
CHEST X RAYCHEST X RAY
DR MAGDI AWAD SASIDR MAGDI AWAD SASI
20152015

The Chest X-rayThe Chest X-ray
is probably one of the most commonly is probably one of the most commonly seen plain films, and is one of the seen plain films, and is one of the most difficult to mastermost difficult to master
There are many ways to evaluate the There are many ways to evaluate the chestchest..
A systematic approach is usually the A systematic approach is usually the best One methodbest One method..

What causes the blacks, whites What causes the blacks, whites and grays of an x-ray imageand grays of an x-ray image??
X-ray beams contains x-ray photons of X-ray beams contains x-ray photons of differing energiesdiffering energies
As these photons pass through a As these photons pass through a patientpatient……
Some are absorbed completelySome are absorbed completely
Some penetrated directly to the plain filmSome penetrated directly to the plain film
Some are absorbed partially, andSome are absorbed partially, and
While others are deflected (Scatter)While others are deflected (Scatter)

TissueTissue DensityDensity
A product of the type of tissue and the A product of the type of tissue and the thickness of that tissuethickness of that tissue
Results in differential absorptionResults in differential absorption

Differential AbsorptionDifferential AbsorptionPenetration of the x-ray beam is dependent Penetration of the x-ray beam is dependent on tissue densityon tissue density
Denser object = less penetrationDenser object = less penetration
Less beam striking the film (more Less beam striking the film (more absorption) = absorption) = WHITERWHITER
More beam striking the film = More beam striking the film = BLACKERBLACKER

Glass Test Tube
Air
Fat
Water
Bone + Water
Metal

Differential AbsorptionDifferential AbsorptionBlackBlackAir (Lungs / Trachea / Outside the body)Air (Lungs / Trachea / Outside the body)
Fat (Perirenal fat / Fascial plane)Fat (Perirenal fat / Fascial plane)
Water (Muscle / Organs)Water (Muscle / Organs)
Bone (Bone / Atherosclerotic plaquing)Bone (Bone / Atherosclerotic plaquing)
WhiteWhiteMetal (Fillings / Markers / Ortho devices)Metal (Fillings / Markers / Ortho devices)

Radiographic ImageRadiographic Image
Adjacent structures of similar densities Adjacent structures of similar densities are not visualizedare not visualized
Kidney (water density) against liver Kidney (water density) against liver (water density)(water density)

Radiographic ImageRadiographic Image
Adjacent structures of different Adjacent structures of different densities are visualizeddensities are visualized
Liver (water density) next to Bowel (air Liver (water density) next to Bowel (air density)density)

PA CXR Left Lateral CXR


Normally a PA and Lateral View are obtained. Normally a PA and Lateral View are obtained. By convention on the PA View, the x-rays By convention on the PA View, the x-rays enter the patient posteriorlyenter the patient posteriorly
and exit anteriorlyand exit anteriorly (with the patients chest on (with the patients chest on the film cassette), therefore minimizing the the film cassette), therefore minimizing the cardiac magnificationcardiac magnification . .
On the lateral view, the patients left side is On the lateral view, the patients left side is against the film, therefore the right side against the film, therefore the right side would be magnifiedwould be magnified
How to approach an X-rayHow to approach an X-ray??




Evaluate the lungs Evaluate the lungs (Interstitium, airways and (Interstitium, airways and Pleura)Pleura)::
Inflation statusInflation status Pleural marginsPleural margins Abnormal densities/lucenciesAbnormal densities/lucencies MassesMasses InfiltratesInfiltrates CalcificationsCalcifications Fissure locations and thickness. The RUL Bronchus Fissure locations and thickness. The RUL Bronchus is always higher than the LUL bronchusis always higher than the LUL bronchus . .
Change your attention to the Change your attention to the blood vesselsblood vessels : :
The size, location and distribution (the left The size, location and distribution (the left pulmonary artery usually is higher the right)pulmonary artery usually is higher the right)..
DonDon’’t forget to check the lateral as this is the best t forget to check the lateral as this is the best way to look at the posterior costophrenic recess, way to look at the posterior costophrenic recess, anterior/posterior mediastinum, and help you anterior/posterior mediastinum, and help you localize lesions suspected on the frontal viewlocalize lesions suspected on the frontal view . .

