JOURNALOF
PSYCHIATRIC
Journal of Psychiatric Research 39 (2005) 85–92RESEARCH
www.elsevier.com/locate/jpsychires
Affective dysregulation and dissociative experience in femalepatients with borderline personality disorder: a startle response study
Ulrich W. Ebner-Priemera, Sandra Badeckb, Cornelia Beckmannb, Amy Wagnerc,Bernd Feigeb, Isabelle Weissd, Klaus Liebb, Martin Bohusa,*
a Department of Psychosomatic Medicine and Psychotherapy, Central Institute of Mental Health, Postfach 12 21 20, 68072 Mannheim, Germanyb Department of Psychiatry and Psychotherapy, University of Freiburg Medical School, Freiburg, Germany
c Department of Psychiatry and Behavioral Sciences, University of Washington, Seattle, WA, USAd Institute of Cell Biology, Swiss Federal Institute of Technology, Zurich, Switzerland
Received 10 November 2003; received in revised form 30 March 2004; accepted 13 May 2004
Abstract
Affective dysregulation and dissociation are currently discussed as core features of borderline personality disorder (BPD). Af-
fective dysregulation is hypothesized to be correlated with increased amygdala functioning and dissociation is linked to inhibited
processing on the amygdala and dampened autonomic output, according to the corticolimbic disconnection model of dissociation
from Sierra and Berrios [Biological Psychiatry 44 (1998) 898]. We assessed startle response, which is mainly mediated by the
amygdala, to investigate the relationship between affective dysregulation and dissociation. We hypothesized that patients with BPD
would reveal enhanced responses to startling tones, but that these would be lessened by the presence of state dissociative experiences.
21 unmedicated female patients with BPD and 21 healthy female controls listened to 15 startling tones (95-dB, 500-ms, 1000-Hz)
while heart rate, skin conductance and orbicularis oculi electromyogram responses were measured. Covariance analysis showed that
the BPD group had a significantly higher startle response in the electromyogram as compared to controls. Furthermore, present-
state dissociative experiences significantly influenced the startle response. Patients with low dissociative experiences revealed en-
hanced startle responses whereas patients with high dissociative experiences showed reduced responses. Our data support affective
dysregulation in BPD as well as the corticolimbic disconnection model of dissociation, at least for EMG. Furthermore, it highlights
the importance of assessing present-state dissociation in basic research as well as psychotherapy.
� 2004 Elsevier Ltd. All rights reserved.
Keywords: Borderline personality disorder; Startle response; Affective dysregulation; Dissociation; Electromyography; Psychophysiology
1. Introduction
This study focuses on the interrelation of two DSM-
IV criteria in borderline personality disorder (BPD):
affective dysregulation or instability and dissociative
symptoms. Affective dysregulation is currently depictedin the scientific literature as the core feature of BPD
(Linehan, 1993; Sanislow et al., 2002; Skodol et al.,
2002a,b; Siever et al., 2002). Support for this view has
been found by several studies (Levine et al., 1997;
Dougherty et al., 1999; Stein, 1996). Although the neu-
* Corresponding author. Tel.: +49-621-1703426; fax: +49-621-
1703172.
E-mail address: [email protected] (M. Bohus).
0022-3956/$ - see front matter � 2004 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jpsychires.2004.05.001
robiological basis of affective dysregulation is unknown
some research suggests that affective dysregulation
might be caused by higher activity of the amygdala
(Corrigan et al., 2000). For example Herpertz et al.
(2001a) found significantly higher activity of the amyg-
dala to unpleasant visual stimuli within BPD patientscompared to healthy controls, as assessed by fMRI.
Although the self-report of valence and arousal did not
differ between groups, the authors suggested that en-
hanced amygdala activation in BPD might reflect in-
tense and slowly subsiding emotions. In addition
alterations of the amygdala in BPD were found, using
MRI-based volumetric measurements (Driessen et al.,
2000; Tebartz van Elst et al., 2001). However, there havealso been laboratory studies using potentiated startle
86 U.W. Ebner-Priemer et al. / Journal of Psychiatric Research 39 (2005) 85–92
that provided no evidence for emotional hyperreactivity
or hypersensitivity in individuals diagnosed with BPD
(Herpertz et al., 1999, 2001b) neither on a psychological
nor on a physiological level.
