
Michael M. Goldberg, M.D.Michael M. Goldberg, M.D.Chairman and CEO
EMISPHERE TECHNOLOGIES, INC.EMISPHERE TECHNOLOGIES, INC.
New York Palace HotelNovember 7-9, 2005

The statements in this presentation and oral statements made by The statements in this presentation and oral statements made by representatives of the Company relating to matters that are not representatives of the Company relating to matters that are not historical facts, including, but without limitation, those regarhistorical facts, including, but without limitation, those regarding ding the timing or potential outcomes of clinical trials and any markthe timing or potential outcomes of clinical trials and any market et that might develop for any of the Company’s product candidates that might develop for any of the Company’s product candidates are forwardare forward--looking statements that involve risks and uncertainties looking statements that involve risks and uncertainties including, but not limited to, the likelihood that any product iincluding, but not limited to, the likelihood that any product in the n the research pipeline can receive regulatory approval in the United research pipeline can receive regulatory approval in the United States or abroad, the ability of Emisphere and/or its partners tStates or abroad, the ability of Emisphere and/or its partners to o develop, manufacture and commercialize products using the develop, manufacture and commercialize products using the Company’s drug delivery technology, Emisphere’s ability to fund Company’s drug delivery technology, Emisphere’s ability to fund such efforts with or without partners, and other risks and such efforts with or without partners, and other risks and uncertainties detailed in the Company’s filings with the Securituncertainties detailed in the Company’s filings with the Securities ies and Exchange Commission.and Exchange Commission.
Safeharbor StatementSafeharbor Statement

PipelinePipeline
NovartisNovartis•• Salmon Calcitonin:Salmon Calcitonin:
Two major clinical programs: Osteoporosis Two major clinical programs: Osteoporosis and Osteoarthritisand Osteoarthritis
•• rhGHrhGH::Potential for Fast Track clinical developmentPotential for Fast Track clinical development
RocheRocheSmall molecule compounds for bone related Small molecule compounds for bone related diseasesdiseases
Novartis/LillyNovartis/Lilly•• PTHPTH

PipelinePipeline (Cont(Cont’’d)d)EmisphereEmisphere•• Heparin:Heparin:
Closest Emisphere product to market Closest Emisphere product to market Completed Phase III protocol discussions with FDA Completed Phase III protocol discussions with FDA
•• Insulin:Insulin:Potential to revolutionize diabetes treatmentPotential to revolutionize diabetes treatmentPhase II study beginningPhase II study beginning
As of 6.30.05As of 6.30.05: 80 U.S. patents issued and 63 U.S. patent applications pending: 80 U.S. patents issued and 63 U.S. patent applications pending
OthersOthers•• AcyclovirAcyclovir•• GLPGLP--1, rhGH, and PYY (Obesity):1, rhGH, and PYY (Obesity):•• Various preVarious pre--clinical undisclosed clinical undisclosed
programs programs
Why Focus on Oral Drugs?Why Focus on Oral Drugs?•• Compelling Market OpportunitiesCompelling Market Opportunities
Therapeutic areas with large underserved Therapeutic areas with large underserved patient populationspatient populations
Strong attraction to major Strong attraction to major pharmaspharmas to expand to expand markets for, and extend patent lives of markets for, and extend patent lives of existing drugsexisting drugs
•• Therapeutic Peptides and ProteinsTherapeutic Peptides and ProteinsLower toxicology and safety issues compared Lower toxicology and safety issues compared to small moleculesto small molecules
Oral delivery enhances existing drug productsOral delivery enhances existing drug products

•• Broadly applicable proprietary drug Broadly applicable proprietary drug delivery technologydelivery technology
•• Shown safe in over 100,000 human Shown safe in over 100,000 human dosingsdosings
•• Does not chemically alter the drug Does not chemically alter the drug moleculemolecule
•• Enables practical dosage formsEnables practical dosage forms•• Low cost and easy to scaleLow cost and easy to scale
eeliligegenn®® TechnologyTechnology

