
Mark Ferguson, M.D.
Seattle Children’s Hospital
University of Washington
Congenital Aortic Anomalies

16 mo with chronic cough

16 mo with chronic cough

Which vessel configuration is LEAST likely based on the
preceding images?
1. Right aortic arch with an aberrant left subclavian artery
2. Pulmonary sling
3. Double aortic arch
4. Left arch with an aberrant right
subclavian artery
Question 1

Which vessel configuration is LEAST likely based on the
preceding images:
1. Right aortic arch with an aberrant left subclavian artery
2. Pulmonary sling
3. Double aortic arch
4. Left arch with an aberrant right
subclavian artery
Answer 1

Double Aortic Arch

Double Aortic Arch

During embryonic vascular development, which aortic/branchial
arch contributes to the normal left-sided aortic arch?
1. II arch
2. III arch
3. IV arch
4. VI arch
Question 2
During embryonic vascular development, which aortic/branchial
arch contributes to the normal left-sided aortic arch?
1. II arch
2. III arch
3. IV arch
4. VI arch
Answer 2

Aortic Arch Development
Third arches: carotid arteries
Fourth arches: aortic arch (AA) on the left side, BCA on right
Sixth arches: right & left PA’s and the ductus arteriosus (DA) Seventh intersegmentals: subclavian arteries First, second, and fifth arches involute.
Based on Edwards’ hypothetical embryonic double aortic arch model

Normal Arch Development
Double Arch Development

Anatomy:
• double arches encircle the esophagus and
trachea (most common vascular ring)
• various forms, most commonly right arch is
dominant with a more superior apex and
descending aorta on the left
Epidemiology:
• vascular rings comprise 1% of surgically
managed cardiovascular malformations
(about half of those are double arches)
• no gender or race predilection
Double Aortic Arch
Clinical presentation:
• respiratory difficulties like stridor but also
including apparent life-threating events
• dysphagia, vomiting, choking, usually >2 yrs of age
Associations:
• usually without other cardiovascular anomalies
• 20% have chromosome band 22q11 deletion
Double Aortic Arch

Imaging:
• Chest Radiographs - may show indentation of trachea
or indeterminate arch sidedness
• Esophagram - bilateral and posterior indentation of
esophagus
• CT - anatomy, determine dominant arch for surgical
planning (contralateral thoracotomy),
evaluate airway compression
• MRI - anatomy, as CT
Double Aortic Arch