Despite the central role of emotional reactivity inBPD, the restriction or absence of emotional experi-
encing, in the form of dissociative behavior, is also
common in BPD (Zanarini et al., 2000) and is one of the
defining DSM-IV criteria. Sierra and Berrios (1998)
published a neurobiological model for depersonalization
disorder, proposing bilateral corticolimbic disconnec-
tion during dissociation. In their model the medial pre-
frontal cortex inhibits processing on the amygdala,causing a reduced emotional experience and a damp-
ening of autonomic output. Recent studies confirm au-
tonomic blunting in dissociation. Sierra et al. (2002)
showed that subjects with depersonalization disorder
exhibited reduced magnitude and increased latency of
skin conductance response to unpleasant stimuli, but
not to non-specific stimuli suggesting a selective inhibi-
tion of emotional processing. Lanius and colleagues(2002) using a traumatic script-driven symptom provo-
cation paradigm posttraumatic stress disorder (PTSD)
could also partially support the model of Sierra and
Berrios. The dissociated PTSD subgroup (present state)
revealed reduced heart rate, increased activation in the
dorsolaterala and medial frontal cortex and did not
exhibit increased amygdala activation. Studies on peri-
traumatic dissociation and physiological response re-vealed controversial results. Griffin et al. (1997) reported
decreased heart rate and galvanic skin response in fe-
male rape victims with high dissociation compared to a
group with low dissociation during baseline and while
reporting about the trauma. In contrast, Kaufmann
et al. (2002) could not show any physiological differ-
ences to trauma-relevant stimuli between PTSD patients
with low and high peritraumatic dissociation. Ladwiget al. (2002) investigated startle response and peritrau-
matic dissociation in survivors of life-threatening car-
diac events. Using several subgroup analyses, the biggest
influence on startle response was the diagnosis of PTSD.
However, we think that the disconnection model of
dissociation from Sierra and Berrios (1998) refers rather
to present state than to peritraumatic dissociation.
Consistent with the disconnection model, clinicianshave observed that dissociation is characterized by de-
creased emotional experiencing (Maldonado and Spie-
gel, 1998). Similarly, behavioral therapists (Foa and
Kozak, 1986; Wagner and Linehan, 1999) view dissoci-
ation as functioning to regulate emotional engagement
in e.g. exposure therapy.
To explore these questions related to the neurobio-
logical underpinnings of affective dysregulation anddissociation in BPD, we employed the acoustic startle
response paradigm (ASR). The neural pathway of the
EMG in the ASR involves three neuronal ‘‘relay sta-
tions’’: The cochlear root neuron, the caudal pontine
reticular nucleus (PnC), and motoneurons in the facial
motor nucleus (Davis et al., 1999). The PnC is mainly
controlled by the medial part of the central nucleus of
the amygdala (Rosen et al., 1991). Enhanced amygdalaactivation (e.g. via electrical stimulation) therefore leads
to enhanced startle response in EMG (Davis et al., 1999;
Rosen and Davis, 1988). Along these lines, studies have
shown that trauma survivors with chronic PTSD dem-
onstrate both exaggerated amygdala response (Rauch
et al., 2000) and elevated responses to startling tones
(Metzger et al., 1999; Shalev et al., 1997, 2000).
Because of the afore mentioned linkage betweenBPD, emotional dysregulation, enhanced amygdala ac-
tivation (Herpertz et al., 2001a) and enhanced startle
response in EMG (Davis et al., 1999; Rosen and Davis,
1988), the ASR is an appropriate paradigm for investi-
gating affective dysregulation in this population. The
first specific hypothesis is: (1) Patients with BPD will
show enhanced responses to startling tones. According
to the corticolimbic disconnection model of dissociationfrom Sierra and Berrios (1998) we examined whether
dissociation is linked with reduced physiological re-
sponsiveness. The second specific hypothesis is: (2)
Present-state dissociative experiences will reduce the
startle response in BPD. To ensure that reduced startle
response is related to present-state dissociative experi-
ences and not to other psychological variables, we in-
vestigated anxiety, depression, trait dissociation andcomorbid PTSD as a confounding variables.
