

www,cdc.gov
EmpathyIdentification with
and understanding ofEmpathy, Compassion.
and understanding of another’s situation,
feelings and motives.

Accessibility to care.
Psychosocial obstacles.
Mobility and stability.
Treatment planning.
Financial.
Communication.
Medical status.
Continuity of care.
Preventive care.
Accessible.Family centered.
Continuous.Comprehensive.Co-coordinated.Companionate.
Culturally competent.Preventive orientated.Individualized recall.
Emergency care.
Dr. Heinrich Hoffman Dr. Heinrich Hoffman • “Let me see if Philip can be a little gentleman; let me
see if he is able to sit still for once at table.” Thus spoke, in earnest tone, the father to his son; and the mother looked very grave to see Philip so misbehave. But Philip he did not mind; his father who was so kind
S th ht tl hild i till … See the naughty, restless child, growing still more rude and wild, till his chair falls over quite. Philip screams with all his might, catches at the cloth, but then, that makes matters worse again. Down upon the ground they fall, glasses, bread, knives forks and all … Poor Papa and poor Mamma look quite cross, and wonder how they shall make their dinner now.”

“… the disorders known as the attention – deficit hyperactive
disorders are the chronic neurological conditionneurological condition
resulting from persistent dysfunction with the central
nervous system and not related to gender, level of intelligence,
or cultural environment.”
Most extensively studied childhood disorder.
Proper assessment and diagnosis are essential for proper intervention.
Not simply a problem of hyperactivity & impulsivity, but the ability to monitor activity in p y, y y
appropriate settings.
Poor ability to relate to time and chronology.
Cognitive / behavioral.
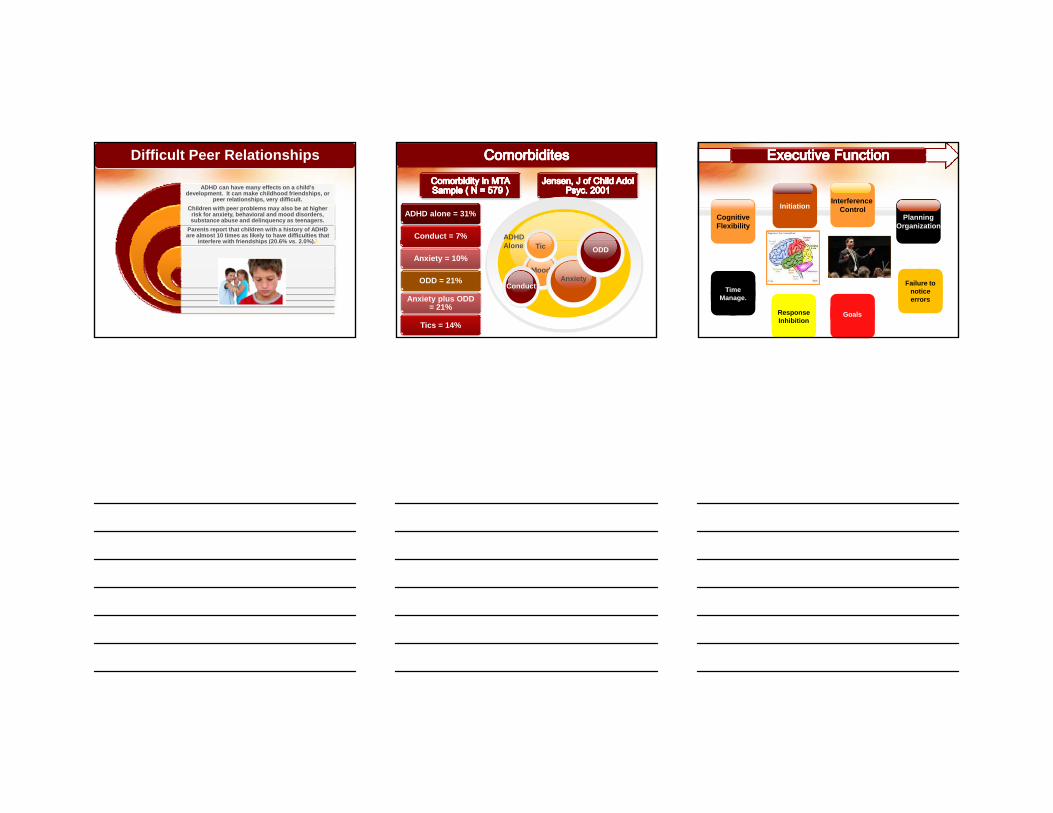
AAP: ADHD Assessment GuidelinesAAP: ADHD Assessment Guidelines
AAP CLINICALGUIDELINES, 2000

