
EU‐funded deployment projects
in the area of ICT for Ageing Well

The emerging demographic change towards an ageing population is introducing drastic changes in our society. We therefore need to find ways to motivate and assist older people to stay active for longer in the labour market, to prevent social isolation and promote societal inclusion and finally to help people stay independent for as long as possible. Information and Communication Technologies (ICT) can play a major role in order to help achieve the above goals. ICT can help elderly individuals to improve their quality of life, stay healthier, live independently for longer, and counteract reduced capabilities which are more prevalent with age. ICT can enable them to remain active at work or in their community. In response to these challenges and opportunities, the European Commission has launched an Action Plan for Ageing Well in the Information Society∗ which includes measures to: Raise awareness and share good practices; Build consensus via stakeholder cooperation; Promote policies to stimulate innovation in the public sector and to overcome technical and regulatory barriers to market development; Accelerate take‐up and innovation; Boost research and innovation.
Updated November 2010
∗ For more information see: http://ec.europa.eu/information_society/activities/einclusion/policy/ageing/action_plan
2/26 •••
List of projects
CommonWell .........................................................................................................4
DREAMING™ ..........................................................................................................6
ISISEMD ..................................................................................................................8
LongLastingMemories (LLM) ................................................................................10
Sociable ................................................................................................................12
T‐Seniority ............................................................................................................14
Clear .....................................................................................................................16
Nexes....................................................................................................................18
InCasa ...................................................................................................................20
Independent.........................................................................................................22
HomeSweetHome ................................................................................................24
••• 3/26
CommonWell
Common Platform Services for Ageing Well in EuropeThe project aims to support high quality independent living for older people by integrating ICT‐based services across provider organisations on open platforms. The results of the pilot operation will be used to extend service provision and promote the wider uptake of this model of care across Europe.
Organisations involved The Pilot Sites (400 users)
• Municipalities (Milton Keynes UK) • UK (Milton Keynes, 100 users) • Multinational companies (Tunstall Group
UK, InterSystems GmbH) • Germany (Bielefeld, 100 users) • Spain (Granada, 100 users)
• Non‐profit (Fundación Andaluza de Servicios Sociales)
• Netherlands (Eindhoven, 100 users)
• SMEs (Stichting Smart Homes NL, Stichting Verzorging en Verpleging Eindhoven NL)
The CommonWell services to be deployed
• Care providers (Ev. Johanneswerk e.V. DE, Johanneswerk im Stadtteil GmbH, Empresa Pública de Emergencias Sanitarias ES)
1. Client‐facing services, integrated chronic disease management and services for independent living, including safety at home, reminders for essential activities and (social) interaction support. • Research organisations (Empirica DE, Work
Research Centre Ireland) 2. Inter‐organisational services, including vital signs monitoring and medication compliance services. Also a patient transfer information service provided by emergency services to manage transfers of clients away from and back to their homes.
Types of users of the CommonWell services
• Client‐facing services (chronic disease management and independent living services) will be used by older Europeans in their homes.
3. Common services, comprising ID management and trust services. Services are delivered to the homes of the elderly on interoperable, standard home platforms.
• Inter‐organisational and common services will be used by charity and public social care professionals and by healthcare staff.
• Structured inter‐organisational services and common services are not used by staff directly but function to support the seamless delivery of high quality chronic disease management and independent living services.
4/26 •••
Expected impact / outcome of CommonWell services
• Improved quality of life for the elderly by contributing to an increase in quality and efficiency of health and social care through integrating activities of staff in different organisations.
• Prolonged independence and a lengthening of time the elderly can live in their own homes due to the proper management of chronic conditions, reducing risks in the home and providing support in managing day‐to‐day activities.
• Supported social interaction through use of the next version of Continua, internet‐based communication including real‐time voice and video.
• A reinvention in the way social care and healthcare providers work together through a specific focus on managing chronic disease.
• Personalisation and integration of chronic disease management with other healthcare and independent living services.
• Addressing the needs of those with cognitive problems through the implementation of services with extremely simple and natural interfaces capable of giving timely and comprehensible reminders.
• Improved continuity of care provided to older people, potentially eliminating all problems arising from transitions between hospital, institutional care, emergency transport and their own home.
• Avoidance of hardware duplication for service providers.
Overall Methodologies and Indicators deployed for impact measuring
• Quarterly reports are delivered to the Project Coordinator using a standard template to help monitor progress, the reaching of objectives and resource consumption at participation level.
Details:
Contact information: Simon Robinson, Empirica Tel. +49 228 985 300 E‐mail: [email protected] Website: http://www.commonwell.eu
Total cost: €5.36m EU contribution: €2.68m
Execution: 01/10/2008 to 30/09/2011
••• 5/26
DREAMING™
Elderly‐Friendly Alarm Handling and Monitoring∗ The project aims to extend the independent life of elderly people while providing them with an equivalent level of safety as they would enjoy in a protected environment such as an elderly home.
∗ The DREAMING name and the Dreaming logo are both trademarks of HIM SA.
The Pilot sites (350 users)
• Denmark (Langeland, Syddanmark, 50 users)
• Estonia (Tallin, 60 users) • Germany (Berlin, 60 users) • Italy (Fruili‐Venezia Giulia, 60 users) • Spain (Barbastro ‐ Aragón, 80 users) • Sweden (Heby – County of Uppsala, 40
users)
The services to be deployed in each of the sites:
1. A Monitoring and Alarm Handling service, consisting of an Environmental Monitoring Subsystem which detects and reports changes in user movement patterns as well as a Health Monitoring Subsystem.
2. eInclusion Services, based on a videoconferencing solution specifically designed for use by elderly people, through means of a TV set.
3. Non‐ICT based services, these are not part of the pilot, but are essential to allow elderly people to live independently in their own homes. These will be provided by the Project partners as part and parcel of their mission but will not be charged to the Project budget.
Organisations involved, the Dreaming Consortium
• Providers of assistance to elderly people (Tesan‐Televita S.r.l, Azienda per i Servizi Sanitari n.1 Triestina, MediPlus, East‐Tallinn Central Hospital, Government of Aragon, Municipality of Heby, Municipality of Langeland)
• Technological partners (Tesan‐Televita S.r.l, HIM SA, Telemedicina Rizzoli S.r.l, TB Solutions)
• Public Health Authorities and Social Service Dept (Azienda per i Servizi Sanitari n.1 Triestina, Region Syddanmark, East‐Tallin Central Hospital, Government of Aragon, Municipality of Heby, County Council of Uppsala, Municipality of Langeland)
• Elderly people representative associations (AGE – the European Older People's Platform)
• Healthcare business and market development specialists (HIM SA)
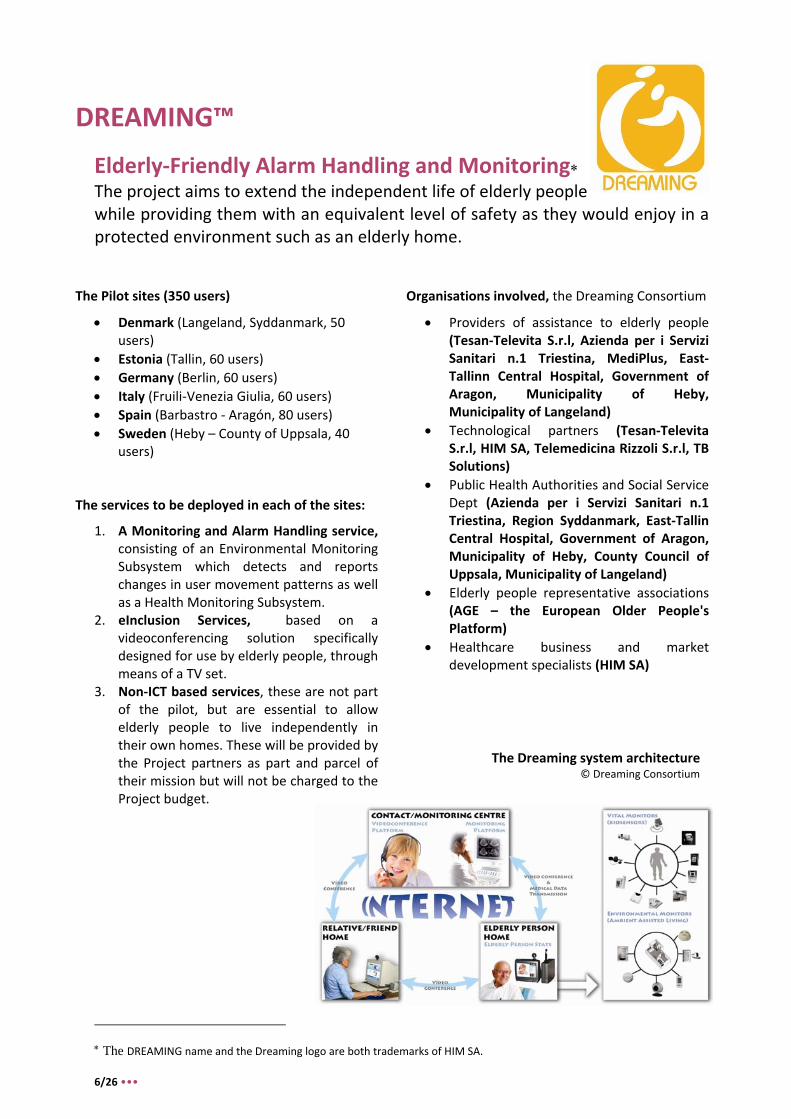
The Dreaming system architecture © Dreaming Consortium
6/26 •••

Types of users of the Dreaming project
• Elderly people are the main users and beneficiaries of the Dreaming services and they will use the medical devices and the videoconferencing service directly.
