


different
• The human dentition : upper and lower arches
• Heterodont: Different teeth to perform
functions
• Two dentitions : primary and permanent.

NUMBER Primary number of teeth: 20 (5 in each quadrant)
Permanent number of teeth: 32 (8 in each
quadrant)

DURATION
Primary teeth -6months to 5 1/2 years
Permanent teeth - 6 years onwards

Chronology of primary teeth -Maxilla
TOOTH 1ST EVIDENCE OF CALCIFICATION (WKS IN UTERO)
ENAMEL COMPLETED
ERUPTION ROOT COMPLETED
MAXILLARY
Central incisor
14(13-16) 1 ½ mo 10(8-12)mo 1 ½ yr
Lateral incisor
16(14 ½-16 ½) 2 ½ mo 11(9-13)mo 2 yr
Cuspid 17(15-18) 9 mo 19(16-22)mo 3 ¼ yr
1st molar 15 ½ (14 ½ -17) 6 mo 16(13-19)mo 2 ½ yr
2nd molar 19(16-231/2 ) 11 mo 29(25-33)mo 3 yr

Chronology of primary teeth-Mandible
TOOTH 1ST EViDENCE OF CALCIFICATION (WKS IN UTERO)
CROWN COMPLETED
ERUPTION ROOT COMPLETED
MANDIBULAR
Central incisor 14(13-16) 2 ½ mo 8(6-10) mo 1 ½ yr
Lateral incisor 16(141/2-) 3 mo 13(10-16) mo 1 ½ yr
Cuspid 17(16-) 9 mo 20(17-23)mo 3 ¼ yr
1st molar 151/2 (141/2 -17) 5 ½ mo 16(14-18)mo 2 ¼ yr
2nd molar 18(17-191/2 ) 10 mo 27(23-31) mo 3 yr

Chronology of permanent teeth
TOOTH HARD TISSUE FORMATION BEGINS
CROWN COMPLETED
ERUPTION ROOT COMPLETED
MAXILLARY
Central incisor 3-4 mo 4-5 yr 7 – 8 yr 10 yr
Lateral incisor 10-12 mo 4-5 yr 8-9 yr 11yr
Cuspid 4 -5 mo 6-7 yr 11-12 yr 13-15 yr
1st premolar 1 ½ -1 ¾ yr 5-6 yr 10-11yr 12-13 yr
2nd premolar 2 – 2 ¼ yr 6-7 yr 10-12 yr 12 -14 yr
1st molar At birth 2 ½ -3 yr 6-7 yr 9-10 yr
2nd molar 2 ½ -3 yr 7-8 yr 12-13 yr 14-16 yr
3rd molar 7-9 yr 12-16 yr 17-21 yr 18 -25 yr

Chronology of permanent teeth
TOOTH HARD TISSUE FORMATION BEGINS
AMOUNT OF ENAMEL AT BIRTH
ENAMEL COMPLETED
ERUPTION ROOT COMPLETED
MANDIBULAR
Central incisor 3 -4 mo 4-5 YR 6-7 yr 9 yr
Lateral incisor 3-4 MO 4-5 YR 7-8 yr 10 yr
Cuspid 4-5 mo 6-7 yr 9-10 yr 12-14 yr
1st premolar 1 ¾ – 2yr Sometime a trace
5-6 yr 10-12 yr 12-13 yr
2nd premolar 2 ¼ - 2 ½ yr 6-7 yr 11-12 yr 13-14yr
1st molar At birth 2 ½ -3 yr 11-12 yr 9 -10 yr
2nd molar 2 ½ -3 yr 7-8 yr 6 -7 yr 14 -15 yr
3rd molar 8 – 10 yr 12-16 yr 11-13 yr 18 – 25 yr

Morphologic difference between
primary and permanent teeth

CROWN

COLOUR • Primary teeth are
usually lighter in color,
bluish white(milky
white)
Permanent teeth are
darker, grayish or
yellowish in color.

Size
• T a
• T t a
he Primary teeth re smaller in all dimensions.
he Permanent
eeth are larger in ll dimensions.

Bucco – lingual surface • Primary teeth-
Buccal – lingual surface of molars especially 1st molar converge towards occlusal surface so they have narrow occlusal table.
• Permanent teeth –
There is less occlusal convergence of buccal lingual surface of molars towards occlusal surface.

