Download - Connecting People Intervention
Policy context
Social Exclusion Unit report on mental health (2004)
• Initiated current direction towards social inclusion in mental health services
• Importance of community participation and strong networks
• Policy implementation led by National Social Inclusion Programme, headed by Prof David Morris
Policy context
The Big Society (2010)
•Give communities more power
•Encourage people to take an active role in their communities
•Transfer power from central to local government
•Support co-ops, mutuals, charities and social enterprises
•Publish government data
Policy contextMental health strategy (2011)
1. More people will have good mental health
2. More people with mental health problems will recover
3. More people with mental health problems will have good physical health
4. More people will have a positive experience of care and support
5. Fewer people will suffer avoidable harm
6. Fewer people will experience stigma and discrimination
Policy context
RSA Connected Communities (2010)
•An example of an initiative which links policy agendas
•Investigates how services can mobilise networks to support people
•Explores how solutions can be co-produced external to services
•Connecting People Intervention is the inverse – facilitating services to be more outward-facing
Theoretical contextEconomic capital: Resources that can be used to produce financial gains (Marx, 1867)
Cultural capital: Information resources and socially valued assets, e.g. knowledge of the arts, music or literature (Bourdieu, 1997)
Human capital: Qualifications, training and work experience (Becker 1964)
Social capital: Sum of resources (actual or potential) that accrue to a person or group from access to a network of relationships or membership in a group (Bourdieu, 1997)
Community capital: Combination of capitals within a defined area or community, required to help people fulfil their potential (Hancock, 2001)
Erotic capital: Beauty, sex appeal, charm, liveliness, presentation (Hakim, 2010)
Theoretical context
1. Provision of information• about the most effective interventions or health behaviours• about job opportunities or other ways of enhancing socio-economic position
and quality of life2. Additive effect of resources
• power and authority of network members may add to an individual’s power and social status to effect exposure and vulnerability to health risks
