
Avoiding and Managing Avoiding and Managing Complications for Lap Complications for Lap Inguinal Hernia RepairInguinal Hernia Repair
Bruce Ramshaw MD FACSBruce Ramshaw MD FACS
Consultant, Halifax HealthConsultant, Halifax Health
Daytona Beach, FLDaytona Beach, FL

TEP (Total Extraperitoneal)TEP (Total Extraperitoneal)

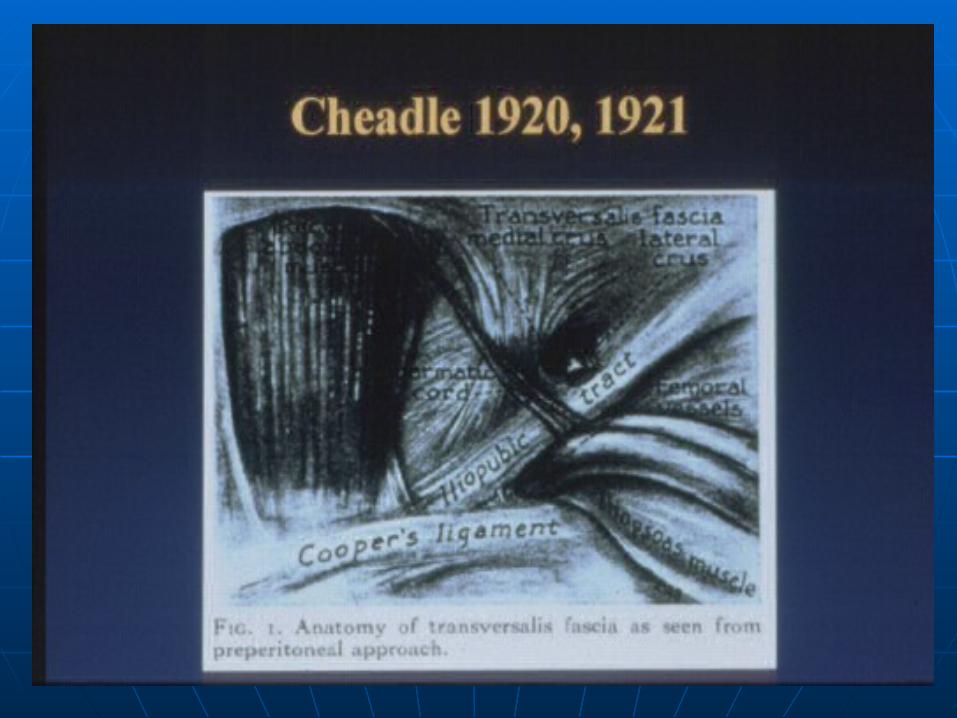
ANATOMYANATOMY
Very complexVery complex
Unfamiliar to most open surgeonsUnfamiliar to most open surgeons
ConsistentConsistent
Need to see over and overNeed to see over and over