Canada 3.8-9.4% of
children.
Australia
Netherlands 1.3% teens
Australia3.4% of
children.
New Zealand6.7%
children, 2-3% teens.
Germany4.2%
children.
India
5-29% children.
China 6-9% children.
PE usually normal.
Increased incidence of
“soft” neurologic
i
Dysmorphicfeatures.
signs.
Careful developmental
analysis.
Vision.
Hearing.
18 criteria. 9 inattention symptoms.
9 hyperactivity / impulsivity symptoms.
Individuals must display 6 of 9
inattention symptoms or 6 of 9 hyperactivity -impulsivity features for at least 6 months.
Two distinct settings –global diagnosis.
Symptoms present on a regular basis for
more than 6 months.
3 subtypes.

Inattention
1. Inattention to details.2. Difficulty sustaining attention.3. Seems not to listen.4 Fails to finish
Impulsivity
1. Blurts out answers.
2. Difficulty waiting turn.
3. Often interrupts or intrudes.
Hyperactivity
1. Fidgets / squirms.
2. Unable to remain seated.
3. Cannot play quietly.
4. Talks excessively4. Fails to finish
tasks.5. Avoids tasks that requires attention.6. Loses items.7. Easily distracted.8. Forgetful in daily activities.9. Organizing.
excessively.5. “On the Go” –
motor driven.6. Runs and
climbs excessively.
Inattentive
6 of 9
Hyperactive
Impulse
6 of 9
Combined
6 of 9 in both
Inattentive HyperactiveImpulsive
Male / Female 1 : 1 3-9 : 1
Accidents Less Common Common
Peer Relations Unpopular Rejected
Co-Morbidities Anxiety / Depression
ODD / CD
Outcomes Less symptom decline than hyperactivity
ODD/CD poorerHyperactivity declines with puberty
ADHD can have many effects on a child's development. It can make childhood friendships, or
peer relationships, very difficult.Children with peer problems may also be at higher
risk for anxiety, behavioral and mood disorders, substance abuse and delinquency as teenagers.
Parents report that children with a history of ADHD are almost 10 times as likely to have difficulties that
interfere ith friendships (20 6% s 2 0%) 1
Difficult Peer Relationships
interfere with friendships (20.6% vs. 2.0%).1 ADHD
ADHD alone = 31%
Conduct = 7%
Mood
ConductAnxiety
Tic ODDAlone
Anxiety = 10%
ODD = 21%
Anxiety plus ODD = 21%
Tics = 14%
CognitiveFlexibility
PlanningOrganization
InitiationInterference
Control
TimeManage.
ResponseInhibition
Goals
Failure to notice errors

Genetic factors.
Biochemical / neurotransmitter.
Lack of a single identifiable
etiology.
Environmental.
Social.
“Polycausality”.
Genetic susceptibility.
Heritable estimates 0.5 – 0.98.
Monozygotic twins 0.8 -0.99 (Faraone, 2000).
Hyper / Impulsive breeds true.
Inattentive, Combined do not (Faraone,2000).

