DR R DE LACY
ULCERATIVE COLITIS
DEFINITION
� Inflammation of the lining of the large bowel (colon and rectum)
� Aetiology is poorly understood
� Genetic factors - aggregation in families
- identical twin concordance 10%
- dizygotic twin concordance 3%
- ethnic diff in incidence
- genetic markers and linkages
� Environmental factors – diet, breastfeeding
ONSET
� Adolescence to early adulthood
� 15-25 yrs, seeing patients as young as 3 years of age
SYMPTOMS
� Rectal bleeding
� Diarrhoea
� Abdominal cramps
� Weight loss
� Fever
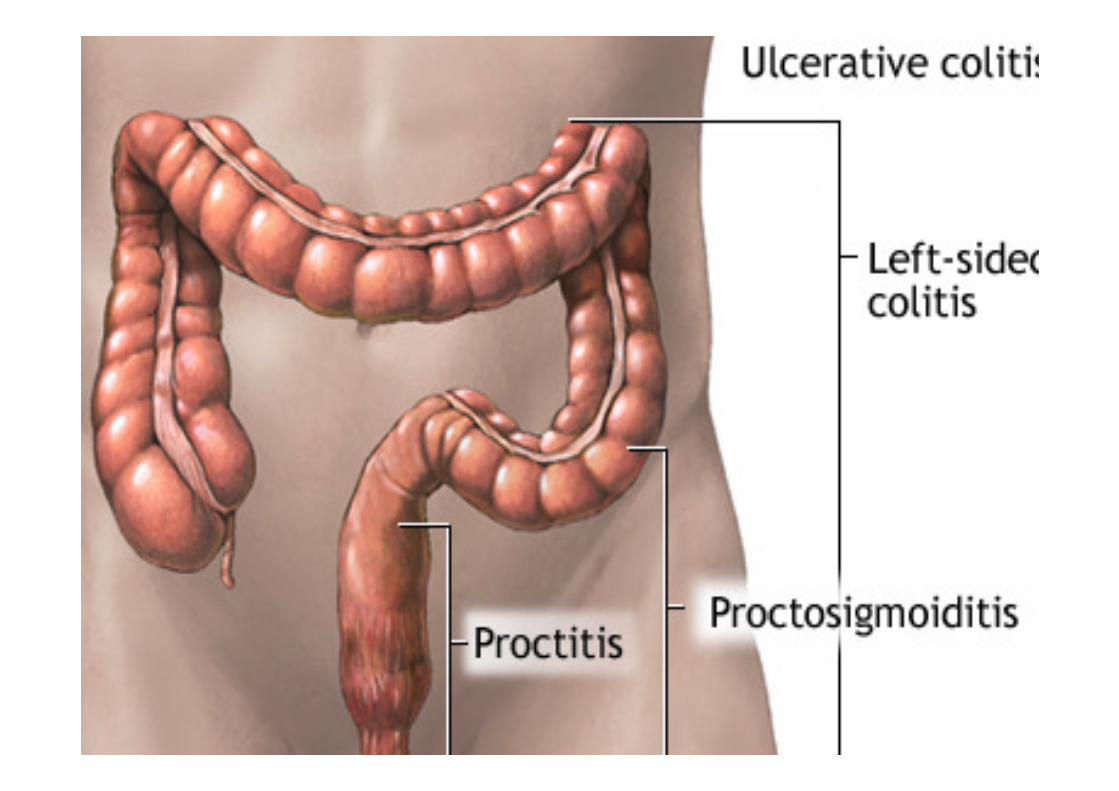
CLASSIFICATION
ULCERATIVE PROCTITIS
PROCTOSIGMOIDITIS
LEFT-SIDED COLITIS
PANCOLITIS
FULMINANT COLITIS
SEVERITY OF DISEASE
� Mild disease - less than 4 stools/day
- with or without blood
- mild abdominal pain or cramping
- tenesmus
- no systemic signs of toxicity
- normal ESR
SEVERITY OF DISEASE
� Moderate disease - > 4 stools/day
- minimal signs of toxicity- anaemia not requiring transfusion
- moderate abdominal pain
- low grade fever
� Severe disease - > 6 bloody stools/day
- evidence of toxicity
- fever, tachycardia
- anaemia
- elevated ESR
SEVERITY OF DISEASE
� Fulminant disease- > 10 stools/day
- continuous bleeding