Right Aortic Arch with Aberrant Left Subclavian Artery
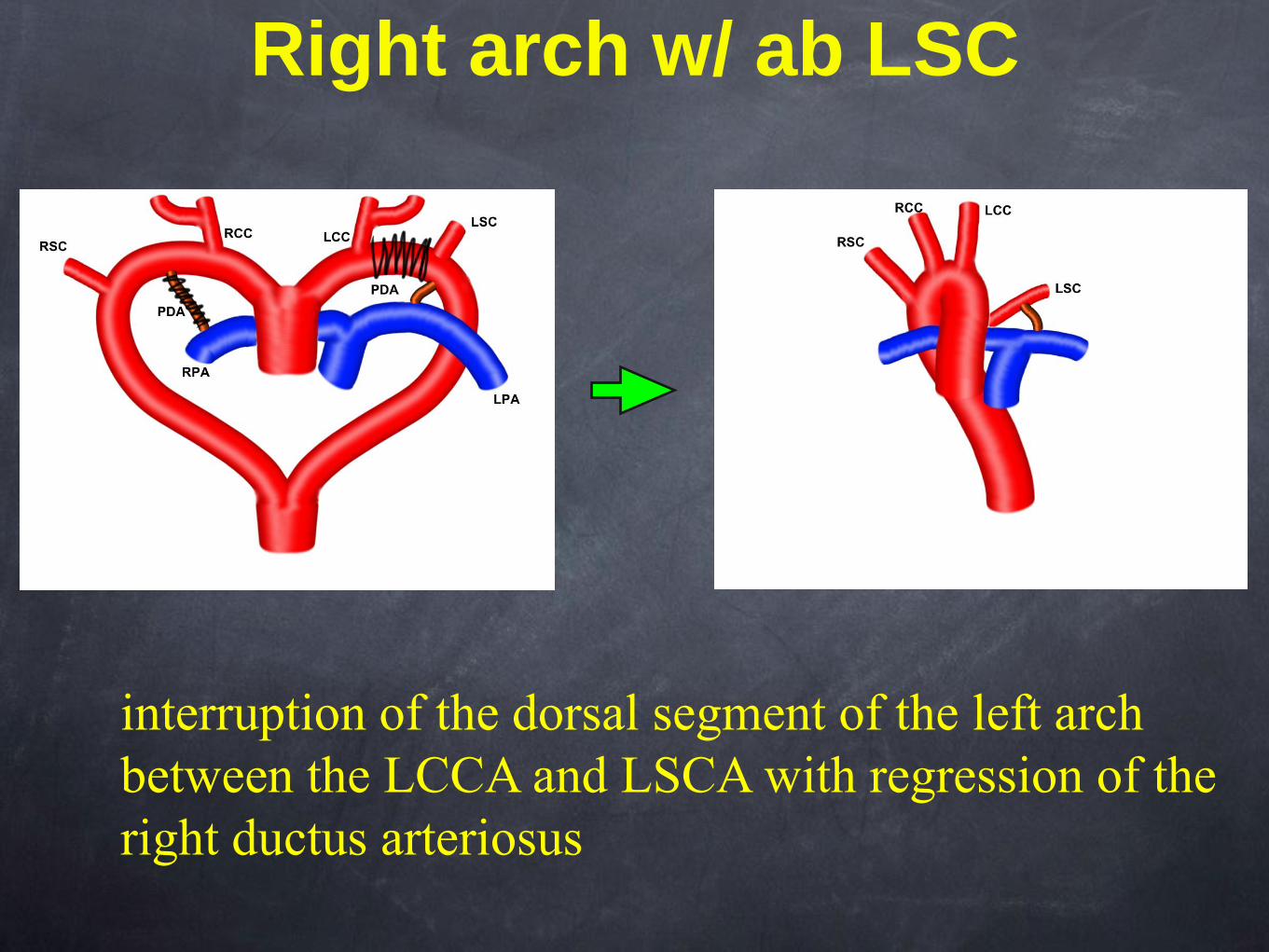
Right arch w/ ab LSC
interruption of the dorsal segment of the left arch
between the LCCA and LSCA with regression of the
right ductus arteriosus

• left ligamentum arteriosum can form a vascular ring
• Kommerell’s diverticulum - remnant of left dorsal
aortic root
• can be associated with a midline descending aorta
• Two major regions of potential airway compression
1. level of arch and ab subclavian artery
2. level of carina or main bronchi
Right Aortic Arch w/ ab LSC

9 yo with headaches

Aortic Coarctation
Focal Long Segment w/ Collaterals

Question 3
Which of the following is a characteristic of aortic coarctation?
1. Reverse figure-of-three sign on frontal chest radiograph
2. Associated with berry aneurysms of the circle of Willis
3. First and second rib notching secondary to collateral vessels
4. Right ventricular hypertrophy

Answer 3
Which of the following is a characteristic of aortic coarctation?
1. Reverse figure-of-three sign on frontal chest radiograph
2. Associated with berry aneurysms of the circle of Willis
3. First and second rib notching secondary to collateral vessels
supplied by costocervical trunk
4. Right ventricular hypertrophy
3

Pathophysiology:
• defect in vessel media, posterior infolding which
may be circumferential
• located near the ductus arteriosus
• can have tubular hypoplasia of arch
• post-stenotic dilation
• collateral vessels (intercostal and internal mammary)
Epidemiology:
• 5-10% of all congenital cardiac lesions
• untreated - < 20% survive to age 50 yrs
• males > females up to 2:1
Aortic Coarctation

Clinical presentation (depends on severity):
• infancy - CHF, acidosis, poor
perfusion of lower body
• post infancy - asymptomatic, murmur, htn,
HA, leg cramps, cold feet
Associations:
• Turner’s syndrome (XO)
• Bicuspid Aortic Valve
• VSD
• PDA
• Berry aneurysms of the circle of Willis
Aortic Coarctation