Note the Note the ““Special InterestSpecial Interest”” and often missed areas and often missed areas twicetwice : :
ApicesApices (esp. RUL- where most cancer lives) (esp. RUL- where most cancer lives) PeripheralPeripheral lung margins lung margins Hilar,Hilar, retrocardiac, cardiophrenic and costophrenic retrocardiac, cardiophrenic and costophrenic anglesangles..
Focus attention now to the MediastinumFocus attention now to the Mediastinum : :Evaluate Size, shape, position in both viewsEvaluate Size, shape, position in both views PA/LAT. Attention to the mediastinal linesPA/LAT. Attention to the mediastinal lines
HeartHeart : : Check both PA/LAT views. Size, shape, and Check both PA/LAT views. Size, shape, and
silhouette. Look for any chamber silhouette. Look for any chamber enlargement. Evaluate course of Aorta and enlargement. Evaluate course of Aorta and position of arch, Pulmonary Arteriesposition of arch, Pulmonary Arteries . .Margin of SVC (frontal View)Margin of SVC (frontal View) . .

““ATMLL” Search PatternATMLL” Search Pattern
RememberRemember
A = AbdomenA = Abdomen
T = ThoraxT = Thorax
M = MediastinumM = Mediastinum
L = Lungs (unilaterally)L = Lungs (unilaterally)
L = Lungs (bilaterally)L = Lungs (bilaterally)


Structures Visualized:
Stomach gas bubble
Splenic flexure
Liver
Hemidiaphragms
Abdomen dz that can mimic Lung disease include:
Subphrenic abscess
Diaphragmatic hernia
Hiatal Hernia

Searching the Bony “ThoraxSearching the Bony “Thorax””Start at the right base, look at the soft Start at the right base, look at the soft tissues of the chest wall, ribs, spine and tissues of the chest wall, ribs, spine and shoulder girdleshoulder girdle
Go up one side and come down on opposite Go up one side and come down on opposite sideside
RememberRemember::Posterior ribs descend medial to lateralPosterior ribs descend medial to lateralAnterior ribs descend lateral to medialAnterior ribs descend lateral to medial


Searching the “MediastinumSearching the “Mediastinum””
An organized search of the An organized search of the mediastinum is complicated because mediastinum is complicated because of all the overlapping structuresof all the overlapping structures..
Start with a global look for contour Start with a global look for contour abnormalities, then follow with a abnormalities, then follow with a more detailed searchmore detailed search
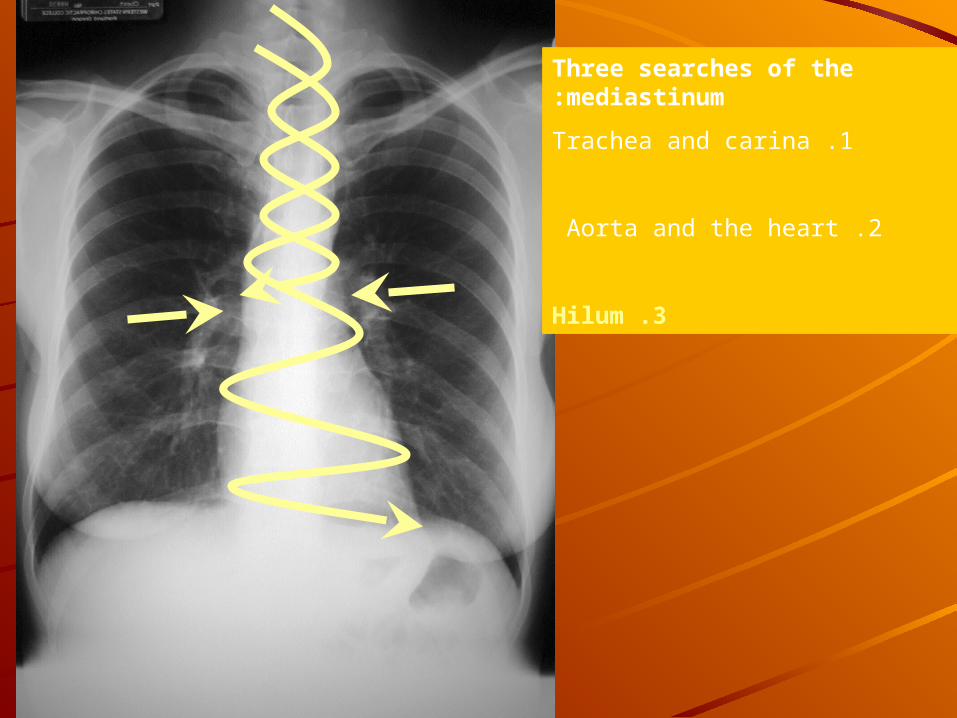
Three searches of the mediastinum:
1 .Trachea and carina
2 .Aorta and the heart
3 .Hilum
Three searches of the mediastinum:
1 .Trachea and carina
2 .Aorta and the heart
3 .Hilum
Three searches of the mediastinum:
1 .Trachea and carina
2 .Aorta and the heart
3 .Hilum
Three searches of the mediastinum:
1 .Trachea and carina
2 .Aorta and the heart
3 .Hilum
Searching the “LungsSearching the “Lungs””Since most chest x-rays are ordered to Since most chest x-rays are ordered to evaluated for lung disease, so the lungs evaluated for lung disease, so the lungs are examined lastare examined last..
They are important, so their evaluation They are important, so their evaluation should be more through, therefore we should be more through, therefore we evaluate them twiceevaluate them twice..
Once individuallyOnce individuallySecond time comparing right and leftSecond time comparing right and left