Severe hyperkinetic with
fetal distress. Taylor 1991.
Maternal bleeding,
smoking, illicit drug use. S i h
Chronic infancy sleep problems.
Thunstrum Sprinch-Burkminster
1993.
LBW.Kotimaa 2003, Thapar 2003.
Pre-term birth. Breslau 1996, Whitaker 1997.
Thunstrum2002. LES.
Peterson 2001.
Parental mental health.
Russo 1994.
Marital discord.
Milberger1997,
Edwards 1995.
No evidence of food dyes.
Mattes 1981.
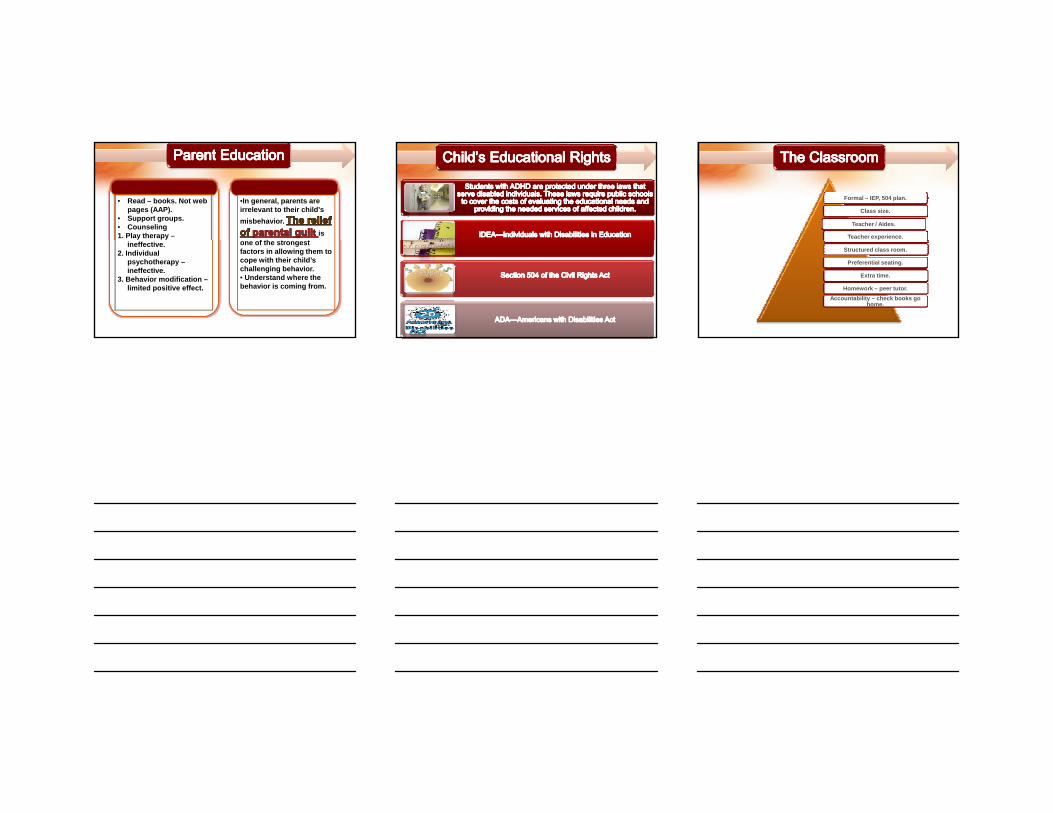
ForgetfulLosing things
ProcrastinationIndecision
Children Adults
Poor org.Follow through complex tasks
Difficulty comp tasksNo multitaskingShifting attention
g gLack of focusEasily distracted
Poor time management
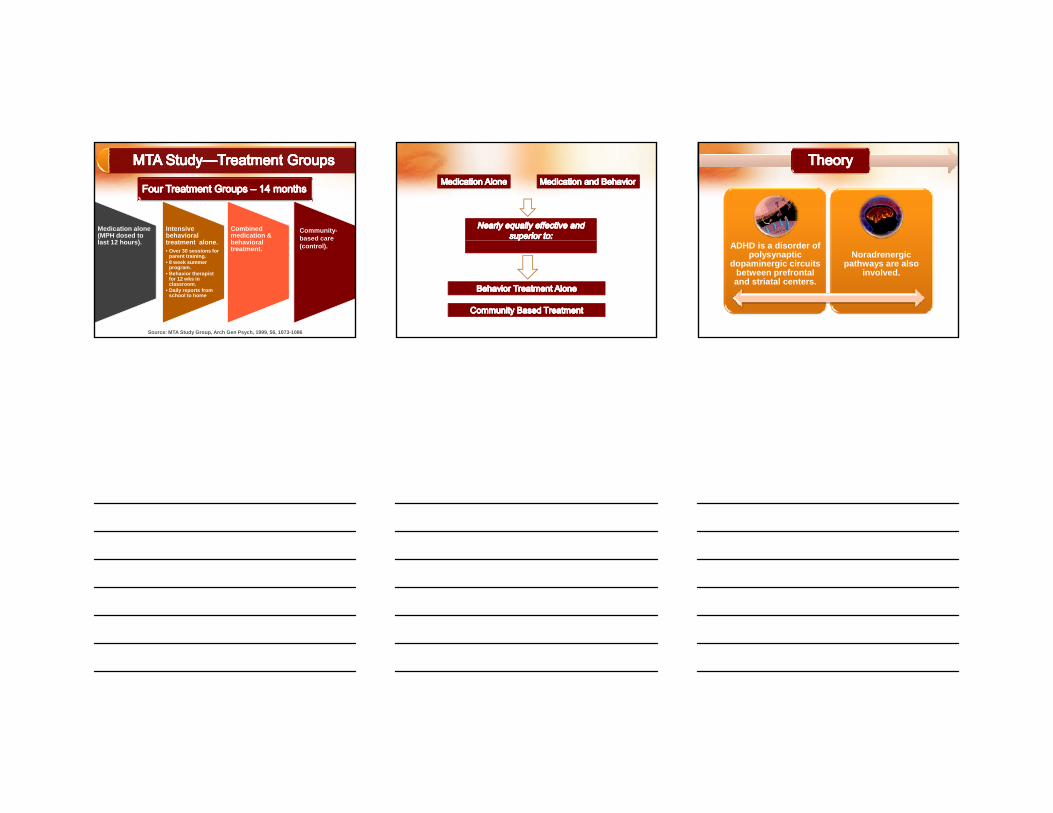
SquirmsOn the goCannot sit quietlyTalks excessively
Highly active jobLong hoursConstant activity
Child Adult
Cannot wait turnBlurtsIntrudesInterrupts
ImpatientLow frustration levelsSnap decisionsLoses temper easily
Talks excessively Easily bored