Imaging:
• Chest Radiographs - “3” sign, rib notching, edema, CM
• Esophagram - reverse “3” sign
• CT - anatomy (site, severity, morphology, collaterals)
• MRI
anatomy
gradient (peak velocities)
collateral flow using phase contrast techniques
evaluate for bicuspid AV, VSD, or LVH
Aortic Coarctation

6 yo with dysphagia

6 yo with dysphagia

Cervical Arch with Aneurysm
• perhaps formation of aortic arch
from third rather than fourth arch or
lack of caudal migration of 4th arch
• rare anomaly but with 20%
complicated by aneurysm
• often asymptomatic, can have
vascular ring-like symptoms or
supraclavicular pulsatile mass
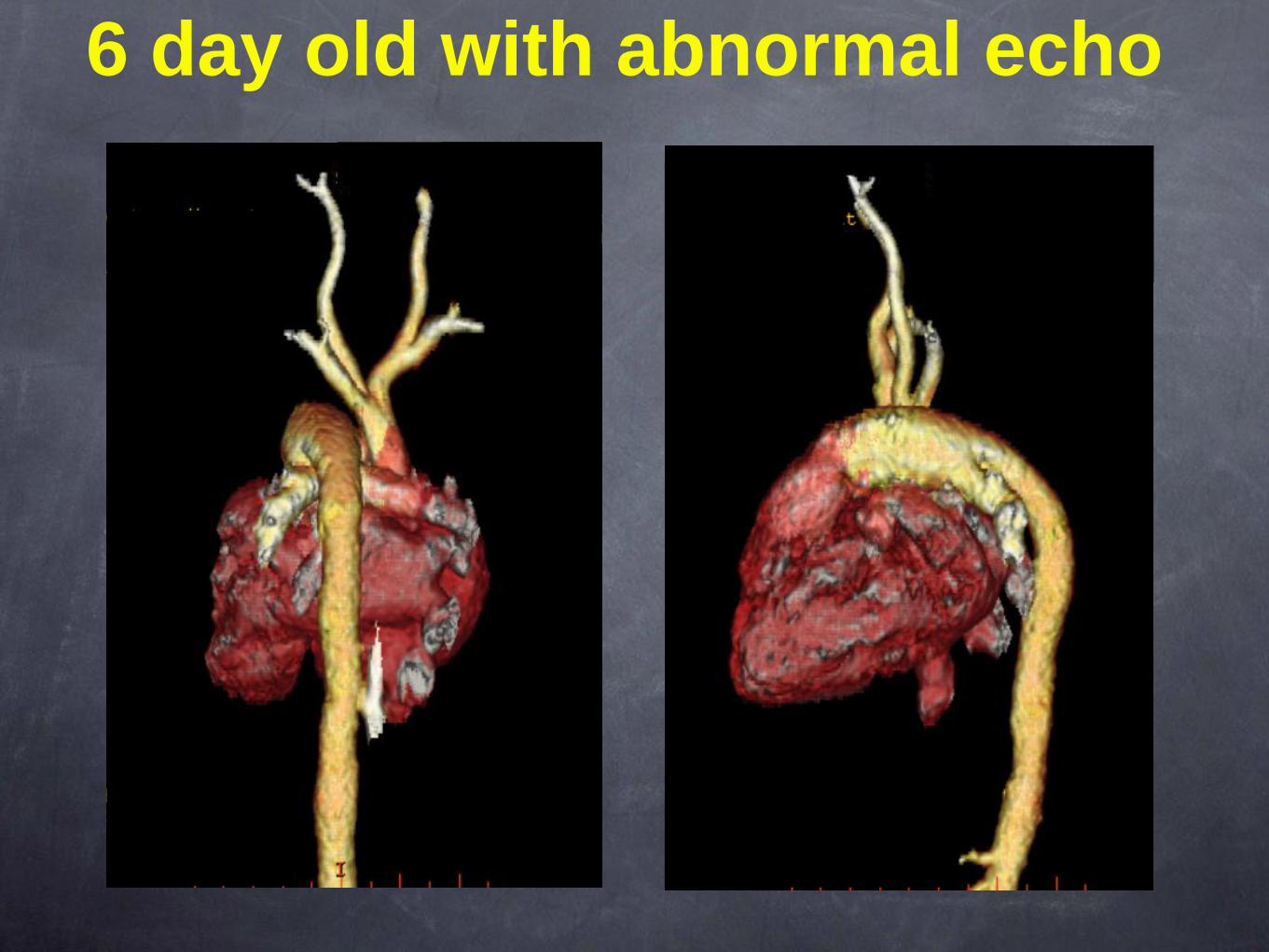
6 day old with abnormal echo