Structures Visualized:
Costophrenic angles
Lung fields
Pulmonary vasculature
Right minor fissure

Search Pattern:
Abdomen
Thoracic cage and bones
Mediastinum
Lungs
Search Pattern:
Abdomen
Thoracic cage and bones
Mediastinum
Lungs
Search Pattern:
Abdomen
Thoracic cage and bones
Mediastinum
Lungs
Search Pattern:
Abdomen
Thoracic cage and bones
Mediastinum
Lungs
Search Pattern:
Abdomen
Thoracic cage and bones
Mediastinum
Lungs

Vessels
Aortic Arch
Pulmonary Artery
Left Atrium
Left Ventricle
Inferior Vena Cava
Right Atrium
Ascending Aorta
Superior Vena Cava

Descending Aorta
Aortic Knob/Arch
Ascending Aorta
Right Ventricle
Inferior Vena Cava
Left Ventricle
Left Atrium

Upper
Middle
Lower
Lung Fields
Let’s look at the normal Lung Structures

Lateral Costophrenic Sulci
(Recesses, Angles)
Cardiophrenic Sulci
(Recesses, Angles

What to look forWhat to look for……Abnormal densityAbnormal density
Usually air versus waterUsually air versus water
Abnormal shapeAbnormal shapeLung fieldLung fieldMediastinumMediastinum
Abnormal sizeAbnormal sizeLung fieldLung fieldMediastinumMediastinum
Abnormal locationAbnormal locationHemidiaphragm, hila, mediastinum, trachea, Hemidiaphragm, hila, mediastinum, trachea, fissure, vasculaturefissure, vasculature