• neo-material gains of network resources3. Social credentials
• direct intervention of network members in health care4. Maintenance of subjective social status
• Network resources could mitigate against loss of personal resources. Shared resources maintain identification with a social group
Empirical context
Wealth, power and status of network members can benefit other individuals in that network (Lin 2001)
Informal social networks are influential in helping unemployed people find work (Perri 6 1997)
Social capital helps reemployment (Sprengers et al 1988) and has an effect on income (Boxman et al 1991)
Social capital is positively associated with current occupational status (Flap & Volker 2001)
Social capital can lead to greater occupational prestige, income and political influence when mobilised (Lin & Erickson 2008)
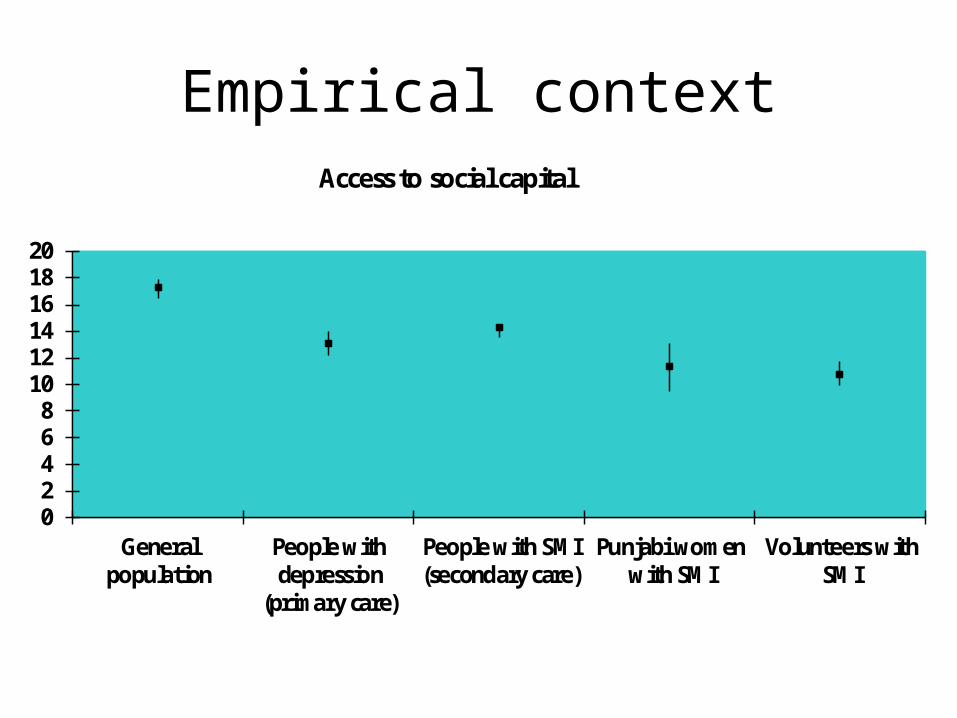
Empirical context
02468
101214161820
Generalpopulation
People withdepression
(primary care)
People with SMI(secondary care)
Punjabi womenwith SMI
Volunteers withSMI
Access to social capital
Empirical context
There is a cross-sectional inverse association between trust and common mental disorders (de Silva et al 2005); and between access to social capital and depression (Webber & Huxley 2007; Song & Lin 2009)
Social capital is associated with improvements in quality of life, though insecure attachment styles pose a barrier to people with depression accessing their social capital (Webber 2011)
High levels of trust lower the risk of depression (Fujiwara & Kawachi 2008)Low workplace social capital increases the risk of depression (Kouvonen et al 2008)
Empirical context
• Incidence of schizophrenia in ethnic minorities is related to percentage of ethnic minorities in the area (Boydell et al 2001)• In areas 28-60% ethnic minorities = 2.4• In areas 13-28% ethnic minorities = 3.6• In areas 8-12% ethnic minorities = 4.4
• Ethnic density effect in schizophrenia has been confirmed in a study using smaller areas (Schofield 2010)
• Cumulative social disadvantage is associated with increased risk of psychosis in Black Caribbean men (Morgan 2008)
• Social hostility or racism can’t explain excess of psychosis in Black Caribbean men in comparison with Asian men.
• Is social capital a buffer to adversity and has a protective role in terms of mental health?
