
1
Appropriate Customization of Radiation Therapy for Stage II and III Rectal Cancer: An ASTRO
Clinical Practice Statement Using the RAND/UCLA Appropriateness Method
Karyn A. Goodman, M.D., M.S.1*, Caroline E. Patton, M.A.2, George A. Fisher, M.D., Ph.D.3, Sarah E.
Hoffe, M.D.4, Michael G. Haddock, M.D.5, Parag J. Parikh, M.D.,6 John Kim, M.D.7, Nancy Baxter,
M.D., Ph.D.8, Brian G. Czito, M.D.9, Theodore S. Hong, M.D.10, Joseph M. Herman, M.D., M.S.11,
Christopher H. Crane, M.D.12, Karen E. Hoffman, M.D.12
1. Department of Radiation Oncology, University of Colorado, Aurora, CO
2. American Society of Radiation Oncology, Fairfax, VA
3. Department of Medical Oncology, Stanford University, Stanford, CA
4. Department of Radiation Oncology, Moffitt Cancer Center, Tampa, FL
5. Department of Radiation Oncology, Mayo Clinic, Rochester, MN
6. Department of Radiation Oncology, Washington University, St. Louis, MO
7. Department of Radiation Oncology, Princess Margaret Cancer Centre, University of Toronto,
Toronto, ON, Canada
8. Division of General Surgery, St. Michael’s Hospital, University of Toronto, Toronto, ON,
Canada
9. Department of Radiation Oncology, Duke University, Durham, NC
10. Department of Radiation Oncology, Massachusetts General Hospital, Boston, MA
11. Department of Radiation Oncology, Johns Hopkins University, Baltimore, MD
12. Department of Radiation Oncology, M.D. Anderson Cancer Center, Houston, TX
* Corresponding author: Caroline Patton, MA, American Society of Radiation Oncology, 8280 Willow
Oaks Corporate Drive, Suite 500, Fairfax, VA 22031, 703-286-1560 (phone), 703-286-1561 (fax),
Conflict of Interest Disclosure Statement:
Working Group
Before initiation of this Clinical Practice Statement, all members of the working group were required to
complete disclosure statements. These statements are maintained at the ASTRO headquarters in Fairfax,
VA and pertinent disclosures are published with the report. The ASTRO Conflict of Interest Disclosure
Statement seeks to provide a broad disclosure of outside interests. Where a potential conflict is detected,
remedial measures to address any potential conflict are taken and will be noted in the disclosure
statement. Nancy Baxter, MD, PhD receives research funding from Pfizer. Brian Czito, MD receives

2
research funding from Abbvie and serves on an advisory board for Pfizer. George Fisher, MD, PhD
receives research funding from Bristol Myers Squibb, Genentech, Tercica, New Link Genetics, Polaris
Group, and Advanced Accelerator Applications. He serves on an advisory board for Genentech.
Theodore Hong, MD, serves on advisory boards for Novartis and Eisai. John Kim, MD receives research
funding from Philips. Parag Parikh, MD receives research funding, honoraria, and travel expenses from
Varian and research funding from Philips. He owns stock in Innovative Pulmonary Solutions and
consults for Ethicon. The Best Practices Subcommittee chairs reviewed these disclosures and
determined they do not present a conflict with respect to these members’ work on this Clinical Practice
Statement.
Expert Panel
Harvey Mamon, MD, PhD received honoraria from UptoDate. Jeffrey Tokar, MD consulted for Boston
Scientific. He served on an advisory board for and received honoraria and travel expenses from
Augmenix. Dr. Tokar was also a board member for the Center for GI Innovation and Technology
(CGIT) and received patent fees. Richard Goldberg, MD received research funding and honoraria from
Sanofi and served on a data and safety monitoring board for Lilly. Salma Jabbour, MD provided a talk
for Abbott Laboratories.
Acknowledgements:
The authors thank the expert panel: George J. Chang, MD, MS, David Dietz, MD, Patrick Francke, MD,
Julio Garcia-Aguilar, MD, PhD, Richard Goldberg, MD, Salma Jabbour, MD, Bruce Lin, MD, Harvey
Mamon, MD, PhD, Marilyn M. Schapira, MD, MPH, and Jeffrey Tokar, MD. They also acknowledge

3
Eunice Chang, PhD for conducting the expert panel rating statistics and Margaret Amankwa-Sakyi for
literature review assistance.

4
Introduction
Treatment of rectal cancer has made great strides over the last five decades with improvements
in surgical techniques and the use of combined modality therapy. Prior to the use of the total mesorectal
excision (TME) technique, surgery alone resulted in local recurrence rates of 30-60% for locally
advanced disease.1 The use of adjuvant 5-fluorouracil (5-FU)-based chemoradiation reduced local
failure rates to 10-12% and improved overall survival compared to surgery alone,2-4 leading to the 1990
National Cancer Institute (NCI) consensus statement recommending adjuvant chemotherapy and
radiotherapy for all patients with stage II or III (T3-4 or node positive) rectal cancer.5 The phase III
randomized German Rectal Study subsequently demonstrated an improvement in the 10-year cumulative
incidence of local relapse and reduced acute and overall toxicity rates with the use of pre-operative
versus post-operative chemoradiation.6,7 This study has established the standard of care for stage II or
III rectal cancer as neoadjuvant 5-FU-based chemotherapy with conventionally fractionated radiotherapy
to 50.4 Gy.8-10
However, a number of important questions remain regarding how to define subgroups of stage II
and III and individualize use of multimodality therapy. With 5-year survival rates upwards of 75% for
these patients,6 weighing potential long-term effects of surgery, radiotherapy and chemotherapy must be
considered in determining appropriate management strategies. Given the potential morbidity associated
with a multimodality approach, there are emerging efforts to identify subgroups of patients who can
safely forgo a component of standard management without sacrificing disease control.11
There have been attempts to further stratify Stage II and III rectal cancer patients by risk to
identify subgroups that could potentially be over-treated using tri-modality therapy. In a pooled analysis
of prospective and randomized datasets of patients treated with or without chemotherapy and/or
radiation after radical rectal resection, Gunderson et al. identified three risk groups among Stage II and
5
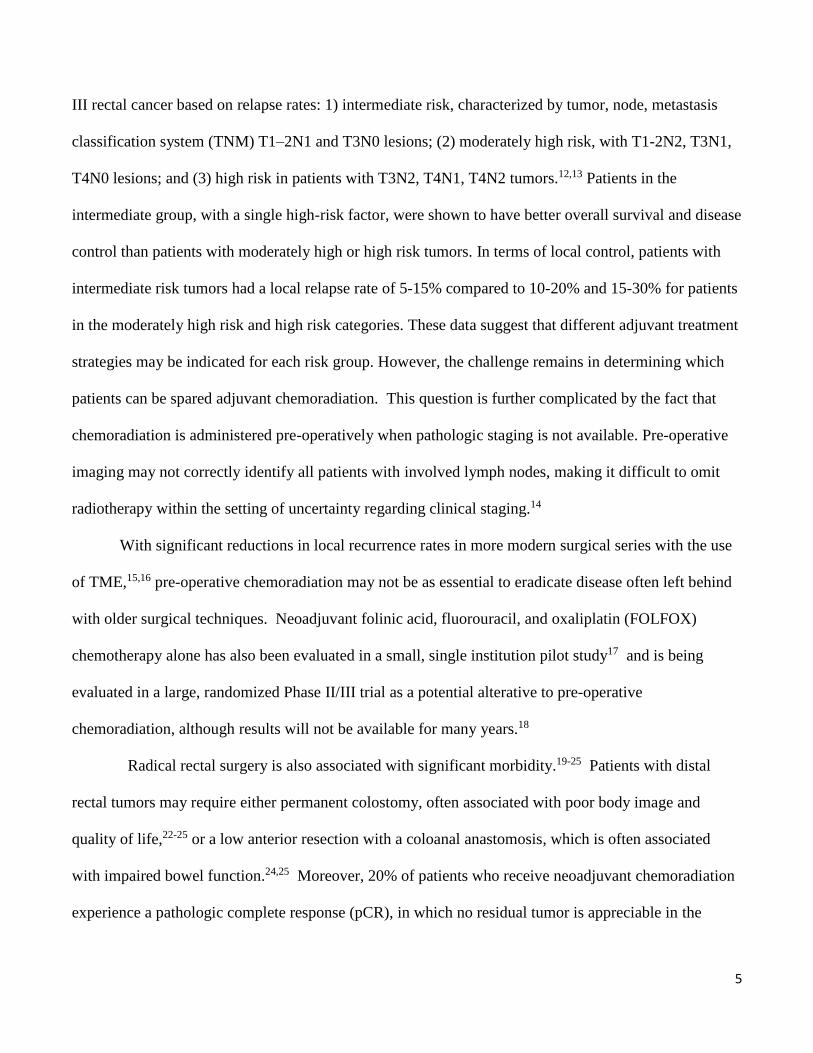
III rectal cancer based on relapse rates: 1) intermediate risk, characterized by tumor, node, metastasis
classification system (TNM) T1–2N1 and T3N0 lesions; (2) moderately high risk, with T1-2N2, T3N1,
T4N0 lesions; and (3) high risk in patients with T3N2, T4N1, T4N2 tumors.12,13 Patients in the
intermediate group, with a single high-risk factor, were shown to have better overall survival and disease
control than patients with moderately high or high risk tumors. In terms of local control, patients with
intermediate risk tumors had a local relapse rate of 5-15% compared to 10-20% and 15-30% for patients
in the moderately high risk and high risk categories. These data suggest that different adjuvant treatment
strategies may be indicated for each risk group. However, the challenge remains in determining which
patients can be spared adjuvant chemoradiation. This question is further complicated by the fact that
chemoradiation is administered pre-operatively when pathologic staging is not available. Pre-operative
imaging may not correctly identify all patients with involved lymph nodes, making it difficult to omit
radiotherapy within the setting of uncertainty regarding clinical staging.14
With significant reductions in local recurrence rates in more modern surgical series with the use
of TME,15,16 pre-operative chemoradiation may not be as essential to eradicate disease often left behind
with older surgical techniques. Neoadjuvant folinic acid, fluorouracil, and oxaliplatin (FOLFOX)
chemotherapy alone has also been evaluated in a small, single institution pilot study17 and is being
evaluated in a large, randomized Phase II/III trial as a potential alterative to pre-operative
chemoradiation, although results will not be available for many years.18
Radical rectal surgery is also associated with significant morbidity.19-25 Patients with distal
rectal tumors may require either permanent colostomy, often associated with poor body image and
quality of life,22-25 or a low anterior resection with a coloanal anastomosis, which is often associated
with impaired bowel function.24,25 Moreover, 20% of patients who receive neoadjuvant chemoradiation
experience a pathologic complete response (pCR), in which no residual tumor is appreciable in the

6
surgical specimen.26,27 These patients have particularly favorable outcomes, compared to those with
residual cancer at the time of TME,27,28 and may not derive additional benefit from radical surgery.
Recent studies have demonstrated the feasibility of non-operative management for highly selected
patients achieving clinical complete response (cCR) to chemoradiotherapy, suggesting that surgery can
potentially be omitted, which could significantly improve long-term quality of life, particularly in the
group of patients for whom an operation would result in a permanent colostomy.29-32
Scope and purpose
While the establishment of tri-modality therapy for rectal cancer, including surgery,
radiotherapy, and chemotherapy, is the result of decades of randomized trials designed to address key
questions, ambiguity remains due to patient and disease heterogeneity and the emerging attempt to better
customize treatment strategies. Moreover, a growing body of evidence indicates that subgroups of stage
II and III patients have differing risk profiles and warrant a more tailored therapeutic approach that
spares unnecessary morbidity while achieving good outcomes. The current standard approach using the
same therapeutic regimen for all Stage II or II rectal cancer patients suggests additional study is required
to further refine specific approaches. Ultimately, the goal will be to intensify treatment for tumors
demonstrating aggressive biologic behavior and limit treatment for more indolent tumors. Without better
validated biomarkers, clinicians are faced with making decisions about therapy based on stage, tumor
location, and other clinical factors. Currently, there are limited data and clinical guidance available to
help clinicians navigate the emerging options and, therefore, the American Society for Radiation
Oncology (ASTRO) proposed the development of a Clinical Practice Statement to address two clinical
situations that provide opportunities for a more individualized approach. Specific questions addressed
included:

7
How to appropriately individualize the use of (neo)adjuvant radiation therapy for patients with
T3-4 or node positive rectal cancer.
How to appropriately customize non-surgical therapy for rectal cancer patients who are
medically inoperable or who have low-lying tumors and are attempting to avoid an
abdominoperineal resection.
We thus sought to employ the RAND/ University of California-Los Angeles (UCLA)
Appropriateness Method to define best practice with respect to neoadjuvant or adjuvant radiation
therapy and non-operative management among stage II or III rectal cancer patients. Specific clinical
scenarios incorporating known risk factors for recurrence were developed to help stratify these patients
into more discrete subgroups and were presented to a multi-specialty expert panel to determine
appropriate management for these cases. The Clinical Practice Statement also addresses radiation
techniques, such as intensity modulated radiotherapy (IMRT), and other clinical considerations. We
believe that a Clinical Practice Statement on this subject will be useful for oncology and for day to day
management of rectal cancer patients.
Methods and Materials
Process
The ASTRO Board of Directors approved the creation of a Clinical Practice Statement on how to
appropriately customize radiation therapy for stage II and III rectal cancer in May 2013. A working
group of physicians from radiation oncology, medical oncology, and surgery who specialize in
gastrointestinal cancers oversaw a comprehensive literature review conducted by ASTRO staff and
developed the scenarios and definitions during a series of discussions by conference call and electronic
mail. A multidisciplinary expert panel was selected to review the literature and rate the scenarios. The

8
working group reconvened to interpret the ratings from the expert panel and draft the Clinical Practice
Statement. The document was reviewed by the expert panel, the Best Practices Subcommittee, and the
Clinical Affairs and Quality Committee. It also underwent four weeks of public comment during March
and April 2015. The final draft was approved by the Board of Directors in June 2015.
This Clinical Practice Statement uses the RAND/UCLA Appropriateness Method, which was
created during the 1980s with the goal of offering a rigorous way to “combine the best available
scientific evidence with the collective judgment of experts to yield a statement regarding the
appropriateness of performing a procedure at the level of patient-specific symptoms, medical history and
test results.”33 This method has been applied to a wide range of medical disciplines, including a number
of other oncology topics,34-38 and incorporates a multidisciplinary expert panel to rate the scenarios in
order to mitigate the fact that physicians often rate treatments they deliver as more appropriate than
those they do not.39,40
For this Clinical Practice Statement, each scenario was rated Appropriate, May Be Appropriate,
or Rarely Appropriate. An Appropriate rating indicates that the expected benefit for the patient is
sufficiently greater than the risks under most circumstances to make it worthwhile and reasonable to use
the treatment. However, because a therapy is Appropriate does not mean it is required in all patients like
those described in the scenario. Similarly, a Rarely Appropriate rating shows that the anticipated risks
are considered higher than the benefits in most patients with the characteristics in that scenario, but
should not be taken to mean that it is never reasonable to apply the intervention under those
circumstances. Treatments rated May Be Appropriate have evidence that is limited, mixed, or subject to
disagreement or the balance of the risks and benefits is currently unclear. However, the therapy may be
appropriate and reasonable for some patients similar to those in the scenario.

