Download - Descriptive Assessment of Depression and Anxiety Symptoms in an Outpatient Obstetric Clinic Sample
A Descriptive Assessment of Depression & Anxiety Symptoms
in an Outpatient Obstetric Clinic Sample: Screening for Symptoms in the Context of
Substance Use Histories
Teresa A. Lillis, M.A., ABI.1,2, Stephen Lassen, PhD.2, & Erin Smith, B.S.2
1. Rush University Medical Center, Dept. of Behavioral Sciences, Chicago, IL.2. University of Kansas Medical Center, Dept. of Pediatrics, Kansas City, KS.
✔
Conflict of Interest Disclosures for Speakers
1. I do not have any relationships with any entities producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients, OR
2. I have the following relationships with entities producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients:
Type of Potential Conflict Details of Potential Conflict
Grant/Research Support
Consultant
Speakers’ Bureaus
Financial support
Other
3. The material presented in this lecture has no relationship with any of these potential conflicts, OR
4. This talk presents material that is related to one or more of these potential conflicts, and the following objective references are provided as support for this lecture:
1.
2.
3.
Health Promotion in the Postpartum• The birth of a child is a considered the greatest change in the family
life cycle (Nystrom & Ohrling, 2004).• A time of excitement and joy as well as considerable stress.
• North American women receive a great detail of medical attention and advice during pregnancy, but much less in the postpartum (Ayoola et al., 2010).• This shift can leave women vulnerable to psychological problems
arising in the postpartum.• Adequate screening for postpartum psychological issues with
provision of appropriate treatment-related referrals may improve the long-term health outcomes of both mothers and their babies.
Mental Health in the Postpartum• Postpartum Depression (PPD)is the most common mental health
issue.• Prevalence 10-20% of U.S. women and ~15% of women world-wide (Beck
et al., 2001; O’Hara et al., 2009).• Diagnostic criteria for PPD are the same as for a Major Depressive Episode
• For the previous two weeks:• Down/depressed mood nearly every day AND/OR loss of interest or pleasure in
previously enjoyable activities• Five or more of the following symptoms present most days:
• Significant change in appetite or weight• Insomnia or hypersomnia• Psychomotor agitation/retardation• Fatigue/loss of energy• Feelings of worthless/guilt• Difficulty concentrating/making decisions• Suicidal thoughts/plans/intent/attempts
• Onset limited 2 weeks-12 months postpartum.• Different from the “baby blues.”
• Birth-2 weeks postpartum; mildly depressed mood, tearfulness, fatigue.
Mental Health in the Postpartum Cont.
• Anxiety-related issues may also occur.• 12-20% experience generalized anxiety symptoms (Farr et al., 2014; Stuart et
al, 1998; Wenzel et al., 2005; Vesga-Lopez et al., 2008)• OCD symptoms in 11% (Miller et al., 2013)• PTSD symptoms in 9% (Beck et al., 2011)
• Depression and Anxiety disorders are highly comorbid in perinatal populations (Cohen & Pearlstein, 2010).• Discrete symptom presentation is the exception rather than the rule.
• Precise etiology for psychiatric disorder manifestation in perinatal populations is unclear.• Likely a diathesis stress disorder.
• An existing predisposition or genetic vulnerability is triggered by stress of pregnancy or labor/delivery.
• Risk Factors (Brockington, 2004):• History of Depression/Anxiety/other mental disorder, especially during
pregnancy• Poor social support• Lower Age, SES, and minority status
Perinatal Maternal Substance Use• The perinatal period is generally a time of reduced substance use
• Approximately 8-18% of childbearing women continue use of illicit and licit drugs (Connelly et al., 2014).
• Deleterious health outcomes related to perinatal substance use:• Prematurity, intrauterine/neonatal demise and poor long-term child
health outcomes (Bonello et al., 2014)
• In the general population, substance use is highly correlated with mental illness• Some studies have found perinatal substance use to be related to
worsening psychiatric symptoms severity in the perinatal period (Connelly et al.; Chisolm et al., 2009)
• Relationship remains unclear as other studies have not demonstrated this relationship (Forray et al., 2013).
Screening for Postpartum Mental Health
• Mental health screening integration into obstetric and well-child visits has improved (Olson et al., 2002; Guirguis-Blake et al., 2003).
• Most common screener, Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987).• Beck Depression Inventory (BDI-II; Beck, 1996), CES-D, Postpartum
Depression Screening Scale (PDSS; Beck & gable, 2000), Patient Health Questionnaire-9 (PHQ-9; Spitzer et al., 1999), etc.
• The stigma of reporting emotional distress in the postpartum persists• Many at-risk postpartum women continue to missed by their
healthcare providers.• Systematic screening with treatment referral and follow-up needed to
improve maternal/child health outcomes (Gjerdingen & Barbara, 2007).
Current Study• A sample of 84 women from a Midwest Academic Medical Center
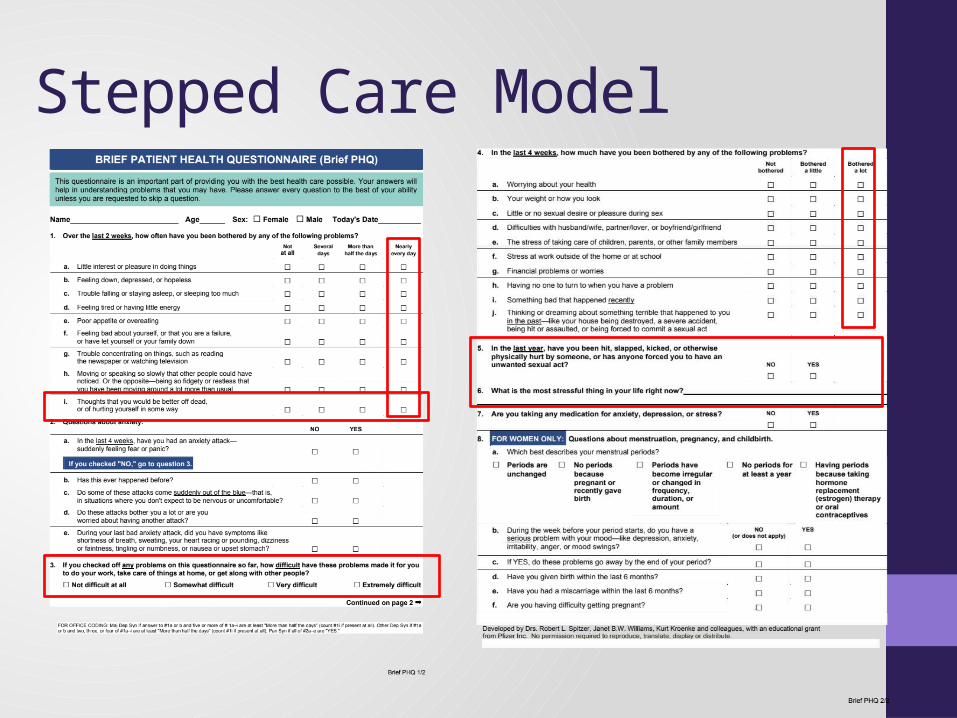
Obstetric Clinic completed the Brief-Patient Health Questionnaire (B-PHQ; Sptizer et al., 2000) at their 6-week postpartum visit.
• Brief-PHQ was chosen for its:• Brevity• Assessment of depression and anxiety symptoms• Comprehensive coverage of psychosocial stressors • Items pertaining to women’s health issues
• Limited/targeted EMR chart review conducted to confirm:• Ethnicity• Obstetric history• Characteristics from most recent delivery• Substance use history
Purpose of Study
• Describe frequency/severity of depression and anxiety symptoms reported in the obstetric sample.
• Assess the relationship between depression/anxiety symptoms and substance use history.
• Inform recommendations for postpartum mental health screening.