Therapeutic AreasTherapeutic Areas
•• Coagulation/DVT Coagulation/DVT –– Heparin Heparin -- $4 billion market$4 billion market
•• Diabetes Diabetes –– Insulin Insulin -- $6 billion market$6 billion market
•• Osteoporosis Osteoporosis –– Calcitonin, PTH, Other Calcitonin, PTH, Other -- $6 billion $6 billion marketmarket
•• Growth Disorders Growth Disorders –– rhGHrhGH -- $2 billion market$2 billion market
•• Osteoarthritis Osteoarthritis –– Calcitonin Calcitonin -- $2+ billion market$2+ billion market
•• Obesity Obesity –– GLPGLP--1, 1, rhGHrhGH, and PYY, and PYY

•• eeliligegenn®® technology uses a carrier to technology uses a carrier to enable drug transport across biological enable drug transport across biological membranes.membranes.
Does not change the composition of the drugDoes not change the composition of the drug
Provides a weak physical interactionProvides a weak physical interaction
•• eeliligengen®® technology transports drug technology transports drug passively and passively and transcellularlytranscellularly without without compromising cell integritycompromising cell integrity
Maintains membrane structural integrity Maintains membrane structural integrity
Maintains integrity of tight junctionsMaintains integrity of tight junctions
Mechanism of ActionMechanism of Action

Partnered Partnered and Feasibility and Feasibility ProgramsPrograms

Salmon CalcitoninSalmon Calcitonin•• Indication:Indication: OsteoporosisOsteoporosis
Novartis published Phase IIa study consisting of 277 Novartis published Phase IIa study consisting of 277 subjects treated for 3 months and achieving statistically subjects treated for 3 months and achieving statistically significant results significant results Phase III studies scheduled to begin 1/06Phase III studies scheduled to begin 1/06
•• Indication:Indication: OsteoarthritisOsteoarthritisSuppresses cartilage degradationSuppresses cartilage degradationProvides pain reliefProvides pain reliefPhase III studies scheduled to begin 1/06Phase III studies scheduled to begin 1/06Phase II study completed Phase II study completed –– results to be presented in results to be presented in DecemberDecember

- - - - -
0 -
-10 -
-20 -
-30 -
-40 -
-50 -
PLB 0.15mg 0.4mg 1.0mg 2.5mg
Oral Salmon Calcitonin Induced Suppression of Urinary Collagen Type II Degradation in Postmenopausal Women: A New Potential Treatment of Osteoarthritis
Urinary CTX-I
Treatment Group
Urinary CTX-II
Treatment Group- - - - -
0 -
-10 -
-20 -
-30 -
-40 -
-50 -
PLB 0.15mg 0.4mg 1.0mg 2.5mg
% C
hang
e in
U-C
TX-I
from
bas
elin
e
% C
hang
e in
U-C
TX-II
from
bas
elin
e
**
****
**
* * p<0.05; ** ** p<0.005 compared with placebo
** **** **
2626 3232 3434 3131 2929

Partnered Program: Partnered Program: rhGHrhGH•• Novartis clinical formulation ready for testingNovartis clinical formulation ready for testing
•• Demonstrated delivery in humansDemonstrated delivery in humans
•• Novartis to pay all development costs Novartis to pay all development costs and conduct clinical trialsand conduct clinical trials
•• Multiple dose human study to begin Q1 2006Multiple dose human study to begin Q1 2006
•• Growth Hormone clinical uses increasingGrowth Hormone clinical uses increasingHGH HGH TrmtTrmt Reduces Abdominal Visceral Fat in Reduces Abdominal Visceral Fat in Postmenopausal Women with Abdominal Obesity: Postmenopausal Women with Abdominal Obesity: A 12 Month PlaceboA 12 Month Placebo--Controlled TrialControlled Trial Journal of Clinical Journal of Clinical Endocrinology & Metabolism 90(3):1466Endocrinology & Metabolism 90(3):1466--14741474