Access to Extraperitoneal SpaceAccess to Extraperitoneal Space
Unfamiliar AnatomyUnfamiliar Anatomy
Consistent AnatomyConsistent Anatomy
ObesityObesity
Previous SurgeryPrevious Surgery
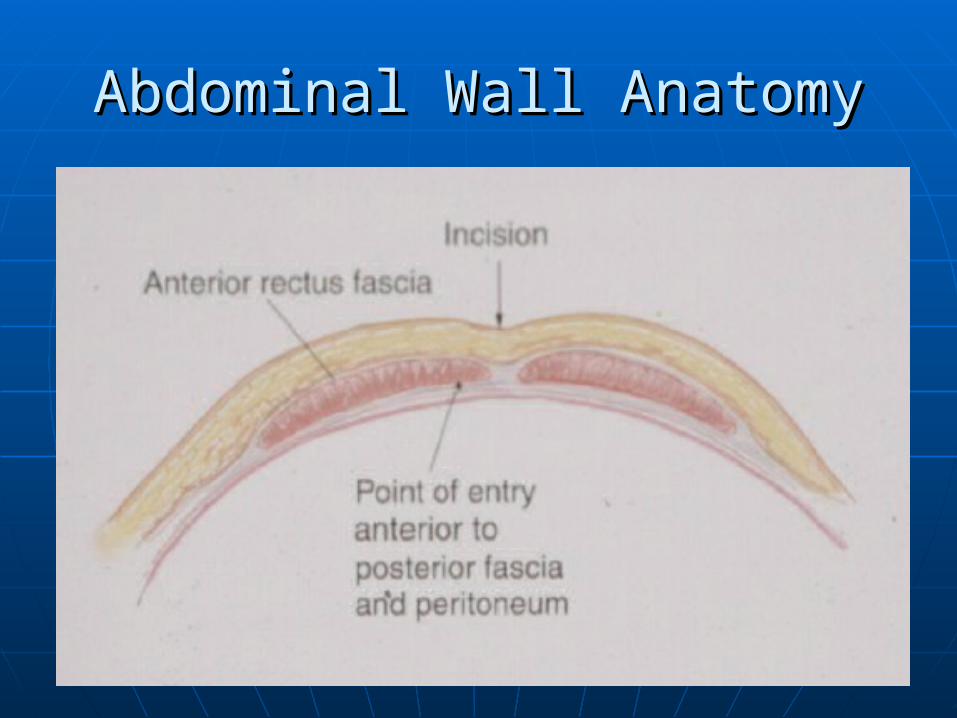
Abdominal Wall AnatomyAbdominal Wall Anatomy
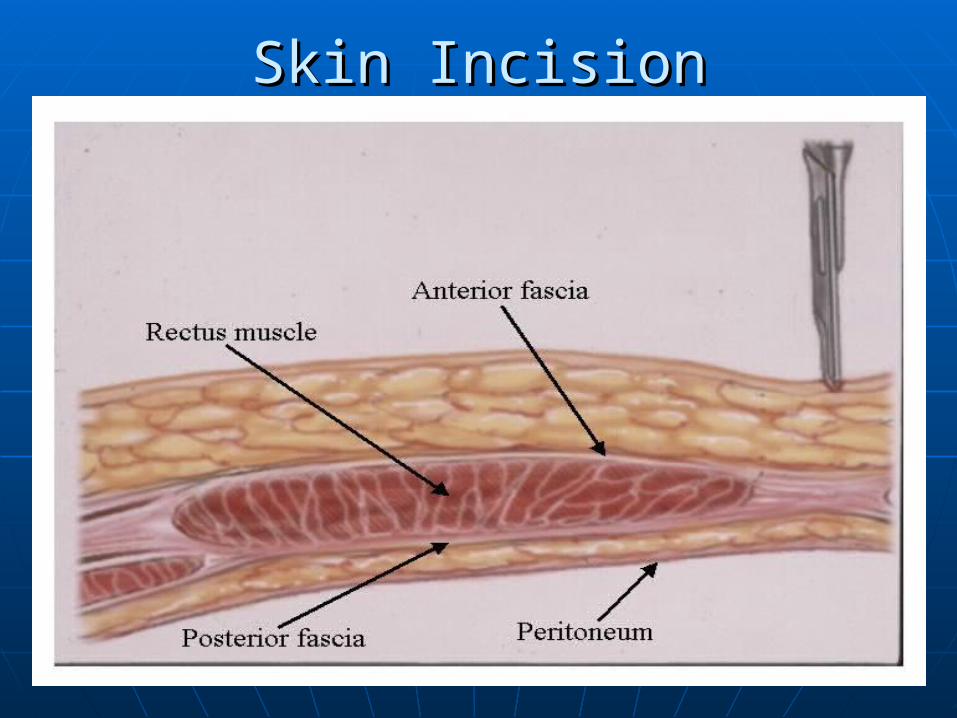
Skin IncisionSkin Incision

Balloon DissectionBalloon Dissection
Different Types of Balloon DissectorsDifferent Types of Balloon Dissectors
Degree of Balloon DistentionDegree of Balloon Distention
Previous SurgeryPrevious Surgery
BleedingBleeding