9
Literature review
A systematic literature review was carried out using MEDLINE PubMed, Embase, and the
Cochrane Library to identify studies published between January 1990 and July 2013 that evaluated
patients 18 years or older with stage II or III rectal cancer receiving radiotherapy and/or chemotherapy.
Both resectable and medically inoperable patients were included. The electronic searches were
supplemented by hand searches and a total of 1571 articles were initially retrieved. These were screened
based on the exclusion criteria to remove articles that were: case reports, stage I or IV only, non-English
language, recurrent disease, abstract only, phase I studies, focused on tolerability or dosage without
survival or relapse outcomes, or otherwise not relevant. For trials of neoadjuvant or adjuvant radiation
therapy, studies that were retrospective or had ten patients or fewer were also excluded. Where the same
study was reported at multiple time points, only the latest one was retained. Ultimately, 228 full-text
articles were selected for inclusion and the data were abstracted to create detailed literature tables.
Literature summaries were also developed.
Clinical scenarios and definitions of terms
The scenarios were split into four sections: neoadjuvant therapy, adjuvant therapy, medically
inoperable patients, and patients seeking to avoid abdominoperineal resection (APR). First, the working
group compiled a list of factors that might influence physicians’ choice of therapy. Second, factors
relevant to each section were combined to create a set of scenarios representing patients a radiation
oncologist might see in practice, along with potentially appropriate therapies. Both the factors included
and the treatments assessed varied by section and are described in the Results. The Clinical Practice
Statement also included two questions addressing the relative appropriateness of delivering neoadjuvant
and adjuvant radiation with three-dimensional conformal radiation therapy (3D-CRT) versus IMRT.

10
There were 237 total initial scenarios. A definition list was also created to give a common understanding
of the terms across all participants in the project.
Expert Panel
The expert panel was charged with rating the scenarios based on the literature review and
definitions developed by the working group. The panel was composed of physicians in radiation
oncology (including both specialists and a non-specialist in gastrointestinal tumors), medical oncology,
colorectal surgery, gastroenterology, and general internal medicine. Prospective participants were
identified through nominations from ASTRO committees and external outreach to other medical
specialty societies. Invited panelists were selected by the Best Practices Subcommittee based on
specialty, geographic region, practice setting, and availability for the in-person meeting and
subsequently screened for potential conflicts and bias. The final ten-member panel (Table 1) was made
up of eight physicians who worked in academic settings and two who were in private or community-
based practice.
Table 1. Expert Panel Members
Specialty Name Institution
Radiation Oncology Patrick Francke, MD 21st Century Oncology, Myrtle Beach, SC
Salma Jabbour, MD Rutgers University, New Brunswick, NJ
Harvey Mamon, MD, PhD Brigham and Women’s Hospital and Dana Farber
Cancer Institute, Boston, MA
Medical Oncology Richard Goldberg, MD Ohio State University, Columbus, OH
Bruce Lin, MD Virginia Mason Medical Center, Seattle, WA
Colorectal Surgery George Chang, MD M.D. Anderson Cancer Center, Houston, TX
Julio Garcia-Aguilar, MD, PhD Memorial Sloan-Kettering Cancer Center, New York,
NY
David Dietz, MD Cleveland Clinic, Cleveland, OH
Gastroenterology Jeffrey Tokar, MD Fox Chase Cancer Center, Philadelphia, PA
General Internal
Medicine
Marilyn Schapira, MD, PhD University of Pennsylvania, Philadelphia, PA
Moderator Michael Broder, MD Partnership for Health Analytic Research, LLC,
Beverly Hills, CA

11
Rating process and panel meeting
For each scenario, the panel rated the appropriateness of the treatment from 1 to 9. A “1”
indicated much greater anticipated harm than benefit and a “9” much higher expected benefit than harm.
A “5” signified balanced harm and benefit or that the rater felt unable to reach a conclusion.
Additionally, panelists were instructed to envision an “average patient” treated by an “average
physician” in an “average facility” and not to consider cost or cost-effectiveness. Prior to rating, an
orientation to the rating procedure and materials was held. The expert panel rated the scenarios in two
rounds. The initial rating was performed independently via an online survey during February and March,
2014.
A face-to-face meeting of the expert panel was held on April 5th, 2014 in Alexandria, Virginia
and was overseen and moderated by a moderator experienced in the RAND process. Each panelist
received an individualized form showing their own rating per indication and the median and mean
distance from the median for the entire panel. During the meeting, the panelists discussed the scenarios
and then re-rated them using the same survey and process. Panelists were not forced to reach agreement.
The expert panel was asked in July 2014 to rate three scenarios a third time due to inconsistencies in the
second round results and the resulting ratings replaced those from the second round.
Statistical analyses
Ratings for the first and second rounds were analyzed by a statistician using SAS statistical
software. For the third round, due to the small number of ratings, Excel was used. For all rounds, the
median and the mean distance from the median were calculated for each scenario. The median was used
to measure central tendency because the responses were ordinal and the distance between points on the

12
scale was not fixed. Average distance from the median was used to measure dispersion. Treatments were
rated Rarely Appropriate when the median was 1 to 3 without disagreement, May Be Appropriate when
it was 4 to 6 or there was disagreement, and Appropriate when it was 7 to 9 without disagreement.
Disagreement was defined as ≥3 ratings from 1 to 3 and ≥3 from 7 to 9 on the same item.
Results
The expert panel evaluated 237 scenarios during the initial round of rating and 209 during the
second. The scenarios were organized in four sections and an additional question on IMRT. Throughout
the scenarios, only patients with stage II or III rectal cancer were included. In the first round, 28.3% (67
scenarios) were rated Appropriate, 38.4% (91 scenarios) were rated May Be Appropriate, and 33.3% (79
scenarios) were rated Rarely Appropriate. There was disagreement on 7.2% (17 scenarios). After face-
to-face discussion, 27.3% (57 scenarios) were rated Appropriate, 44.0% (92 scenarios) were rated May
Be Appropriate, and 28.7% (60 scenarios) were rated Rarely Appropriate. There was only one second
round scenario with disagreement. Three scenarios were rated a third time due to an inconsistency in the
ratings during the second round. As a result, one scenario moved from a rating of May Be Appropriate
to Rarely Appropriate and one scenario changed from a rating of Rarely Appropriate to May Be
Appropriate. The third scenario remained the same.
Neoadjuvant therapy
The first section included 105 scenarios. It considered the role of the distance of the distal edge
of the tumor from the anal verge, distance from the radial tumor edge to edge of mesorectal fascia
(based on magnetic resonance imaging [MRI]), and risk classification on the appropriateness of
radiation and/or chemotherapy. Intermediate risk was defined as T1-2N1 or T3N0. Moderately high risk

13
included T1-2N2, T3N1, or T4N0 tumors. High risk encompassed T3N2 or T4N1-2. These
classifications were adapted from Gunderson et al.13 The use of distance to the edge of the mesorectal
fascia on MRI (see Figure 1 for example) reflects the trend in the United States for MRI to replace
endoscopic ultrasonography (ERUS) as the standard for staging, although ERUS may still be more
reliable at distinguishing between T2 and T3 disease. It also aligns with the National Comprehensive
Cancer Network (NCCN) guideline on rectal cancer, which likewise considers MRI part of the staging
workup.8 For patients in the high risk category, the distance from the tumor to the mesorectal fascia was
not included in the scenarios.
Figure 1. Rectal MRI axial T2 image
Five treatments were rated: short-course radiation, endorectal brachytherapy, chemoradiation,
chemotherapy alone, and no neoadjuvant therapy. Short-course radiation was assumed to be 25 Gy in 5
fractions based on the Dutch TME study41,42 and endorectal brachytherapy was based on a Canadian
regimen of high-dose rate intraluminal delivery of a dose of 26 Gy in 4 fractions using an endoluminal

14
applicator and Iridium-192 afterloading technique.43 Standard chemoradiation was considered to be 45
Gy to the whole pelvis with a conedown to exclude small bowel to 50.4 Gy with concurrent infusional
5-FU or capecitabine. Neoadjuvant chemotherapy alone was assumed to be FOLFOX.17
For the initial round, 26.7% (28 scenarios) were rated Appropriate, 16.2% (17 scenarios) were
rated May Be Appropriate, and 57.1% (60 scenarios) were rated Rarely Appropriate. Disagreement was
present on 8.6% (9 scenarios). At the meeting, 27.6% (29 scenarios) were rated Appropriate, 24.8% (26
scenarios) were rated May Be Appropriate, and 47.6% (50 scenarios) were rated Rarely Appropriate.
There were no scenarios with disagreement. In the third round, one scenario was changed to Rarely
Appropriate from May Be Appropriate and another became May Be Appropriate from Rarely
Appropriate.
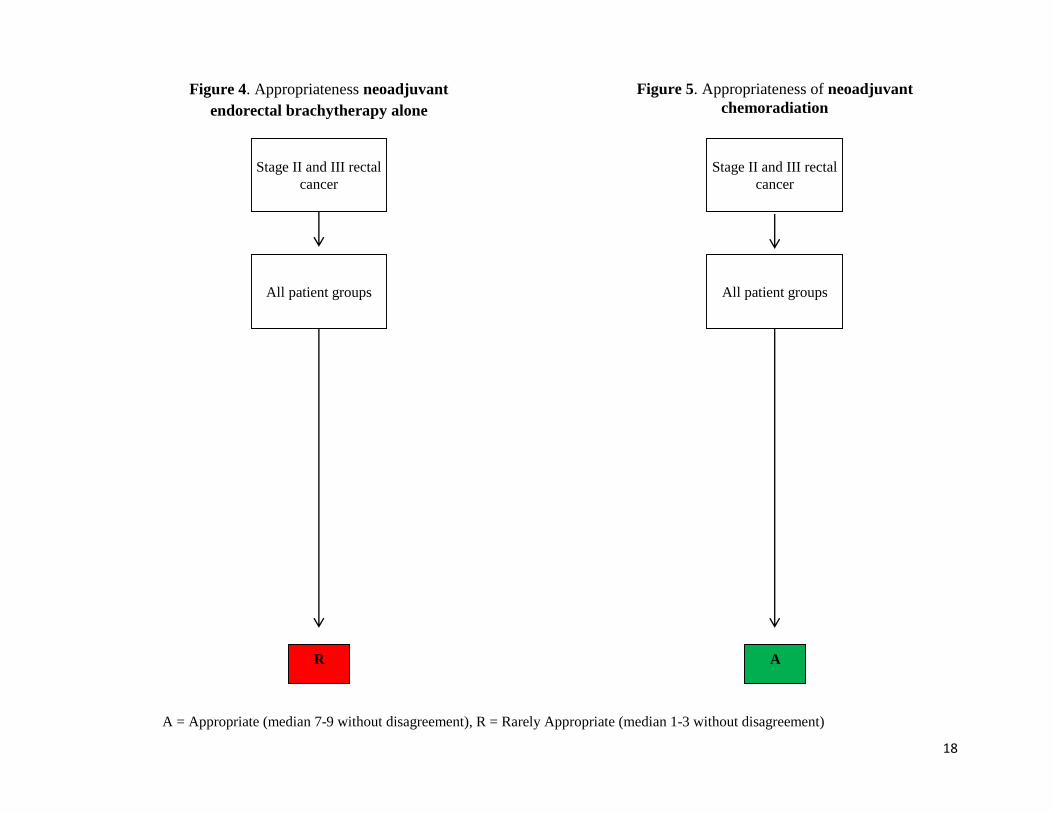
The expert panel always rated conventionally fractionated chemoradiation Appropriate for
patients with stage II and III rectal cancer with a median rating of 9 (Figure 5). While the ratings were
not as high (medians 5 to 7) as for long-course chemoradiation, the panel also rated neoadjuvant short-
course radiation May Be Appropriate to Appropriate depending on risk and tumor location (Figure 2).
There were no situations where short-course radiation was rated Rarely Appropriate. The panel rated
neoadjuvant chemotherapy alone May Be Appropriate for certain patients, particularly those with large
margins from the mesorectal fascia in intermediate and moderately high risk disease. Panelists mostly
rated this approach Rarely Appropriate in patients with closer mesorectal fascia margins as well as high
risk disease (Figure 3). The expert panel rated endorectal brachytherapy alone as Rarely Appropriate for
all patients (Figure 4) although it was noted that this could be considered in the setting of a clinical trial.
Finally, regarding panelists’ views on omitting neoadjuvant therapy in stage II and III rectal cancer, they
rated it May Be Appropriate in patients with intermediate risk disease ≥5 cm from the anal verge with
non-threatened mesorectal fascia, and moderately high risk disease that was >10 cm from the anal verge

15
and had no threatened mesorectal fascia (Figure 6). In other situations, the expert panel rated it Rarely
Appropriate to not offer neoadjuvant therapy.

