
Anatomy and Physiology of Pain
“Pain is a more terrible lord of mankind than even death itself.”
Albert Schweitzer
Pain definitions:(The International Association for the Study of Pain (IASP)
An unpleasant sensory and emotional experience associated with actual or potential tissue damage
May not be directly proportional to amount of tissue injury
This definition recognizes that pain is a perception and not a sensation!!
Pain definitions:(hierarchical model of pain)
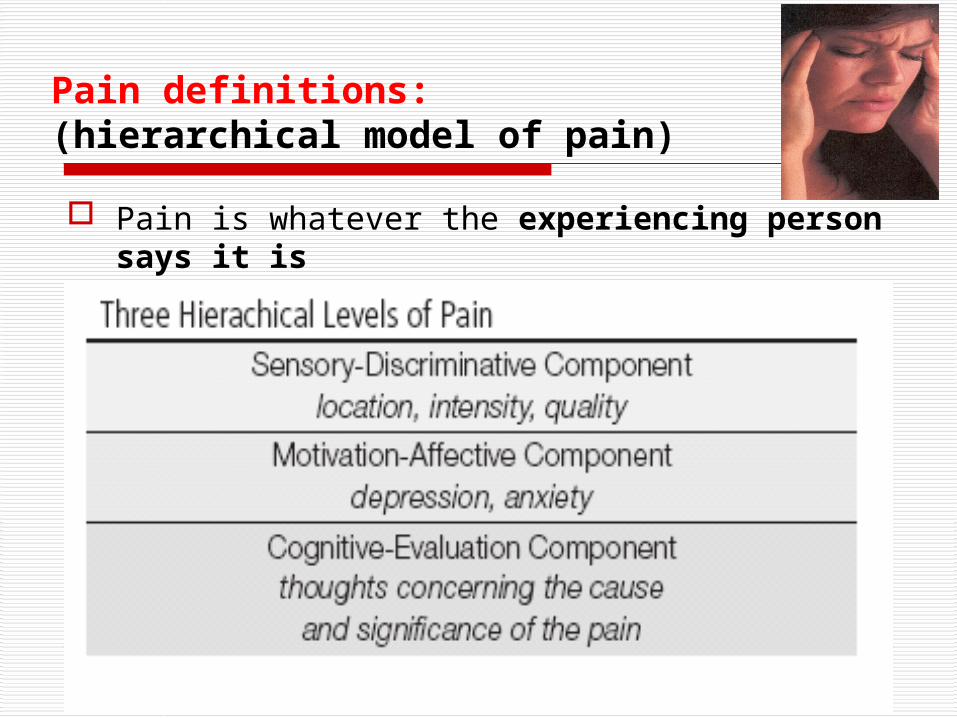
Pain is whatever the experiencing person says it is
Pain definitions - implication of both the IASP and the hierarchical model of pain
As a perception, pain may or may not correlate with an identifiable source of injury
The activity in the body’s “nociceptive” system, which senses noxious stimuli and generates a physiological and behavioral
response, can be initiated by injury and sustained by
neuroplastic changes even after healing
activity in this system can occur in the absence of any discrete injury but in association with a recognizable disease
Pain definitions - implication of both the IASP and the hierarchical model of pain
In some cases, pain can develop and be unrelated to any identifiable physical process
In all cases, the reality that pain is a perception indicates the potential for: profound influence of
psychological and emotional factors, cognitions
and varied external events
Pain definitions - implication of both the IASP and the hierarchical model of pain - concept of pain as perception
It is almost always best to believe that the patient is experiencing what is being reported.
Because there is no objective indicator for pain, experts agree that the best clinical approach in most circumstances is to assume that the patient is reporting a true experience, even in the absence of a clear explanation.
Importantly, accepting a patient’s complaint of pain as valid does not require clinical identification of a physical cause, or demand the initiation of a specific treatment.

Pain definitions - implication of both the IASP and the hierarchical model of pain - concept of pain as perception
Almost always, it is a sound foundation for assessment and an important beginning in developing an effective physician-patient dialogue.
The risk that rare cases of malingering or factitious disorder may lead the credulous physician to initial error is more than balanced by the benefits associated with a stance of compassionate acceptance and concern.