Balloon ShapesBalloon Shapes

Lateral ViewLateral View


View Through the BalloonView Through the Balloon

Trocar PlacementTrocar Placement

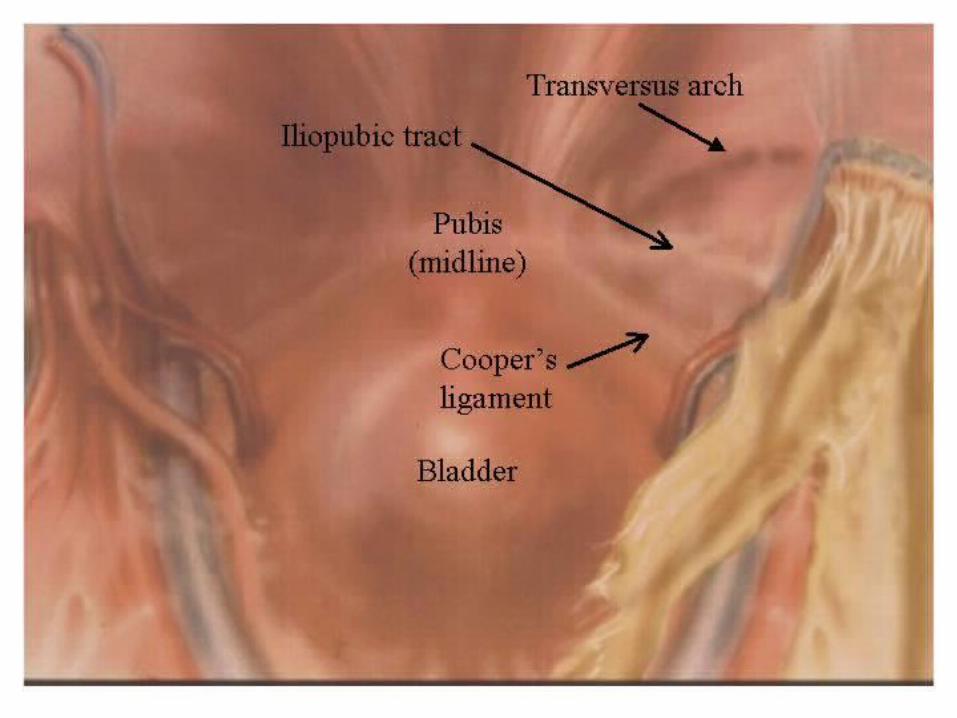
Medial DissectionMedial Dissection
Usually accomplished by the balloonUsually accomplished by the balloon