16
Risk classification*
Distance from anal
verge
Distance from tumor
edge to edge of
mesorectal fascia^
Stage II and III
rectal cancer
Moderately high
risk disease High risk disease
Intermediate risk
disease
>10 cm ≤10 cm
≥2 mm
M A M M
<5 cm ≥5 cm
A
≥2 mm <2 mm
A M
<2 mm
* Intermediate risk = T1-2N1, T3N0, Moderately high risk = T1-2N2, T3N1, High risk = T3N2, T4N1-2
^ Based on MRI
A = Appropriate (median 7-9 without disagreement), M = May Be Appropriate (median 4-6 or disagreement)
Figure 2. Appropriateness of neoadjuvant short-course RT

17
* Intermediate risk = T1-2N1, T3N0, Moderately high risk = T1-2N2, T3N1, High risk = T3N2, T4N1-2
^ Based on MRI
M = May Be Appropriate (median 4-6 or disagreement), R = Rarely Appropriate (median 1-3 without disagreement)
Risk classification*
Distance from anal
verge
Distance from tumor
edge to edge of
mesorectal fascia^
Stage II and III rectal
cancer
High risk
disease
R
Moderately high
risk disease
>10 cm <5 cm 5-10 cm
R
>5
mm
≤5
mm
R M
≥2
mm
<2
mm
R M
Intermediate
risk disease
<5 cm 5-10 cm
>5
mm
≤5
mm
R M
≥2
mm
<2
mm
R M
>10 cm
M
Figure 3. Appropriateness of neoadjuvant chemotherapy alone
18
Stage II and III rectal
cancer
R
All patient groups
Stage II and III rectal
cancer
A
All patient groups
A = Appropriate (median 7-9 without disagreement), R = Rarely Appropriate (median 1-3 without disagreement)
Figure 4. Appropriateness neoadjuvant
endorectal brachytherapy alone
Figure 5. Appropriateness of neoadjuvant
chemoradiation

19
Stage II and III rectal
cancer
High risk
disease
R
Intermediate
risk disease
<5 cm
R
5-10 cm
R M
>5
mm
≤5
mm
>10 cm
≥2
mm
<2
mm
R M
Moderately high
risk disease
≤10 cm
R
>10 cm
>5
mm
≤5
mm
M R
Risk classification*
Distance from anal
verge
Distance from tumor
edge to edge of
mesorectal fascia^
* Intermediate risk = T1-2N1, T3N0, Moderately high risk = T1-2N2, T3N1, High risk = T3N2, T4N1-2
^ Based on MRI
M = May Be Appropriate (median 4-6 or disagreement), R = Rarely Appropriate (median 1-3 without disagreement)
Figure 6. Appropriateness of no neoadjuvant therapy

20
Adjuvant therapy 1
There were 38 scenarios in the second section addressing the options for adjuvant therapy in 2
stage II and III rectal cancer. Only patients with no gross residual disease after curative surgery were 3
included and patients had not received neoadjuvant therapy. The scenarios looked at the impact of 4
circumferential resection margin (CRM), risk classification, distance from the anal verge, and total nodal 5
count. A positive margin was defined as tumor within 1 mm from the inked margin. The first round 6
resulted in 52.6% (20 scenarios) rated May Be Appropriate, and 47.4% (18 scenarios) rated Appropriate. 7
There was disagreement on 5.3% (2 scenarios). For the second round, 50.0% (19 scenarios) were rated 8
Appropriate and 50.0% (19 scenarios) were rated May Be Appropriate. Disagreement was seen on 2.6% 9
(1 scenario). No scenarios were rated Rarely Appropriate in either round. 10
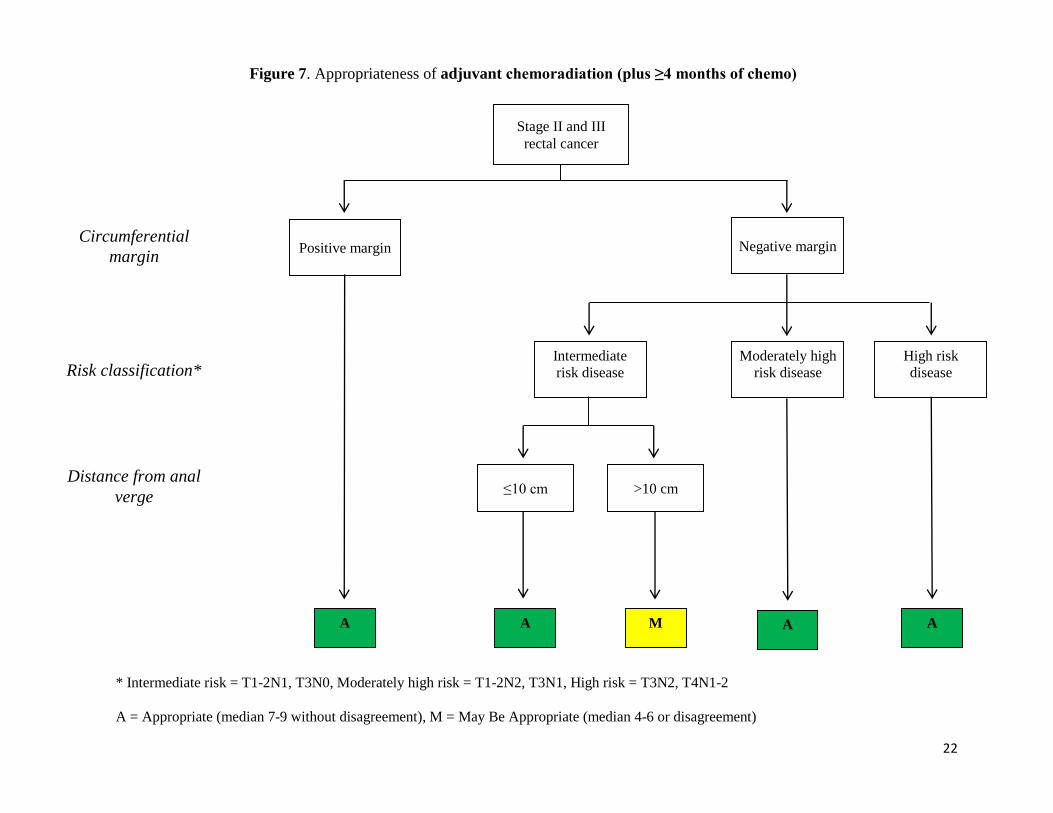
The expert panel was asked to consider the benefit of chemoradiation in addition to ≥4 months of 11
chemotherapy and of chemotherapy alone in the adjuvant setting in the setting of a patient resected with 12
a positive CRM. Chemoradiation was assumed to be standard, long-course pelvic radiotherapy with 13
concurrent infusional 5-FU or capecitabine and chemotherapy could be adjuvant 5-FU and leucovorin, 14
FOLFOX, capecitabine, or CapeOx. Panel members identified the occurrence of a positive margin in a 15
patient who did not undergo pre-operative chemoradiation as “inadvertent” and potentially suggestive of 16
poor quality surgery in the era of TME, more accurate pre-operative staging and imaging, and the 17
established role of pre-operative pelvic radiotherapy. The panel rating of 9 (the maximum in the 18
Appropriate category) indicated a strong agreement for chemoradiation in addition to ≥4 months of 19
chemotherapy (Figure 7). The panel rating of 4 for chemotherapy alone just met criteria for May Be 20
Appropriate, reflecting some uncertainty to this approach in the setting of positive margins, although it 21
may be suitable in some scenarios (Figure 8). 22
21
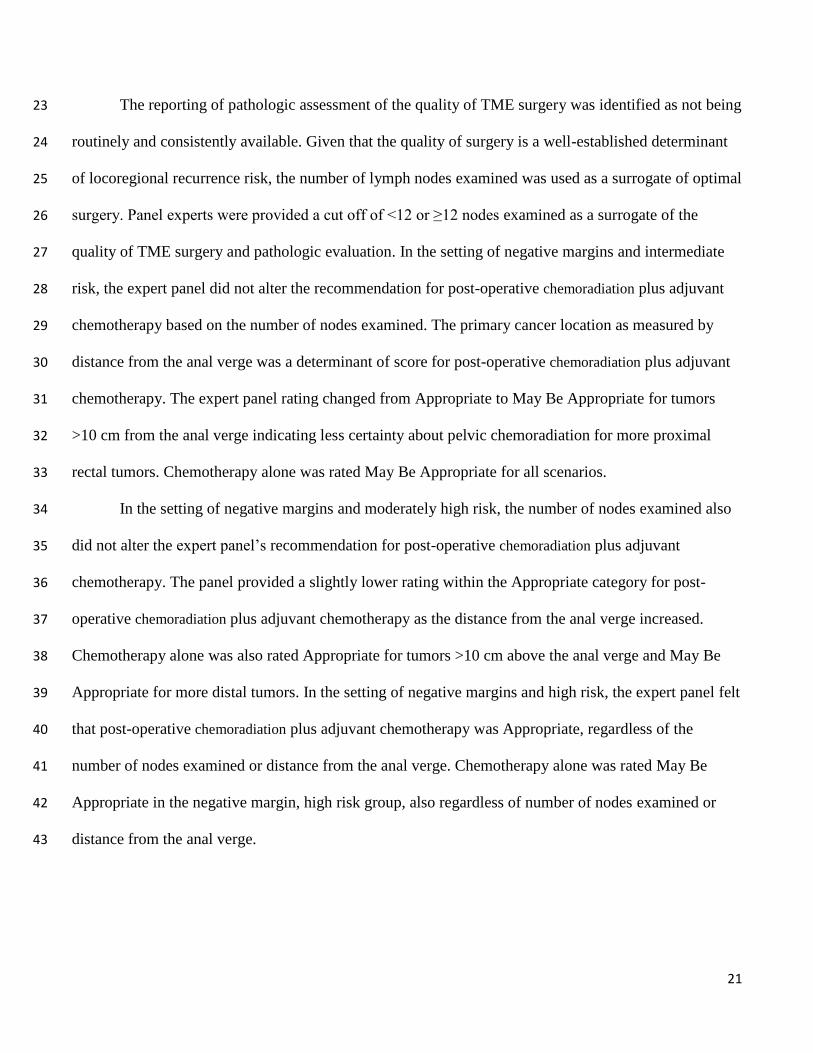
The reporting of pathologic assessment of the quality of TME surgery was identified as not being 23
routinely and consistently available. Given that the quality of surgery is a well-established determinant 24
of locoregional recurrence risk, the number of lymph nodes examined was used as a surrogate of optimal 25
surgery. Panel experts were provided a cut off of <12 or ≥12 nodes examined as a surrogate of the 26
quality of TME surgery and pathologic evaluation. In the setting of negative margins and intermediate 27
risk, the expert panel did not alter the recommendation for post-operative chemoradiation plus adjuvant 28
chemotherapy based on the number of nodes examined. The primary cancer location as measured by 29
distance from the anal verge was a determinant of score for post-operative chemoradiation plus adjuvant 30
chemotherapy. The expert panel rating changed from Appropriate to May Be Appropriate for tumors 31
>10 cm from the anal verge indicating less certainty about pelvic chemoradiation for more proximal 32
rectal tumors. Chemotherapy alone was rated May Be Appropriate for all scenarios. 33
In the setting of negative margins and moderately high risk, the number of nodes examined also 34
did not alter the expert panel’s recommendation for post-operative chemoradiation plus adjuvant 35
chemotherapy. The panel provided a slightly lower rating within the Appropriate category for post-36
operative chemoradiation plus adjuvant chemotherapy as the distance from the anal verge increased. 37
Chemotherapy alone was also rated Appropriate for tumors >10 cm above the anal verge and May Be 38
Appropriate for more distal tumors. In the setting of negative margins and high risk, the expert panel felt 39
that post-operative chemoradiation plus adjuvant chemotherapy was Appropriate, regardless of the 40
number of nodes examined or distance from the anal verge. Chemotherapy alone was rated May Be 41
Appropriate in the negative margin, high risk group, also regardless of number of nodes examined or 42
distance from the anal verge. 43
22
* Intermediate risk = T1-2N1, T3N0, Moderately high risk = T1-2N2, T3N1, High risk = T3N2, T4N1-2
A = Appropriate (median 7-9 without disagreement), M = May Be Appropriate (median 4-6 or disagreement)
Risk classification*
Distance from anal
verge
Circumferential
margin
≤10 cm
Stage II and III
rectal cancer
Negative margin Positive margin
A A A M
High risk
disease
Intermediate
risk disease
>10 cm
Moderately high
risk disease
A
Figure 7. Appropriateness of adjuvant chemoradiation (plus ≥4 months of chemo)

