
La patologia valvolare
dell’anziano: problemi
decisionali complessi
Ottavio Alfieri
S.Raffaele University Hospital
Milan
61° CONGRESSO NAZIONALE SIGG, Napoli, 2016

Bulk of Population Growth
The Economist, May 14th 2011

Longevity

Nkomo, Lancet 2006

The Burden of Valve Disease
Survival
100
80
60
40
20
0
0 1 2 3 4 5 6 7 8
Su
rviv
al
(%)
Expected
Observed
P < 0.001
Years
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).
Treament of severe valve desease
has a favorable impact on survival
at any age

Frailty
Frailty is a Phenotype
Physical Function Fatigue
Weakness Muscle Wasting
Limited Life Space Isolation
Cognition Depression
Nutrition Weight Loss
Comorbidity (>2 conditions)
Disability (>1 ADL) 25% 66%
27%
Courtesy Karen Alexander

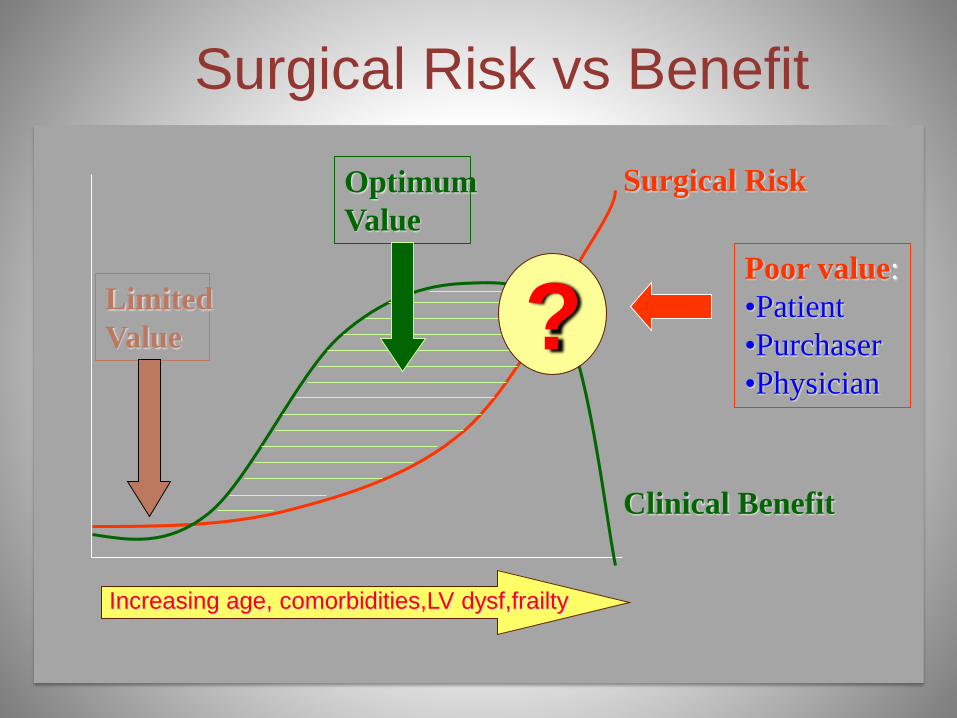
Poor value:
•Patient
•Purchaser
•Physician
Optimum
Value
Surgical Risk
Clinical Benefit
Limited
Value ?
Increasing age, comorbidities,LV dysf,frailty
Surgical Risk vs Benefit