• Caregivers will help elderly people when their manual skills and/or intellectual faculties decline. • Contact Centre operators will have access to the Decision Support System for monitoring and
elderly assistance purposes. • Social Workers will be activated if and when there is a need for intervention. They will mainly use
the videoconferencing service to keep in touch with the elderly people they look after when they cannot assist them in person. They will also have access to the Decision Support System but this will be limited to information which is relevant for their work (access to clinical data will not be allowed, in principle).
• General Practitioners and Community Nurses will be given access to the Decision Support System and they will be automatically notified by the Decision Support System or by the Contact Centre operators when their intervention is required.
• Emergency services will be automatically notified by the Decision Support System or by the Contact Centre operators when the situation detected by the Monitoring and Alarm Handling service requires immediate action (fire, gas leak, fall, life threatening health conditions, etc.)
Expected impact/outcome of the Dreaming project
• Substantially prolonged independence, including extending the time the elderly can live in their own homes and manage their day‐to‐day activities.
• Improved social interaction through videoconferencing, helping to maintain the cognitive condition of the elderly.
• Improved quality of life of older people and their families. • Opening up of an internal market for ICT based solutions for the elderly. The ageing society is an
EU‐wide issue. Demand exists within Europe for a solution as validated by Dreaming. • Improved access to information, as caregivers will be better informed through the automatic
messaging facilities provided by the Decision Support System and can remotely access the data of the elderly person relevant for their work.
• Improved working conditions and efficiency of healthcare professionals and social workers as they will be dispatched only when really required and a greater amount of tele‐working may result.
• Improved emergency services response time as they will be alerted more quickly as a result of data monitoring.
Overall methodologies and indicators for measuring impact:
• The benefits of the Dreaming system will be measured by comparing a number of indicators for those receiving the Dreaming service (the Study Group) with those of another homogenous group of elders (the Control Group) over the 30 month pilot.
Details:
Contact information: Marco d'Angelantonio, HiMsa Tel. +32 2 307 64 66 E‐mail: [email protected] Website: http://www.dreaming‐project.org
Total cost: €5.54m EU contribution: €2.77m
Execution: 01/05/2008 to 30/04/2011
••• 7/26
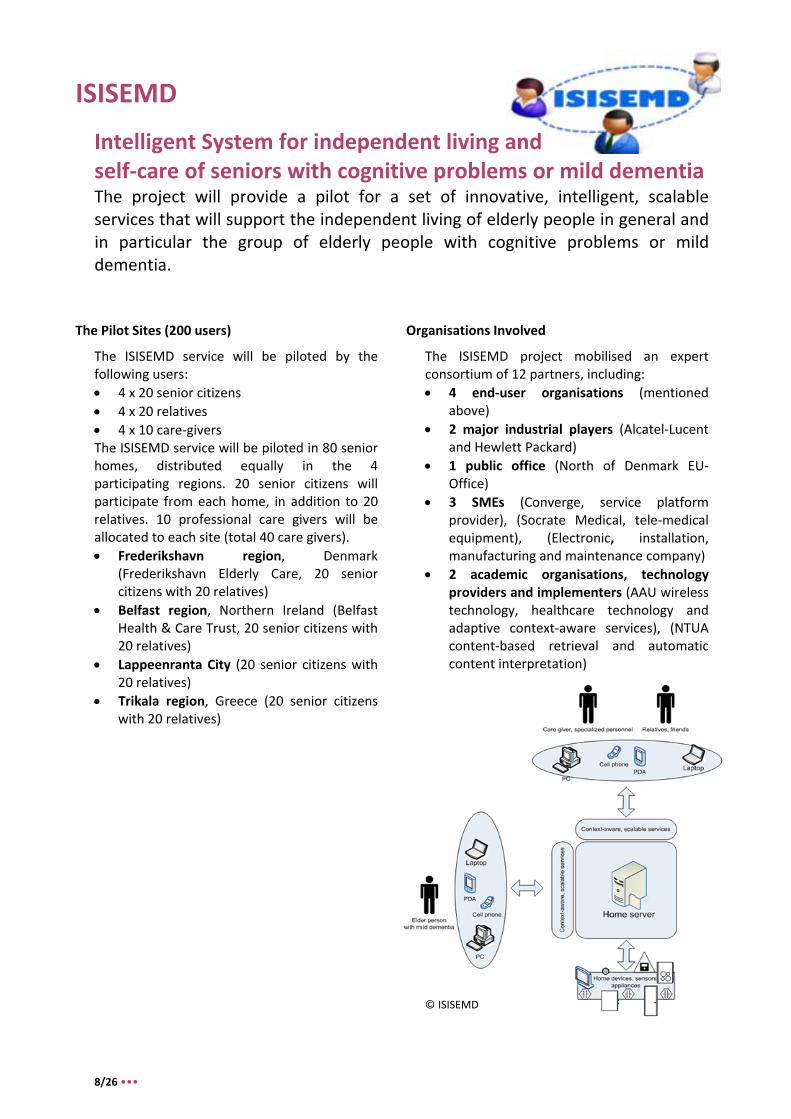
ISISEMD
Intelligent System for independent living and self‐care of seniors with cognitive problems or mild dementia The project will provide a pilot for a set of innovative, intelligent, scalable services that will support the independent living of elderly people in general and in particular the group of elderly people with cognitive problems or mild dementia.
The Pilot Sites (200 users)
The ISISEMD service will be piloted by the following users: • 4 x 20 senior citizens • 4 x 20 relatives • 4 x 10 care‐givers The ISISEMD service will be piloted in 80 senior homes, distributed equally in the 4 participating regions. 20 senior citizens will participate from each home, in addition to 20 relatives. 10 professional care givers will be allocated to each site (total 40 care givers). • Frederikshavn region, Denmark
(Frederikshavn Elderly Care, 20 senior citizens with 20 relatives)
• Belfast region, Northern Ireland (Belfast Health & Care Trust, 20 senior citizens with 20 relatives)
• Lappeenranta City (20 senior citizens with 20 relatives)
• Trikala region, Greece (20 senior citizens with 20 relatives)
Organisations Involved
The ISISEMD project mobilised an expert consortium of 12 partners, including: • 4 end‐user organisations (mentioned
above) • 2 major industrial players (Alcatel‐Lucent
and Hewlett Packard) • 1 public office (North of Denmark EU‐
Office) • 3 SMEs (Converge, service platform
provider), (Socrate Medical, tele‐medical equipment), (Electronic, installation, manufacturing and maintenance company)
• 2 academic organisations, technology providers and implementers (AAU wireless technology, healthcare technology and adaptive context‐aware services), (NTUA content‐based retrieval and automatic content interpretation)
© ISISEMD
8/26 •••

Isisemd services to be deployed:
1. Intelligent scalable supporting services, within the home in the context of ambient assisted living for the elderly or those with pre or mild dementia. 2. Networking technologies, aimed at achieving communication between in‐home sensors, devices and terminals. 3. Context‐aware technologies, including perceptual processing, wearable computing and techniques involving the collection of local‐environment data. 4. Ambient, context‐aware service integration, including home control, the monitoring and recognition of user activities as well as services facilitating communication with friends, relatives and caretakers. These services will feature user‐friendly interfaces including capabilities for natural interaction. 5. Intelligent additional services for relations and caregivers, aimed at keeping relatives informed about the activities of their loved ones and alerting care‐givers in case of emergency.
