Extension of Social Protection:
Community-based health insurance
Céline Peyron, ITC- ILO, Trade Union Training on Social Protection, 13 May 2004
Extension of Social Protection:
Community-based health insurance
Céline Peyron, ITC- ILO, Trade Union Training on Social Protection, 13 May 2004
ContentContentContentContent
1. Health micro-insurance : a strategy for the extension of social security
2. Definition, principles and models of HMIS
3. Linkages
4. Limitations and impact of HMIS

1. Health micro-insurance: a
strategy for the extension
of social security
1. Health micro-insurance: a
strategy for the extension
of social security
ILO objective on Social Protection
ILO objective on Social Protection
Enhance
the coverage and effectiveness of the Social Protection
for
ALL

Strategies for extending health Strategies for extending health insuranceinsurance
Strategies for extending health Strategies for extending health insuranceinsurance
Strengthening of national health insurance schemes:
– Extending social insurance coverage
– Universal benefits
– Social assistance
Encouraging decentralized mechanisms
Creation of linkages between both

2. Definition, principles and
models of health micro-
insurance schemes
2. Definition, principles and
models of health micro-
insurance schemes
Health micro-insurance schemes: Objectives
Health micro-insurance schemes: Objectives
To support populations’ initiatives in organizing themselves their access to health :
Providing access to health to members
Negotiating with health care providers quality services at lowest possible costs
Prevention and information on Health problems
Income security and stability
Reinforcing solidarity and equity
Participation of all beneficiaries in social matters

Health Micro-Insurance Schemes: Definition
Health Micro-Insurance Schemes: Definition
“Micro-insurance refers to various schemes set up by self-employed and informal economy
workers to meet their priority social protection needs. The mechanism used in these schemes is generally the provision of
mutual support through the pooling of resources based on the principals of
insurance. “
Source: ILO, World Labour Report 2000: Income security and social protection in a changing world, (ILO: Geneva).

Growth statistics in West AfricaGrowth statistics in West Africa
1997 2000 ProjectsBenin 11 23 19Burkina Faso 6 26 18Cameroon 18 20 7Ivory Coast 29Guinea 6 27 5Mali 7 22MauritaniaNiger 6 12 3Senegal 19 29 31Tchad 3 4Togo 0 + 8 projects 7 5
76 199 88
Health micro-insurance:Schemes
Health micro-insurance:Schemes
Mutual Benefits Association (Trade Union)
Community Based Schemes Integrated Schemes in an Hospital
managementMicro-finance Institutes
INDIA : THE COMPENDIUMINDIA : THE COMPENDIUM
• 48 schemes found operational
• 8 new shemes under preparation
• intervention of multiple actors
• 11 states already concerned
• partnerships with insurance co.
• around 2,6 millions beneficiaries
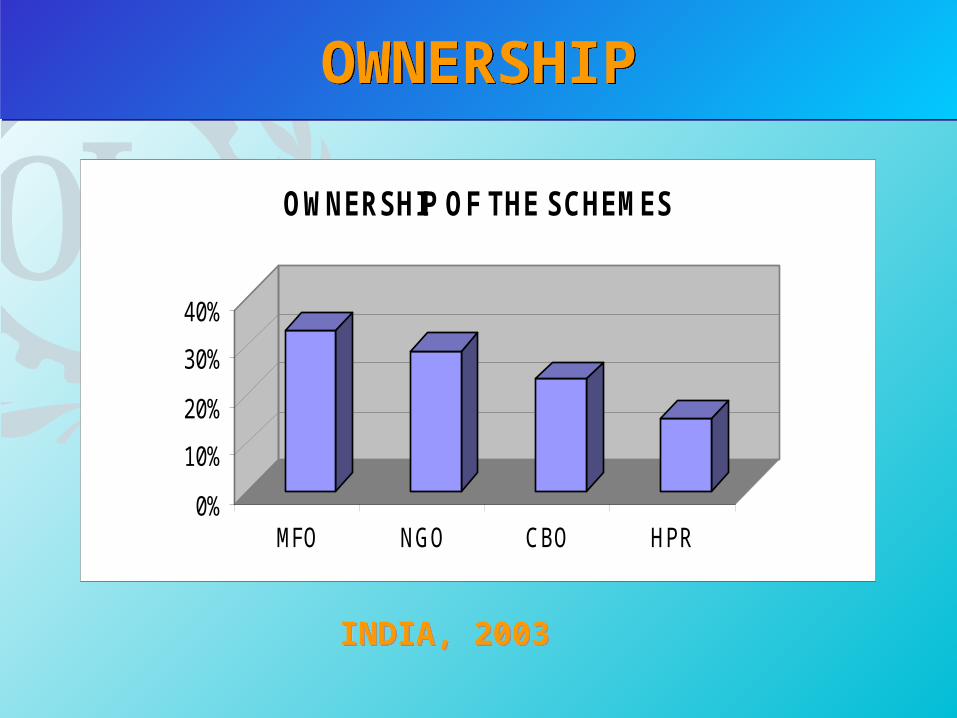
OWNERSHIPOWNERSHIP
0%
10%
20%
30%
40%
MFO NGO CBO HPR
OWNERSHIP OF THE SCHEMES
INDIA, 2003INDIA, 2003