Guidelines on the management of valvular heart
disease (version 2012)The Joint Task Force on the Management of Valvular Heart Disease of the European Society of
Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)
Authors/Task Force Members: Alec Vahanian (Chairperson) (France), Ottavio Alfieri (Chairperson) (Italy),
Felicita Andreotti (Italy), Manuel J. Antunes (Portugal), Gonzalo Barón-Esquivias (Spain), Helmut Baumgartner
(Germany), Michael Andrew Borger (Germany),Thierry P. Carrel (Switzerland), Michele De Bonis (Italy),
Arturo Evangelista (Spain), Volkmar Falk (Switzerland), Bernard Iung (France), Patrizio Lancellotti (Belgium),
Luc Pierard (Belgium), Susanna Price (UK), Hans-Joachim Schäfers (Germany), Gerhard Schuler (Germany),
Janina Stepinska (Poland), Karl Swedberg (Sweden), Johanna Takkenberg (The Netherlands), Ulrich Otto Von
Oppell (UK), Stephan Windecker (Switzerland), Jose Luis Zamorano (Spain), Marian Zembala (Poland)
ESC Committee for Practice Guidelines (CPG): Jeroen J. Bax (Chairperson) (The Netherlands), Helmut Baumgartner (Germany), Claudio
Ceconi (Italy), Veronica Dean (France), Christi Deaton (UK), Robert Fagard (Belgium), Christian Funck-Brentano (France), David Hasdai
(Israel), Arno Hoes (The Netherlands), Paulus Kirchhof (United Kingdom), Juhani Knuuti (Finland), Philippe Kolh (Belgium),
Theresa McDonagh (UK), Cyril Moulin (France), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Udo Sechtem (Germany),
Per Anton Sirnes (Norway), Michal Tendera (Poland), Adam Torbicki (Poland), Alec Vahanian (France), Stephan Windecker (Switzerland)
Document Reviewers: Bogdan A. Popescu (ESC CPG Review Coordinator) (Romania), Ludwig Von Segesser (EACTS).
Review Coordinator) (Switzerland), Luigi P. Badano (Italy), Matjaž Bunc (Slovenia), Marc J. Claeys (Belgium), Niksa Drinkovic (Croatia),
Gerasimos Filippatos (Greece), Gilbert Habib (France), A. Pieter Kappetein (The Netherlands), Roland Kassab (Lebanon), Gregory Y.H. Lip
(UK), Neil Moat (UK), Georg Nickenig (Germany), Catherine M. Otto (USA), John Pepper, (UK), Nicolo Piazza (Germany),
Petronella G. Pieper (The Netherlands), Raphael Rosenhek (Austria), Naltin Shuka (Albania), Ehud Schwammenthal
(Israel), Juerg, Schwitter (Switzerland), Pilar Tornos Mas (Spain), Pedro T.Trindade (Switzerland), Thomas Walther (Germany).
European Heart Journal
doi:10.1093/eurheartj/ehs109
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

Treatment of Valve
disease
SURGEONSCARDIOLOGISTS
Imaging specialists (Echo, CT, MRI)
Anesthesiologists
The « Heart Team »
Other specialists:
Geriatricians ……

Heart Team
• Complexity of the disease
• Complexity of the patient
• Expansion of the therapeutic options


Essential questions in the evaluationof a patient for valvular intervention
• Is valvular heart disease severe?
• Does the patient have symptoms?
• Are symptoms related to valvular disease?
• What are patient life expectancy and expected quality of life?
• Do the expected benefits of intervention (versus spontaneous
outcome) outweigh its risks?
• What are the patient's wishes?
• Are local resources optimal for planned intervention?
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

