
©Pathway Health 2013
Disease State Management –
Redesigning and Aligning Your Clinical Department
Louann Lawson, BA, RN, RAC-CT, CIMT
Nurse Consultant/Clinical Reimbursement Lead
Pathway Health
WHCA/WiCAL 65th Annual Fall Convention
October 20, 2016

©Pathway Health 2013
As the health care delivery market continues to reform itself, size and efficiency become important issues for providers. New models
of clinical care delivery are evolving, including disease-specific practice. Post-acute care providers are key in new or
revised clinical models. Join this presentation to gain a further understanding
of the top three disease states that are currently included in the new models of
clinical care.
Description
2

©Pathway Health 2013
• Understand how to set up a system to assist licensed professionals to improve competencies around specific disease states.
• Develop disease state assessment expectations.
• Identify key expectations for disease state management across a provider continuum.
Objectives
3
©Pathway Health 2013
The Whole New World for PAC
©Pathway Health 2013
“If you don’t pay attention
to this issue*, you may be
closed in 5 years”
Joe Ouslander, Health Policy &
Aging Fellowship ‘Elevator
Speech’
October 2012
* Re-Hospitalization
Re-Hospitalization
5

©Pathway Health 2013
Percentage of Short-Stay Residents who were Re-hospitalized after a
Nursing Home Admission
Percentage of Short-Stay Residents who have had an Outpatient Emergency
Department Visit
Percentage of Short-Stay Residents who were Successfully Discharged to
the Community
NEW Quality Measures
6

©Pathway Health 2013
• For the three claims-based measures, facilities are divided into five groups based on the national distribution of the measure.
– The top-performing 10 percent of facilities receive 100 points;
– The poorest performing 20 percent of facilities receive 20 points;
– The middle 70 percent of facilities are divided into three equally sized groups (each including approximately 23.3 percent of nursing homes) and receive 40, 60 or 80 points.
Nursing Home Care QMs Rating
7

©Pathway Health 2013
Star Cut-points for MDS Quality Measure Summary Score (updated July 2016)
QM Rating Point Range July 2016
★ 275 – 669
★★ 670 – 759
★★★ 760 – 829
★★★★ 830 – 904
★★★★★ 905 – 1350
8
The five new QMs will be phased in between July 2016 and January 2017. In July 2016, they will have 50% the weight of the current measures. In January 2017, they will have
the same weight as the current measures.

©Pathway Health 2013
Value Based Purchasing
9
Sh
utt
er S
tock

SNFRM estimates risk-standardized rate of all-cause, unplanned hospital readmissions of Medicare SNF beneficiaries within 30 days of discharge from their prior proximal acute hospitalization
• Hospital readmissions are identified through Medicare claims • Readmissions within 30-day window are counted regardless of
whether the beneficiary is readmitted directly from SNF or had been discharged from SNF
• Risk-adjusted based on patient demographics, principal diagnosis in
prior hospitalization, comorbidities, and other health status variables that affect probability of readmission
• Excludes planned readmissions since these are not indicative of poor
quality • The FY2019 SNFRM will be in use for the first year of the program
Previously Finalized Measure: SNF 30-Day All Cause Readmission Measure
(SNFRM)

Adopts the SNFRM methodology and assesses the risk-standardized rate of unplanned, potentially preventable readmissions (PPRs) for Medicare fee-for-service (FFS) Skilled Nursing Facility (SNF) patients within 30 days of discharge from a prior proximal hospitalization.
• The 30-day risk window for the SNFPPR measure includes PPRs before a beneficiary
is discharged from a SNF (Within-PAC Stay) and PPRs after a beneficiary is
discharged from a SNF. The Within-PAC Stay list of potentially preventable conditions
is applied before SNF discharge, and the Post-Discharge list is applied for the
remainder of the 30 days after SNF discharge, if any.
• Risk-adjusted based on patient demographics, principal diagnosis in prior
hospitalization, comorbidities, and other health status variables that affect probability
of readmission
• Excludes planned readmissions because these are not indicative of poor quality
• Pursuant to statute, we will propose to replace the SNFRM with the SNFPPR in future
rulemaking
Proposed Measure: SNF 30-Day Potentially Preventable Readmission
Measure (SNFPPR)

©Pathway Health 2013
www.cms.gov/Medicare/Quality-Initiatives-
Patient-Assessment-Instruments/Value-
Based-Programs/Other-VBPs/Final-Measure-
Specification.pdf
(732 pages)
SNF Potentially Preventable Readmission

©Pathway Health 2013
Medicare FFS VBP Quality Incentive

©Pathway Health 2013
Medicare Payment Features:
• Performance standards must include both achievement and improvement
• SNF Performance Scores must be ranked from low to high
• 2% of SNFs’ Medicare payments will be withheld to fund incentive payments
• Incentive payments must total 50-70% of amount withheld
• No exclusions in statute for SNFs based on volume
Protecting Access to Medicare Act of 2014

