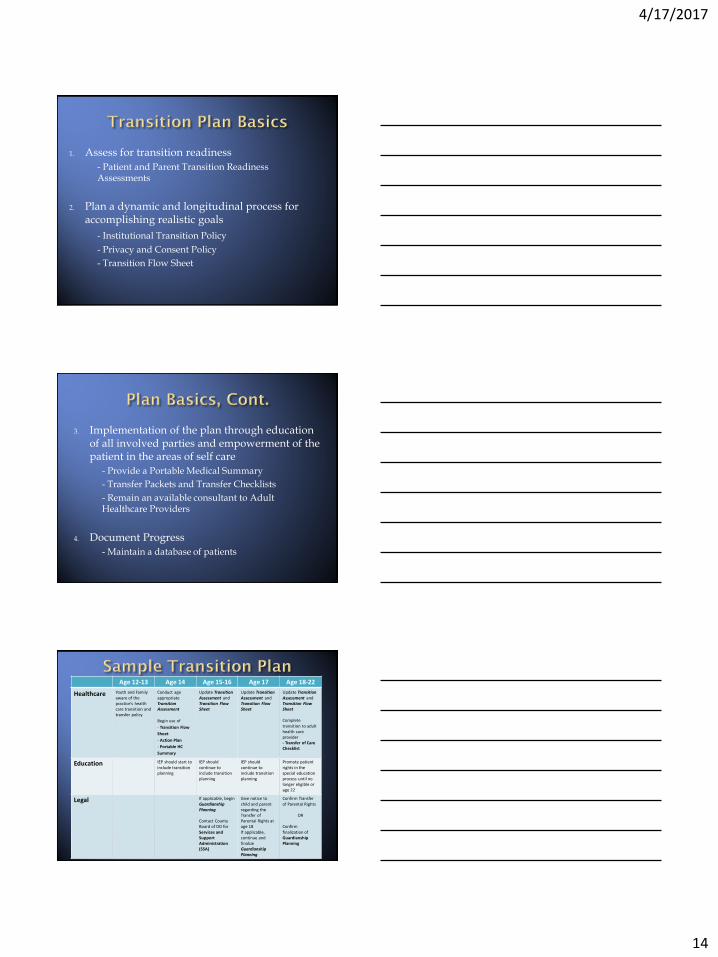
Age 12-13 Age 14 Age 15-16 Age 17 Age 18-22
Healthcare Youth and Family aware of the practice’s health care transition and transfer policy
Conduct age appropriate Transition Assessment
Begin use of
- Transition Flow
Sheet
- Action Plan
- Portable HC
Summary
Update Transition Assessment and Transition Flow Sheet
Update Transition Assessment and Transition Flow Sheet
Update Transition Assessment and Transition Flow Sheet Complete transition to adult health care provider - Transfer of Care Checklist
Education IEP should start to include transition planning
IEP should continue to include transition planning
IEP should continue to include transition planning
Promote patient rights in the special education process until no longer eligible or age 22
Legal If applicable, begin Guardianship Planning Contact County Board of DD for Services and Support Administration (SSA)
Give notice to child and parent regarding the Transfer of Parental Rights at age 18 If applicable, continue and finalize Guardianship Planning
Confirm Transfer of Parental Rights
OR
Confirm finalization of Guardianship Planning
4/17/2017
15
Why is it important?
Build consensus
Address fairness
Meet expectations
Allow for planning and systematic processes
Benefits?
Plan cohesion across providers
Patients, families and providers understand
What is expected in the transition process
Time frames
Potential pitfalls
Decrease gaps in care
Consistent with the law
Clarify roles of patients and parents in decision making
Create a safe and comfortable environment for those 18 and over to discuss private concerns regarding their health
Build patient competencies and patient-centeredness
Ensure consistency within the practice

4/17/2017
16
Evaluate youth and young adults’ current healthcare knowledge base and skills
Identify areas that need further education
Youth/young adults and parents learn more about managing their condition and becoming ready for an adult model of care
Everyone is aware of next steps
Providers and families are able to work collectively to gain necessary skills

4/17/2017
17
Why are they important?
Ensure availability of updated medical information
Ability to consolidate and communicate with clear information via Email
Fax
Phone
In person
Across health systems
Facilitate transition of care from pediatric/adolescent to adult healthcare practices
Maintain consistency from patient to patient
Assist with coordination of care across providers and subspecialties
Useful for team or individual provider models of transition
Document and track transition completion
4/17/2017
18
“I am convinced that most people do not grow up. We marry and dare to have children and call that growing up. I think what we do is mostly grow old. We carry accumulation of years in our bodies, and on our faces, but generally our real selves, the children inside, are innocent and shy as magnolias.”
― Maya Angelou, Letter to My Daughter
At the national level
Work with public, private insurers and health plans on:
Outreach and education to families and patients
Care management support
Payment and quality incentives for healthcare providers
Develop youth and parent leadership on transition and education opportunities to build awareness
Continue Healthcare and Community Transition research to find more effective approaches
At the state level
Develop a statewide registry of adult healthcare providers willing to provide quality care to transitioned youth with chronic illnesses, developmental/intellectual disabilities, and mental health issues
Expand transition training opportunities for healthcare professionals of all avenues
Development of Healthcare Transitions Committees
Continue initiatives for transition education for both adult and pediatric providers