2. Materials and methods
2.1. Subjects
Twenty one female patients with BPD (10 inpatients,11 outpatients) and a comparison group of 21 female
healthy controls (HC) participated in this study. The
BPD sample was recruited from consecutively admitted
patients to a DBT-treatment program (Bohus et al.,
2000). Patients were randomly assigned to inpatient or
outpatient treatment. All patients fulfilled DSM-IV
criteria for BPD, assessed by the appropriate segment of
the Structured Clinical Interview for DSM-IV Person-ality Disorders (SCID-II; First et al., 1996) and scored a
minimum of 8 points on the Revised Diagnostic Inter-
view for Borderlines (DIB-R; Zanarini et al., 1989). Axis
I comorbidity was assessed by the Structured Clinical
Interview for DSM-IV Axis I Disorders (SCID-I; First
et al., 1997). Patients with a lifetime history of schizo-
phrenia, bipolar I disorder or alcohol and drug addic-
tion were excluded. Trained psychologists administeredall diagnostic instruments. Eighteen patients from the
BPD group had current comorbid Axis I disorders, in-
cluding major depressive disorder ðn ¼ 6Þ, anxiety dis-
U.W. Ebner-Priemer et al. / Journal of Psychiatric Research 39 (2005) 85–92 87
orders without PTSD ðn ¼ 11Þ, PTSD ðn ¼ 9Þ, obses-sive-compulsive disorder ðn ¼ 2Þ, and eating disorders
ðn ¼ 8Þ. The healthy controls were randomly selected
individuals from the national resident register of the
City of Freiburg, Germany, contacted by telephone.Exclusion criteria for the control group included the
diagnosis of BPD (SCID-II for DSM-IV), any Axis-I
disorder (MINI-SCID; Sheehan et al., 1998), current
psychotherapy or self-report of any first-degree relative
with a mental disorder. Individuals for both groups were
required to be free of medication for a minimum of 4
weeks prior to the study, except for contraceptive.
Groups were matched for sex (all females) and age(Table 1). All subjects were paid for participating in
the study. After complete description of the study to the
subjects, written informed consent was obtained. The
study was approved by the ethical board of the Uni-
versity of Freiburg, Medical School, Germany, in ac-
cordance to the declaration of Helsinki.
2.2. Psychometric measures
To assess present-state dissociative experiences the
‘‘Dissociation-Tension-Scale’’ (DSS; Stiglmayr et al.,
2001) was used. This self-rating scale consists of 19 items
concerning somatic (e.g. perception of pain, vision and
hearing) as well as psychological dissociation (e.g. de-
realization, depersonalization, amnesia). All items were
derived from the DES (Bernstein and Putnam, 1986)and the Somatoform Dissociation Questionnaire (SDQ-
20; Nijenhuis et al., 1996). Reliability analysis (internal
consistency) of the DSS resulted in a Cronbach’s a of 0.9(Stiglmayr et al., 2001). The cut-off value for having
severe dissociative features is 2.7 in a possible range
from 0.0 to 9.0 (Stiglmayr et al., 2001). Some authors
emphasize the distinction between different aspects of
dissociation, e.g. somatoform and psychological di-mensions (Nijenhuis et al., 1996). However, Stiglmayr
and colleagues (2001) did not find any support for this
Table 1
Results of demographic, self-report and physiological resting period data of
BPD mean (SD) H
Age 28.5 (8.1) 2
Dissociation: present-state (DSS) 1.38 (1.25) 0
Dissociation: trait (DES) 22.8 (7.75) 3
Depression (BDI) 25.0 (12.2) 1
Anxiety (STAI – state) 51.7 (10.1) 3
Audiometric examination (dB) 10.9 (4.3) 1
EMG: resting perioda 1.09 (0.42) 1
SCL: resting perioda 6.51 (4.0) 6
HR: resting perioda 69.7 (9.0) 7
EMG, electromyogram; SCL, skin conductance level; HR, heart rate.aResting period¼mean of pre-experiment and post-experiment resting pe
distinction in patients with BPD. For that reason sub-
scales of dissociation were not used in this study.
Trait dissociation was assessed by the ‘‘Dissociative
Experience Scale’’ (DES; Bernstein and Putnam, 1986),
anxiety by the ‘‘State Trait Anxiety Inventory’’ (STAI;Spielberger et al., 1970), and depressive symptoms by
the ‘‘Beck Depression Inventory’’ (BDI; Beck et al.,
1961). Hearing thresholds of all participants were spec-
ified with the auditory module of the NEUROSCAN-
System.