Term Proposed Definition
Achievement Threshold The 25th percentile of national SNF performance on the quality measure during calendar year (CY) 2015
Benchmark The mean of the best decile of national SNF performance on the quality measure during CY 2015
Improvement Threshold The specific SNF’s performance on the specified measure during CY 2015
Performance Period CY 2017
Baseline Period CY 2015
Proposed Performance Definitions for the PY 2019 SNF VBP
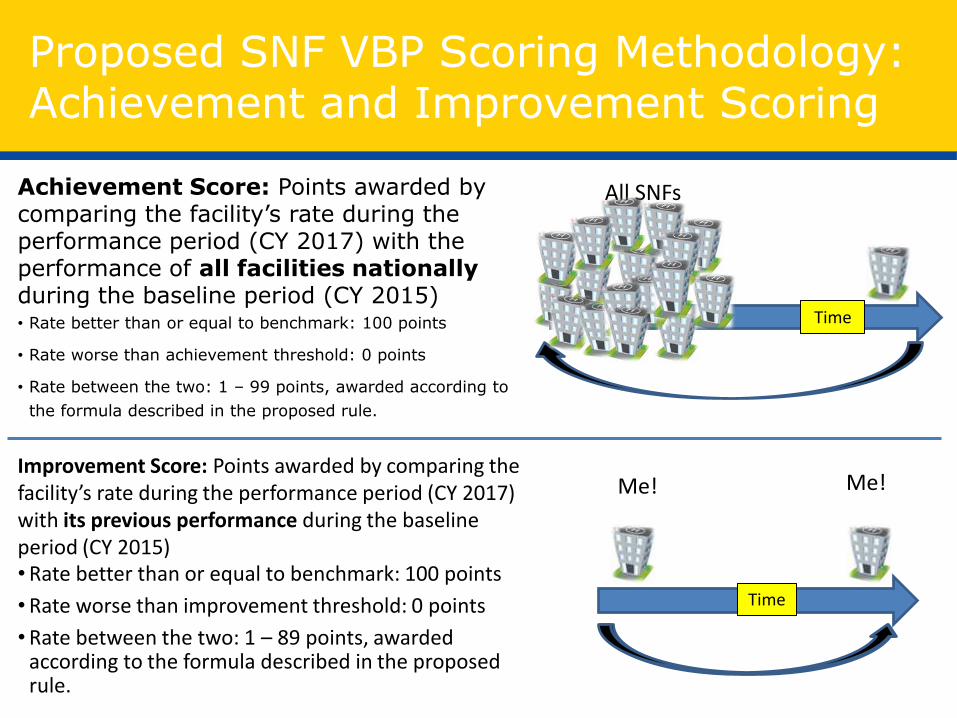
Achievement Score: Points awarded by comparing the facility’s rate during the performance period (CY 2017) with the performance of all facilities nationally during the baseline period (CY 2015) • Rate better than or equal to benchmark: 100 points
• Rate worse than achievement threshold: 0 points
• Rate between the two: 1 – 99 points, awarded according to
the formula described in the proposed rule.
Proposed SNF VBP Scoring Methodology: Achievement and Improvement Scoring
Improvement Score: Points awarded by comparing the facility’s rate during the performance period (CY 2017) with its previous performance during the baseline period (CY 2015) • Rate better than or equal to benchmark: 100 points
• Rate worse than improvement threshold: 0 points
• Rate between the two: 1 – 89 points, awarded according to the formula described in the proposed rule.
Time
Me! Me!
Time
All SNFs

©Pathway Health 2013
Medicare Payment Risks
ONLY FOR TRADITIONAL MEDICARE PART A STAYS

©Pathway Health 2013
• Increased discharge planning responsibilities
• Baseline care plan required within 48 hours of admission
• Trauma informed care
• Sufficient nursing staff with the appropriate competencies and skills sets to provide nursing and related services .. As determined by resident assessments and individual plans of care
• Competency and skill set verification of nurses
NEW State Operations Manual
18

©Pathway Health 2013
Nursing Home Quality of Care Collaborative Change Package
• Lead with a sense of purpose
• Recruit and retain quality staff
• Connect with residents in the celebration of life
• Nourish team work and communication
• Be a continuous learning environment
• Provide exceptional and compassionate clinical care that treats the whole person
• Construct solid business practices that support your mission statement
19

©Pathway Health 2013
Strategies for Success
Assess Readiness
Capabilities and
Competencies
Partner and Collaboration
Technology