Aetiologies of Single Valvular Heart Diseasesin the Euro Heart Survey
Iung et al. Eur Heart J 2003;24:1244-53
0%
20%
40%
60%
80%
100%
Other
Ischemic
Congenital
Inflammatory
Endocarditis
Rheumatic
Degenerative
AS
43%
AR
13%
MR
32%
MS
12%
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).
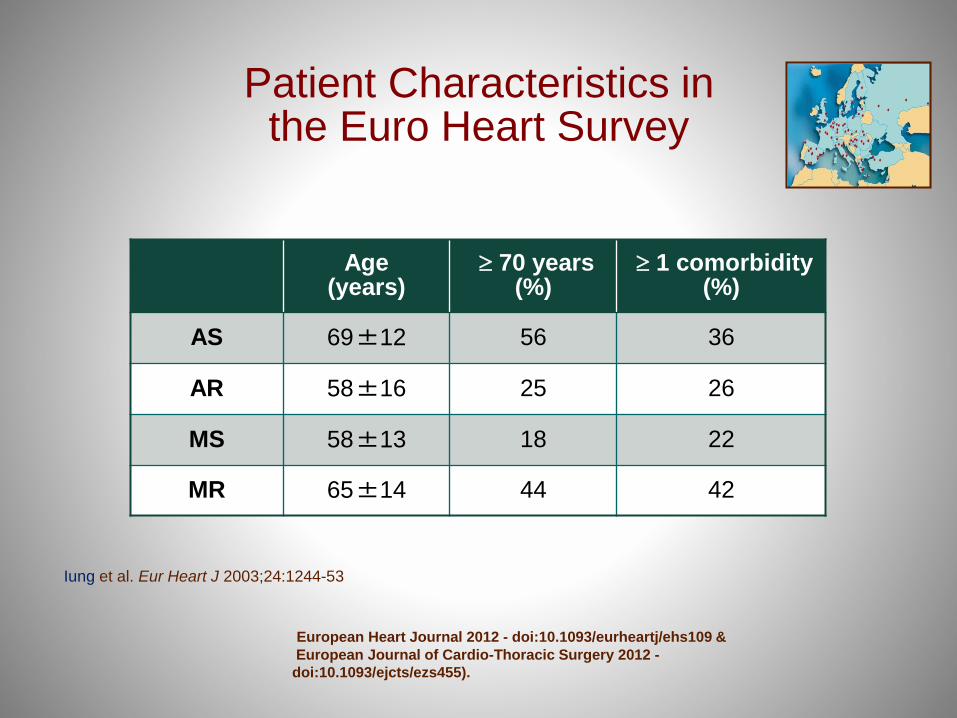
Patient Characteristics inthe Euro Heart Survey
Age(years)
70 years(%)
1 comorbidity(%)
AS 69±12 56 36
AR 58±16 25 26
MS 58±13 18 22
MR 65±14 44 42
Iung et al. Eur Heart J 2003;24:1244-53
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).
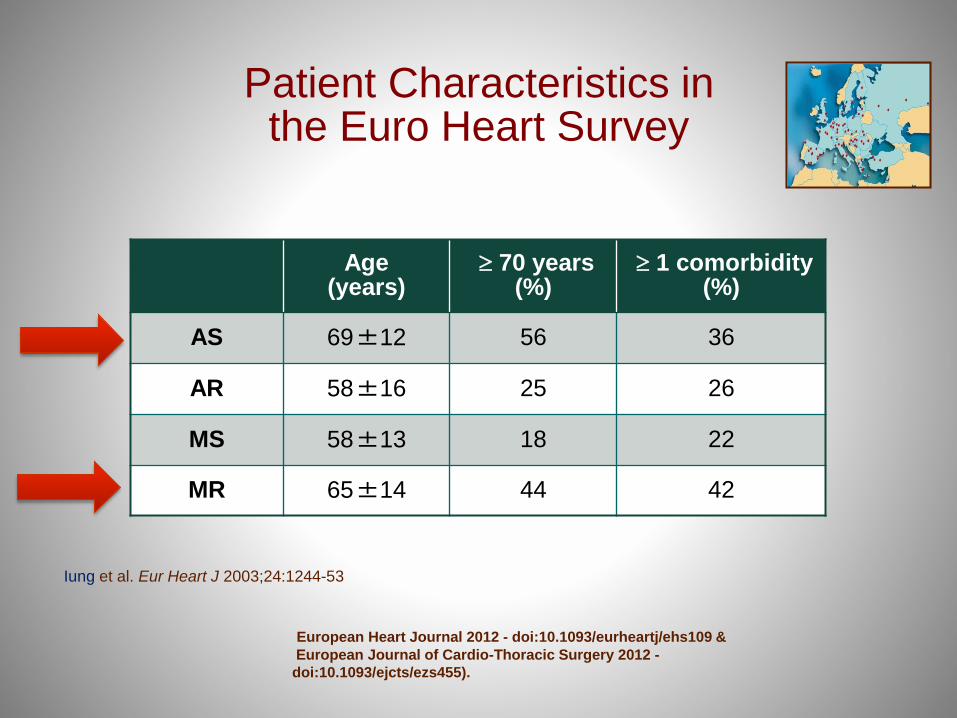
Patient Characteristics inthe Euro Heart Survey
Age(years)
70 years(%)
1 comorbidity(%)
AS 69±12 56 36
AR 58±16 25 26
MS 58±13 18 22
MR 65±14 44 42
Iung et al. Eur Heart J 2003;24:1244-53
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

