
Enhanced Role of the PA for Wound Closure in CV Surgery
Heather Austin, PA-C
Cardiothoracic Surgery
Denver, Colorado
1
1
Disclaimers
Heather Austin, PA-C is a paid consultant of Ethicon US, LLC.This promotional educational activity is brought to you by Ethicon US, LLC. and is not certified for continuing medical education.This presentation reflects the opinion of Heather Austin, PA-C. The materials presented do not necessarily represent the opinion of Ethicon US, LLC.For complete indications, contraindications, warnings, precautions, and adverse reactions, please reference full package insert.
2
2

3
3

Today’s discussion will focus on skin and fascia only, so I would like to start with a brief anatomic overview. A cross section of skin and fascia is shown here. As you know, these tissues are composed of layers.
Skin: composed of the outer epidermis and inner epidermis, containing hair, sweat glands, nerve endings, and capillariesSubcutaneous tissue: a layer of loose connective tissue, containing larger blood vessels and fat Fascia and muscle: composed of muscle and muscle aponeuroses, which form the fascia, covering deeper structures
Basic Anatomy of Skin and Fascia
Epidermis
Dermis
Subcutaneous
tissue (fat)
Fascia/muscle
4

Many Factors Influence Wound Healing
5
5

Surgical Technique Influences Wound Healing and Optimal Outcomes
Sound surgical technique is necessary to achieve excellent surgical outcomes
Who is Dr. Halsted? •
What did he do for the field of surgery?•
6
6

7
Tenets of HalstedTissue management
• Obliteration of dead space and adequate removal
of material
• Careful hemostasis to improve conditions for the
procedure and limit infection and dead space
• Sharp anatomic dissection of tissues
• Avoidance of tension
• Gentle handling of tissue William S. Halsted, M.D.
7

For complete indications, contraindications, warnings, precautions, and adverse reactions, please reference full package insert.
*The bleeding situations identified reflect customer insights/market research on optimal adjunctive hemostat utilization. The product solutions should only be used in accordance with their instructions for use.Product recommendations should not supplant medical judgment. Surgeon preference, experience, and patient needs may dictate alternate technique. Review all relevant precautions,the indications, contraindications, warnings, and information for use. Please see package inserts for Full Prescribing Information. The visual does not reflect any sequential order in use.
References: 1.Hemostasis Optimization Program and Next StepsMeeting, dated 06/30/2014. 2. Full Prescribing Information, SURGICEL®Absorbable Hemostat (oxidized regenerated cellulose).Somerville, NJ: Ethicon,Inc.;2010.3. Full Prescribing Information, EVARREST®Fibrin Sealant Patch. Somerville, NJ: Ethicon,Inc.;2014. 4. Full Prescribing Information, SURGIFLO®Hemostatic Matrix. Somerville, NJ: Ethicon,Inc.;2012.5. Full Prescribing Information, EVICEL®Fibrin Sealant (Human). Somerville, NJ: Ethicon, Inc.;2014.
SURGICEL®Absorbable Hemostats
SURGIFLO®Hemostatic Matrix
EVARRESTFibrin Sealant Patch
EVICEL®FibrinSealant (Human)
Continuous oozingWill not stop with compression/
simple packing.The solution
for this bleeding ismore time
consuming than it isdifficult.1
Oxidized regeneratedcellulose (ORC)
An absorbable plant-based
biomaterial that expedites the
hemostasis process by serving
as a scaffold for platelet adhesion
and aggregation that leads to
quick clot formation.2
ProblematicEventhoughthebleedingisaccessible,itcouldbe
trouble. It is more than routine
and likely to be resistant toconventional means and
requires immediate attention
causing disruption to the normal
progression of surgery.1
Fibrin patchFibrinogen/thrombin patch
provides mechanical integrity
and supports clot formation
independently of the patient
coagulation profile in indicated
patients.3
Difficult to accessBleeding that occurs in tight andirregular spaces and you cannot
see the exact source of the bleed.
You are concerned accessing a
tight space will cause more harm.1
Flowable gelatinA gelatin-based foam that flows
into the bleeding area and
serves as a scaffold for platelet
adhesion and can be combined
with thrombin to expedite clot
formation.4
Potentialre-bleeding riskBleeding may be addressed
intraoperatively, but could
later develop into moreserious complications,
especially in high-risk
patients.1
Fibrin sealantFibrinogen and thrombin,
when mixed, create a fibrin
clot independent of the
patient coagulation profile.5
High-pressurevessel bleedingA leak in a high-pressurevessel (aortic or peripheral
vascular suture line) that has
been stopped but could be
catastrophic if it leaks post-op.1
CAT
EGO
RY
SOLU
TIO
NS
BLE
EDIN
G
SIT
UA
TIO
NS
Vascular sealantA surgical adhesive that
secures suture lines and
provides a mechanical seal.
Addressing Surgical BleedingSituations With Adjunctive Hemostats*
© 2017 EthiconUS,LLC.All Rights Reserved. 085690-
171207
8
8

9
Defining Wound Healing
• A wound is a break in the skin that may be accompanied by disruption
to the underlying tissues1
• A healed wound is one where1
– Connective tissues have been repaired
– Wound has been completely epithelialized by regeneration
– Has returned to its normal anatomic structure and function without the need for continued
drainage or dressing
• Some wounds fail to heal properly, resulting in chronic, non healing
wounds, requiring continued management2
• Aberrations in certain phases of healing can result in excessive healing
(e.g. hypertrophic scars, keloids)2
1. Enoch and Leaper. Surgery. 2008;26:31. 2. Ethridge et al. Wound healing. In: Sabiston Textbook of Surgery. 18th ed. 2007
9