©Pathway Health 2013
Assess Readiness
21

©Pathway Health 2013
• Measuring Readiness
– Systemic analysis of organization
– Ability to take on transformational process or change
• QI Readiness
Clinical Readiness
22 http://www.hrsa.gov/quality/toolbox/508pdfs/readinessassessment.pdf

©Pathway Health 2013
Clinical Readiness
Assess Clinical Readiness
– Your Role
– Industry initiatives
– Market initiatives and expectations
– Quality Outcomes
• Payer and External Expectations
• Consequences
– Internal competency process
– Right People and Right Roles
23

©Pathway Health 2013
Capabilities and Competencies
24

©Pathway Health 2013
• Are we confident in our preadmission process?
• Is our admission assessment and management process solid?
• Do our nurses have excellent head-to-toe assessment skills?
• Do our nurses understand disease processes?
• Do our nurses understand pharmacology related to disease processes and management?
• What is our process for comprehensive discharge care planning upon admission?
• What systems do we have in place to ensure good assessment, communication and follow through for early identification of changes in condition?
A Few Questions…….
25
©Pathway Health 2013
• Assess current status
• Determine targeted population
• Develop capabilities list
• Utilize best practice standard tools for listing, communication strategy
• Medical Director, physicians, and extenders – input and agreement
• Internal and External Communication
• Monitor via QAPI
Clinical Capabilities
26

©Pathway Health 2013
Clinical Competence
• Assess Clinical Competencies
– Process competencies; e.g., admission, discharge
– Technology competencies; e.g., equipment, EHR
– Disease state competencies
• Right Individual in the Right Role
• Engage Vendors
– Lab , Radiology, Tele-health, Diagnostic, Pharmacy

©Pathway Health 2013
• Admission Assessment (Baseline):
• Vitals, Weight, Height
• Allergies
• Diagnoses
• Body Audit/Skin Condition
• Neurological Evaluation
• Cardiovascular/Respiratory
• Musculoskeletal
• Gastrointestinal/Genitourinary
• Oral/Dental
• Communication, Vision, Hearing
• Sleep Patterns/Pain
• Fall Risk, Devices
• Mood/Behavior
Capabilities & Competencies
28

©Pathway Health 2013
• Medical Record
– H&P
– Diagnosis List
– Physician Orders
– Lab or Diagnostic Testing
– Consultation Reports
– Medication and Treatment List
– Therapy Notes
– Wound Care Notes (if applicable)
– Dietary Reports
– Discharge Summary
Capabilities & Competencies
29

©Pathway Health 2013
• Care Assessment and Management Skills
– Pain interview, assessment, and management needs
– S/S or identified infection
– B&B information (LBM, voiding status, etc.)
– Vitals (Normal? Unstable?)
– Weight and weight history
– Special procedures (IV’s, TPN, resp. care, etc.)
– Abnormal (or pending)labs
– Mood and Behavior concerns
– Fall risk
– Device use
– Psychotropic drug use
– **Medication Reconciliation
Capabilities & Competencies
30

©Pathway Health 2013
• Care Planning
– Initial
• Safety, Skin, ADLs, Reason for skilled stay, Discharge status
– Comprehensive
• Chronic Disease Management, CAAs
– Acute
• Infections, Falls, Injuries, etc.
Capabilities & Competencies
31
©Pathway Health 2013
• Strategies for Competency:
– Education
– Post-Test
– Competency Skills Checklist:
• Heart Sounds
• Lung Sounds
• Vital Signs
– Temperature
– Pulse
– Respirations
– Blood Pressure
– Oxygen Saturation
Capabilities & Competencies
32

33
Knows
(Knowledge)
Knows How
(Competence)
Shows How
(Performance)
Does
(Action)
Framework for Clinical Assessment
(G. Miller, MD)
©Pathway Health 2013
Clinical Capacity
• Assess Clinical Capacity
– Safely manage acute conditions
– Disease state programs
– Episodic Management
– Rapid turnaround for admissions
– All hours
• Engage Medical Director and Physicians
– Specialists
– Extenders
Sh
utt
er S
tock

©Pathway Health 2013
Clinical Capacity
• Partnership and Collaboration
– Acute care – clinical strategies
– Diagnostics
– Telemedicine
– Performance Reviews
• Determine benchmarks
– Internal
– External entities

©Pathway Health 2013
Partner and Collaboration
36

©Pathway Health 2013
• Clinical integration readiness assessment
– Are you ready to plug into acute care/physician networks and payer payment models?
– Have you met with partner leaders to review clinical paths, expectations, performance metrics and monitoring processes?
– Are you the provider of choice in marketplace?
– Do you have development, training, tracking of clinical standards and benchmarks in place?
– Do you have a data management strategy and operational processes for monitoring performance?
– Is entire organization prepped and versed on QAPI?
Clinical Integration and Partners
37