23
1
* Intermediate risk = T1-2N1, T3N0, Moderately high risk = T1-2N2, T3N1, High risk = T3N2, T4N1-2
A = Appropriate (median 7-9 without disagreement), M = May Be Appropriate (median 4-6 or disagreement)
Risk classification*
Distance from anal
verge
Circumferential
margin
≤10 cm
Stage II and III
rectal cancer
Negative margin Positive margin
A M
High risk
disease
Intermediate
risk disease
>10 cm
Moderately high
risk disease
M M M
Figure 8. Appropriateness of adjuvant chemotherapy alone

24
Medically inoperable patients 2
The third section contained 60 scenarios. The factors considered in this section were 3
performance status, presence of local symptoms, and distance from the anal verge. Good performance 4
status was defined as Eastern Cooperative Oncology Group (ECOG) performance status 0 to 1 and poor 5
performance status as ECOG performance status 2 or greater. The appropriateness of five treatments 6
was rated: external beam radiation alone, endorectal brachytherapy, chemoradiation alone, 7
chemoradiation plus endorectal brachytherapy, and chemotherapy alone. In the first round, 18.3% (11 8
scenarios) were rated Rarely Appropriate, 71.7% (43 scenarios) were rated May Be Appropriate, and 9
10% (6 scenarios) were rated Appropriate. Only 1.7% (1 scenario) had disagreement. In the second 10
round, 10.0% (6 scenarios) were rated Appropriate, 73.3% (44 scenarios) rated May Be Appropriate, 11
and 16.7% (10 scenarios) rated Rarely Appropriate. There were no scenarios with disagreement. 12
Although data regarding best treatment for medically inoperable rectal cancer are limited, there 13
was general agreement from the expert panel across all scenarios. Chemoradiation alone was 14
consistently rated Appropriate for good performance status patients and May Be Appropriate for poor 15
performance status patients (Figure 12). External beam radiation alone was rated May Be Appropriate 16
for all medically inoperable scenarios (Figure 11). Chemotherapy alone was also rated May Be 17
Appropriate, although supporting data are limited (Figure 13). Endorectal brachytherapy alone was not 18
rated Appropriate for any scenario, but rather was largely rated May Be Appropriate for tumors less than 19
10 cm from the anal verge (Figure 9). The combination of chemoradiation and endorectal brachytherapy 20
was rated May Be Appropriate for scenarios with tumor <10 cm from the anal verge with the exception 21
of poor performance status patients with tumors 5-10 cm from the anal verge, which was rated Rarely 22
Appropriate (Figure 10). 23

25
Location from the anal verge was only a factor for endorectal brachytherapy and the presence or 24
absence of symptoms had minimal impact on ratings. It is important to note that, if definitive doses of 25
endorectal brachytherapy are delivered (6.5 Gy x 4), patients may have increased rectal symptoms if 26
they do not undergo resection. The only effect of performance status was on the use of chemotherapy in 27
combination with radiation, which was rated Appropriate in good performance status patients. These 28
were the only scenarios rated Appropriate by the panel. Patients with medically inoperable rectal cancer 29
were rated May Be Appropriate for external beam radiation alone or chemotherapy alone, for most 30
scenarios for endorectal brachytherapy alone and chemoradiation plus endorectal brachytherapy if < 10 31
cm from verge, and for chemoradiation with poor performance status. 32

26
Medically inoperable
stage II and III rectal
cancer
Present Absent
>10 cm ≤10 cm
M R
Performance status
Local Symptoms
Distance from anal
verge
Poor performance
status (ECOG ≥2)
Good performance
status (ECOG 0-1)
≥5 cm <5 cm >10 cm ≤10 cm
M R M R
M = May Be Appropriate (median 4-6 or disagreement), R = Rarely Appropriate (median 1-3 without disagreement)
Figure 9. Appropriateness of definitive endorectal brachytherapy

27
M = May Be Appropriate (median 4-6 or disagreement), R = Rarely Appropriate (median 1-3 without disagreement)
Performance status
Local Symptoms
Distance from anal
verge
Medically inoperable
stage II and III rectal
cancer
Poor
performance
status
Good
performance
status
Present Absent
>10 cm ≤10 cm
M R
≥5 cm <5 cm
M R
>10 cm ≤10 cm
M R
Figure 10. Appropriateness of definitive chemoradiation plus endorectal brachytherapy

28
1
2
A = Appropriate (median 7-9 without disagreement), M = May Be Appropriate (median 4-6 or disagreement)
Medically inoperable
stage II and III rectal
cancer
M
All patient groups
Figure 11. Appropriateness of definitive
EBRT
Medically inoperable
stage II and III rectal
cancer
M
Poor
performance
status
Good
performance
status
A
Figure 12. Appropriateness of definitive
chemoradiation
Medically inoperable
stage II and III rectal
cancer
M
All patient groups
Figure 13. Appropriateness of definitive
chemotherapy alone

29
Patients seeking to avoid/refusing APR 3
The fourth section was comprised of 32 scenarios in the initial round. All patients covered had 4
low-lying tumors (<5 cm from the anal verge) and were otherwise operative candidates but were 5
attempting to achieve response to chemoradiation and avoid permanent colostomy. It was specified that 6
patients who progressed or did not respond to chemoradiation (based on physician assessment) should 7
receive an APR. The scenarios incorporated three factors: nodal status, T-category, and whether a full 8
thickness transanal excision had been performed. Patients who had T1 or T2 tumors and were node 9
negative were excluded since they have stage I disease and are outside the scope of this Clinical Practice 10
Statement. The treatments rated in the first round were endorectal brachytherapy, chemoradiation, 11
chemoradiation together with endorectal brachytherapy, and APR. 12
After extensive discussion during the in-person meeting, the expert panel, which was composed 13
of a multidisciplinary group including several colorectal surgeons, decided not to rate the individual 14
scenarios since the overall question was whether there is any alternative to an APR in patients who 15
refuse surgery. The surgeons also made the argument that, although the original scenarios made a 16
distinction between whether a patient had a full thickness transanal excision or not, if a full-thickness 17
transanal excision were possible then a low anterior resection with a coloanal anastomosis could be 18
performed and an APR is not needed. The panel was also concerned that by rating the radiation options, 19
they would be recommending use of a non-standard therapy rather than having another surgeon 20
potentially perform a radical resection without an APR. Therefore, the panel opted to replace the section 21
with a single new question regarding patients with stage II or III very low lying tumors refusing the 22
standard treatment, APR, and emphasized the fact that this was in the setting of patient refusal and 23
therefore outside of the standard approach. Panelists were asked to then rate chemoradiation (standard 24
30
dose), chemoradiation (standard dose) plus endorectal brachytherapy boost, and chemoradiation with 25
external beam radiation boost. 26
In the first round, using the original questions, 25% (8 scenarios) were rated Rarely Appropriate, 27
28.1% (9 scenarios) were rated May Be Appropriate, and 46.9% (15 scenarios) were rated Appropriate. 28
Disagreement was found for 12.5% (4 scenarios). In the second round, with the new question, all three 29
scenarios were rated Appropriate with no disagreement. The panel felt that in the scenario of patient 30
refusal of an APR, any of the radiation approaches could be justified (Figures 14 to 16). 31

31
32
33
Figure 14. Appropriateness of definitive
chemoradiation (standard dose)
Stage II and III rectal
cancer
A
Patient with very low
lying tumor refusing
abdominoperineal
resection
Figure 15. Appropriateness of definitive
chemoradiation (standard dose) plus endorectal
brachytherapy
Stage II and III rectal
cancer
A
Patient with very low
lying tumor refusing
abdominoperineal
resection
Figure 16. Appropriateness of definitive
chemoradiation (standard dose) with EBRT
boost
Stage II and III rectal
cancer
A
Patient with very low
lying tumor refusing
abdominoperineal
resection
A = Appropriate (median 7-9 without disagreement)
32
IMRT 34
In addition to the four sections, two supplemental questions were also included, which asked the 35
Expert Panel to rate the appropriateness of using IMRT to deliver neoadjuvant and adjuvant treatment. 36
IMRT was rated May Be Appropriate in both settings during the first round, with disagreement seen for 37
neoadjuvant therapy. For the second round of rating, neoadjuvant therapy was separated into short-38
course RT and chemoradiation at the request of the expert panel. All three options were subsequently 39
rated May Be Appropriate, with no disagreement. 40
While the question addressed the use of IMRT in three different scenarios, neoadjuvant short-41
course pelvic radiotherapy, neoadjuvant long-course chemoradiation, and adjuvant chemoradiation, the 42
ratings were all May Be Appropriate (Figures 17 to 19). Further distinction between the situations was 43
not possible due to the lack of familiarity with the technical aspects of IMRT versus 3D-CRT among the 44
non-radiation oncologists on the panel. Thus, the multidisciplinary expert panelists deferred for this 45
question to the radiation oncologists who generally felt that the use of IMRT would be a case-by-case 46
decision and there might be extenuating circumstances when it would add substantial benefit. 47

33
48
Figure 17. Appropriateness of neoadjuvant short-
course RT delivered with IMRT
Stage II and III rectal
cancer
M
Figure 18. Appropriateness of neoadjuvant
chemoradiation delivered with IMRT
Stage II and III rectal
cancer
M
Figure 19. Appropriateness of adjuvant therapy
delivered with IMRT
Stage II and III rectal
cancer
M
M = May Be Appropriate (median 4-6 or disagreement)
34
Discussion 49
The analysis of the ratings of the many clinical scenarios that were evaluated by the expert panel 50
demonstrate that, while a standard treatment approach exists in stage II and III rectal cancer, further 51
studies are necessary to refine the treatment recommendations. The expert panelists had very good 52
agreement (only one final scenario had disagreement) for the appropriateness of the various treatment 53
options presented, which reflects the excellent multidisciplinary approach that has been applied to the 54
management of rectal cancer. Emerging options such as short-course radiotherapy, neoadjuvant 55
chemotherapy alone, and non-operative management in the setting of patient refusal of an APR were 56
included in this Clinical Practice Statement, despite the lack of widespread use or limited high level 57
evidence regarding these options in the United States, to provide practicing radiation oncologists with 58
the current assessment of the appropriateness of these options. Given the strong relationship between the 59
quality of TME surgery and local recurrence, a relationship that is not mitigated by the use of adjuvant 60
radiation,44 we assumed high quality TME surgery was performed when rating scenarios that included 61
surgery. 62
63
Neoadjuvant therapy 64
Patients presenting for neoadjuvant therapy before definitive surgery make the bulk of referrals 65
for rectal cancer to the radiation oncologist. Following the seminal German rectal cancer trial,7 it was 66
established that neoadjuvant chemoradiation improves local control with decreased toxicity as compared 67
with adjuvant chemoradiation. The approach offered in this trial, conventionally fractionated radiation 68
therapy with concurrent 5-FU based chemotherapy, was considered appropriate by all of the expert 69
panel members for stage II and stage III rectal cancer. This is also reflected in other clinical guidelines, 70
such as the NCCN8 and Cancer Care Ontario.45 71

35
More interestingly, panelists rated neoadjuvant short-course radiation therapy Appropriate in 72
many patients with non-threatened mesorectal fascia margins and May Be Appropriate in other patients. 73
This is consistent with the fact that short-course is not intended for downstaging as usually surgery is 74
performed within one to two weeks of finishing radiation therapy. The ratings have also been supported 75
by randomized studies comparing short-course with conventional chemoradiation,46,47 selective adjuvant 76
therapy,48 and no therapy.42 There are also ongoing randomized studies looking to incorporate short-77
course radiation with neoadjuvant chemotherapy.49,50 Although the use of short-course radiation has 78
been relatively uncommon in North America and has only recently been included in the current NCCN 79
guidelines, the Appropriate rating from the expert panel in this Clinical Practice Statement, based on 80
level I evidence supporting short-course radiation as an option, supports this as an acceptable 81
option.51,52 82
Another emerging area is the use of neoadjuvant chemotherapy alone for selected patients with 83
stage II or III rectal cancer. While the accrual of a large, phase III randomized trial is ongoing,18 the 84
expert panel rated this approach May Be Appropriate for selected patients in intermediate and 85
moderately high risk disease with non-threatened mesorectal fascia. There was no patient group that 86
neoadjuvant chemotherapy alone was rated Appropriate for and this regimen is not offered in the NCCN 87
guidelines currently. However, NCCN does now include induction chemotherapy followed by 88
chemoradiation, which was not part of the scenarios for this clinical practice statement. 89
Neoadjuvant brachytherapy alone was rated Rarely Appropriate across the scenarios. This has 90
been performed by select centers.53 This remains an area of active investigation and may be more 91
relevant in patients who are not surgical candidates, as described in the medically inoperable section, or 92
as a boost in well-selected patients.54 Finally, the expert panel rated forgoing neoadjuvant therapy 93
altogether for certain patients with stage II or III rectal cancer May Be Appropriate. These included 94

