
AaBa
b
c
d
AA
A
Mdeebrmdpwelp©
K
I
HtsihN
L
0
British Journal of Oral and Maxillofacial Surgery 52 (2014) 128–133
Available online at www.sciencedirect.com
nalysis of time taken to discuss new patients with headnd neck cancer in multidisciplinary team meetings.J. Mullan a,b,∗, J.S. Brown a, D. Lowe a,c, S.N. Rogers a,c, R.J. Shaw a,d
Oral and Maxillofacial Surgery Department, Aintree University Hospital NHS Foundation Trust, Longmoor Lane, Liverpool L9 7AL, United KingdomUniversity of Liverpool, United KingdomEvidence-Based Practice Research Centre (EPRC), Faculty of Health, Edge Hill University, United KingdomHead & Neck Surgery, Department of Molecular & Clinical Cancer Medicine, University of Liverpool, United Kingdom
ccepted 7 October 2013vailable online 23 November 2013
bstract
ultidisciplinary team (MDT) meetings have an important role in the management of head and neck cancer. Increasing incidence of theisease and a drive towards centralised meetings on large numbers of patients mean that effective discussions are pertinent. We aimed tovaluate new cases within a single high volume head and neck cancer MDT and to explore the relation between the time taken to discussach case, the number of discussants, and type of case. A total of 105 patients with a new diagnosis of head and neck malignancy or complexenign tumour were discussed at 10 head and neck cancer MDT meetings. A single observer timed each discussion using a stopwatch, andecorded the number of discussants and the diagnosis and characteristics of each patient. Timings ranged from 15 to 480 s (8 min) with aean of 119 s (2 min), and the duration of discussion correlated closely with the number of discussants (rs = 0.63, p < 0.001). The longest
iscussions concerned patients with advanced T stage (p = 0.006) and advanced N stage (p = 0.009) disease, the elderly (p = 0.02) and maleatients (p = 0.05). Tumour site and histological findings were not significant factors in the duration of discussion. Most discussions on patientsith early stage tumours were short (T1: 58% less than 60 s, mean 90) and fewer people contributed. Many patients, particularly those with
arly stage disease, require little discussion, and their treatment might reasonably be planned according to an agreed protocol, which would
eave more time and resources for those that require greater multidisciplinary input. Further studies may highlight extended discussions onatients with head and neck cancer, which may prompt a review of protocols and current evidence.2013 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.
eywords: Multidisciplinary team; MDT; Head and neck cancer; Discussion length
irayt
ntroduction
ead and neck cancer covers a wide spectrum of histologicalypes in a complex anatomical site, and patients often haveerious coexisting conditions. Data suggest that the overall
ncidence of the disease in the UK is rising. The nationalead and neck cancer audit by DAHNOs (Data for Head andeck Oncologists) estimated that between 2010 and 2011 the∗ Corresponding author at: 17 Norbury Avenue, Mossley Hill, Liverpool18 1JQ, United Kingdom.
E-mail address: [email protected] (B.J. Mullan).
st
fowe(
266-4356/$ – see front matter © 2013 The British Association of Oral and Maxillofaciahttp://dx.doi.org/10.1016/j.bjoms.2013.10.001
ncidence had risen by over 600 cases (from 6747 to 7354,espectively) in England and Wales and included neoplasmsrising from the oral cavity, larynx, oropharynx, hypophar-nx, nasopharynx, and major salivary glands.1,2 Allied withhis there is a continued trend to manage cancer cases in amaller number of high volume centres,1,2 which highlightshe need for efficient and meaningful discussions.
Diagnosis and treatment of these patients require inputrom multiple medical professionals and a further spectrumf allied health professionals. Management involves dealing
ith the effects of the disease itself as well as the disablingffects of treatment, and to do this a multidisciplinary teamMDT) approach has become widely adopted.3 It has been
l Surgeons. Published by Elsevier Ltd. All rights reserved.