Expected impact/outcome of the Isisemd project
• Improved ability for the elderly to self‐care, through support for basic daily activities, which could help prevent potential health hazards.
• Enhanced efficiency of medical staff and professional care‐givers. • Economic boost, as a result of the need for products tailored to the specialised needs of older
people. 'Smart Home' companies may also stand to benefit from the Isisemd project. • Beneficial social impact, through strengthened daily interaction and the prevention of social
isolation.
Overall methodologies and indicators used to measure impact
4‐phased implementation (each phase lasting 12 months), means that the project will start as a small‐scale post‐pilot service and will later develop to involve larger scale pilots.
• Phase 1 will aim to provide an early adoption of the ISISEMD service in practice. • Phase 2 will aim to demonstrate the capability of the system in a full‐scale rollout. This phase will
build on the citizen services lessons from phase 1 and extend coverage to over 3000 homes in 4 regions.
• Phase 3 will aim for consolidation of the system configuration, mass deployment and customisation. This phase will grow the citizen population to 6000 by adding 2‐3 more regions to its coverage.
• Phase 4 will aim to validate the Isisemd platform in a successful, full‐scale implementation of the system. This phase will further grow the citizen population to 15,000 by extending its coverage further into the European level.
Details:
Contact information: Kjeld Bundgaard Olesen, Aalborg Kommune Tel. +32 2 282 0371 E‐mail: [email protected] Website: http://www.isisemd.eu
Total cost: €4.52m EU contribution: €2.26m
Execution: 01/03/2009 to 31/08/2011
© European Commission
••• 9/26
LongLastingMemories (LLM) The project aims to achieve the full benefits of existing cognitive and physical training regimes while reducing the need for supervision and guidance.
The Pilot Sites
• Austria (Schwechat, 20 users) • France (Paris, 500 users) • Greece (Thessaloniki & Athens 300 users) • Spain (Zamora & Salamanca, 200 users) • UK (London & Birmingham, 350 users)
The LongLastingMemories services to be deployed
• Merged ICT within an AAL environment, providing a unified service controlled and monitored by a universal, user‐friendly device.
• Cognitive training through 'Brain Fitness' software.
• Scheduled physical training with tailored motivational support through interactive screens and training equipment.
• Embedded processing units and a general purpose PC for the coordination and management of the AAL environment, the running of cognitive training software and the storing and processing of cognitive and physical training performance information.
• The e‐Home Solution, using small sensors to detect abnormal movement and falls.
Organisations Involved
• Coordinator (Aristotle University of Thessaloniki)
• 1 Academic organisation (University of Konstanz, Germany)
• 3 Research organisations (Institute for Language and Speech Processing, Central European Institute of Technology and FUNDACIÓN INTRAS)
• 4 SMEs (Global Security Intelligence, e‐Seniors, Investigación y Desarrollo Informático/ IDI EIKON and Tero LTD)
• 3 public organisation (IGNA/HCV, the Health Centre of Vyronas, Milton Keynes Council, Municipality of Schwechat)
Types of users of the LongLastingMemories services
• Older people generally and older people living independently inside an LLM environment, utilising its AAL services.
• Visitors to day care centres. • Hospitalised users, who may use the AAL
environment while following the cognitive training and may also use the physical training component as complementary to their physiotherapy sessions.
• Providers of end user support services, i.e. "professionals" acting as de facto "prescriptors" of the service and public administrations promoting and backing public‐private‐partnerships and funding initiatives under the corresponding National Programmes.
10/26 •••

Expected impact/outcome of the LongLastingMemories services
• Guaranteed assisted living through constant monitoring of the environment. • Enhancement of mental capability, thereby helping to extend the time citizens can remain in their
own homes. • Increased user self‐esteem, through gains in independent and the alleviation of feelings of
embarrassment or fear that overtakes elderly people, especially when they are in an unstable condition or one that requires intensive care.
• Improved day care centre services, through the provision of continuous attention and mental training.
• Reduced day care centre running costs, due to a reduced need for intensive patient care. • Alleviation of exclusion, solitude and depression in the Third Age, through the use of ICT. • Reduced accident risk (e.g. falls) as a result of the program's positive influence against cognitive
decline. • Immediate emergency response, thereby alleviating the common fears of relatives and caretakers
of leaving parents or patients alone.
Overall methodologies and indicators used to measure impact
• The achievement of the project's objectives is expected to be measurable based upon pre‐defined indicators and targets. The project is to be measured throughout the pilots using a range of tools, including medical tests, questionnaires and interviews of end‐users.
©LongLastingMemories Details: Contact information: Panagiotis Bamidis, Aristotle University of Thessaloniki Tel. +30 2310 999310 E‐mail: [email protected]
Website: http://www.longlastingmemories.eu
Total cost: €4.72m EU contribution: €2.36m
Execution: 01/06/2009 to 30/11/2011
••• 11/26
Sociable
Motivating Platform for Elderly Networking, Mental Reinforcement and Social Interaction The project will deploy an innovative ICT‐assisted service for assessing and accordingly reinforcing the mental state of the elderly through pleasant gaming activities for cognitive training, while at the same time boosting their social networking and activating their day‐to‐day interpersonal interactions.
The Pilot Sites (350 users)
• Norway (Trodheim Kommune, 48 users) • Greece (Hygeia Hospital, 55 users), (Centre
of Open Protection for Elderly of the Municipality of Peristeri, 65 users)
• Italy (Forli citizens, 55 users), (Morgagni Pierantoni Hospital, 45 users)
• Spain (Velluters residential home and home users, 40 users)
• Belgium (Vzw Cassiers Wzc (CAS) citizens, 42 users)
The Sociable services to be deployed:
1. Balanced and individualised cognitive training games catered to the target users.
2. Multi‐touch, mixed reality interfaces which have already been ergonomically tested and unanimously accepted by numerous users.
3. Networking capabilities enabling aged users to communicate with care centres and other aged individuals.
4. Novel social interaction and motivation services bringing together elderly users that share common interests, experiences, preferences and/or social objectives.
5. Unique operational model and "matching service" involving the mediation and participation of expert users in the care centres in order to create tailored training games and encourage social interaction.
Organisations involved
• Local partners, responsible for carrying out the pilot (representing the envisaged Sociable value chain).
• Public authorities associated with the project at national, regional and local level are responsible in the areas of care or supply of services.
• Technology providers, responsible for the implementation, integration and support of the Sociable service platform.
Types of users of Sociable services
• Individuals with mild dementia and cognitive problems.
• Aged individuals at specialised care centres and those within their home environment.
12/26 •••
Expected impact/outcome of the Sociable services
• Targeted, personalised cognitive training through improved knowledge about the cognitive state of users (e.g. Mini‐Mental State Examination score, Alzheimer's Disease Assessment Scale. The continual provision of patient data will work to constantly improve the quality of patient care.
• Improved training programs and other therapeutic measures through utilisation of an automatic tool for collecting measurements supporting the assessment of an individual's cognitive status.
• Increased social interaction, networking and community‐building with other members of the ageing society, through multi‐touch technology and augmented social interaction via the platform.
• Improved quality of life for those with dementia, as the Sociable scheme will lengthen the time they can live and work independently. This will also reduce the need for early hospitalisation, which will reduce the strain on public health organisations.
• A boost to ICT‐assisted, non‐pharmacological dementia therapy, as it will spread the message that ICT can help towards (among other things) memory training, cognitive stimulation therapy and multimodal therapeutic concepts.