Practice context
NICE Guidelines for Schizophrenia (2009) social interventions:
• family interventions• social skills training• vocational rehabilitation
(nothing about connecting people or engaging with local communities)
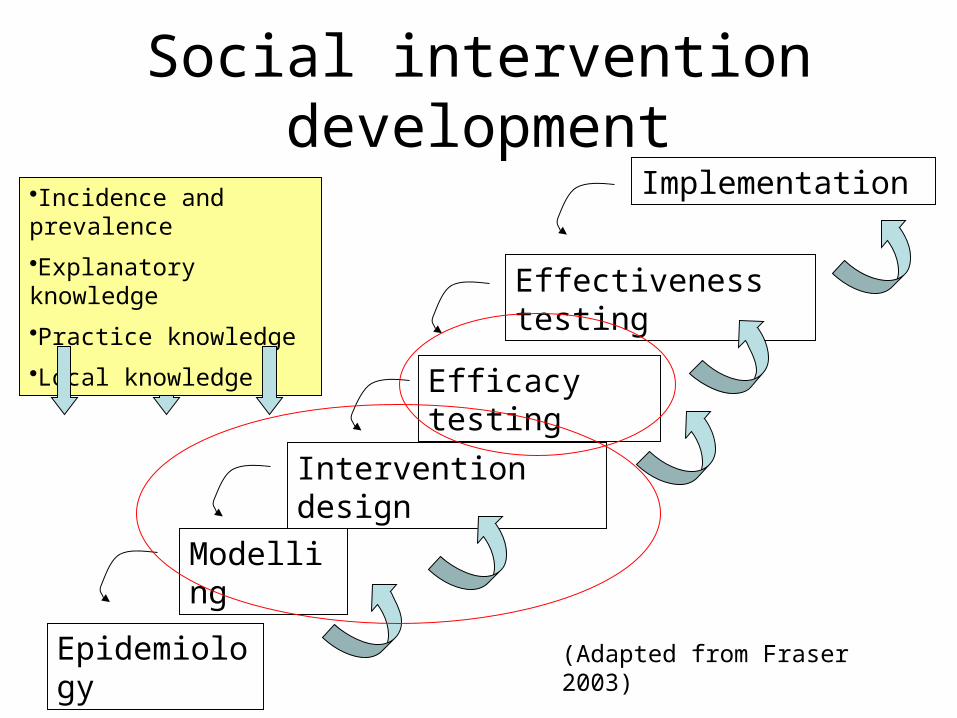
Social intervention development
Epidemiology
Modelling
Intervention design
Efficacy testing
Effectiveness testing
Implementation•Incidence and prevalence
•Explanatory knowledge
•Practice knowledge
•Local knowledge
(Adapted from Fraser 2003)
Method
• Combinative ethnography of social care practice• Semi-structured interviews, observations of practice and focus groups• Exploratory, not evaluative
• Setting: 1. NHS mental health services (mental health professionals and support
time & recovery workers in early intervention in psychosis teams, social inclusion and recovery services)
2. Housing support (supported housing & floating support workers)
3. Third sector (social enterprises, voluntary organisations)• Sample
150 workers, service users, managers, commissioners
Method
Ethnography phase 1Researcher interviews, observes, and holds focus groups with agency
workers, service users and carers to discuss the practice of enhancing service user social participation
Ethnography phase 2:New questions emerging from phase 1 was the focus of phase 2 through
further discussion and conceptualisation of practice Changes in service users from phrase 1 were reflected
Delphi ConsultationIntervention model was developed and revised in liaison with project’s
advisory group and a wider group of stakeholders (incorporating service users, carers, practitioners and researchers)
MethodSystematic Reviews (x3)
Aims: to systematically identify, and evaluate the quality, of the research literature on health and social care interventions that promote the social participation and well-being of adults with a learning disability or mental health problem
1. adults with a learning disability2. adults with a mental health problem3. older adults (+65) with a functional mental health problem
• EPPI Centre Methodology• Data synthesis and quality appraisal grouped by study design to capture
quantitative and qualitative results• Inter-rater reliability at each stage
MethodFidelity measure development
Fidelity measurement is required to answer question: how do you know that the intervention made a difference and not something else?