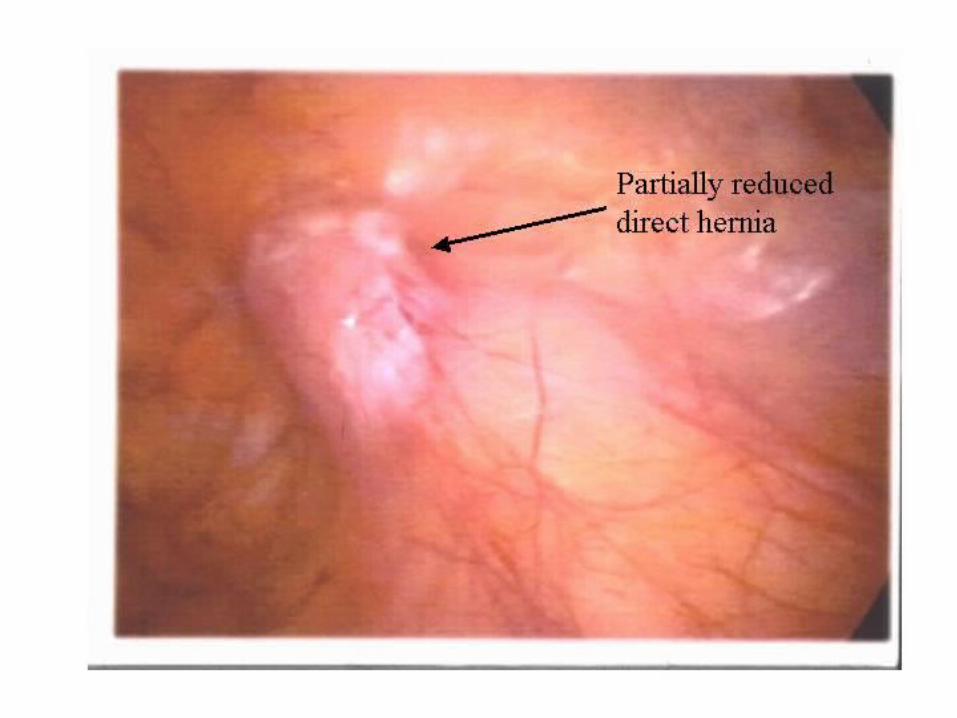
Direct hernia may obscure viewDirect hernia may obscure view
Previous surgeryPrevious surgery
ObesityObesity
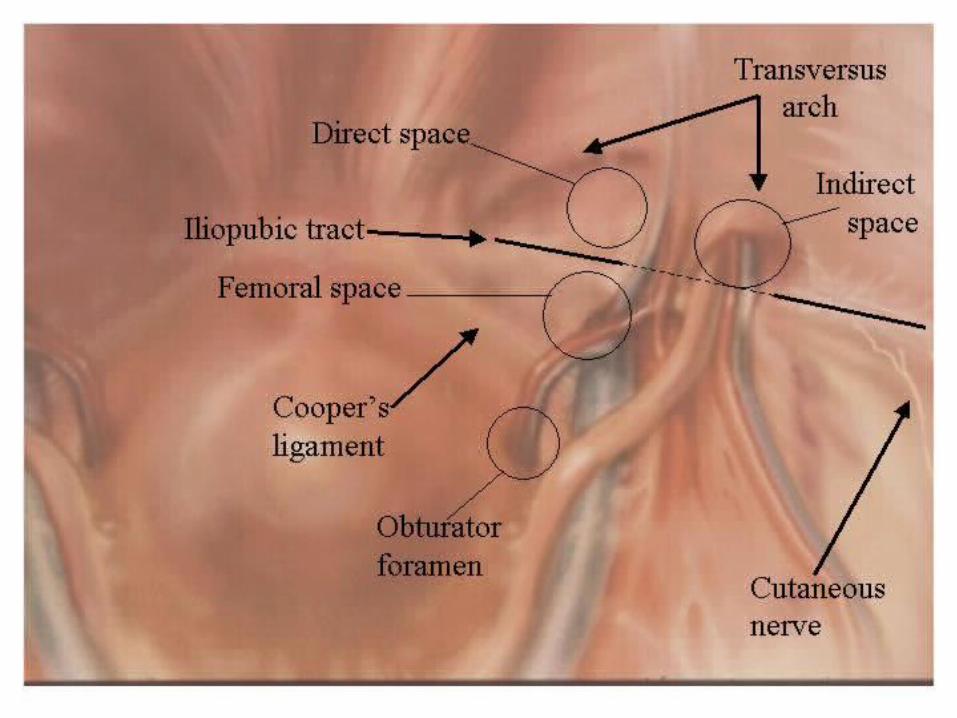
Look for direct, femoral, and obturator Look for direct, femoral, and obturator herniashernias