Which type of interrupted aortic arch is demonstrated?
1. Type A
2. Type B
3. Type C
4. Type D
Question 4

Which type of interrupted aortic arch is demonstrated?
1. Type A
2. Type B
3. Type C
4. Type D
Answer 4
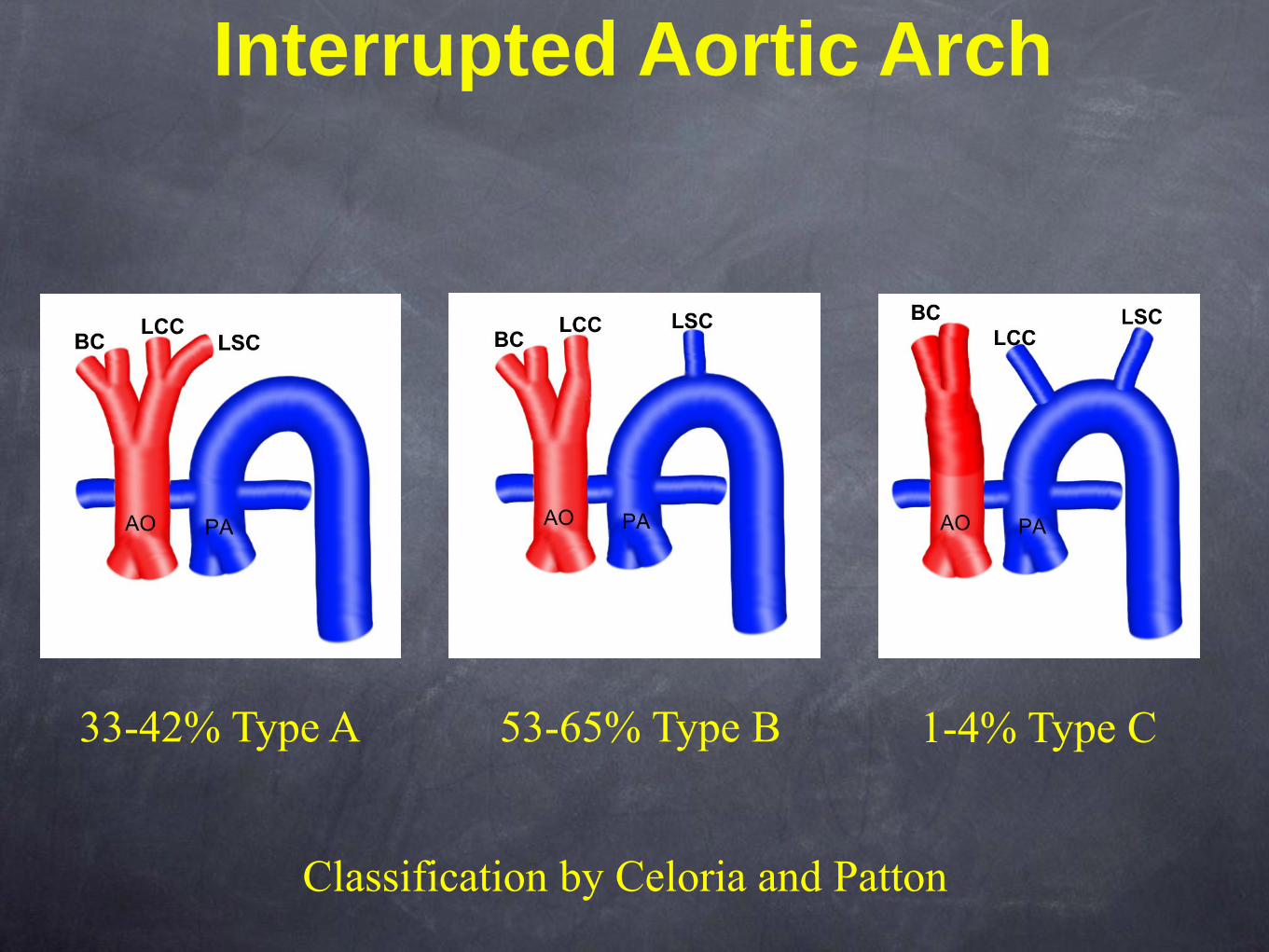
Interrupted Aortic Arch
33-42% Type A 53-65% Type B 1-4% Type C
Classification by Celoria and Patton