10
Our Common Goal
• The goal of tissue management is to help physicians develop a strategy that can
lead to optimal patient outcomes
• Achieving this goal in fascial closure involves improving patient healing and
reducing wound complication
* Low rates of complications in recent publications imply that a strategy can be developed to reduce the occurrence of complications
1. Seiler, et al, Ann Surg 2009;249:576-82. 2. Bloemen, et al, Br J Surg. 2011;98:633-9. 3. Millbourn, et al, Arch Surg 2009; 144:1056-9.
Complication Reported Incidence1,2 Potentially Achievable
Incidence3
Surgical Site Infection (SSI) up to 19% ~5%
Wound dehiscence up to 5% <0.5%*
Incisional hernia up to 23% ~6%
10
11
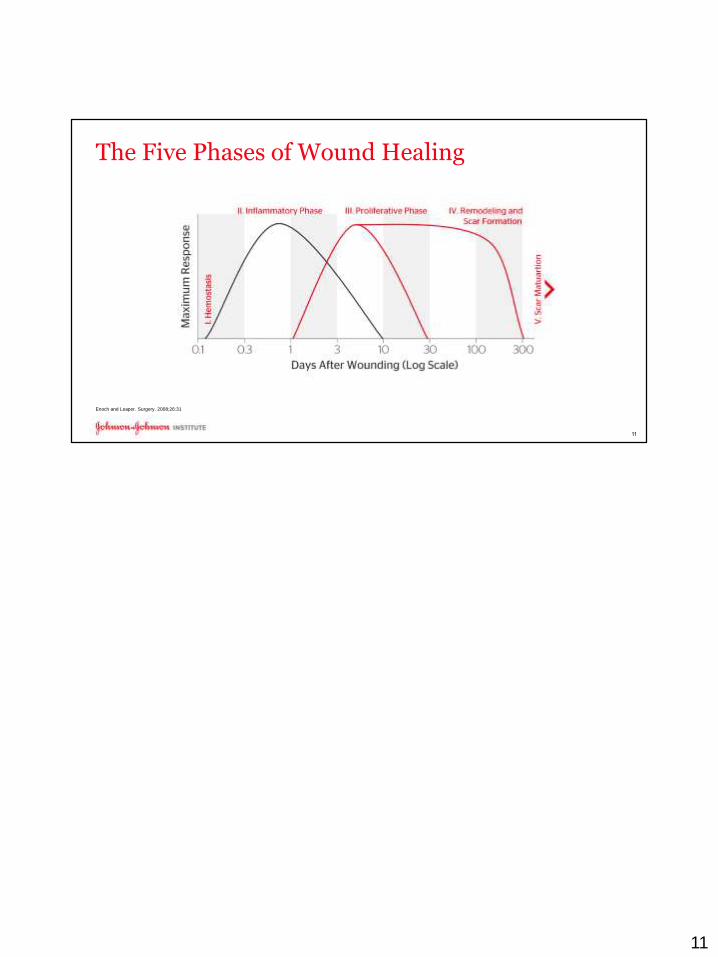
The Five Phases of Wound Healing
Enoch and Leaper. Surgery. 2008;26:31
11

12
Healing Time Guides Choice of Repair Material
*Minimum healing times shown here are for healthy individuals without medical complications
12

13
Overarching Goals for Wound Closure
• Cosmesis– Minimize tissue trauma
– Achieve excellent wound approximation
• Closure strength– Appropriate strength during critical healing period
• Address risk factors for infection– Minimize conduits for infection
– Actively address risk with antimicrobial devices
13

14
Addressing Risk Factors for Infection
SSIs: • Infections that occur in the skin and fascia in the wound created by an invasive
surgical procedure1,2
US: – ≈780,000 / Europe: ≈1.4 million SSIs per year
Increased • risks associated with SSIs1,2
– 2× as likely to die
– 2× as likely to spend time in an ICU
– 5× more likely to be readmitted after discharge
Infection • increases hospital costs1,2
Increases length of stay up to – 21 days worldwide
US: $– 1.6-$3 billion/Europe: €1.5- €19.1 billion per year
SSIs account for an estimated • 17% of healthcare-aquired infections2
SSI = surgical site infection; ICU = intensive care unit; HAI = healthcare-associated infection.
1. National Collaborating Centre for Women’s and Children’s Health. Surgical site infection: prevention and treatment of surgical site infection. Clinical Guideline. October 2008; 2. World Health Organization. WHOGuidelines for Safe Surgery 2009;
14

15
Preventing SSIs
• Many precautions are currently in place to control the risk of bacterial contamination1
– Preoperative skin preparation
– Preoperative trimming
– Preoperative hand and forearm antisepsis by surgical team
– Sterile operative environment
• However, additional controllable risk factors can be addressed with innovative devices2
– Tissue trauma by closure devices such as staples
– Bacterial colonization of the suture
– Entry of bacteria at incision closure during postoperative healing
1. National Collaborating Centre for Women’s and Children’s Health. Surgical site infection: prevention and treatment of surgical site infection. Clinical Guideline. October 2008. 2. World Health Organization. WHO Guidelines for Safe Surgery 2009.
15