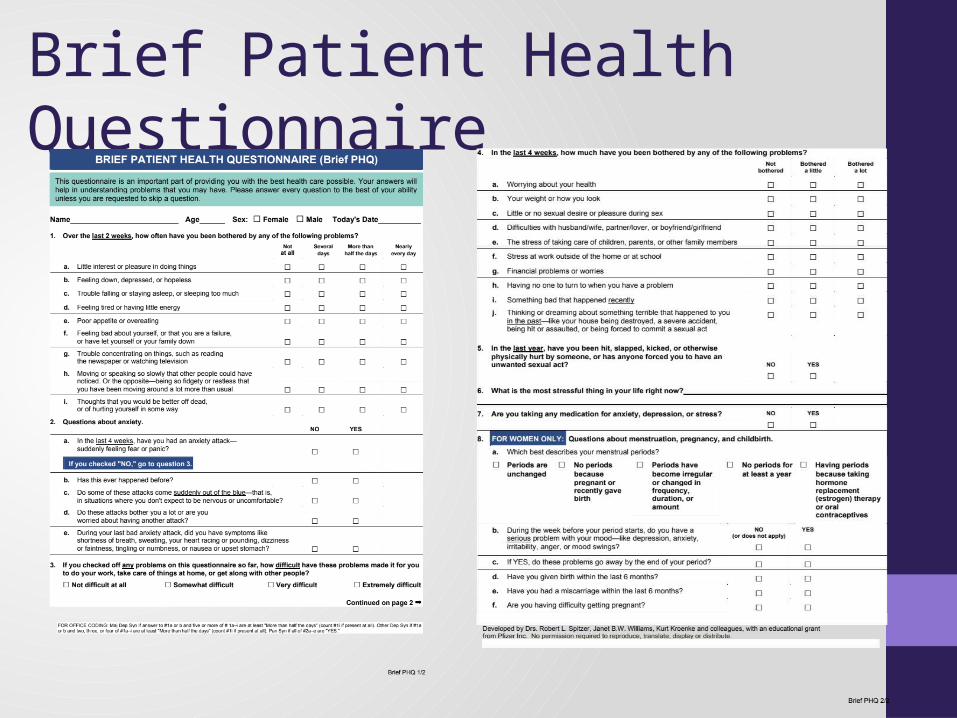
Brief Patient Health Questionnaire
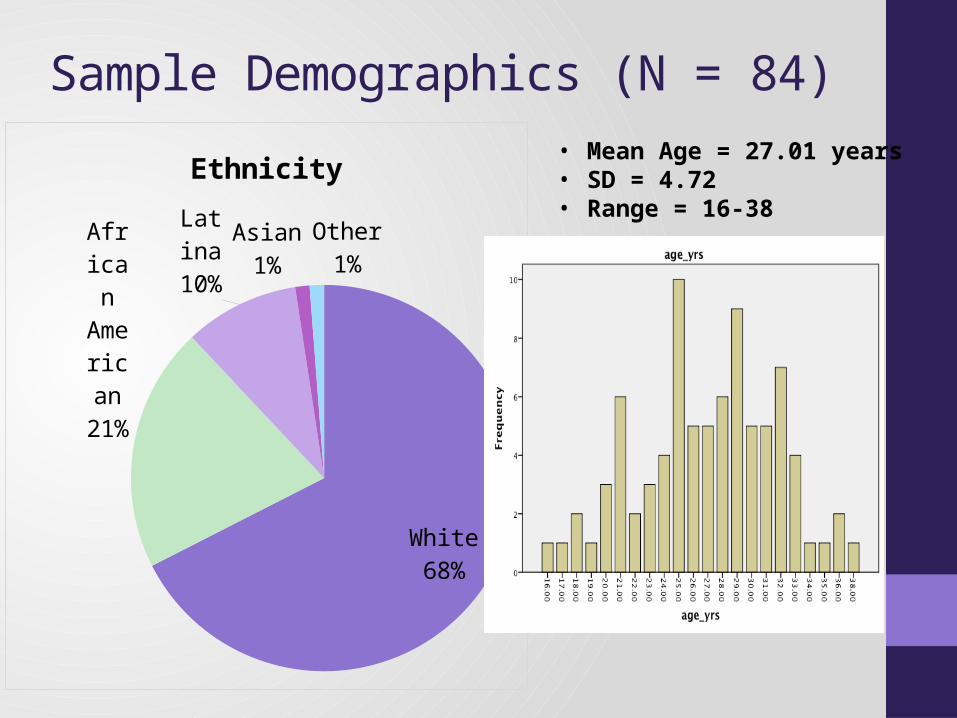
Sample Demographics (N = 84)
White68%
African Amer-ican21%
Latina10%
Asian1%
Other1%
Ethnicity • Mean Age = 27.01 years• SD = 4.72• Range = 16-38
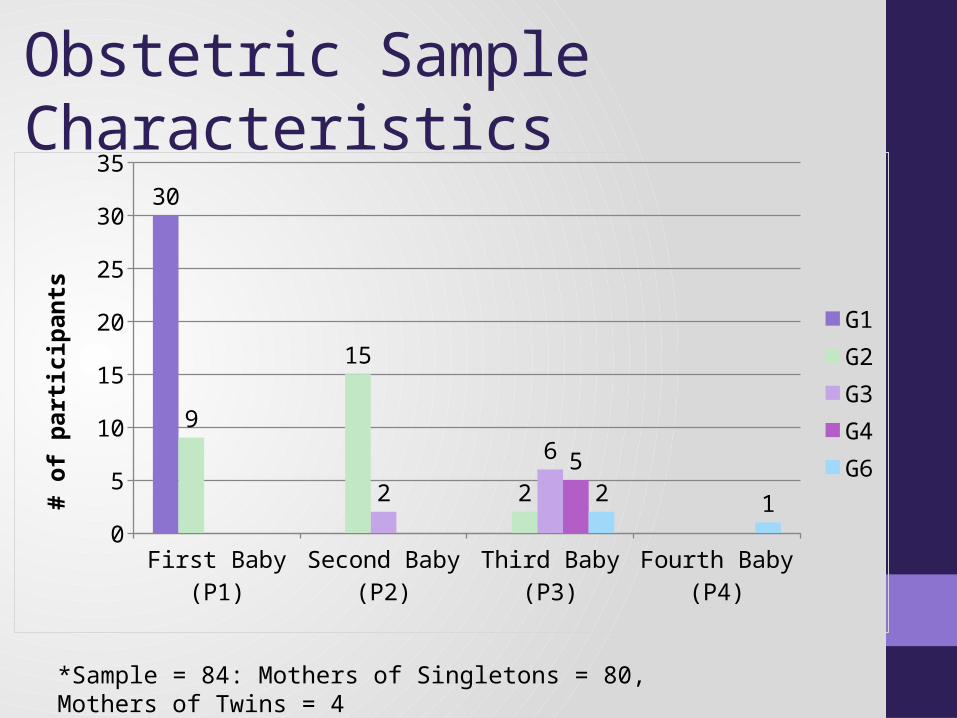
Obstetric Sample Characteristics
First Baby (P1) Second Baby (P2)
Third Baby (P3) Fourth Baby (P4)0
5
10
15
20
25
30
35
30
9
15
22
6 52 1
G1G2G3G4G6
# of
par
ticip
ants
*Sample = 84: Mothers of Singletons = 80, Mothers of Twins = 4
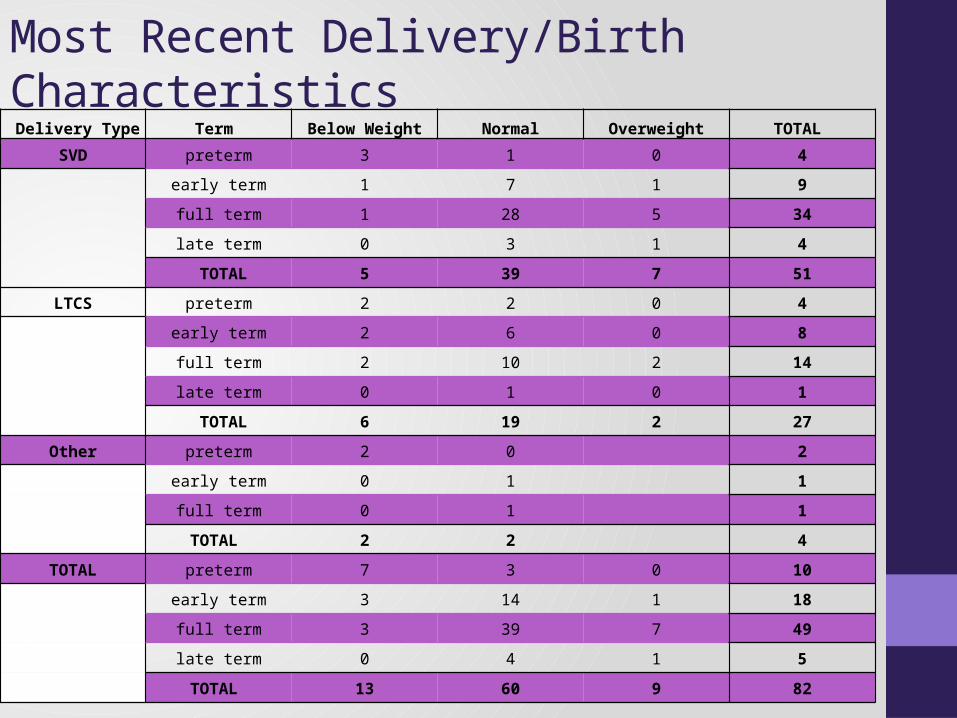
Most Recent Delivery/Birth Characteristics Delivery Type Term Below Weight Normal Overweight TOTAL
SVD preterm 3 1 0 4
early term 1 7 1 9
full term 1 28 5 34
late term 0 3 1 4
TOTAL 5 39 7 51
LTCS preterm 2 2 0 4
early term 2 6 0 8
full term 2 10 2 14
late term 0 1 0 1
TOTAL 6 19 2 27
Other preterm 2 0 2
early term 0 1 1
full term 0 1 1
TOTAL 2 2 4
TOTAL preterm 7 3 0 10
early term 3 14 1 18
full term 3 39 7 49
late term 0 4 1 5
TOTAL 13 60 9 82
EMR Substance Use History• Current/former use information obtained via EMR review.
• Matched updated information to the date of the 6-week visit/Brief-PHQ completion
• Not possible to verify whether former substance use occurred during most recent pregnancy or prior to pregnancy.
• Severity Classification for former/current use:• Smoking:
• Mild = < 1 pack/week • Moderate = 1-2 packs/week• Heavy = > 3 packs/week
• Alcohol:• Mild = “occasional” - 1-2 drinks/week• Moderate = 3-5 drinks/week• Heavy = > 5 drinks/week
• Drugs:• Mild = < 1/year• Moderate = “occasional” - 1-2x/month• Heavy = > 1/week
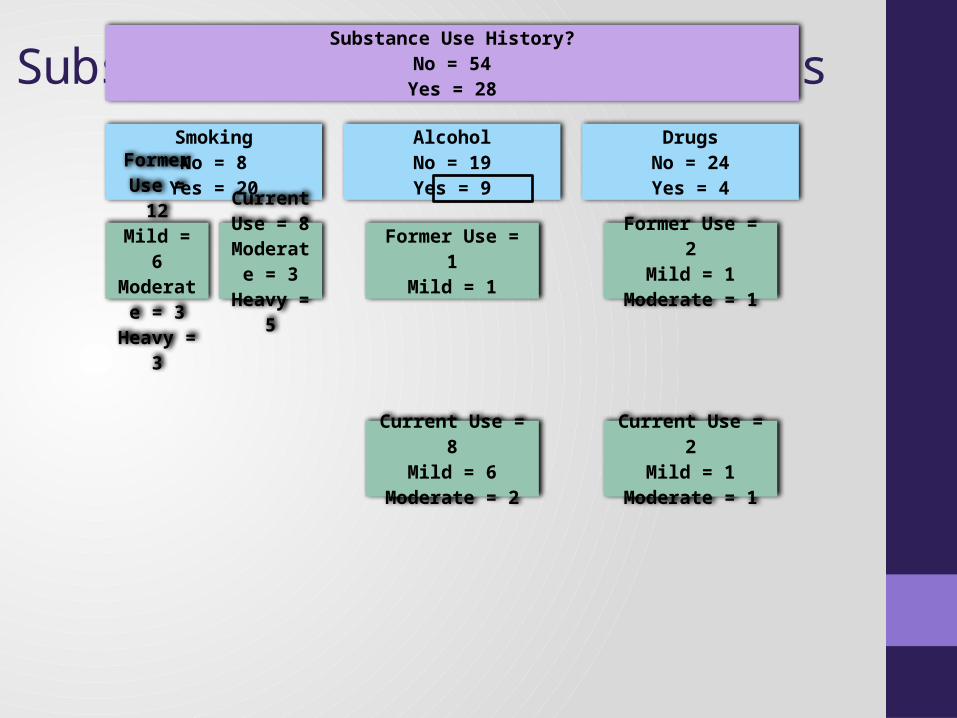
Substance Use CharacteristicsSubstance Use History?