- toxicity
- abdominal tenderness & distension- anaemia – blood transfusion
- colonic dilation
- toxic megacolon
- colonic perforation
EXTRA-INTESTINAL MANIFESTATIONS
� Aphthous ulcer of the mouth
� Clubbing
� Iritis, uveitis, episcleritis
� Seronegative arthritis
� Ankylosing spondylitis
� Sacroiliitis
� Erthyema nodosum
� Pyoderma gangrenosum
� Primary sclerosing cholangitis
� Autoimmune haemolytic anaemia
� Deep vein thrombosis & pulmonary embolism

DIAGNOSIS
� FBC – anaemia, thrombocytosis
� U&E – hypokalaemia, hypomagnesemia, pre-renal
� Liver function tests
� X-ray
� Urinalysis
� Stool culture
� ESR
� CRP
� Perinuclear antineutrophil cytoplasmic antibody (p-ANCA), a myeloperoxidase antigen, is found more commonly in ulcerative colitis
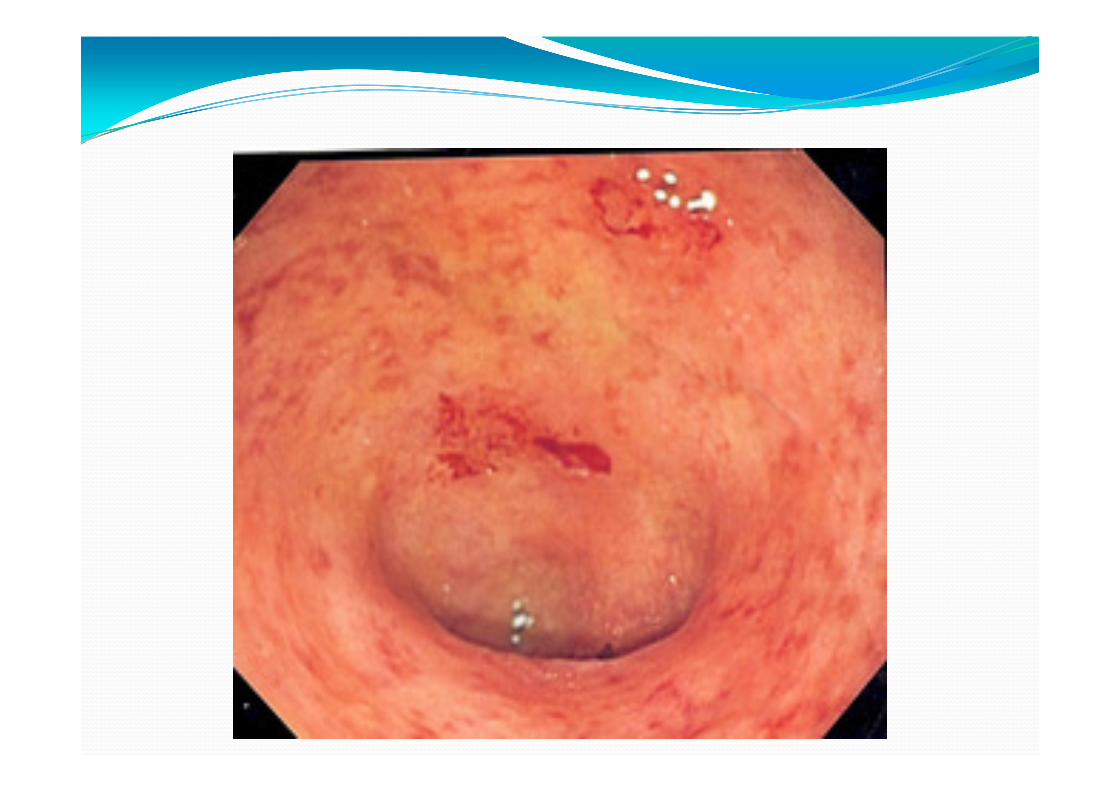
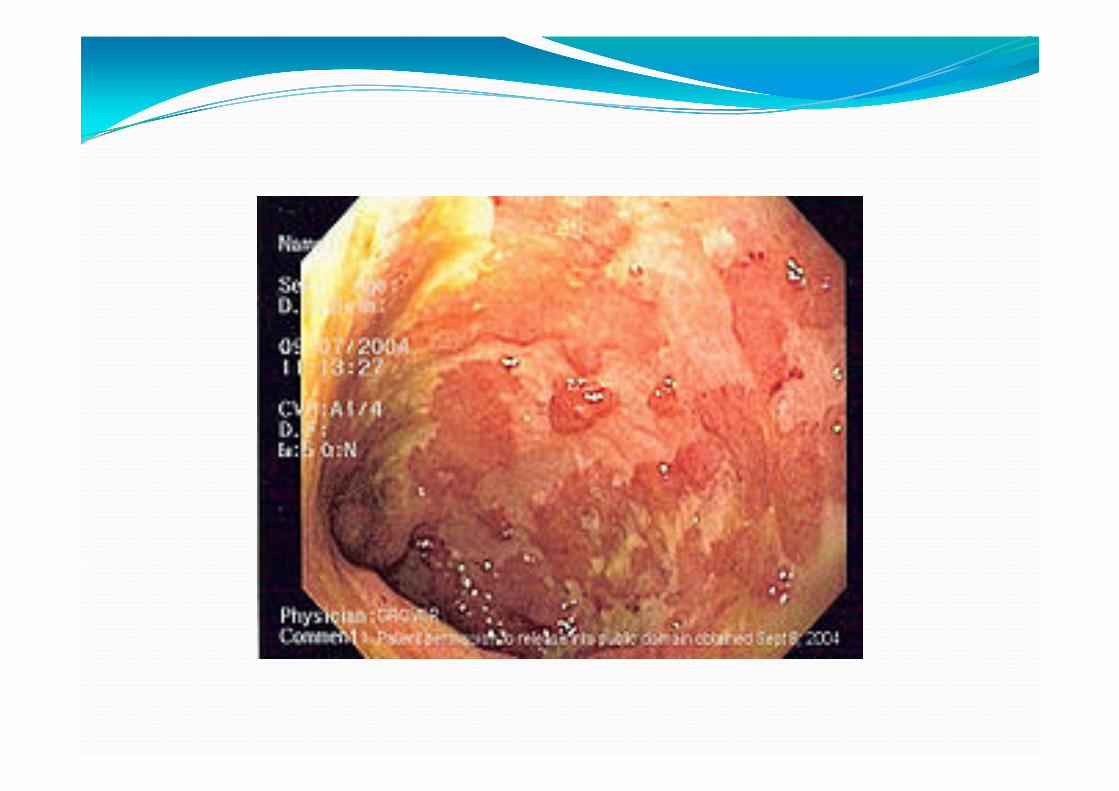
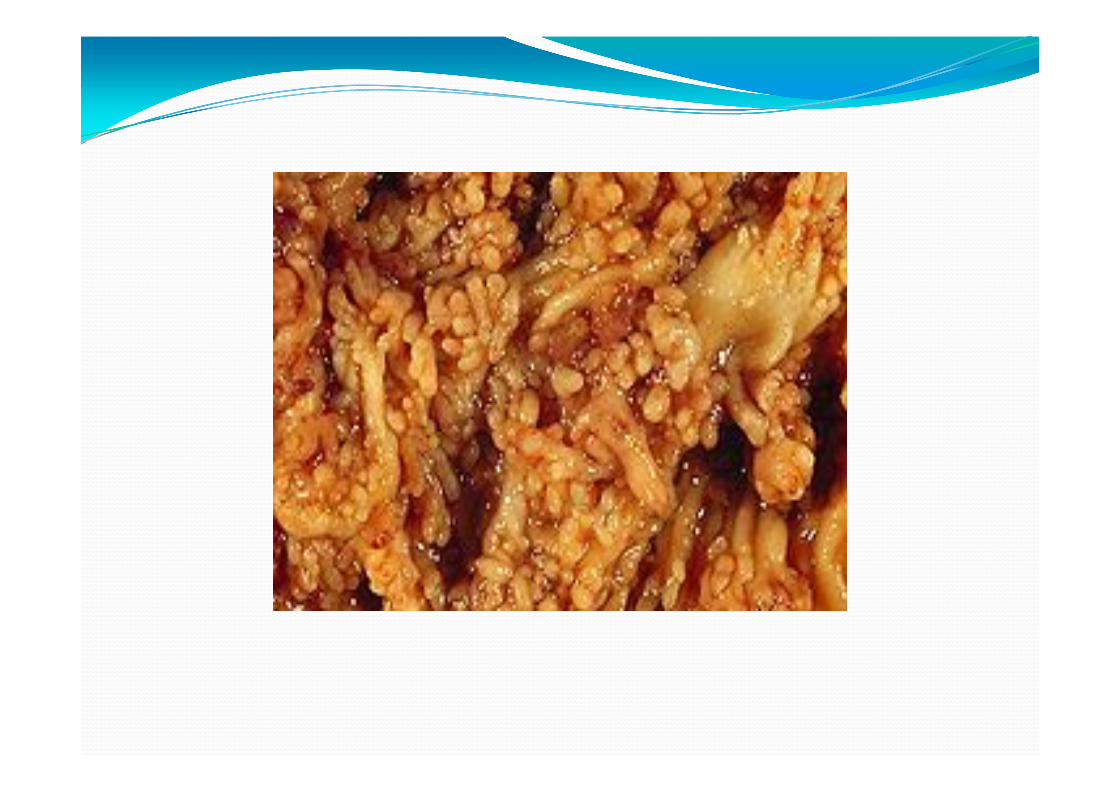
ENDOSCOPY
� Full colonoscopy to the ceacum and terminal ileum
� Loss of the vascular appearance of colon
� Erythema and friability of mucosa
� Superficial ulceration, confluent
� Pseudopolyps
� Continuous from the rectum, universally involved
� Biopsy for histology and culture - CMV
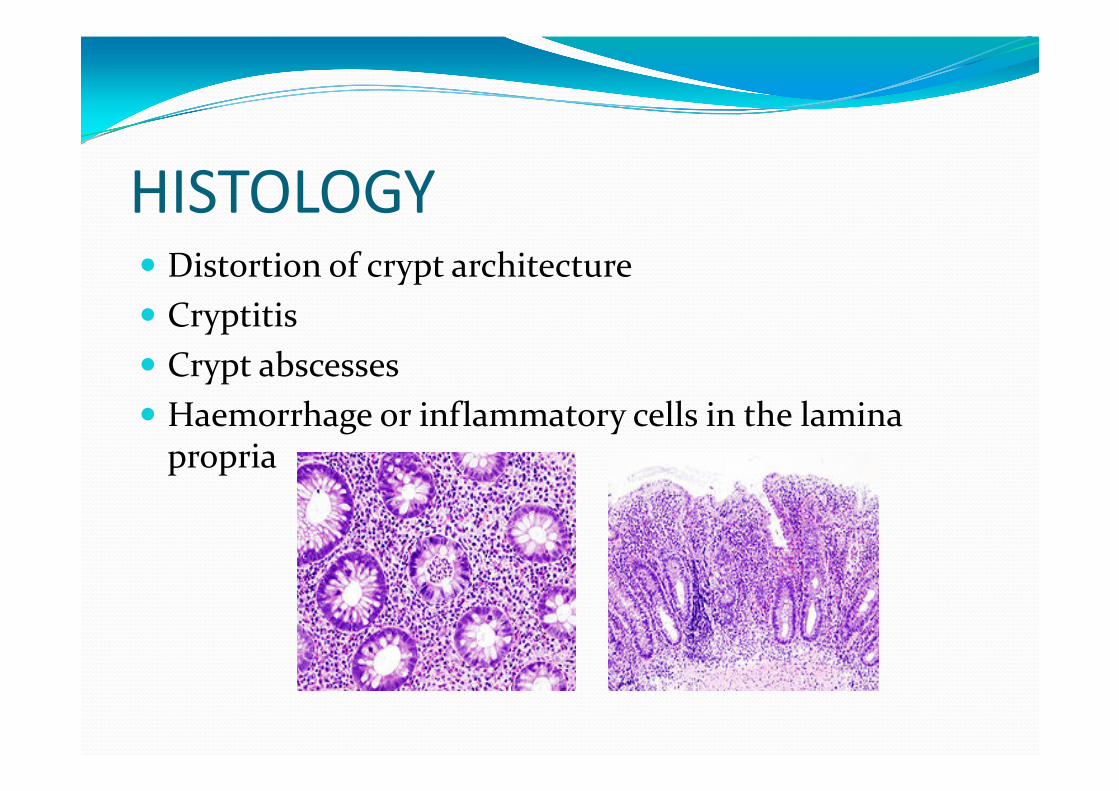