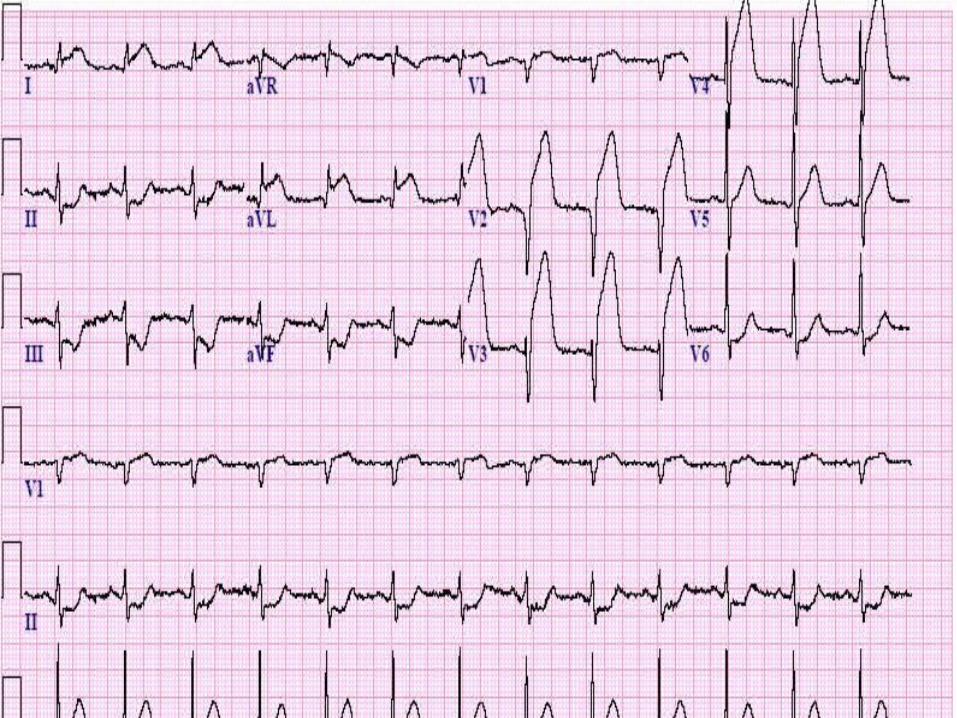
Forty-eight year-old male with longstanding Forty-eight year-old male with longstanding moderately severe aortic insufficiency due to moderately severe aortic insufficiency due to past endocarditis. When the volume of the past endocarditis. When the volume of the regurgitant fraction is significant, there is regurgitant fraction is significant, there is
enlargement of the left ventricle and, enlargement of the left ventricle and, therefore, a globular widening of the cardiac therefore, a globular widening of the cardiac
silhouettesilhouette . .
A CASE OF LVHA CASE OF LVH


congestion


opacity


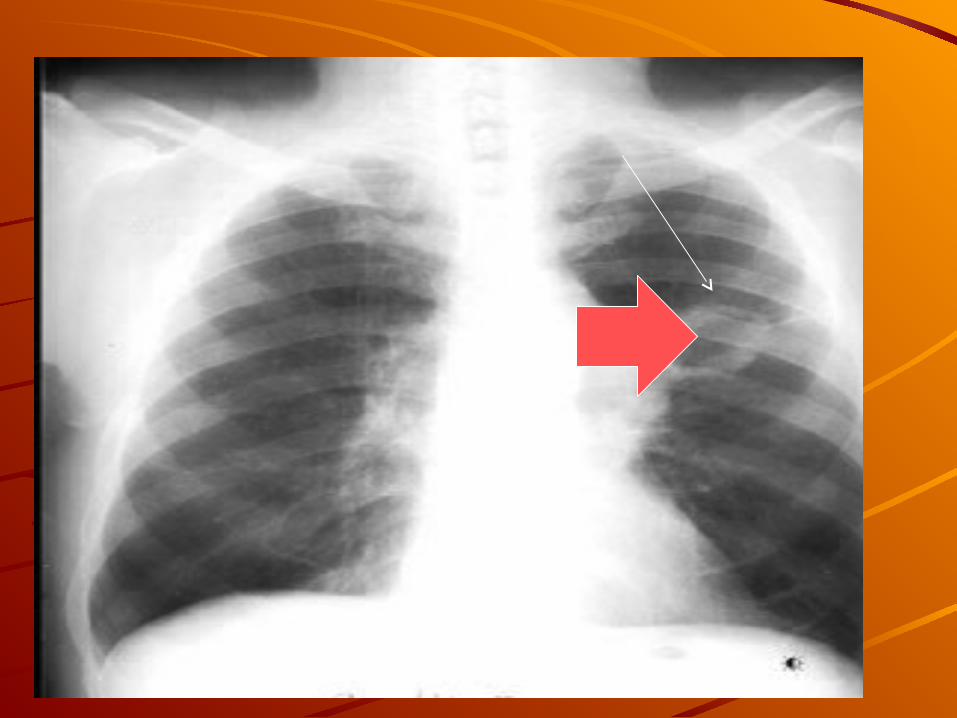
CAVITYCAVITY
Hole in lung with a wall, lumen and contents. Focus of Hole in lung with a wall, lumen and contents. Focus of increased density whose central portion has beenincreased density whose central portion has been replaced by aireplaced by airrFollowing characteristics help in differential diagnosisFollowing characteristics help in differential diagnosisNumberNumber Multiple bilateral cavitiesMultiple bilateral cavities would raise suspicion for would raise suspicion for either bronchogenous or hematogenous either bronchogenous or hematogenous process.process. Hematogenous lesions usually have sharp Hematogenous lesions usually have sharp margins because they are located in the interstitium. margins because they are located in the interstitium. Bronchogenous cavities , the margins are shaggyBronchogenous cavities , the margins are shaggy . .
::BronchogenousBronchogenous 11..Aspiration lung abscessAspiration lung abscess
22..Coccidiomycosis, TuberculosisCoccidiomycosis, Tuberculosis 33..BronchiectasisBronchiectasis 44..HematogenousHematogenous
55..Septic emboliSeptic emboli 66..Metastatic lesionsMetastatic lesions
77..Vasculitis (Wegners granulomatosis)Vasculitis (Wegners granulomatosis)
Single cavitySingle cavityPrimary lung cancerPrimary lung cancer Post traumatic lung cystPost traumatic lung cyst Many other diseasesMany other diseases SizeSizeA large cavity encompassing the entire lobe or lung A large cavity encompassing the entire lobe or lung should raise suspicion forshould raise suspicion for gangrene of lunggangrene of lung LocationLocation
Classical locations for aspiration lung abscess areClassical locations for aspiration lung abscess are superior of lower lobes and axillary sub segments ofof lower lobes and axillary sub segments of anterior and posterior segments of upper lobesanterior and posterior segments of upper lobes . .
Tuberculous cavities are common in superior segments of Tuberculous cavities are common in superior segments of upper and lower lobesupper and lower lobes . .
When a cavity in anterior segment is encountered, a strong When a cavity in anterior segment is encountered, a strong suspicion for lung cancer should be raised. TB and suspicion for lung cancer should be raised. TB and aspiration lung abscess are rare in anterior segmentsaspiration lung abscess are rare in anterior segments
Cancer lung can occur in any segmentCancer lung can occur in any segment