LEVEL OF EXPERIENCELEVEL OF EXPERIENCE
0
5
10
15
< 2y. 3-4y. 5-6y. 7-10y. More
LEVEL OF EXPERIENCE
INDIA, 2003INDIA, 2003

AREAS OF INTERVENTIONAREAS OF INTERVENTION
0%
20%
40%
60%
RURAL R - U URBAN
AREAS OF INTERVENTION
INDIA, 2003INDIA, 2003

SERVICES PROVIDEDSERVICES PROVIDED
0%
20%
40%
60%
LIFE HEALTH ASS. lIVEST.
SERVICES PROVIDED
INDIA, 2003INDIA, 2003

BENEFICIARIESBENEFICIARIES
NUMBER OF BENEFICIARIES
0
5
10
15
<1000 1001-5000 5001-10000
10001-100000
100001-500000
More
INDIA, 2003INDIA, 2003

TYPE OF CONTRIBUTIONTYPE OF CONTRIBUTION
0
10
20
30
VOLUNT. COMPUL. MIX
TYPE OF CONTRIBUTION
INDIA, 2003INDIA, 2003

RISK COVERAGERISK COVERAGE
Out of 28 schemes :
• 16 schemes cover only hospitalisation expenses
• 7 schemes cover only primary health care services
• 5 schemes cover both primary health care & hospitalisation costs
INDIA, 2003INDIA, 2003

SCHEDULE OF CONTRIBUTIONSCHEDULE OF
CONTRIBUTION
0
10
20
30
40
YEARLY MONTH W.ACT.
SCHEDULE OF CONTRIBUTIONS
INDIA, 2003INDIA, 2003

Which are the main characteristics of health
micro-insurance schemes in India?

THE CURRENT TRENDS, IN INDIA…THE CURRENT TRENDS, IN INDIA…
all insurance companies (both public and private) involved in the provision of health micro-insurance products to the poor mainly cover hospitalisation costs…
while…there is a world-wide recognition that the overriding need in developing countries is for primary health care…
Health micro-insurance: Health micro-insurance: PrinciplesPrinciples
Health micro-insurance: Health micro-insurance: PrinciplesPrinciples
population excluded from formal social security
schemes, often low incomes and vulnerable
solidarity and non-profit organisation
voluntary & contributory schemes
pooling of a group’s resources to share risks
(health, pregnancy, death, accidents, belongings)
& organize protection adapted to their needs
benefits package and contributions adapted

Health micro-insurance:Actors
Health micro-insurance:Actors
BeneficiariesHealth care providers (Public services
and private providers)Finance institutesAuthorities (local and national)

Health micro-insurance: Different models
Health micro-insurance: Different models
THE « PARTNERSHIP » MODEL
THE « INTEGRATED » MODEL
THE « INDEPENDENT » MODEL