2.3. Physiologic measures
2.3.1. Data acquisition
Dependent physiologic measures included left orbic-
ularis oculi electromyogram (EMG), skin conductance
(SC) and heart rate (HR). EMG was recorded from 4-
mm (sensor diameter) Beckmann-type Ag/AgCl surface
electrodes filled with electrolyte paste (Genuine Grass
EC2, Grass Instrument Division, Warwick, RI) and
placed according to published specifications over the leftorbicularis oculi muscle (Fridlund and Cacioppo, 1986).
All electrode impedances were kept below 5 kX. Skinconductance was recorded from 7-mm (sensor diameter)
Ag/AgCl-electrodes (Marquette Hellige GmbH, Frei-
burg, Germany) filled with an isotonic EDR jelly
TDE-246 (Steffens, Berlin, Germany; identical to Grass
EC-33) and placed on the thenar and hypothenar emi-
nences of the non-dominant hand. Conductance wasconverted into a voltage signal (10 lS/V reduced to 500
lS/V by voltage divider) using an SC-amplifier MBV
400.2 (Rimkus Medizintechnik, Riemerling, Germany)
with a time constant of 10 s and a 25 Hz low-pass. ECG
was recorded from standard limb electrocardiogram
leads (blue sensor; Medicotest; Germany). All physio-
logical measures were amplified (EMG 10–100 Hz; SC
DC-100 Hz; ECG 1–100 Hz) and recorded using a 32-channel digital EEG system (Synamps; Neuroscan, El
Paso, TX) at a rate of 500 Hz.
female patients with BPD and HC
C mean (SD) Statistics t (df) p
9.7 (8.9) )0.471(40) 0.641
.07 (0.14) 4.76 (20.5) 6 0.001
.3 (2.74) 10.89 (24.9) 6 0.001
.4 (2.7) 8.65 (22.0) 6 0.001
2.8 (6.5) 7.14 (34.5) 6 0.001
0.9 (2.3) 0.021 (40) 0.984
.67 (1.05) )2.174 (22.4) 0.041
.79 (3.1) )0.25 (37) 0.806
0.0 (9.0) )0.09 (40) 0.932
riod.

88 U.W. Ebner-Priemer et al. / Journal of Psychiatric Research 39 (2005) 85–92
2.3.2. Off-line processing
EMG raw scores were high-pass filtered at 57.5 Hz
(extracting the important high-frequency part of the
EMG), rectified and low-pass filtered at 12.5 Hz. The
corresponding short time constant was chosen to letthe rectified signal follow EMG bursts closely, thereby
allowing a precise detection of the onset latency for
failure scores. For precise information about the influ-
ence of sampling rate and time constant on EMG scores,
see Metzger et al. (1999) or Berg and Balaban (1999).
The ECG signal was transformed into a heart rate using
the software program Bio 25 (Foerster, 1998).
2.4. Stimuli
Stimuli consisted of fifteen 95-dB (SPL), 1000 Hz,
500-ms pure tones with 60.1 ms rise and fall time,
generated by a ‘‘LabMaster’’ digital–analog converter,
controlled by the software-program Stim (NEURO-
SCAN). These stimulus parameters are similar to those
used in most of the recent startle-response studies inPTSD (Shalev et al., 1997, 2000; Metzger et al., 1999)
and were chosen for this study to enable comparability.
Startle probes were delivered within a pseudorandom,
inter-trial interval of 33–52 s and binaurally over
headphones (EAR LINK 3a). Sound was controlled
with a precision sound level meter (Br€uell and Kjaer,
Typ 2206; Darmstadt, Germany).
2.5. Procedure
The experiment took place in a sound-attenuated,
temperature-controlled room connected through wires
to the laboratory in which the experimental apparatus
was located. Participants were seated upright in a
comfortable armchair. After the participant was famil-
iarized with the laboratory conditions, the electrodeswere attached. Then psychological assessments for dis-
sociation and anxiety were administered. In a 2 min
resting-period before and after the experiment, physio-
logical parameters were recorded. The participant was
instructed as follows: ‘‘You are going to hear a series of
sounds. Please sit quietly and listen to the sounds as they
come. Keep your eyes open throughout the entire pro-
cedure, which will not last more than 15 min’’ (Englishtranslation of the German instruction).
2.6. Data analysis
Main parameters for analysis were ‘‘response’’ and
‘‘habituation’’ to the 15 startling tones.