No = 54Yes = 28
SmokingNo = 8
Yes = 20
Former Use = 12Mild = 6
Moderate = 3
Heavy = 3
Current Use = 8
Moderate = 3
Heavy = 5
AlcoholNo = 19Yes = 9
Former Use = 1Mild = 1
Current Use = 8Mild = 6
Moderate = 2
DrugsNo = 24Yes = 4
Former Use = 2Mild = 1
Moderate = 1
Current Use = 2Mild = 1
Moderate = 1
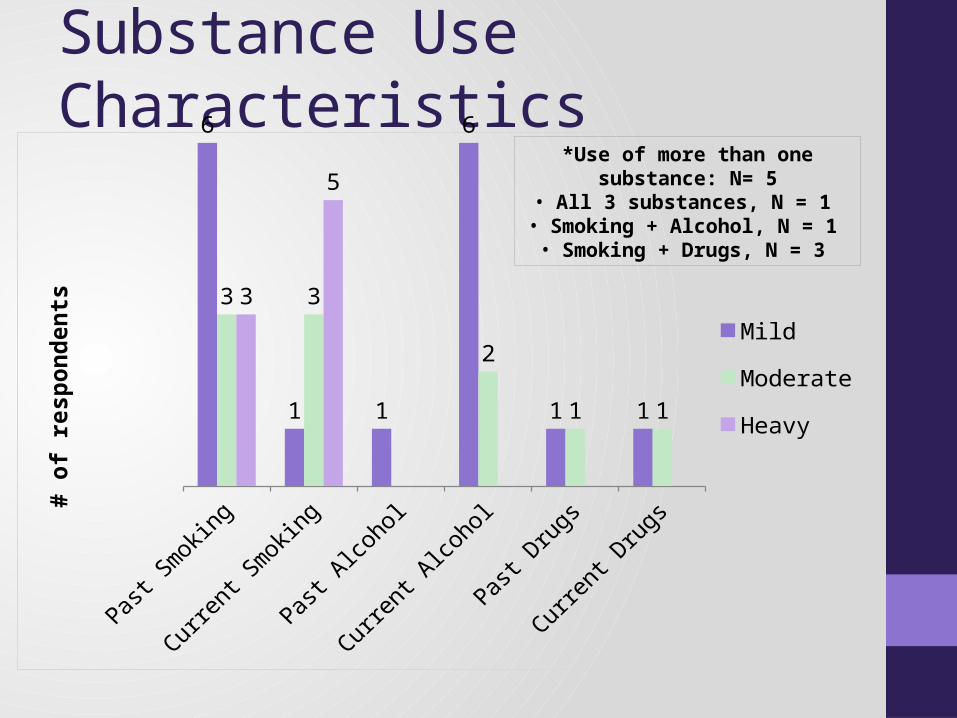
Substance Use Characteristics6
1 1
6
1 1
3 3
2
1 1
3
5
Mild
Moderate
Heavy
# of
resp
onde
nts
*Use of more than one substance: N= 5• All 3 substances, N = 1
• Smoking + Alcohol, N = 1• Smoking + Drugs, N = 3
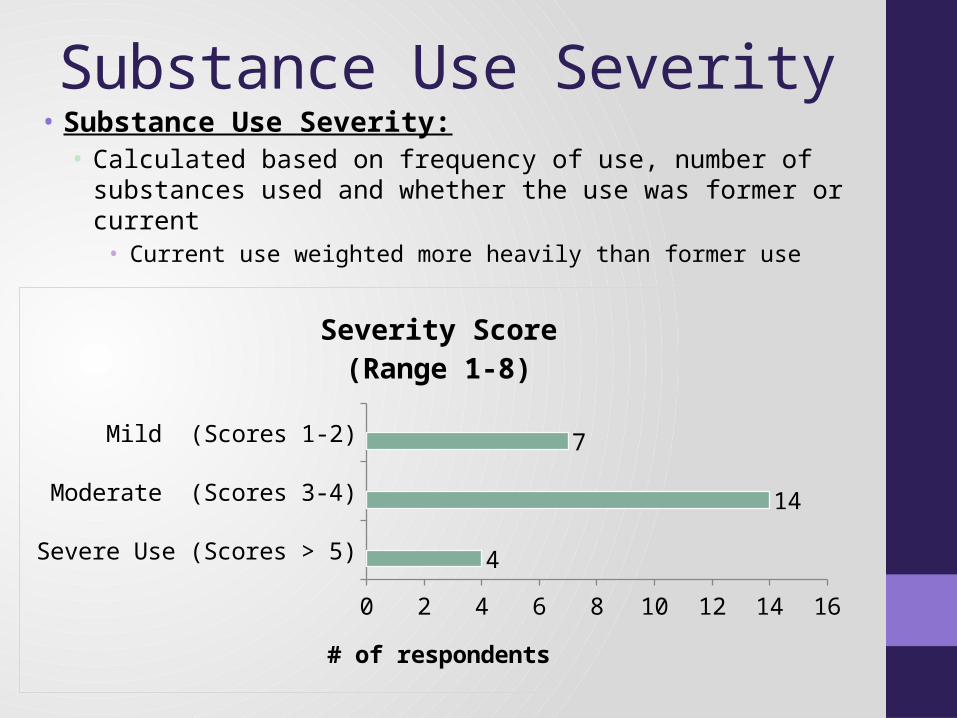
Substance Use Severity• Substance Use Severity:
• Calculated based on frequency of use, number of substances used and whether the use was former or current
• Current use weighted more heavily than former use
Severe Use (Scores > 5)
Moderate (Scores 3-4)
Mild (Scores 1-2)
0 2 4 6 8 10 12 14 16
4
14
7
Severity Score(Range 1-8)
# of respondents
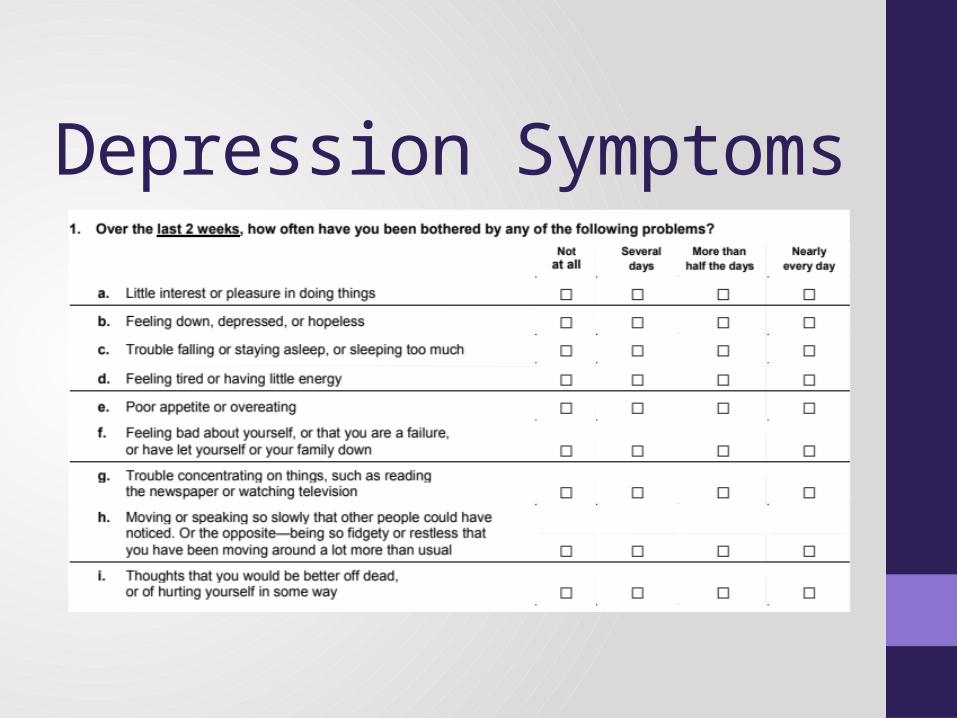
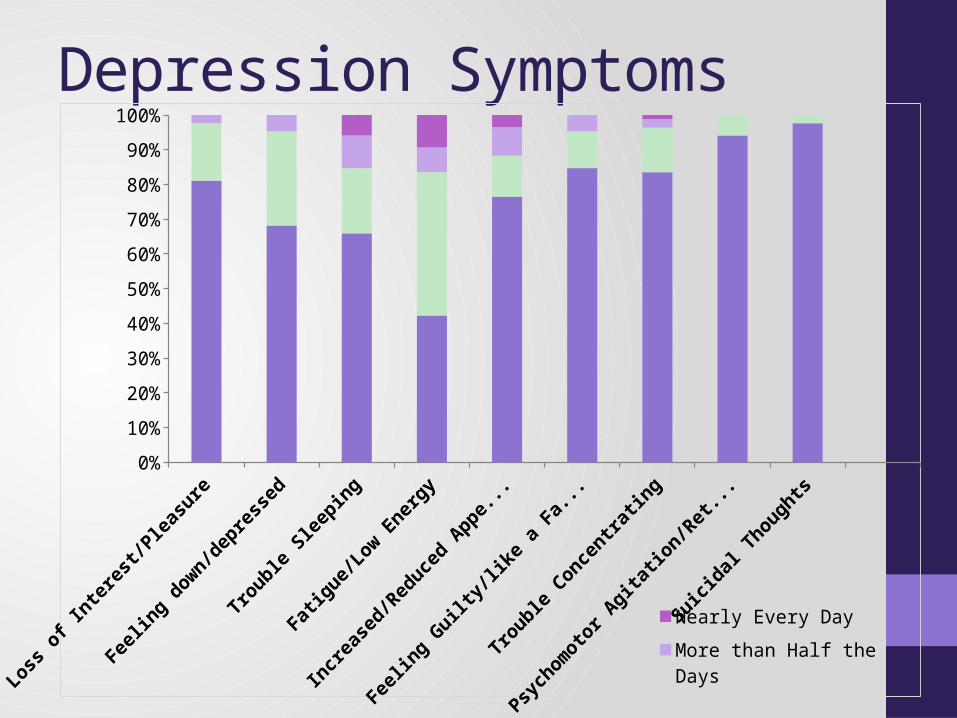