36
patients with mid to high rectal cancers with a non-threatened mesorectal fascia, undergoing TME. This 95
acknowledges that potential patient benefit from neoadjuvant therapy may be diminished by treatment-96
related toxicity, and that these patients may be evaluated for adjuvant therapy based on pathologic 97
findings. 98
99
Adjuvant therapy 100
Since modern practice has established the role of neoadjuvant radiation regimens as the standard 101
treatment for locally advanced rectal tumors,6 a positive CRM should be an uncommon clinical scenario 102
and may reflect inadequate pre-operative imaging, suboptimal TME technique, or very poor or 103
aggressive tumor biology. Understaging or lack of identification of a threatened mesorectal margin pre-104
operatively may also increase the risk of a post-operative positive CRM. When a positive margin does 105
occur, especially in the setting of high-quality surgery, it is associated with poor outcomes and the 106
question of how to address the potentially residual disease in the post-operative setting is always a 107
difficult one. There is no level 1 evidence to guide the management of a positive CRM but data from 108
clinical trials highlight the increased risk of local recurrence.42,44 High rates of long term local failure, 109
48.6% R1 vs. 7.7% R0, were observed on the adjuvant chemoradiation arm of the pre-operative vs. post-110
operative randomized German rectal cancer trial.7 A randomized trial (MRC CR07 + NCIC CTG C016) 111
of selective chemoradiation for patients with a positive CRM demonstrated inferior local control 112
compared to pre-operative short-course pelvic radiation therapy.55 However, there is no clinical trial 113
comparing adjuvant pelvic chemoradiotherapy to chemotherapy or observation alone on the setting of 114
positive margins. In the absence of clinical trials, post-operative chemoradiotherapy plus adjuvant 115
chemotherapy remains the standard treatment regimen in the setting of a positive CRM. 116

37
However, the alternative strategy of adjuvant chemotherapy alone in the setting of positive CRM 117
was also rated May Be Appropriate to Appropriate. This may be an option for patients who are not 118
eligible for post-operative therapy due to comorbid conditions, known contraindications to radiation 119
therapy, or patient refusal. Adjuvant chemotherapy alone might also be appropriate for patients with a 120
very high risk of systemic relapse, with the caution that chemotherapy alone may be associated with a 121
higher rate of locoregional recurrence, which is associated with significant morbidity both from the 122
pelvic recurrence and from any surgical salvage approach. 123
For adjuvant radiation and chemotherapy in the setting of negative CRM , the data are largely 124
derived from studies performed in the pre-TME era, when transmural or node positive cancers had a 125
local recurrence risk as high as 50%,56 which led to the NCI consensus statement in 19905 that adjuvant 126
chemoradiation was the new standard regimen. The expert panel was asked to consider the role of 127
adjuvant chemoradiation in the TME era, considering the individualized local control benefit and the 128
potential for normal tissue toxicity when pelvic radiotherapy is delivered in the post-operative setting.7 129
For most scenarios, adjuvant chemoradiation plus chemotherapy was rated Appropriate (Figure 7). 130
Adjuvant chemotherapy alone was rated May Be Appropriate or Appropriate (Figure 8), indicating that 131
the expert panel supported the approach that, with pathologic information demonstrating that for 132
intermediate risk disease (T3N0, T1-2N1), adjuvant chemotherapy results in similar outcomes as 133
adjuvant chemoradiation, based on pooled analyses of prospective data comparing adjuvant therapy 134
options after surgery. 135
The panel was also provided the number of lymph nodes reported in the pathology report as a 136
surrogate to estimate the adequacy of the surgical resection since this may often be the only quality 137
indicator available. However, node count may be a marker of the quality of pathology as well as surgery 138
and may also reflect disease biology. While the optimal lymph node yield for rectal cancer without 139

38
neoadjuvant therapy is still controversial, the <12 vs. ≥12 nodes examined was used in each risk based 140
scenario.57 Interestingly, the lymph node count did not alter the expert panel’s ratings for most scenarios, 141
thus reflecting the relative lack of utility of nodal count as a measure of quality of rectal cancer surgery. 142
The relationship between the location of the primary rectal cancer as measured by distance from 143
the anal verge and the benefit of pelvic radiotherapy also remains the subject of differing opinions. In 144
the pre-operative setting with TME surgery, secondary subset analyses have evaluated the benefit of 145
pelvic radiotherapy based on primary tumor location. The long term report of the Dutch TME trial 146
demonstrated that the benefit of short-course pre-operative pelvic radiotherapy was greater for greater 147
distance from the anal verge (p=0.03).42 If patients with a positive CRM were excluded from the 148
analysis, the relationship between the distance from the anal verge and radiotherapy disappeared and 149
irradiated patients had higher cancer-specific survival independent of distance from the anal verge.42 150
The Trans-Tasman Radiation Oncology Group (TROG) compared pre-operative short-course pelvic 151
radiotherapy to long-course chemo-radiotherapy in T3 rectal cancers. There was a non-significant 152
(p=0.21) trend toward decreased local recurrence for long-course treatment and tumors <5 cm from the 153
anal verge.47 In the adjuvant setting, 11 year data from the pre-operative vs. post-operative German 154
Rectal Cancer Trial, showed that at 10 years, post-operative chemoradiation was associated with a LR 155
risk of 9.3% vs. 18.7% if no post-operative treatment was delivered if the tumor was at 5 to <10 cm and 156
2.7% vs. 10.4% if the tumor was at 10-16 cm. On multivariate analysis, not receiving chemoradiation 157
was significantly associated with a higher local recurrence risk.7 Overall, there was general agreement 158
among the expert panel that increasing distance from the anal verge was associated with lower risk of 159
local recurrence. 160
For low lying rectal cancers <5cm from the anal verge, there was strong agreement in rating 161
adjuvant chemoradiation Appropriate for all patients regardless of risk category or number of nodes 162
39
examined. Long-term data from the Swedish Rectal Cancer Trial in the pre-TME era shows that the 163
local recurrence rate was 27% for tumors ≤5cm from anal verge, 26% for tumors 6-10 cm, and 12% for 164
tumors ≥11 cm.58 Moreover, the type of surgery performed may be considered as well, since data from 165
the Dutch CKVO trial have shown that, even with a good TME and a negative CRM, APR was 166
associated with presacral local recurrences.59 Post-operative chemoradiation was also associated with a 167
higher risk of local recurrence on multivariate analysis from updated data from the German Rectal 168
Cancer Trial in patients who had surgery that included intersphincteric resection or APR compared with 169
pre-operative radiation (P=0.03).59 170
The panelists rated adjuvant chemotherapy alone May Be Appropriate for patients with low-171
lying rectal cancers, including those where there is concern about an increased risk of toxicity to the 172
anastomosis depending on the type of surgery that has been performed (i.e. a hand-sewn coloanal 173
anastomosis). With post-operative chemoradiation, grade 3-4 anastomotic toxicity was seen in 12% of 174
patients in the German study.6 175
For R0 resected tumors at 5-10 cm from the anal verge, there was again strong consensus that 176
adjuvant regimens containing pelvic radiotherapy are appropriate. The surgeons on the panel noted that 177
more proximal anastomoses would be anticipated to better tolerate pelvic radiation. Strategies to 178
consider chemotherapy alone were also felt to be reasonable. 179
As the distance of the tumor from the anal verge increased to >10 cm, the strength of the 180
recommendation for adjuvant regimens containing radiation decreased. Intermediate risk tumors in this 181
category were rated as May Be Appropriate. Within the intermediate risk category, data from 182
Gunderson et al. have noted a 7% local failure for T1-2/N1 tumors vs. a 9% local failure for T3N0 183
tumors.13 Thus by risk category as well as distance from the anal verge, this category of patients would 184
be expected to have a relatively low rate of local failure, particularly in the more modern era with the 185

40
use of TME. For high risk tumors >10 cm from the anal verge, panelists rated the adjuvant radiation 186
regimens Appropriate but at the lowest end of this category (median of 7). However, it should be noted 187
that the location of the peritoneal reflection can vary in relation to the distance from the anal verge. 188
Therefore tumors at >10 cm from the anal verge may or may not be intraperitoneal. Adjuvant 189
chemotherapy only regimens were rated May Be Appropriate for intermediate and high risk tumors 190
regardless of nodes examined and Appropriate for tumors of moderate risk. 191
192
Medically inoperable 193
Medically inoperable patients are rare and there are limited data to guide choice of therapy. In 194
addition, this group of patients is heterogeneous with regard to reasons for inoperability. Factors other 195
than performance status and presence of symptoms likely impact choice of therapy. Uncontrolled pelvic 196
malignancy is known to be associated with significant symptoms in most patients. Thus, there was clear 197
consensus by the expert panel that local therapy, including some form of chemoradiation, is appropriate 198
in good performance status patients. 199
With the emerging data from the operable patients showing non-operative management may be 200
curative for selected patients with a clinical complete response after pre-operative chemoradiation,31,32,60 201
there was general consensus that chemoradiation was rated Appropriate. External beam radiation 202
combined with endorectal brachytherapy without surgery has been associated with excellent outcomes in 203
patients with favorable rectal cancers (<12 cm from anal verge, <3cm diameter, mobile without 204
ulceration, T1-2, grade 1-2) and may be used for unfavorable patients who are medically inoperable.61,62 205
Local control in more advanced T2-3 distal rectal cancers has been reported in >70% of patients treated 206
with a combination of endorectal brachytherapy, external radiation and interstitial brachytherapy with 5-207
year survival in excess of 60%.63 Given the excellent local control rates reported in selected patients and 208

41
potential for long-term survival, all medically inoperable patients should be evaluated for potentially 209
curative intent radiation therapy. 210
Endorectal brachytherapy alone has been demonstrated to be effective curative treatment for 211
grade 1-2, T1N0, < 3 cm diameter rectal cancers located < 10 cm from the anal verge.64 Extrapolating 212
from these data, the expert panel rated endorectal brachytherapy alone May Be Appropriate for 213
medically inoperable patients with distal tumors. In general, definitive endorectal high dose rate 214
brachytherapy is limited to tumors that are within 15 cm from the anal verge and less than 5 cm in 215
diameter given the dose of radiation to the surface.43,65 Also, endorectal brachytherapy is generally 216
contraindicated in patients with invasion of the anal sphincters given potential effects on sphincter 217
function. It should be noted that there are several approaches to rectal brachytherapy. The endorectal 218
approach based on the use of an endoluminal applicator and delivery of high-dose rate Iridium-192 219
using a remote afterloading technique was the technique evaluated in these clinical scenarios. However, 220
in Europe, early stage rectal tumors may be treated with Contact X-ray (50KV) brachytherapy (Papillon 221
technique) and more advanced tumors are addressed with interstitial transperineal Iridium-192 implants. 222
These approaches were not addressed in this Clinical Practice Statement since they are not commonly 223
employed in the United States. 224
The panel also felt that some patients in this section, particularly those with poor performance 225
status and an absence of local symptoms, should receive palliative treatment. However, this option was 226
not included in the rating. 227
228
Patient refusal of an APR 229
There is also growing interest in non-operative management for operable patients with low-lying 230
rectal cancers who have achieved a cCR to pre-operative chemoradiation to improve quality of life 231

42
following treatment for rectal cancer. While sphincter preservation can be achieved in some patients by 232
performing a low anterior resection with a coloanal anastomosis, these procedures may be associated 233
with impaired long-term bowel function.22 In addition, patients face the morbidity and mortality 234
attendant with major abdominal surgery and the need for temporary diversion if restoration of intestinal 235
continuity is possible. Finally, rectal cancer surgery also impacts sexual functioning. Several prospective 236
studies have evaluated patient-reported quality of life after treatment for rectal cancer and have 237
demonstrated low scores, particularly in patients with stomas or low rectal anastomoses.23-25 238
However, since non-operative management for stage II or III disease is still considered a non-239
standard approach, the panel did not want to rate its use for various clinical scenarios. The decision was 240
to address the situation in which a patient refuses standard therapy and consensus of the panel was that 241
local therapy with chemoradiation with or without endorectal brachytherapy was an inferior but 242
acceptable alternative to radical surgery. As more studies evaluate the non-operative approach with 243
intensive follow-up for patients with complete response to chemoradiation there may be future Clinical 244
Practice Statements that will have sufficient supporting literature to rate more specific clinical scenarios 245
and address additional considerations such as how to assess treatment response after chemoradiation. 246
247
IMRT 248
Further improvements in outcomes for rectal cancer patients may also come with incorporating 249
newer radiotherapy techniques to deliver more focal dose to the tumor and lymph node regions while 250
sparing the radiosensitive structures of the pelvis. By minimizing the toxicity to the normal tissues, 251
acute and long-term toxicities of pelvic radiotherapy may be reduced, thus improving the therapeutic 252
ratio of this approach. IMRT allows for more conformal delivery of radiotherapy by using computed-253
tomography (CT) based planning and sophisticated computational software to generate treatment plans. 254

