Colangiocarcinoma: diretrizes 2014Alessandro Landskron DinizNúcleo de cirurgia abdominalNúcleo de cirurgia abdominal
Introdução
Colangiocarcinomas
• Grupo heterogêneo de tumores
á• Podem surgir de qualquer ponto da árvore biliar, e ainda por transdiferenciação de hepatócitos
• Associado com mortalidade alta
• 60% metastático ao diagnóstico
• Segundo tumor primário de fígado mais comumg p g
• Incidência em ascensão.
• Alguns fatores de riscos semelhantes a HCC (esteatohepatite, cirrose, vírus C)
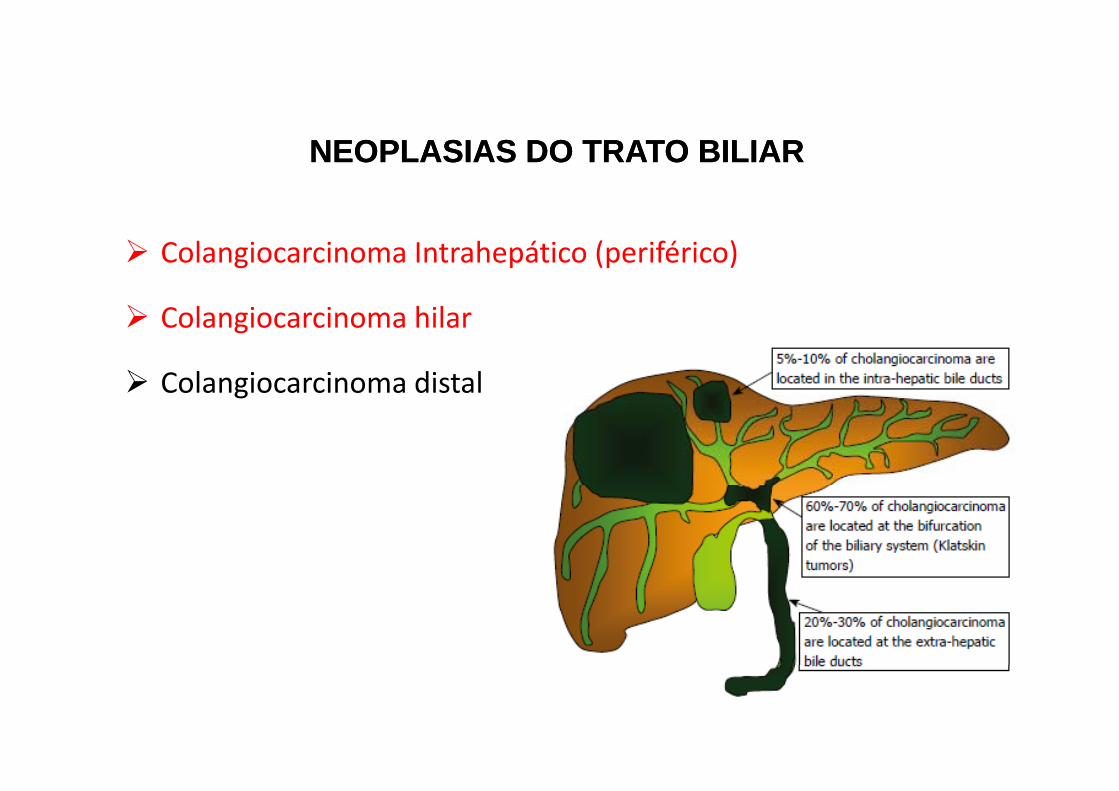
NEOPLASIAS DO TRATO BILIARNEOPLASIAS DO TRATO BILIAR
Colangiocarcinoma Intrahepático (periférico)
l h l Colangiocarcinoma hilar
Colangiocarcinoma distalg

Sintomas
Cholangiocarcinoma
I h i P ihil Di l
Cholangiocarcinoma
Intrahepatic Perihilar Distal
Abdominal Pain X X
Anorexia X X X
Weight loss X X X
Pruritis X XPruritis X X
Jaundice X X
Distended palpable GB X
Asymptomatic XAsymptomatic X
CCIH
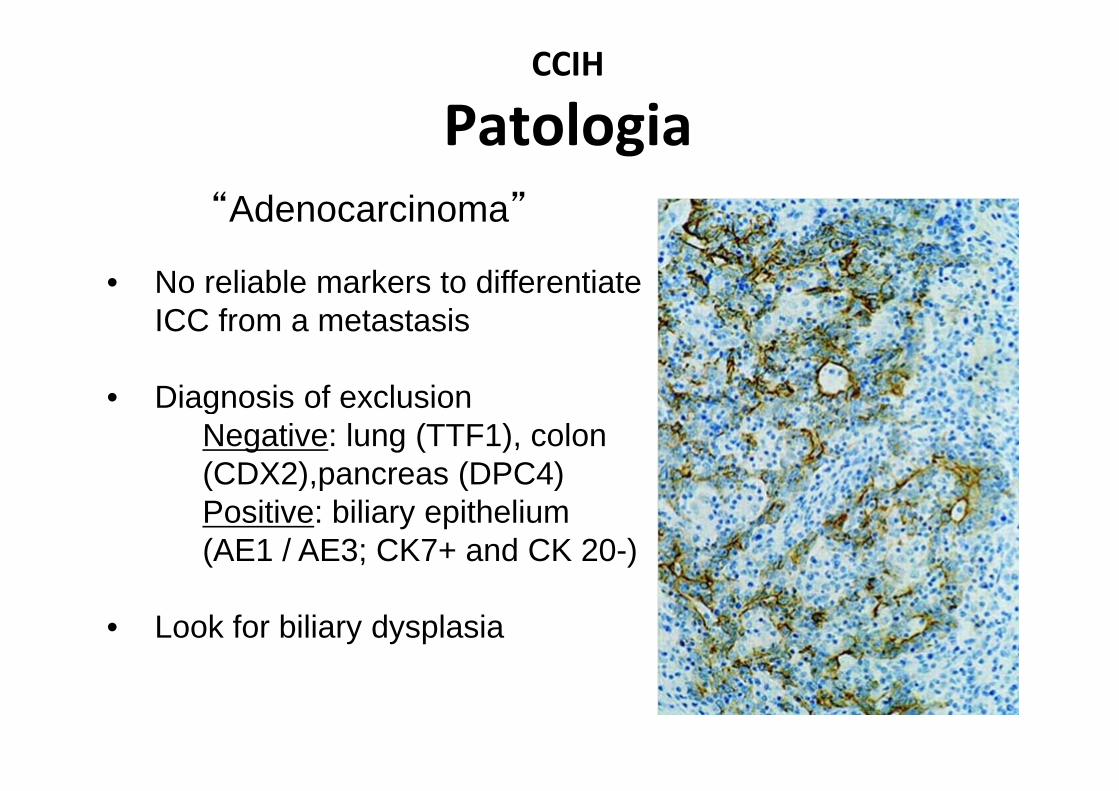
PatologiaPatologia“Adenocarcinoma”
• No reliable markers to differentiate
Adenocarcinoma
ICC from a metastasis
• Diagnosis of exclusion• Diagnosis of exclusionNegative: lung (TTF1), colon (CDX2),pancreas (DPC4)( ),p ( )Positive: biliary epithelium (AE1 / AE3; CK7+ and CK 20-)
• Look for biliary dysplasia

Objetivosj• Colangiocarcinoma Intra-hepático
– Diagnóstico diferencial– Indicações cirúrgicas-controvérsias– Aspectos técnicos– Tratamento sistêmico– Outras alternativas terapêuticas locoregionais.
• Colangiocarcinoma Hilarg– Diagnóstico diferencial e avaliação inicial– Tratamento cirúrgicoTratamento cirúrgico– Terapia Adjuvante– Tratamento paliativoTratamento paliativo
CCIHDi ó ti dif i l li ã éDiagnóstico diferencial e avaliação pré op.
""Massa hepática incidental….
• Mamografia (mulheres)• EDA e Colonoscopia• Imagem axial (TC e RM)• PET‐Scan• Marcadores tumorais• Função hepática• Sorologias

CCIHDi ó ti dif i l li ã éDiagnóstico diferencial e avaliação pré op.
• CEA elevado ~25% dos casos
• CA 19-9 elevado ~50% dos casos
• AFP elevada em < 5% dos casos
Nehls, Sem Liv Dis, 2004

CCIH
ImagemImagemgg
Mass Formingghomogenouslow-attenuation masscapsular retraction peripheral irregular rim enhancementperipheral irregular rim enhancement
Periductal Infiltratingperiductal enhancementperiductal thickening and enhancementirregularly dilated intrahepatic ducts
Intraductal-Growthdiffuse and marked ductectasiadiffuse and marked ductectasiawith or without visible papillary massintraductal cast-like lesionfocal intrahepatic ductal stricture
Photos: Han, Radiographics, 2002

CCIH (LCSGJ)
Incidência de acordo com morfologiaIncidência de acordo com morfologia
50% 10%
10% 30%30%

Ressonância magnética
Mass forming ICC. MR‐enhanced image demonstrates an ill‐defined hypointense mass with peripheral rim enhancement associated with atrophy of the left hepatic lobe and capsular retraction.