Depression Symptoms
Depression Symptoms
Loss
of Interest/
Pleasure
Feelin
g down/d
epressed
Trouble Sl
eeping
Fatigu
e/Low Energy
Increase
d/Reduce
d Appetite
Feelin
g Guilty
/like a Fa
ilure
Trouble Conce
ntrating
Psychomoto
r Agit
ation/Retard
ation
Suici
dal Though
ts0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Nearly Every DayMore than Half the DaysSeveral DaysNot at All
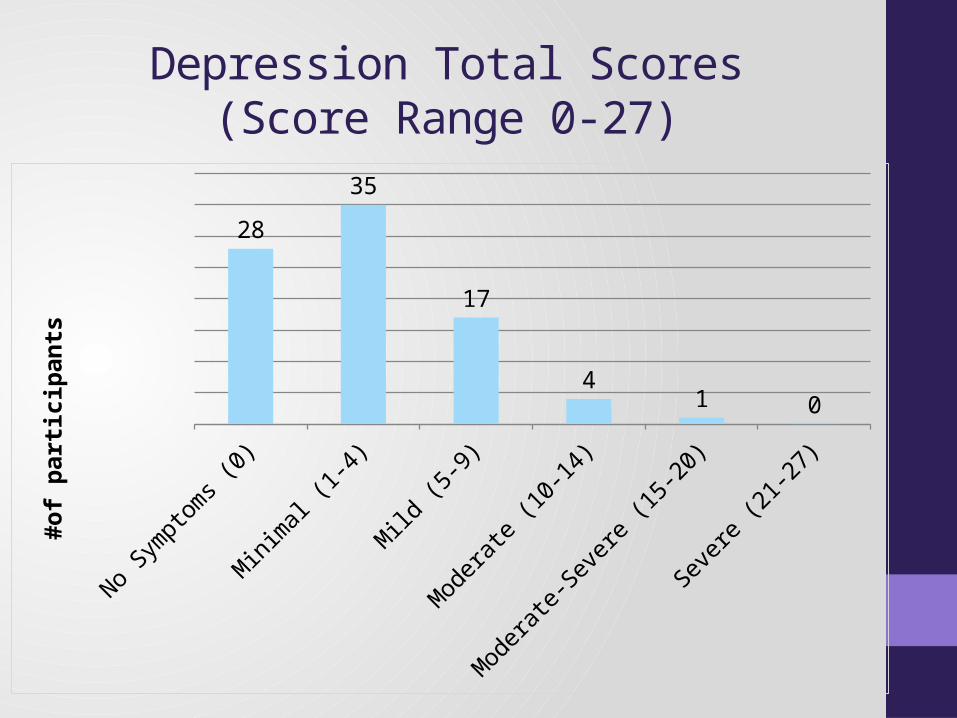
Depression Total Scores(Score Range 0-27)
No Sympto
ms (0)
Minim
al (1-4)
Mild
(5-9)
Moderat
e (10-14)
Moderat
e-Seve
re (15-20)
Seve
re (21-27)
28
35
17
41 0
#of p
artic
ipan
ts
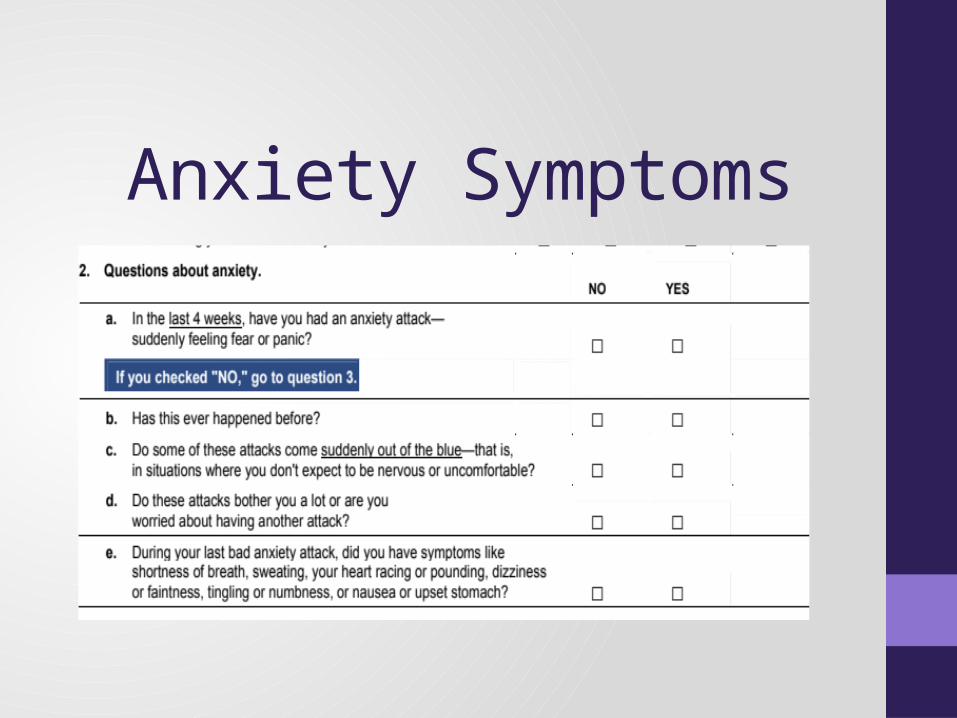
Anxiety Symptoms
Anxiety Symptoms
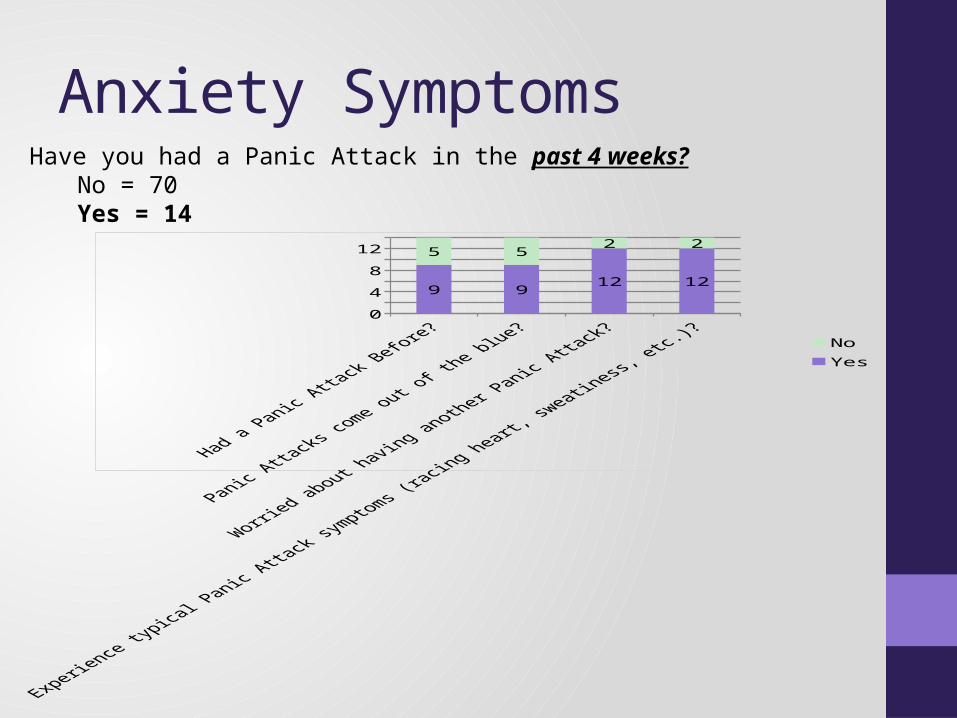
0
4
8
12
9 912 12
5 52 2
NoYes
Have you had a Panic Attack in the past 4 weeks?No = 70Yes = 14
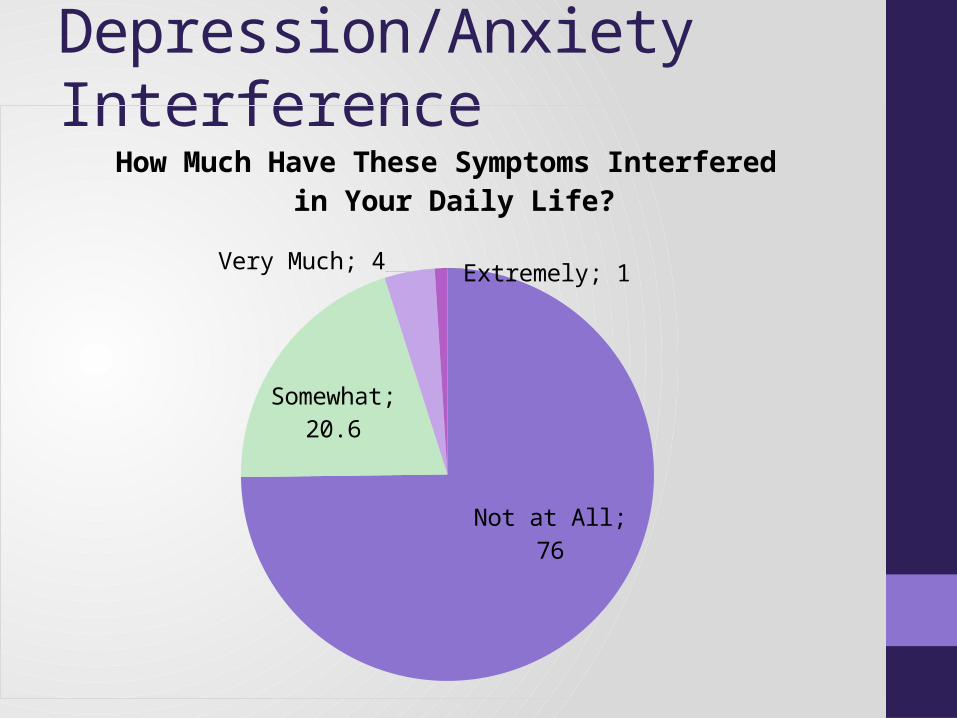
Depression/Anxiety Interference
Not at All; 76
Somewhat; 20.6
Very Much; 4 Extremely; 1
How Much Have These Symptoms Interfered in Your Daily Life?