©Pathway Health 2013
• Transition/Discharge Planning and Admission Process
• Comprehensive Communication
• Coordination of Care
• Resident/Family Teaching with evidence of understanding
• Medication Education and Reconciliation
• Shared Accountability
• Resource-AMDA Clinical Practice Guideline: Transitions of Care in the Long-Term Care Continuum https://www.amda.com/members/flashpapers/papers/TOC/
Care Transition Process
38
39

©Pathway Health 2013
Technology
40

©Pathway Health 2013
Technology
41
• Electronic Health Records – Next Step
• Data Analytics/Predictive Analytics
• Diagnostics and Clinical Integration
• Tele Health/Tele Medicine – At the Bedside
• Store and forward
• Remote monitoring
• Interactive services
• Teleconsultation
• Emergency Care
• Specialists

©Pathway Health 2013
Technology
42
• Patient Portals – SNF, HHA and ALF
• Wearables – Fitbit technology, vitals
• Interoperability
• IoT – devices (LG, HP and others)
– “Internet of Things” or “smart devices”
• Public Data - Data Transparency

©Pathway Health 2013
Disease State Management: CHF, Pneumonia, Acute MI
43

©Pathway Health 2013
• The New York Heart Association functional classification.
• Class I: no limitation is experienced in any activities; there are no symptoms from ordinary activities.
• Class II: slight, mild limitation of activity; the individual is comfortable at rest or with mild exertion.
• Class III: marked limitation of any activity; the Individual is comfortable only at rest.
• Class IV: any physical activity brings on discomfort and symptoms occur at rest.
• American College of Cardiology/American Heart Association.
• Stage A: Individuals at high risk for developing HF in the future but no functional or structural heart disorder.
• Stage B: a structural heart disorder but no symptoms at any stage.
• Stage C: previous or current symptoms of heart failure in the context of an underlying structural heart problem, but managed with medical treatment.
• Stage D: advanced disease requiring hospital-based support, a heart transplant or palliative care.
CHF Classification
44

©Pathway Health 2013
• Failure of the left ventricle causes congestion of the pulmonary vasculature, and so the symptoms are predominantly respiratory in nature. Backward failure can be subdivided into failure of the left atrium, the left ventricle or both within the left circuit. Symptoms include:
• Dyspnea upon exertion and in severe cases, dyspnea at rest.
• Orthopnea, often measured in the number of pillows required to lie comfortably, and in severe cases, the individual may resort to sleeping while sitting up.
• Paroxysmal nocturnal dyspnea - a sudden nighttime attack of severe breathlessness, usually several hours after going to sleep. Becoming fatigued easily and exercise intolerance are also common complaints related to respiratory compromise.
• Wheezing may occur.
• Symptoms of poor systemic circulation such as dizziness, confusion and cool extremities at rest.
Left-Sided Failure
45

©Pathway Health 2013
• Failure of the right ventricle leads to congestion of systemic capillaries generating excess fluid accumulation in the body. Symptoms include: Peripheral edema usually affecting the dependent parts of the body first with noted foot and ankle swelling in people who are standing up, and sacral edema in people who are predominantly lying down. Jugular Venous Distention with advancing symptoms.
• Nocturia may occur when fluid from the legs is returned to the bloodstream while lying down at night.
• In progressively severe cases, ascites and hepatomegaly may develop causing abdominal distension.
• Significant liver congestion may result in impaired liver function, and jaundice and even coagulopathy.
• Chronic lower extremity edema may lead to stasis disease, weeping edema and ulceration.
Right-Sided Failure
46

©Pathway Health 2013
• Unrelieved shortness of breath or new shortness of breath at rest
• Unrelieved or new chest pain
• Increased or new anxiety
• Increased or new complaint of fatigue
• Increased or new adventitious lung sounds
• Wheezing or complaint of chest tightness at rest
• Increased or new orthopnea
• Mental status changes – increased confusion or dullness
• Complaint of dizziness with standing
• Increased or new peripheral edema
• Increased or new Sacral edema
• Increased or new jugular venous distension
• Significant weight gain ( 3lbs in one day or >5 lbs in one week)
• Change in vital signs ( Temp > 100°F or 2°F over baseline, AHR > 100 or < 50, Resp > 20, SBP < 90 , or as per MD ordered parameters)
• Decreased O2 saturation (<90% or per MD parameters)
• Environmental factors which exacerbate symptoms
Nursing Assessment/Symptoms of CHF
47