Partnered Program:Partnered Program: Small Molecule Small Molecule Compounds for Bone Related DiseasesCompounds for Bone Related Diseases
•• Roche agreement follows successful preRoche agreement follows successful pre--clinical clinical studies and a successful human study conducted studies and a successful human study conducted by Rocheby Roche
•• Roche to pay all development costs and conduct Roche to pay all development costs and conduct clinical trialsclinical trials
•• Roche to fund long term toxicology studies Roche to fund long term toxicology studies
•• Clinical testing of Roche developed formulations Clinical testing of Roche developed formulations completecomplete
•• Worldwide product sales for class > $5BnWorldwide product sales for class > $5Bn

•• Indication: OsteoporosisIndication: OsteoporosisReverses bone lossReverses bone loss
•• Status: Completed several human studiesStatus: Completed several human studies
•• Previously licensed to Lilly; Lilly blocking Previously licensed to Lilly; Lilly blocking EMIS retrieval of the programEMIS retrieval of the program
Litigation status: Arguments completed 2/9/05; Litigation status: Arguments completed 2/9/05; awaiting court decisionawaiting court decision
•• Option granted to Novartis for $10 million Option granted to Novartis for $10 million investment, to license the program upon investment, to license the program upon successful retrieval from Lillysuccessful retrieval from Lilly
Partnered Program: PTH 1Partnered Program: PTH 1--3434

Registration of Oral Registration of Oral Products Incorporating Products Incorporating Emisphere’s Carrier Emisphere’s Carrier Technology via a Technology via a 505(b)(2) NDA filing 505(b)(2) NDA filing StrategyStrategy

Test Case of 505(b)2
• SNAC Carrier has near complete Tox package• Acyclovir is off patent• Acyclovir absorption is variable with low
bioavailability• Acyclovir dosing large multiple tablets, multiple
times per day • Prodrug of Acyclovir – Valtrex is premium priced
product
Could Emisphere create an improved oral Acyclovir and file under 505(b)2 for registration?
SNACSNAC / Acyclovir
Could Oral SNAC/Acyclovir be approved Could Oral SNAC/Acyclovir be approved under 505(b)2 to compete with Valtrex?under 505(b)2 to compete with Valtrex?

Acyclovir•• Emisphere has received written Emisphere has received written
confirmation from FDA that 505(b)(2) confirmation from FDA that 505(b)(2) is acceptable for Acycloviris acceptable for Acyclovir
•• FDA is still formulating policy for FDA is still formulating policy for protein productsprotein products
•• Analogous situations for other Analogous situations for other candidatescandidates
sNDAsNDA –– Roche’s small moleculeRoche’s small moleculeReduced Phase III patient populations Reduced Phase III patient populations -- HeparinHeparin

Heparin ProgramHeparin Program

Heparin MarketHeparin Market
•• Market at over $3 billion for Market at over $3 billion for injectableinjectable forms forms and growing ~ 15% annually and growing ~ 15% annually
Estimate of peak sales for Exanta was $4 billionEstimate of peak sales for Exanta was $4 billion
•• Used to prevent and treat blood clotsUsed to prevent and treat blood clots•• Oral form would expand the market Oral form would expand the market
for heparinfor heparin•• Significant ongoing investment by Pharma Significant ongoing investment by Pharma
industry to create small molecule drugs that industry to create small molecule drugs that are orally activeare orally active

PROTECT Phase III TrialPROTECT Phase III Trial
2,200 Patient Phase III Trial Initiated in 20002,200 Patient Phase III Trial Initiated in 2000•• PurposePurpose:: Evaluate safety and efficacy of liquid oral Evaluate safety and efficacy of liquid oral
heparin formulation for DVT prevention following heparin formulation for DVT prevention following total hip replacement surgerytotal hip replacement surgery
•• GoalGoal:: Demonstrate superior efficacy and Demonstrate superior efficacy and comparable safety of 30 day dosing of liquid comparable safety of 30 day dosing of liquid heparin vs. 10 day dosing of heparin vs. 10 day dosing of injectableinjectable LOVENOX LOVENOX
•• Detection MethodDetection Method:: VenogramVenogram 30 days following 30 days following surgerysurgery
•• ConclusionConclusion:: Safe mechanism and effective carrier, Safe mechanism and effective carrier, but liquid formulation not ready for but liquid formulation not ready for ““prime timeprime time””