PET- CT
PET ScanPET Scan85% of ICC cases FDG avidChanged surgical management in 30%Identified occult metastatic disease 20-30%Identified occult metastatic disease 20-30%
Helpful to rule out occult primary, but more so to identify other metastatic diseaseidentify other metastatic disease
Anderson et al, JOGS 2004; Kim et al, Eur J Nuc Med 2003
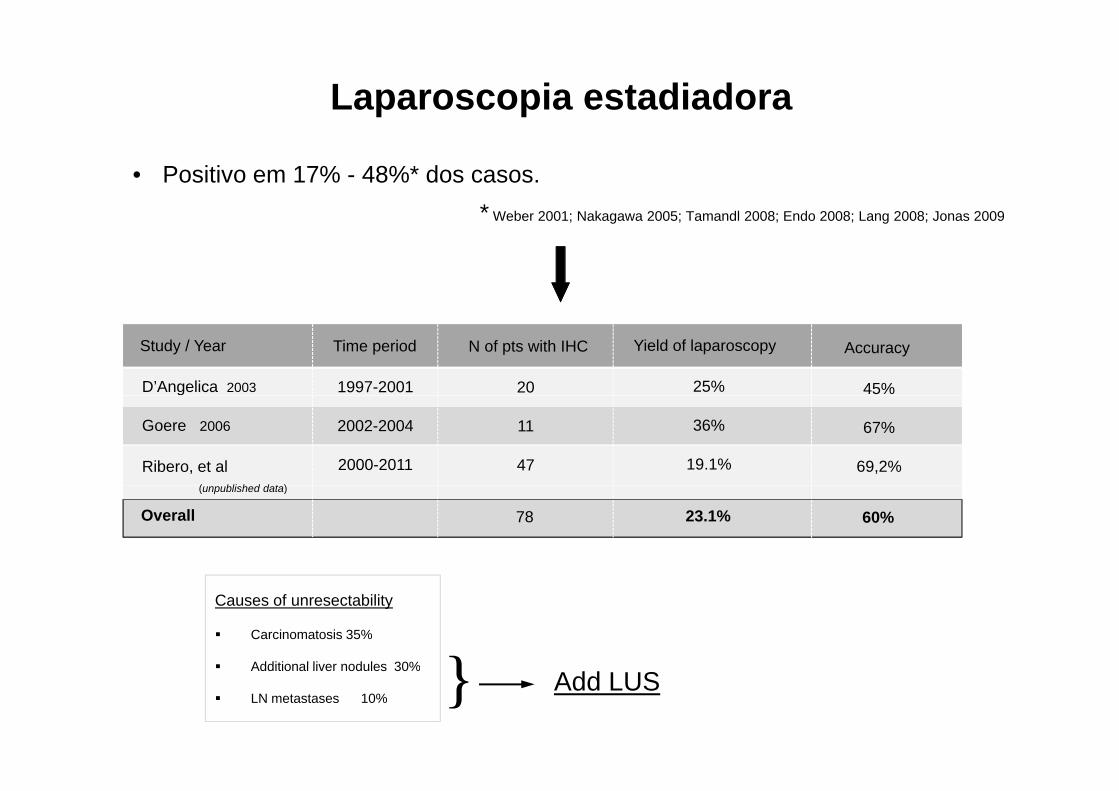
Laparoscopia estadiadora
• Positivo em 17% - 48%* dos casos.* Weber 2001; Nakagawa 2005; Tamandl 2008; Endo 2008; Lang 2008; Jonas 2009Weber 2001; Nakagawa 2005; Tamandl 2008; Endo 2008; Lang 2008; Jonas 2009
Study / Year Time period N of pts with IHC Yield of laparoscopy Accuracy
D’Angelica 2003 1997-2001 20 25% 45%
Goere 2006 2002-2004 11 36% 67%
Ribero, et al( bli h d d t )
2000-2011 47 19.1% 69,2%(unpublished data)
Overall 78 23.1% 60%
Causes of unresectability
Carcinomatosis 35%
Additional liver nodules 30% } Additional liver nodules 30%
LN metastases 10% } Add LUS
Estadiamento
CCIHA li éA li é R d õR d õAvaliaçao pré opAvaliaçao pré op-- RecomendaçõesRecomendações
d l d á l d•Fundamental descartar um primário oculto na presença de um adenocarcinoma do fígado.(endoscopia, PET, etc).
•Imagem axial fundamental em todos os casos, com resultado um pouco superiores favorecendo a RM.
•A sétima edição da AJCC/UICCA é o método de estadiamento recomendado.

CCIHI di õ é i d i ú iIndicações e controvérsias do tratamento cirúrgico.
A cirurgia é o tratamento mais efetivo, sendo o único
com potencial curativo.
Contraindicações absolutasContraindicações absolutas• Carcinomatose peritoneal• Múltiplos tumores bilaterais.• Metástase extra‐ hepática (pulmão, osso…)
CCIH
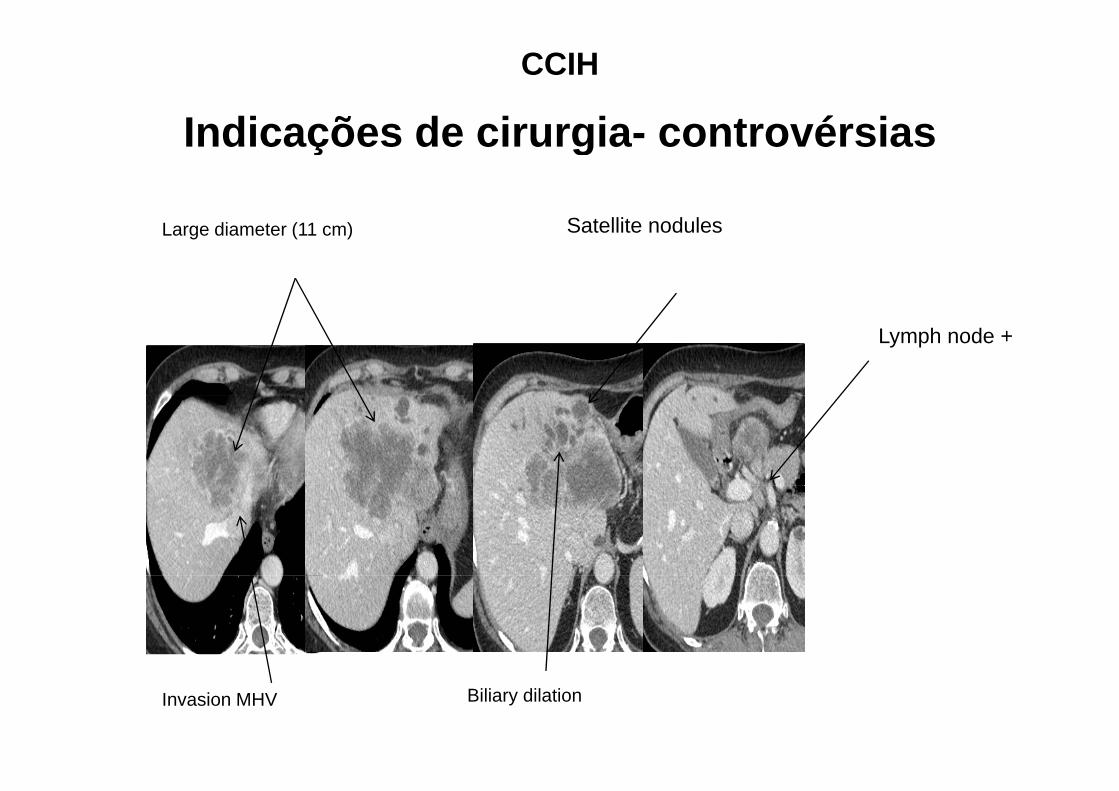
Indicações de cirurgia controvérsiasIndicações de cirurgia- controvérsias
Large diameter (11 cm) Satellite nodules
Lymph node +
Invasion MHV Biliary dilation
CCIH
The Italian experienceThe Italian experience
• Multi-institutional series of 574 patients (1995-2011) Registry sponsored by the IHPBA Italian Chapter
• Setting: 12 tertiary referral centers
• Inclusion criteria Pathologically confirmed IHC Curative intent liver resection Mixed IHC-HCC excluded
•Indications“if can be completely resected with a sufficient liver
t”* Ribero D et al. Arch Surg 2012; 20:1-7 (updated)
remnant”
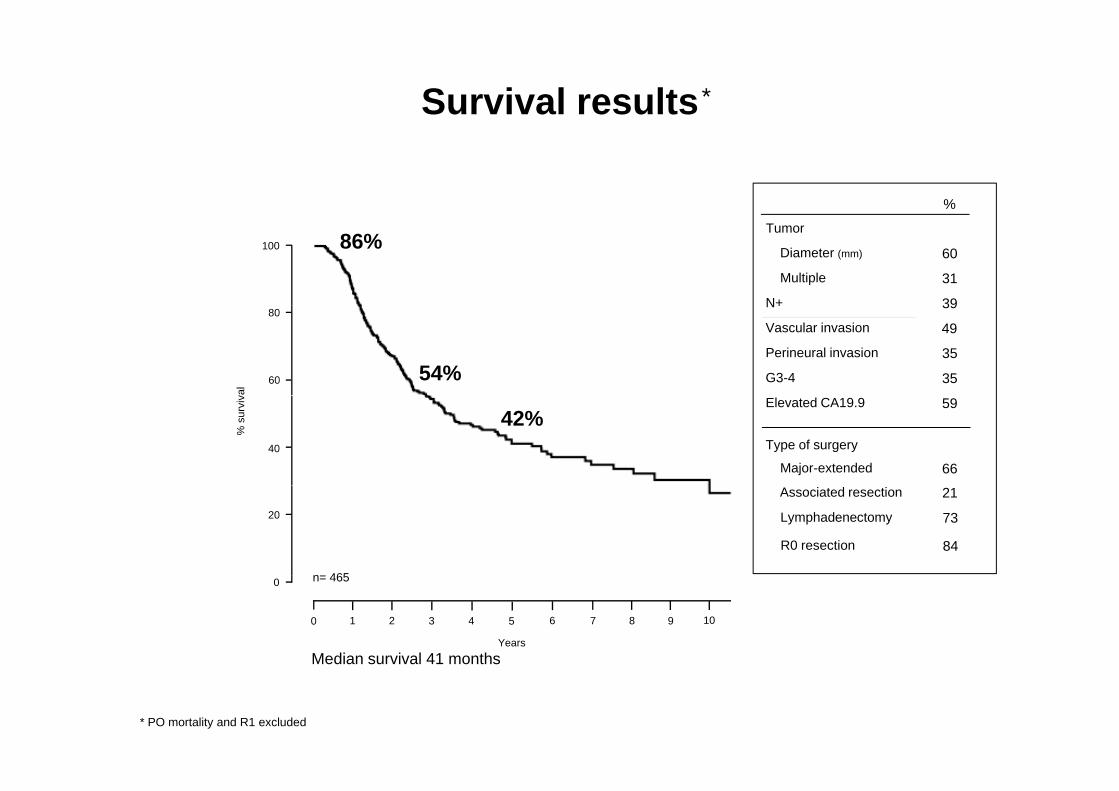
Survival results *
%
100 86%Tumor
Diameter (mm) 60
Multiple 31
N+ 39
60
80
val
54%
N 39
Vascular invasion
Perineural invasion 35
G3-4 35
49
40
% s
urvi
v
42%Elevated CA19.9 59
Type of surgery
Major-extended 66
20
n 465
Associated resection 21
Lymphadenectomy 73
R0 resection 84
0 1 2 3 4 5 6 7 8 9 10
0
Years
Median survival 41 months
n= 465
* PO mortality and R1 excluded