Types of Pain
1. Acute - a protective mechanism a protective mechanism that alerts the individual to a that alerts the individual to a condition or condition or experience that is experience that is immediatelyimmediately harmful to the bodyharmful to the body;; Onset - usually sudden Onset - usually sudden
2. Chronic - is persistentis persistent or or intermittentintermittent usually defined as lasting usually defined as lasting at at least least 6 6
monthsmonths

Types of PainResponses to acute painResponses to acute pain
diaphoresis diaphoresis pallor or flushingpallor or flushing increased heart rateincreased heart rate elevated blood pressure elevated blood pressure blood flow to the viscera, blood flow to the viscera, kidney kidney and skinand skin gastric acid secretion gastric acid secretion gastric motilitygastric motility nausea occasionally occursnausea occasionally occurs increased respiratory rateincreased respiratory rate dilated pupilsdilated pupils blood sugarblood sugar fearfear general sense of unpleasantness general sense of unpleasantness anxietyanxiety
Types of Pain - response to chronic pain
Psychological responsePsychological response Intermittent pain Intermittent pain produces a physiologic response produces a physiologic response
similar to acute painsimilar to acute pain Persistent pain Persistent pain allows for adaptation (functions of allows for adaptation (functions of
the body are normal but the pain is not reliefed)the body are normal but the pain is not reliefed)
Chronic pain Chronic pain producesproduces significant significant behavioural behavioural and and psychological changespsychological changes:: depression depression an attempt to keep pain - related behaviouran attempt to keep pain - related behaviour to a to a
minimumminimum sleeping disorderssleeping disorders preoccupation with the pain preoccupation with the pain tendency to deny paintendency to deny pain
The pain thresholdThe pain threshold - the point at which a - the point at which a stimulus is stimulus is perceived as painperceived as pain..
It does It does not vary significantly among not vary significantly among healthy healthy people people or in the same person over time or in the same person over time
PPerceptual dominanceerceptual dominance -- iintense pain ntense pain at one location may at one location may cause an cause an increase in the pain threshold increase in the pain threshold in another in another location location
The pain tolerance - duration of time or the intensity of pain that an individual will endured before initiation overt pain responses.
It is influenced by: - persons cultural prescriptions
- expectations - role behaviours - physical and mental health
Pain Pain tthreshold and hreshold and ppain ain ttoleranceolerance

Pain tolerance Pain tolerance is generally is generally decreaseddecreased:: with repeated exposure to pain with repeated exposure to pain by fatigue, anger, boredom, apprehensionby fatigue, anger, boredom, apprehension sleep deprivationsleep deprivation
Tolerance to pain may be Tolerance to pain may be increasedincreased:: by alcohol consumption by alcohol consumption medication, hypnosis medication, hypnosis warmth, distracting activities warmth, distracting activities strong beliefs or faith strong beliefs or faith
Pain tolerance Pain tolerance varies greatlyvaries greatlyamong peopleamong people in the in the samesame personperson over time over time aa decrease in pain tolerance decrease in pain tolerance is also evident in the is also evident in the elderlyelderlywomenwomen appear appear to be more to be more tolerant tolerant to pain than mento pain than men
Pain Pain tthreshold and hreshold and ppain ain ttoleranceolerance
Children and the elderlyChildren and the elderly may experience or express may experience or express pain pain differently than adultsdifferently than adults:: InfantsInfants in the in the first 1 to 2 daysfirst 1 to 2 days of life are of life are less less sensitivesensitive to pain (or they simply lack the ability to to pain (or they simply lack the ability to verbalise the pain experience)verbalise the pain experience) A full behavioural response A full behavioural response to pain is to pain is apparent apparent at 3 to 12 month of life at 3 to 12 month of life Older children, between the ages of Older children, between the ages of 15 and 18 15 and 18 yearsyears, , tend to have a lowertend to have a lower pain threshold than do pain threshold than do adultsadultsPain threshold tends to Pain threshold tends to increase with ageingincrease with ageing
tthis change is probably caused by his change is probably caused by peripheral peripheral neuropathiesneuropathies
and changes in the and changes in the thickness of the skinthickness of the skin
Age anAge andd pperception of erception of ppainain
Clasification of Pain - by pathophysiology
1. Nociceptive pain (stimuli from somatic and visceral structures)
2. Neuropathic pain (stimuli abnormally processed by the nervous system)
3.3. Psychogenic painPsychogenic pain is pain for which there is pain for which there is is ununknown physical causeknown physical cause but but processing processing of sensitive information in CNS of sensitive information in CNS is is ddysturbedysturbed
4.4. mixed mixed painpain
5.5. iidiopathicdiopathic pain pain
Nociceptive Pain and its Mechanisms
Clinically, pain can be labeled “nociceptive” if it is inferred that the pain is due to ongoing activation of the nociceptive system by tissue injury.
Although neuroplastic changes (such as those underlying tissue sensitization) are clearly involved, nociceptive pain is presumed to occur as a result of the normal activation of the sensory system by noxious stimuli, a process that involves 4 basic processes
Transduction Transmission Perception of pain Modulation of pain
Nociceptive Pain and its Mechanisms
Tissue injury activates primary afferent neurons called nociceptors, which are small diameter afferent neurons (with A-delta and C-fibers)
Nociceptors respond to noxious stimuli Nociceptors are found in
skin muscle joints and some visceral tissues.