Interrupted Aortic Arch
Anatomy:
• complete discontinuity between ascending and
descending aorta
• simple or complex
simple - VSD and PDA
complex - truncus, TGA, double outlet RV
Epidemiology:
• 1% of congenital heart disease
• 25% have DiGeorge syndrome

Clinical presentation:
• heart failure (particularly with closure of ductus
arteriosus), cyanosis, poor peripheral pulses
Imaging:
• Chest Radiographs - CM with increased pulm
vascularity
and edema in critically ill newborn
midline
trachea and inconspicuous aortic knob
• CT - anatomy, determine type
• MRI - anatomy, as CT
Interrupted Aortic Arch

17 yo with scoliosis
5 cm

Which is often associated with Marfan syndrome?
1. Coagulopathy
2. Arterial tortuosity
3. Mitral valve prolapse
4. Coronary artery aneurysm
Question 6

Answer 6
Which is often associated with Marfan syndrome?
1. Coagulopathy
2. Arterial tortuosity - Loeys-Dietz feature
3. Mitral valve prolapse
4. Coronary artery aneurysm - Kawasaki’s feature

Marfan Syndrome
• Definition: Inherited connective tissue disorder with an
autosomal dominant transmission
• Incidence: 1 per 5000
• 25% represent new mutations
• Fibrillin protein dysfunction which prevents proper microfibril
formation.
• Premature medial degeneration with risk of aortic dilation and
subsequent dissection or rupture

Marfan Syndrome
Imaging:
screening and surveillance with MRA
evaluate for progressive aortic enlargement and
complications

References:
Edwards JE. Anomalies of the derivatives of the aortic arch system. Med Clin North Am
(1948) vol. 32 pp. 925 - 949.
Hernanz-Schulman. Vascular rings: a practical approach to imaging diagnosis. Pediatr
Radiol (2005) vol. 35 (10) pp. 961-79
Donnelly et al. Aberrant subclavian arteries: cross-sectional imaging findings in infants and
children referred for evaluation of extrinsic airway compression. AJR Am J Roentgenol
(2002) vol. 178 (5) pp. 1269-74
Farsak et al. Cervical aortic arch with aneurysm formation. Eur J Cardiothorac Surg (1998)
vol. 14 (4) pp. 437-9
Kimura-Hayama et al. Uncommon congenital and acquired aortic diseases: role of
multidetector CT angiography. Radiographics : a review publication of the Radiological
Society of North America, Inc (2010) vol. 30 (1) pp. 79-98
Yoo SJ, MacDonald C, Babyn P, eds. Chest Radiographic Interpretation in Pediatric Cardiac
Patients. New York, NY: Thieme Medical Publishers, Inc., 2010.
Ho V and Reddy G, eds. Cardiovascular Imaging. St. Louis, MO: Elsevier, 2011
Celoria GC, Patton RB. Congenital absence of the aortic arch. Am Heart J 1959;58:407–
413.
Collett RW, Edwards JE. Persistent truncus arteriosus: a classification according to
anatomic types. Surg Clin North Am 1949;29:1245–1270.