000Fatal Bleeds
3/145/200/14Major/TotalBleeds
7%4% (p=0.013)7%SAEs
01*1*HIT* = not attributed to study drug per protocol; HIT = 0 in patients not receiving prohibited injectable heparin
Injectable LOVENOX®
30 mg (10-day treatment regimen)
N=716
High dose oral-heparin
90,000 units/2.25g SNAC (30-day
treatment regimen)N=736
Low dose oral-heparin
60,000 units/1.5g SNAC (30-day
treatment regimen)N=728
PROTECT Phase III ResultsPROTECT Phase III ResultsSafety Analysis ITT Population

55%4%Relative risk reduction
28%18%27%Total DVT’s)
Injectable LOVENOX®30 mg (10-day treatment regimen)
High dose oral-heparin90,000 units/2.25g SNAC (30-day treatment regimen)
Low dose oral-heparin60,000 units/1.5g SNAC (30-day treatment regimen)
USA/Canada/ Australia
USA/Canada/Australia SitesUSA/Canada/Australia Sites(Post(Post--hoc Analysis)hoc Analysis)
ITTIV population (ITTIV population (N = 299)N = 299)
Oral Heparin: PROTECTOral Heparin: PROTECT

Emisphere Oral Heparin
Emisphere softgel capsule
Emisphere tablet
Multi-Vitamin

Heparin SC Injection vs. Oral Heparin/SNAC Heparin SC Injection vs. Oral Heparin/SNAC Solution and Soft Gel CapsSolution and Soft Gel Caps
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
-3 -1 1 3 5 7 9
Time (hours)
anti-
Fact
or X
a (IU
/mL)
7,500 Heparin Units SC
5000 Heparin Units SC
2.4 g SNAC/90,000 Units Heparin (18 mL Soln)
500 mg SNAC/75,000 Units Heparin (2 SGC)
1149 mg SNAC/75,000 Units Heparin (3 SGC)

Oral USP Heparin Xa : IIa ratio (n=15)Oral USP Heparin Xa : IIa ratio (n=15)
1.071.051.00Ratio
0.150.400.33IIa (IU/ml)
0.160.420.33Xa (IU/ml)
Liquid4.5:1
Capsule2.5:1
Capsule1:1

Equivalence Comparison of Biological Activity
4.1Lovenox 3
3.8Lovenox 2
4.0Lovenox 1
3.7Amphastar 3
3.6Amphastar 2
3.6Amphastar 1
Anti-Xa/Anti-IIa
Xa : IIa RatioXa : IIa RatioAmphastarAmphastar FDA SubmissionFDA Submission

Heparin is Heparin StudyHeparin is Heparin Study
Oral delivery of heparin does not alter the Oral delivery of heparin does not alter the heparin as compared with injecting the heparin as compared with injecting the heparin (either iv or sc)heparin (either iv or sc)
•• Biologically Biologically –– Shaker A. Shaker A. MousaMousa, Ph.D., Ph.D. Albany Albany College of PharmacyCollege of Pharmacy
APTT, antiAPTT, anti--Xa, antiXa, anti--IIa, and TFPIIIa, and TFPI
•• Chemically Chemically –– Robert J. Robert J. LinhardtLinhardt, Ph.D., RPI, Ph.D., RPIStructural evaluation on the oligosaccharide components Structural evaluation on the oligosaccharide components in the mixtures.in the mixtures.Quantification and comparison of the molecular Quantification and comparison of the molecular configurations between the heparin administered orally configurations between the heparin administered orally and the heparin administered intravenously and sc.and the heparin administered intravenously and sc.
•• Regulatory ImplicationsRegulatory ImplicationsUnknown at presentUnknown at presentCommitment from FDA to modify clinical demands Commitment from FDA to modify clinical demands upon review of data generatedupon review of data generated

What’s New in the Heparin MarketWhat’s New in the Heparin Market
•• Generic Generic LMWHsLMWHsLovenox Lovenox -- AmphastarAmphastar, , TevaTeva, , MomentaMomenta, , Aventis(?)Aventis(?)
•• Modified HeparinsModified HeparinsNeurochemNeurochem –– Alzheimer'sAlzheimer'sKeryxKeryx –– ProteinuriaProteinuria
•• Clinical UsageClinical UsageExtended Prophylaxis Extended Prophylaxis –– Medical ptsMedical ptsOncologyOncology
•• CompetitionCompetitionOral Direct Xa and IIa (thrombin) inhibitorsOral Direct Xa and IIa (thrombin) inhibitors