Wall ThicknessWall ThicknessThick walls Lung abscessLung abscess Necrotizing squamous cell lung cancerNecrotizing squamous cell lung cancer Wegners granulomatosisWegners granulomatosis BlastomycosisBlastomycosis
Thin walledThin walledCoccidiomycosisCoccidiomycosis
Metastatic cavitating squamous cell carcinoma from Cervixfrom Cervix M. Kansasii infectionM. Kansasii infection Congenital or acquired bullaeCongenital or acquired bullae Posttraumatic cystsPosttraumatic cysts Open negative TBOpen negative TB
Lining of wallLining of wall
The lining of wall is irregular and nodular inThe lining of wall is irregular and nodular in cancer lung or shaggy in lung abscessor shaggy in lung abscess . The . The appearance is akin toappearance is akin to
stalactites and stalagmitesstalactites and stalagmites

EtiologyEtiologyCavity can be encountered in practically most lung diseasesCavity can be encountered in practically most lung diseases
Primary Lung CancerPrimary Lung Cancer Thick wall Shaggy lumen Eccentric cavitation Necrotizing PneumoniaNecrotizing Pneumonia
Lung abscessLung abscess Gravity dependant segmentsGravity dependant segments Thick wallThick wall Air-fluid levelsAir-fluid levels TuberculosisTuberculosis Superior segmentsSuperior segments Infiltrate aroundInfiltrate around BilateralBilateral Fungal infectionsFungal infections AspergillusAspergillus Fungous ballFungous ball Sub acute invasive aspergillosisSub acute invasive aspergillosis
Metastatic diseaseMetastatic disease Thin walledThin walled ( (Squamous cellSquamous cell)) Thick walThick walll ( (AdenocaAdenoca))



