Download - Fertility preservation 3

Fertility Preservation in Cancer Patients
Dr. Khaled R Darhouse, MRCOG
Consultant Obstetrician & GynaecologistReproductive Medicine & Assisted Conception
King Abdulaziz University HospitalJeddah – Saudi Arabia
The Gonads
• The primary function of both ovaries and testis is REPRODUCTION
• Reproduction is the passage of parental genetic material onto the next generation
Life Expectancy
• In 1900 the average life expectancy of men was 46.3 years and of women was 48.3 years.
• At the turn of the millennium men now expect to live to be 73.8 and women to be 79.5 years old.
• In a hundred years life expectancy has nearly doubled.

National Geographic MagazineMay 2013
• THIS BABY WILL LIVE TO BE 120
• New science could lead to long lives

Longer life
• The longer the people live the more they’ll expect to get cancer.
• Advantages in cancer treatment over the past two decades have led to remarkable improvements in survival rates.
• Indeed, during the past 5 years, the overall death rates from cancer have fallen by more than 1.6% per year.

General Fertility Preservation
• Women are increasingly postponing childbearing to later in life for social, career or financial reasons
• Incidence of most cancers increase with age

Cancer Fertility Preservation
• In women, ~10% of cancers occur in those <45 years old. Chemotherapy, radiotherapy and bone marrow transplantation can cure >90% of girls and young women with diseases that require such treatments.
• However, these treatments can result in premature ovarian failure, depending on the follicular reserve, the age of the patient and the type and dose of drugs used.

Improved Five Year Survival(1966 -2000)

Five Year SurvivalChildhood Cancers

Cure for Children but at a Cost
• Sustain and improve survival rates• Minimise late effects• Treatment is in conflict with normal childhood
growth and development

Risk Assessment for Fertility Preservation
• Intrinsic Factors• Health status of the patient• Consent of patient or parents• Assessment of ovarian reserve
• Extrinsic Factors• Nature of planned treatment• Available time• Availability of expertise
Wallace H, Critchley H and Anderson R JCO 2012
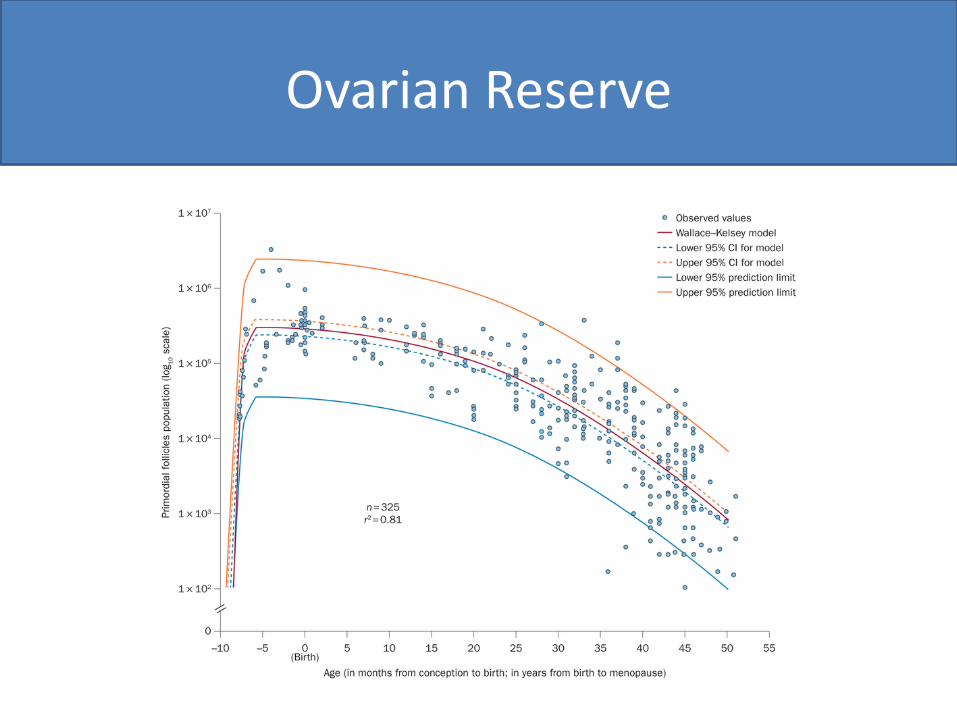
Ovarian Reserve
Infertility Risk Factors
• Radiotherapy• Irradiation of field of ovaries or testis• Total body irradiation
• Chemotherapy• Busulphan• Cyclophosphamide• Melphalan• Mustine• Procarbazine