• Pri the in r oc cu tee
Per
the hei me
MESIO DISTAL DIMENSION
mary teeth are wider in ir mesiodistal diameter elation to their cervico- clusal height which give p appearance to anterior th .
manent teeth are larger in
ir cervico-occlusal ght in relation to the siodistal diameter.
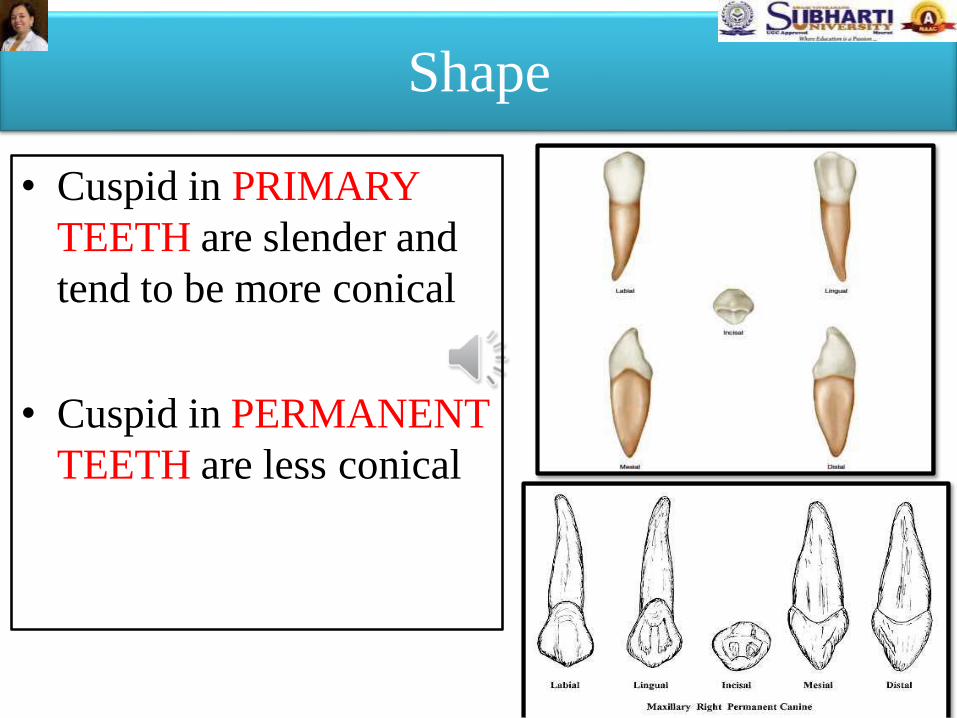
Shape
• Cuspid in PRIMARY
TEETH are slender and
tend to be more conical
• Cuspid in PERMANENT
TEETH are less conical

Cervical
• Primary teeth - Molars are more bulbous and are sharply constricted cervically (bell shape).
• Permanent teeth - They have less constriction on neck.

Cervical ridge
• Primary teeth- cervical ridges are more pronounced especially on the buccal aspect of the 1st molar.
• Permanent teeth- cervical ridges are flatter.

Occlusal Plane
• PRIMARY TEETH
– relatively flat
• PERMANENT
TEETH – more
curved contour

Contact area
• Primary teeth-
The contact areas between
molars are broader , flatter
and are situated gingivally.
• Permanent teeth –
The contact point between
permanent molars are
situated occlusally.


Clinical significance
• Buccal and lingual margins of proximal box in
class II restoration should extend towards the
embrasure to make them accessible for self
cleansing
As proximal caries starts below the contact
area gingival seat must be taken below the
contact area.

• Pri
ma
• Per
ma
Mamelons
mary teeth have no
melons .
manent teeth have
melons.

Molar dimension
• Permanent teeth- 1st molar is larger in dimension than second molar.
• Primary teeth- 1st molar is
smaller in dimension than second molar.


Size
• Primary teeth – roots are larger and more slender in comparison to crown size
• Permanent teeth – root
are short and bulbous in comparison to crown size

Maxillary and mandibular anterior teeth
• Extraction of anterior teeth is accomplished
with a rotational movement.

Maxillary and mandibular molars
• Primary molars – roots smaller in diameter and
more divergent than permanent molars.
• Slow
force
continuous palatal/lingual and buccal
allowing for the expansion of the
alveolar bone to accommodate the divergent
roots and reduce the risk of root fracture.


Furcation
• Primary teeth – more towards cervical area , root trunk smaller
• Permanent teeth –
towards apical , root trunk is larger

Clinical implication
• Slightest infection in the pulp can lead into the
bifurcation area.
• Care must be taken during access opening into
pulp chamber to prevent perforation through
floor into the furcation area.

Resorption
• Primary teeth – undergo physiologic resorption during shedding of teeth.
• Permanent teeth – physiologic Resorption is absent.

Resorption pattern
• Permanent incisor and canines develop
lingually to primary teeth - resorption of
primary teeth begins in lingual direction.
• Resorption of root of primary molars begins on
inner surface (inter-radicular dentin) because
the early developing bicuspid are found
between them

Revision
• 1. Primary Teeth are known as milk teeth
• They have refractive index similar to that of milk .
• 2. Roots of a primary teeth are
• Flared and slender


Pulp chamber
• Primary teeth –larger in
relation to crown size.
Pulpal outline follows the
DEJ more closely.
• Pulp horns closer to outer
surface.
• Permanent teeth – smaller
in relation to crown size.