HISTOLOGY
� Distortion of crypt architecture
� Cryptitis
� Crypt abscesses
� Haemorrhage or inflammatory cells in the lamina propria
DIFFERENTIAL DIAGNOSIS
� Crohn’s disease
� Indeterminate colitis
� Infective colitis
� Pseudomembranous colitis
� Ischaemic colitis
� Chemical colitis
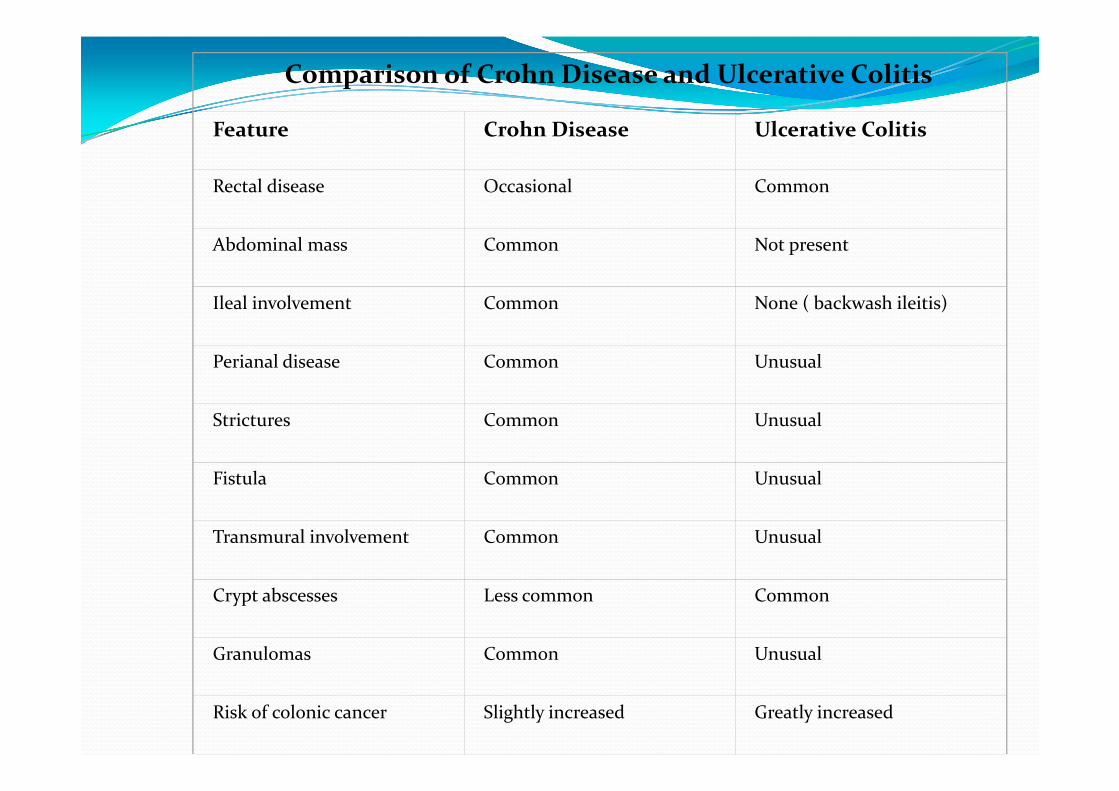
Comparison of Crohn Disease and Ulcerative Colitis
Feature Crohn Disease Ulcerative Colitis
Rectal disease Occasional Common
Abdominal mass Common Not present
Ileal involvement Common None ( backwash ileitis)
Perianal disease Common Unusual
Strictures Common Unusual
Fistula Common Unusual
Transmural involvement Common Unusual
Crypt abscesses Less common Common
Granulomas Common Unusual
Risk of colonic cancer Slightly increased Greatly increased
MANAGEMENT
MEDICATION
� Aminosalicylates – sulfasalazine
� Corticosteroids – prednisone
� Azathioprine
� Infliximab
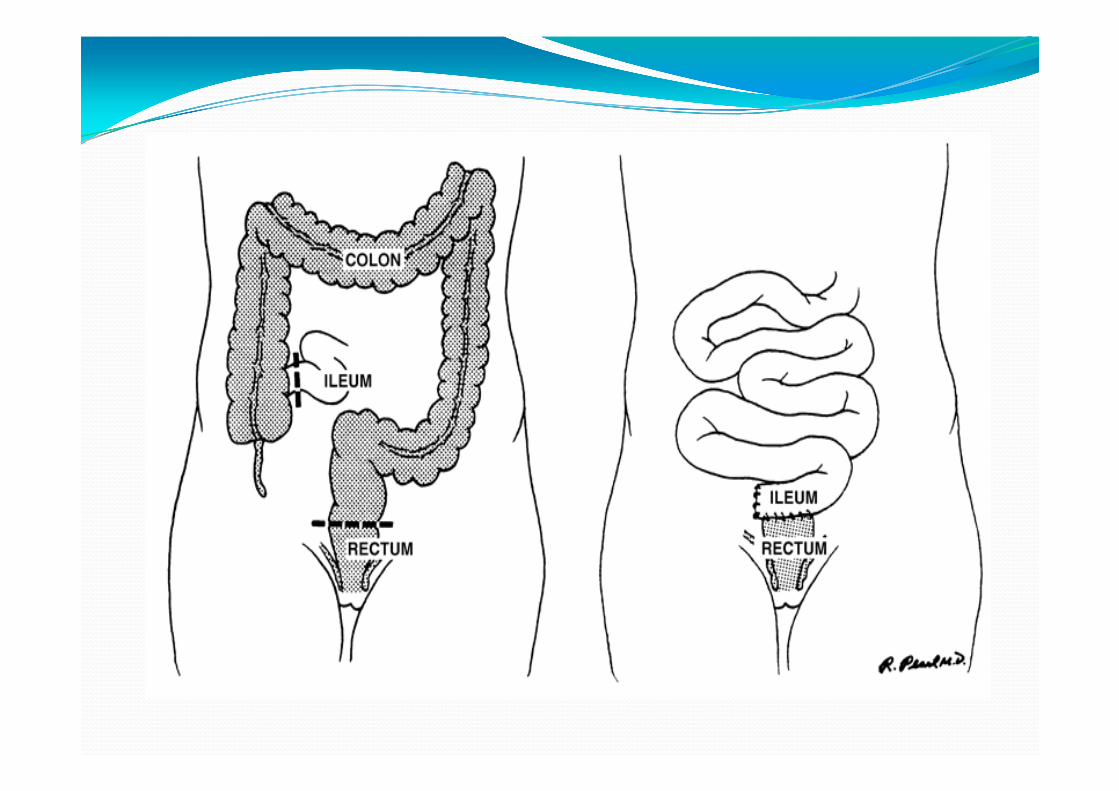
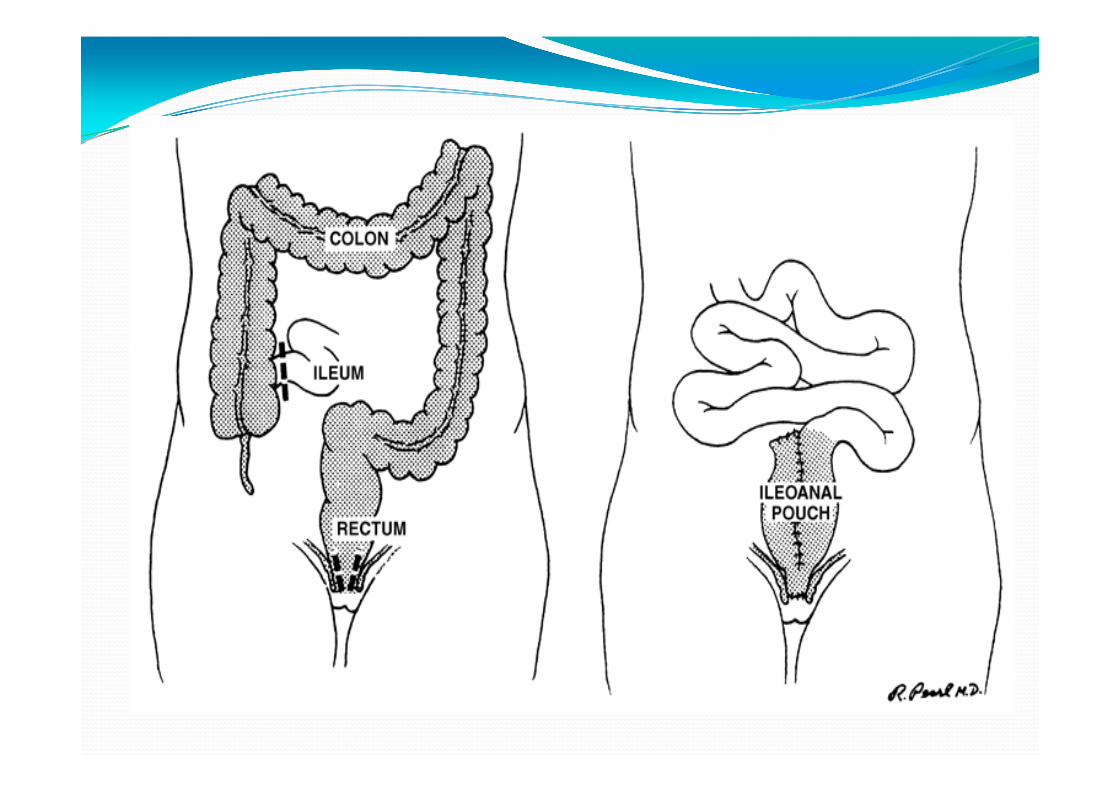
SURGERY
COLECTOMY
Indications
� Failed medical management
� Exsanguinating haemorrhage
� Colonic perforation
� Carcinoma
� Toxic megacolon

CROHN’S DISEASE
� Idiopathic, chronic transmural inflammation