ChildrenChildren AdultsAdults1. Poor grades.2. Repeating grades.3. Fewer friends.4. Disruptive in school.5 S h l i
1. Poor employment hx.2. Poor driving record.3. Academic
underachievement.4 Multiple marriages5. School suspensions.
6. Increased drop out rates.7. Delinquency / conduct
problems.8. Disruption of family
function.
4. Multiple marriages.5. Legal problems.6. Accidents / injuries.7. Teenage pregnancy.8. STD.9. Smoking.
Barkley RA et al. J Am Acad Child Adol Psych; 2006
ClassroomEducation
ADHD
Home Medication
•In general, parents are irrelevant to their child's misbehavior.
is f th t t
• Read – books. Not web pages (AAP).
• Support groups.• Counseling1. Play therapy –
one of the strongest factors in allowing them to cope with their child’s challenging behavior.• Understand where the behavior is coming from.
ineffective.2. Individual
psychotherapy –ineffective.
3. Behavior modification –limited positive effect.
Formal – IEP, 504 plan.
Class size.
Teacher / Aides.
Teacher experience.
Structured class room.
Preferential seating.
Extra time.
Homework – peer tutor.Accountability – check books go
home.

The ClassroomThe Classroom
Tests – accommodations.
Homework.
U k th thUse peaks rather than average.
Classroom situation.
Bottom line – ADHD don't need all accommodations, but only those that address
specific difficulties and you don’t want the child to hate school : fail and destroy self-
confidence.
Technique Description ExamplePositive Reinforcement Privileges contingent on
performance.Play on X-box.
Time-out Removing access to positive reinforcement due to problem
Hits sib impulsively –goes to room. Time out applies to dental team.p
behavior.pp
Response cost Withdrawing rewards contingent on problem or unwanted behavior.
Child loses free time for not doing homework.
Token economy Combines positive reinforcement and response cost.
Earns “stars” for doing homework, loses “stars” for misbehavior. Used for dental treatment.