2.6.1. Response
Response in EMG, SC and HR for each trial was
calculated by subtracting average baseline levels imme-
diately preceding the onset of the tone (EMG, SC, HR:
0–2 s before tone onset) from the maximum response in
the respective time windows after startle onset (EMG:
21–150 ms; SC: 1–4 s, HR: 1–4 s). EMG trials with re-
sponse onset 6 20 ms or P 120 ms were rejected. Re-
sponse onset was defined as time until the EMG increasereaches the response-criterion. The number of rejected
responses was below 1%. Control of SC artifacts fol-
lowed published specifications (Boucsein, 1992).
2.6.2. Habituation
Habituation was assessed by two methods: ‘‘slope’’
and ‘‘trial to non-response’’ (trial to criterion¼TTC).
Relative habituation was defined as the slope of the re-gression equation y ¼ bxþ a for trials 2–15, where y is
the square root of the response score and x is the log
trial number. The first trial was dropped as usual
(Lykken et al., 1988). The non-response criterion is de-
fined as an EMG and SC response of <0.35 lV and
<0.01 lS, respectively. TTC, as a parameter of absolute
habituation, is defined as the number of trials until the
subject reaches two consecutive non-response trials. Toreduce the variance associated with unusually large re-
sponses, square root transformations were performed on
the response scores of EMG, SC, and HR prior to the
statistical analysis. The software Bio 25 (Foerster, 1998)
was administered to control artifacts and calculate
physiological raw data.
To examine the group differences in physiological
resting period, demographics, and self-report question-naires, t test for independent samples were used. For the
analysis of group differences in the physiological re-
sponse parameters controlling for present-state disso-
ciative experiences, covariance analysis (ANCOVA) was
performed. A covariance analysis was chosen instead of
a 2-factorial analysis (with dissociation as a second
factor) because there was insufficient variation in DSS
scores in the HC group for this type of analysis. Fur-thermore, 2-factorial analysis (or post hoc tests of sub-
groups) would eliminate most of the interesting variance
in dissociation. To assess the influence of anxiety, de-
pression, and comorbid PTSD on the physiological re-
sponse, multiple linear regression analyses were used. A
p-value of 6 0.05 conferred statistical significance. All
analyses were two-tailed.
3. Results
3.1. Demographic and psychometric data
Demographic and psychometric data are presented in
Table 1. Patients with BPD reported significantly higher
values in the present-state dissociation (DSS), trait dis-sociation (DES), depression (BDI) and anxiety (STAI).
The correlation between DSS and DES was significant
(r ¼ 0:61; p6 0:001).

U.W. Ebner-Priemer et al. / Journal of Psychiatric Research 39 (2005) 85–92 89
3.2. Audiometric examination and physiological resting
period data
Audiometric examination revealed comparable re-
sults and no hearing impairment in patients and controls(Table 1). Physiological resting period values (mean of
pre-experiment and post-experiment resting periods) are
given in Table 1. Whereas the mean resting period scores
for HR and SCL were comparable between patients and
controls, the EMG mean resting period scores were
significantly lower in the patients with BPD. Because
EMG raw scores depend strongly on the extent of skin
abrading and electrode placement, raw score compari-sons of group differences are problematic (Tassinary and
Cacioppo, 2000). However, to assess a possible impact
of low resting scores on the amplitude of the startle re-
sponse, EMG resting values were included as a control
variable in the multiple regression analysis. Anyway, it
should be noted that previous studies have not shown
such an influence (Ornitz et al., 1996).
3.3. Physiological responses
EMG, SC and HR scores and the results of the sta-
tistical analyses are shown in Table 2. Three patients
and three HC were non-responders for EMG, and two
patients and one HC were non-responders for SC; these
subjects were therefore excluded from the analyses.