•• Solid dosage formSolid dosage formConvenient, tasteless, and well toleratedConvenient, tasteless, and well tolerated
•• Method of endpoint detectionMethod of endpoint detectionUltrasound/nonUltrasound/non--invasive vs. invasive vs. venogramvenogram/invasive/invasive
•• Trial designTrial design –– Fewer centers and U.S. basedFewer centers and U.S. based•• ComparatorComparator –– CoumadinCoumadin vs. Lovenoxvs. Lovenox•• EndpointEndpoint –– NonNon-- inferiority vs. Superiorityinferiority vs. Superiority•• Less ExpensiveLess Expensive -- Especially if oral heparin vs. Especially if oral heparin vs.
sc and IV study successfulsc and IV study successful
Leveraging Our ExperienceLeveraging Our Experience

Insulin ProgramInsulin Program

•• 177 million diabetics worldwide 177 million diabetics worldwide
•• 95% are Type 2 diabetics95% are Type 2 diabetics
•• 40% of Type 2 diabetics use insulin 40% of Type 2 diabetics use insulin to control the diseaseto control the disease
•• 2004 worldwide sales of 2004 worldwide sales of injectableinjectableinsulinsinsulins are estimated at $6 billion are estimated at $6 billion
Insulin MarketInsulin Market

Insulin as a DrugInsulin as a Drug• Physiologic hormone for glucose
homeostasis• No upper dose limit (exc. hypoglycemia)• No limit to degree of A1C lowering • Rapid glycemic response• No non-responders• Durable glycemic control• No transitional loss of control
Virtues of Insulin

Percentage of Patients with Percentage of Patients with Diabetes Having A1C<7%Diabetes Having A1C<7%
Effectiveness of Current Therapies

Why Does Insulin Therapy Fail?Why Does Insulin Therapy Fail?
• Patient adherence and compliance
• Hypoglycemia and weight gain concerns
• Non-physiological pharmacokinetics
• Insulin as “Last Resort” therapy
• Parenteral insulin targets primarily muscle and fat, NOT liver
Shortcomings of Insulin Therapy

Physiologic Glucoregulation by InsulinPhysiologic Glucoregulation by Insulin

EnteralEnteral & & ParenteralParenteral InsulinInsulin--Both Important!Both Important!Enteral Parenteral

β-CellFunction(%) Postprandial
HyperglycemiaIGT Type 2
DiabetesPhase I Type 2
DiabetesPhase II
Type 2 DiabetesPhase III
25
100
75
0
50
12 -10 -6 -2 0 2 6 10 14
Years From Diagnosis
Glucose Appearance in Plasma After Glucose Appearance in Plasma After Oral Glucose in Type 2 DiabetesOral Glucose in Type 2 Diabetes

Insulin Resistance in Type 2 DiabetesInsulin Resistance in Type 2 Diabetes
Effect on Liver and Peripheral TissuesEffect on Liver and Peripheral Tissues
Adapted from Groop LC et al. Diabetologia 1993;36:1326-1331.

Baseline 4 Months Baseline 4 Months
Mean pl. glucose (mM) 15.0 6.8 14.5 4.8Mean HbA1c 14.8 10.0 13.8 5.5Total insulin IU/day 53 50 52 40Lactate
Pyruvate
Alanine
Glycerol
NEFA
Cortisol
Subcutaneous Infusion Intraportal Infusion
Rationale: Determine feasibility of a new method of intraportal infusion via the umbilical vein in IDDM 12 Patients mean age 24 (22-26) mean weight 66.3kg, mean duration of IDDM >10 years
X = normalized
xxx
x
Comparison of Peripheral and Portal Comparison of Peripheral and Portal Routes of Insulin Infusion in IDDM PatientsRoutes of Insulin Infusion in IDDM Patients
Shishko et al. Diabetes 41:1042, 1992