� Leads to fibrosis and obstructive symptoms
� Affects gastrointestinal tract from mouth to anus
� Imbalance between pro and anti-inflammatory mediators
� 30% small bowel involvement
� 30% colon only involvement
� 40% small and colon
PRESENTATION
� Chronic diarrhoea
� Abdominal pain
� Low-grade fever
� Weight loss
� Fatigability
� Cologastric fistulae- feculent vomiting
� Enterovesicular fistulae- recurrent UTI, pneumaturia
� Enterovaginal fistulae- feculent vaginal discharge
� Enterocutaneous fistulae- feculent skin soiling
� Intraabdominal, retroperitoneal abscesses
PRESENTATION
� 50-70% children have terminal ileum involvement
� 30-40% children gastric or duodenal inflammation
� Pancreatitis
� 30% patients – peri-anal complications- skin tags, perianal abscesses & fistulae, anal fissures
DIFFERENTIAL DIAGNOSIS
� Amoebiasis
� Appendicitis
� Behcet disease
� Celiac disease
� Gastroenteritis-bacterial/viral
� Giardiasis
� Ulcerative colitis
� IBS
DIAGNOSIS� FBC – anaemia, thrombocytosis
� U&E – hypokalaemia, hypomagnesemia, pre-renal
� Liver function tests- hypoalbuminaemia
� X-ray
� Urinalysis
� Stool culture
� ESR
� CRP
� Anti-S cerevisiae antibodies [ASCA]) are found more commonly in Crohn disease – higher rate of surgery