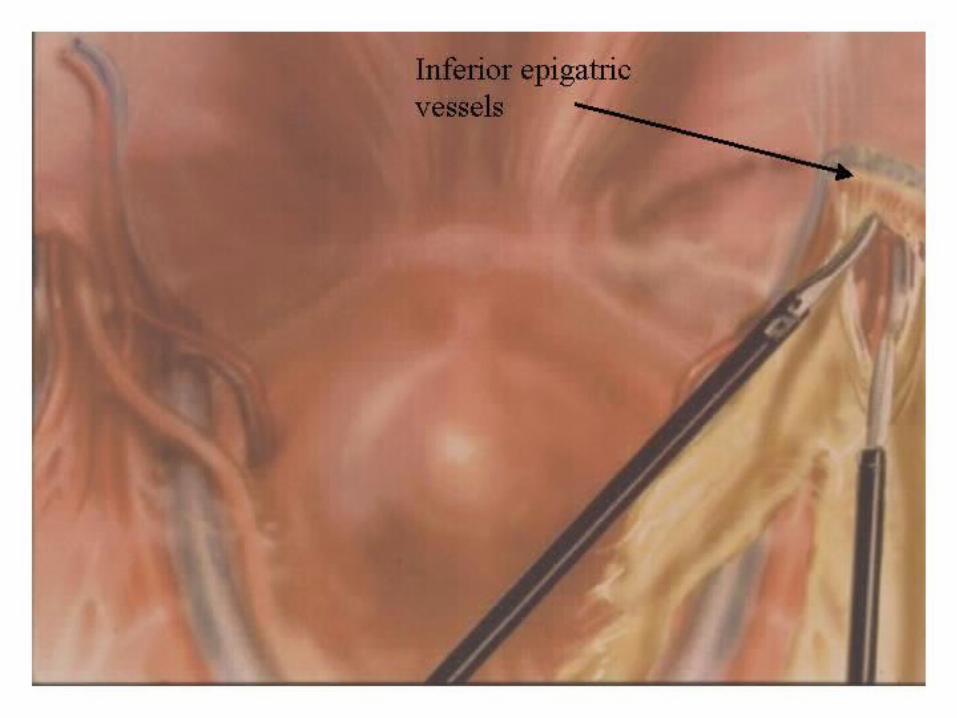
Inferior Epigastric Vessels

Direct HerniaDirect Hernia

Lateral DissectionLateral Dissection
The most difficult part of the dissectionThe most difficult part of the dissection
Stay just posterior to inferior epigastricsStay just posterior to inferior epigastrics
Look for lateral abdominal wallLook for lateral abdominal wall
Avoid posterior structuresAvoid posterior structures
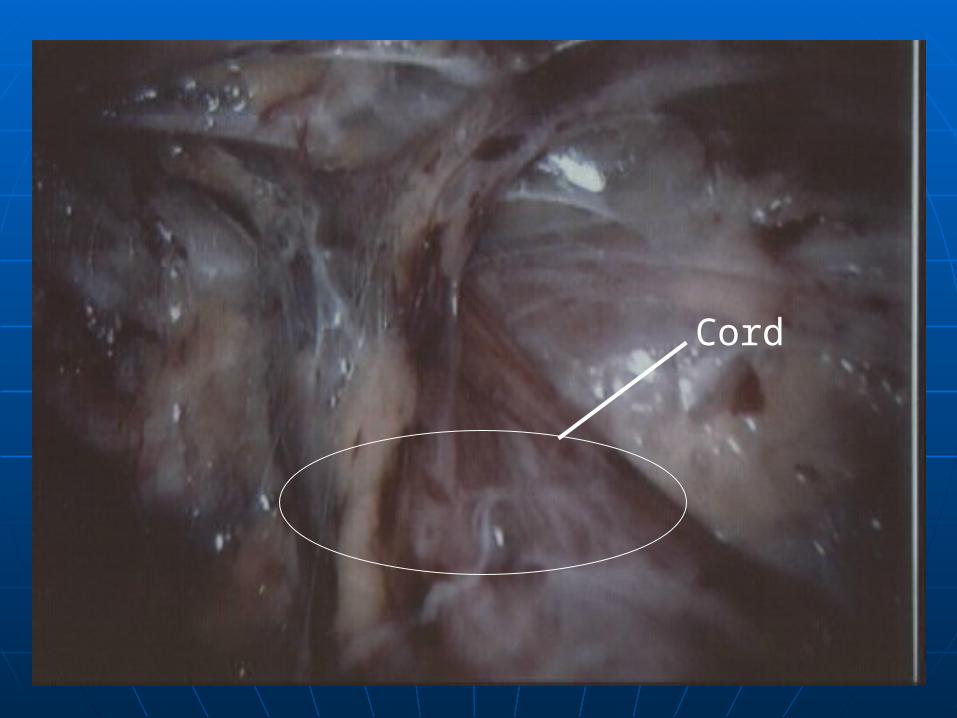
Cord
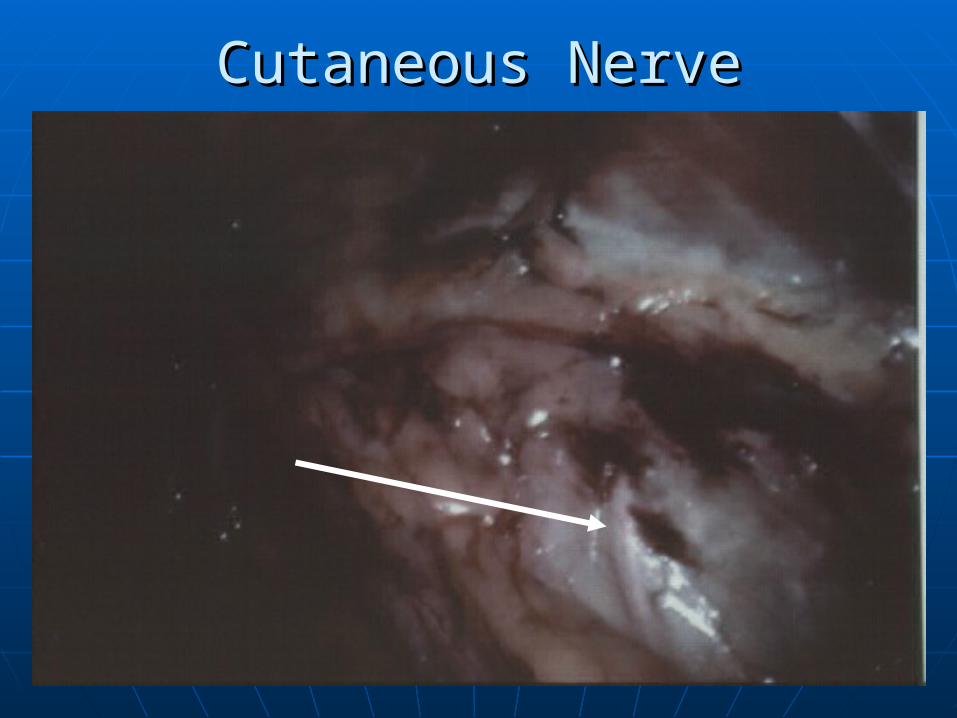
Cutaneous NerveCutaneous Nerve