• Stimulated economical development through helping a variety of stakeholders to discover new business opportunities and generate new revenue streams.
• Creation of royalty‐free standards enabling interconnection and interoperability of care/leisure centres across Europe.
Overall methodologies and indicators used to measure impact
All deliverables will have two assessment versions, one to be released in the middle of the pilot operations and a final one, at the end of the project for all pilot sites.
• 1a Interim Assessment of the SOCIABLE Platform and Services (M27): Report on the Assessment of the quality and effectiveness of the provided functionality and services.
• 1b Final Assessment of the SOCIABLE Platform and Services (M36): Report on the Assessment of the quality and effectiveness of the provided functionality and services.
• 2a Interim Techno‐Economic Evaluation (M27): Report on the evaluation of the platform from a technical/technological and economic viewpoint.
• 2b Final Techno‐Economic Evaluation (M36): Report on the evaluation of the platform from a technical/technological and economic viewpoint.
• 3a Interim Evaluation from Elderly‐Users (M27): Evaluation of the SOCIABLE platform and services from the seniors’ point of view.
• 3b Final Evaluation from Elderly‐Users (M36): Evaluation of the SOCIABLE platform and services from the seniors’ point of view.
Details:
Contact information: Stelios Pantelopoulos, Singular Logic Tel. +30 210 6266260 E‐mail: [email protected] Website: http://www.sociable‐project.eu
Total cost: €4.60m EU contribution: €2.30m
Execution: 01/05/2009 to 30/04/2012
Picture from the Euronews report on the Netcarity and Eldergames EU funded projects. © Euronews/European Commission
••• 13/26
T‐Seniority
Expanding the Benefits of Information Society to Older People through Digital TV Channels The project aims to significantly improve the quality of life of the ageing population and ensure their efficient health and social care by specifying and demonstrating innovative ICT enabled products and services.
The Pilot Sites (2850 users)
• Spain (Soria, 500 users) (Tarragona, 100 users)
• Italy (Regione Toscana, 600 users) • Greece (Thesaloniki, 400 users) (Athens,
200 users) • UK (Kirklees, 100 users) • France (Provence, 50 users) (Lorraine, 700
users) • Cyprus (Nicosia, Limassol, Larnaca‐Paphos,
100 users) • Finland (Tampere, 100 users)
The T‐Seniority services to be deployed
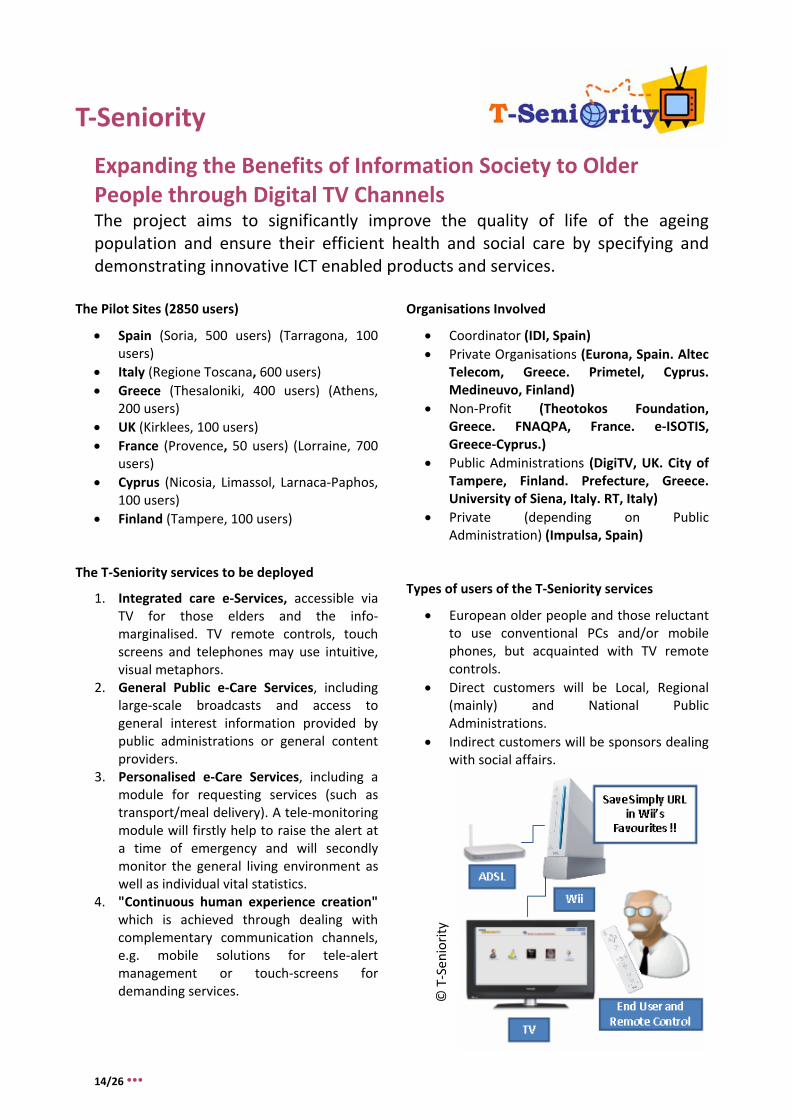
1. Integrated care e‐Services, accessible via TV for those elders and the info‐marginalised. TV remote controls, touch screens and telephones may use intuitive, visual metaphors.
2. General Public e‐Care Services, including large‐scale broadcasts and access to general interest information provided by public administrations or general content providers.
3. Personalised e‐Care Services, including a module for requesting services (such as transport/meal delivery). A tele‐monitoring module will firstly help to raise the alert at a time of emergency and will secondly monitor the general living environment as well as individual vital statistics.
4. "Continuous human experience creation" which is achieved through dealing with complementary communication channels, e.g. mobile solutions for tele‐alert management or touch‐screens for demanding services.
Organisations Involved
• Coordinator (IDI, Spain) • Private Organisations (Eurona, Spain. Altec
Telecom, Greece. Primetel, Cyprus. Medineuvo, Finland)
• Non‐Profit (Theotokos Foundation, Greece. FNAQPA, France. e‐ISOTIS, Greece‐Cyprus.)
• Public Administrations (DigiTV, UK. City of Tampere, Finland. Prefecture, Greece. University of Siena, Italy. RT, Italy)
• Private (depending on Public Administration) (Impulsa, Spain)
Types of users of the T‐Seniority services
• European older people and those reluctant to use conventional PCs and/or mobile phones, but acquainted with TV remote controls.
• Direct customers will be Local, Regional (mainly) and National Public Administrations.
• Indirect customers will be sponsors dealing with social affairs.
© T‐Sen
iority
14/26 •••

Expected impact/outcome of the T‐Seniority services • Improved efficiency and response time. Moving beyond one‐to‐one communication, the service
will allow communication from one individual to many in real‐time. • Greater ability for access to personalised, select content. Information generated will be reached
through various communication channels (Web, SMS, e‐mail etc) • Multi‐modal services will reach the final users without being necessarily linked to a concrete
"hard" complement. • Easily approachable users, reached in a natural way and by multiple means of communication. • Creation of a "common interface", which may help improve final‐user acknowledgement,
acceptance, learning and usage of new value‐added services.
Overall methodologies and indicators used to measure impact At the end of the project a full deployment feasibility report will be created, which will consist of the following elements:
• A demonstration of the operational service in 7 Member States involving a significant number of users in real‐life conditions.
• Additional demonstrations regarding the deployment of 'first and second wave' nations as part of the pan‐European movement.
• Peer service reviews, through a series of dissemination activities in the form of local trials in e‐Inclusion areas, as well as workshops/seminars/conferences and thematic fairs.
• Documented feedback from the user population, including the description of specific challenges and barriers to be overcome to help aid full deployment
T‐Seniority services
© T‐Seniority
Details: Contact information: Miguel Alborg, EIKON SL Tel. +34 96 1124000 E‐mail: [email protected] Website: http://tseniority.idieikon.com
Total cost: €5.34m EU contribution: €2.67m
Execution: 01/07/2008 to 31/12/2010
••• 15/26
Clear
Clinical Leading Environment for the Assessment and Validation of Rehabilitation Protocols in Home Care The project will set up an innovative e‐Health service based on the development of protocols for rehabilitation and chronic disease management therapies, which can be implemented at home following well defined procedures under the control of medical staff.