16
Implants Can Increase Risk of Infection
• Like all implants, sutures can be colonized by bacteria, which can
lead to biofilm formation1
Colonization of a
suture knot
Colonization of a
braided suture
1. Mangram et al. Infect Control Hosp Epidemiol. 1999;20:250
16

17
Plus Antibacterial Sutures with IRGACARE® MP (Triclosan)The only commercially available sutures with antibacterial protection
• Centers for Disease Control and Prevention
(CDC) Guideline for the Prevention of Surgical
Site Infections 2017 “Consider the use of
triclosan-coated sutures for the prevention of
SSI”*
– *The CDC, WHO, ACS & SIS guidelines on reducing
the risk of surgical site infections are general to
triclosan-coated sutures and are not specific to any one
brand.
• Triclosan coated sutures are now supported by
CDC, World Health Organization, American
College of Surgeons, and Surgical Infection
Society The petri dish image is for
illustrative purposes only.
Zone of inhibition testing
results can vary.1. Infection prevention and control. World Health Organization website. http://www.who.int/gpsc/en/. Accessed November 3, 2016. 2. American College of Surgeons and Surgical
Infection Society: Surgical Site Infection Guidelines, 2016 Update. Journal of the American College of Surgeons. DOI: http://dx.-doi.org/10.1016/j.jamcollsurg.2016.10.029.3. Ming et
al. Surg Infect (Larchmt). 2008;9:451; 4. Wang_2013_The European Journal of Health Economics_ePub_Mar_24_2013.pdf; 5. Edmiston CE, Daoud FC, Leaper D. Is there an
evidence-based argument for embracing an antimicrobial (triclosan)-coated suture technology to reduce the risk for surgical-site infections? A meta-analysis. Surgery.
2013;154:89100. 6. Ford HR, Jones P,Gaines B, Reblock K, Simpkins DL. Intraoperative Handling and Wound Healing: Controlled Clinical Trial Comparing Coated VICRYL® Plus
Antibacterial Suture (Coated Polyglactin 910 Suture with Triclosan) with Coated VICRYL® Suture (Coated Polyglactin 910 Suture). Surg Infect (Larchmt). 2005;6(3):313-321.
• Have been shown in vitro to inhibit bacterial
colonization of the suture for 7 days or more1
• Are effective against pathogens commonly
associated with SSIs1-3
• Prospectively planned meta-analysis of
randomized clinical trials were performed on the
use of suture containing triclosan to lower
surgical site infection rates4,5
• Retain the same handling and performance
characterisics as non-antibacterial suture from the
same materials6
17

Example: Fascia Healing Time Will Impact Closure Choice
• Until the wound regains sufficient strength, the closure device must bear the fascial load of recovering patients1
• Secure fascial closure can help minimize the risk of acute wound-healing failures, such as dehiscence and infection
1 Dubay, et al. Surg Clin N Am 83: 463–481 18
For example, in fascia, research has shown that the wound’s mechanical load is in the red line and the wound’s strength in blue, which is 0 at time 0 is shown here.
Until the wound is bridged by new tissue formation, the wound is completely dependent on the closure device for its initial holding strength.
So while this graph is an example of fascia, this concept applies to all tissues.

INSECT Trial• 3 methods of abdominal wall closure• 625 patients• Seiler et al found no significant benefit related to any specific closure method
• It did find that using a mass closure continuous suture had less cost and decreased OR time v. interrupted stiches.
• Even distribution of tension across the entire length of the suture, resultingin minimal tissue strangulation. Excessive tension leads to tissue necrosis and failure
• Interrupted stiches ensured if suture breakage the incision was held intact with the other suture
19
Seiler_2005_Annals of Surgery_Interrupted or continuous slowly absorbable sutures – Design of a multi-centre randomised trial to evaluate abdominal closure techniques INSECT-Trial [ISRCTN24023541].
19

Fascia Closure Interrupted Suture
20
20

21
21

22
22

Fascia Closure with Continuous Suture
23
23

Normal, healthy scar tissue will develop with proper closure and healing and displays the following features:
Flat surfaceNarrowMatches the skin color
When healing is impaired, abnormal scarring may result. Several examples of complicated and abnormal scarring are shown here.Surgical teams may use several techniques to help prevent abnormal scarring:
Gentle surgical techniqueMinimization of tissue tension
Langers̕ linesTissue perfusion and oxygenationInfection prevention Occlusive dressings Topical adhesives
Why Should You Care About Cosmesis? • Preventing Abnormal
Scarring• Occurs in: Skin
• Key points for prevention:• Precise surgical technique
• Minimize tissue tension• Lines of Langer
• Tissue perfusion and oxygenation
• Prevent infection
• Occlusive dressings
Elevated Depressed
Hypertrophic Keloids
Téot. Wound Repair Regen. 2002;10:93.
Ethridge RT, Leong M and Phillips LG. Wound Healing. In: Townsend CM, Beauchamp RD, Evers BM and Mattox KL, eds.
Sabiston Textbook of Surgery. 18th ed. Saunders, 2007:191-216. 24