ConsolidationConsolidation
The following are radiological criteria to call a The following are radiological criteria to call a shadow on CXR ----consolidationshadow on CXR ----consolidation
: :Lobar or Segmental DensityLobar or Segmental Density : :The density should either correspond to the lobe or The density should either correspond to the lobe or
lung segmentlung segment Air BronchogramAir Bronchogram::
Presence of air bronchogram would confirm an Presence of air bronchogram would confirm an alveolar processalveolar process..No Loss of Lung VolumeNo Loss of Lung Volume
Lung volumes increase in early stages of Lung volumes increase in early stages of consolidation. In later stages there can be some consolidation. In later stages there can be some amount of loss of lung volume due to secretions amount of loss of lung volume due to secretions obstructing airways. As a general rule, there is no obstructing airways. As a general rule, there is no significant loss of lung volume in consolidationsignificant loss of lung volume in consolidation

The 'silhouette' signThe 'silhouette' signThe silhouette sign is a misnomer! It should be The silhouette sign is a misnomer! It should be called the 'loss of silhouette' sign. Normal called the 'loss of silhouette' sign. Normal adjacent anatomical structures of differing adjacent anatomical structures of differing densities form a crisp 'silhouette,' or contour. densities form a crisp 'silhouette,' or contour. Loss of a specific contour can help determine the Loss of a specific contour can help determine the position of a disease processposition of a disease process . .
For example, the heart (a soft tissue density For example, the heart (a soft tissue density structure - near white) lies adjacent to lung tissue structure - near white) lies adjacent to lung tissue (near air density - near black). A crisp contour or (near air density - near black). A crisp contour or 'silhouette' is formed at the interface of these two 'silhouette' is formed at the interface of these two tissue densities. Loss of clarity of the right heart tissue densities. Loss of clarity of the right heart contour (formed by the right atrium) implies contour (formed by the right atrium) implies disease of the right middle lobe which lies next to disease of the right middle lobe which lies next to the right atrium. Loss of distinction of the left the right atrium. Loss of distinction of the left heart contour indicates an abnormality of the heart contour indicates an abnormality of the lingula (part of the left upper lobe which wraps lingula (part of the left upper lobe which wraps over the left ventricleover the left ventricle))..

Air bronchogramAir bronchogram

Consolidation / Left Lower LobeConsolidation / Left Lower Lobe
Density in left lower lung fieldDensity in left lower lung field
Left heart silhouette intactLeft heart silhouette intact
Loss of diaphragmatic silhouetteLoss of diaphragmatic silhouette
No shift of mediastinumNo shift of mediastinum
Blunting of costophrenic angleBlunting of costophrenic angle



Lobar Pneumonia Right Middle LobeLobar Pneumonia Right Middle Lobe Vague density right lower lung fieldVague density right lower lung field Indistinct right cardiac silhouetteIndistinct right cardiac silhouette Intact diaphragmatic silhouetteIntact diaphragmatic silhouette LateralLateralDensity corresponding to RMLDensity corresponding to RML No loss of lung volumeNo loss of lung volume Air bronchogram (not demonstrable in this Air bronchogram (not demonstrable in this presentationpresentation))


Atelectasis is the loss of lung volume and Atelectasis is the loss of lung volume and therefore a direct sign is the displacement therefore a direct sign is the displacement of interlobular fissures. Generally this is of interlobular fissures. Generally this is accompanied by increased density and accompanied by increased density and possibly elevation of the hemidiaphragm, possibly elevation of the hemidiaphragm, mediastinal displacement, or mediastinal displacement, or compensatory over-inflation. If there has compensatory over-inflation. If there has been resorption of air within the been resorption of air within the atelectatic segment, there is generally an atelectatic segment, there is generally an absence of air bronchogramsabsence of air bronchograms






Mitral stenosis generally creates a Mitral stenosis generally creates a characteristic configuration dominated by characteristic configuration dominated by enlargement of the left atrium. Note that enlargement of the left atrium. Note that the left mainstem bronchus is elevated the left mainstem bronchus is elevated and lies more horizontal than normal. The and lies more horizontal than normal. The tissue boundary angulated away from the tissue boundary angulated away from the spinal column below the left mainstem spinal column below the left mainstem bronchus represents the lateral boundary bronchus represents the lateral boundary
of the enlarged left atriumof the enlarged left atrium. . MoreMore......