Aortic Stenosis 75 years
(n=398)
No Severe AS
(n=114)
Severe AS
(n=284)
No Symptoms
(n=68)
Symptoms
(n=216)
Intervention
(n=144) 67%
No Intervention
(n=72) 33%
Current Management of Severe SymptomaticAS in the Elderly
Iung et al. Eur Heart J 2005;26:2714-2720
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

Isolated MR > 75 years
(n=887)
No Severe MR
(n=347)
Severe MR
(n=540)
No Symptoms
(n=144)
Symptoms
(n=396)
Intervention
(n=203) 51%
No Intervention
(n=193) 49%
Current Managementof Severe MR
Mirabel et al. Eur Heart J 2007;28:1358-1365
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

Sources: 1 S.J. Lester et al., “The Natural History and Rate of Progression of Aortic
Stenosis,” Chest 1998
2 C.M. Otto, “Valve Disease: Timing of Aortic Valve Surgery,” Heart 2000
Chart: Ross J Jr, Braunwald E. Aortic stenosis. Circulation. 1968;38 (Suppl 1):61-7.
…Aortic stenosis is life-threatening and
progresses rapidly…
40 50 60 70 800
20
40
60
80
100
Age
Years
Survival
Percent Onset
severe
symptoms
Avg. survival
Years
Angina
Syncope
Failure
Latent
Period
(Increasing
Obstruction,
Myocardial
Overload)
0 2 4 6

LIFE EXPECTANCY AFTER AVR
Life expectancy for men in normal populations versus life expectancy after
implantation of a prosthetic valve
0
5
10
15
20
25
30
35
45 50 55 60 65 70 75 80
Age (yrs)
Life e
xpecta
ncy (
yrs
)
LE normal BC population
LE normal Dutch population
LE normal UK population
LE normal US population
LE (US) with MECH
LE (US) with BIO
Patient outcome after AVR with mechanical or bioprostheses: weighing lifetime anticoagulant-related event risk against reoperation
risk Martijn W.A. van Ge§ldorp1, W.R. Eric Jamieson2, Jian Ye2, Guy J. Fradet2, A. Pieter Kappetein1, Marinus J.C. Eijkemans3, Gary
L. Grunkemeier4, Ad J.J.C. Bogers1, Johanna J.M. Takkenberg1
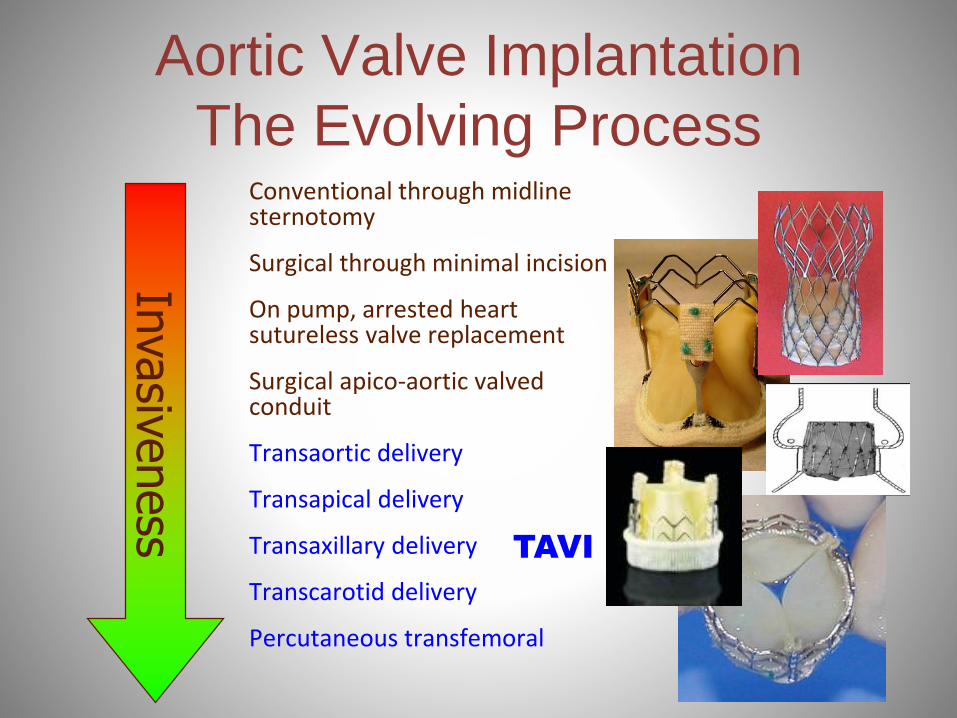
Aortic Valve Implantation
The Evolving ProcessConventional through midline sternotomy
Surgical through minimal incision
On pump, arrested heart sutureless valve replacement
Surgical apico-aortic valved conduit
Transaortic delivery
Transapical delivery
Transaxillary delivery
Transcarotid delivery
Percutaneous transfemoral
Invasiveness
TAVI