Depression/Anxiety Symptom Summary• Most commonly reported depression symptoms:
• 1. Fatigue/Low Energy• 2. Trouble Sleeping• 3. Feeling Down/Depressed
• Severity of symptoms reported:• 33% experienced NO symptoms• 61% minimal-mild symptom severity• 6% moderate-severe symptom severity
• Only 14 respondents indicated a history of experiencing panic attacks
• 75% of the respondents did not feel impaired at all by depression and/or anxiety symptoms
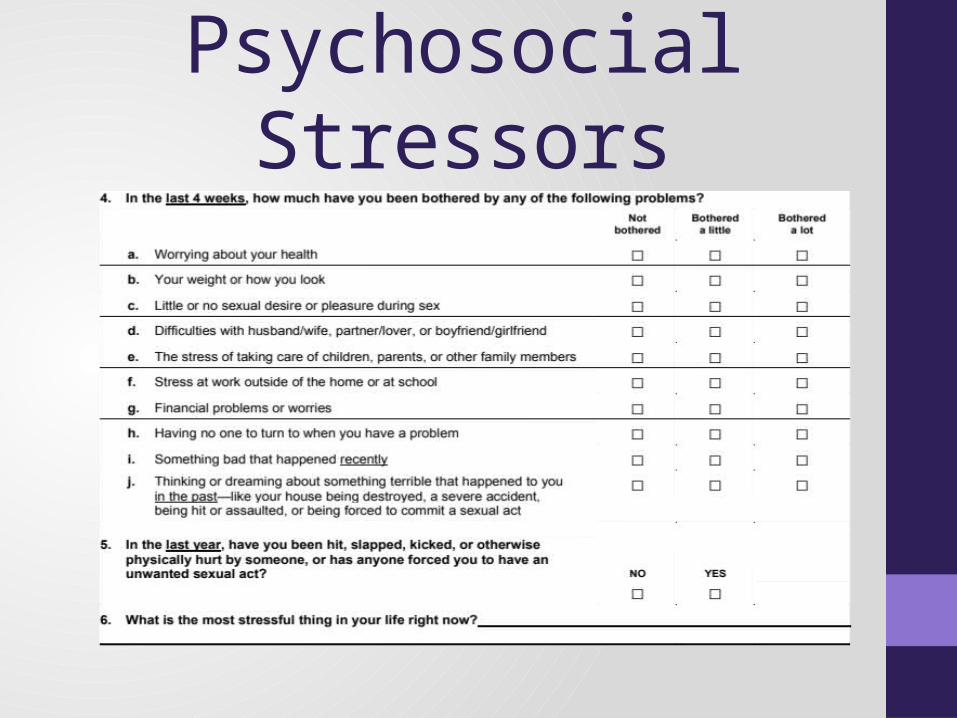
Psychosocial Stressors
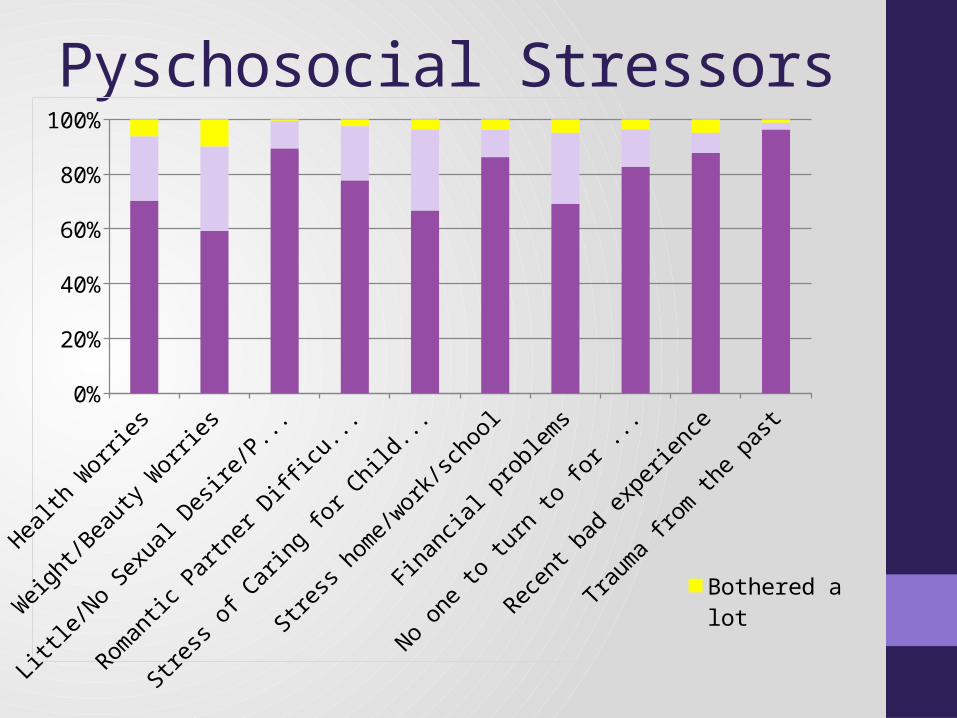
Pyschosocial Stressors
Health W
orries
Weigh
t/Beau
ty W
orries
Little/N
o Sexu
al Desir
e/Pleasu
re
Romantic P
artner D
ifficu
lties
Stress
of Cari
ng for C
hildren/Fa
mily
Stress
home/work/
school
Finan
cial p
roblems
No one to tu
rn to
for h
elp
Recent b
ad exp
erience
Trauma f
rom th
e past0%
10%20%30%40%50%60%70%80%90%
100%
Bothered a lot
Bothered a little
Not at all
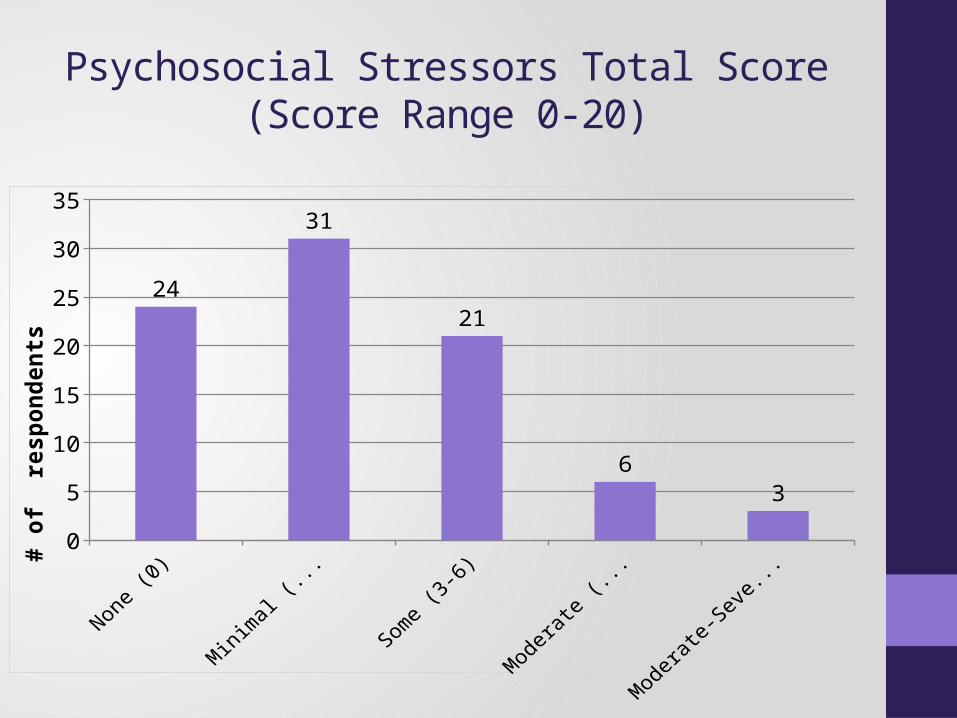
Psychosocial Stressors Total Score(Score Range 0-20)
0
5
10
15
20
25
30
35
24
31
21
63
# of
res
pond
ents
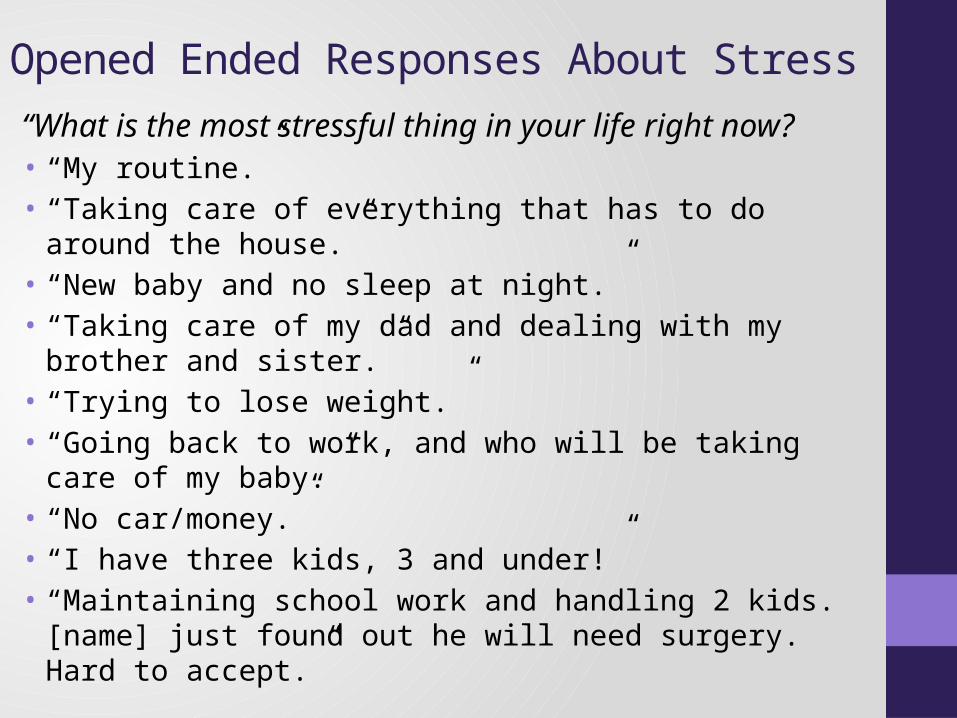
Opened Ended Responses About Stress
“What is the most stressful thing in your life right now?• “My routine.”• “Taking care of everything that has to do around the house.”• “New baby and no sleep at night.”• “Taking care of my dad and dealing with my brother and sister.”• “Trying to lose weight.”• “Going back to work, and who will be taking care of my baby.”• “No car/money.”• “I have three kids, 3 and under!”• “Maintaining school work and handling 2 kids. [name] just found out
he will need surgery. Hard to accept.”