l and M
rsiistcataccr
msMwIabIlaass
srhc(wowwabfto
M
WhHimpccoe
iwtdbod
cidcto
aocdowwp
wai
R
Tapmc(
9cpT(wwanbcn4
B.J. Mullan et al. / British Journal of Ora
ecommended that all patients with head and neck cancer areeen by a MDT irrespective of type or stage,1–3 and theres evidence that this increases the accuracy of cancer stag-ng and improves outcomes.4,5 Friedland et al.6 comparedurvival of patients who had been treated by an MDT withhose who had not, and showed that survival was signifi-antly better in those treated by an MDT when stage, aget diagnosis, and year of diagnosis were controlled for inhe analysis. The perceived benefits of treatment by an MDTre improved communication between health professionals,oordinated and continuous patient care, better clinical out-omes, and better opportunities for education, audit, andesearch.7
Following the Improving Outcomes Guidance recom-endations of 2004 there has been a move towards larger
pecialist centres. However, big is not always best, and anDT in a large centre might not cope with the increasedorkload.8 There is also concern about the lack of level
evidence to support the benefits of an MDT approach,6
nd it is difficult to make valid comparisons of outcomesetween centres.3 Nevertheless, in the absence of level I orI data, these studies form the basis of the clinical guide-ines which inform current best practice.6 Some cliniciansrgue that delays and expense may justify the referral of onlydvanced cases of malignancy to the MDT, and that earlytage disease that is treated outside an MDT would achieveimilar outcomes.9
This study is based on a large MDT in a regional unit thaterves a population of over 2.8 million, and around 900 neweferrals are discussed each year. The region has a particularlyigh incidence of squamous cell carcinoma with 450 newases/year, which reflects an incidence of 16/100,000/yearcompared with the UK mean of 12/100,000/year).10 Theeekly MDT lasts an hour, during which new complex benignr malignant neoplasms followed by PET scans, and patientsith recurrence and ongoing tumours are discussed. It endsith the histopathological staging of primary tumours that
re going to be resected. Patients with cancers of the skullase and thyroid are discussed separately; each is scheduledor 30 min once a fortnight. Our aim was to explore the factorshat influence the duration of the discussion and the numberf discussants for new cases.
ethod
e prospectively studied discussions on new cases at 10ead and neck MDT meetings held at Aintree Universityospital over 2 periods in 2011. Five were consecutive meet-
ngs between January and February, and 5 were consecutiveeetings between August and September. Discussions on all
atients with a new diagnosis of head and neck cancer or
omplex benign tumour in these periods were included. Dis-ussions on PET scans and patients with disease of the thyroidr base of the skull, recurrence, or ongoing tumours, werexcluded.g
ab
axillofacial Surgery 52 (2014) 128–133 129
A single observer used a stopwatch to time the discussionsn seconds from when a case was announced until the nextas announced. The duration of any discussion not relevant
o the case was noted and the time deducted. If a case wasiscussed on more than one occasion during the same meetingecause a member of the team had not been present initiallyr a subsequent case had similarities, the total sum of theiscussions was recorded.
The number of people who contributed verbally to eachase was recorded (including the chair). During the meet-ng the coordinator filled out the Somerset Cancer Registeratabase, a UK web-based clinical data collection register forancer with a designated head and neck section. From this,he patient’s characteristics, type of disease, and the outcomef the meeting were extracted for the purposes of the study.
Spearman’s correlation was used to quantify the associ-tion between numerical or ordinal characteristics (durationf discussion, age, and number discussing the case). Asso-iations between the patient’s characteristics and duration ofiscussion in seconds were tested using the Mann–Whitneyr Kruskal–Wallis test as appropriate, as were associationsith the number discussing the case. Duration of discussionas also grouped (up to 60 s, 61–120, and more than 120 s) torovide a better descriptive presentation of results in Table 1.
The single observer recorded the total number of peopleho attended the meeting including those who arrived late
nd those who departed before the end. The position of thosen the discussion and their roles were not recorded.
esults
he mean (SD) age of the 105 patients was 62 (16) years,nd 75 (71%) were male. A total of 15 (14%) had com-lex benign or non-malignant disease, and 90 (86%) had newalignancies. Tumour sites were larynx (n = 32, 30%), oral
avity (n = 21, 20%), oropharynx (n = 26, 25%), and othern = 23, 22%). In 3 cases it was not known.