CCIH- Indicações de cirurgia- controvérsias
Múltiplos nódulos
• Problema relevante (~30% up to 59%)
Múltiplos nódulos….
Diferenciar….Nódulos satélites??Nódulos satélites??Metastáses intrahepáticas??
VS
Yes NoYes No
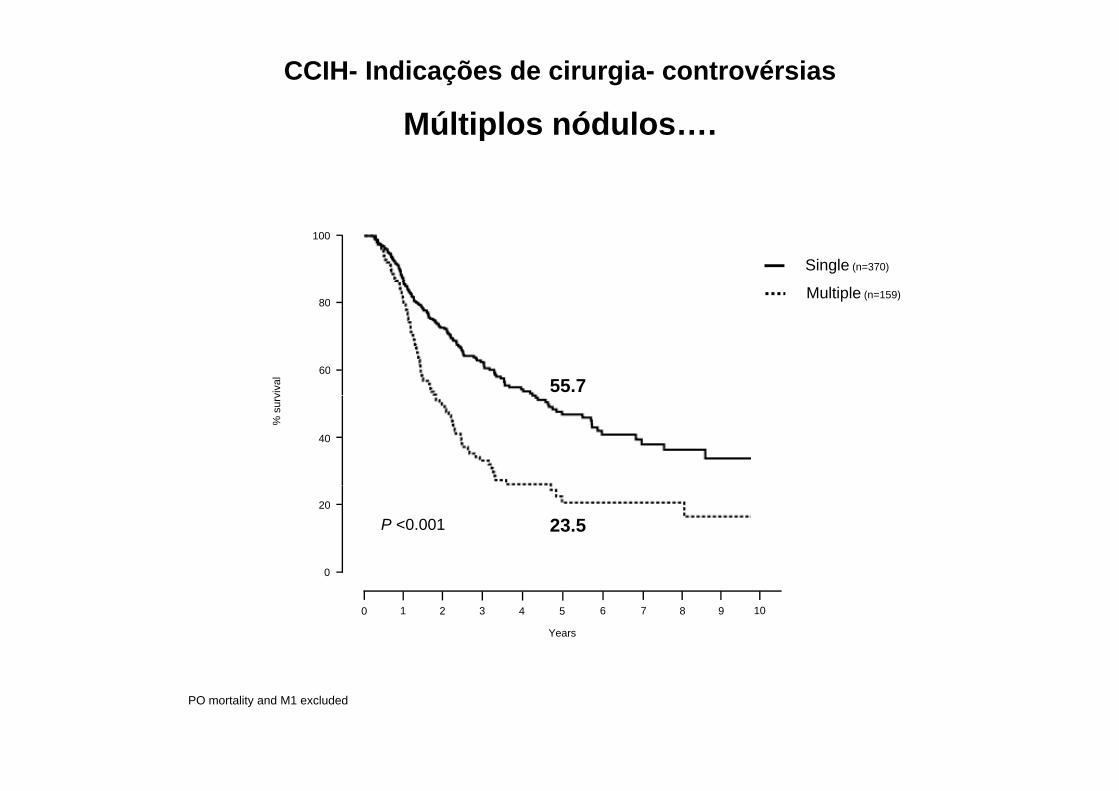
CCIH- Indicações de cirurgia- controvérsias
Múltiplos nódulosMúltiplos nódulos….
80
100
Single (n=370)
Multiple (n=159)
60
80
viva
l 55.7
40
% s
urv
0
20
23.5P <0.001
0 1 2 3 4 5 6 7 8 9 10
0
Years
PO mortality and M1 excluded
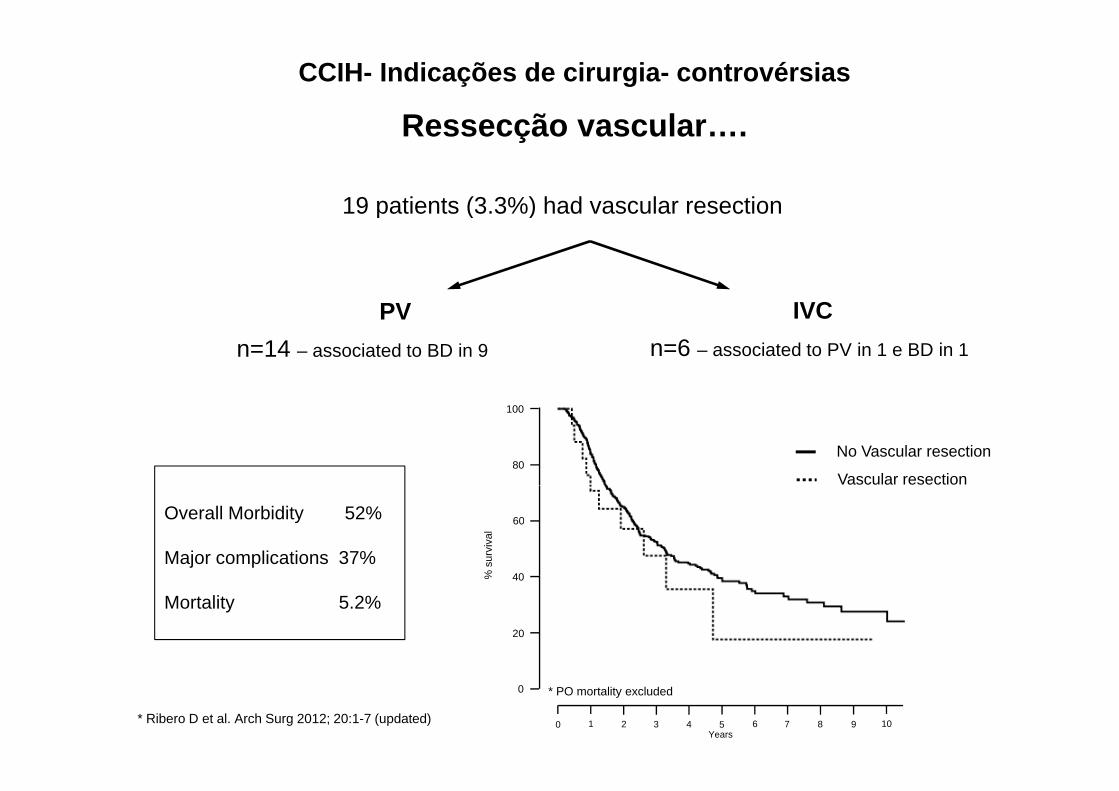
CCIH- Indicações de cirurgia- controvérsias
Ressecção vascular
19 patients (3.3%) had vascular resection
Ressecção vascular….
p ( )
PV IVCPVn=14 – associated to BD in 9
IVCn=6 – associated to PV in 1 e BD in 1
80
100
No Vascular resection
Vascular resection
Overall Morbidity 52%
Major complications 37%40
60
% s
urvi
val
Mortality 5.2%20
40%
0 1 2 3 4 5 6 7 8 9 10
0
Years
* PO mortality excluded
* Ribero D et al. Arch Surg 2012; 20:1-7 (updated)

CCIH- Indicações de cirurgia- controvérsias
Recidiva local….Recidiva local….
301 resected IHC
53 5% recurred53.5% recurred
Intrahepatic61%
Extrahepatic21%
Intra-Extrahepatic18%

CCIH- Indicações de cirurgia- controvérsias
Recidiva local - ressecçãoRecidiva local - ressecção….
39 re-resections * 88%100
M lti l
Single
100%
85%
Tumor diameter (mm) 26
Tumor number(single vs multiple) 12/17
72%
50%60
80
al
Multiple
68%
Preoperative CTx 36%
R0 resections 100%40%
sur
viva
After re-resection0
20
After first resection
0 1 2 3 4 5 6 7 8 9 10Years
* Patient selection done using the same criteria adopted for primary tumor
CCIH- Indicações de cirurgia- controvérsias
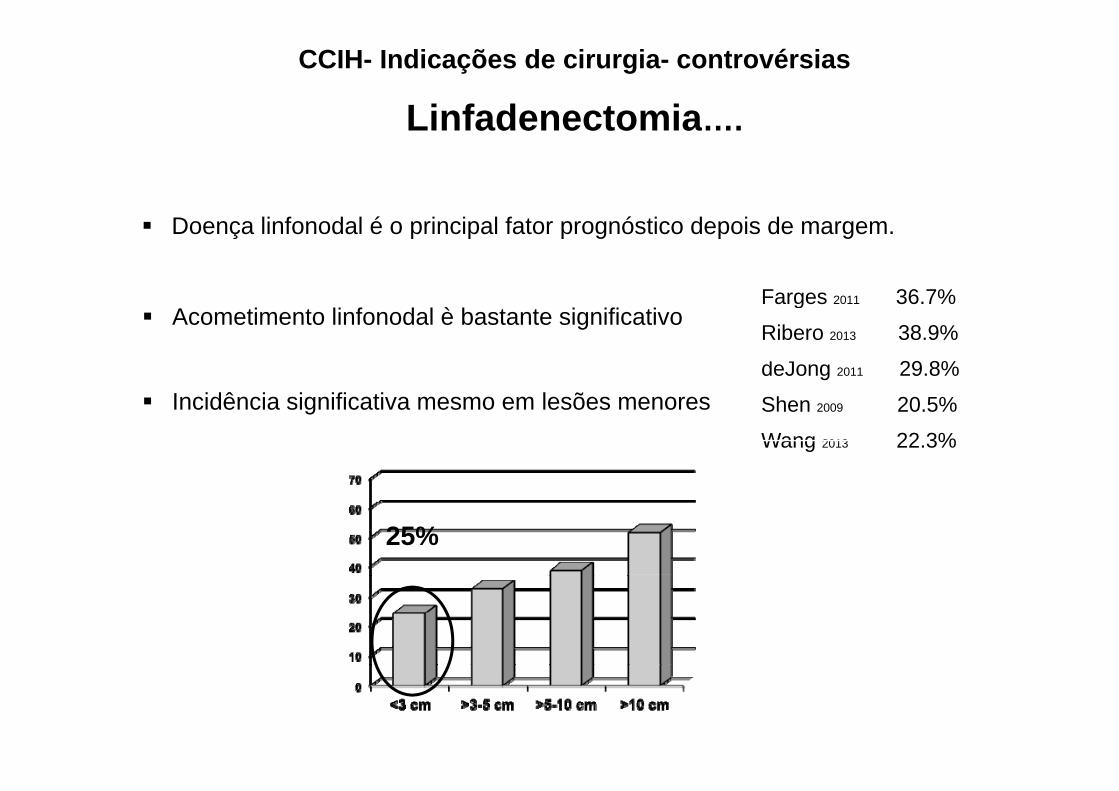
Linfadenectomia….Linfadenectomia….
Doença linfonodal é o principal fator prognóstico depois de margem.
Farges 2011 36.7% Acometimento linfonodal è bastante significativo
g
Ribero 2013 38.9%
deJong 2011 29.8%I idê i i ifi ti l õ Shen 2009 20.5%
Wang 2013 22.3%
Incidência significativa mesmo em lesões menores
25%
CCIH- Indicações de cirurgia- controvérsias
Argumentos a favor da linfadenectomia….
D fi ó ti
Argumentos a favor da linfadenectomia….
Define prognóstico
Melhor estadiamento
Pode orientar tratamentos adjuvantes.
• Redução de recidiva loco-regional
?• Melhora sobrevida ?