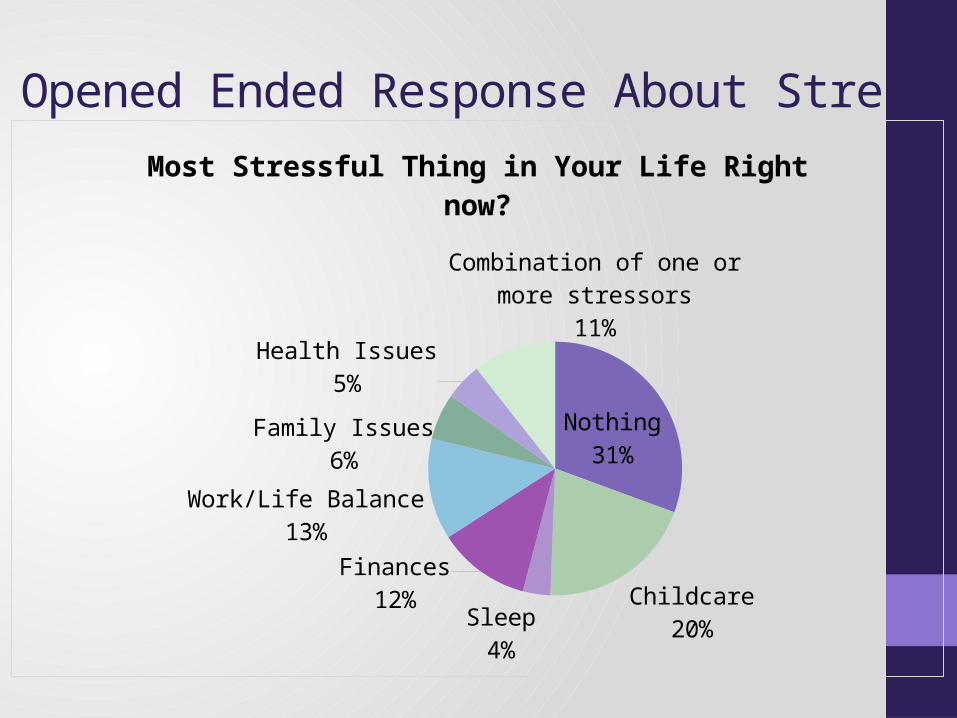
Opened Ended Response About Stress
Nothing31%
Childcare20%
Sleep3%
Finances12%
Work/Life Balance13%
Family Issues6%
Health Issues5%
Combination of one or more stressors
11%
Most Stressful Thing in Your Life Right now?
Summary of Psychosocial Stressors• Most commonly reported stressors:
• 1. Concerns about weight/beauty• 2. Financial Concerns• 3. Stress/Demands of Childcare
• More variability in severity of stress:• 28% report no stress• 62% report minimal-moderate stress• 10% report severe stress
• Most stressful thing in life right now?• 20% = Childcare• 13% = Work/Life Balance Issues• 12% = Finances
Statistical Relationships:Depression, Anxiety &
Substance Use
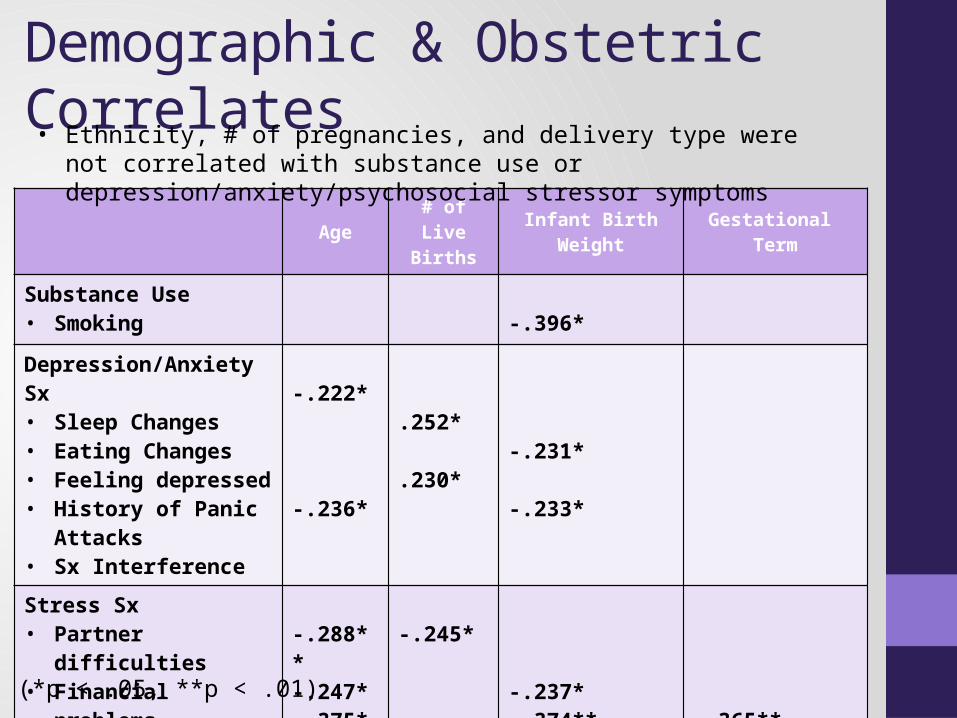
Demographic & Obstetric Correlates
Age # of Live Births Infant Birth Weight Gestational
Term
Substance Use• Smoking -.396*
Depression/Anxiety Sx• Sleep Changes• Eating Changes• Feeling depressed• History of Panic Attacks• Sx Interference
-.222*
-.236*
.252*
.230*-.231*
-.233*
Stress Sx• Partner difficulties• Financial problems• No social support• Recent trauma• Childcare stress
-.288**-.247*-.375**
-.245*
-.237*-.374** -.365**
-.366**
(*p < .05, **p < .01)
• Ethnicity, # of pregnancies, and delivery type were not correlated with substance use or depression/anxiety/psychosocial stressor symptoms
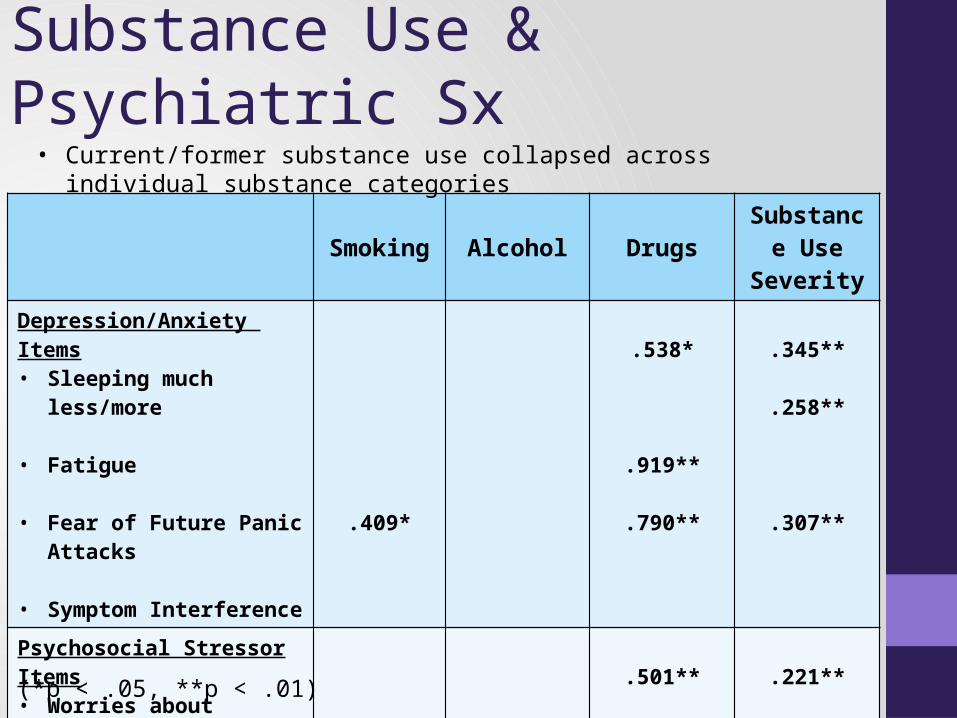
Substance Use & Psychiatric Sx
Smoking Alcohol Drugs Substance Use Severity
Depression/Anxiety Items• Sleeping much less/more
• Fatigue
• Fear of Future Panic Attacks
• Symptom Interference .409*
.538*
.919**
.790**
.345**
.258**
.307**
Psychosocial Stressor Items• Worries about weight/looks
• Childcare Stress .394*
.501** .221**
(*p < .05, **p < .01)
• Current/former substance use collapsed across individual substance categories
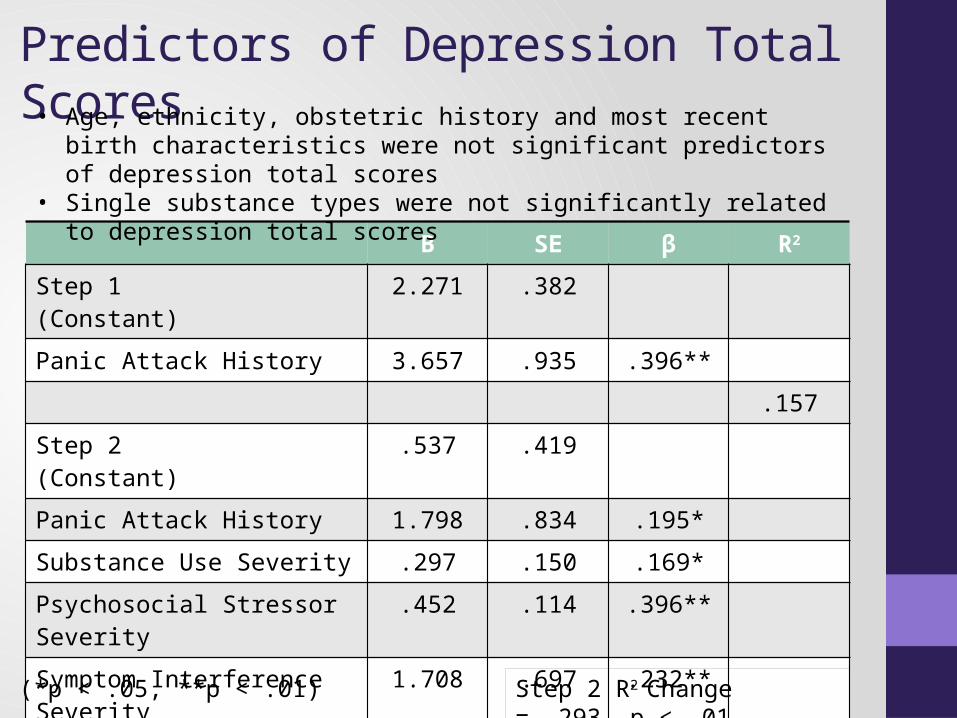
Predictors of Depression Total Scores
B SE β R2
Step 1(Constant)
2.271 .382
Panic Attack History 3.657 .935 .396**.157
Step 2(Constant)
.537 .419
Panic Attack History 1.798 .834 .195*Substance Use Severity .297 .150 .169*Psychosocial Stressor Severity .452 .114 .396**Symptom Interference Severity 1.708 .697 .232**
.450
Step 2 R2 Change = .293, p < .01(*p < .05, **p < .01)
• Age, ethnicity, obstetric history and most recent birth characteristics were not significant predictors of depression total scores
• Single substance types were not significantly related to depression total scores
Summary of Statistical Relationships• Demographic & Obstetric Relationships:
• Age:• Younger respondents reported more sleep disruption, more psychiatric
symptom interference, more relationship and financial stress and low social support
• Parity:• women with more children were more likely to have had a recent panic
attack and report changes in their eating habits• Women with fewer children reported more relationship stress
• Infant Birth Weight:• lower infant birth weight was related to smoking history, feeling
depressed, greater psychiatric symptom interference, low social support and recent trauma.