The Connecting People Intervention Fidelity Scale (CPIFS) will measure variation in fidelity to the intervention model at an individual level (to capture expected variation in practice at the individual worker level)
Inherently complex due to personalised nature of interventions; main focus will be on fidelity to intervention model
Items refined in Delphi Consultation; psychometric properties evaluated in pilot study
MethodQuasi-experimental study to pilot intervention
• Intervention model adapted for use with adults with learning disabilities and older adults with mental health problems
• Scoping study identifies about 15 agencies who are willing and able to implement intervention in the three social care user groups
• 3-day intervention training provided to each agency• 240 new referrals are interviewed at baseline and 12-month follow-up
Outcomes being measured:• Social participation (SCOPE, Huxley et al 2012)• Well-being (WEMWBS, Tennant et al 2007)• Access to social capital (RG-UK, Webber & Huxley 2007)
MethodQuasi-experimental study to pilot intervention
Potential confounding factors:• Socio-demographics• Attachment style (RQ, Bartholomew & Horowitz 1991)• Life events (RLEQ, Norbeck 1984)
Hypothesis: Higher fidelity to CPI will be associated with improved outcomes
Economic evaluation:• Service use (CSRI, Beecham et al 2001)• EQ-5D (EuroQOL 1990)• ICECAP-A (Al-Janabi & Coast 2009)
Process evaluation will involve qualitative interviews with service users, workers and managers
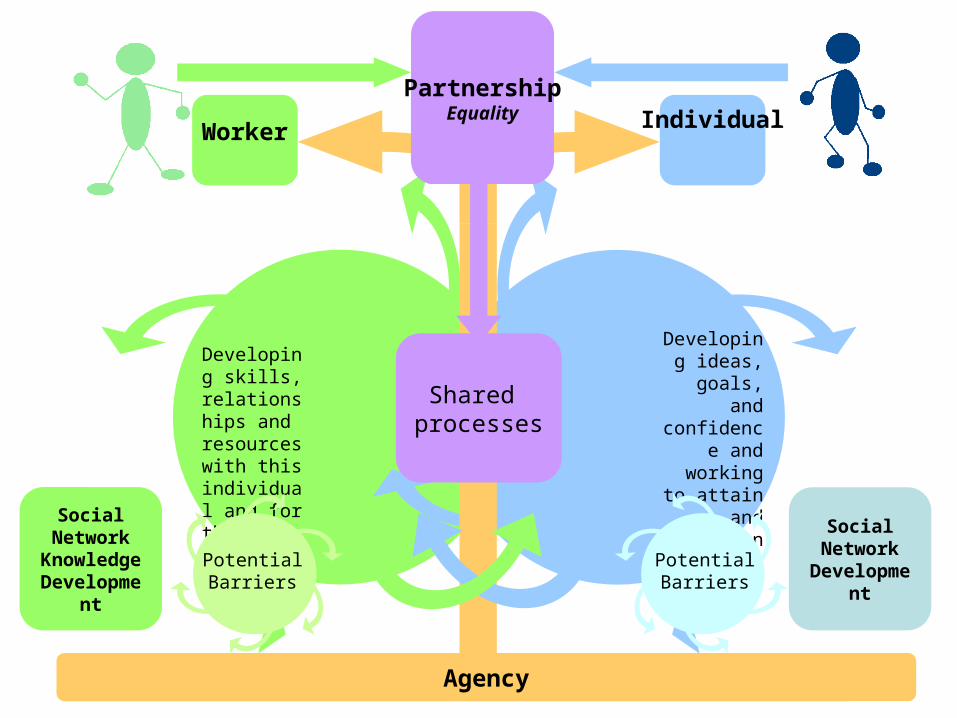
Social Network
Knowledge Development
Social Network
Development
Worker IndividualPartnership
Equality
Agency
Developing skills, relationships and resources with this individual and for the future
Shared processes
Developing ideas, goals,
and confidence
and working to attain and
expand on these
PotentialBarriers
PotentialBarriers
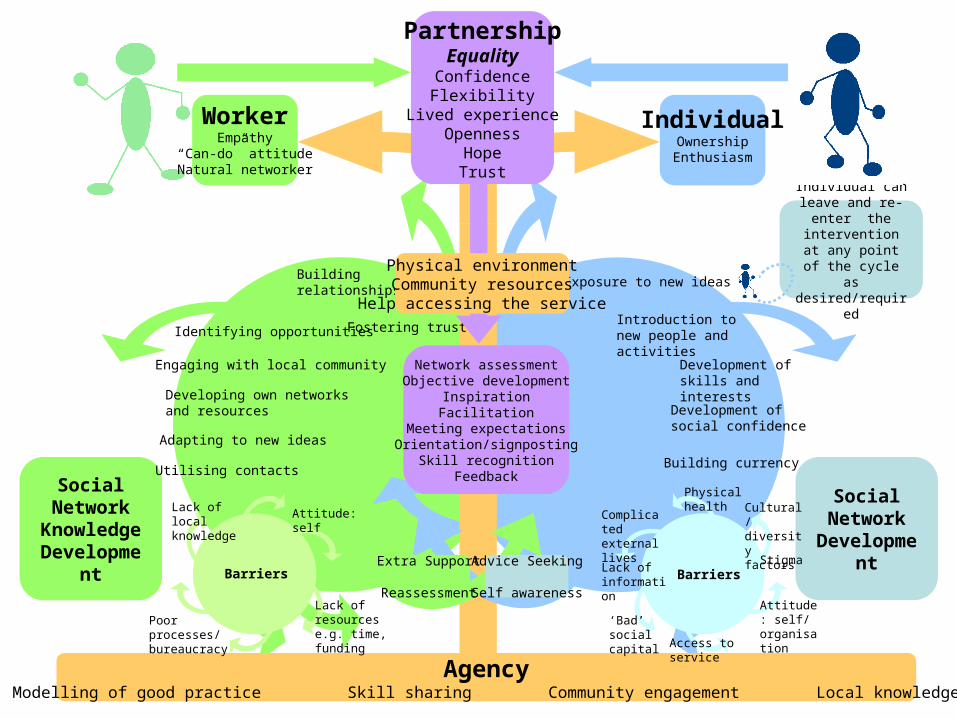
Individual can leave and re-enter the
intervention at any point of the cycle as
desired/required
Social Network
Knowledge Development
Social Network
Development
Network assessmentObjective development
InspirationFacilitation
Meeting expectationsOrientation/signposting
Skill recognitionFeedback
Adapting to new ideas
Utilising contacts
Buildingrelationships
Fostering trust
Developing own networksand resources