Before moving on to the next section, here is a brief summary of what we have discussed thus far:
Healing of acute wounds involves a complex, dynamic series of events.Optimal wound healing occurs by primary intention, but this is not possible in all cases.Many factors may delay or impede wound healing, resulting in long-term complications, but steps can be taken to ensure the best outcomes for your patients.SSI prevention is a critical factor in achieving optimal acute and long-term wound healing.
Wound Healing Summary• Healing of acute wounds involves a complex,
dynamic series of events
• Many factors may delay or impede wound healing, resulting in long-term complications, but steps can be taken to ensure the best outcomes for your patients
• Cosmesis, strength, and addressing risk factors for infection are the overarching goals of wound closure
• SSI prevention is a critical factor in achieving optimal acute and long-term wound healing
25

On the diagram on the screen, the recommended traditional closure options are on the left and the recommended innovative options are on the right.
For Skin:To briefly recap, the ideal closure device for skin should cause minimal tissue trauma, provide maximum strength for the critical wound healing period (5 to 7 days), and should address the risk of infection and provide optimal short-and long-term cosmetic outcomes.
In terms of a traditional closure-only option, closing with MONOCRYL™ Plus is the recommended choice for its strength and infection protection.
When you factor in the innovative closure options, there are now more choices to customize the wound closure method for the specific patient needs.First let’s consider the DERMABOND devices.
DERMABOND devices can give sufficient wound closing strength and infection protection, and excellent cosmesis as they don’t penetrate/puncture the skin like sutures or staples.
For small incisions, DERMABOND® Mini can be used alone without sutures. For medium to long length incisions, DERMABOND ADVANCED™ or PRINEO™ can be used for skin closure.
As an alternative to sutures, STRATAFIX™ Spiral PGA-PCL can be used to give the surgeon the greatest consistency, security, and efficiency in closure.
For deep tissue support below the skin, VICRYL™ Plus or STRATAFIX™ PDO are recommended.
For FasciaTo recap, the ideal closure device for fascia should have low reactivity, maximum strength for the critical wound healing period (14 to 28 days), and should address the risk of infection.For traditional wound closure options, PDS™ Plus Sutures provide optimal wound support for closing fascia due to the strength and infection protection.For innovative options, STRATAFIX™ Symmetric PDS Plus is recommended for this layer as gives greater consistency, security, and efficiency in closure than traditional suture.
Suggestions for Closure
Disclaimer: These are suggestions only. The choice of suture should take into consideration the individual patient, the individual tissue and other factors as determined by the health care practitioner.
26

27
27

28
Suggestions for Closure
Disclaimer: These are suggestions only. The choice of suture should take into consideration the individual patient, the individual tissue and other factors as determined by the health care practitioner.
28

29
Do Traditional Sutures Meet All Needs?Limitations of interrupted closure
with traditional suture:
Limitations of continuous closure
with traditional suture:
• Inconsistent distribution of tension
• Knot-related complications1
• Time consuming2,3
• Strength and security can be
compromised with a break in the suture4,5
Pictures are for technique demonstration only. 1. Sissener T. Comp Anim. 2006;11:14-19. 2. Boutros S, et al. J Trauma Injury Infect Crit Care. 2000;48(3):495-497. 3. Seiler CM, et al. Ann Surg. 2009;249(3):576-582. 4. Wong
NL. J Dermatol Surg Oncol. 1993;19:923-931. 5. Dubay DA, et al. Surg Clin North Am. 2003;83(3):463-481.
29

30
STRATAFIX™ Knotless Tissue Control DevicesEliminate the need to compromise
• More strength and security– Interrupted suturing without knot-related complications1
• More efficiency – More efficient than continuous suturing1,*
• More consistency– Tension control and approximation during closure1,*
*Compared to traditional sutures
1. Ethicon, Inc.: STRATAFIX Claims Matrix SFX-308-12. 2013. (Claim #50)
30

31
STRATAFIX™ Knotless Tissue Control DevicesAn unmatched portfolio to meet our customer's needs
1. Ethicon, Inc. STRATAFIX Knotless Tissue Control Devices Consolidated Claims Matrix SFX-308-12. 2013. 2. Ethicon, Inc. AST-2013-0603: Performance Testing of STRATAFIX SYMMETRIC PDS PLUS Size 0 & 1 devices—initiation strength in
porcine tissue. 2014.
The petri dish image is for illustrative purposes only.
Zone of inhibition testing results can vary.
The petri dish image is for illustrative purposes only.
Zone of inhibition testing results can vary.
31

32
STRATAFIX™ Knotless Tissue Control DevicesThe most versatile knotless tissue control device
STRATAFIX™ Spiral
MONOCRYL™ Plus
STRATAFIX™
Spiral PDS™ Plus
STRATAFIX™ Spiral
PolypropyleneTissue HealingSTRATAFIX™
Symmetric PDS™ Plus
1-2 Weeks
1-2 Weeks
3+ Weeks
4-6 Weeks
Varies
Fascia
SkinSubcuticular
SkinSubcutaneous
Deep Tissue
Organ
Only Ethicon offers tissue control devices, with Plus antibacterial technology, that provide appropriate strength for closing high-tension areas, such as fascia1*
*Refers to STRATAFIX™ Symmetric PDS™ Plus Device only
1. Ethicon, Inc.: STRATAFIX Claims Matrix SFX-308-12. 2013.
32

33
STRATAFIX™ Symmetric PDS™ PlusKnotless Tissue Control Device
• Proven to have superior tissue holding strength in fascia1
– 22% superior to Looped PDS
– 32% better than Vicryl® Interrupted
1. Ethicon, Inc.: STRATAFIX Comparative Data. 2015
33