The Pilot Sites (800‐1000 users)
• Italy: (ca. 250 users) • Netherlands: (ca. 250 users) • Poland: (ca. 250 users) • Spain: (ca. 250 users)
The Clear services to be deployed
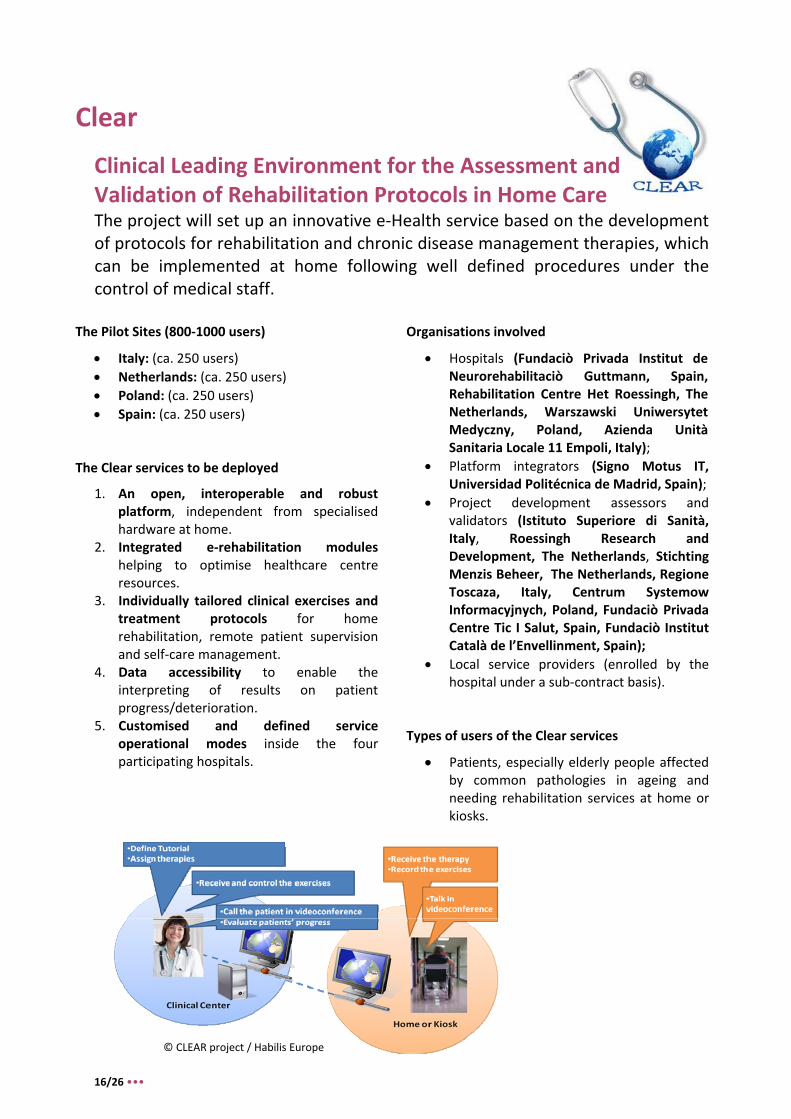
1. An open, interoperable and robust platform, independent from specialised hardware at home.
2. Integrated e‐rehabilitation modules helping to optimise healthcare centre resources.
3. Individually tailored clinical exercises and treatment protocols for home rehabilitation, remote patient supervision and self‐care management.
4. Data accessibility to enable the interpreting of results on patient progress/deterioration.
5. Customised and defined service operational modes inside the four participating hospitals.
Organisations involved
• Hospitals (Fundaciò Privada Institut de Neurorehabilitaciò Guttmann, Spain, Rehabilitation Centre Het Roessingh, The Netherlands, Warszawski Uniwersytet Medyczny, Poland, Azienda Unità Sanitaria Locale 11 Empoli, Italy);
• Platform integrators (Signo Motus IT, Universidad Politécnica de Madrid, Spain);
• Project development assessors and validators (Istituto Superiore di Sanità, Italy, Roessingh Research and Development, The Netherlands, Stichting Menzis Beheer, The Netherlands, Regione Toscaza, Italy, Centrum Systemow Informacyjnych, Poland, Fundaciò Privada Centre Tic I Salut, Spain, Fundaciò Institut Català de l’Envellinment, Spain);
• Local service providers (enrolled by the hospital under a sub‐contract basis).
Types of users of the Clear services
• Patients, especially elderly people affected by common pathologies in ageing and needing rehabilitation services at home or kiosks.
© CLEAR project / Habilis Europe
16/26 •••
••• 17/26
Expected impact/outcome of the Clear Project
1. Improved quality of life for patients through a reduced need to attend healthcare centres. 2. Improved healthcare centre effectiveness through being able to treat more patients at the same
time. 3. Greater understanding of the socio‐economic impact of the e‐Health services proposed, which will
help both the future adaptability and economic viability of healthcare systems. 4. Standardisation and coordination of the activities of national companies, to provide a pan‐
European service customised in each Member State. 5. Contribute to the impact of the ICT PSP as the project is conceived as a platform to deliver services
that will benefit patients in general, and particularly elderly people. 6. Increased European SME market potential as the structure of the service itself attributes an
important role to the Local Service Providers, which will have the task of technically assisting local hospitals and healthcare centres.
7. Increased quality of European rehabilitation practice through the push for common standards, making it possible to design rehabilitation paths that can be implemented remotely.
Overall methodologies and indicators used to measure impact
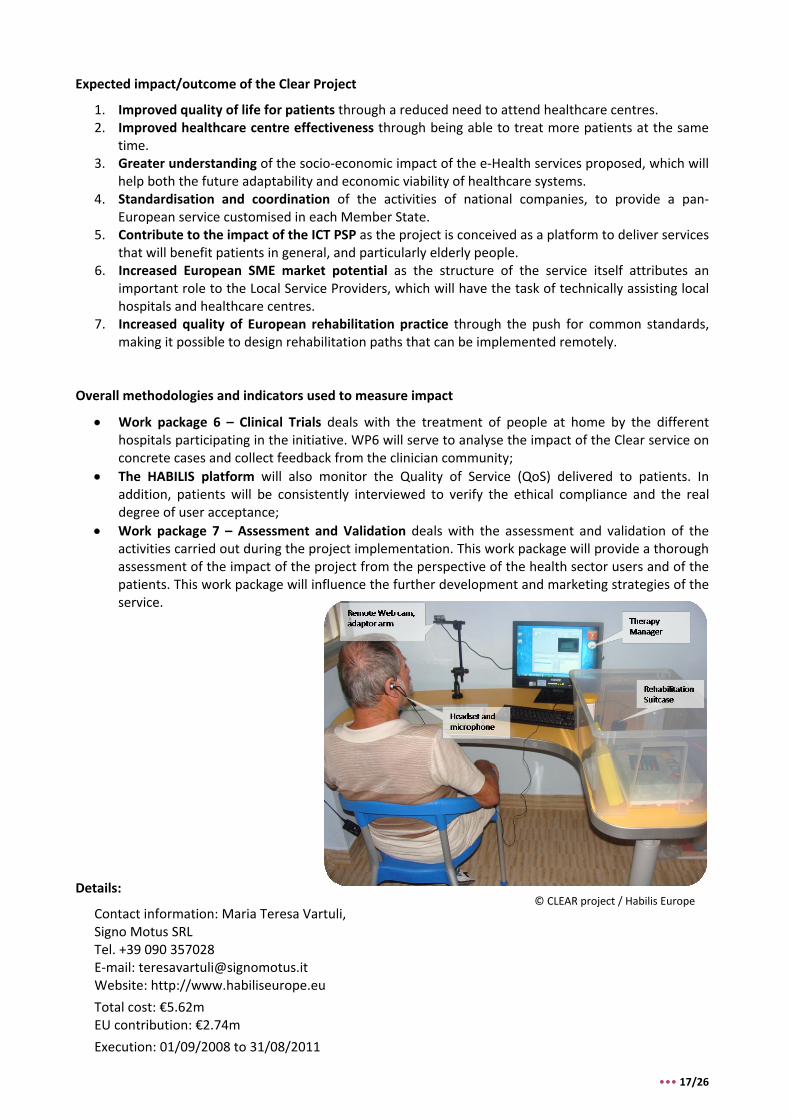
• Work package 6 – Clinical Trials deals with the treatment of people at home by the different hospitals participating in the initiative. WP6 will serve to analyse the impact of the Clear service on concrete cases and collect feedback from the clinician community;
• The HABILIS platform will also monitor the Quality of Service (QoS) delivered to patients. In addition, patients will be consistently interviewed to verify the ethical compliance and the real degree of user acceptance;
• Work package 7 – Assessment and Validation deals with the assessment and validation of the activities carried out during the project implementation. This work package will provide a thorough assessment of the impact of the project from the perspective of the health sector users and of the patients. This work package will influence the further development and marketing strategies of the service.