4/17/2017
19
At the community level
Encourage the formation and evolution of local patient and parent support groups/organizations
Research and clinical experience is very clear – they already turn to each other but information is not always accurate
Healthcare Professionals should be available for consultation and community lecturing opportunities
At the institution level
Develop and update patient registries for tracking youth in need of transition services
Quality Improvement initiatives
Medical education curriculum changes
2012 survey suggests both perceived interest and need for organized transition curriculum that could be targeted to learners at various levels and across different specialties
Embed Healthcare Transition documents and resources into the EMR

4/17/2017
20
www.gottransition.org www.floridahats.org www.youth-move.org/transition-timeline Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home; American Academy of Pediatrics, American Academy of Family Physicians, and American College of Physicians, Transitions Clinical Report Authoring Group; Pediatrics 2011;128;182; originally published online June 27, 2011; DOI: 10.1542/peds.2011-0969 National Survey of Children with Special Health Care Needs, 2009/10
Barbour, A., MD, B. Downing, MD, K. Hawkins, MD, P. McManus, MHS, N. Quion, MD, L. Tuchman, MD, P. White, MD, MA. Health Care Transition for Adolescents and Young Adults. Presentation. April 26, 2012. Bindels-de Heus, K.G.C.B., et al. “Transferring Young People with Profound Intellectual and Multiple Disabilities from Pediatric to Adult Medical Care: Parents Experiences and Recommendations.” Intellectual and Developmental Disabilities 51 (2013) : 176-189. Bjorquist, E., E. Nordmark, I. Hallstom. “Living in Transition – Experiences of Health and Well-Being and the Needs of Adolescents with Cerebral Palsy.” Child: Care, Health and Development 41 (2014) : 258-265. Fernandes, S.M. et al. “Transition and Transfer of Adolescents and Young Adults with Pediatric Onset Chronic Disease: The Patient and Parent Perspective.” Journal of Pediatric Rehabilitation Medicine: An Interdisciplinary Approach 7 (2014) : 43-51. Gleeson, H., S. McCartney, and V. Lidstone. “Everybody’s Business: Transition and the Role of Adult Physicians.” Clinical Medicine 12 (2012) : 561 -566. Kennedy, A. and S. Sawyer. “Transition from Pediatric to Adult Services: Are We Getting it Right?” Current Opinion in Pediatrics 20 (2008) : 403-409. Kuhlthau, K.A. et al. “Pediatric Provider’s Perspectives on the Transition to Adult Health Care for Youth with Autism Spectrum Disorder: Current Strategies and Promising New Directions.” Autism 19 (2015) : 262-271. Lin, S.C., M.T. Lee, and T. A. Adirim. “Transition Outcomes for Young Adults with Disabilities.” Journal of Pediatric Rehabilitation Medicine: An Interdisciplinary Approach 8 (2015) : 23-30. McLaughlin, S.E. et al. “Transition of Adolescents with Chronic Health Conditions to Adult Primary Care: Factors Associated with Physician Acceptance.” Journal of Pediatric Rehabilitation Medicine: An Interdisciplinary Approach 7 (2014) : 63-70. McManus, M.A. et al. “Current Status of Transition Preparation Among Youth with Special Needs in the United States.” Pediatrics 131 (2013) : 1090-1097. McManus, M.A. et al. “Pediatric to Adult Transition : A Quality Improvement Model for Primary Care.” Journal of Adolescent Health 56 (2015) : 73-78. Mennito, S. “Resident Preferences for a Curriculum in Healthcare Transitions for Young Adults.” Southern Medical Journal 105 (2012 ) : 462-466. Olesen, D.G. and N.L. Swigonski. “Transition to Adulthood: The Important Role of the Pediatrician.” Pediatrics 113 (2004) : 159 -162. Reiss, J.G., R.W. Gibson, and L.R. Walker. “Health Care Transition: Youth, Family, and Provider Perspectives.” Pediatrics 115 (2005) : 112-120. Peter, N.G. et al. “Transition from Pediatric to Adult Care: Internists’ Perspectives.” Pediatrics 123 (2009) : 417 -423. Watson, J.R. et al. “Models of Transitional Care for Young People with Complex Health Needs : A Scoping Review.” Child: Care, Health and Development 37 (2011) : 780-791. Woodward, J.F., N.L. Swigonski, and M.R. Ciccarelli. “Assessing the Health, Functional Characteristics, and Health Needs of Youth Attending a Noncatagorical Transition Support Program.” Journal of Adolescent Health 51 (2012) : 272-278.