THE « PARTNERSHIP » MODELTHE « PARTNERSHIP » MODEL
HMISHealth
structureHealth
structure
The HMIS is linked with the health provider by means of an agreementThe HMIS is linked with the health
provider by means of an agreement

5000 MEMBERSCollaboration with 5 hospitals IT developed management
MicroCare Health Plan,MicroCare Health Plan,UGANDAUGANDA
MicroCare Health Plan,MicroCare Health Plan,UGANDAUGANDA
THE « PARTNERSHIP » MODELTHE « PARTNERSHIP » MODEL
HEALTH CARE PROVIDED medical consultations hospitalisations specialized tests surgery diagnostics and check-up medicine delivery services dental care ophtalmological consultations COVERAGE Of HEALTH CARE COST 100% ANNUAL CONTRIBUTION PER FAMILY : 60 $US (6 members)
MicroCare Health Plan,MicroCare Health Plan,UGANDAUGANDA
MicroCare Health Plan,MicroCare Health Plan,UGANDAUGANDA
THE « PARTNERSHIP » MODELTHE « PARTNERSHIP » MODEL

THE “INDEPENDENT” MODELTHE “INDEPENDENT” MODEL
The HMIS has no contractual links with the health provider
The HMIS has no contractual links with the health provider
HMISHealth
providerHealth
provider

Created in 1992 From a Women
Workers ’ Trade Union, of the informal economy (created in 1972)
90.000 beneficiaries
Vimo SEWA- INDIAVimo SEWA- INDIAVimo SEWA- INDIAVimo SEWA- INDIA
THE “INDEPENDENT” MODEL
CARE SERVICES PACKAGE INCLUDING : Health Insurance (hospitalization), including services for delivery
protection, Life Insurance, including insurance in case of invalidity, and Belongings Insurance (lost or damages to property or working
material) HEALTH CARE COVERED : 30 $USMAX PER YEAR MATERNITY PROTECTION : 7,5 $US on the 8th month of
pregnancy CONTRIBUTION : 1,5 $US / Year
Vimo SEWA- INDEVimo SEWA- INDEVimo SEWA- INDEVimo SEWA- INDE
THE “INDEPENDENT” MODEL
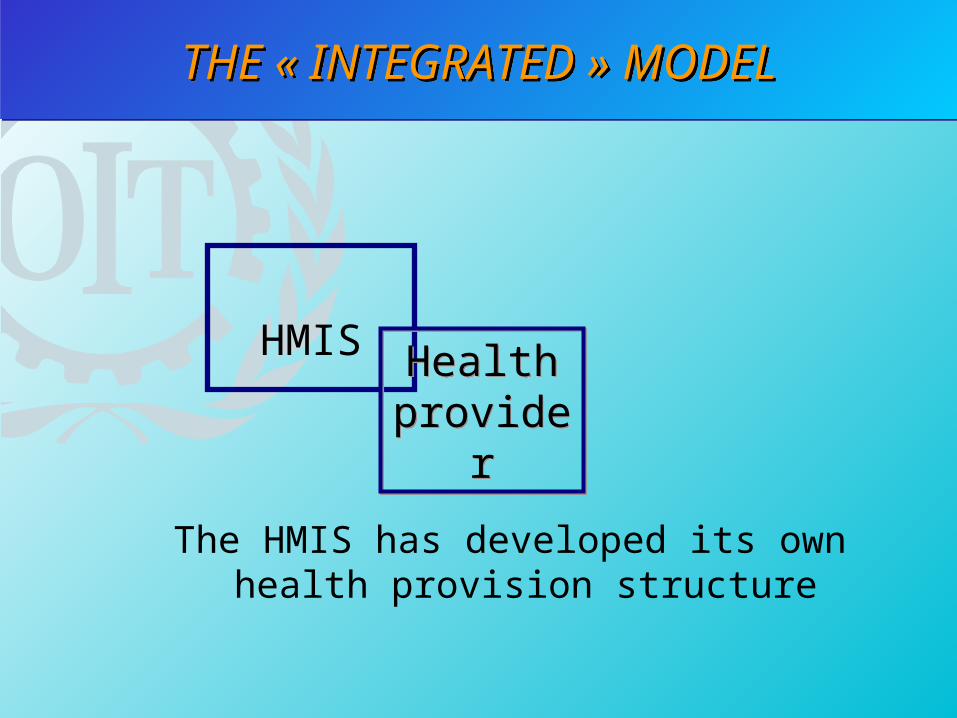
THE « INTEGRATED » MODELTHE « INTEGRATED » MODEL
HMISHealth
providerHealth
provider
The HMIS has developed its own health provision structure