Gonadotoxicity
Presentation Copyright: Dr. Khaled R Darhouse
Cytotoxic agents according to the degree of gonadotoxicity
High risk Intermediate risk Low/no risk
Cyclophosphamide Doxorubicin Methotrexate
Busulfan Cisplatin Bleomycin
Melphalan Carboplatin 5-Fluorouracil
Chlorambucil Actinomycin-D
Dacarbazine Mercaptopurine
Procarbazine Vincristine
Ifosfamide
Thiotepa
Nitrogen mustard
Reference: Lobo R; N Engl J Med2005 353,64–73.

Infertility Risk
• Low Risk (<20%)• ALL• Wilms’ tumour• Brain tumours (RTx <24Gy)• Soft tissue sarcomas• Hodgkin’s lymphoma I/II

Infertility Risk
• Medium Risk• AML• Osteosarcoma• Ewing’s sarcoma II/III• Nuroblastoma• Brain tumours (RTx > 24Gy)• Hodgkin’s lymphoma III/IV
Infertility Risk
• High Risk (<80%)• Total Body Irradiation• Pelvic / testis irradiation• Pre-BMT chemotherapy• Ewing’s tumour IV• Pelvic Hodgkin’s lymphoma

Radiation-Induced Ovarian Damage
• Human Oocyts• Primordial follicles
• LD 50 <2 Gy
Wallace, Thompson and Kelsey, Hum Reprod 2003

Radiation-Induced Ovarian Damage
• Human Oocyts• Primordial follicles
• LD 50 <2 Gy
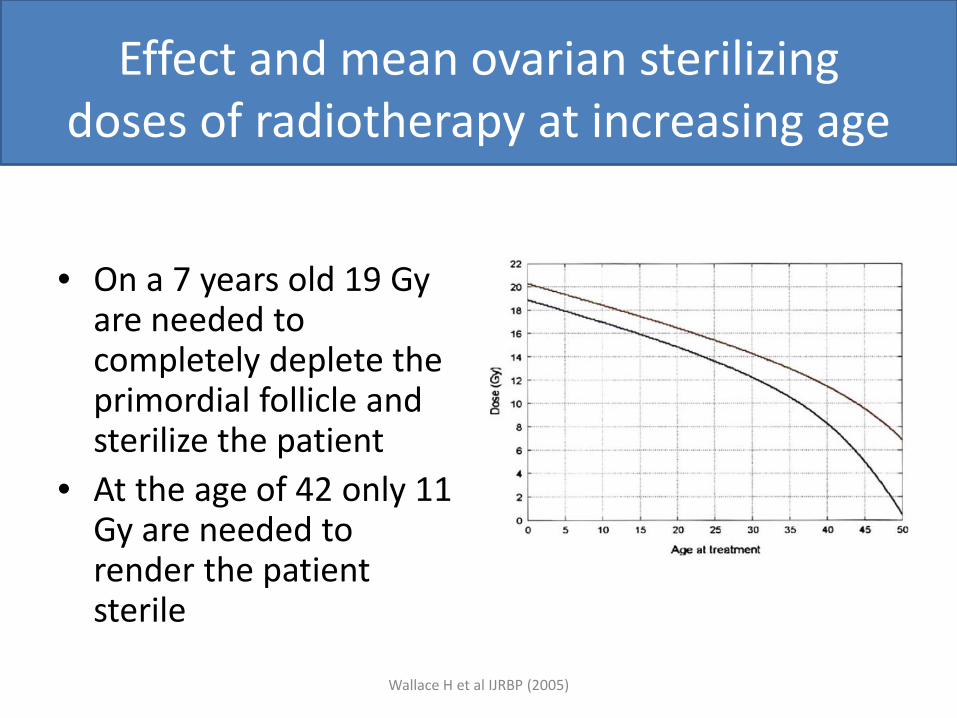
Effect and mean ovarian sterilizing doses of radiotherapy at increasing age
• On a 7 years old 19 Gyare needed to completely deplete the primordial follicle and sterilize the patient
• At the age of 42 only 11 Gy are needed to render the patient sterile
Wallace H et al IJRBP (2005)