Details: © CLEAR project / Habilis Europe
Contact information: Maria Teresa Vartuli, Signo Motus SRL Tel. +39 090 357028 E‐mail: [email protected] Website: http://www.habiliseurope.eu
Total cost: €5.62m EU contribution: €2.74m
Execution: 01/09/2008 to 31/08/2011

Nexes
Supporting Healthier and Independent Living for Chronic Patients and the Elderly The project will deploy integrated care services for chronic patients based on structured interventions addressing prevention, healthcare and social support.
The Pilot Sites (5200 users)
• Spain: Barcelona • Norway: Central Norway Regional Health
Authority • Greece: Athens
The Nexes services to be deployed
1. Well‐being and rehabilitation services, promoting early diagnosis and healthy lifestyles of clinically stable chronic patients, enhancing their self‐management and improving compliance with prescribed treatments. Physical activity and cognitive aspects will be the principal components.
2. Enhanced care support of unplanned hospitalisations among patients with high risk of admissions.
3. Home hospitalisation & early discharge of patients with severe exacerbations of their chronic conditions.
4. Support diagnostic and/or therapeutic procedures.
Organisations involved
• 1 municipality (Trondheim Kommune) • Research organisations (Fundació Clínic
per a la Recerca Biomèdica, Institute of Social and Preventive Medicine, Stiftelsen Sintef, Telefonica Investigación y Desarrollo SA Unipersonal)
• SMEs (Santair SA, Intracom SA Telecom Solutions, TXT e‐solutions SpA)
• Healthcare providers (Sotiria Hospital, St Olav’s Hospital HF as a subsidiary to Helse Midt‐Norge RHF, Fundació Privada Centre TIC i Salut, Hospital Clínic i Provincial de Barcelona)
Types of users of the Nexes services
• Citizens at risk (patients and carers) • Health and community professionals
providing services in their respective domains.
18/26 •••
Expected impact/outcome of the Nexes services
• Heightened independence through extending the time the elderly can live in their own homes and self‐manage their day‐to‐day activities.
• 'Wellness' creation through the promotion of healthier lifestyles, enhanced self‐management, early diagnosis and improved compliance with physical and cognitive activity regimes.
• Increased effectiveness of care systems, through wide implementation of the service by public authorities in conjunction with industrial players helping to create sustainable and innovative chronic disease management services.
• Awareness of the operative aspects of the solution, gained through the field study, including organisational bottlenecks, legal and ethical barriers and the role of reimbursement schemes.
• Market‐level sustainability will be assured through the involvement of industrial players in each of the sites, helping to guarantee that the interests of the groups are represented in the business plan.
• Boosted European industry, particularly among SMEs in new markets for innovative ICT‐based products and services for independent living and chronic disease management.
• Increased "stay‐at‐home" caring, which will not only benefit individuals and patients, but also their informal carers as they will be better prepared to support the recipient of the services.
Overall methodologies and indicators used to measure impact
An extended follow‐up over 12‐18 months will involve the evaluation of three levels of activities.
1. High relevance evaluation category:
• Clinical effectiveness: The effect of ICT‐supported care on immediate, intermediate, or long‐term health outcomes compared to traditional care.
• Technical effectiveness: Whether the system is objectively reliable and usable (incl. quality of transmission and down periods). If ICT affected the use of services, the timeliness of care or the burden of obtaining care compared to traditional care.
2. Moderate relevance
• Cost: The cost of ICT‐supported integrated care services for healthcare providers compared to the alternatives. Direct cost incl. medical and non‐medical, facilities, patient trips.
• Clinical acceptance: Satisfaction of consulting clinicians with the ICT‐supported services compared to the alternatives.
3. Low relevance
• Patient satisfaction: Will not be measured as results from past evaluations demonstrate that patient satisfaction has been nearly universally high, thereby inhibiting the ability to discern the sensitivity of satisfaction to other factors.
Details:
Contact information: Emili Bargalló, Fundacio Privada Clinic per a la Recerca Biomedica Tel. +34 932275707 E‐mail: [email protected] Website: http://nexeshealth.eu
Total cost: €4.76m EU contribution: €2.38m
Execution: 01/05/2008 to 01/05/2011 © European Commission
19/26 •••
InCasa
Integrated Network for Completely Assisted Senior Citizen’s Autonomy The project aims at developing a system to support the ageing population and facilitates in helping them to remain in their own homes.
The Pilot Sites (150‐200 users)
(deployment of the InCasa project is divided into two steps)
1. 5‐10 users pilot the service in each country over 2‐3 months (model validation and solution fine‐tuning)
2. 30‐40 users pilot the (tuned) service in each country (from month 3 to the project end) in addition to step 1 users.
InCasa services to be deployed
• Home Sensor Networks (HSN) and Personal Health Sensors (PHS) to help monitor the lifestyles of the elderly and interact when necessary with citizens themselves or with the Service Provider.
• Human Monitoring Sensors (HMS): portable/wearable human monitoring devices.
• Integration with territorial social and health care.
• User habit profiling through motion and contact sensors.
• Smart phone/Base Station connected to HSN and HMS to collect and send data.
• Automatic emergency calls through SPP logics.
• Audio/visual interaction (pre‐existing devices/new deployments)
• Smart Personal Platform (SPP): habits application to elaborate data coming from HSN and PHS + Social and Health care data repository for data analysis and diffusion to a variety of professional users;
Organisations involved
• Consortium coordinator (Santer Reply S.p.a)
• Healthcare providers (Fundación Hospital de Calahorra, Konstantopouleio General Hospital of Nea Ionia Agia Olga, Chorleywood Health Centre)
• Research organisations (In‐JeT ApS, Institut National de la Santé et de la Recherche Medicale, Steinbeis Innovation Center Embedded Design and Networking)
• 1 Provincial agency (Agenzia Territoriale per la Casa della Provincia di Torino, Italy)
• 1 Multinational (Telefonica I+D) • Educational establishments (Department
of Information Systems and Computing, Brunel University, Institute of Communication and Computer Systems – NTUA, Athens)
• Hi‐Tech Industry (CNet Sweden AB, INVENT s.a.s)
Types of users of the InCasa services
• European citizens, over 65 years old, living alone with a sufficient level of autonomy and self‐care ability.
20/26 •••
Expected outcome of the InCasa services
• Improved patient data collection and monitoring, leading to earlier decision making. • Greater continuity of care as a result of wider interaction between the elderly and care providers. • Improved physical health, psychological status and social relations through an integrated care
plan and focused profiling activity. • Increased independence as a result of in‐home monitoring systems. • Reduced need for voluntary or premature hospitalisation due to boosted self‐confidence and the
ability for the elderly to remain home for longer. • Social connectedness, with subsequent health and well‐being benefits. • Stimulated European healthcare industry. InCasa should provide a clear indication about the
relevance of the pay‐back model of this investment. The pay‐per‐use, joined business model between the private sector and public sector should also gain validation.
Overall methodologies and indicators used to measure impact
The impact of project goals will be measured through specific Questionnaires, and through specific health and social care indicators. All these data will be shared (anonymously) across the EU, to improve epidemiologists' activities and to set research studies correctly. Considering EU traditional indicators for elderly people, the Key Performance Indicators measured during pilots will be:
1. Health and social cover (life expectancy of elderly people) 2. Support (elderly people and external contacts) 3. Skill acquisition 4. Elderly people's perception of their own image 5. Elderly people's satisfaction with regard to services 6. Elderly people's satisfaction with regard to their living conditions.