©Pathway Health 2013
• BUN / Creatinine – Elevated due to decreased perfusion of the kidneys & diuretic use or low with fluid overload
• Hgb / Hct – Elevated with dehydration or low with fluid overload
• Glucose – may be elevated with stress, diabetes
• Chloride - Low value may indicate increasing or new CHF
• Potassium
– Low value may be due to non-potassium sparing diuretics & certain cardiac drugs
– High value may be due to potassium sparing diuretics & certain cardiac drugsNursing Interventions for CHF
• Sodium
– Low value may indicate fluid overload and dilutional hyponatremia
– Side effect of ACE Inhibitors
– High value may indicate dehydration due to diuretics
• BNP - B-type Natriuretic Peptide
BNP is a substance secreted from the ventricles or lower chambers of the heart in response to changes in pressure that occur when heart failure develops and worsens.
– BNP < 100 pg/mL indicates no heart failure
– BNP < 100-300 pg/ml suggests heart failure is present
– BNP >300 pg/mL indicates mild heart failure
– BNP > 600 pg/mL indicates moderate heart failure.
– BNP > 900 pg/mL indicates severe heart failure.
Significant Lab Values with CHF
48
©Pathway Health 2013
• Complete a full head to toe assessment including oral assessment
• Complete full vital signs & compare to baseline
• Perform blood glucose check if diabetic
• Obtain weight & compare to baseline and trend over the past two weeks if available
• Check medications to identify omissions of cardiac or diuretic medications
• Obtain information about food and fluid intake to identify high sodium intake, fluid consumption or possible dehydration
• Refer to Dietician
• Notify physician of findings
• Implement new orders (draw labs, order x-rays, adjust medications)
• Educate resident on reportable symptoms
Nursing Interventions for CHF
49

©Pathway Health 2013
• Vital signs monitoring, recording, and reporting – watch for changes from baseline
• Daily weight monitoring, recording and reporting weight gain ( 3lbs in one day or >5 lbs in one week)
• Edema management including elevation, compression, measuring abdomen
• Dietary instructions based on physician’s ordered diet including reading labels and portions
• Respiratory symptoms including O2 saturation and when to report changes
• Energy conservation – alternation of activity and rest
• Instruct on exercise program / restrictions per orders
• Oxygen administration and safety as indicated
• Identify environmental factors needing modification (air conditioning, smoking, assistive devices) and provide information on available community resources
• Medication management:
– Medications they take and why
– Administration schedule (including what to do if a dose is missed)
– Adverse side effects (what is common & what to report)
– Special instructions including pharmacy information, and how to access financial assistance if needed.
Resident/Caregiver Education: CHF
50

©Pathway Health 2013
• Pneumonia is an inflammatory condition of the lung—especially affecting the microscopic air sacs (alveoli)—associated with fever, chest symptoms, and a lack of air space (consolidation) on a chest X-ray. Pneumonia is typically caused by an infection but there are a number of other causes. Infectious agents include: bacteria, viruses, fungi, and parasites.
• Pneumonia is a particular concern in persons over the age of 65 or who have a chronic illness or a weak immune system. Pneumonia can also occur in young, healthy people.
• Nursing interventions for the individual with Pneumonia will focus primarily on:
– Symptom recognition of post-acute complications
– Medication management
– Oxygen use / management
– Lifestyle modifications to prevent complications & re-occurrence
Pneumonia
51

©Pathway Health 2013
• Most commonly classified by where or how it was acquired
– community-acquired, aspiration, healthcare-associated, hospital-acquired, and ventilator-associated pneumonia
• Pneumonia may also be classified by the area of lung affected
• lobar pneumonia, bronchial pneumonia and acute interstitial pneumonia
• Pneumonia may be classified by the causative organism
• Pneumonia in children may additionally be classified based on signs and symptoms as non-severe, severe, or very severe
•
Pneumonia Classification
52

©Pathway Health 2013
RED ALERT: Potential for Sepsis
• Sepsis refers to the systemic inflammatory response to infection (sepsis). It may present with symptoms such as fever, hypotension, reduced urine output, or acute change in mental status.
• Fever above 100° F or temperature below 96.8°F, Heart rate higher than 90 beats/minute, Respiratory rate greater than or equal to 25 breaths/minute.
Pneumonia Can Lead to Sepsis
53

©Pathway Health 2013
• Presents with labored breathing or increased shortness of breath beyond baseline
• Reports or presents with new or worsening cough
• Presents with change in baseline mental status (confusion, irritability, dullness)
• Reports or presents with an increased amount or change in color or consistency of sputum
• Presents with s/s of hypoxia:
– Presents with circum-oral (around the mouth) or nail bed cyanosis
– Oxygen Saturation < 94%, >3% from baseline or below MD parameters
– Reports or presents with increased anxiety
• Reports or presents with muscle pain secondary to coughing & respiratory effort
• Reports or presents with decrease in appetite
• Significant weight gain or loss since last visit ( 3 pounds in one day or >5 pounds in one week)
• Respiratory Assessment reveals new or worsened adventitious lung sounds:
– Rales , rhonchi, rubs, wheeze or stridor present upon inspiration or expiration with auscultation.
• Presents with new or worsening edema, abdominal distention, or jugular venous distention
– (S/SX of Congestive Heart Failure – CHF a potential complication due to pulmonary hypertension)
Assessment/Symptoms: Pneumonia
54