Ruiz et al. J Am Coll Cardiol. July 14,
2015,66(2):169-183
TAVI OPTIONS

Indications for transcatheter aortic valve
implantationClass Level
TAVI should only be undertaken with a multidisciplinary “heart team” including
cardiologists and cardiac surgeons and other specialists if necessary.I C
TAVI should only be performed in hospitals with cardiac surgery on-site. I C
TAVI is indicated in patients with severe symptomatic AS who are not suitable for
AVR as assessed by a “ heart team” and who are likely to gain improvement in their
quality of life and to have a life expectancy of more than 1 year after consideration
of their comorbidities.
I B
TAVI should be considered in high risk patients with severe symptomatic AS who
may still be suitable for surgery, but in whom TAVI is favoured by a “heart team”
based on the individual risk profile and anatomic suitability.IIa B
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

Published April 2012


Published April 2012
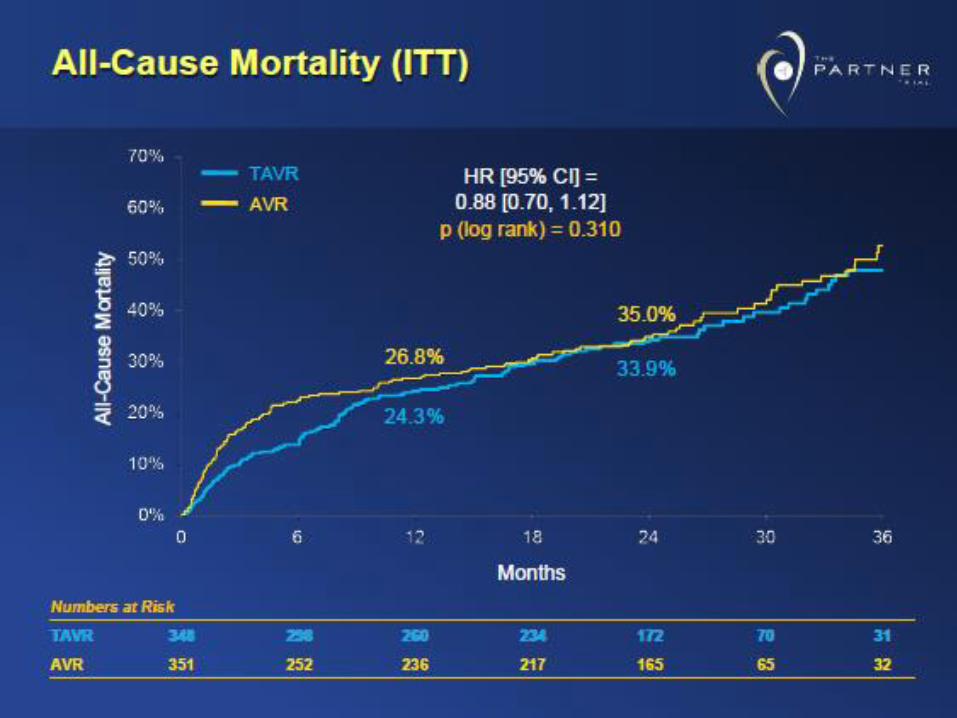

US CoreValve High-Risk Trial
2014


All-Cause Mortality STS ≤7%
312015


Transfemoral rather than
Transapical

Procedural Recovery Non-procedure related
Gaudiani et al. presented at the AATS, 2016
Alec Vahanian MD,Bichat Hospital, Paris,University Paris VII
Performance
Safety (mortality ,stroke)
Vascular complications
Perivalvular leaks
Conduction defects
Durability
Alec Vahanian MD,Bichat Hospital, Paris,University Paris VII
Surgical AVR will be limited to contraindications to TAVI
and to pts requiring combined cardiac or aortic surgery


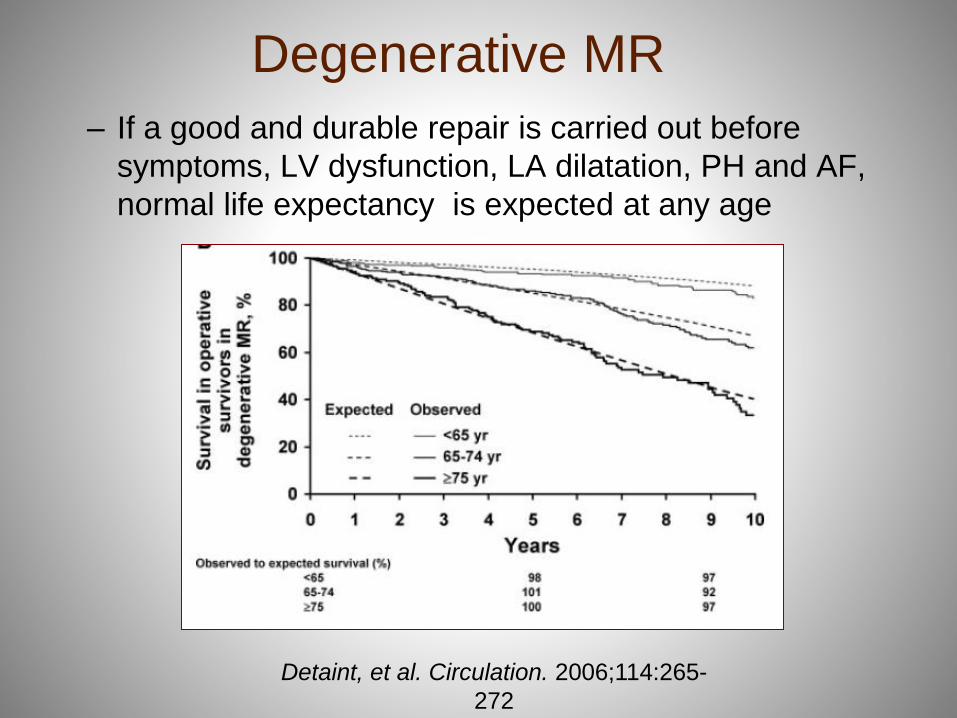
– If a good and durable repair is carried out before
symptoms, LV dysfunction, LA dilatation, PH and AF,
normal life expectancy is expected at any age
Detaint, et al. Circulation. 2006;114:265-
272
Degenerative MR

Neochord Inc.