In the ANCOVA for EMG, a highly significant groupeffect was found in response to the 15 tones, such that
the BPD group showed a higher response. Further, there
was a significant effect for the covariate, present-state
dissociative experiences. Examining habituation as
number of trials needed to reach the EMG non-response
criterion (TTC), the ANCOVA again revealed a highly
significant effect for group, such that the BPD group
Table 2
Response scores of electromyogram, skin conductance and heart rate and the
BPD HC
Mean (SD) Mean (SD)
EMG
Response 2–15 # 1.45 (0.90) 1.01 (0.47)
TTC 10.33 (5.93) 7.94 (5.42)
Slope )0.26 (0.41) )0.26 (0.36)
SC
Response 2–15 # 0.53 (0.3) 0.37 (0.2)
TTC 7.84 (4.8) 6.40 (5.0)
Slope )0.61 (0.31) )0.27 (0.47)
HR
Response 2–15 # 4.52 (2.5) 4.98 (3.3)
Slope 0.04 (1.1) )0.54 (1.2)
EMG, electromyogram; SC, skin conductance; HR, heart rate; Response
transformation; df (EMG)¼ 1.33, df (SC)¼ 1.36, df (HR)¼ 1.39, n(EMG
HC¼ 21.
needed more trials, and for the covariate, present-state
dissociation. No effect was found for relative habitua-
tion (slope). No differences were found in SC and HR
for all parameters (response, TTC and slope).
To further assess whether the results of the EMG canbe explained by other confounding variables, two mul-
tiple regression analysis were computed, predicting
mean response and TTC. Each had one fixed factor
(group: BPD vs. HC) and the following stepwise (for-
ward entry) factors: present-state dissociation (DSS),
anxiety (STAI), PTSD diagnosis, and EMG baseline
levels (resting period). For both (mean response, TTC),
only the overall model with the factors group and dis-sociation accounted significantly for the variance (mean
response: R2 (group and DSS) ¼ 0.21; F ð2:33Þ ¼ 4:32;p ¼ 0:022; TTC : R2 (group and DSS)¼ 0.34;
F ð2:33Þ ¼ 8:46; p ¼ 0:001). Anxiety, PTSD and EMG
baseline level were not significant predictors in either
equation. Furthermore, a model with group alone (BPD
vs. HC) as well as a model with present-state dissocia-
tion (DSS) alone did not account significantly for thevariance.
To show the direction of the influence of present-state
dissociation on EMG graphically, we split the group of
patients with BPD into two subgroups along the median
of the DSS. The HC group was not split because of
insufficient variation in DSS scores (see Table 1). We
designated the two BPD subgroups as low (0.53� 0.34)
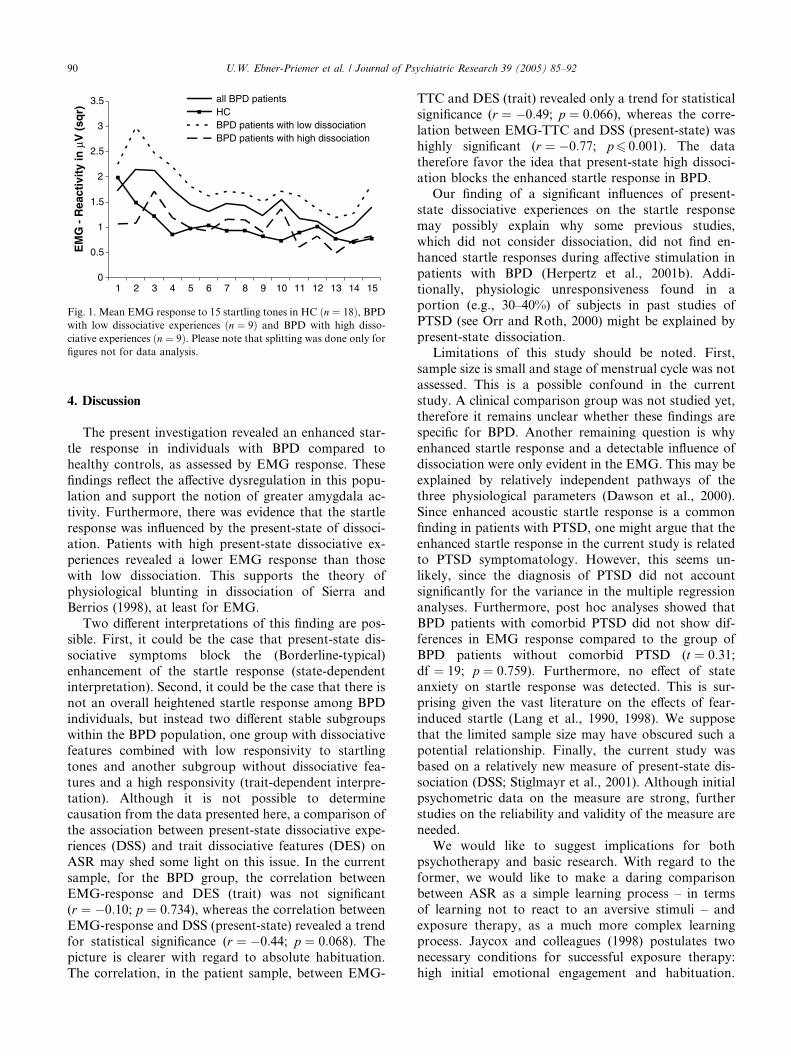
and high (2.51� 1.11) present-state dissociative experi-ences. As shown in Fig. 1, the startle responses to the 15
tones in the subgroup with low present-state dissociation
(dotted line) were higher than those of the subgroup
with high present-state dissociation (dashed line) and
those of the controls (solid line). T test revealed nearly
significant difference for reactivity between the two
subgroups (T ð16Þ ¼ 2:09; p ¼ 0:054).