Diffuse Alveolar DiseaseDiffuse Alveolar Disease Radiological SignsRadiological SignsButterfly distribution / Medullary distributionButterfly distribution / Medullary distribution Lobar or segmental distributionLobar or segmental distribution Air bronchogramAir bronchogram AlveologramAlveologram Patchy, confluent shadowsPatchy, confluent shadows Soft fluffy edgesSoft fluffy edges Acinar nodulesAcinar nodules Rapid changesRapid changes No significant loss of lung volumeNo significant loss of lung volume Ground glass appearance on HRCTGround glass appearance on HRCT

Useful Clinical ClassificationUseful Clinical Classification::AcuteAcute ChronicChronic Acute Diffuse Alveolar DiseaseAcute Diffuse Alveolar DiseaseWaterWater Pulmonary edema - CardiogenicPulmonary edema - Cardiogenic Neurogenic pulmonary edemaNeurogenic pulmonary edema
BloodBlood SLESLE Goodpasture's syndromeGoodpasture's syndrome Idiopathic pulmonary hemosiderosisIdiopathic pulmonary hemosiderosis Wegener's granulomatosisWegener's granulomatosis
InflammatoryInflammatory Cytomegalovirus pneumoniaCytomegalovirus pneumonia Pneumocystis carinii pneumoniaPneumocystis carinii pneumonia InfluenzaInfluenza Chicken pox pneumoniaChicken pox pneumonia Fat embolismFat embolism Amniotic fluid embolismAmniotic fluid embolism Adult respiratory distress syndromeAdult respiratory distress syndrome
Chronic Alveolar DiseaseChronic Alveolar Disease::Alveolar proteinosisAlveolar proteinosis Alveolar cell carcinomaAlveolar cell carcinoma Mineral oil pneumoniaMineral oil pneumonia Alveolar form of sarcoidosisAlveolar form of sarcoidosis Alveolar form of lymphomaAlveolar form of lymphoma Alveolar form of tuberculosisAlveolar form of tuberculosis Alveolar metastases from cancer of the Alveolar metastases from cancer of the pancreaspancreas Desquamative interstitial pneumoniaDesquamative interstitial pneumonia



Milary TuberculosisMilary TuberculosisInterstitial nodulesInterstitial nodules
Uniform sizeUniform size Sharper edgesSharper edges

BILATERAL LYMPHADENOPATHYBILATERAL LYMPHADENOPATHY




HoneycombingHoneycombing
Seen in end stage lung diseaseSeen in end stage lung disease
Indicative of diffuse interstitial fibrosisIndicative of diffuse interstitial fibrosis
Due to bronchiolectasiaDue to bronchiolectasia
Most of the time in basesMost of the time in bases
Upper lobe distribution seen inUpper lobe distribution seen in
eosinophilic granulomaeosinophilic granuloma

RFTRFT
Case 1 UREA = 250mgCase 1 UREA = 250mg
CREATININE=14mgCREATININE=14mg
SERUM K = 6.6mmolSERUM K = 6.6mmol
SERUM Na = 145 mmolSERUM Na = 145 mmol
Case 2 UREA = 110mgCase 2 UREA = 110mg
CREATININE = 4mgCREATININE = 4mg
SERUM K = 4.4mmolSERUM K = 4.4mmol
SERUM Na = 155mmolSERUM Na = 155mmol


LFTLFTSGOTSGPT
S. ALBUMIND.BILIRUBIN TIME PROTHROMBIN
4OO IU650 IU
4.2 gm 8 mg 12 14 sec
40 IU 30 IU
2.2 gm 2 mg 12 18 sec
250 IU 360 IU
3.5 gm 6 mg 12 14 sec
20 IU 35 IU
3.9 gm 12.4 mg 12 20 secALP 540 IU

BLOODBLOODHBWBCPLATELE
TMCV 80–100
fL
MCH 27 to 31 picograms/cell
MCHC32 to 36
g/dL
5 GM4.5 X103/cmm
650 x103/cmm
24 25 24
4 GM 2.5 X 103/cmm
50 X103/cmm
35 32 34
8 GM125 X 103 /cmm
550x103/cmm
27 29 32

THANKSTHANKS