DIAGNOSIS
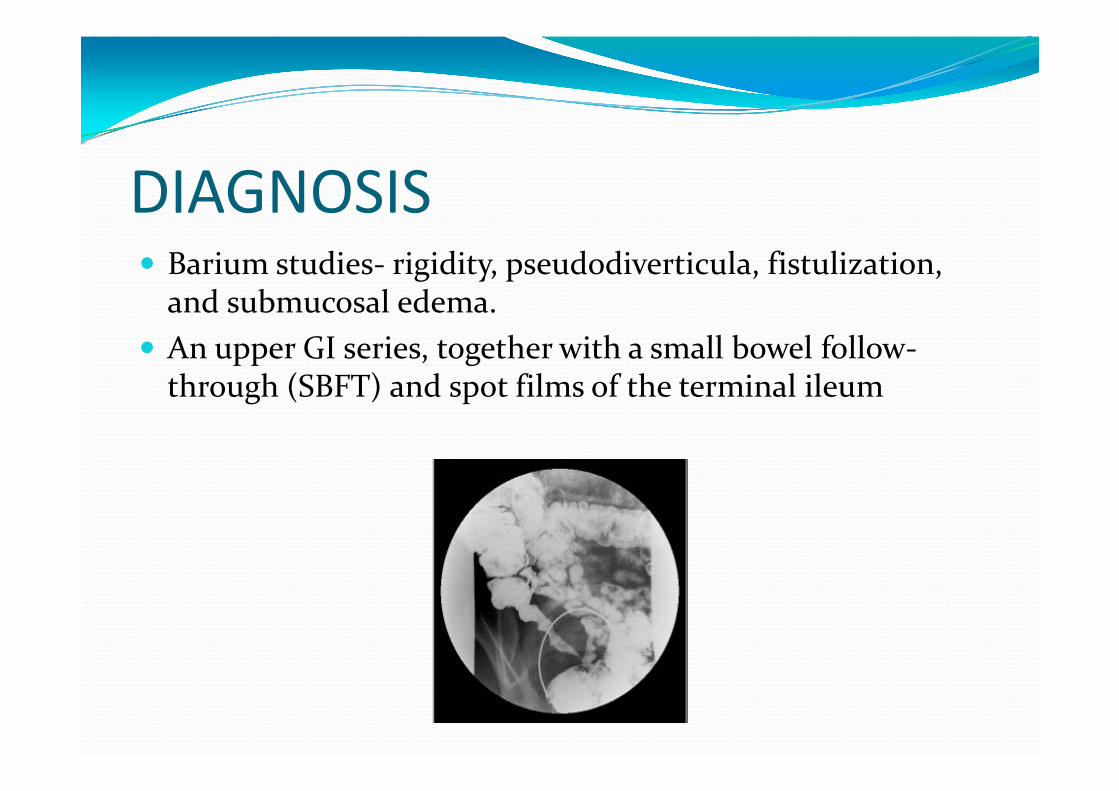
� Barium studies- rigidity, pseudodiverticula, fistulization, and submucosal edema.
� An upper GI series, together with a small bowel follow-through (SBFT) and spot films of the terminal ileum
DIAGNOSIS� CT is helpful in the assessment of extramural complications, as well as
hepatobiliary and renal complications.
� It may show bowel wall thickening, mesenteric edema, abscesses, or fistulae.
� MRI has been shown to yield a higher sensitivity and specificity than ileocolonoscopy (criterion standard) for both the diagnosis of Crohndisease and the determination of severity.
� MRI is especially useful in the evaluation of pelvic and perianal disease when investigating for evidence of perianal disease
� MRI can be superior to CT in demonstrating pelvic lesions. Because of differential water content, MRI can differentiate active inflammation from fibrosis, and can distinguish between inflammatory and (fixed) fibrostenotic lesions in Crohn disease.
DIAGNOSIS
� MR Enterography (MRE) and CT enterography (CTE) are being used increasingly for evaluation of the small bowel.
� Both of these modalities are as sensitive and specific as SBFT for detecting small bowel inflammation and may be more accurate for detecting extraentericcomplications, including fistulae and abscesses.
� MRE is a particularly attractive option because of the lack of radiation exposure.
DIAGNOSIS
� Ultrasonography is a quick and inexpensive screening method to aid in the diagnosis of IBD or in repeated evaluation of patients for complications.
� Abdominal ultrasonography can be used to rule out gallbladder and kidney stones.
� This modality can also detect enlarged lymph nodes, abscesses, stenoses, and fistulae.
� This technique allows the differentiation of simple from complex fistulae, as well as the assessment of the tracts of the fistulae in relation to the sphincter muscle.
DIAGNOSIS� Radionucleotide scanning may be helpful in assessing the
severity and extent of the disease in patients who are too ill to undergo colonoscopy or barium studies.
� Leukocytes labeled with either technetium-99m (99m Tc )-HMPAO or indium-111 (111 In) can be used to assess for active bowel inflammation
� Compared with the111 In label, the99m Tc HMPAO label has better imaging characteristics and can be imaged much sooner after injection.