©Pathway Health 2013
• HCT – may be elevated due to hypoxia or dehydration
• HGB – may be elevated due to hypoxia or dehydration
• RBC – may be elevated due to hypoxia or dehydration
• ESR (sedimentation rate) – may be elevated with inflammation or infection
• WBC – may be elevated with stress or infection
• Glucose – may be elevated due to steroid use to treat the pneumonia symptoms or due to infection may be low due to stress and high energy requirements
Lab Values r/t Pneumonia
55

©Pathway Health 2013
• Complete a full head to toe assessment
• Complete vital signs & notify MD if:
– Single oral temp >100°F, repeated oral temps > 99°F or temp 2°F above baseline
– Systolic BP<90 mmHg
– Heart rate >100 beats/min
– Respiratory rate ≥ 25 breaths /min
– Oxygen Saturation < 94%, >3% from baseline or below MD parameters
– Blood glucose <70 or >400mg/dl
• Observe use of incentive spirometer to identify any decline in function
• Monitor oxygen use & check settings to ensure the liter flow is per MD orders.
• Complete a cardiac assessment if presenting with S/S of CHF – listen to heart sounds, check edema, abdominal distention.
• Assess skin turgor, mucous membranes for s/s dehydration
• Check the resident’s medications, including inhalers & nebulizers to identify if any omissions have occurred.
• Notify the physician of any abnormal findings from the nursing assessment.
Nursing Interventions: Pneumonia
56

©Pathway Health 2013
• Implement any new orders:
– Draw labs
– Order X-rays, tests
– Adjust medications
– Administer IV fluids or medications as ordered
– Order equipment if needed (O2, Nebulizer, IV supplies)
– Educate resident/ caregiver on plan of care changes
• Have the client return demonstrate or verbalize the use of metered dose inhalers and nebulizers to ensure they are able to self-administer correctly as appropriate
• Instruct resident in use of oxygen if ordered (settings, safety)
• Instruct resident / caregiver on all medications (what, why, schedule for administration, routine & reportable side effects, prn parameters)
• Instruct resident on diet and exercise programs as ordered
• Instruct the resident on energy conservation
• Provide smoking cessation support / resources if indicated
Nursing Interventions: Pneumonia
57

©Pathway Health 2013
• A myocardial infarction, also called heart attack, usually occurs when a blood clot blocks the flow of blood through a coronary artery — a blood vessel that feeds blood to a part of the heart muscle. A coronary attack (heart attack) occurs when the blood flow that brings oxygen to the heart muscle is severely reduced or cut off completely. Interrupted blood flow to the heart can damage or destroy a part of the heart muscle.
• Post-acute management of the individual will focus on:
– Individual symptom identification via cardiac assessment
– Medication management
– Education
– Lifestyle adjustment
– Exercise / Activity modification
– Post-surgical care as indicated
Management of Post-Acute MI
58

©Pathway Health 2013
• Type 1 – Spontaneous myocardial infarction related to ischemia due to a primary coronary event such as plaque erosion and/or rupture, fissuring, or dissection
• Type 2 – Myocardial infarction secondary to ischemia due to either increased oxygen demand or decreased supply, e.g. coronary artery spasm, coronary embolism, anemia, arrhythmias, hypertension, or hypotension
• Type 3 – Sudden unexpected cardiac death, including cardiac arrest, often with symptoms suggestive of myocardial ischemia, accompanied by new ST elevation, or new LBBB, or evidence of fresh thrombus in a coronary artery by angiography and/or at autopsy, but death occurring before blood samples could be obtained, or at a time before the appearance of cardiac biomarkers in the blood
• Type 4 – Associated with coronary angioplasty or stents:
– Type 4a – Myocardial infarction associated with PCI
– Type 4b – Myocardial infarction associated with stent thrombosis as documented by angiography or at autopsy
• Type 5 – Myocardial infarction associated with CABG
MI Classifications
59