Extensão da linfadenectomiaTh 7th Ed TNM d ti- The 7th Ed. TNM recommendations -
Regional nodes
Distant metastases
77
11
77
999999
9999 9988
88
1212
12
77
12
12
1233
33
77
8888
13
13
13
13
Up to 54% of pts have mets in these LNsOkami J et al. J Gastrointest Surg 2003
50% of pts with mets in these LNs have no hilar metsNozaki Y et al. Cancer 1998

Field of lymphadenectomy
EsophagusEsophagus
Gastric art.Gastric art.
Gastric veinGastric veinPortal veinPortal vein
Bile ductBile duct
Hepatic artHepatic art
Gastric veinGastric veinPortal veinPortal vein
Splenic art.Splenic art.
Hepatic art.Hepatic art.
Recomendações cirurgia CCIHRecomendações- cirurgia CCIH
• Ressecabilidade é definida pela possibilidade de ressecção completa da lesão com um fígado remanescente adequando (R0)D t h áti t últi l bil b li f d• Doença extra-hepática, tumores múltiplos bilobares e linfonodos retroperitoneais, são contraindicações para cirurgia
• Uso da laparoscopia para estadiamento deve ser rotineira• Uso da laparoscopia para estadiamento deve ser rotineira• Linfadenectomia regional deve ser "standard”• A resseção vascular associada deve ser realizado em casos bemA resseção vascular associada, deve ser realizado em casos bem
selecionados, porém, pode conferir pior prognóstico
CCIH
Tratamento sistêmico
• Evidência baixa em opções de tratamento adjuvante• Evidência baixa em opções de tratamento adjuvante• Opção inicial, sempre gemcitabine + cisplatin• Outras alternativas gemcitabine / 5‐FU• Outras alternativas gemcitabine / 5‐FU• Segunda linha não está definida• Tratamento regional com Debiri pode ser uma opçãoTratamento regional com Debiri pode ser uma opção• Estudos fase II com tumores extra‐hepaticos…• Clinical trials
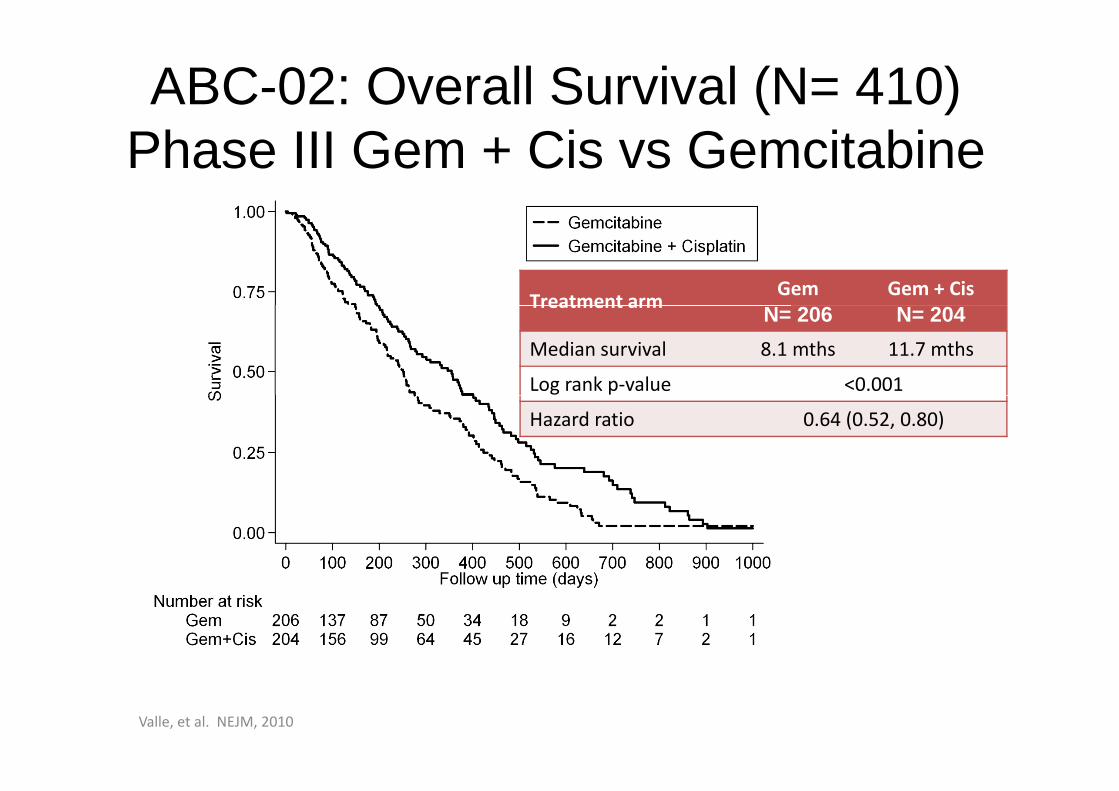
ABC-02: Overall Survival (N= 410)Phase III Gem + Cis vs Gemcitabine
Treatment armGem Gem + Cis
Treatment arm N= 206 N= 204Median survival 8.1 mths 11.7 mths
Log rank p‐value <0.001
Hazard ratio 0.64 (0.52, 0.80)
Valle, et al. NEJM, 2010
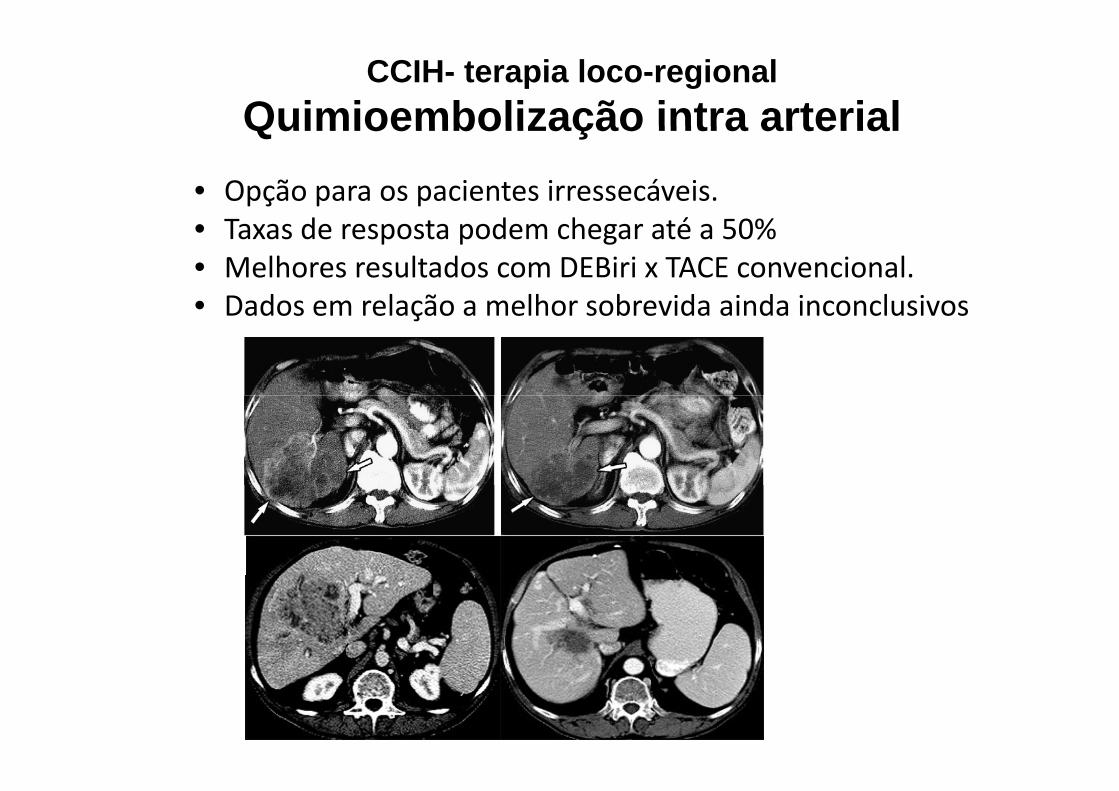
CCIH- terapia loco-regionalQuimioembolização intra arterialQuimioembolização intra arterial
• Opção para os pacientes irressecáveis.• Taxas de resposta podem chegar até a 50%• Melhores resultados com DEBiri x TACE convencional.• Dados em relação a melhor sobrevida ainda inconclusivos• Dados em relação a melhor sobrevida ainda inconclusivos
Consensus StatementsConsensus Statements
• Tratamento adjuvante– Pacientes ressecados com margem positiva ou linfonodos positivos, a exposição
tratamento sistêmico pode ser uma opção. Utilização de esquemas com gencitabina 5Fu.
– Considerar adição da radioterapia sempre após discussão multidisciplinar– Randomized trials evaluating gemcitabine, capecitabine, gemcitabine and
oxaliplatin will mature over next couple of years
• Cholangiocarcinoma avançado• Cholangiocarcinoma avançado– Quando necessário, o alívio da obstrução biliar é fundamental (stent)– Phase III trial suporta cisplatin/gemcitabine como front line– A utilização de terapias regionais podem ser uma opção, mas necessitam de
estudos mais robustos