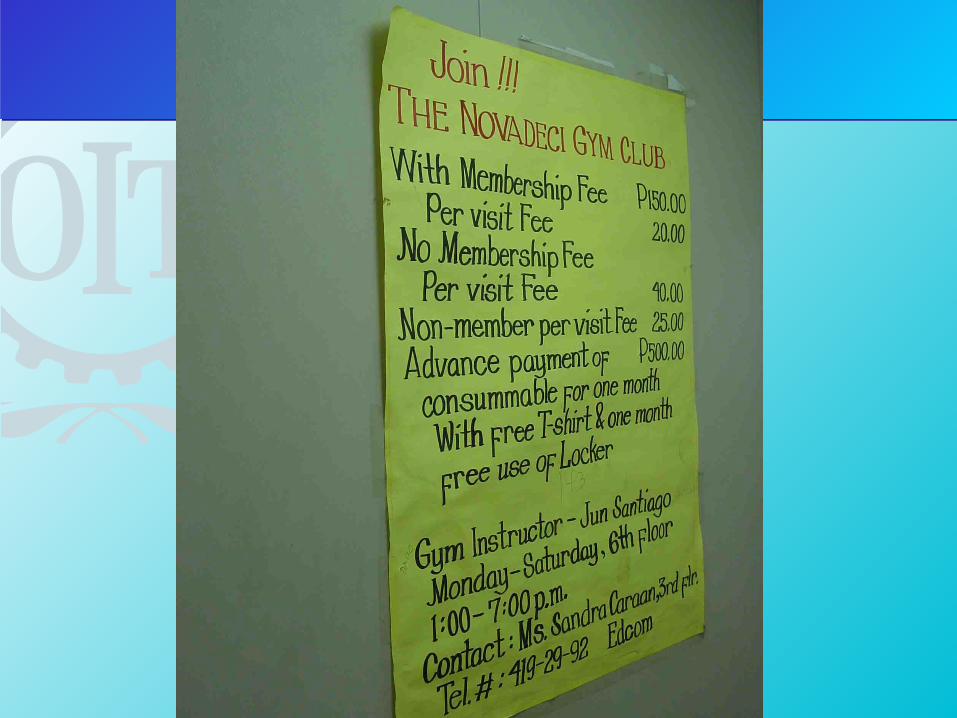
Created in 1976 MANY SERVICES: Health,
life/death, occupational injured, micro-credit, fire insurance, ...
covers 6500 families (it means 24000 beneficiaries)
NOVADECI - PhilippinesNOVADECI - PhilippinesNOVADECI - PhilippinesNOVADECI - Philippines
THE « INTEGRATED » MODEL
NOVADECI - NOVADECI -
Philippines PharmacyPhilippines Pharmacy
NOVADECI - NOVADECI -
Philippines PharmacyPhilippines Pharmacy
THE « INTEGRATED » MODELTHE « INTEGRATED » MODEL



Steps in setting up health micro-insurance scheme
Steps in setting up health micro-insurance scheme
Diagnostic - informationSetting up steering committeePre- and feasibility studyAgreement-preparation providersPreparation of management and monitoring
toolsLauching schemeFunctionning and monitoring HMIS