The median (IQR) time taken to discuss the cases was0 (60–180) s (range 15–480), with a total time over all theases of 208 min (mean 119 s). The median (IQR) number ofeople involved in the discussion was 4 (3–5) (range 1–10).he discussions were longer the more people that joined in
rs = 0.63, p < 0.001, Fig. 1). The median duration was 30 shen fewer than 3 people took part (n = 8), 90 s when thereere 3 (n = 39) or 4 (n = 22), 165 s when there were 5 (n = 20),
nd 180 s when there were more than 5 (n = 16). There waso significant difference in the times taken to discuss casesetween the 2 periods (p = 0.48) or in the number of dis-ussants (p = 0.08). In the first group of meetings the meanumber of discussants was 3.8; in the second group it was.3. The mean duration of discussion was 125 s in the first
roup of meetings and 113 s in the second.There was no significant correlation between age in yearsnd duration of discussion (rs = −0.07, p = 0.50). Relationsetween other factors and duration of discussion are shown

130 B.J. Mullan et al. / British Journal of Oral and Maxillofacial Surgery 52 (2014) 128–133
Table 1Clinical factors in relation to the time (s) taken by the multidisciplinary team (MDT) to discuss new cases.
No. of patients Up to 60 s 61–120 s More than 120 s Mean no. of seconds p-Value
Total 105 29 (28) 43 (41) 33 (31) 119Sex
Male 75 18 (24) 30 (40) 27 (36) 129 0.05Female 30 11 (37) 13 (43) 6 (20) 96
Age group (years)<55 25 7 (28) 10 (40) 8 (32) 116 0.0255–64 33 7 (21) 13 (39) 13 (39) 12765–74 27 13 (48) 9 (33) 5 (19) 8875+ 20 2 (10) 11 (55) 7 (35) 151
SpecialtyEar, nose and throat 61 15 (25) 25 (41) 21 (34) 125 0.24Maxillofacial unit 44 14 (32) 18 (41) 12 (27) 110
MDT meetingsFirst 5 50 14 (28) 18 (36) 18 (36) 125 0.48Second 5 55 15 (27) 25 (45) 15 (27) 113
TypeComplex benign 15 4 (27) 9 (60) 2 (13) 98 0.54Cancer 90 25 (28) 34 (38) 31 (34) 122
Site (3 not known)Larynx 32 7 (22) 14 (44) 11 (34) 121 0.56Oral 21 9 (43) 4 (19) 8 (38) 100Oropharynx 26 6 (23) 14 (54) 6 (23) 121
Other 23 6 (26) 9 (39) 8 (34) 136T stage
1 19 11 (58) 6 (32) 2 (11) 90 0.0062 24 5 (21) 8 (33) 11 (46) 133
3–4 27 4 (15) 11 (41) 12 (44) 138Not done or not known 35 9 (26) 18 (51) 8 (23) 110
N stage0 11 5 (45) 2 (18) 4 (36) 123 0.0091 12 1 (8) 6 (50) 5 (42) 1352–3 17 1 (6) 7 (41) 9 (53) 163Not done or not known 65 22 (34) 28 (43) 15 (23) 104
TreatmentOperation 50 19 (38) 19 (38) 12 (24) 102 0.09Radiotherapy 14 2 (14) 9 (64) 3 (21) 115Further investigation 11 2 (18) 2 (18) 7 (64) 175Others 30 6 (20) 13 (43) 11 (37) 128
Chemoradiotherapy 6 – – – –Specialist palliative care 6 – – – –Watch and wait 6 – – – –No treatment 4 – – – –Operation and PORT 3 – – – –Chemotherapy 2 – – – –Offered operation or radiotherapy 1 – – – –
D
igpsunfTs
at
sa
42
D
Other 2 –
ata are number (%). PORT: postoperative radiotherapy.
n Table 1. There was a significant difference between ageroups with the least time being given to discussions ofatients aged 65–74 years. Discussions on patients with Ttage 1 tumours and those whose N stage was not done ornknown were the shortest. Other borderline trends for sig-ificance suggest that discussions on patients that requiredurther investigation and on male patients were longer.here were no significant differences in regard to tumourite.