Efficacy and Safety of Inhaled InsulinEfficacy and Safety of Inhaled Insulin
•• Inhaled Insulin is effective as a stand Inhaled Insulin is effective as a stand alone agent in Type II patients failing diet alone agent in Type II patients failing diet and exerciseand exercise
44% of pts had HbA1c < 7 after 12 weeks of Rx 44% of pts had HbA1c < 7 after 12 weeks of Rx (mean A1c at study start 9.5)(mean A1c at study start 9.5)Dose 15 mg (~400 IU/day)Dose 15 mg (~400 IU/day)Results slightly better than Avandia 4 mg Results slightly better than Avandia 4 mg b.i.d.(rosiglitazoneb.i.d.(rosiglitazone))
•• Safety of Inhaled InsulinSafety of Inhaled Insulin0.7 episodes of hypoglycemia/patient/month 0.7 episodes of hypoglycemia/patient/month (14X Avandia rate)(14X Avandia rate)6% incidence of anti insulin antibodies (0% Avandia)6% incidence of anti insulin antibodies (0% Avandia)2 kg weight gain over 12 weeks (2.4X Avandia)2 kg weight gain over 12 weeks (2.4X Avandia)“Small” changes in pulmonary function observed “Small” changes in pulmonary function observed (FEV(FEV1 1 decline 16X Avandia) decline 16X Avandia)
Diabetes Care, Volume 28, Number 8, August 2005

Emisphere Oral Insulin TabletsEmisphere Oral Insulin Tablets
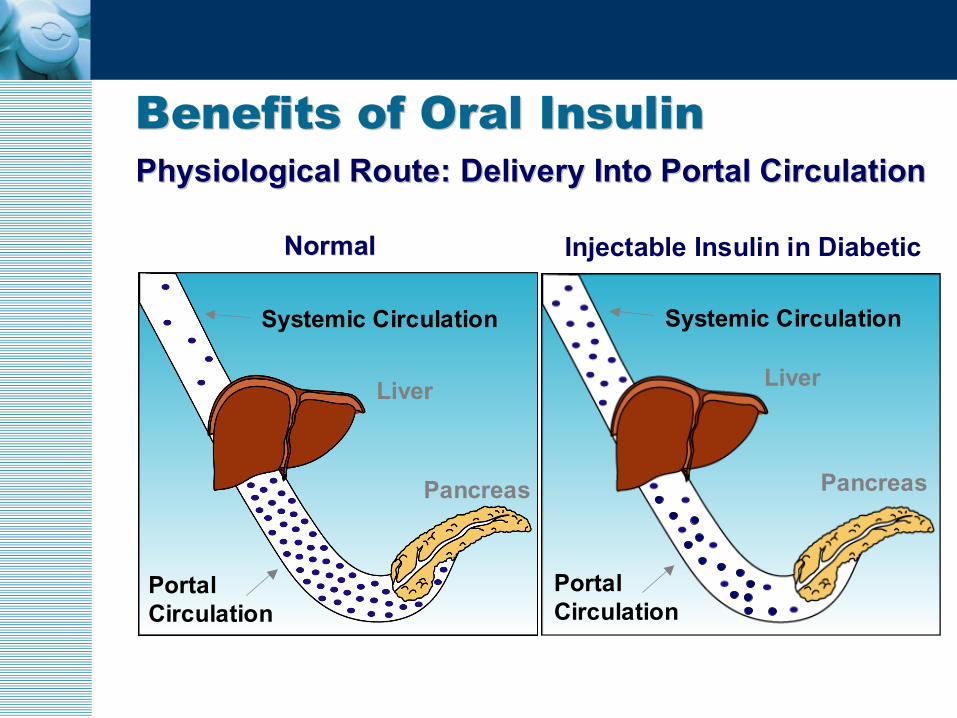
Portal Circulation
Pancreas
Liver
Systemic Circulation
Portal Circulation
Pancreas
Liver
Systemic Circulation
NormalNormal Injectable Insulin in Diabetic
Physiological Route: Delivery Into Portal CirculationPhysiological Route: Delivery Into Portal CirculationBenefits of Oral InsulinBenefits of Oral Insulin