34
DERMABOND® Skin Closure DevicesCore technology
• The core technology is the Topical Skin Adhesive– Clinically proven, proprietary formulation of 2-octyl cyanoacrylate combined with additives to ensure controlled
application and consistent polymerization1
• Topical skin closure method that does not puncture skin (unlike sutures and staples)
• Provides strength and protection to many types of wounds and skin incisions– Binds to skin and quickly polymerizes to create a strong, flexible film that is waterproof3
– Up to the strength of 3-0 Monocryl (poliglecaprone 25) subcuticular suture ex vivo*4
*Clinical Significance Unknown
1. DERMABOND Advanced™ PI; 3. Ethicon, Inc.: Prineo report 07PD048 by Keplinger 4. CSR: 06TR071, Bhende 6/22/2012: In vitro study of Dermabond Prineo Skin Closure System to kill bacteria on contact
34

35
Addressing Risk Factors Associated with SSIs
Provide a flexible microbial barrier with • 99%
protection in vitro for 72 hours against organisms
commonly responsible for SSIs1.2*
Demonstrated in vitro • inhibition of gram-positive
bacteria (MRSA and MRSE†) and gram-negative
bacteria (E coli)1,2,‡
Effective • microbial barrier that prevents bacteria
from entering the incision site1,2,‡
*Staphylococcus epidermidis (S epidermidis)/Escherichia coli (E coli)/ Staphylococcus aureus (S aureus)/Pseudomonas aeruginosa/Enterococcus faecium. †MRSA=Methicillin-resistant S aureus,
MRSE=Methicillin-resistant S epidermidis. ‡Clinical significance is unknown 1. Ethicon, Inc. DERMABOND PRINEO Skin Closure System Matrix. 043337-151113. 2. Ethicon, Inc. DERMABOND Topical Skin Adhesive 043048-
151106.
35

36
DERMABOND® Skin Closure DevicesPortfolio of products
36

37
DERMABOND® Skin Closure Devices22 cm, 42 cm and 60 cm
• A 2-octyl cyanoacrylate topical skin adhesive for
proven strength*1 and microbial protection†2
– Sets in approximately 60 seconds when applied to mesh2
– Two-hour working time3
• Combines the proven strength, flexibility, and
antimicrobial protection of DERMABOND
ADVANCED® Topical Skin Adhesive with the added
support and security of a self-adhering mesh to further
facilitate both wound-edge approximation and an
optimal healing environment.4
– Contains initiator that accelerates polymerization of liquid adhesive
*In porcine skin models † In vitro studies. 1. Shapiro AJ, Dinsmore RC, North JH Jr. Tensile strength of wound closure with cyanoacrylate glue. Am Surg. 2001;67(11):1113-1115. 2. DERMABOND PRINEO Skin Closure System (22 cm)
[package insert]. Somerville, NJ: Ethicon, Inc. 2014. 3. Ethicon, Inc.: McCrum LM. Study 06PD058: DERMABOND ProTape working time and polymer characterization as a function of working time. 2006.
4. Ethicon, Inc.: DERMABOND PRINEO Skin Closure System Matrix. 043320-151113.
37

Staples
38
38

DERMABOND® PRINEO® Skin Closure System: Technique Video
39
Here is a video of the PRINEO technique.

Dermabond Prineo
40
40
41
41
42
42

43
43

44
44

45
45

46
EVICEL® Fibrin Sealant (Human) IMPORTANT SAFETY INFORMATION
IndicationEVICEL® Fibrin Sealant (Human) is indicated as an adjunct to hemostasis for use in patients undergoing surgery, when control of bleeding by standard surgical techniques (such as suture, ligature, or cautery) is ineffective or impractical.
Contraindications▪Do not inject directly into the circulatory system. Intravascular application of EVICEL® may result in life-threatening thromboembolic events.▪Do not use in individuals known to have anaphylactic or severe systemic reaction to human blood products.▪Do not use for the treatment of severe or brisk arterial bleeding.▪Do not use EVICEL® for spraying in endoscopic or laparoscopic procedures where the minimum recommended distance from the applicator tip to the target site cannot be ensured.
Warnings and Precautions▪Life-threatening air or gas embolism has occurred with the use of spray devices employing a pressure regulator to administer EVICEL®. This event appears to be related to the use of the spray device at pressures higher than recommended and/or at distances closer than recommended to the surface of the tissue.▪Monitor changes in blood pressure, pulse, oxygen saturation, and end-tidal CO2 when spraying EVICEL® because of the possibility of gas embolism.▪To reduce the risk of potentially life-threatening gas embolism, spray EVICEL® using only pressurized CO2 gas at the pressures and distances recommended for the specific tips.▪Use EVICEL® spray application only if it is possible to accurately judge the spray distance, especially during endoscopic or laparoscopic procedures.▪Prior to applying EVICEL®, dry surface areas of the wound by standard techniques (e.g. intermittent application of compresses, swabs, use of suction devices). Prepare and administer EVICEL® according to the instructions and with only devices recommended for this product.▪May carry a risk of transmitting infectious agents, e.g. viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent and theoretically, the Creutzfeldt-Jakob disease (CJD) agent.
The most common adverse reactions reported in clinical trials are peripheral edema, abdominal abscess, infection, hematoma, incision site hemorrhage, vascular graft occlusion, postoperative wound complication and decreased hemoglobin.
For complete indications, contraindications, warnings, precautions, and adverse reactions, please reference full package insert.
021323-170803
46