3. Linkages
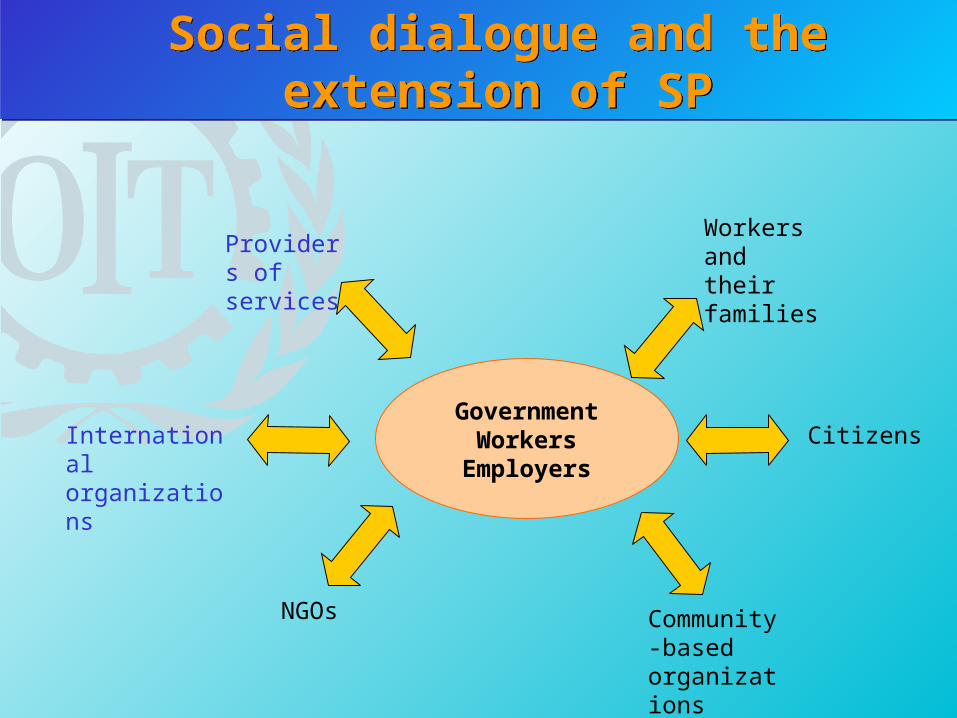
Social dialogue and the extension of SPSocial dialogue and the extension of SP
GovernmentWorkersEmployers
Providers of services
Workers and their families
Community-based organizations
NGOs
International organizations
Citizens

Conclusion: linkages HMIS with Trade-Unions
Conclusion: linkages HMIS with Trade-Unions
• Promotion
• Setting-up their own HMIS system
• Negotiation to improve health care services (quality and quantity)
• Campaign for prevention and health education
4- Limitations and impact of health micro-insurance schemes

Health micro-insurance:Limitations
Health micro-insurance:Limitations
a partial and immediate response to an unmet collective responsibility
resource pooling & risks shared in a limited group of people, mostly low income and vulnerable
not necessarily a guarantee of equity for the poor
limited care services providescapacity of poor to contribute fluctuates
with income

• Moral hazard of over-consumption
• Moral hazard of over-prescription
• Adverse selection
• Fraud and abuse
• Catastrophic events
Health micro-insurance: Risks
Health micro-insurance: Risks
Group workGroup work
1. What can be the relevance of HMIS in terms of gender equality?
2. Is HMIS possible for HIV/AIDS affected targets?

1. Gender and HMIS1. Gender and HMIS
• Strenghtening of the status of the women
• Health situation of women and access to health care
• Methodology of supporting and promoting women
• Fight against social injustice

1. Gender and HMIS1. Gender and HMIS
Participation of women in management of HMIS
Reduce poverty and inequity between sexes
Protection of domestic workers Women mainly employed in informal
economy
2.- HMIS and HIV/AIDS2.- HMIS and HIV/AIDS
Suitable if: Expansion of the members (Affected /
Infected) Benefits package limited to primary
health care Funds from National campaigns and
NGO’s projects

2. Advantages of HMIS to prevent HIV/AIDS
2. Advantages of HMIS to prevent HIV/AIDS
Access to health care Prevention Voluntary and confidential counselling
and testing Improvement capacity of health
providers Address stigma and discrimination Channel ressources to the local level

THANK YOU ! !THANK YOU ! !