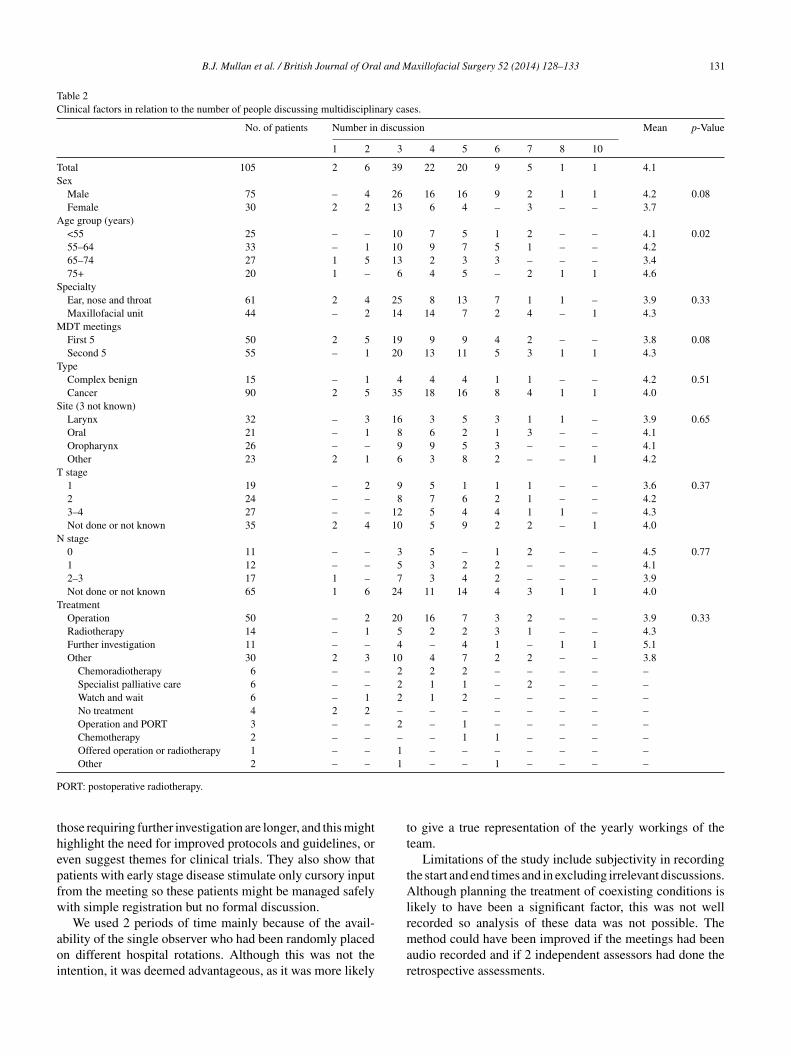
There was no significant correlation between age in yearsnd the number of discussants (rs = −0.04, p = 0.68). Rela-ions between other factors and the number of discussants are
TaMt
– – –
hown in Table 2. Similar trends were noted with regard toge group and sex, but less so for tumour staging.
The total number of staff on the MDT attendance list was0, and a mean of 26 people attended the meetings (range0–31).
iscussion
o our knowledge, this is the first report to look specificallyt the time taken to discuss each new case at a head and neckDT. Our results show that discussions on male patients,
he elderly, those with advanced locoregional disease and
B.J. Mullan et al. / British Journal of Oral and Maxillofacial Surgery 52 (2014) 128–133 131
Table 2Clinical factors in relation to the number of people discussing multidisciplinary cases.