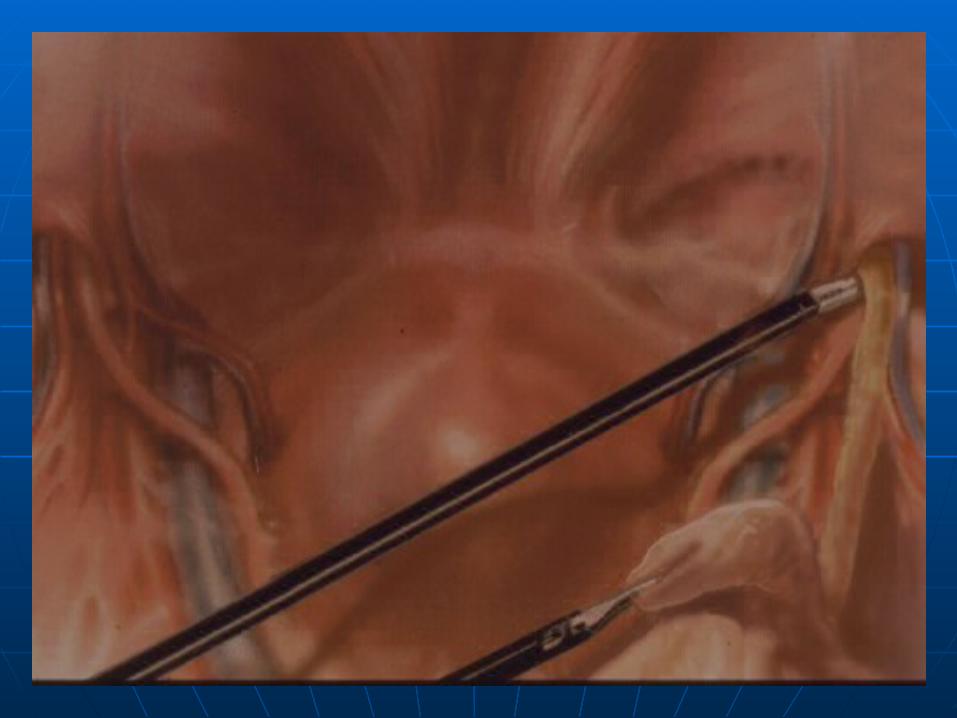
Exploration of the CordExploration of the Cord
Indirect sac located anteriomedialIndirect sac located anteriomedial
Lipoma located anteriolateralLipoma located anteriolateral
Vas located posteriomedialVas located posteriomedial
Cord vessels located posteriolateralCord vessels located posteriolateral


Lipoma of the CordLipoma of the Cord



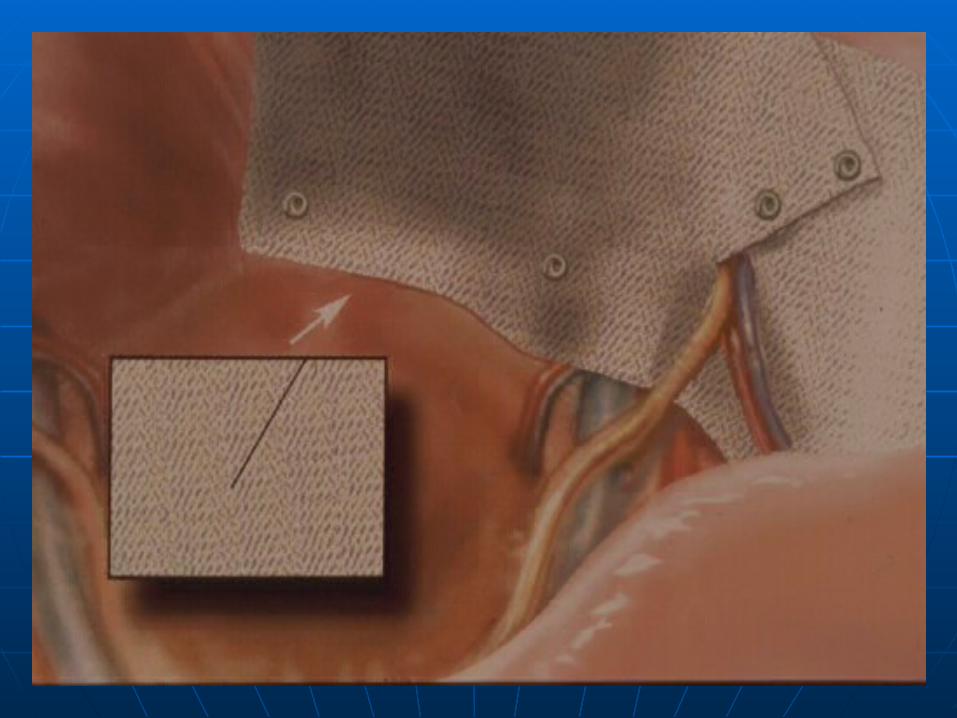
Mesh PlacementMesh Placement
Large mesh- at least 4 x 6 inchesLarge mesh- at least 4 x 6 inches
Slit or no slitSlit or no slit
Anatomic or FlatAnatomic or Flat
MemoryMemory