65–75 % of 5899 children assigned to stimulant medication vs. 4-30% to placebo improved (161 RCT by Greenhill, 1998).
Review of 78 studies by Jadad et al. (1999) consistently supported the superiority of stimulant over non-drug treatment.
ADHD Multimodal Treatment Analysis (MTA) conducted by AAP – large randomized controlled study in children 7 to 10 years of age showed stimulant along with behavior therapy showed greatest improvement in academic performance and measures of conduct.
Medication alone (MPH dosed to l t 12 h )
Intensive behavioral t t t l
Combined medication & b h i l
Community-based care
Source: MTA Study Group, Arch Gen Psych, 1999, 56, 1073-1086
last 12 hours). treatment alone.• Over 30 sessions for
parent training. • 8 week summer
program.• Behavior therapist
for 12 wks in classroom.
• Daily reports from school to home
behavioral treatment.
based care (control). ADHD is a disorder of
polysynaptic dopaminergic circuits
between prefrontal and striatal centers.
Noradrenergic pathways are also
involved.

Dopamine.
• Reward seeking behavior.
• Central psychomotor neurotransmitter.
• Bowden 1988, Cook 1995, Doughtery 1999
• LaHoste 1996, Malone 1994 R t 1999
Norepinephrine.
1994, Rappaport 1999
• Heilman 1991, Shekim1979, Shen, 1984, Zametkin 1984.
Psychostimulants – increase arousal, alertness, reduce fatigue.
Methylphenidate.
Dextroamphetamine.
Amphetamine salts.
Non – Stimulant.
Atomoxetine.
AMPH/MPH diffuses into vesicle Releasing DA into cytoplasm
Storage vesicle
NEURON ( NEURON ( presynapticpresynaptic )
AMPH and MPH blocks uptakeInto vesicle
AMPH is taken into cellCausing DA release
into synapseDA TransporterMPH and AMPH
Inhibit transporter uptake

Why Newer MedicationsWhy Newer Medications?
Stimulants are short acting – 3 / 5 hours.
Multiple doses cause peaks & valleys giving rise to roller coaster effect
through the day.
Smooth effect through day is desirable.g y
Going to school nurse is stigmatizing.
Public hysteria about side effects.
Market competition $$$$$.
Newer drug delivery systems.
• Slow smooth release.Transdermal patch
Combination.
Prodrug• Transdermal – patch.
Enantiomers and isomers.
• Dextro / levo.
Prodrug.
Newer classes of drugs.
• Noradrenergic / nonstimulant.
Osmotic Release Oral
System (OROS)
• Adderall XR.• Ritalin LA
Pulsated Delivery Beads
• DaytranaTransdermalsystem

Generic Class Daily Dosage Duration
StimulantsMPHShort Acting (Ritalin, Metadate) BID / TID 3-5 hrs
Intermediate (Ritalin SR, Metadate ER) QD / BID 3-8 hrs
LA (Concerta) QD 8-12 hrs
AmphetamineShort Acting (Dexedrine) BID / TID 4-6 hrs
Intermediate (Adderall) QD / BID 6-8 hrs
LA (Adderall XR) QD 8-12 hrs
RCT report 4-10%.
Most dose related.
RCT report 4-10%.
Most dose related.
RCT report 4-10%.
Most dose related.JitterinessHeadache
Delayed sleep
Reduced appetite
Stomachache
More effect on above avj. children.
Most in year one, less in year 2, levels off in y ,
3yd year.
Effect on wt and ht is dose dependent – 2 cm ht and 2.7 kgs wt. in 3
years
No rebound after stimulant discontinued.

School
Family therapy

Structure TSD. N2O, Sedation, OR
Avoid treatment
during drug holidaysy
PreventionTraumaChild abuse

If this were my kid!!!!!If this were my kid!!!!!The purpose of this study was to
compare the oral and demographic characteristics of children with attention-deficit The children with ADHD had a
statistically higher prevalence ofhyperactivity disorder (ADHD) to those of a control group of
children. A sample of 25 dental records of children medicated for
ADHD was compared to 127 records of healthy children not
receiving any medication.
statistically higher prevalence of toothache, bruxism, bleeding
gums, and oral trauma histories than the control group (chi
square, p < 0.05).
Bimstein E, Primoch R. Spec Care Dentist. 2008 May-Jun;28(3):107-10.
Biological disorder exacerbated by social factors.
At the extreme
of normal behavior variation.
Treated because of associated distress
and disability.
Life-long condition.

Early short appointments.Positive reinforcement.
Concept
ConceptKnow your drugs.
Be cool.
Avoid drug holidays.
Keep disorder in mind.
Concept
Concept