Nociceptive Pain and its Mechanisms
Nociceptive primary afferent neurons are varied: Most are “silent” - active only when suprathreshold stimuli impinge Some are specific to one type of stimulus, such as
mechanical or thermal
but most are polymodalThe number and size of the receptive fields served by each fiber may be small or large, respectively
Nociceptive Pain and its Mechanisms
nociceptors free nerve endings has capacity to distinguish between noxious and innocuous stimuli when exposed to mechanical (incision or tumor growth) thermal (burn) chemical (toxic substance) stimuli
tissue damage occurs substances are released by the damaged
tissue which facilitates the movement of pain impulse to the spinal cord
Substances released
The substances released from the traumatized tissue are: prostaglandins bradykinin serotonin substance P Histamine Protons NGFThe role of this substances provide opportunities for the
development of new analgesic drugs
So, for instance
Non-steroidal anti-inflammatories, such as ibuprofen, are effective in minimizing pain because they minimize the effects of these substances released, especially prostaglandins
Corticosteroids, such as dexamethasone used for cancer pain, also interferes with the production of prostaglandins

1. Transduction sufficient amounts of noxious stimulation
cause the cell membrane of the neuron (nervous system cell) to become permeable to sodium ions, allowing the ions to rush into the cell and creating a temporary positive charge
then potassium transfers back into the cell, thus changing the charge back to a negative one
with this depolarization and repolarization, the noxious stimuli is converted to an impulse
this impulse takes just milliseconds to occur
Some analgesics relieve pain primarily by decreasing the sodium and potassium transfers at the neuron level, thereby slowing or stopping pain transmission Examples—local anesthetics,
anticonvulsants used for neuropathic pain, migraines
2.Transmission
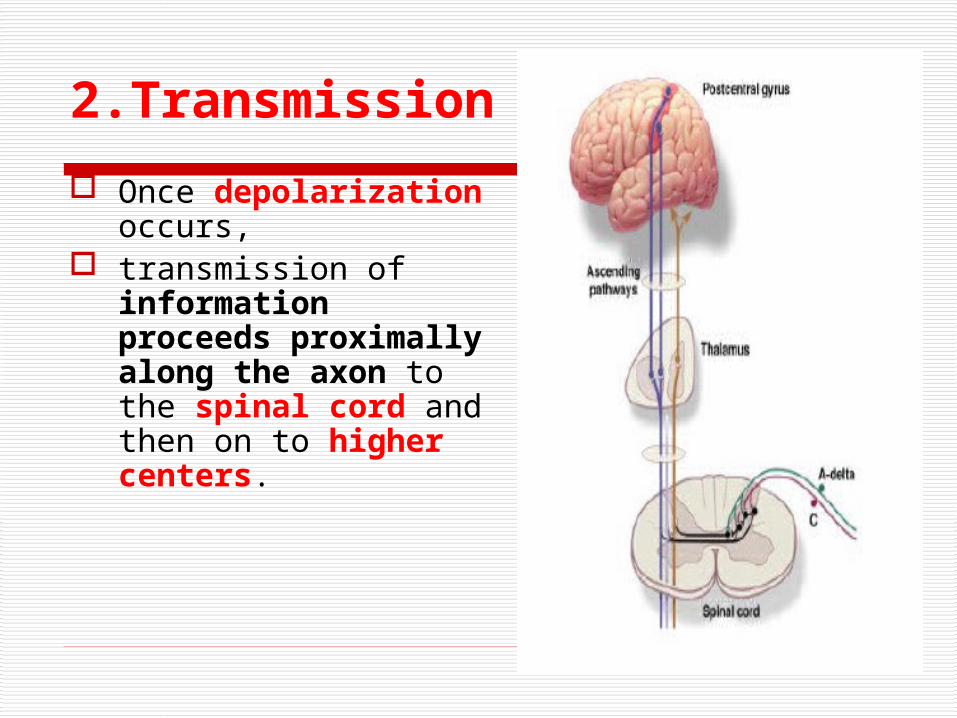
Once depolarization occurs,
transmission of information proceeds proximally along the axon to the spinal cord and then on to higher centers.