Engaging with local community
Identifying opportunitiesIntroduction to new people and activities
Development ofskills and interests
Building currency
Exposure to new ideas
Development ofsocial confidence
WorkerEmpathy
“Can-do” attitudeNatural networker
IndividualOwnershipEnthusiasm
PartnershipEquality
ConfidenceFlexibility
Lived experienceOpenness
HopeTrust
AgencyModelling of good practice Skill sharing Community engagement Local knowledge
Advice Seeking
Self awareness
Extra Support
Reassessment
Physical environmentCommunity resources
Help accessing the service
Physical health
Attitude: self/ organisation
Lack of information
Access to service
Stigma
‘Bad’ social capital
Complicated external lives
Barriers
Cultural/ diversity factors
Barriers
Attitude: self
Lack of resources e.g. time, funding
Poor processes/ bureaucracy
Lack of local knowledge
Individual can leave and re-enter the
intervention at any point of the cycle as
desired/required
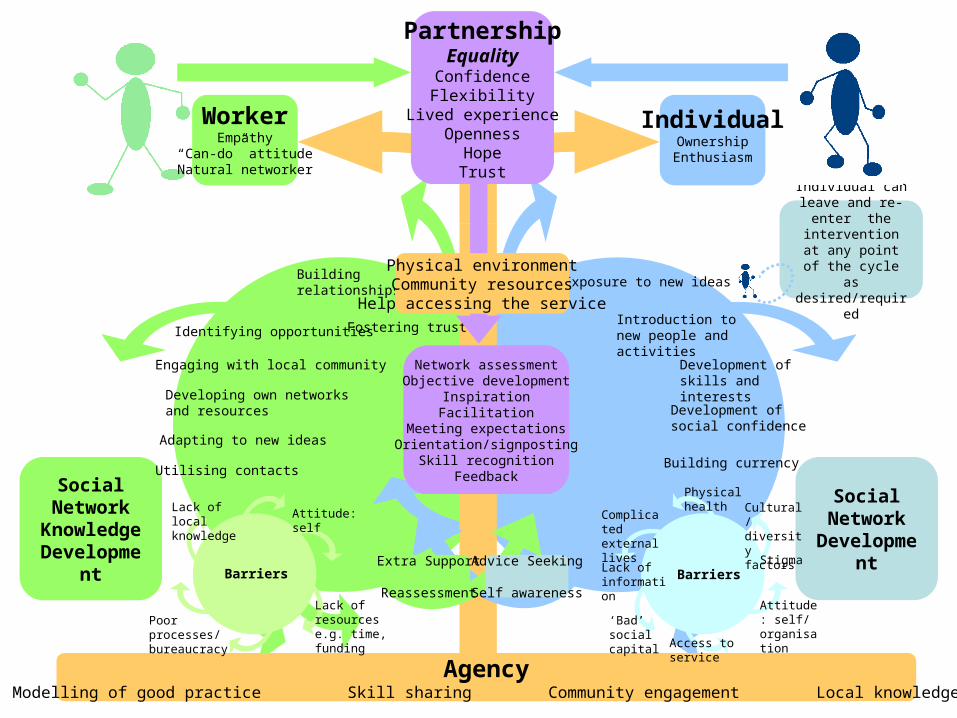
Social Network
Knowledge Development
Social Network
Development
Network assessmentObjective development
InspirationFacilitation
Meeting expectationsOrientation/signposting
Skill recognitionFeedback
Adapting to new ideas
Utilising contacts
Buildingrelationships
Fostering trust
Developing own networksand resources
Engaging with local community
Identifying opportunitiesIntroduction to new people and activities
Development ofskills and interests
Building currency
Exposure to new ideas
Development ofsocial confidence
WorkerEmpathy
“Can-do” attitudeNatural networker
IndividualOwnershipEnthusiasm
PartnershipEquality
ConfidenceFlexibility
Lived experienceOpenness
HopeTrust
AgencyModelling of good practice Skill sharing Community engagement Local knowledge
Advice Seeking
Self awareness
Extra Support
Reassessment
Physical environmentCommunity resources
Help accessing the service
Physical health
Attitude: self/ organisation
Lack of information
Access to service
Stigma
‘Bad’ social capital
Complicated external lives
Barriers
Cultural/ diversity factors
Barriers
Attitude: self
Lack of resources e.g. time, funding
Poor processes/ bureaucracy
Lack of local knowledge
The Practice Guidance

Thank youPlease do not hesitate to contact us for further information.
www.connectingpeoplestudy.net
https://www.facebook.com/pages/Connecting-People-Study/224658480937124