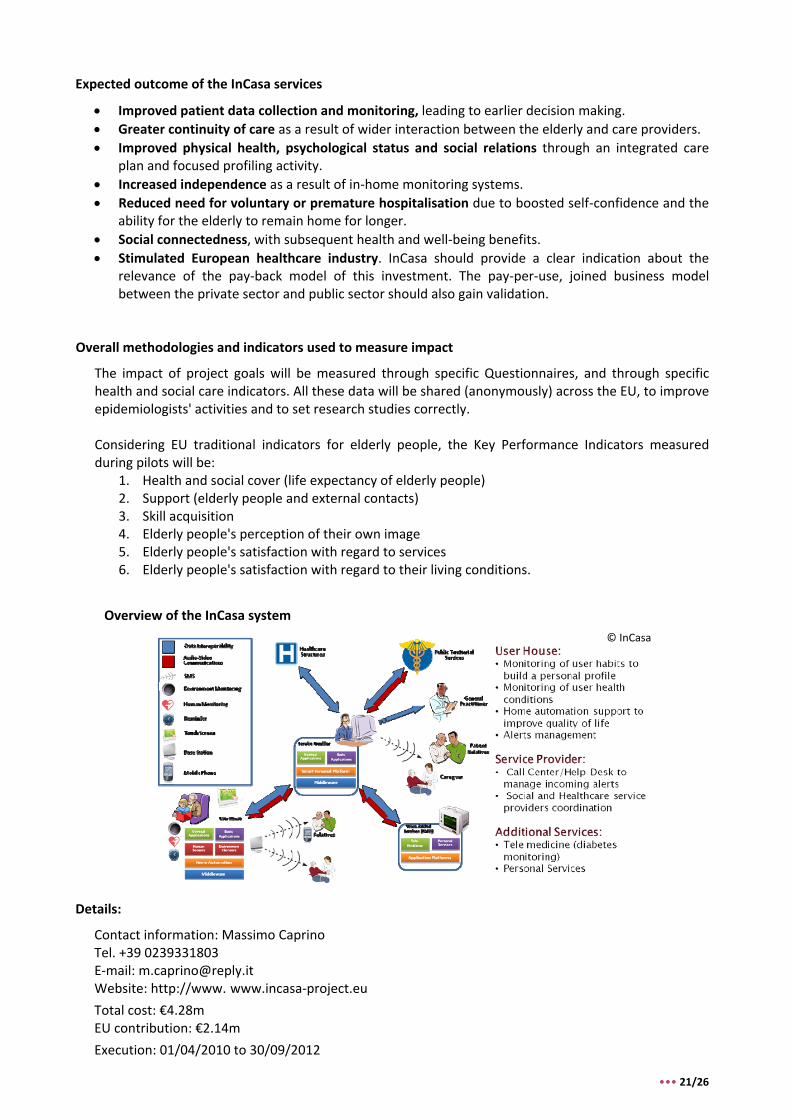
Overview of the InCasa system
© InCasa
Details:
Contact information: Massimo Caprino Tel. +39 0239331803 E‐mail: [email protected] Website: http://www. www.incasa‐project.eu Total cost: €4.28m EU contribution: €2.14m
Execution: 01/04/2010 to 30/09/2012
••• 21/26
Independent
ICT Enabled Service Integration for Independent Living The mission of the project is to define, deliver and pilot a multiplatform digital infrastructure supporting coordinated cross‐sector delivery of sufficient and timely support, thereby effectively preventing or at least slowing the way many older people today inexorably slip towards the edges of safe independent living.
The Pilot Sites (1850 users)
• Greece (Trikala, 400 users) • Ireland (Dublin, 300 users) • Netherlands (Geldrop, 100 users) • UK (Milton Keynes, 200 users) (Hull, 450
users) • Spain (Malaga, 400 users)
The Independent services to be deployed
• Integrated services for independent living, through providing interoperable technology components enabling cooperative healthcare delivery, social care and independence‐enhancing support.
• Collaborative support, among families, voluntary organisations and public services, supporting older people in advance of a need for care.
• Daily Living and Activation Services, including risk management through personal alarms and/or monitoring. On‐demand personal support such as reassurance and emotional support in case of bereavement.
• Physical exercise and cognitive training, including "brain gyms" and interlinking elderly people with social organisations.
• Continued Wellness Services, helping the elderly with disease management through vital signs monitoring.
• Self‐care services, including use of web/TV for distributing preventative information.
Organisations involved
• Municipalities (Milton Keynes UK, Kingston‐upon‐Hull UK)
• Council‐owned companies (Connect MK Ltd, DEKA/KAPI/eTrikala GR)
• Research organisations (University of Hull, TSB ES, Alzheimer Society of Ireland)
• SMEs (Adepteq UK, Stichting Smart Homes NL, Vidavo GR, Emergency Response Ltd IE, Work Research Centre Ltd IE)
• Multinational companies (Philips Technologie UK, Empirica DE)
• Non‐Profit (Fundación Andaluza de Servicios Sociales ES)
• Care providers (St. Anna Care Group NL, Tunstall Healthcare Ltd UK, Salud Responde ES)
Types of users of the Independent services
• Primary users, older people living independently in Europe with a range of needs for support and care.
• Support providers, including social care and healthcare professionals, informal carers and voluntary helpers / charity workers.
22/26 •••
Expected outcome of the Independent services
• Continued 'wellness' and quality of life of the elderly through helping them remain active and able to cope with daily life.
• Opening‐up of communication channels, providing a more general support infrastructure enabling carers with a specialist platform to use that platform in many ways.
• Increased communication and coordinated working of care‐professionals, third sector organisations and family members as a result of integrating affordable technology.
• Increased personalisation of support, technology can be used to monitor, reassure and quickly respond to patient needs.
• More support for sufferers of cognitive ageing or early dementia, through comprehensive assistance to aid independent living.
• Reduced social isolation, through video telephony and provision of local information. • Less technology duplication and greater efficiency, through use of integrated solutions for third‐
sector support and formal services. Ubiquitous patient information will speed‐up care delivery.
Overall Methodologies and Indicators deployed for impact measuring
1. Independence increase: Progress towards extending the time older people can live at home is a core aim of the Objective 1.3 of the work programme and progress will be quantified after year three.
2. Healthcare savings: Quantitative progress measurement will concentrate on annual savings in healthcare per supported person after year three.
3. User satisfaction: Measurement of user satisfaction represents a key means of assessing progress, and is expected to be measurable from year two on.
4. Realised service provision: Real‐world, multi‐user pilots will be measured in terms of the number of citizens provided with service access. Measurement of this indicator will again be possible from year two on.
5. Tested prototype services: It is at the core of the proposed project to cover a range of support needs older people have by integrating yet disjointed ‘silo’‐type service solutions. The number of services tested therefore provides a useful indicator to measure progress in this regard. Here, progress will be measurable across the full project duration.
© European Commission Details:
Contact information: Simon Robinson, Empirica
Tel. +49 228 985 300
E‐mail: [email protected]
Website: http://www.independent‐project.eu
Total cost: €5.25m
EU contribution: €2.63m
Execution: 01/01/2010 to 31/12/2012
••• 23/26
HomeSweetHome
Health Monitoring and Social Integration Environment for Supporting Wide Extension of Independent Life at Home The project is centered around the goal of measuring the real impact of monitoring, cognitive training and e‐Inclusion services on the quality of life of the elderly, the cost of social and healthcare delivered to them, and on a number of social indicators.