• Gestational Term: • Shorter gestation was related to recent trauma and greater childcare stress
Summary Cont.• Substance Use & Psychiatric Symptom Relationships:
• Smoking and drug use history and overall substance use severity were strongly, positively related to increased impairment from psychiatric symptoms.
• Drug use and overall substance use severity were strongly related to items reflecting exhaustion and fatigue and worries about weight/looks.
• Current alcohol use was predominantly mild in this sample subset and was only related to increased childcare stress.
Summary Cont.• Although the sample as a whole generally appeared high-
functioning and with relatively low levels of reported distress, variability in depression scores were related to a number of psychosocial factors:• A history of panic attacks predicted higher depression scores.• After controlling for panic attack history, higher depression scores
were predicted by:• greater psychosocial distress• greater impairment from psychiatric symptoms• Increased substance use severity

Limitations & Recommendations
Limitations• Small, homogenous sample
• Relatively high-functioning, non-distressed• Cross-sectional assessment
• No ability for longitudinal follow-up of sample to confirm/disconfirm onset of mental health problem with appropriate diagnostic tools.
• Not able to confirm pre-existing mental health diagnoses.• EMR review to assess substance use may have resulted in an
under/over-estimation of actual current/former substance use• Brief-PHQ’s lack of assessment of anxiety disorders and
symptoms, outside panic attack history
Where Do We Go From Here?• Women should continued to be screened for perinatal mental
distress.• Risk factors to consider based on this study:
• Younger mothers, multiparous mothers, and mothers with a history of shorter gestation and/or low infant birth weight
• Comorbid mental health problems• History of substance use, especially the number of substances used
and the frequency of use• Reported impairment from psychiatric symptoms• Number and severity of psychosocial stressors
How Do We Get There From Here?• Although any screener is better than no screener…
• Screeners with items that ask about “stress” in addition to face valid depression/anxiety items may circumvent propensity for underreporting
• Screening for postpartum substance use also prone to underreporting (Magura & Kang, 1996; Osterea et al., 2001).• Quasi-anonymous methods may increase perinatal substance use
disclosure (Beatty, Chase, & Ondersma, 2013).• Chart review not ideal, but may provide a context for assessing
overall physical and psychological risk in the postpartum• Good screening needs good follow-up.
• Treatment-related and follow-up referral decisions could be conceptualized with Stepped Care Model.
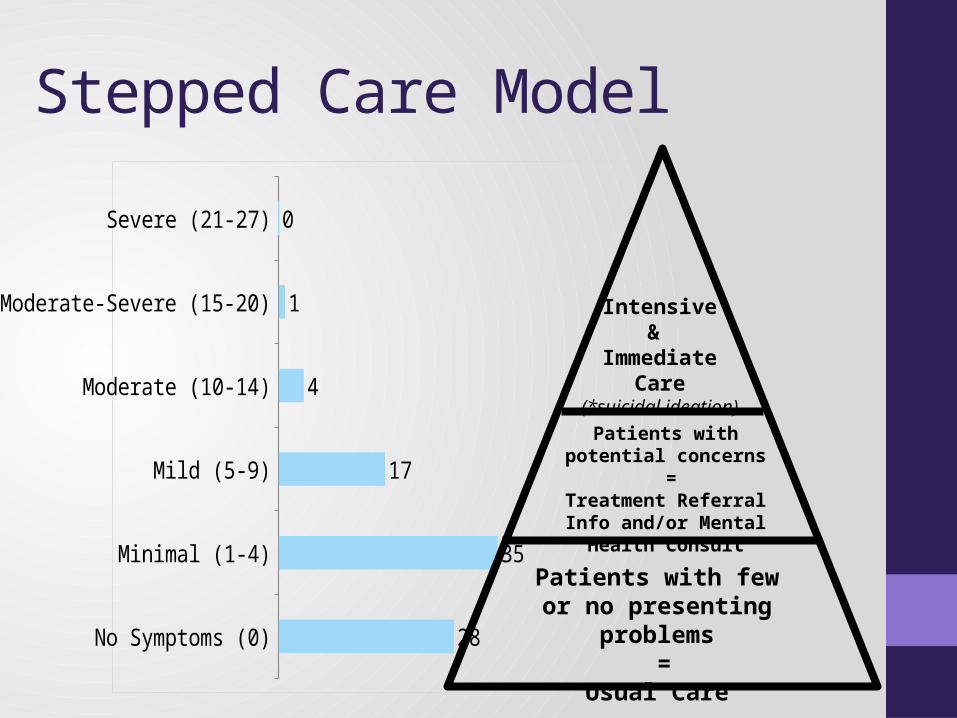
Stepped Care Model
No Symptoms (0)
Minimal (1-4)
Mild (5-9)
Moderate (10-14)
Moderate-Severe (15-20)
Severe (21-27)
28
35
17
4
1
0
Patients with few or no presenting problems
=Usual Care
Patients with potential concerns
=Treatment Referral Info
and/or Mental Health Consult
Intensive&
Immediate Care(*suicidal ideation)
Stepped Care Model
Stepped Care Model Decision Making: Sample Language
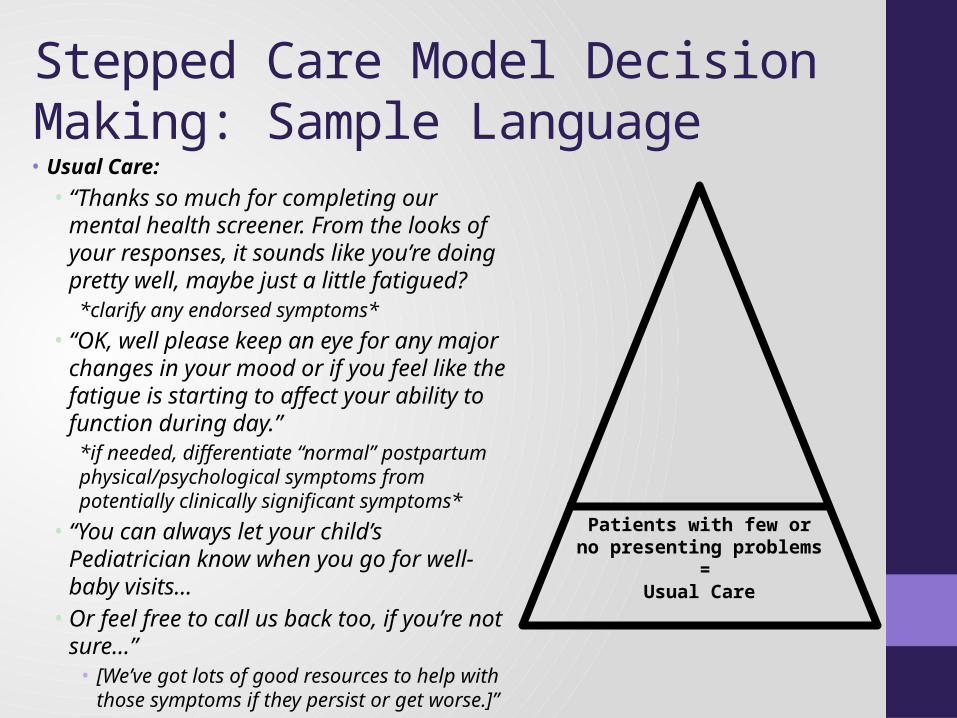
Patients with few or no presenting problems
=Usual Care
• Usual Care:• “Thanks so much for completing our mental
health screener. From the looks of your responses, it sounds like you’re doing pretty well, maybe just a little fatigued?
*clarify any endorsed symptoms*• “OK, well please keep an eye for any major
changes in your mood or if you feel like the fatigue is starting to affect your ability to function during day.”
*if needed, differentiate “normal” postpartum physical/psychological symptoms from potentially clinically significant symptoms*
• “You can always let your child’s Pediatrician know when you go for well-baby visits…
• Or feel free to call us back too, if you’re not sure…”
• [We’ve got lots of good resources to help with those symptoms if they persist or get worse.]”