2.Transmission
Transmission across the first central synapse may be influenced by activity in the primary afferent itself and modulatory neural pathways
that originate segmentally or supraspinally
further modulation results from processes initated by glial cells.
2.Transmission
Impulse spinal cord brain stem thalamus central structures of brain pain is processed
Neurotransmitters are needed to continue the pain impulse from the spinal cord to the brain
3. Perception of Pain
the end result of the neural activity of pain transmission
it is believed pain perception occurs in the cortical structures behavioral strategies and therapy can be
applied to reduce pain brain can accommodate a limited number of
signals — distraction, imagery, relaxation signals may get
through the gate, leaving limited signals (such as pain) to be transmitted to the higher structures
4.Modulation of Pain
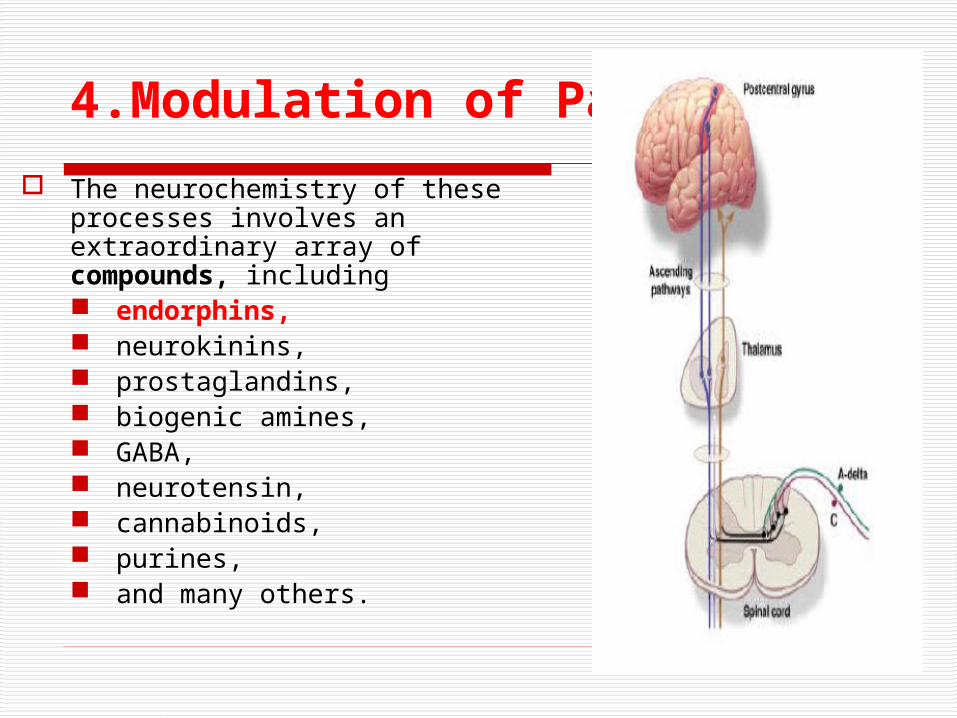
The neurochemistry of these processes involves an extraordinary array of compounds, including endorphins, neurokinins, prostaglandins, biogenic amines, GABA, neurotensin, cannabinoids, purines, and many others.
4.Modulation of Pain
The endorphinergic pain modulatory pathways are characterized by multiple endogenous ligands and different types of opioid receptors: mu, delta, and kappa.
Endorphins are present in the periphery, on nerve endings, immune-related cells and other tissues,
Endorphins are widely distributed in the central nervous system (CNS).
They are involved in many neuroregulatory processes apart from pain control, including the stress response and motor control systems.
Opioid drugs mimic the action of endogenous opioid ligands. Most of the drugs used for pain are full mu receptor agonists.
4.Modulation of Pain
Other pain modulating systems, such as those that use monoamines (serotonin, norepinephrine and dopamine), histamine, acetylcholine, cannabinoids, growth factors and other compounds,
are targets for nontraditional analgesics, such as specific antidepressants and anticonvulsants.
It is likely that entirely novel analgesic compounds will become commercially available in the future as drug development programs target these systems.
4.Modulation of Pain
changing or inhibiting pain impulses in the descending tract (brain spinal cord)
descending fibers also release substances such as norepinephrine and serotonin (referred to as endogenous opioids or endorphins) which have the capability of inhibiting the transmission of noxious stimuli
cancer pain responds to antidepressants which interfere with the reuptake of serotonin and norepinephrine which increases their availability to inhibit noxious stimuli
Clinical Characteristics of Nociceptive Pain
acute (short-lived, remitting) persistent (long-lived, chronic), primarily involve injury to somatic or visceral tissues. “somatic pain”- pain related to ongoing activation of
nociceptors that innervate somatic structures, such as bone, joint, muscle and connective tissues,
this pain is recognized by identification of a lesion characterisitics typically include a well localized site
and an experience described as aching, squeezing, stabbing, or throbbing.
Clinical Characteristics of Nociceptive Pain
Arthritis and metastatic bone pain are examples of somatic pain.
Pain arising from stimulation of afferent receptors in the viscera is referred to as visceral pain. Visceral pain caused by obstruction of hollow viscus is poorly localized and
is often described as cramping and gnawing, with a daily pattern of varying intensity.
when organ capsules or other structures such as myocardium, are involved, however, the pain usually is well localized and described as sharp, stabbing or throbbing,
descriptors similar to those associated with somatic pain.