� However, imaging must typically be performed within an hour after injection of99m Tc-HMPAO-labeled leukocytes, as there is normal excretion into the bowel after this time, unlike111 In-labeled leukocytes, which have no normal bowel excretion.
DIAGNOSIS
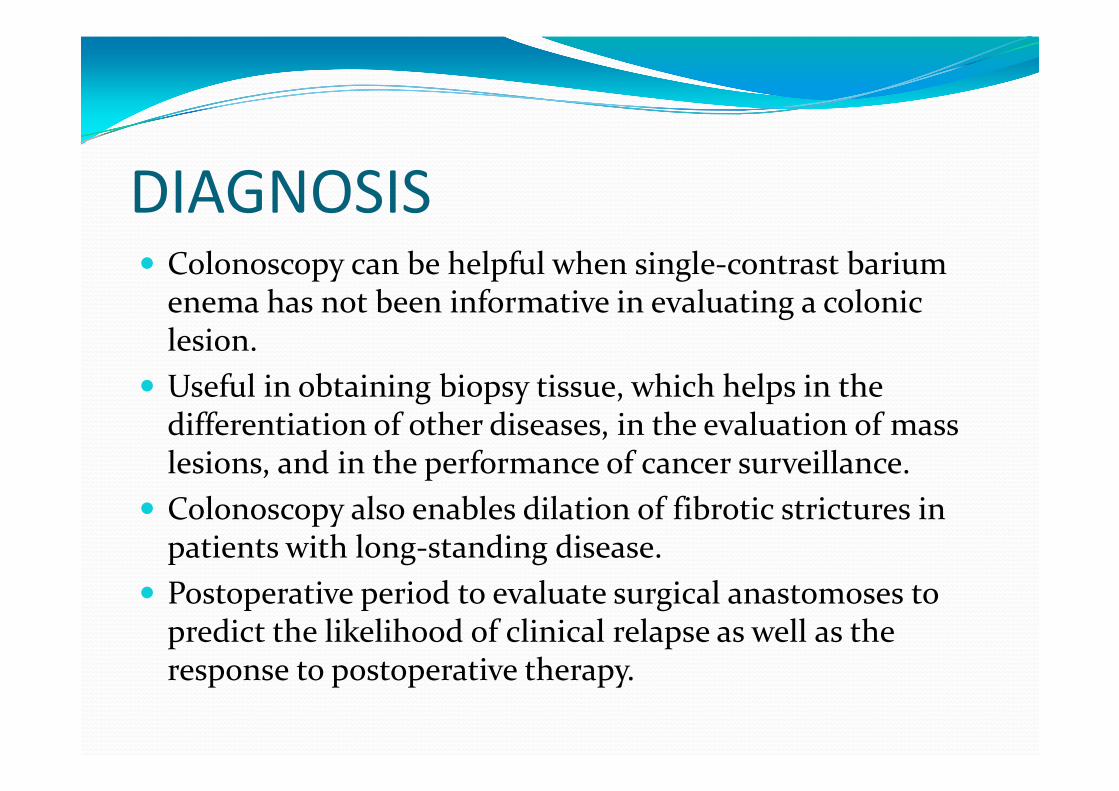
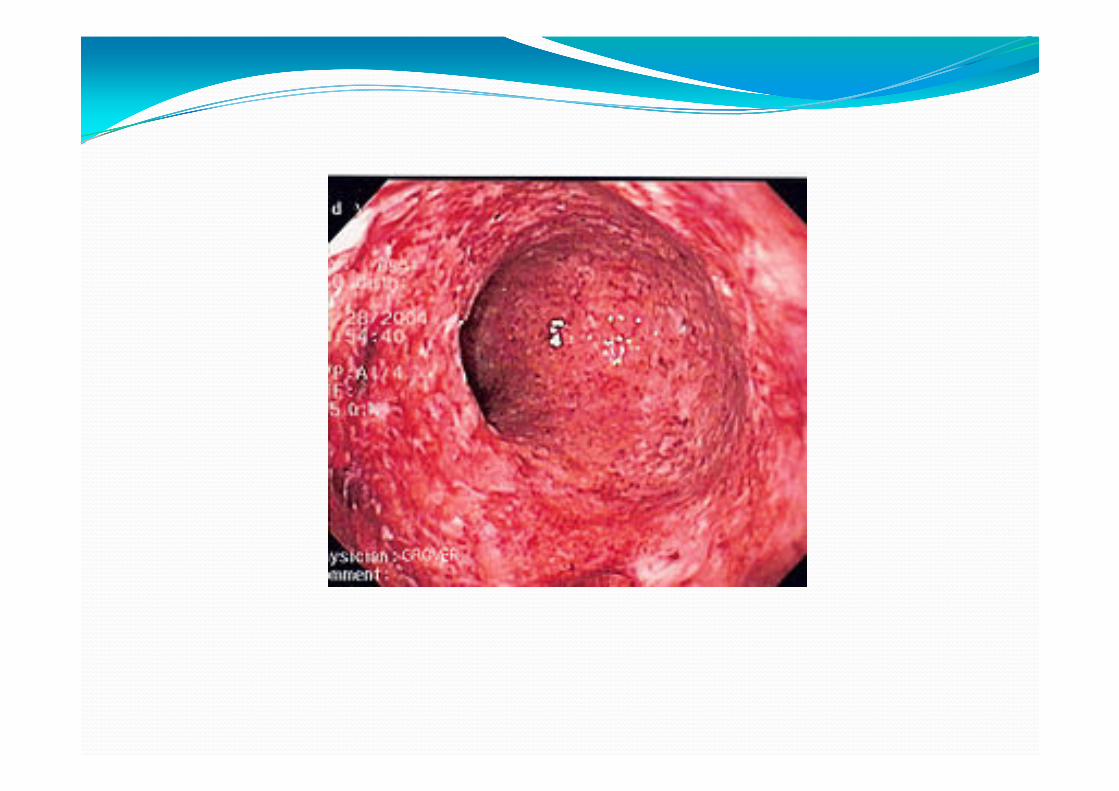
� Colonoscopy can be helpful when single-contrast barium enema has not been informative in evaluating a colonic lesion.