"Tumor contendo uma intersecção de elementos deHepato-colangiocarcinoma
Tumor contendo uma intersecção de elementos de colangiocarcinoma e hepatocarcinoma"
Type A Separate nodules
WHO Classification of Tumours of the Digestive System 4th ed. 2009
Type A. Separate nodules(Double cancer)Present at different sites within the same liver.liver.
Type B. Contiguous nodulesd d l hPresent at adjacent sites and mingle with
continued growth.
Type C. Intermingling noduleCombined within the same tumor.
“Strict” Combined HCC-CC

Experiences @ Tokyo University Hospital (1995-2009)
681 patients underwent hepatectomy for the primary liver
cHCC CC HCC ICC
681 patients underwent hepatectomy for the primary liver cancer (Allen-Lisa type C); 3.7% of all the surgical cases
cHCC-CC (n=25)
HCC (n=577)
ICC(n=79) P value
age 61 66 62 ND
Gender (male) 76% 78% 53% vs ICC, 0.06
HBV 24% 20% 9% vs ICC, 0.01
HCV 52% 63% 19% ICC 0 0003HCV 52% 63% 19% vs ICC, 0.0003
Cirrhosis 52% 56% 4% 0.94, 0.0001
AFP (ng/ml) 172 27 4 vs. ICC ,<0.001AFP (ng/ml) 172 27 4 vs. ICC ,<0.001
PIVKA-II (mAU/ml) 45 64 19 ND
CEA (ng/ml) 3.2 ND 4.1 ND
CA19-9 (U/ml) 50 24 112 0.02
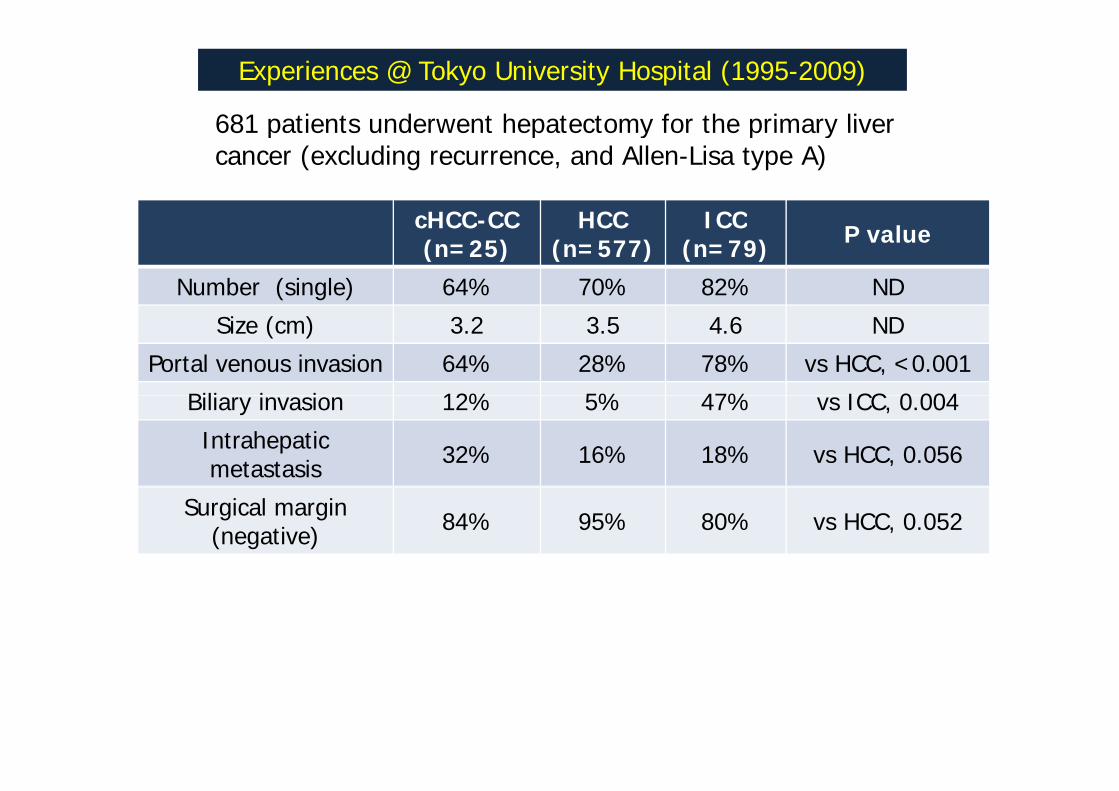
Experiences @ Tokyo University Hospital (1995-2009)
681 patients underwent hepatectomy for the primary liver
cHCC CC HCC ICC
681 patients underwent hepatectomy for the primary liver cancer (excluding recurrence, and Allen-Lisa type A)
cHCC-CC (n=25)
HCC (n=577)
ICC(n=79) P value
Number (single) 64% 70% 82% ND
Size (cm) 3.2 3.5 4.6 ND
Portal venous invasion 64% 28% 78% vs HCC, <0.001
Bili i i 12% 5% 47% ICC 0 004Biliary invasion 12% 5% 47% vs ICC, 0.004
Intrahepaticmetastasis 32% 16% 18% vs HCC, 0.056
Surgical margin (negative) 84% 95% 80% vs HCC, 0.052

Experiences @ Tokyo University Hospital (1995-2009)
cHCC CC HCC ICC
Recurrence pattern
cHCC-CC (n=25)
HCC (n=577)
ICC(n=79) P value
Overall 76% 73% 61% ND
Breakdown of recurrenceIntrahepatic 95% 93% 67% vs ICC, 0.027
E t h ti 26% 7% 77% 0 016 0 001Extrahepatic 26% 7% 77% 0.016, <0.001
Both of them 21% 3% 44% ND
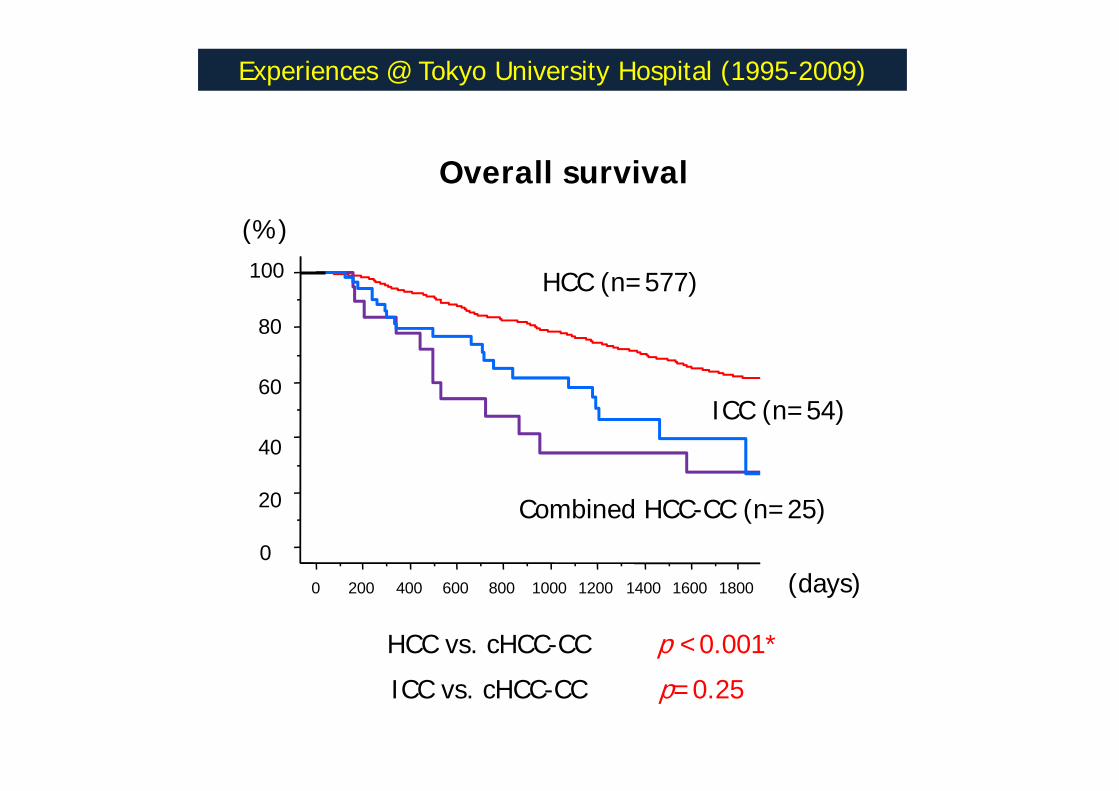
Experiences @ Tokyo University Hospital (1995-2009)
Overall survival
100 HCC (n=577)
(%)
60
80
40
ICC (n=54)
0
20 Combined HCC-CC (n=25)
(d )0 200 400 600 800 1000 1200 1400 1600 1800 (days)
p <0.001*HCC vs. cHCC-CC
p=0.25ICC vs. cHCC-CC

Consensus Statement on Combined HCC-CCCombined HCC CC
Tumor raro com dois fenótipos no mesmo microambiante.
Diagnóstico pré operatório é difícil e muitas vezes só ocorre após a diferenciação imuno histoquímica.ç q
O tratamento cirúrgico é a melhor opção quando ressecáveis.
A sobrevida é inferior ao HCC e Colangiocarcinomas puros.