Uterine volume and age at irradiation
Bath et al BJOG (2005)

Uterine function after cancer treatment
• Uterine damage, manifest by impaired growth and blood flow, is likely a consequence of pelvic irradiation.
• Uterine volume correlates with age at irradiation.
• Exposure to pelvic irradiation is associated with increased miscarriage, mid-trimester pregnancy loss, preterm labour low birth weight and post-partum haemorrhage.
Sex Hormone Therapy for Childhood Cancer Survivors
• The most appropriate dose and route of administration of sex hormone replacement to young women with ovarian failure after pelvic irradiation that provides adequate concentrations of oestrogen to ensure optimal uterine growth during adolescence has not yet been established
OPTIONS OF FERTILITY PRESERVATION
• Envolves: Oncologists, Paediatricians, Gynaecologists and Urologist/Andrologists
• Men: • Sperm cryopreservation
• Women:• Embryo cryopreservation• Oocyte cryopreservation• Ovarian tissue cryopreservation

OPTIONS OF FERTILITY PRESERVATION
• In pre-pubertal men testicular tissue cryopreservation is experimental, but is the only option currently available
• Sperm cryopreservation is a well established and successful method routinely used.

OPTIONS OF FERTILITY PRESERVATION
OPTIONS OF FERTILITY PRESERVATION
• Ovarian function suppression • Oral contraceptive pills• GnRHa
• Embryo cryopreservation• Well-established with good success• Married• Post-pubertal• Delay in cancer treatment• Legal issues

OPTIONS OF FERTILITY PRESERVATION
• Oocyte cryopreservation• Mature oocytes• Immature oocytes with IVM• Post-pubertal• Delay in cancer treatment
• Ovarian tissue cryopreservation• Pre-pubertal / Post-pubertal• No delay in cancer treatment• Expertise

Mature Oocyte Cryopreservation
• Need for a stimulated cycle• Tailored stimulation protocols• GnRHa trigger• Should not delay chemo/radiotherapy• Disastrous consequences with complications • Harvest of good quality oocytes should be
expected• Not recommended after chemotherapy is
initiated
Mature Oocyte Cryopreservation
• Survival rate of vitrified oocytes is now approximately 96.9%
• Pregnancy rates after oocyte vitrification• 10 oocytes = 40%• 12 oocytes = 60%• 20 oocytes = 90%