43
However, the increased cost and lack of reimbursement for IMRT in many gastrointestinal cancers has 255
also impacted on its use. For this reason, the question was framed to identify specific situations where 256
IMRT might be more useful, for instance with higher dose-per-fraction, such as with neoadjuvant short-257
course RT where late effects have been shown to be significantly elevated versus surgery alone,19 as 258
well as in the post-operative setting, which is associated with more toxicity compared to neo-adjuvant 259
therapy.6 260
The use of IMRT for long-course neoadjuvant chemoradiation has been controversial in rectal 261
cancer given the lack of data addressing the benefit of a more conformal approach over standard 3-262
dimensional conformal radiotherapy. The only prospective study evaluating the use of IMRT in rectal 263
cancer was a yet-to-be published, single-arm Phase II trial, RTOG 0822. This study evaluated the use of 264
concurrent capecitabine and oxaliplatin with pelvic radiotherapy using IMRT planning. The primary 265
endpoint was an improvement in Grade 2 or higher gastrointestinal toxicity in this study as compared to 266
the RTOG 0247 trial, which used the same chemotherapy regimen with non-IMRT pelvic 267
radiotherapy.66 RTOG 0822 failed to demonstrate a significant benefit to the use of IMRT. However, 268
interpretation of this study is limited by the use of concurrent oxaliplatin with 5-FU based 269
chemoradiation given there have been four large, phase III randomized trials demonstrating increased GI 270
toxicity when oxaliplatin is added to pre-operative chemoradiation.67-70 IMRT planning may not have 271
been able to overcome the effect of the oxaliplatin on GI toxicity. Several retrospective studies have 272
demonstrated a reduction in GI toxicity using IMRT over 3D-CRT for rectal cancer.71,72 273
IMRT is most likely to be of benefit when inclusion of external iliac lymph nodes is indicated on 274
the basis of a T4 tumor with adherence to or invasion of an anterior organ that has lymphatic drainage to 275
external iliac nodes, when there is a large volume of non-displaceable small bowel in the pelvis, or when 276
treatment of the inguinal nodal regions or perineal scar is indicated. IMRT may also be indicated in 277

44
patients with medical comorbidities such as inflammatory bowel disease, or a pelvic kidney, which may 278
be associated with higher toxicity from pelvic radiotherapy. 279
280
Conclusion/Future Directions 281
Radiotherapy remains a standard component of management of rectal cancer; however, there is 282
still the need to further refine its role as part of neoadjuvant, adjuvant and definitive therapy in order to 283
better tailor therapy for patients with rectal cancer. This Clinical Practice Statement provides a 284
comprehensive overview of the therapeutic options for patients with locally advanced (Stage II/III) 285
rectal cancer and further classifies this larger group into subgroups based on known risk factors that 286
were described in the clinical scenarios. By utilizing a multi-disciplinary panel of experts, and including 287
both GI-specialized and non-GI-specialized radiation oncologists, the process effectively removes biases 288
which could result from a tendency to recommend treatments that are delivered by the panelists. Thus, 289
the appropriateness ratings were not only individualized and risk-stratified, but also representative of the 290
overall community of practitioners treating rectal cancer. Nonetheless, the ratings should not be taken 291
as absolutes, as there may be unique circumstances that require clinicians and patients to use best 292
clinical judgment in optimal decision making. The use of novel techniques such as IMRT was 293
considered in this Clinical Practice Statement and was felt to be potentially appropriate because it may 294
lead to less toxicity. However, further study to assess the impact of this approach on treatment outcomes 295
is warranted to ensure the appropriate technology utilization and this questions may be better answered 296
in future Clinical Practice Statements. 297
In the future, results of ongoing trials may help clarify areas of uncertainty, particularly with 298
regard to the use of neoadjuvant FOLFOX as an alternative to chemoradiation for selected risk-groups 299
of patients and the possibility of pursuing non-operative management in patients who have a complete 300

45
clinical response after chemoradiation. On-going studies of both molecular and imaging biomarkers may 301
also improve risk stratification and allow for more tailored therapies for rectal cancer patients. 302
Meanwhile, this Clinical Practice Statement will serve as an overview of options to help guide 303
physicians as we move toward more individualized approaches for our patients. 304
305
1. Gastrointestinal Tumor Study Group. Prolongation of the disease-free interval in surgically 306 treated rectal carcinoma. N Engl J Med. 1985;312(23):1465-1472. 307
2. Fisher B, Wolmark N, Rockette H, et al. Postoperative adjuvant chemotherapy or radiation 308
therapy for rectal cancer: results from NSABP protocol R-01. J Natl Cancer Inst. 1988;80(1):21-309 29. 310
3. Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk 311 rectal carcinoma. N Engl J Med. 1991;324:709-715. 312
4. Gastrointestinal Tumor Study Group. Radiation therapy and fluorouracil with or without 313 semustine for the treatment of patients with surgical adjuvant adenocarcinoma of the rectum. J 314 Clin Oncol. 1992;10:549-557. 315
5. National Institutes of Health Consensus Conference. Adjuvant therapy for patients with colon 316 and rectal cancer. JAMA. 1990;264(11):1444-1450. 317
6. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy 318 for rectal cancer. N Engl J Med. 2004;351(17):1731-1740. 319
7. Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for 320
locally advanced rectal cancer: Results of the German CAO/ARO/AIO-94 randomized phase III 321
trial after a median follow-up of 11 years. J Clin Oncol. 2012;30:1926-1933. 322 8. Benson AB, Venook AP, Bekaii-Saab T, et al. NCCN Clinical Practice Guidelines in Oncology: 323
Rectal Cancer. 2015;Version 2.2015. www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. 324
9. Jones WE, 3rd, Thomas CR, Jr., Herman JM, et al. ACR appropriateness criteria(R) resectable 325 rectal cancer. Radiat Oncol. 2012;7:161. 326
10. Union for International Cancer Control. Early Stage Rectal Cancer: 2014 Review of Cancer 327 Medicines on the WHO List of Essential Medicines. 2014. 328
www.who.int/selection_medicines/.../EarlyStageRectal.pdf. Accessed March 4, 2015. 329 11. Heald RJ, Beets G, Carvalho C. Report from a consensus meeting: response to 330
chemoradiotherapy in rectal cancer - predictor of cure and a crucial new choice for the patient: 331 on behalf of the Champalimaud 2014 Faculty for 'Rectal cancer: when NOT to operate'. 332 Colorectal Dis. 2014;16(5):334-337. 333
12. Gunderson LL, Sargent DJ, Tepper JE, et al. Impact of T and N substage on survival and disease 334 relapse in adjuvant rectal cancer: a pooled analysis. Int J Radiat Oncol Biol Phys. 2002;54:386-335
396. 336 13. Gunderson LL, Sargent DJ, Tepper JE, et al. Impact of T and N stage and treatment on survival 337
and relapse in adjuvant rectal cancer: a pooled analysis. J Clin Oncol. 2004;22:1785-1796. 338 14. Nougaret S, Reinhold C, Mikhael HW, Rouanet P, Bibeau F, Brown G. The use of MR imaging 339
in treatment planning for patients with rectal carcinoma: have you checked the "DISTANCE"? 340 Radiology. 2013;268(2):330-344. 341

46
15. Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. 342
Lancet. 1986;1(8496):1479-1482. 343 16. Enker WE, Thaler HT, Cranor ML, Polyak T. Total mesorectal excision in the operative 344
treatment of carcinoma of the rectum. J Am Coll Surg. 1995;181(4):335-346. 345
17. Schrag D, Weiser MR, Goodman KA, et al. Neoadjuvant chemotherapy without routine use of 346 radiation therapy for patients with locally advanced rectal cancer: a pilot trial. J Clin Oncol. 347 2014;32(6):513-518. 348
18. National Cancer Institute. Chemotherapy Alone or Chemotherapy Plus Radiation Therapy in 349 Treating Patients With Locally Advanced Rectal Cancer Undergoing Surgery. 350
http://www.cancer.gov/clinicaltrials/search/view?cdrid=715321&version=HealthProfessional. 351 Accessed August 25, 2014. 352
19. Peeters KC, Velde CJvd, Leer JW, et al. Late side effects of short-course preoperative 353 radiotherapy combined with total mesorectal excision for rectal cancer: increased bowel 354
dysfunction in irradiated patients--a Dutch colorectal cancer group study. J Clin Oncol. 355 2005;23:6199-6206. 356
20. Hendren SK, O'Connor BI, Liu M, et al. Prevalence of male and female sexual dysfunction is 357 high following surgery for rectal cancer. Ann Surg. 2005;242(2):212-223. 358
21. Lange MM, den Dulk M, Bossema ER, et al. Risk factors for faecal incontinence after rectal 359 cancer treatment. Br J Surg. 2007;94(10):1278-1284. 360
22. Kasparek MS, Hassan I, Cima RR, Larson DR, Gullerud RE, Wolff BG. Quality of life after 361
coloanal anastomosis and abdominoperineal resection for distal rectal cancers: sphincter 362 preservation vs quality of life. Colorectal Dis. 2011;13(8):872-877. 363
23. Engel J, Kerr J, Schlesinger-Raab A, Eckel R, Sauer H, Holzel D. Quality of life in rectal cancer 364 patients: a four-year prospective study. Ann Surg. 2003;238(2):203-213. 365
24. Grumann MM, Noack EM, Hoffmann IA, Schlag PM. Comparison of quality of life in patients 366
undergoing abdominoperineal extirpation or anterior resection for rectal cancer. Ann Surg. 367
2001;233(2):149-156. 368 25. Wilson TR, Alexander DJ. Clinical and non-clinical factors influencing postoperative health-369
related quality of life in patients with colorectal cancer. Br J Surg. 2008;95(11):1408-1415. 370
26. Janjan NA, Khoo VS, Abbruzzese J, et al. Tumor downstaging and sphincter preservation with 371 preoperative chemoradiation in locally advanced rectal cancer: the M. D. Anderson Cancer 372
Center experience. Int J Radiat Oncol Biol Phys. 1999;44:1027-1038. 373 27. de Campos-Lobato LF, Stocchi L, da Luz Moreira A, et al. Pathologic complete response after 374
neoadjuvant treatment for rectal cancer decreases distant recurrence and could eradicate local 375 recurrence. Ann Surg Oncol. 2011;18(6):1590-1598. 376
28. Maas M, Nelemans PJ, Valentini V, et al. Long-term outcome in patients with a pathological 377 complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient 378 data. Lancet Oncol. 2010;11(9):835-844. 379
29. Habr-Gama A, Perez RO, Nadalin W, et al. Operative versus nonoperative treatment for stage 0 380 distal rectal cancer following chemoradiation therapy: long-term results. Ann Surg. 381
2004;240:711-717. 382 30. Habr-Gama A, Perez RO, Proscurshim I, et al. Patterns of failure and survival for nonoperative 383
treatment of stage c0 distal rectal cancer following neoadjuvant chemoradiation therapy. J 384 Gastrointest Surg. 2006;10:1319-1328. 385
31. Maas M, Beets-Tan RG, Lambregts DM, et al. Wait-and-see policy for clinical complete 386 responders after chemoradiation for rectal cancer. J Clin Oncol. 2011;29:4633-4640. 387
47
32. Smith JD, Ruby JA, Goodman KA, et al. Nonoperative management of rectal cancer with 388
complete clinical response after neoadjuvant therapy. Ann Surg. 2012;256:965-972. 389 33. Fitch K, Bernstein SJ, Aguilar MD, et al. The RAND/UCLA Appropriateness Method User’s 390
Manual. Santa Monica, CA: RAND; 2001. 391
34. Halbert RJ, Figlin RA, Atkins MB, et al. Treatment of patients with metastatic renal cell cancer: 392 a RAND Appropriateness Panel. Cancer. 2006;107:2375-2383. 393
35. Poston GJ, Adam R, Alberts S, et al. OncoSurge: a strategy for improving resectability with 394 curative intent in metastatic colorectal cancer. J Clin Oncol. 2005;23:7125-7134. 395
36. Strosberg JR, Fisher GA, Benson AB, et al. Systemic treatment in unresectable metastatic well-396
differentiated carcinoid tumors: consensus results from a modified delphi process. Pancreas. 397 2013;42(3):397-404. 398
37. Dubois RW, Swetter SM, Atkins M, et al. Developing indications for the use of sentinel lymph 399 node biopsy and adjuvant high-dose interferon alfa-2b in melanoma. Arch Dermatol. 400
2001;137:1217-1224. 401 38. Gale RP, Park RE, Dubois RW, et al. Delphi-panel analysis of appropriateness of high-dose 402
therapy and bone marrow transplants in adults with acute myelogenous leukemia in 1st 403 remission. Leuk Res. 1999;23:709-718. 404
39. Herrin J, Etchason JA, Kahan JP, Brook RH, Ballard DJ. Effect of panel composition on 405 physician ratings of appropriateness of abdominal aortic aneurysm surgery: elucidating 406 differences between multispecialty panel results and specialty society recommendations. Health 407
Policy. 1997;42:67-81. 408 40. Kahan JP, Park RE, Leape LL, et al. Variations by specialty in physician ratings of the 409
appropriateness and necessity of indications for procedures. Med care. 1996;34(6):512-523. 410 41. Kapiteijn E, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total 411
mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345:638-646. 412
42. van Gijn W, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total 413
mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, 414 randomised controlled TME trial. Lancet Oncol. 2011;12(6):575-582. 415
43. Hesselager C, Vuong T, Pahlman L, et al. Short-term outcome after neoadjuvant high-dose-rate 416
endorectal brachytherapy or short-course external beam radiotherapy in resectable rectal cancer. 417 Colorectal Dis. 2013;15(6):662-666. 418
44. Quirke P, Steele R, Monson J, et al. Effect of the plane of surgery achieved on local recurrence 419 in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and 420
NCIC-CTG CO16 randomised clinical trial. Lancet. 2009;373(9666):821-828. 421 45. Wong R, Berry S, Spithoff K, et al. Preoperative or postoperative therapy for the management of 422
patients with stage II or III rectal cancer. Toronto, ON: Cancer Care Ontario; 2008 (endorsed 423 2013): https://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=14008. Accessed 424 September 23, 2014. 425
46. Bujko K, Nowacki MP, Nasierowska-Guttmejer A, Michalski W, Bebenek M, Kryj M. Long-426 term results of a randomized trial comparing preoperative short-course radiotherapy with 427
preoperative conventionally fractionated chemoradiation for rectal cancer. Br J Surg. 428 2006;93:1215-1223. 429
47. Ngan SY, Burmeister B, Fisher RJ, et al. Randomized trial of short-course radiotherapy versus 430 long-course chemoradiation comparing rates of local recurrence in patients with T3 rectal cancer: 431 Trans-Tasman Radiation Oncology Group trial 01.04. J Clin Oncol. 2012;30:3827-3833. 432