©Pathway Health 2013
• Cardiac Status Evaluation
– Change in baseline heart rate or rhythm
– Change in lung sounds
– New symptom presentation of edema, fatigue, mental status, any vital signs changes
– Significant weight change ( 3 lbs in one day or >5 lbs in one week) or as directed through physician specific parameters for the individual
• Pain Management – Chest Pain & surgical site if applicable
– Angina or tightness with increased severity or frequency
– Chest pain not relieved by rest or medication
– Surgical incision complication of pain
• Oxygen Use (if applicable)
– Safety concerns with smoking
– Tripping hazards
– Incorrect liter flow
• Lifestyle Modifications
– Smoking
– Alcohol or drug use
– Failure to follow recommended diet & exercise program
• Signs & Symptoms of Infection
– Surgical site with change in appearance or drainage
– Lung sounds changes
Nursing Assessment/Symptoms
60

©Pathway Health 2013
• Signs & Symptoms of Depression / Anxiety
– Expression of thoughts which may indicate potential for severe depression or suicidal ideation
– Poor concentration with education / unrealistic fear
• Knowledge deficit related to medications
• Knowledge deficit related to exercise program
• Knowledge deficit related to dietary requirements
• Knowledge deficit related to lab values & tests
Nursing Assessment/Symptoms
61

©Pathway Health 2013
• Complete a full head to toe assessment including an oral assessment
• Complete vital signs including apical & radial pulse, O2 sats & weight – compare to baseline
• Notify the physician/extender of vital signs that are outside of any parameters that may have been established per the physician/extender
• Question the resident about any new symptoms identified
• Evaluate signs & symptoms of chest pain including
– Onset
– Duration
– Location
– Quality
– Relief with rest or medications? Both?
• Evaluate surgical incision(s), change dressings, obtain swab culture as indicated
• Evaluate medication use to identify any omissions or inappropriate use
Nursing Interventions
62

©Pathway Health 2013
• Explore / question resident about feelings of depression / anxiety – make mental health referral or notify physician for immediate evaluation
• Notify the physician of any findings which suggest worsening or uncontrolled cardiac symptoms or infection
• Implement physician’s orders (draw labs, order tests, adjust medications)
• Educate on reportable symptoms
Nursing Interventions
63

©Pathway Health 2013
• Vital signs monitoring, recording, and reporting
• Daily weight monitoring, recording and reporting
• Edema management if applicable
• Dietary instructions based on physician’s ordered diet including reading labels and portions
• Exercise regimen / cardiac rehab program
• Respiratory symptoms including O2 saturation and when to report changes
• Energy conservation – alternation of activity and rest
• Oxygen administration and safety as indicated
• Medication management:
– What medications they take and why
– Administration of nitrogycerin
– Anticoagulation therapy – self administration
– Required lab tests (PT/INR, PTT as indicated)
– Administration schedule (including what to do if a dose is missed)
– Adverse side effects (what is common & what to report)
– Special instructions including pharmacy information, and how to access financial assistance if needed.
– Mental health resources available including support groups
Resident/Caregiver Education
64

©Pathway Health 2013
• Provide instruction / support with cessation of smoking
• Provide instruction on Oxygen use
• Provide instruction on reportable symptoms of MI:
– Pressure, a feeling of fullness or a squeezing pain in the center of your chest that lasts for more than a few minutes
– Pain extending beyond your chest to your shoulder, arm, back, or even to your teeth and jaw
– Increasing episodes of chest pain
– Prolonged pain in the upper abdomen
– Shortness of breath
– Sweating or cold sweat
– Impending sense of doom
– Fainting
– Nausea and vomiting
• Particular symptoms for women
– Heartburn or abdominal pain
– Clammy skin
– Lightheadedness or dizziness
– Unusual or unexplained fatigue
Resident/Caregiver Education
65

©Pathway Health 2013 66
Final Thoughts

©Pathway Health 2013
1. Prepare a “Needs Assessment” of our Clinical Team!
a. Communication System for Changes of Condition
b. Assessment Skills of the Nurses
c. Knowledge of Disease States
d. Pharmacology knowledge for nurses
e. Comprehensive, person-centered care planning
f. Communication
g. Documentation
67

©Pathway Health 2013
2. Engage Key Players:
a. Medical Director
b. Practitioners
c. Acute Care Partners
d. Pharmacy Consultant
e. Lab/Radiology
f. Home Care, Assisted Living, Hospice entities
68

©Pathway Health 2013
3. Develop Your System
a. Policies and Procedures
b. EHR/Forms Management
c. Assessment Process
d. Care Plan Process (Including
Discharge Care Planning)
c. Communication Process
d. Staff Education
e. Practitioner Education
f. Resident/Family Education
g. Evaluation and Follow-up 69