No. of patients Number in discussion Mean p-Value
1 2 3 4 5 6 7 8 10
Total 105 2 6 39 22 20 9 5 1 1 4.1Sex
Male 75 – 4 26 16 16 9 2 1 1 4.2 0.08Female 30 2 2 13 6 4 – 3 – – 3.7
Age group (years)<55 25 – – 10 7 5 1 2 – – 4.1 0.0255–64 33 – 1 10 9 7 5 1 – – 4.265–74 27 1 5 13 2 3 3 – – – 3.475+ 20 1 – 6 4 5 – 2 1 1 4.6
SpecialtyEar, nose and throat 61 2 4 25 8 13 7 1 1 – 3.9 0.33Maxillofacial unit 44 – 2 14 14 7 2 4 – 1 4.3
MDT meetingsFirst 5 50 2 5 19 9 9 4 2 – – 3.8 0.08Second 5 55 – 1 20 13 11 5 3 1 1 4.3
TypeComplex benign 15 – 1 4 4 4 1 1 – – 4.2 0.51Cancer 90 2 5 35 18 16 8 4 1 1 4.0
Site (3 not known)Larynx 32 – 3 16 3 5 3 1 1 – 3.9 0.65Oral 21 – 1 8 6 2 1 3 – – 4.1Oropharynx 26 – – 9 9 5 3 – – – 4.1Other 23 2 1 6 3 8 2 – – 1 4.2
T stage1 19 – 2 9 5 1 1 1 – – 3.6 0.372 24 – – 8 7 6 2 1 – – 4.23–4 27 – – 12 5 4 4 1 1 – 4.3Not done or not known 35 2 4 10 5 9 2 2 – 1 4.0
N stage0 11 – – 3 5 – 1 2 – – 4.5 0.771 12 – – 5 3 2 2 – – – 4.12–3 17 1 – 7 3 4 2 – – – 3.9Not done or not known 65 1 6 24 11 14 4 3 1 1 4.0
TreatmentOperation 50 – 2 20 16 7 3 2 – – 3.9 0.33Radiotherapy 14 – 1 5 2 2 3 1 – – 4.3Further investigation 11 – – 4 – 4 1 – 1 1 5.1Other 30 2 3 10 4 7 2 2 – – 3.8
Chemoradiotherapy 6 – – 2 2 2 – – – – –Specialist palliative care 6 – – 2 1 1 – 2 – – –Watch and wait 6 – 1 2 1 2 – – – – –No treatment 4 2 2 – – – – – – – –Operation and PORT 3 – – 2 – 1 – – – – –Chemotherapy 2 – – – – 1 1 – – – –Offered operation or radiotherapy 1 – – 1 – – – – – – –Other 2 – – 1 – – 1 – – – –
P
thepfw
aoi
tt
tAlr
ORT: postoperative radiotherapy.
hose requiring further investigation are longer, and this mightighlight the need for improved protocols and guidelines, orven suggest themes for clinical trials. They also show thatatients with early stage disease stimulate only cursory inputrom the meeting so these patients might be managed safelyith simple registration but no formal discussion.We used 2 periods of time mainly because of the avail-
bility of the single observer who had been randomly placedn different hospital rotations. Although this was not thentention, it was deemed advantageous, as it was more likely
mar
o give a true representation of the yearly workings of theeam.
Limitations of the study include subjectivity in recordinghe start and end times and in excluding irrelevant discussions.lthough planning the treatment of coexisting conditions is
ikely to have been a significant factor, this was not wellecorded so analysis of these data was not possible. The
ethod could have been improved if the meetings had beenudio recorded and if 2 independent assessors had done theetrospective assessments.

132 B.J. Mullan et al. / British Journal of Oral and M
Fig. 1. Association between the number of people in the multidisciplinarytS
iwotwro(
4Ttismlsir
licoifabmocFpeco
pdtc
obmcsMm
ateata(bfaoontM
C
T
E
N
R
eam (MDT) discussion and duration of discussion for 105 new cases.pearman correlation rs = 0.63, p < 0.001.
In the opinion of the observer the discussions oftennvolved the same small group of MDT members. In future itould be beneficial to record the specialty, grade, and namef the person who put the case forward to find out whetherhe same people participate in most of the discussions, andhether more discussion occurs when they are absent. In ret-
ospect it would also have been of interest to record discussionf recruitment to the National Institute for Health ResearchNIHR) portfolio trials.
All cases discussed in under 60 s involved no more than people, and in 47 of the 105 cases it was no more than 3.he chair, the presenting clinician (usually a surgeon), and
he radiologist spoke in all cases. As most radiological find-ngs should have been reported formally (including full TNMtaging) before the meeting, discussion about the patients’anagement could be questioned. However, our study had
imitations because in a large number of cases the full TNMtaging was not recorded. The number of people who partic-pated in the discussion was recorded but not their specificole.