48
48. Stephens RJ, Thompson LC, Quirke P, et al. Impact of short-course preoperative radiotherapy 433
for rectal cancer on patients. J Clin Oncol. 2010;28:4233-4239. 434 49. Myerson RJ, Tan B, Hunt S, et al. Five fractions of radiation therapy followed by 4 cycles of 435
FOLFOX chemotherapy as preoperative treatment for rectal cancer. Int J Radiat Oncol Biol 436
Phys. 2014;88(4):829-836. 437 50. Nilsson PJ, van Etten B, Hospers GA, et al. Short-course radiotherapy followed by neo-adjuvant 438
chemotherapy in locally advanced rectal cancer--the RAPIDO trial. BMC cancer. 2013;13:279. 439 51. Benson AB, Venook AP, Bekaii-Saab T, et al. NCCN Clinical Practice Guidelines in Oncology: 440
Rectal Cancer. 2016;Version 1.2016. www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. 441
52. Benson A, Venook A, Bekaii-Saab T, et al. NCCN Clinical Practice Guidelines in Oncology: 442 Rectal Cancer. Version 1.2015: www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. 443 Accessed September 23, 2014. 444
53. Vuong T, Devic S, Moftah B, Evans M, Podgorsak EB. High-dose-rate endorectal brachytherapy 445
in the treatment of locally advanced rectal carcinoma: technical aspects. Brachytherapy. 446 2005;4(3):230-235. 447
54. Appelt AL, Vogelius IR, Ploen J, et al. Long-term results of a randomized trial in locally 448 advanced rectal cancer: no benefit from adding a brachytherapy boost. Int J Radiat Oncol Biol 449
Phys. 2014;90(1):110-118. 450 55. Sebag-Montefiore D, Stephens RJ, Steele R, et al. Preoperative radiotherapy versus selective 451
postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG 452
C016): a multicentre, randomised trial. Lancet. 2009;373:811-820. 453 56. Rich T, Gunderson LL, Lew R, Galdibini JJ, Cohen AM, Donaldson G. Patterns of recurrence of 454
rectal cancer after potentially curative surgery. Cancer. 1983;52(7):1317-1329. 455 57. Bhangu A, Kiran RP, Brown G, Goldin R, Tekkis P. Establishing the optimum lymph node yield 456
for diagnosis of stage III rectal cancer. Tech Coloproctol. 2014;18(8):709-717. 457
58. Folkesson J, Birgisson H, Pahlman L, Cedermark B, Glimelius B, Gunnarsson U. Swedish 458
Rectal Cancer Trial: long lasting benefits from radiotherapy on survival and local recurrence 459 rate. J Clin Oncol. 2005;23:5644-5650. 460
59. Kusters M, Marijnen CA, van de Velde CJ, et al. Patterns of local recurrence in rectal cancer; a 461
study of the Dutch TME trial. Eur J Surg Oncol. 2010;36(5):470-476. 462 60. Habr-Gama A, Gama-Rodrigues J, Sao Juliao GP, et al. Local recurrence after complete clinical 463
response and watch and wait in rectal cancer after neoadjuvant chemoradiation: impact of 464 salvage therapy on local disease control. Int J Radiat Oncol Biol Phys. 2014;88(4):822-828. 465
61. Kodner IJ, Gilley MT, Shemesh EI, Fleshman JW, Fry RD, Myerson RJ. Radiation therapy as 466 definitive treatment for selected invasive rectal cancer. Surgery. 1993;114:850-856; discussion 467 856-857. 468
62. Maingon P, Guerif S, Darsouni R, et al. Conservative management of rectal adenocarcinoma by 469 radiotherapy. Int J Radiat Oncol Biol Phys. 1998;40:1077-1085. 470
63. Gerard JP, Chapet O, Ramaioli A, Romestaing P. Long-term control of T2-T3 rectal 471 adenocarcinoma with radiotherapy alone. Int J Radiat Oncol Biol Phys. 2002;54:142-149. 472
64. Papillon J. Present status of radiation therapy in the conservative management of rectal cancer. 473 Radiother Oncol. 1990;17:275-283. 474
65. Vuong T, Devic S, Podgorsak E. High dose rate endorectal brachytherapy as a neoadjuvant 475 treatment for patients with resectable rectal cancer. Clinical oncology (Royal College of 476 Radiologists (Great Britain)). 2007;19(9):701-705. 477

49
66. Garofalo M, Moughan J, Hong T, et al. RTOG 0822: A Phase II Study of Preoperative (PREOP) 478
Chemoradiotherapy (CRT) Utilizing IMRT in Combination with Capecitabine (C) and 479 Oxaliplatin (O) for Patients with Locally Advanced Rectal Cancer. Int J Radiat Oncol Biol Phys. 480 2011;81(2):S3-S4. 481
67. Aschele C, Cionini L, Lonardi S, et al. Primary tumor response to preoperative chemoradiation 482 with or without oxaliplatin in locally advanced rectal cancer: pathologic results of the STAR-01 483 randomized phase III trial. J Clin Oncol. 2011;29:2773-2780. 484
68. Gerard JP, Azria D, Gourgou-Bourgade S, et al. Comparison of two neoadjuvant 485 chemoradiotherapy regimens for locally advanced rectal cancer: results of the phase III trial 486
ACCORD 12/0405-Prodige 2. J Clin Oncol. 2010;28:1638-1644. 487 69. O'Connell MJ, Colangelo LH, Beart RW, et al. Capecitabine and oxaliplatin in the preoperative 488
multimodality treatment of rectal cancer: surgical end points from National Surgical Adjuvant 489 Breast and Bowel Project trial R-04. J Clin Oncol. Jun 20 2014;32(18):1927-1934. 490
70. Rodel C, Liersch T, Becker H, et al. Preoperative chemoradiotherapy and postoperative 491 chemotherapy with fluorouracil and oxaliplatin versus fluorouracil alone in locally advanced 492
rectal cancer: Initial results of the German CAO/ARO/AIO-04 randomised phase 3 trial. Lancet 493 Oncol. 2012;13:679-687. 494
71. Samuelian JM, Callister MD, Ashman JB, Young-Fadok TM, Borad MJ, Gunderson LL. 495 Reduced acute bowel toxicity in patients treated with intensity-modulated radiotherapy for rectal 496 cancer. Int J Radiat Oncol Biol Phys. 2012;82:1981-1987. 497
72. Yang TJ, Oh JH, Son CH, et al. Predictors of acute gastrointestinal toxicity during pelvic 498
chemoradiotherapy in patients with rectal cancer. Gastrointest Cancer Res. 2013;6(5-6):129-136. 499
500
Appendix 1: Complete rating tables 501
502 Section 1: Neoadjuvant therapy 503 504 Neoadjuvant therapy, intermediate risk, <5 cm from anal verge 505
Short-course
RT
Endorectal
brachytherapy
Chemoradiation Chemotherapy
alone
No neoadjuvant
therapy
Tumor edge < 2 mm
from edge of
mesorectal fascia 6
2
9
3
1
Tumor edge 2-5 mm
from edge of
mesorectal fascia 7 3
Tumor edge >5 mm
from edge of
mesorectal fascia
5
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 506 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 507 508 509 Neoadjuvant therapy, intermediate risk, 5-10 cm from anal verge 510

50
Short-course
RT
Endorectal
brachytherapy
Chemoradiation Chemotherapy
alone
No neoadjuvant
therapy
Tumor edge < 2 mm
from edge of
mesorectal fascia 5
2 9
3 1
Tumor edge 2-5 mm
from edge of
mesorectal fascia 7
4
3
Tumor edge >5 mm
from edge of
mesorectal fascia 4
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 511 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 512 513 514 Neoadjuvant therapy, intermediate risk, >10 cm from anal verge 515
Short-course
RT
Endorectal
brachytherapy
Chemoradiation Chemotherapy
alone
No neoadjuvant
therapy
Tumor edge < 2 mm
from edge of
mesorectal fascia
6 1
9
4
3
Tumor edge 2-5 mm
from edge of
mesorectal fascia 8
5
Tumor edge >5 mm
from edge of
mesorectal fascia 5 6
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 516 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 517 518 519 Neoadjuvant therapy, moderately high risk, <5 cm from anal verge 520
Short-course
RT
Endorectal
brachytherapy
Chemoradiation Chemotherapy
alone
No neoadjuvant
therapy
Tumor edge < 2 mm
from edge of
mesorectal fascia 5
2 9 3
1 Tumor edge 2-5 mm
from edge of
mesorectal fascia 6
Tumor edge >5 mm
from edge of
mesorectal fascia
2
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 521 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 522 523 524 Neoadjuvant therapy, moderately high risk, 5-10 cm from anal verge 525
Short-course
RT
Endorectal
brachytherapy
Chemoradiation Chemotherapy
alone
No neoadjuvant
therapy
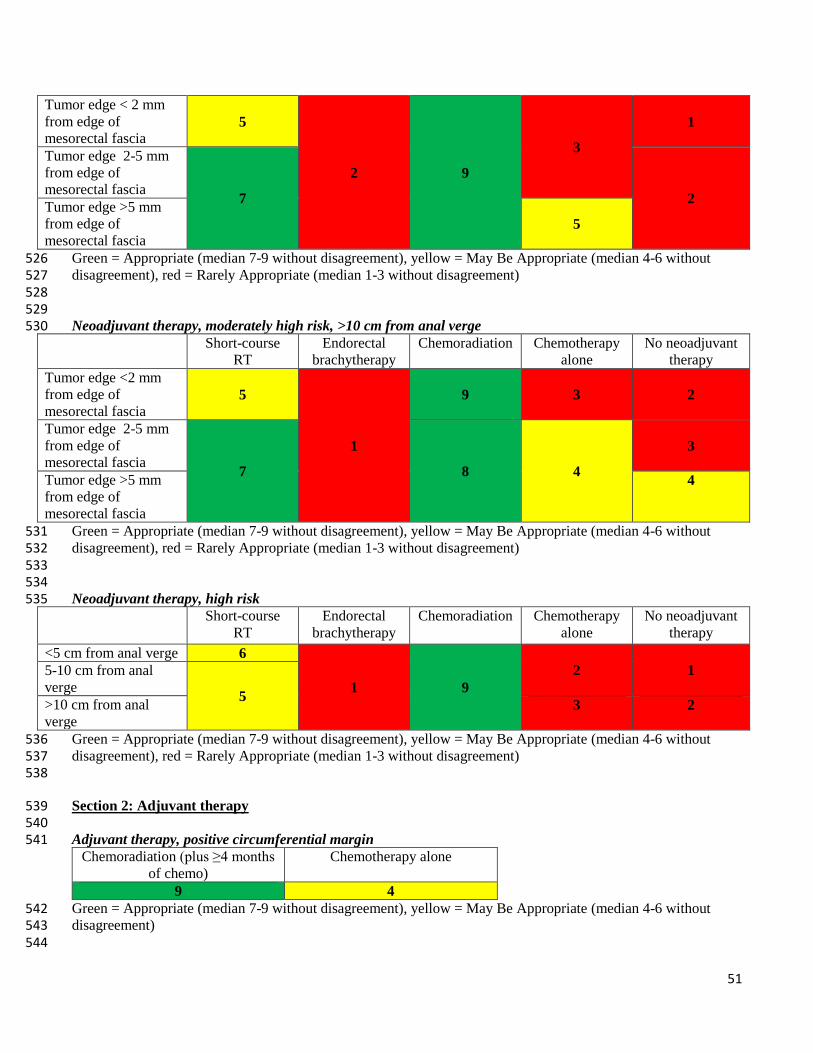
51
Tumor edge < 2 mm
from edge of
mesorectal fascia 5
2 9
3
1
Tumor edge 2-5 mm
from edge of
mesorectal fascia 7 2
Tumor edge >5 mm
from edge of
mesorectal fascia
5
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 526 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 527 528 529 Neoadjuvant therapy, moderately high risk, >10 cm from anal verge 530
Short-course
RT
Endorectal
brachytherapy
Chemoradiation Chemotherapy
alone
No neoadjuvant
therapy
Tumor edge <2 mm
from edge of
mesorectal fascia 5
1
9 3 2
Tumor edge 2-5 mm
from edge of
mesorectal fascia 7 8 4
3
Tumor edge >5 mm
from edge of
mesorectal fascia
4
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 531 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 532 533 534 Neoadjuvant therapy, high risk 535
Short-course
RT
Endorectal
brachytherapy
Chemoradiation Chemotherapy
alone
No neoadjuvant
therapy
<5 cm from anal verge 6
1 9
2 1 5-10 cm from anal
verge 5
>10 cm from anal
verge 3 2
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 536 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 537 538
Section 2: Adjuvant therapy 539 540 Adjuvant therapy, positive circumferential margin 541
Chemoradiation (plus ≥4 months
of chemo)
Chemotherapy alone
9 4
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 542 disagreement) 543 544
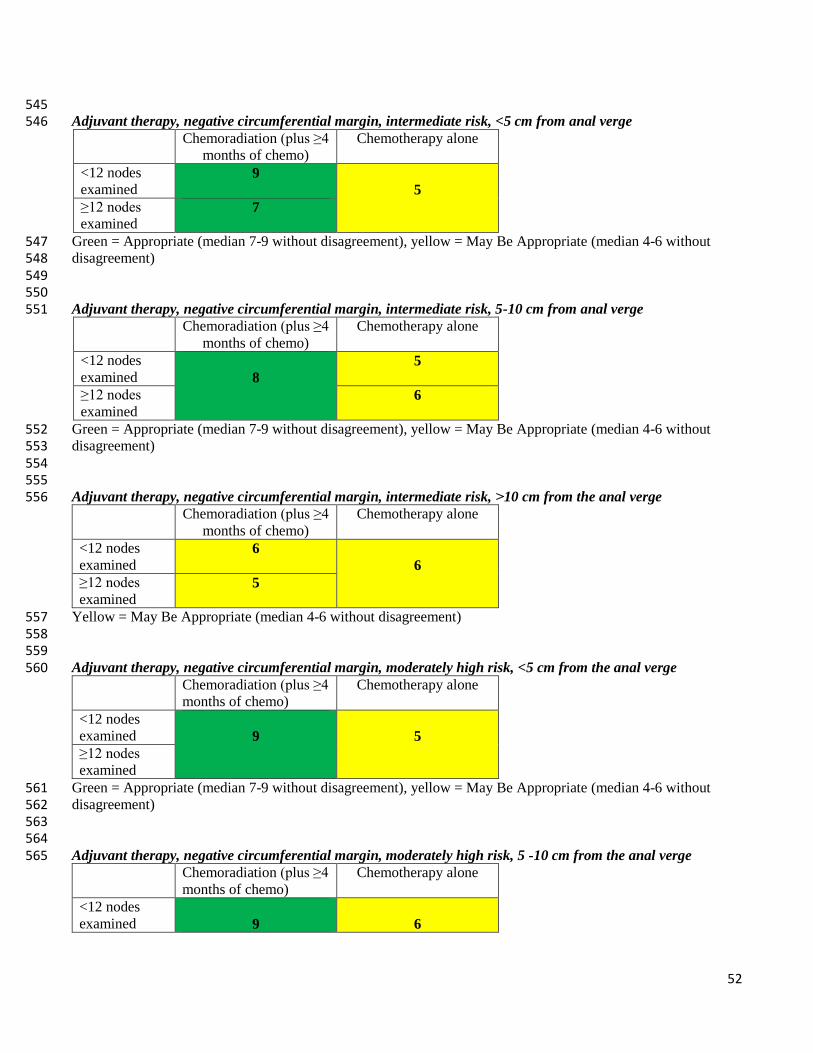
52
545 Adjuvant therapy, negative circumferential margin, intermediate risk, <5 cm from anal verge 546
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined 9
5
≥12 nodes
examined 7
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 547 disagreement) 548 549 550 Adjuvant therapy, negative circumferential margin, intermediate risk, 5-10 cm from anal verge 551
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined
8
5
≥12 nodes
examined 6
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 552 disagreement) 553 554 555 Adjuvant therapy, negative circumferential margin, intermediate risk, ˃10 cm from the anal verge 556
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined 6
6
≥12 nodes
examined 5
Yellow = May Be Appropriate (median 4-6 without disagreement) 557 558 559 Adjuvant therapy, negative circumferential margin, moderately high risk, <5 cm from the anal verge 560
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined
9
5
≥12 nodes
examined
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 561 disagreement) 562 563 564 Adjuvant therapy, negative circumferential margin, moderately high risk, 5 -10 cm from the anal verge 565
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined
9
6