©Pathway Health 2013
Communication System for Acute Changes in Condition:
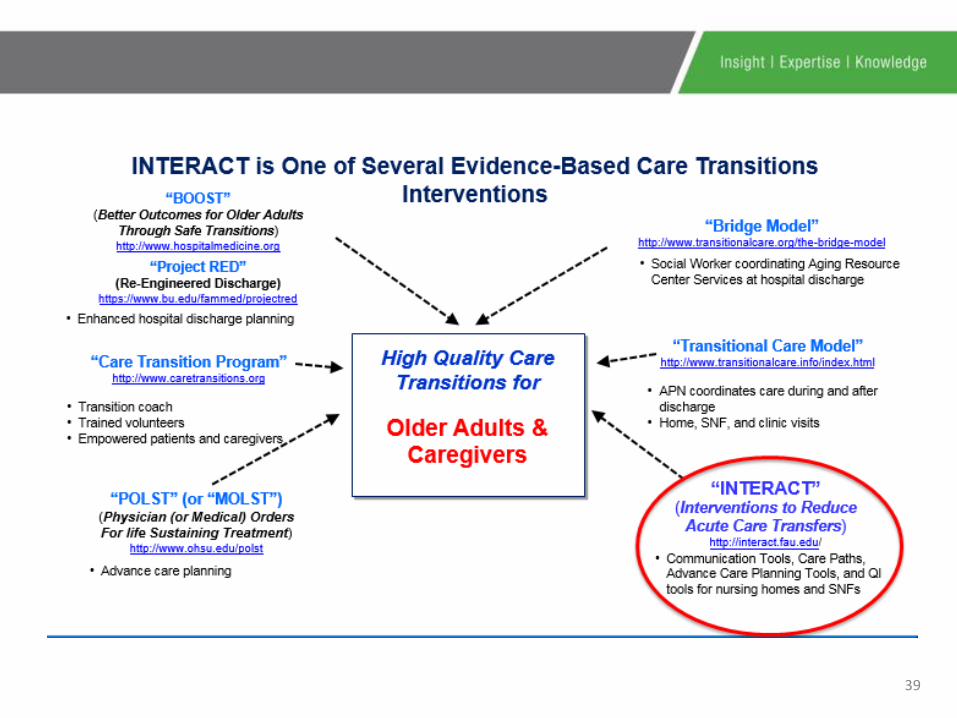
• INTERACT™ 4.0 Quality Improvement Program
What System are YOU using?
70
http://interact.fau.edu/

©Pathway Health 2013
Action Plan
AREA OF CONCERN RECOMMENDATIONS GOAL DATE RESPONSIBLE PERSON
Lung Assessment not completed with resident s/s “productive cough”(Pneumonia dx)
1. Nurse re-educated in assessment process with return demonstration of lung assessment.
2. Nurse re-education in documentation requirements.
3. Follow up review of assessment and documentation each shift
8/1/16 8/1/16 Beginning 8/15/16
DON or Nurse Manager DON or Nurse Manager DON or Nurse Manager

©Pathway Health 2013
QAPI Action Plan
72

©Pathway Health 2013
• CMS:
– https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-04-21-2.html
– https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/Other-VBPs/SNF-VBP.html
References and Resources
73
©Pathway Health 2013
• CMS Innovation Center:
– https://innovation.cms.gov/
• Protecting Access to Medicare Act of 2014:
– https://www.congress.gov/113/plaws/publ93/PLAW-113publ93.pdf
References and Resources
74

©Pathway Health 2013
• AMDA: The Society For Post-Acute and Long-Term Care Medicine. Transitions of Care-Clinical Practice Guideline:
– http://www.paltc.org/product-store/transitions-care-cpg
• National Quality Strategy:
– http://www.ahrq.gov/workingforquality/
References and Resources
75

©Pathway Health 2013
• http://www.mayoclinic.com/health/heart-failure/DS00061 http://www.heart.org/HEARTORG/Conditions/HeartFailure/Heart-Failure_UCM_002019_SubHomePage.jsp
• my.clevelandclinic.org/heart/services/tests/labtests/bnp.aspx
References and Resources
76

©Pathway Health 2013
• www.ncbi.nlm.nih.gov
• www.lung.org/lung-disease/pneumonia
• www.clevelandclinicmeded.com/.../diseasemanagement
• Stone, Nimalie D., et al, Infection Control and Hospital Epidemiology, “Surveillance Definitions of Infections in Long-Term Care Facilities: Revisiting the McGeer Criteria”, Vol. 33, No. 10 (October 2012), pp. 965-977
References and Resources
77

©Pathway Health 2013
• www.nurse-ocha.com/2007/06/nursing-care-plan-for-mci
• www.escardio.org/guidelines.../guidelines-universal-MI-slides.pdf
References and Resources
78

©Pathway Health 2013
Disease State Management –
Redesigning and Aligning Your Clinical Department
Louann Lawson, BA, RN, RAC-CT, CIMT
Nurse Consultant/Clinical Reimbursement Lead