Inguinodynia – The ProblemInguinodynia – The Problem
Chronic groin pain after any type of Chronic groin pain after any type of inguinal hernia repair is potentially inguinal hernia repair is potentially disablingdisabling• Neuralgia, parasthesia, hypoesthesia, Neuralgia, parasthesia, hypoesthesia,
hyperesthesiahyperesthesia• Unable to work, limited physical & social Unable to work, limited physical & social
activities, sleep disturbances, psychic activities, sleep disturbances, psychic distressdistress
5-7% of patients experiencing post-5-7% of patients experiencing post-hernia repair groin pain begin hernia repair groin pain begin litigation. Most cases are settled.litigation. Most cases are settled. (General Surgery News, Feb 2004)(General Surgery News, Feb 2004)
InguinodyniaInguinodynia
• Prospective series of open Prospective series of open Lichtenstein hernia repairs:Lichtenstein hernia repairs:
At 1 yr f/u 19% of patients had pain, 6% At 1 yr f/u 19% of patients had pain, 6% moderate or severemoderate or severe
• Callesen, Bech & Kehlet Callesen, Bech & Kehlet Br J SurgBr J Surg 1999 1999
• Scottish population based studyScottish population based study 43% respondents with mild pain43% respondents with mild pain 3% severe, very severe pain3% severe, very severe pain
• Courtney, Duffy, Serpell & O’Dwyer. Courtney, Duffy, Serpell & O’Dwyer. Br J Br J SurgSurg 2002 2002

InguinodyniaInguinodynia• Pain 1 year s/p hernia repair – over 800 Pain 1 year s/p hernia repair – over 800
patients:patients: Pain present in 28.7% lap and Pain present in 28.7% lap and 36.7%36.7% open open 3 patients reported severe pain in open group3 patients reported severe pain in open group
• MRC Laparoscopic Groin Hernia Trial Group,MRC Laparoscopic Groin Hernia Trial Group, Lancet Lancet 1999 1999
• Pain present at one year in 28.7% of patients Pain present at one year in 28.7% of patients in Danish National Hernia Database studyin Danish National Hernia Database study
11% pain impaired work or leisure activity11% pain impaired work or leisure activity 4.5% sought treatment4.5% sought treatment
• Bay-Neilsen, Perkins & Kehlet, Bay-Neilsen, Perkins & Kehlet, Ann SurgAnn Surg 2001 2001

The cutaneous nervesThe cutaneous nerves
Anterior view Posterior viewAnterior view Posterior view

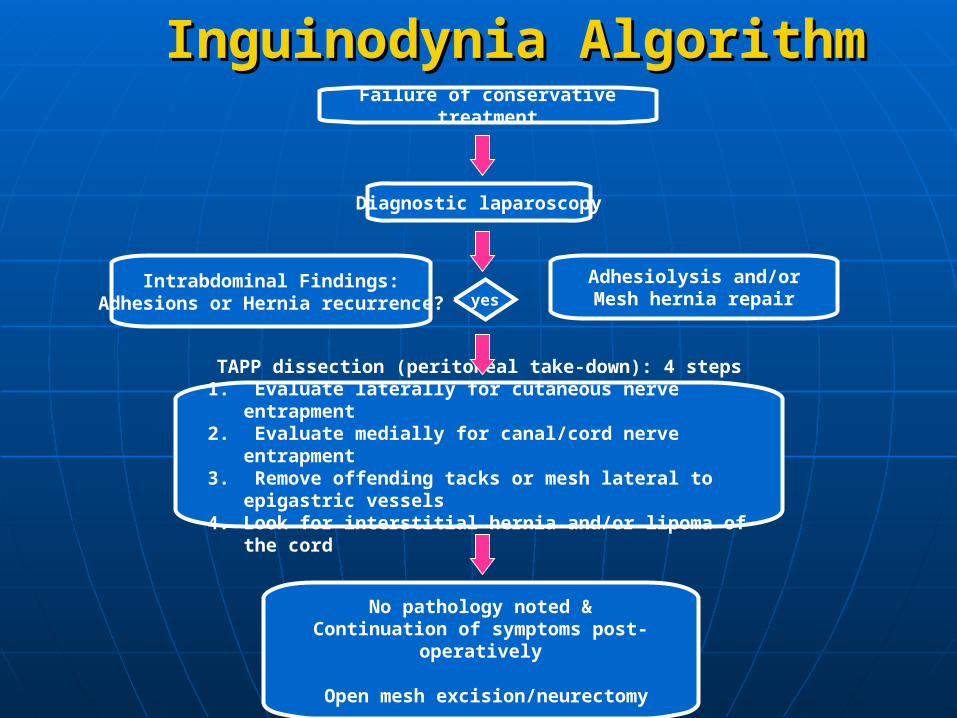
Failure of conservative treatment
Diagnostic laparoscopy
Intrabdominal Findings:Adhesions or Hernia recurrence? yes
Adhesiolysis and/orMesh hernia repair
TAPP dissection (peritoneal take-down): 4 steps1. Evaluate laterally for cutaneous nerve entrapment2. Evaluate medially for canal/cord nerve entrapment3. Remove offending tacks or mesh lateral to epigastric
vessels4. Look for interstitial hernia and/or lipoma of the cord
No pathology noted &Continuation of symptoms post-
operatively
Open mesh excision/neurectomy
Inguinodynia AlgorithmInguinodynia Algorithm