Mitra Clip
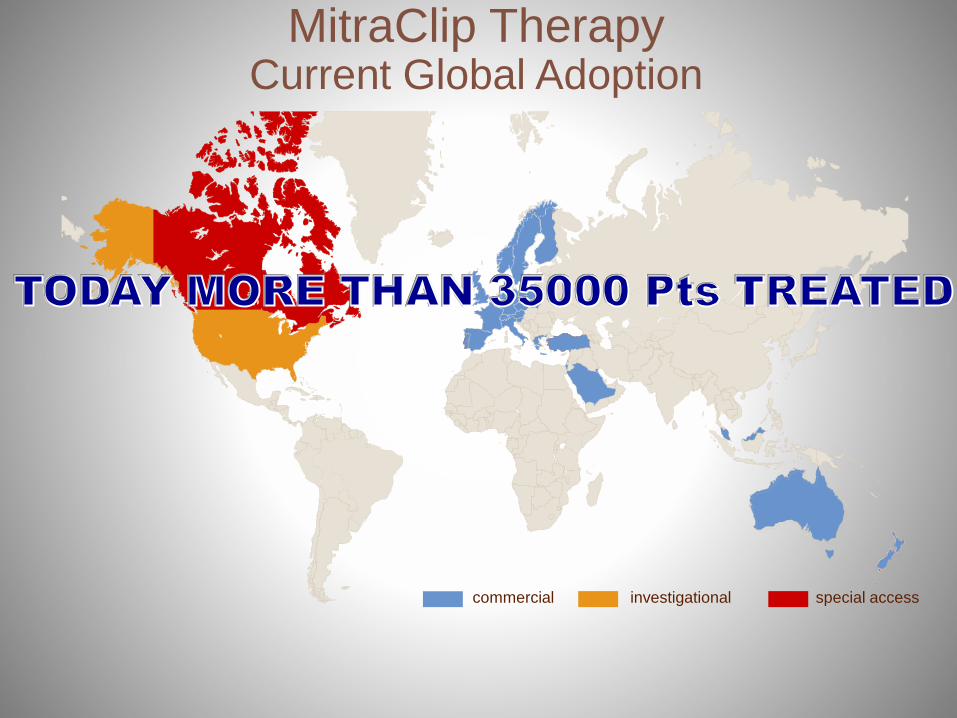
MitraClip Therapy Current Global Adoption
investigational special accesscommercial

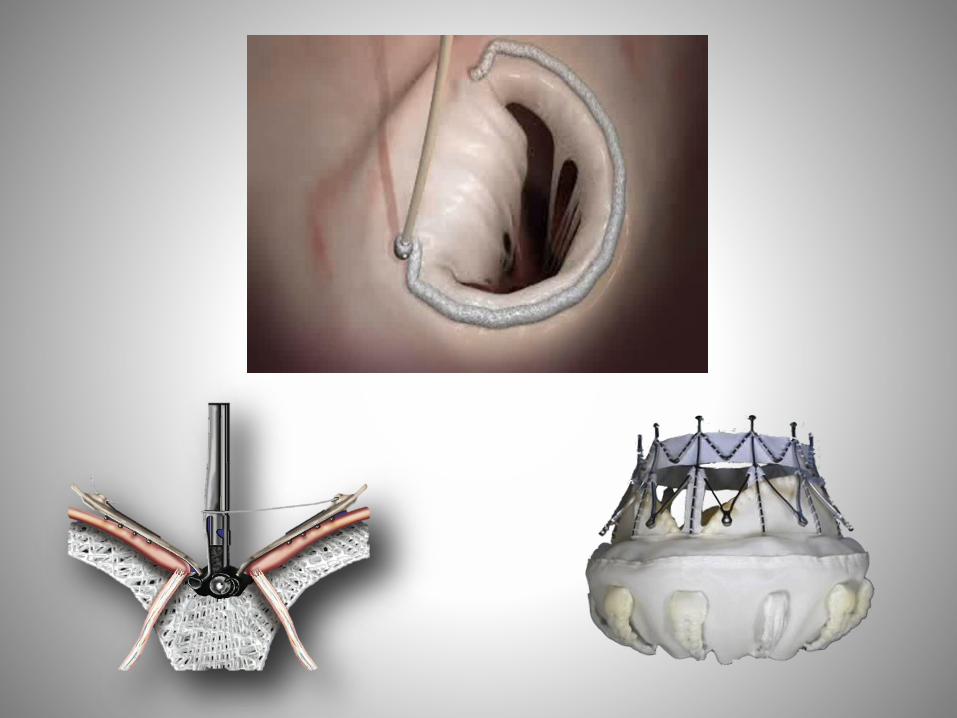
Transcatheter Annuloplasty
Coronary sinus remodeling
SL dimensions cinching
RF/Ultrasound remodeling
External compression
Direct annuloplasty
How Does Cardioband Work?
48