Clinical Characteristics of Nociceptive Pain
Nociceptive pain may involve acute or chronic inflammation.
The physiology of inflammation is complex. an immune component retrograde release of substances from C polymodal
nociceptors - “neurogenic inflammation” - involves the release from nerve endings of compounds such as substance P, serotonin, histamine, acetylcholine, and bradykinin.
these substances activate and sensitize other nociceptors. Prostaglandins produced by injured tissues also may
enhance the nociceptive response to inflammation by lowering the threshold to noxious stimulation.

Neuropathic Pain and its Mechanisms
abnormal processing of the impulses either by the peripheral or central nervous system
may be caused by injury (amputation and subsequent phantom limb
pain) scar tissue from surgery (back surgery high risk) nerve entrapment (carpal tunnel) damaged nerves (diabetic neuropathy)
unclear why depolarization and transmission of pain impulse are spontaneous and repetitive

It occurs as a result of injury to or dysfunction of the nervous system itself, peripheral or central
Deaferentation pain - form of neuropathic pain: a term implying that sensory deficit in the painful area is a prominent feature (anesthesia dolorosa)
Phantom pain- pain localised into non-existing organ (tissue)
Long-lasting pain after short-lasting pain stimulus
Neuropathic Pain and its Neuropathic Pain and its MechanismsMechanisms
Acute PainAcute PainSomaticVisceralReffered pain
Somatic pain is superficial coming from the skin or close to the surface of the body.
Visceral pain refers to pain in internal organs, the abdomen, or chest.
Referred pain is pain that is present in an area removed or distant from its point of origin.
The area of referred pain is supplied by the nerves from the same spinal segment as the actual site of pain.
Clinical Manifestation of PainClinical Manifestation of Pain
I. Nervous system intact1. nociceptive pain
2. nociceptive - neurogenic pain (nerve trunk pain)
II. Permanent functional and/or morphological abnormalities of the nervous system (preganglionic, spinal - supraspinal)
1. neurogenic pain
2. neuropathic pain
3. deafferentation pain
Different types of chronic somatic painDifferent types of chronic somatic pain
The most commonThe most common chronic pain chronic pain
1. Persistent low back pain result of poor muscle tone, inactivity, muscle strain, sudden vigorous exercise
2. Chronic pain associated with cancer
3. Neuralgias - results from damages of peripheral nerves
Causalgia - severe burning pain appearing 1 to 2 weeks after the nerve injury associated with discoloration
and changes in the texture of the skin in the affected area.
Reflex sympathetic dystrophies - occur after peripheral
nerve injury and is characterised by continuous
severe burning pain. Vasomotor changes are
present (vasodilatation vasoconstriction
cool cyanotic and edematous extremities).
The most common chronic pain