EVARREST® Fibrin Sealant Patch
Important Safety Information
Indications and Usage
EVARREST® is a fibrin sealant patch indicated for use with manual compression as an adjunct to hemostasis in adult patients undergoing surgery, when control of bleeding by
conventional surgical techniques (such as suture, ligature, and cautery) is ineffective or impractical.
Limitations for Use
Cannot be used in place of sutures or other forms of mechanical ligation in the treatment of major arterial or venous bleeding.
Not for use in children under one month of age
Laparoscopic and other minimally invasive surgeries where manual compression would be difficult to achieve.
Important Safety Information
For topical use only. Apply immediate manual compression over the entire surface of the patch and maintain contact pressure for 3 minutes to control the bleeding.
Do not apply intravascularly. This can result in life threatening thromboembolic events.
Do not use to treat bleeding from large defects in arteries or veins where the injured vascular wall requires conventional surgical repair and maintenance of vessel patency or
where there would be persistent exposure of EVARREST® to blood flow and/or pressure during absorption of the product. Thrombosis can occur if absorbed systemically.
Do not use in individuals known to have anaphylactic or severe systemic reaction to human blood products. EVARREST ® can cause hypersensitivity reactions including
anaphylaxis.
Avoid application to contaminated areas of the body or in the presence of active infection. Infection can occur.
EVARREST contains oxidized regenerated cellulose which adheres to bleeding surfaces. Inadvertent adhesions can occur.
Avoid use in, around, or in proximity to, foramina in bone or areas of bony confines where swelling may cause compression.
Use the least number of patches required to cover the entire bleeding area. Portions of excess patch material can become dislodged and migrate to other areas of the body.
Do not use more than eight 2x4 inch (5.1 x 10.2 cm) or more than four 4x4 inch (10.2 x 10.2 cm) patches.
Use in patients who have been previously exposed to EVARREST® has not been studied.
May carry a risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent.
The adverse reactions reported during clinical trials occurred in less than 1% of all cases and included deep venous thrombosis, pulmonary embolism, blood fibrinogen increase,
anastomotic hemorrhage, post procedural and intra-abdominal hemorrhage, abdominal distension, anemia, gastrointestinal hemorrhage, thoracic cavity drainage, pleural
effusion, abdominal abscess, ascites, localized intra-abdominal fluid collection, cardiac failure, operative hemorrhage, and ischemic bowel.
Pediatrics: Safety and effectiveness in pediatric patients have not been established. Use in children under the age of one m onth may be unsafe or ineffective due to small size
and limited ability to apply the patch as recommended.
Please see package insert for EVARREST® Full Prescribing Information.
To report SUSPECTED ADVERSE REACTIONS, contact ETHICON Customer Support Center at 1-877-384-4266 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
030813-171115 47
47

48
EVITHROM® Thrombin, Topical (Human) for Topical Use Only
Lyophilized Powder for Solution
EVITHROM® is a topical thrombin indicated as an aid to hemostasis whenever oozing blood and minor bleeding from capillaries and small venules
is accessible and control of bleeding by standard surgical techniques (such as suture, ligature or cautery) is ineffective or impractical.
EVITHROM® may be used in conjunction with an Absorbable Gelatin Sponge, USP.
Important Safety Information
•For topical use only.
•Do not inject.
•Apply EVITHROM® on the surface of bleeding tissue only.
•The amount of EVITHROM® required depends upon the area of tissue to be treated and the method of application. In clinical studies, volumes up
to 10 ml were used in conjunction with Absorbable Gelatin Sponge.
•Do not use for the treatment of severe or brisk arterial bleeding.
•Do not use in individuals known to have anaphylactic or severe systemic reaction to human blood products. Hypersensitivity reactions, including
anaphylaxis, may occur.
•There is a potential risk of thrombosis if absorbed systemically.
•May carry a risk of transmitting infectious agents such as viruses and theoretically, the Creutzfeldt-Jakob disease (CJD) agent, despite
manufacturing steps designed to reduce the risk of viral transmission.
•The most common adverse reactions during clinical trial (reported in at least 2% of subjects treated with EVITHROM®) were prolonged activated
partial thromboplastin time, increased INR, decreased lymphocyte count, prolonged prothrombin time and increased neutrophil count.
•None of the patients treated with EVITHROM developed antibodies to human thrombin or to human Factor V/Va. The clinical significance of these
findings is unknown.
For complete indications, contraindications, warnings, precautions, and adverse reactions, please reference full package insert.
021328-180430
48
49
SURGICEL Essential Product Information
INDICATIONS
SURGICEL® Absorbable Hemostat (oxidized regenerated cellulose) is used adjunctively in surgical procedures to assist in the control of capillary, venous, and small arterial
hemorrhage when ligation or other conventional methods of control are impractical or ineffective. SURGICEL® ORIGINAL, SURGICEL® FIBRILLAR™, SURGICEL® NU-KNIT®, and
SURGICEL® SNoW™ Absorbable Hemostats can be cut to size for use in endoscopic procedures.
PRECAUTIONS
Use only as much SURGICEL® Absorbable Hemostat as is necessary for hemostasis, holding it firmly in place until bleeding stops. Remove any excess before surgical closure in order
to facilitate absorption and minimize the possibility of foreign body reaction.
In urological procedures, minimal amounts of SURGICEL® Absorbable Hemostat should be used and care must be exercised to prevent plugging of the urethra, ureter, or a catheter by
dislodged portions of the product.
Since absorption of SURGICEL® Absorbable Hemostat could be prevented in chemically cauterized areas, its use should not be preceded by application of silver nitrate or any other
escharotic chemicals.
If SURGICEL® Absorbable Hemostat is used temporarily to line the cavity of large open wounds, it should be placed so as not to overlap the skin edges. It should also be removed from
open wounds by forceps or by irrigation with sterile water or saline solution after bleeding has stopped.
Precautions should be taken in otorhinolaryngologic surgery to assure that none of the material is aspirated by the patient. (Examples: controlling hemorrhage after tonsillectomy and
controlling epistaxis.)
Care should be taken not to apply SURGICEL® Absorbable Hemostat too tightly when it is used as a wrap during vascular surgery (see Adverse Reactions section of the complete
product package insert).
ADVERSE EVENTS
“Encapsulation” of fluid and foreign body reactions have been reported.
There have been reports of stenotic effect when SURGICEL® Absorbable Hemostat has been applied as a wrap during vascular surgery.
Paralysis and nerve damage have been reported when SURGICEL® Absorbable Hemostat was used around, in, or in proximity to foramina in bone, areas of bony confine, the spinal
cord, and/or the optic nerve and chiasm.
Blindness has been reported in connection with surgical repair of a lacerated left frontal lobe when SURGICEL® Absorbable Hem ostat was placed in the anterior cranial fossa.
Possible prolongation of drainage in cholecystectomies and difficulty passing urine per urethra after prostatectomy have been reported.
For more information, please consult your doctor or for product quality and technical questions, call 1-800-795-0012. For complete product information including indications,
contraindications, warnings, precautions, and adverse reactions, please reference the individual product package inserts.
063768-180827
49