Clinical significance
• HIGHER PULP HORNS- care must be taken during
restorative procedures in primary teeth especially over
mesial pulp horns.
• PULPAL FLOOR IS CONCAVE as opposed to
permanent teeth

CELLULARITY
• Primary teeth – high degree of cellularity and
vascularity
• Permanent teeth – less degree of cellularity
and vascularity

Primary teeth - Pulp nerve fibers pass to the
odontoblastic area, where they terminate as
free nerve endings.
Permanent teeth- Nerve fibers terminate
mainly among the odontoblasts and even
beyond the predentin.
Nerve fibers
Bernick S. Innervation of the teeth and periodontium. Dent Clin North Am 1959;
p.503.

• Density of the innervation of the primary tooth
is not as great as that of the permanent tooth
and may be the reason why primary teeth are
less sensitive to operative procedure.
• Neural tissue is the first to degenerate when
root resorption begins, just as it is the last
tissue to mature when the pulp develops.

Clinical significance
• Primary teeth have high potential for repair
as reparative dentin formation is more
More chances of spread of infection –
space involvement (Cellulitis)
Permanent teeth have less potential for repair

Accessory canal
• Primary teeth - floor of pulp chamber is more
porous.
• Accessory canal directly leads to inter-
radicular furcation area.
• Permanent teeth – floor of pulp chamber do
not have many accessory canal.

Accessory (or lateral) canals also occur, located
most commonly in the apical third of the root and in
maxillary and mandibular molars are common in the
furcation area.

Root canals
• Primary teeth – canals are thin tortuous and
have a branching path (ribbon like).
• Permanent teeth – canals are well defined
with less branching.

Clinical implication
• Variation in root canal makes it difficult to
remove necrotic tissue by instrumentation.
Profuse irrigation with 5.25°7% sodium
hypochlorite (NaOC1) is recommended .

Apical foramen
• Primary teeth- apical foramen is enlarged thus having abundant blood supply
• Permanent teeth-
constricted apical foramen thus having reduced blood supply


Enamel • Primary teeth-
Enamel is thinner and has a more consistent depth of about 1mm thickness throughout the crown. The enamel rods at the cervical slopes occlusally from the DEJ. Density of enamel rods is higher in deciduous.
• Permanent teeth –
The enamel is thicker and has a thickness of about 2-3 mm. the enamel rods are oriented gingivally from the DEJ.

Enamel thickness

Direction of enamel rod

Clinical significance
• As enamel rod of primary molars is towards
occlusal surface there is no need for beveling
the gingival seat in primary molars
• Beveling is done in permanent teeth because of
apical or horizontal inclination of enamel rods
in permanent molars

Incremental line
• Primary teeth-
incremental line of
retzius are less
common.
• Permanent teeth -
incremental line of
retzius are more
common

Dentin
• Primary teeth – greater thickness of the
dentinal wall over the occlusal fossa of molars.
• Permanent teeth- lesser thickness of dentin
over the pulpal wall at the occlusal fossa of
molars.

DENTIN
• Primary teeth - dentinal tubule are less
regular. Interglobular dentin is absent.
• Permanent teeth- dentinal tubules are more
regular. Interglobular dentin is present

CLINICAL SIGNIFICANCE
• Thickness of enamel and dentin is thin in
primary teeth so the pulp is proportionately
higher due to this caries can progress to pulp
faster ,
• Etching time in primary teeth is 90-120 sec
whereas in permanent teeth is 30 sec because
more organic matter in enamel of primary teeth

NEONATAL LINE
Primary teeth - present in both enamel and dentin.
Permanent teeth- seen only in 1st
permanent molar as mineralization takes place at birth.

Neonatal line
• Line reflects the abrupt changes in
environment that occur at birth
• Accentuated line of Retzius – enamel
• Accentuated line of contour – dentin

CEMENTUM
PRIMARY TEETH
• Cementum is very thin
and of primary type.
• Secondary cementum is
characteristically absent.
PERMANENT TEETH
• Secondary cementum is
present.

CEMENTODENTINAL JUNCTION
PRIMARY TEETH
• Cementodentinal junction is
scalloped.
PERMANENT TEETH
• Dentin surface upon which
cementum is deposited is
smooth.

CEMENTOENAMEL JUNCTION

CEMENTOENAMEL JUNCTION
• PRIMARY TEETH
• cementum meets
enamel at sharp line
• 2nd common is cementum overlapping the enamel
• Enamel and cementum do not meet is rare
• PERMANENT TEETH
60%- cementum overlaps
the enamel
30%- cementum meets enamel at sharp line
10%- enamel and cementum do not meet.

Question
Enamel of primary teeth is and has more consistent