� Useful in obtaining biopsy tissue, which helps in the differentiation of other diseases, in the evaluation of mass lesions, and in the performance of cancer surveillance.
� Colonoscopy also enables dilation of fibrotic strictures in patients with long-standing disease.
� Postoperative period to evaluate surgical anastomoses to predict the likelihood of clinical relapse as well as the response to postoperative therapy.

DIAGNOSIS
� Upper GI endoscopy with biopsy is helpful in differentiating Crohn disease from peptic ulcer disease in patients with upper GI tract symptoms.
� Endoscopic retrograde cholangiopancreatography(ERCP) is helpful both as a diagnostic procedure and a therapeutic tool in patients with sclerosing cholangitis and stricture formation.
� Endoscopic ultrasonography (EUS) and magnetic resonance cholangiopancreatography (MRCP) may provide equally valuable information without invasive complications.

DIAGNOSIS
� Escherichia coli anti-ompC (outer membrane porin C) can be found in greater than 50% of Crohn disease cases, and in only a small percentage of ulcerative colitis cases.
� Pseudomonas fluorescens (anti-12) may be found in greater than 50% of Crohn disease cases and in only 10% of ulcerative colitis cases.
� Flagellin like antigen (anti-Cbir1) is associated independently with small bowel, intestinal penetrating, and fibrostenosing disease.
� These tests further increase sensitivity and diagnostic value.
MANAGEMENT� Chronic diarrhea in Crohn disease responds well to antidiarrheal
agents such as loperamide (2-4 mg), diphenoxylate with atropine (1 tab), and tincture of opium (8-15 gtt). Such agents may be administered up to 4 times daily, but they should not be given to patients with active colitis because of the risk of developing toxic megacolon.
� Patients with terminal ileal disease may not absorb bile acids normally, which can lead to secretory diarrhea in the colon. These patients may benefit from bile acid sequestrants (eg, cholestyramine [2-4 g], colestipol [5 g] bid/tid ac).
� Abdominal cramps may be reduced with hyoscyamine (0.125 mg). These drugs should not be used if there is the possibility of a bowel obstruction.
MANAGEMENT OF INFLAMMATION� Anti-inflammatory drugs or antibiotics are helpful. � Sulfasalazine does not alleviate small bowel disease. � Mesalamine (Asacol, Rowasa, Canasa) that release 5-ASA in the distal
small bowel secondary to pH changes more useful in patients with small intestinal Crohn disease.
� Antituberculosis therapy, macrolides, fluoroquinolones, 5-nitroimidazoles, and rifaximin (alone or in combination) have been shown to induce remission in active Crohn disease and ulcerative colitis. Further trials of antibiotic therapy are necessary in order to determine the best course of single or combination antibiotic therapy.
� Long-term maintenance with mesalamine (800 mg tid) may delay clinical relapse. Prednisone (Deltasone, Orasone) (40-60 mg/d) is generally helpful in acute inflammation.

MANAGEMENT OF INFLAMMATION
� Steroids are not indicated for maintenance therapy because of serious complications, such as aseptic necrosis of the hip, osteoporosis, cataract, diabetes, and hypertension.
� Accordingly, once remission is achieved, the agent is slowly tapered (5-10 mg q1-2wk).
� If steroid withdrawal proves difficult, immunosuppressantssuch as azathioprine (Imuran) (2 mg/kg/d) or its active metabolite, 6-MP, may be considered. Response is usually observed within 3-6 months.
� Mycophenolate mofetil (CellCept) 500 mg twice a day in 2 divided doses is well tolerated by patients and can be used to reduce the steroid dose.
MANAGEMENT OF FISTULAE
� Fistulae between bowel loops (eg, ileoileal, ileocecal, ileosigmoid) are usually benign and may not produce any major problems.
� Medical management is used to treat underlying infections and symptoms with oral metronidazole (Flagyl, 1 g/d) for at least 1-2 months.
� Infliximab is effective in patients who have refractory perianal and enterocutaneous fistulae.
� Current clinical practice is to use it as an intravenous (IV) infusion of 5 mg/kg at 0 weeks, 2 weeks, and 6 weeks, followed by maintenance IV infusions every 8 weeks. On average, the effect lasts for 12 weeks.
SURGERY
INDICATIONS
� Persistent symptoms despite high-dose corticosteroids
� Treatment-related complications, including intra-abdominal abscesses
� Medically intractable fistulae
� Fibrotic strictures with obstructive symptoms
� Toxic megacolon
� Intractable haemorrhage
� Perforation
� Cancer
SURGERY
� Crohn disease has no surgical cure.
� Within 20 years of the onset of symptoms, 75-80% of patients with Crohn disease require surgery
� Twenty to 30% of patients experience a recurrence of disease within the first postoperative year.
� Hence, every attempt at conserving the small bowel should be made in the surgical approach to Crohndisease.
� The most common complication of Crohn disease is small bowel obstruction, occurring in 30%-50% of patients
SURGERY
� The most common complication of surgery for Crohndisease is the development of intraperitonealadhesions.
� Patients with Crohn disease undergoing abdominal surgery are also at an increased risk for developing enterocutaneous fistulae as a result of their surgery.