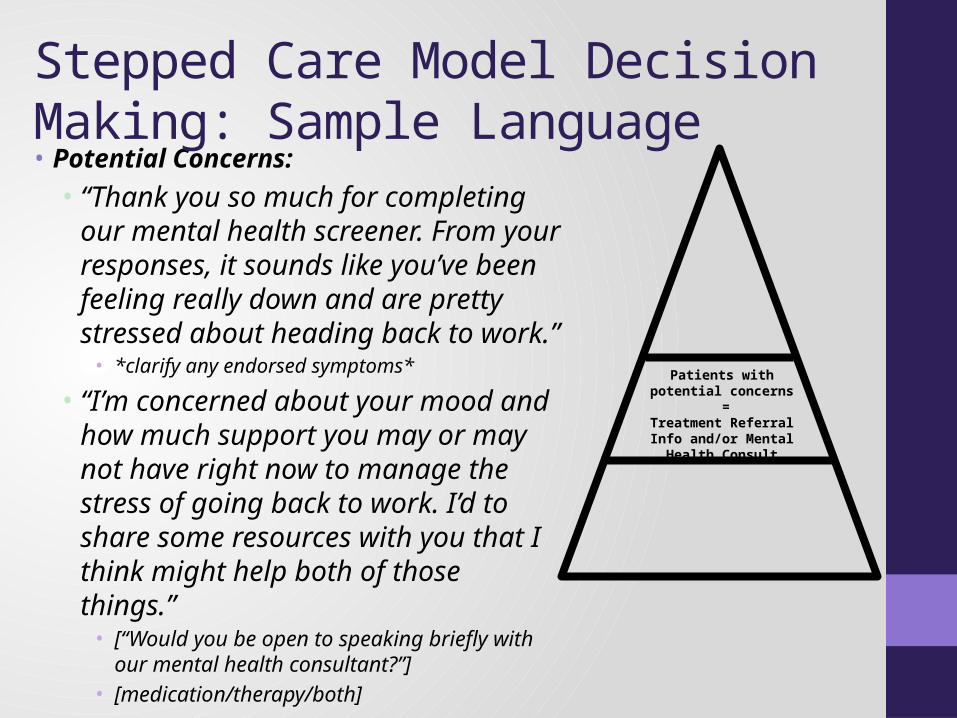
Patients with potential concerns
=Treatment Referral Info
and/or Mental Health Consult
• Potential Concerns:• “Thank you so much for completing
our mental health screener. From your responses, it sounds like you’ve been feeling really down and are pretty stressed about heading back to work.”
• *clarify any endorsed symptoms*
• “I’m concerned about your mood and how much support you may or may not have right now to manage the stress of going back to work. I’d to share some resources with you that I think might help both of those things.”
• [“Would you be open to speaking briefly with our mental health consultant?”]
• [medication/therapy/both]
Stepped Care Model Decision Making: Sample Language
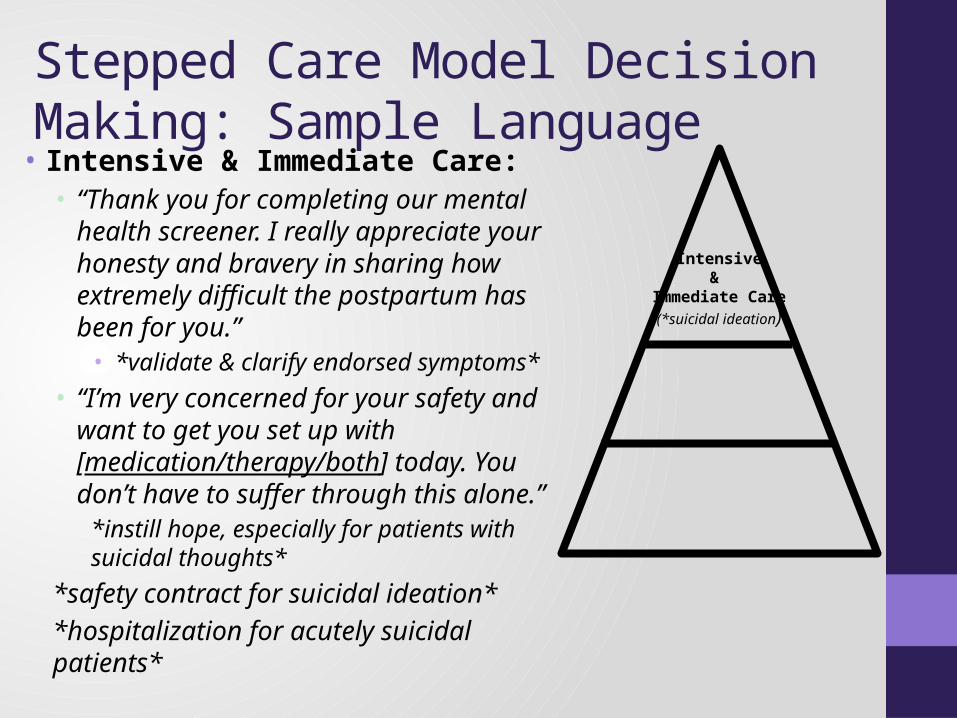
Intensive&
Immediate Care(*suicidal ideation)
• Intensive & Immediate Care:• “Thank you for completing our mental
health screener. I really appreciate your honesty and bravery in sharing how extremely difficult the postpartum has been for you.”
• *validate & clarify endorsed symptoms*• “I’m very concerned for your safety and
want to get you set up with [medication/therapy/both] today. You don’t have to suffer through this alone.”
*instill hope, especially for patients with suicidal thoughts*
*safety contract for suicidal ideation**hospitalization for acutely suicidal patients*
Stepped Care Model Decision Making: Sample Language
Acknowledgments• Dr. Stephen Lassen, Clinical Supervisor• Ms. Erin Smith, Research Assistant• University of Kansas Medical Center OBGYN Department & Staff
• Dr. Carl Weiner, Department Chair• KUMED OBGYN Attending Physicians & Residents
References1.Ayoola, A.B., Nettleman, M.D., Stommel, M., & Canady, R.B. (2010). Time of Pregnancy Recognition and Prenatal Care Use: A Population based Study in the United States. ‐ Birth, 37(1), 37-43.
2.Beck, A. T., & Steer, R. A. (1993). Beck Depression Inventory Manual. San Antonio, TX: The Psychological Corporation. Harcort Brace & Company.
3.Beck, C. T., & Gable, R. (2001). Further validation of the Postpartum Depression Screening Scale. Nurs Res, 50(3), 10.
4.Beck CT, Gable RK, Sakala C, Declercq ER. (2011). Posttraumatic stress disorder in new mothers: results from a two-stage U.S. national survey. Birth,38:216–227.
5.Bonello, Michelle R, Xu, Fenglian, Li, Zhuoyang, Burns, Lucy, Austin, Marie-Paule, & Sullivan, Elizabeth A. (2014). Mental and Behavioral Disorders Due to Substance Abuse and Perinatal Outcomes: A Study Based on Linked Population Data in New South Wales, Australia. International journal of environmental research and public health, 11(5), 4991-5005.
6.Chisolm, Margaret S, Acquavita, Shauna P, Kaltenbach, Karol, Winklbaur, Bernadette, Heil, Sarah H, Martin, Peter R, . . . Tuten, Michelle. (2011). Cigarette Smoking and Neonatal Outcomes in Depressed and Non-Depressed Opioid-Dependent Agonist-Maintained Pregnant Patients. Addictive disorders & their treatment, 10(4), 180.
7.Connelly, C. D., Hazen, A. L., Baker-Ericzen, M. J., Landsverk, J., & Horwitz, S. M. (2013). Is screening for depression in the perinatal period enough? The co-occurrence of depression, substance abuse, and intimate partner violence in culturally diverse pregnant women. J Womens Health (Larchmt), 22(10), 844-852. doi: 10.1089/jwh.2012.4121
8.Forray, A., Gotman, N., Kershaw, T., & Yonkers, K. A. (2014). Perinatal smoking and depression in women with concurrent substance use. Addict Behav, 39(4), 749-756. doi: 10.1016/j.addbeh.2013.12.008
9.Gjerdingen, Dwenda K, & Yawn, Barbara P. (2007). Postpartum depression screening: importance, methods, barriers, and recommendations for practice. The Journal of the American Board of Family Medicine, 20(3), 280-288.
10.Hanusa, B. H., Scholle, S. H., Haskett, R. F., Spadaro, K., & Wisner, K. L. (2008). Screening for depression in the postpartum period: a comparison of three instruments. J Womens Health (Larchmt), 17(4), 585-596. doi: 10.1089/jwh.2006.0248.
11.Miller ES, Chu C, Gollan J, Gossett DR. Obsessive-compulsive symptoms during the postpartum period. A prospective cohort. (2013). J Reprod Med,58:115–122.
12.Nystrom, K., & Ohrling, K. (2004). Parenthood experiences during the child's first year: literature review. J Adv Nurs, 46(3), 319-330. doi: 10.1111/j.1365-2648.2004.02991.x JAN2991 [pii]
13.O'Hara, M. W., & Swain, A.M. (1996). Rates and risk of postpartum depression – A meta-analysis 8:37–54, 1996. International Review of Psychiatry, 8, 18.
14.Sohr-Preston, S., & Scaramella, L. (2006). Implications of timing of maternal depressive symptoms for early cognitive and language development. Clin Child Fam Psychol Rev, 9(1), 19.
15.Spitzer, Robert L, Williams, Janet BW, Kroenke, Kurt, Hornyak, Raymond, & McMurray, Julia. (2000). Validity and utility of the PRIME-MD patient health questionnaire in assessment of 3000 obstetric-gynecologic patients: the PRIME-MD Patient Health Questionnaire Obstetrics-Gynecology Study. Am J Obstet Gynecol, 183(3), 759-769.
16.Stuart S, Couser G, Schilder K, O’Hara MW, Gorman L. (1998). Postpartum anxiety and depression: onset and comorbidity in a community sample. J Nerv Ment Dis, 186:420–424.
17.Sword, W., Busser, D., Ganann, R., McMillan, T., & Swinton, M. (2008). Women's care-seeking experiences after referral for postpartum depression. Qual Health Res, 18(9), 1161-1173. doi: 18/9/1161 [pii].10.1177/1049732308321736
18.Wenzel A, Haugen EN, Jackson LC, Brendle JR. (2005). Anxiety symptoms and disorders at eight weeks postpartum. J Anxiety Disord,19:295–311.
19.Wisner, K. L., Parry, B. L., & Piontek, C. M. (2002). Clinical practice. Postpartum depression. N Engl J Med, 347(3), 194-199. doi: 10.1056/NEJMcp011542347/3/194 [pii].
20.Vesga-Lopez O, Blanco C, Keyes K, Olfson M, Grant BF, Hasin DS. (2008). Psychiatric disorders in pregnant and postpartum women in the United States. Arch Gen Psychiatry, 65: 805–815.