Ovarian Tissue Cryopreservation
• Percentage of patients undergoing OTC:• 96.2% of patients were < 35 years• 52.5% of patients were < 24 years• 17.2% of patients were < 14 years
Ovarian Tissue Cryopreservation
• Harvesting by laparotomy or laparoscopy• How much of the ovarian cortex should be
removed?• Size and thickness of cortical strips• Cellular injury and damage
• Hypoxia• Dehydration• Freezing
• Slow freezing or vitrification?
Ovarian Tissue Cryopreservation
• Re-implantation could be either orthotopic or hetrotopic
• More than 50% of primordial follicles are lost due to hypoxia
• Thawing process injury• High FSH and low AMH deplete surviving
primordial follicles
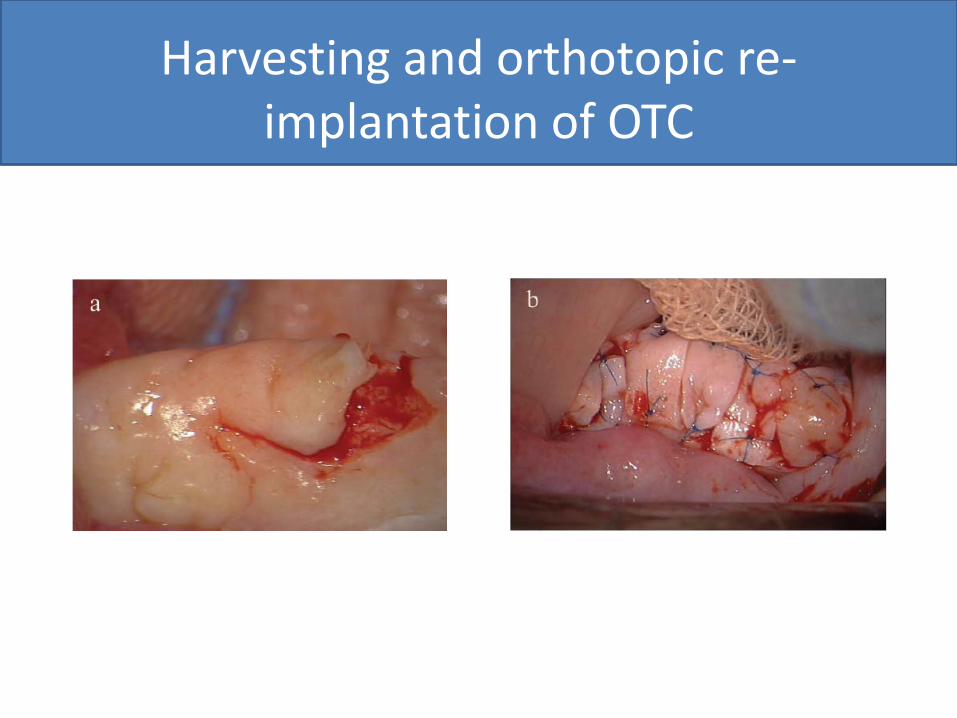
Harvesting and orthotopic re-implantation of OTC

FSH Levels Post-Orthotopicreimplantation

LH, FSH and E2 levels post reimplantation of OTC
Ovarian Tissue Cryopreservation
• Orthotopic reimplantation allows for spontaneous pregnancy
• Hetrotopic reimplantation necessitates IVF-ICSI
• Major concern is reintroduction of malignant cells after remission / cure.

Ovarian Tissue Cryopreservation
Ovarian Tissue Cryopreservation
• It is unknown how many cases of reimplantation were carried out throughout the world
• In a series of 60 reported cases the live birth rate is 23%
• Young children are the ideal candidates• No pregnancies reported following the
reimplanation of ovarain tissue harvested pre-pubertally
The Future
• In vitro follicular maturation after ovarian tissue culture
• Isolated primordial follicle culture in the lab• Artificial ovaries

The Future
• Stem cell gamete production• Experimental success in producing both eggs and
sperms• Successful in producing normal and fertile mice• Must pass rigorous testing• Might be available in at least 10 years
• Lyophilization and Freeze-Drying• Eggs• Sperms• Embryos

Conclusion
• Fertility preservation has become an established branch of reproductive medicine.
• Multidisciplinary team approach and individualisation of cases are key to its success.
• Fertility preservation should be discussed with men and women in the fertile age group who are about to embark in cancer treatment

Conclusion
• Fertility preservation gives hope in future reproduction and hope of a life after cancer.
• Embryo freezing is most successful method to date.
• For prepubertal men and women gonadaltissue freezing is the only available method availlable.
• Many new promising methods wil be available in the near future.
Thank You
Dr. Khaled R Darhouse, MRCOG
Consultant Obstetrician & GynaecologistReproductive Medicine & Assisted Conception
King Abdulaziz University HospitalJeddah – Saudi Arabia