The most common chronic pain
4. Myofascial pain syndromes - second most common cause of chronic pain.
include: myositis, fibrositis, myalgia, muscle
strain, injury to the muscle and fascia
The pain is a result of muscle spasm, tenderness and stiffness

5. Hemiagnosia a loss of ability to identify the source of pain on one side (the affected side) of the body. Application of painful stimuli to the affected side thus produces
anxiety, moaning, agitation and distress but no attempt to withdrawal from or push aside the offending stimulus. Emotional and autonomic responses to the pain my be intensified.
● Hemiagnosia is associated with stroke that produces paralysis and hypersensitivity to painful stimuli in the affected side
6. Phantom limb pain6. Phantom limb pain - - is pain that an individual feels in amputated limb
The most common chronic pain
MP - a part of somatic deep pain,
it is common in rheumathology and sports medicine
is rather diffuse and difficult to locate MP is not a prominent feature of the serious progressive diseases
affecting muscle, e.g. the muscular dystrophies, denervation, or metabolic myopathies, but it is a feature of
rhabdomyolysis Muscles are relatively insensitive to pain when elicited by needle
prick or knife cut, but overlying fascia is very sensitive to pain.
Events, processes which may lead to muscular pain are: metabolic events: metabolic depletion ( ATP muscular contracture) accumulation of unwanted metabolities (K+, bradykinin)
Pathophysiology of muscle painPathophysiology of muscle pain (MP) (MP)

Visceral pain:Visceral pain: TTypesypes - - angina pectoris, myocardial infarction, acute angina pectoris, myocardial infarction, acute
pancreatitis, cephalic pain, prostatic pain, pancreatitis, cephalic pain, prostatic pain,
nenephrphrlolytiatic painlolytiatic pain
Receptors:Receptors: unmyelinated C – fibresunmyelinated C – fibresFor human pathophysiology the kinds of stimuli apt to For human pathophysiology the kinds of stimuli apt to induce pain in the viscera are important. induce pain in the viscera are important.
It is well-known that the stimuli likely toIt is well-known that the stimuli likely to induce cutaneous induce cutaneous
pain are not algogenicpain are not algogenic inin the viscera. This explains why in the viscera. This explains why in
the past the viscera werethe past the viscera were considered to be insensitive considered to be insensitive
to painto pain
Pathophysiology of visceral painPathophysiology of visceral pain

• 1. abnormal distention and contraction of the hollow viscera muscle walls
2. rapid stretching of the capsule of such solid visceral organs as are the liver, spleen, pancreas...
3. abrupt anoxemia of visceral muscles4. formation and accumulation of pain - producing
substances
5. direct action of chemical stimuli (oesophagus,
stomach)
6. traction or compression of ligaments and vessels
7. inflammatory processes
8. necrosis of some structures (myocardium, pancreas)
Adequate stimuli of inducing visceral pain:

a) it is a) it is dull, deep, not well defineddull, deep, not well defined, and differently , and differently described by the patientsdescribed by the patients b) b) sometimes sometimes it is it is difficult to locatedifficult to locate this type of pain this type of pain because it because it tends to tends to iirrrradiateadiate c) it is often accompanied by a c) it is often accompanied by a sense of malaisesense of malaise d) it induces d) it induces strong autonomic reflex phenomenastrong autonomic reflex phenomena (much more pronounced than in pain of somatic origin) (much more pronounced than in pain of somatic origin) -- diffuse sweating, vasomotor responses, changes of diffuse sweating, vasomotor responses, changes of arterial pressure and heart rate, and an intense psychic arterial pressure and heart rate, and an intense psychic alarm reaction alarm reaction --"angor animi" - in angina pectoris)"angor animi" - in angina pectoris)
There are many visceral sensation that are unpleasant but below the level of pain, e.g. feeling of disagreeable fullness or acidity of the stomach or undefined and unpleasant thoracic or abdominal sensation.
These visceral sensation may precede the onset of visceral pain
Characteristic feature of true visceral Characteristic feature of true visceral painpain