Colangiocarcinoma HilarColangiocarcinoma Hilar
• Avaliação e diagnóstico diferencial
• Tratamento cirúrgico- indicaçõesg ç
• Papel do tratamento adjuvante
Introdução“Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis: An unusual tumor with distinctive clinical and pathological features”pathological features”
Am J Med 1965, Feb 38 p241-256.
• Gerald Klatskin –YaleN 13• N=13
…”death in this disease is usually attributable to hepatocellular failure and/or hepatobiliary infection secondary to unrelieved biliary obstruction rather than to massive invasion of the liver by tumor or to extrahepatic metastases, (3) palliative surgery aimed at relieving biliary obstruction may restore the patient to a good state of health for a remarkably long period of time, and (4) such palliation may be achieved by internal drainage of only one of the major intrahepatic bile d t ”ducts”….
Colangiocarcinoma Hilar
Abordagem Inicial CA 19 9 P ó i A ili l i CA 19.9‐ Prognóstico – Auxiliar para laparoscopia estadiadora.
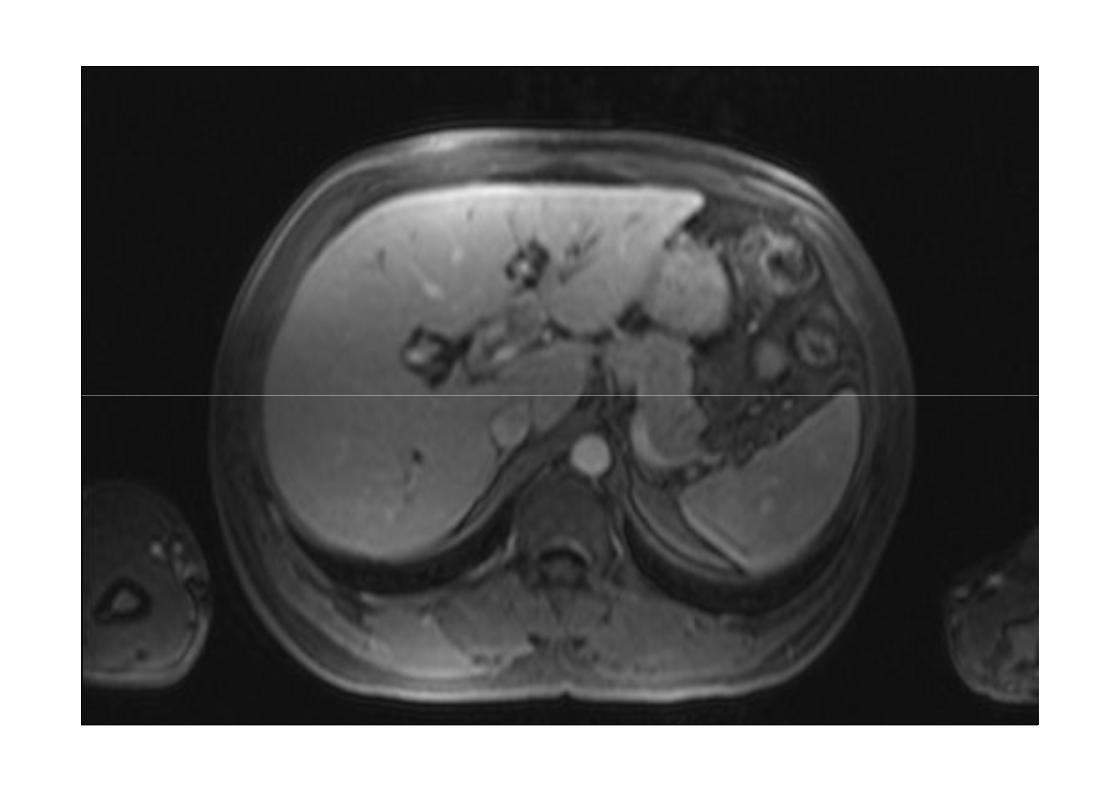
T fi Tó A li á Tomografia Tórax‐ Avaliar metástases. TC ou RM abdome superior…
– Envolvimento ductal– Extensão radial do tumor‐ envolvimento vascular, etc….A li fi hi fi l l– Avaliar atrofia ou hipertrofia contralateral
PET CT
Colangiocarcinoma Hilar
Abordagem Inicial• Drenagem biliar pré‐ operatória? ?
• Sempre?Sempre?
• As vezes?Bilirrubina >5 mg dl? ? > 10 mg dl??
Maioria das vezes decisão inicial não é do Cirurgião hepatobiliar!!Pacientes com infecção sempre drenar!!
Via percutãnea preferencial!! (permite drenagem seletiva e sem contaminação ascendente )contaminação ascendente....)
CCH
Diagnóstico diferencial
• Doenças inflamatórias– Colangite esclerosante (pode coexistir com a g (pneoplasia)
– IgG4 (auto imune)IgG4 (auto imune)
• Litiase intra‐ hepática• Biópsia pré‐op necessária??