53
≥12 nodes
examined
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 566 disagreement) 567 568 569 Adjuvant therapy, negative circumferential margin, moderately high risk, ˃10 cm from the anal verge 570
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined 8
7
≥12 nodes
examined 7
Green = Appropriate (median 7-9 without disagreement) 571 572 573 Adjuvant therapy, negative circumferential margin, high risk, <5 cm from the anal verge 574
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined
9
6
≥12 nodes
examined 5
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 575 disagreement) 576 577 578 Adjuvant therapy, negative circumferential margin, high risk, 5 -10 cm from the anal verge 579
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined
9
5
≥12 nodes
examined 5
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 580 disagreement), grey = May Be Appropriate due to disagreement 581 582 Adjuvant therapy, negative circumferential margin, high risk, ˃10 cm from the anal verge 583
Chemoradiation (plus ≥4
months of chemo)
Chemotherapy alone
<12 nodes
examined
7
6
≥12 nodes
examined
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 584 disagreement) 585 586 587 Section 3: Medically inoperable patients 588 589

54
Medically inoperable, good performance status (ECOG 0-1), local symptoms present 590 External beam
RT alone
Endorectal
brachytherapy
Chemoradiation Chemoradiation
plus endorectal
brachytherapy
Chemotherapy
alone
<5 cm from anal verge
5
4
9
6
4 5-10 cm from anal
verge 5
>10 cm from anal
verge 1 1 5
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 591 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 592 593
Medically inoperable, good performance status (ECOG 0-1), local symptoms absent 594 External beam
RT alone
Endorectal
brachytherapy
Chemoradiation Chemoradiation
plus endorectal
brachytherapy
Chemotherapy
alone
<5 cm from anal verge
5
4
9
6
5 5-10 cm from anal
verge 3 5
>10 cm from anal
verge 2 1 6
Green = Appropriate (median 7-9 without disagreement), yellow = May Be Appropriate (median 4-6 without 595 disagreement), red = Rarely Appropriate (median 1-3 without disagreement) 596 597
Medically inoperable, poor performance status (ECOG ≥2), local symptoms present 598 External beam
RT alone
Endorectal
brachytherapy
Chemoradiation Chemoradiation
plus endorectal
brachytherapy
Chemotherapy
alone
<5 cm from anal verge
6
5
5 5
4 5-10 cm from anal
verge 6 4
>10 cm from anal
verge 1 5 1
Yellow = May Be Appropriate (median 4-6 without disagreement), red = Rarely Appropriate (median 1-3 without 599 disagreement) 600 601
Medically inoperable, poor performance status (ECOG ≥2), local symptoms absent 602 External beam
RT alone
Endorectal
brachytherapy
Chemoradiation Chemoradiation
plus endorectal
brachytherapy
Chemotherapy
alone
<5 cm from anal verge
6
5
5
4
4 5-10 cm from anal
verge 4 3

55
>10 cm from anal
verge 1 1
Yellow = May Be Appropriate (median 4-6 without disagreement), red = Rarely Appropriate (median 1-3 without 603 disagreement) 604 605
Section 4: Patients with very low lying tumor refusing APR 606
Patient with very low lying tumor refusing abdominoperineal resection 607 Chemoradiation (standard dose) Chemoradiation (standard dose)
plus endorectal brachytherapy
Chemoradiation with EBRT boost
7 7 7
Green = Appropriate (median 7–9 without disagreement) 608 609
Intensity-modulated radiation therapy 610
Please rate the appropriateness of using IMRT to deliver: 611 Neoadjuvant short-course RT Neoadjuvant chemoradiation Adjuvant therapy
5 5 5
Yellow = May Be Appropriate (median 4-6 without disagreement) 612 613
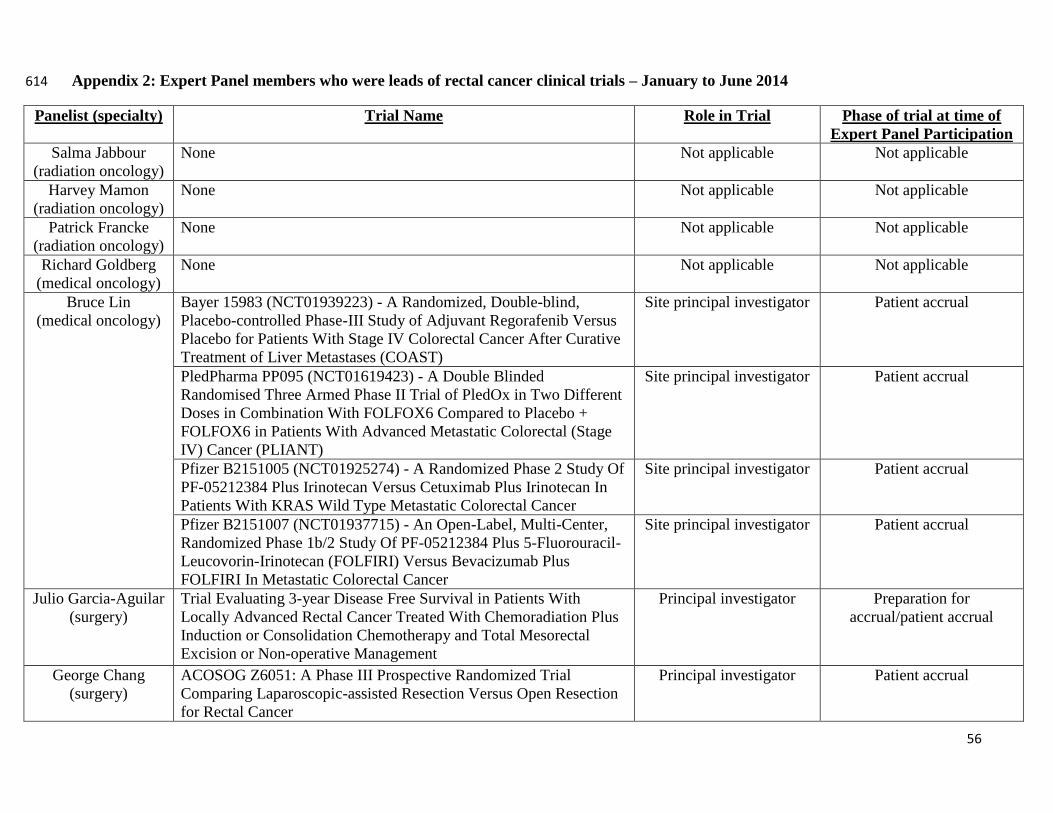
56
Appendix 2: Expert Panel members who were leads of rectal cancer clinical trials – January to June 2014 614
Panelist (specialty) Trial Name Role in Trial Phase of trial at time of
Expert Panel Participation
Salma Jabbour
(radiation oncology)
None Not applicable Not applicable
Harvey Mamon
(radiation oncology)
None Not applicable Not applicable
Patrick Francke
(radiation oncology)
None Not applicable Not applicable
Richard Goldberg
(medical oncology)
None Not applicable Not applicable
Bruce Lin
(medical oncology)
Bayer 15983 (NCT01939223) - A Randomized, Double-blind,
Placebo-controlled Phase-III Study of Adjuvant Regorafenib Versus
Placebo for Patients With Stage IV Colorectal Cancer After Curative
Treatment of Liver Metastases (COAST)
Site principal investigator Patient accrual
PledPharma PP095 (NCT01619423) - A Double Blinded
Randomised Three Armed Phase II Trial of PledOx in Two Different
Doses in Combination With FOLFOX6 Compared to Placebo +
FOLFOX6 in Patients With Advanced Metastatic Colorectal (Stage
IV) Cancer (PLIANT)
Site principal investigator Patient accrual
Pfizer B2151005 (NCT01925274) - A Randomized Phase 2 Study Of
PF-05212384 Plus Irinotecan Versus Cetuximab Plus Irinotecan In
Patients With KRAS Wild Type Metastatic Colorectal Cancer
Site principal investigator Patient accrual
Pfizer B2151007 (NCT01937715) - An Open-Label, Multi-Center,
Randomized Phase 1b/2 Study Of PF-05212384 Plus 5-Fluorouracil-
Leucovorin-Irinotecan (FOLFIRI) Versus Bevacizumab Plus
FOLFIRI In Metastatic Colorectal Cancer
Site principal investigator Patient accrual
Julio Garcia-Aguilar
(surgery)
Trial Evaluating 3-year Disease Free Survival in Patients With
Locally Advanced Rectal Cancer Treated With Chemoradiation Plus
Induction or Consolidation Chemotherapy and Total Mesorectal
Excision or Non-operative Management
Principal investigator Preparation for
accrual/patient accrual
George Chang
(surgery)
ACOSOG Z6051: A Phase III Prospective Randomized Trial
Comparing Laparoscopic-assisted Resection Versus Open Resection
for Rectal Cancer
Principal investigator Patient accrual

57
NCCTG N1048: A Phase II/III Trial of Neoadjuvant FOLFOX, with
Selective Use Of Combined Modality Chemoradiation versus
Preoperative Combined Modality Chemoradiation for Locally
Advanced Rectal Cancer Patients Undergoing Low Anterior
Resection with Total Mesorectal Excision
Principal investigator Patient accrual
A single blind, randomized, controlled study to evaluate the safety
and effectiveness of EVICEL as an adjunct to GI anastomosis
techniques, 2012-0235
Principal investigator Patient accrual
David Dietz
(surgery)
Timing of rectal cancer response to chemoradiation Site principal investigator Data analysis
Jeffrey Tokar
(gastroenterology)
CGI-066: Assessing Intratumoral Heterogeneity and Chemoradiation
Response In Locally Advanced Rectal Cancer Utilizing Sequencing
and PET/CT
Sub-investigator Patient accrual
(CIRB) N1048: A Phase II/III trial of Neoadjuvant FOLFOX, with
Selective Use of Combined Modality Chemoradiation versus
Preoperative Combined Modality Chemoradiation for Locally
Advanced Rectal Cancer Patients Undergoing Low Anterior
Resection with Total Mesorectal Excision
Sub-investigator Patient accrual
Marilyn Schapira
(internal med)
None Not applicable Not applicable
615