Organisations involved: The Pilot Sites (105 users)
• Health Authorities (Departament de Salut de la Generalitat de Catalunya, Azienda USL di Latina, Health Service Executive North‐Eastern Area, Louth County Council)
• Belgium (City of Antwerp, 30 users) • Catalonia (Town of Badalona, 15 users) • Ireland (North Eastern Region, 30 users) • Italy (Town of Latina, 30 users)
• Social Authorities (Zorgbedrijf Antwerpen, Louth County Council, Municipalities of the Latina Province)
HomeSweetHome services to be deployed • Social Service Providers (Zorgbedrijf
Antwerpen, Zorgbedrijf De VoorZorg, Badalona Serveis Assistencials, Darco Servizi, Louth County Council, Municipalities of the Latina Province)
1. Elderly‐friendly videoconferencing, designed for those with no prior exposure to ICT with limited manual skills. In addition to interactive conferencing, this service also provides basic easy‐to‐access information. • Health Care Providers (ZNA ‐ Hospital
Network Antwerpen, Badalona Serveis Assistencials, Departament de Salut de la Generalitat de Catalunya, Azienda USL di Latina, Health Service Executive North‐Eastern Area)
2. Domotic Subsystem (home automation), aimed at enabling people to manage their homes (through the use of actuators) even when their mobility is declining. Contact Centre operators or authorised persons can also control home functions remotely. • Technology Providers (Digipolis, Klinisch
Psychologe St. Franciskusziekenhuis, Health Information Management SA, Telemedicina Rizzoli, Universita La Sapienza ‐ CATTID I, Netwell Centre)
3. Navigation Subsystem, aimed at helping those who are lost to find a predetermined location.
4. Mental Faculty Maintaining Subsystem, using computer games aimed at maintaining the mental faculties.
• Contact Centre Providers (Darco Servizi, EuroCross)
• Healthcare Insurers (Christelijke Mutualiteit Antwerpen)
• Elderly People Representative Association (AGE ‐ European Older People’s Platform)
• Business Consultants (Health Information Management SA)
24/26 •••
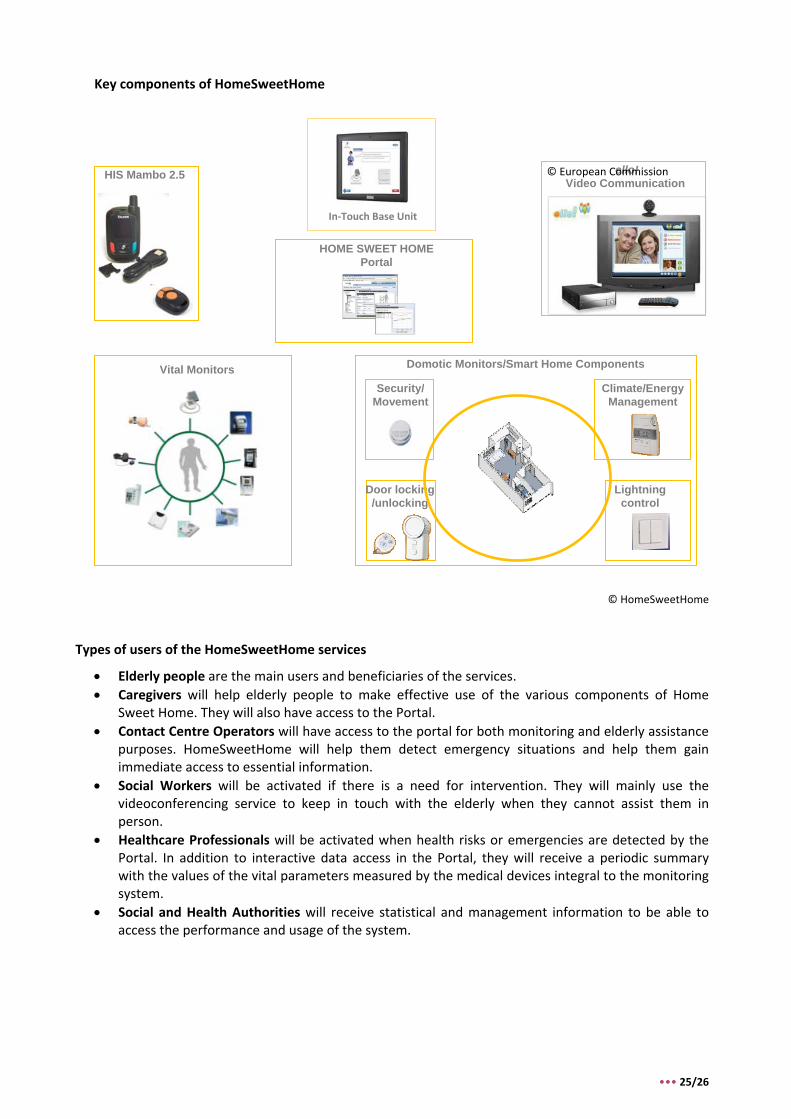
Key components of HomeSweetHome
Vital Monitors
In‐Touch Base Unit
HIS Mambo 2.5
HOME SWEET HOME Portal
Domotic Monitors/Smart Home Components
Security/Movement
Climate/Energy Management
Door locking /unlocking
Lightning control
ello! Video Communication
© European Commission
© HomeSweetHome
Types of users of the HomeSweetHome services
• Elderly people are the main users and beneficiaries of the services. • Caregivers will help elderly people to make effective use of the various components of Home
Sweet Home. They will also have access to the Portal. • Contact Centre Operators will have access to the portal for both monitoring and elderly assistance
purposes. HomeSweetHome will help them detect emergency situations and help them gain immediate access to essential information.
• Social Workers will be activated if there is a need for intervention. They will mainly use the videoconferencing service to keep in touch with the elderly when they cannot assist them in person.
• Healthcare Professionals will be activated when health risks or emergencies are detected by the Portal. In addition to interactive data access in the Portal, they will receive a periodic summary with the values of the vital parameters measured by the medical devices integral to the monitoring system.
• Social and Health Authorities will receive statistical and management information to be able to access the performance and usage of the system.
••• 25/26
Expected outcome of the HomeSweetHome services and Indicators deployed for impact measuring
• Objective 1: Improving the quality of life of elderly people by extending their independent life. • Impact indicator 1.1: Percentage of elderly people in the Study Group whose quality of life has
improved. • Impact indicator 1.2: Percentage of reduction in undetected situations of risk in the Study
Group compared to the Control Group. • Impact indicator 1.3: Reduction in undetected falls in the Study Group.
• Objective 2: Improving the quality of life of caregivers and relatives by offering both respite from the care routine. • Impact indicator 2.1: Percentage of caregivers and relatives of elderly people inserted in the
Study Group who believe that their quality of life has improved. • Objective 3: Improving the social connection of elderly people by allowing them to stay in touch
with their loved ones and the Contact Centre, through an intuitive videoconferencing system. • Impact indicator 3.1: Percentage of elderly people who believe that this aspect of their quality
of life has improved in the Study Group compared to the Control Group. • Objective 4: Compensating for growing physical impairments by easy‐to‐use domotic (home‐
automation) devices. • Impact indicator 4.1: Extension of Independent life in the Study Group compared to the
Control Group • Objective 5: Demonstrating a more efficient business model for care provision, which reduces the
cost of social and health care to elderly people. • Impact indicator 5.1: Percentage reduction in the routine care expenditure • Impact indicator 5.2: Reduction in the Study Group compared to the Control Group in number
and duration of hospitalisation episodes • Impact indicator 5.3: Reduction in number of accesses to Emergency Rooms.
• Objective 6: Exploring alternative work flows which compensate for the ever growing shortage of formal caregivers through the deployment of affordable, reliable and user‐friendly technology. • Impact indicator 6.1: Transfer of workload from formal caregivers and homecare personnel to
elderly people, their informal caregivers and relatives. • Objective 7: Demonstrating that the same technology for AAL can be deployed successfully in
different health and social services set‐ups. • Impact indicator 7.1: Effort necessary to adapt the solution to local health and social services
set‐ups
Details:
Contact information: Marco d'Angelantonio, HiMsa Tel. +32 2 307 64 66 E‐mail: [email protected] Website: http://www.homesweethome‐project.eu
Total cost: €4.91m EU contribution: €2.44m
Execution: 01/03/2010 to 28/02/2013
26/26 •••


For further information: ICT for Inclusion Tel: +32 (0)2 29 90245 Directorate General for Information Society and Media European Commission, BU31 01/66 B‐1049 Brussels Belgium [email protected] http://ec.europa.eu/einclusion