MultiMulti--Dose, 14 Day Tablet StudyDose, 14 Day Tablet StudyRandomized, controlled, doubleRandomized, controlled, double--blind, parallel group blind, parallel group pilot study in pilot study in outout--patient setting in subjects with type 2 patient setting in subjects with type 2 diabetes welldiabetes well--controlled with dietary treatment.controlled with dietary treatment.
•• 1313--patient study (seven treated; six control)patient study (seven treated; six control)•• Each subject received either 300 IU insulin+160 mg carrier or Each subject received either 300 IU insulin+160 mg carrier or
200 mg carrier alone 200 mg carrier alone qidqid (administered as 2 tablets 10 min (administered as 2 tablets 10 min before main meals and before bedtime) over 14 days.before main meals and before bedtime) over 14 days.
•• Evaluated safety, effect and tolerability of oral insulin tabletEvaluated safety, effect and tolerability of oral insulin tablets s •• Key parameters evaluated:Key parameters evaluated:
Serum fructosamineOral glucose toleranceInsulin sensitivity and secretion
Profil Institute

•• EMISPHERE oral insulin tablets positively EMISPHERE oral insulin tablets positively impacted glycemic control in earlyimpacted glycemic control in early--stage type 2 stage type 2 diabetics based on certain key parametersdiabetics based on certain key parameters
•• Oral insulin was wellOral insulin was well--tolerated:tolerated:
No hypoglycemiaNo hypoglycemia
No serious adverse eventsNo serious adverse events
No weight gainNo weight gain
•• Blood glucose excursions were significantly Blood glucose excursions were significantly reduced after tworeduced after two--week treatmentweek treatment
2003 Multi2003 Multi--Dose Study ResultsDose Study Results

2003 Multi2003 Multi--Dose Study ResultsDose Study Results
AUC-BG0-1h[mg * h/dl]
AUC-INS0-1h[µU * h/ml]
HOMA-IR Fructosamine[µmol/l]
OGTTINS-Cmax[µU/ml]
AUC-BGtotal[mg * h/dl]
Triple Meal Test

Oral Insulin Phase II StudyOral Insulin Phase II Study
•• Type 2 Diabetes failing Type 2 Diabetes failing monotherapymonotherapy•• Design Design –– 9090--day double blind placebo controlledday double blind placebo controlled•• Location Location –– India (6 Centers managed by a local India (6 Centers managed by a local
CRO)CRO)•• Subjects on metformin will be randomized to Subjects on metformin will be randomized to
active or placeboactive or placebo•• Active: Tablets each containing 150U of Insulin and 80 Active: Tablets each containing 150U of Insulin and 80
mg of carrier + metforminmg of carrier + metformin•• Control: Placebo + metforminControl: Placebo + metformin
•• Number of Subjects: 120Number of Subjects: 120•• Efficacy Endpoints: HbA1c, glycemic control, Efficacy Endpoints: HbA1c, glycemic control,
weight changeweight change•• Safety Endpoints: Hypoglycemic episodes, Safety Endpoints: Hypoglycemic episodes,
insulin antibodiesinsulin antibodies

Oral Insulin Phase 2 StudyOral Insulin Phase 2 Study
•• Dose and ScheduleDose and ScheduleFirst Treatment Arm:First Treatment Arm: Two Insulin/4Two Insulin/4--CNAB CNAB tablets 4 times a day tablets 4 times a day Second Treatment Arm:Second Treatment Arm: Two Insulin/4Two Insulin/4--CNAB CNAB tablets 2 times a day and two placebo tablets 2 tablets 2 times a day and two placebo tablets 2 times a daytimes a dayThird Treatment Arm:Third Treatment Arm: One Insulin/4One Insulin/4--CNAB CNAB tablet and one placebo tablet 4 times a daytablet and one placebo tablet 4 times a dayFourth Treatment Arm:Fourth Treatment Arm: Two placebo tablets 4 Two placebo tablets 4 times a daytimes a day

EMISPHERE TECHNOLOGIES, INC.EMISPHERE TECHNOLOGIES, INC.