Refered pain = when an algogenic process affecting a visceral recurs frequently or becomes more intense and prolonged, the location becomes more exact and the painfull sensation is progressively felt in more superficial structures
Refered pain may be accompanied by allodynia and cutaneous and muscular hyperalgesia
Mechanisms involved in refered pain creation: convergence of impulses from viscera and from the skin in the CNS:
Sensory impulses from the viscera create an irritable focus in the segment at which they enter the spinal cord.
Afferent impulses from the skin entering the same segment are thereby facilitated, giving rise to true cutaneous pain.
senzitization of neurons in dorsal horn
Refered visceral pain (transferred pain)Refered visceral pain (transferred pain)

Painful visceral afferent impulses activate anterior horn motor cells to produce rigidity of the muscle (visceromotor reflexes)
A similar activation of anterolateral autonomic cells induces pyloerection, vasoconstriction, and other sympathetic phenomena
These mechanisms, which in modern terms can be defined as positive sympathetic and motor feedback loops, are fundamental in refered pain
It is clear that painful stimulation of visceral structures evokes a visceromuscular reflex, so that some muscles contract and become a new source of pain
ReReffered visceral pain (transferred pain)ered visceral pain (transferred pain)

It has been observed that the local anesthetic block of the
sympathetic ganglia led to the disappearance, or at least to a
marked decrease, of refered pain, allodynia, hyperalgesia.
In some conditions, reffered somatic pain is long-lasting,
increases progressively, and is accompanied by dystrophy
of somatic structures.
Possible mechanisms: onset of self-maintaining vicious circle impulses: peripheral tissue afferent fibers
central nervous system
peripheral tissue somatic and sympathetic efferent fibres
Refered visceral pain (transferred pain)Refered visceral pain (transferred pain)


Intricate conditions - in some types of pain, e.g. chest pain, is difficult to distinguish the true cause of pain because such kind of pain may be related to cervical osteoarthrosis, esophageal hernia, or cholecystitis.
It is difficult to ascertain whether these intricate conditions are due to a simple addition of impulses from different sources in the CNS or to somatovisceral and viscerosomatic reflex mechanisms.

It has been demonstrated that theIt has been demonstrated that the mnemonic processmnemonic process is is facilitated if the experience to be retained isfacilitated if the experience to be retained is repeated many repeated many timestimes or is accompanied by or is accompanied by pleasant or unpleasant emotions. pleasant or unpleasant emotions.
PainPain is, at least in part, ais, at least in part, a learned experiencelearned experience - e.g. during the - e.g. during the
first renal first renal colic, true parietal pain followed visceral paincolic, true parietal pain followed visceral pain after a after a
variablevariable interval. interval. In subsequent episodes of In subsequent episodes of renal colic pain, parietal pain renal colic pain, parietal pain
developed promptly and was not preceded by true visceral developed promptly and was not preceded by true visceral
pain. pain. ThisThis is is probably due to theprobably due to the activation of mnemonic traces.activation of mnemonic traces.

Silent myocardial ischemia (SMI)Chest pain is only a late and inconstant marker of episodes of transient MI in vasospastic angina (30 %), in stable angina (50 %)
Mechanisms of SMI1. a) Lack of the pain is, in part, related to the duration and
severity of MI. 1. Episodes shorter than 3 min, and those accompanied
by a modest impairment of left ventricle ( in end-diastolic pressure inferior to 6 mm Hg) are always painless.
2. Longer and more severe episodes are acccompanied by chest pain in some instances but not in others.
b) Pacients with predominantly SMI appear to have a generalized defective perception of pain (threshold and tolerance).
Mechanism: level of circulating -endorphin (?)

Disturbances in pain perception and nociception
Most of the disturbances are congenital
a) Congenital analgesia - nociceptive stimuli are not processed and/or
integrated at a level of brain. Patient does not feel a pain b) Congenital sensoric neuropathy - nociceptive stimuli are
not transmitted by peripheral
nerves or by spinal afferent tracts.
Acquired disturbances in pain perception and nociception They may occur at syringomyely, disturbances of parietal lobe of brain, in patients suffering from neuropathy (e.g.
chronic diabetes mellitus)