AdhesionsAdhesions

Recurrent HerniaRecurrent Hernia

TacksTacks

PlugsPlugs
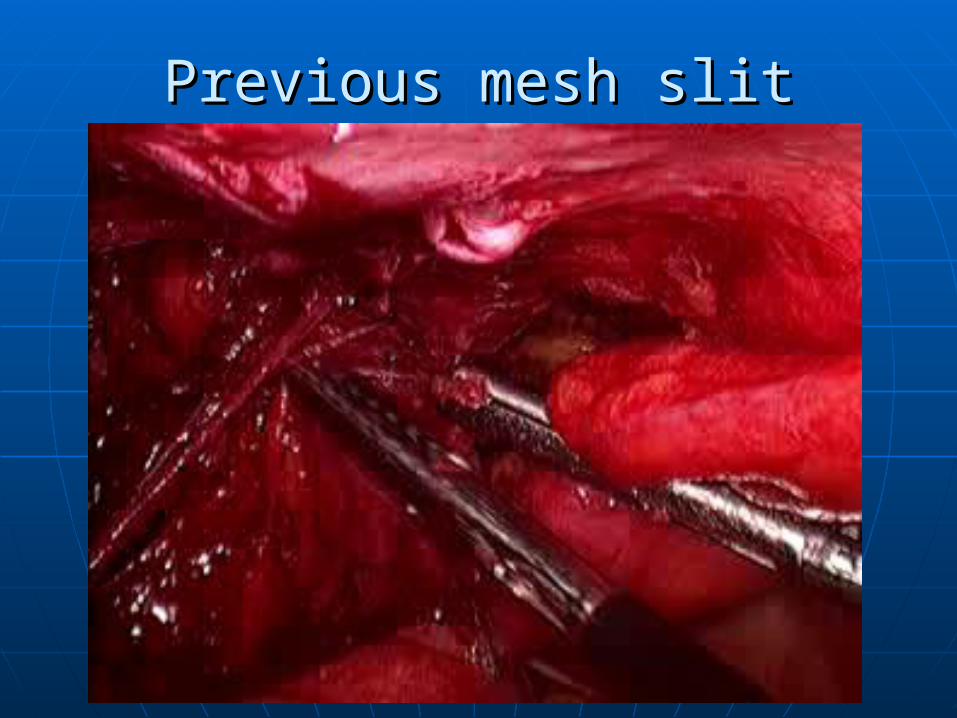
Previous mesh slitPrevious mesh slit
Inguinodynia- Case studyInguinodynia- Case study
280 lb ex-NFL football player (40 y.o)280 lb ex-NFL football player (40 y.o) Lap LIH (3-D max, minimal fixation)Lap LIH (3-D max, minimal fixation) Severe pain almost immediatelySevere pain almost immediately Three operations over three yearsThree operations over three years
- two by primary surgeon - two by primary surgeon
- one for open neurectomy by expert - one for open neurectomy by expert 100 lb wt. loss, loss of all employment, 100 lb wt. loss, loss of all employment,
severe depression, NFL permanent severe depression, NFL permanent disabilitydisability

Previous mesh- no slitPrevious mesh- no slit

Open mesh excisionOpen mesh excision
THANK YOUTHANK YOU
Questions?Questions?