Fully Percutaneous Mitral Repair

Transcatheter Mitral Valve Replacement
CardiAQ Tendyne Tiara
Fortis Cephe
a
Cardiovalve High Life
Twelve

Tiara case done in San Raffaele
Fully successful case perform in less than 40 min
/
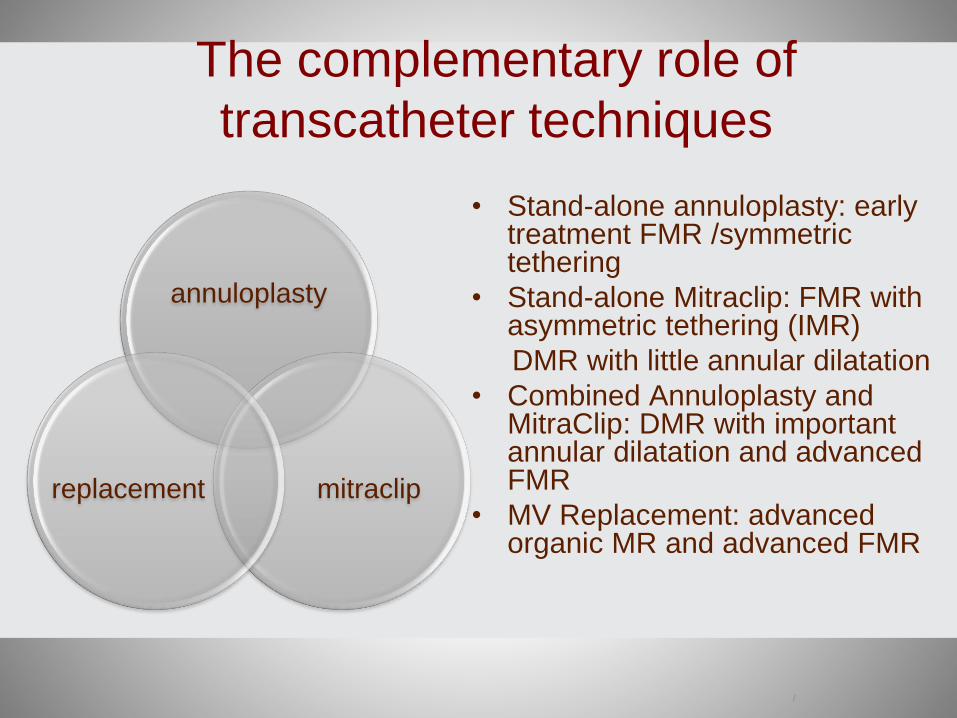
• Stand-alone annuloplasty: earlytreatment FMR /symmetrictethering
• Stand-alone Mitraclip: FMR with asymmetric tethering (IMR)
DMR with little annular dilatation
• Combined Annuloplasty and MitraClip: DMR with importantannular dilatation and advancedFMR
• MV Replacement: advancedorganic MR and advanced FMR
The complementary role of
transcatheter techniques
annuloplasty
mitraclipreplacement