50
SURGICEL® Powder Absorbable Hemostat Essential Product Information
INDICATIONS
SURGICEL® Powder (oxidized regenerated cellulose) is used adjunctively in surgical procedures to assist in the control of capillary, venous, and small arterial hemorrhage when ligation or other
conventional methods of control are impractical or ineffective.
CONTRAINDICATIONS
• Do not inject or place SURGICEL® Powder into an open blood vessel. Do not use to treat bleeding from large defects in arteries or veins.
• SURGICEL® Powder should not be used to control hemorrhage from large arteries or veins.
• When SURGICEL® Powder is used to help achieve hemostasis in, around, or in proximity to foramina in bone, areas of bony confine, the spinal cord, or the optic nerve and chiasm, it must always be
removed after hemostasis is achieved since it will swell and could exert unwanted pressure.
• SURGICEL® Powder should not be used for implantation in bone defects, such as fractures, since there is a possibility of interference with callus formation and a theoretical chance of cyst formation.
WARNINGS
• Closing with SURGICEL® Powder in a contaminated wound without drainage may lead to complications and should be avoided.
• SURGICEL® Powder should not be impregnated with anti-infective agents or with other materials such as buffering or hemostatic substances.
• SURGICEL® Powder is dry and there may be difficulties in precise delivery under certain circumstances. Unintentional device placement may result in powder scattering and device migration that may
increase the risk of adhesion formation.
• Although SURGICEL® Powder is bactericidal against a wide range of pathogenic microorganisms, it is not intended as a substitute for systemically administered therapeutic or prophylactic antimicrobial
agents to control or to prevent postoperative infections.
• Do not attempt to trim the applicator tip.
PRECAUTIONS
•SURGICEL® Powder should not be used in conjunction with autologous blood salvage circuits, because its fragments may pass through the transfusion filters of blood-scavenging systems.
•Use only as much SURGICEL® Powder (oxidized regenerated cellulose) as is necessary and apply only where needed for hemostasis. Remove any excess before surgical closure in order to facilitate
absorption and to minimize the possibility of foreign body reaction.
•In urological procedures, minimal amounts of SURGICEL® Powder should be used and care must be exercised to prevent plugging of the urethra, ureter, or a catheter by dislodged portions of the
product.
•Since absorption of SURGICEL® Powder could be prevented in chemically cauterized areas, its use should not be preceded by application of silver nitrate or any other escharotic chemicals.
•If SURGICEL® Powder is used temporarily to line the cavity of open wounds, it should be removed by irrigation with sterile water or saline solution after bleeding has stopped.
•Precautions should be taken in otorhinolaryngologic surgery to ensure that none of the material is aspirated by the patient (e.g., controlling hemorrhage after tonsillectomy and controlling epistaxis).
•This applicator tip is not intended for laparoscopic or other endoscopic use.
ADVERSE EVENTS
•Paralysis and nerve damage have been reported when other SURGICEL® products were used around, in, or in proximity to foramina in bone, areas of bony confine, the spinal cord, and/or the optic nerve
and chiasm.
•Blindness has been reported in connection with surgical repair of a lacerated left frontal lobe when other SURGICEL® products were placed in the anterior cranial fossa (see WARNINGS and
PRECAUTIONS).
•Foreign body reactions have been reported with other products from the SURGICEL® Family of Absorbable Hemostats.
•Burning has been reported when other SURGICEL® products were applied after nasal polyp removal. Headache, burning, stinging, and sneezing in epistaxis and other rhinological procedures, and
stinging when SURGICEL® product was applied on surface wounds (varicose ulcerations, dermabrasions, and donor sites) have also been reported.
•For more information and technical questions, call 1-800-795-0012. For complete information including indications, contraindications, warnings, precautions, adverse reactions, and directions for use,
consult the product package insert.
071582-180827
50