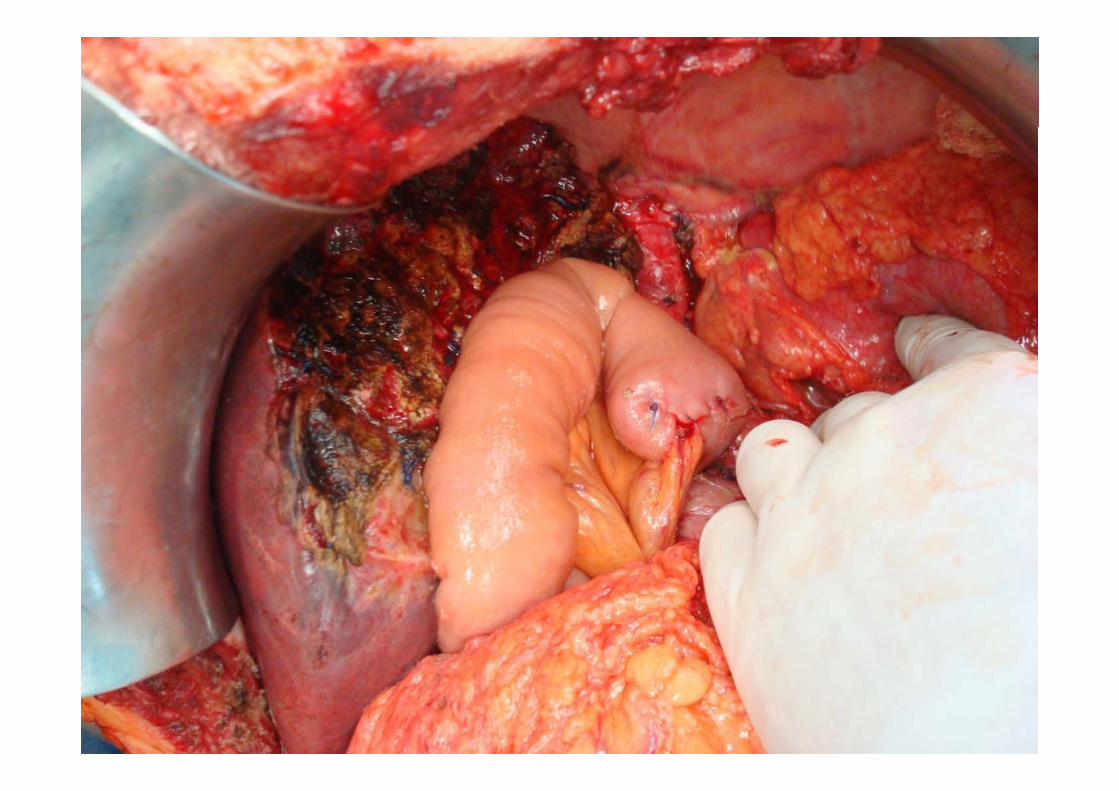
CCH- Cirurgia
Extensão de ressecção
Ressecção hepática associada > R0
D’ Angelica Surgery Today 2004
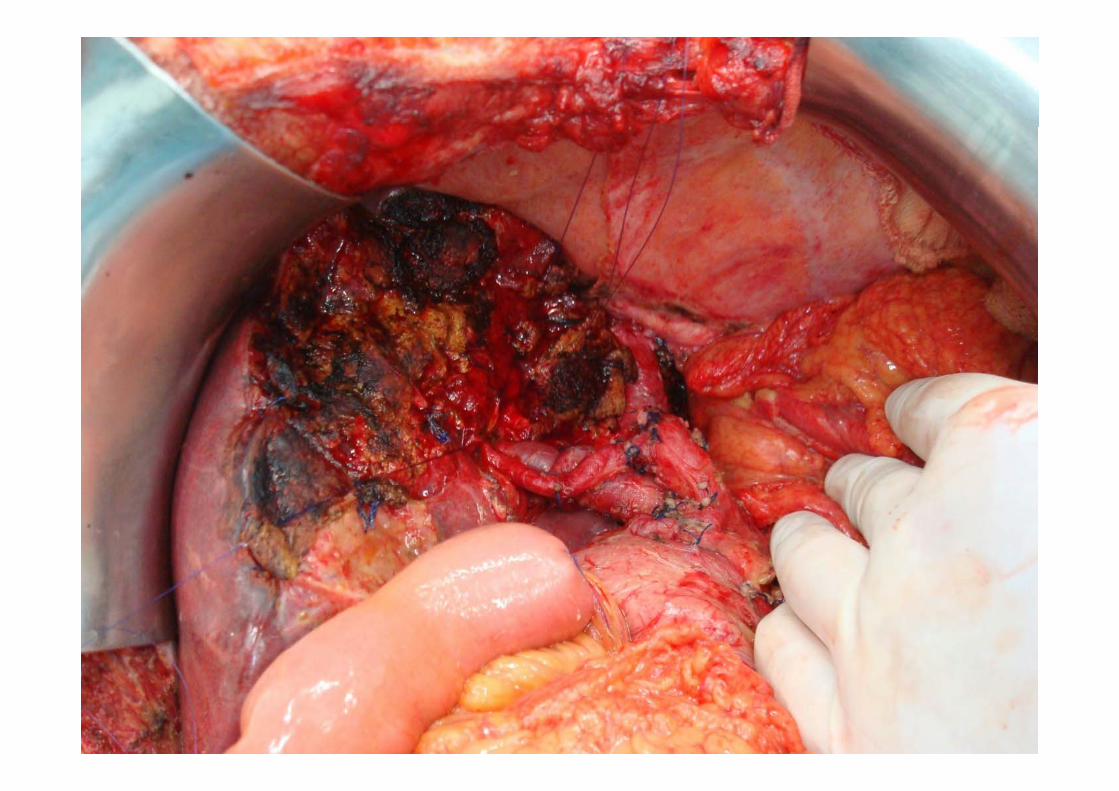
CCH Ci iCCH- Cirurgia
Tática cirúrgica....g
3b3b
i d d d i biliHepatectomia Esquerda + Caudado+ via biliar “Modified Hanging Liver”
CCH- Cirurgia
i f d iLinfadenectomia
Papel ainda incerto, do ponto de vista terapêutico.pPapel significativo como estadiamento.Li í d i l i di l ALimítes devem incluir medialmente a Ao hepática comum, ligamento hepato‐ duodenal e lateralmente linfonodos retropancreáticos.A presença de doença linfonodal estáA presença de doença linfonodal está associada com pior sobrevida.
D’angelica, M Surg Today 2004
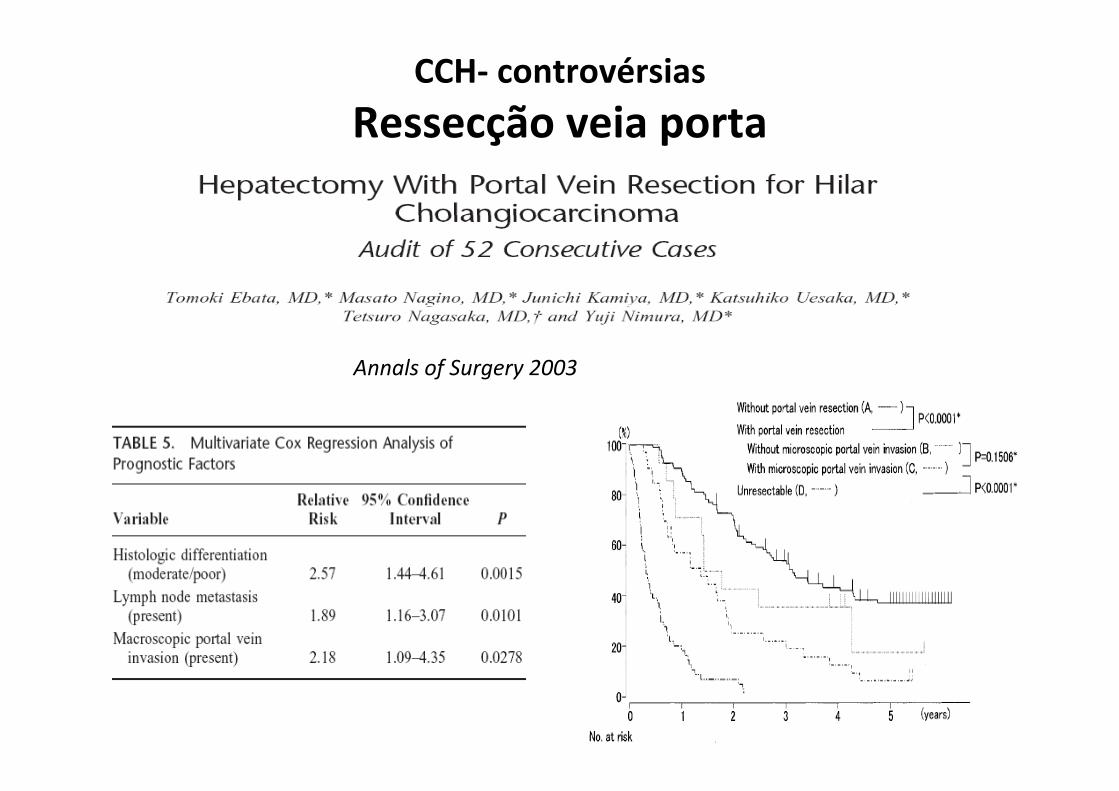
CCH- controvérsias
Ressecção veia portaRessecção veia porta
Annals of Surgery 2003
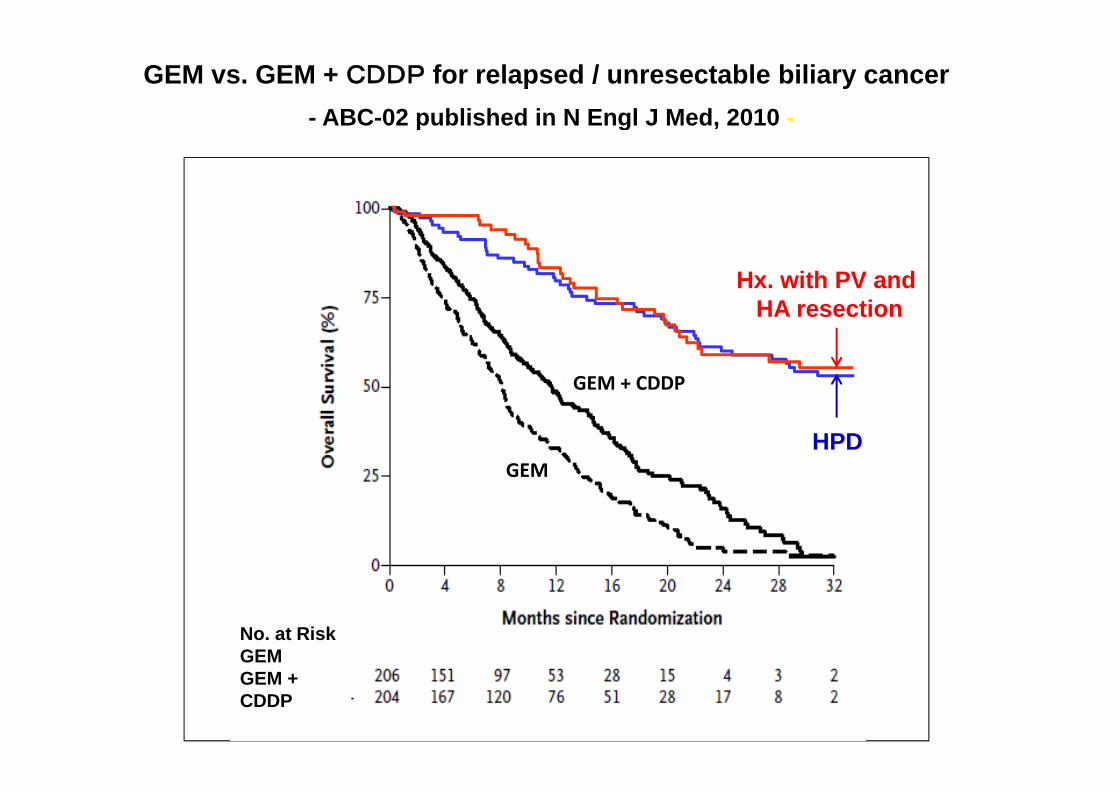
GEM vs. GEM + CDDP for relapsed / unresectable biliary cancer- ABC-02 published in N Engl J Med, 2010 -p g ,
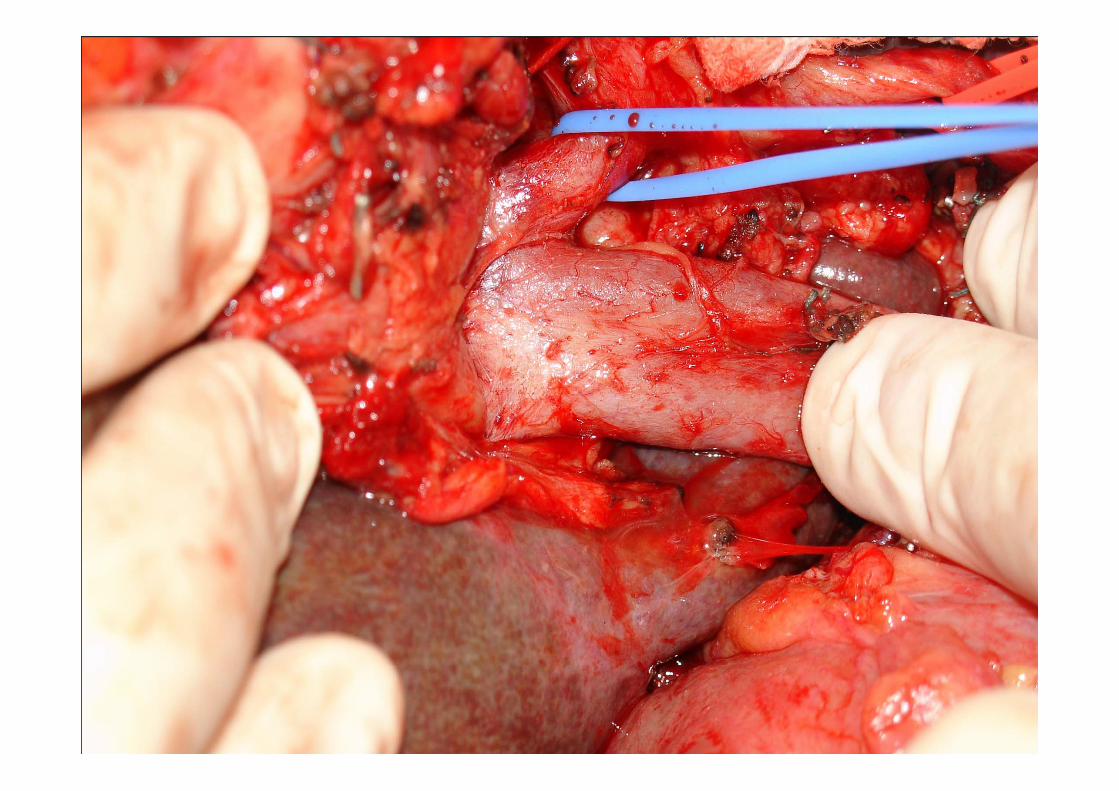
Hx. with PV and HA resection
GEM + CDDP
HA resection
GEMHPD
No. at RiskGEMGEM + CDDP
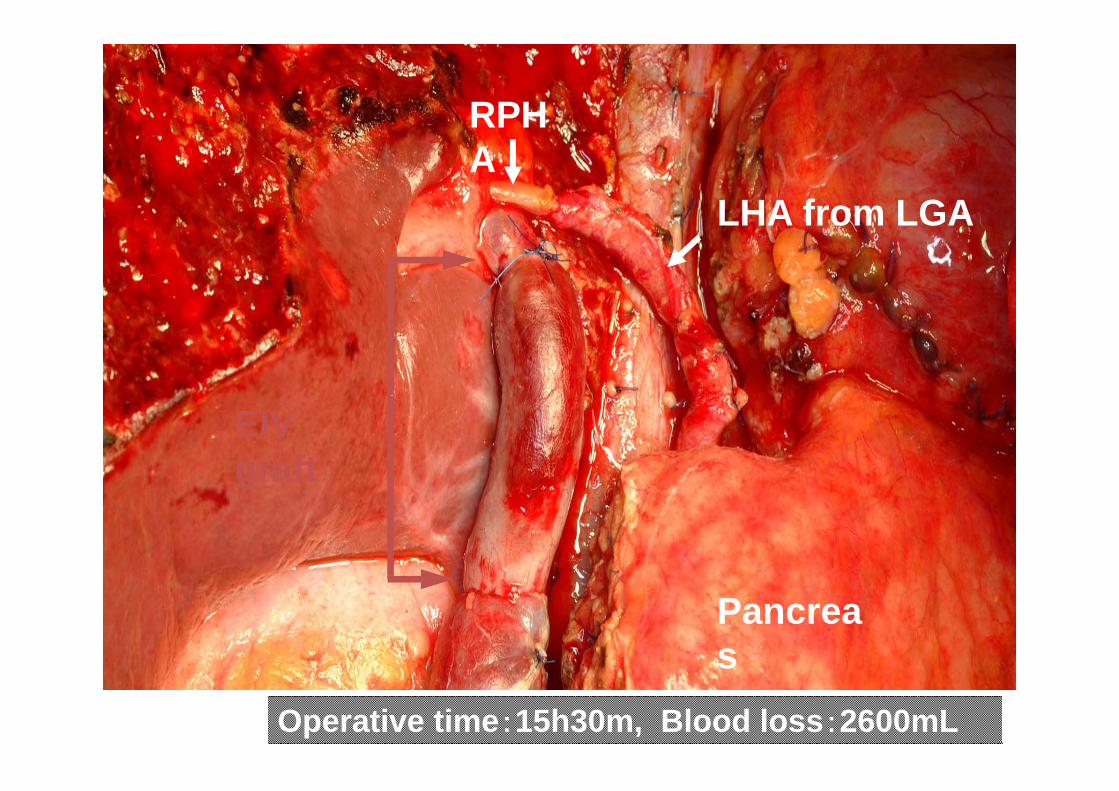
RPHRPHA
LHA from LGALHA from LGA
EIV graftg
Pancreas
Operative time:15h30m, Blood loss:2600mL
s