The aim of an MDT is to ensure that a uniform and highevel of specialist care with appropriate multidisciplinarynput is available to all patients. With the introduction of can-er networks in the UK following the Calman Hine report,3
pportunities for audit and clinical trials have also beenmproved. The complexity of cancer treatment and the needor a multidisciplinary approach require that clinicians have
certain minimum caseload and competence to ensure theest standards of care.11 However, these data show that in aeeting about a large number of patients, many are discussed
nly briefly, and with an increasing incidence of disease andonstrained finances, some rationalisation may be needed.riedland et al.6 showed improved survival and increasedrescription of multimodal treatment for higher stage dis-
ase in patients discussed by a MDT. It might seem logical tooncentrate resources on patients with complex needs, seri-us coexisting conditions, or locally advanced disease, whichaxillofacial Surgery 52 (2014) 128–133
redicate multimodal treatment. For those with early stageisease who are relatively fit and need a single method ofreatment, discussions may be less likely to improve theirare.
Our results show that in the cases of 2 female patients,nly one person spoke, and no treatment was recommendedy the team. Both had presented with neck lumps but pri-ary tumours had been identified elsewhere. Although they
ould be seen as outliers they highlight cases that fit thistudy’s initial criterion and criteria of the head and neck
DT, but realistically may not need to be presented at aeeting.We acknowledge that the MDT has a role in the man-
gement of head and neck cancer and we support the viewhat a centralised meeting of the team allows discussion andnsures that decision-making is fully rationalised. We alsocknowledge that teams in other centres in the UK and acrosshe world differ in their organisation and in the resourcesvailable, the number of meetings, and in those who attendsome also include the patients and their family).2,3,8 It maye beneficial to look into these aspects and also to continueurther research into the meetings to identify subgroups suchs those with early disease, that could be managed with-ut discussion. There is also a need to explore the rolef the MDT in NIHR portfolio recruitment for head andeck trials and cohort studies, and for further research intohe role of allied health professionals in the head and neck
DT.
onflict of interest
here are no conflicts of interest.
thics statement/confirmation of patient permission
o ethical approval needed.
eferences
1. National Head and Neck Cancer Audit. Key findings for Englandand Wales for the audit period October 2009 to November 2010.DAHNO sixth annual report. NHS Information Centre. Available fromhttp://www.ic.nhs.uk/canceraudits
2. National Head and Neck Cancer Audit. Key findings for Englandand Wales for the audit period October 2010 to November 2011.DAHNO seventh annual report. NHS Information Centre. Available fromhttp://www.ic.nhs.uk/canceraudits
3. Calman K, Hine D, Expert Advisory Group on Cancer. A policyframework for commissioning cancer services: a report to the chiefmedical officers of England and Wales. London: Department of Health;1995. Available from http://www.dhcarenetworks.org.uk/ library/Resources/ICN/Policy documents/Calman Hine.pdf
4. Birchall M, Bailey D, King P, South West Cancer Intelligence ServiceHead and Neck Tumour Panel. Effect of process standards on survival ofpatients with head and neck cancer in the south and west of England. BrJ Cancer 2004;91:1477–81.

l and M
1
2007;19:216–21.11. Olofsson J. Multidisciplinary team a prerequisite in the manage-
B.J. Mullan et al. / British Journal of Ora
5. Stephens MR, Lewis WG, Brewster AE, et al. Multidisciplinary teammanagement is associated with improved outcomes after surgery foresophageal cancer. Dis Esophagus 2006;19:164–71.
6. Friedland PL, Bozic B, Dewar J, et al. Impact of multidisciplinaryteam management in head and neck cancer patients. Br J Cancer2011;104:1246–8.
7. Westin T, Stalfors J. Tumour boards/multidisciplinary head and neckcancer meetings: are they of value to patients, treating staff or a politicaladditional drain on healthcare resources? Curr Opin Otolaryngol Head
Neck Surg 2008;16:103–7.8. Bradley PJ, Zutshi B, Nutting CM. An audit of clinical resources availablefor the care of head and neck cancer patients in England. Clin Oncol (RColl Radiol) 2005;17:604–9.
axillofacial Surgery 52 (2014) 128–133 133
9. Taylor C, Ramirez AJ, Cancer Research UK Promoting Early Pre-sentation Group. Multidisciplinary team members’ views about MDTworking: results from a survey commissioned by the National CancerAction Team. London: National Health Service; 2009. Available fromhttp://www.ncin.org.uk/view?rid=137
0. Murdoch D. Standard, and novel cytotoxic and molecular-targeted,therapies for HNSCC: an evidence-based review. Curr Opin Oncol
ment of head and neck cancer? Eur Arch Otorhinolaryngol 2009;266:159–60.