SURGIFLO® Hemostatic Matrix Kit Essential Product Information
(Made from Absorbable Gelatin Sponge, USP) with ThrombinDESCRIPTION: SURGIFLO® with Thrombin (SURGIFLO® Hemostatic Matrix Kit) is intended for hemostatic use by applying to a bleeding surface.
ACTIONS
When used in appropriate amounts SURGIFLO® is absorbed completely within 4 to 6 weeks.
INTENDED USE/INDICATIONS
SURGIFLO®, mixed with thrombin solution, is indicated in surgical procedures (other than ophthalmic) as an adjunct to hemostasis when control of bleeding by ligature or other conventional methods is
ineffective or impractical.
CONTRAINDICATIONS
Do not use SURGIFLO® in intravascular compartments because of the risk of embolization.•
Do not use SURGIFLO® in patients with known allergies to porcine gelatin.•
Do not use SURGIFLO® in closure of skin incisions because it may interfere with the healing of skin edges. This interference • is due to mechanical interposition of gelatin and is not secondary to
intrinsic interference with wound healing.
WARNINGS
SURGIFLO® should not be used in the presence of infection and should be used with caution in contaminated areas of the body• • SURGIFLO® should not be used in instances of pumping arterial
hemorrhage. SURGIFLO® will not act as a tampon or plug in a bleeding site.
SURGIFLO® should be removed from the site of application when used in, around, or in proximity to foramina in bone, areas of • bony confine, the spinal cord, and/or the optic nerve and chiasm
because it may swell resulting in nerve damage.
Excess SURGIFLO® should be removed once hemostasis has been achieved.•
The safety and effectiveness of SURGIFLO® for use in ophthalmic procedures has not been established.•
SURGIFLO® should not be used for controlling post• -partum intrauterine bleeding or menorrhagia.
The safety and effectiveness of SURGIFLO® has not been established in children and pregnant women.•
The blue flexible applicator tip should not be trimmed to avoid exposing internal guidewire.•
The white straight applicator tip should be trimmed away from the surgical area. Cut a square angle to avoid creating a sharp• tip.
PRECAUTIONS
Safe and effective use of SURGIFOAM® Sponge has been reported in a published neurologic retrospective study involving • 1700 cases in Europe. Safe and effective use in neurosurgery has not been
proven through randomized, controlled clinical studies in the United States.
SURGIFLO® is supplied as a sterile product and cannot be • resterilized. • SURGIFLO® should not be used for packing unless excess product that is not needed to maintain hemostasis is removed.
SURGIFLO® may swell up to 20% upon contact with additional fluid.
SURGIFLO® should not be used in conjunction with autologous blood salvage circuits. •
SURGIFLO® should not be used in conjunction with • methylmethacrylate adhesives. • In urological procedures, SURGIFLO® should not be left in the renal pelvis or ureters to eliminate the potential
foci for calculus formation.
51
51

SURGIFLO® Hemostatic Matrix Kit Essential Product Information
(Made from Absorbable Gelatin Sponge, USP) with Thrombin CONTINUED
ADVERE EVENTS
A total of 142 patients received SURGIFOAM® Sponge during a clinical trial comparing SURGIFOAM® Sponge to another absorbable gelatin sponge. In general, the following adverse events
have been reported with the use of absorbable porcine gelatin-based hemostatic agents:
• Gelatin-based hemostatic agents may serve as a nidus for infection and abscess formation and have been reported to potentiate bacterial growth.
• Giant cell granulomas have been observed at implant sites when used in the brain.
• Compression of the brain and spinal cord resulting from the accumulation of sterile fluid have been observed.
• Multiple neurologic events were reported when absorbable gelatin-based hemostatic agents were used in laminectomy operations, including cauda equina syndrome, spinal stenosis,
meningitis, arachnoiditis, headaches, paresthesias, pain, bladder and bowel dysfunction, and impotence.
• The use of absorbable gelatin-based hemostatic agents during the repair of dural defects associated with laminectomy and craniotomy operations, has been associated with fever, infection,
leg paresthesias, neck and back pain, bladder and bowel incontinence, cauda equina syndrome, neurogenic bladder, impotence, and paresis.
• The use of absorbable gelatin-based hemostatic agents has been associated with paralysis, due to device migration into foramina in the bone around the spinal cord, and blindness, due to
device migration in the orbit of the eye, during lobectomy, laminectomy, and repair of a frontal skull fracture and lacerated lobe.
• Foreign body reactions, “encapsulation” of fluid, and hematoma have been observed at implant sites.
• Excessive fibrosis and prolonged fixation of a tendon have been reported when absorbable gelatin-based sponges were used in severed tendon repair.
• Toxic shock syndrome was reported in association with the use of absorbable gelatin-based hemostats in nasal surgery.
• Fever, failure of absorption, and hearing loss have been observed when absorbable hemostatic agents were used during tympanoplasty.
52
52

Thank You for your time
and attention!
© Medical Device Business Services, Inc. 2019. 104945-190107 53
53