CCH
O õ d t t t dj tOpções de tratamento adjuvante• Dados limitados na literaturaDados limitados na literatura• Estudos retrospectivos favorecem tratamento
b d d dcombinado de radio e quimioterapia• Melhor taxa de controle local com tratamento com radio e quimioterapia.M lh d b id ??• Melhora de sobrevida??
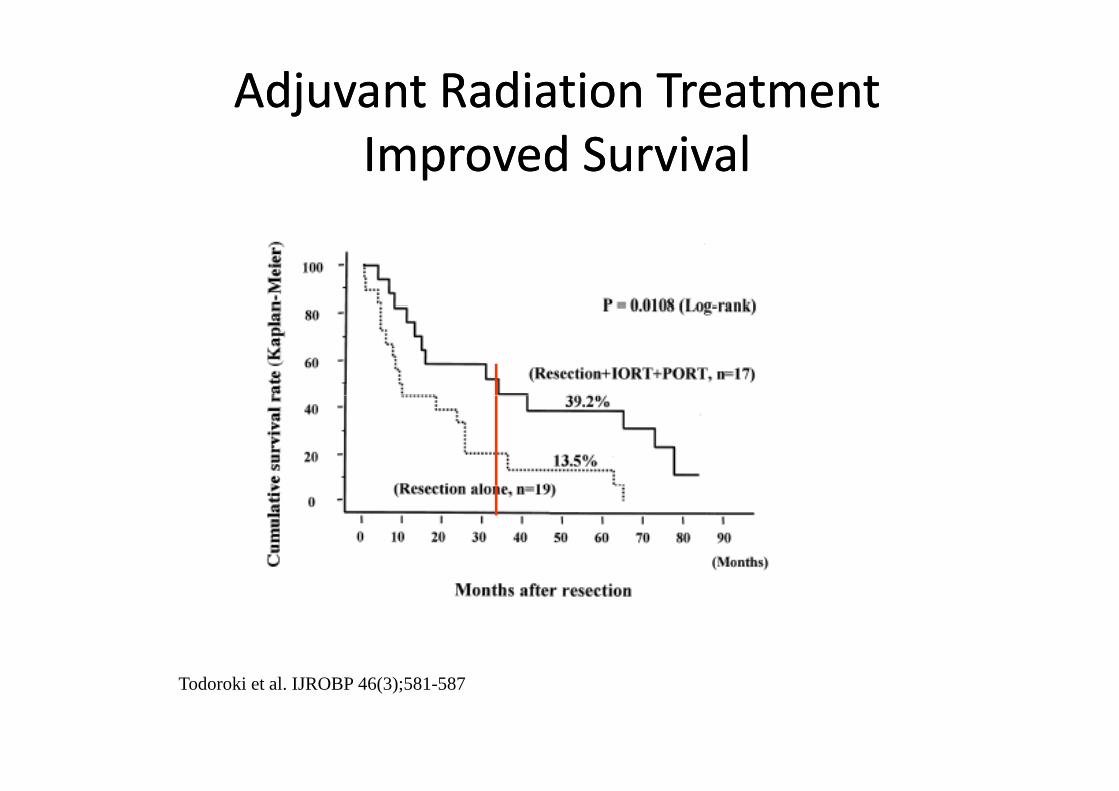
Adjuvant Radiation TreatmentAdjuvant Radiation TreatmentImproved SurvivalImproved Survival
Todoroki et al. IJROBP 46(3);581-587
MDACC seriesPatient Characteristics n=65
• All patients had resected EHBT– Gallbladder and ampullary tumors excluded
• 42 pts – margin positive or pN+42 pts margin positive or pN+– received post‐op CXRT
• 23 pts – R0 and pN0 – received no adjuvant treatmentj
Borghero Y, Crane et al Ann Surg Onc 2008
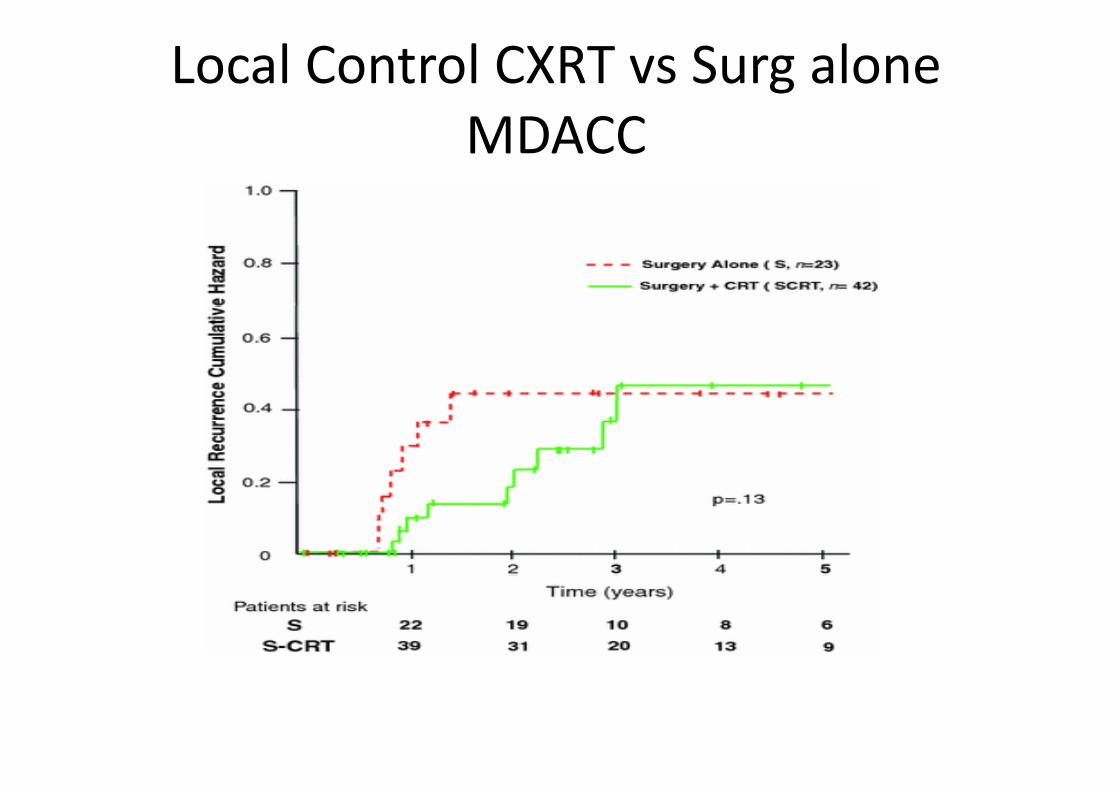
Local Control CXRT vs Surg aloneMDACCMDACC
Borghero Y, Crane et al Ann Surg Onc 2008

Overall Survival CXRT vs Surg aloneMDACC
Median OS
42 mo ( 26 ‐ 59)42 mo ( 26 59)
38 mo (29 ‐ 48)
Borghero Y, Crane et al Ann Surg Onc 2008
Role of adjuvant therapy in patients with resectable hilar cholangiocarcinoma (HCA)resectable hilar cholangiocarcinoma (HCA)
• Estudos retrospectivos sugerem melhora do controle local, podendo levar a modesto ganho de sobrevida para pacientes com margem positiva, ou linfonodos positivos.
• R0 N0? Seguimento é uma opção• Adjuvant chemotherapy should be considered in patient with node
positive disease.• Quimioterapia seguida de re‐ estadiamento e radioterapia é uma Q p g p
opção defendida por muitos especialistas.
ConclusõesConclusões• Colangiocarcinomas são tumores raros de alta agressividadeColangiocarcinomas são tumores raros de alta agressividade.• Pacientes potencialmente ressecáveis devem ser
encaminhados para tratamento cirúrgico após exaustivoencaminhados para tratamento cirúrgico após exaustivoestadiamento, visando descartar doença extra‐hepática,tendo em vista ser esta a única opção potencialmentecurativa.
• A utilização de terapia multimodal em pacientes operadosd li d iã l idi i lideve ser sempre avaliada em reunião multidisciplinar.
• Para os pacientes com recidiva ou doença localmenteavançada o tratamento sistêmico associado ou nãoavançada, o tratamento sistêmico associado ou nãoradioterapia deve ser a primeira escolha de tratamento.