results of the statistical analysis of female patients with BPD and HC
Main effect: group Covariate: DSS
F p F p
8.42 0.007 4.88 0.034
12.9 0.001 14.7 0.001
0.03 0.868 0.04 0.849
2.61 0.115 0.01 0.940
1.60 0.214 0.79 0.381
2.68 0.511 0.44 0.110
0.09 0.925 0.10 0.751
0.49 0.490 1.17 0.490
1–15, response to tone 1–15; TTC, trial to non-response; #, square root
) BPD¼ 18, HC¼ 18, n(SC) BPD¼ 19, HC¼ 20, n(HR) BPD¼ 21,
0
0.5
1
1.5
2
2.5
3
3.5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
EM
G -
Rea
ctiv
ity
in µ
V (
sqr)
all BPD patientsHCBPD patients with low dissociationBPD patients with high dissociation
Fig. 1. Mean EMG response to 15 startling tones in HC ðn ¼ 18Þ, BPDwith low dissociative experiences ðn ¼ 9Þ and BPD with high disso-
ciative experiences ðn ¼ 9Þ. Please note that splitting was done only for
figures not for data analysis.
90 U.W. Ebner-Priemer et al. / Journal of Psychiatric Research 39 (2005) 85–92
4. Discussion
The present investigation revealed an enhanced star-
tle response in individuals with BPD compared to
healthy controls, as assessed by EMG response. These
findings reflect the affective dysregulation in this popu-
lation and support the notion of greater amygdala ac-
tivity. Furthermore, there was evidence that the startle
response was influenced by the present-state of dissoci-
ation. Patients with high present-state dissociative ex-periences revealed a lower EMG response than those
with low dissociation. This supports the theory of
physiological blunting in dissociation of Sierra and
Berrios (1998), at least for EMG.
Two different interpretations of this finding are pos-
sible. First, it could be the case that present-state dis-
sociative symptoms block the (Borderline-typical)
enhancement of the startle response (state-dependentinterpretation). Second, it could be the case that there is
not an overall heightened startle response among BPD
individuals, but instead two different stable subgroups
within the BPD population, one group with dissociative
features combined with low responsivity to startling
tones and another subgroup without dissociative fea-
tures and a high responsivity (trait-dependent interpre-
tation). Although it is not possible to determinecausation from the data presented here, a comparison of
the association between present-state dissociative expe-
riences (DSS) and trait dissociative features (DES) on
ASR may shed some light on this issue. In the current
sample, for the BPD group, the correlation between
EMG-response and DES (trait) was not significant
(r ¼ �0:10; p ¼ 0:734), whereas the correlation between
EMG-response and DSS (present-state) revealed a trendfor statistical significance (r ¼ �0:44; p ¼ 0:068). The
picture is clearer with regard to absolute habituation.
The correlation, in the patient sample, between EMG-
TTC and DES (trait) revealed only a trend for statistical
significance (r ¼ �0:49; p ¼ 0:066), whereas the corre-
lation between EMG-TTC and DSS (present-state) was
highly significant (r ¼ �0:77; p6 0:001). The data
therefore favor the idea that present-state high dissoci-ation blocks the enhanced startle response in BPD.
Our finding of a significant influences of present-
state dissociative experiences on the startle response
may possibly explain why some previous studies,
which did not consider dissociation, did not find en-
hanced startle responses during affective stimulation in
patients with BPD (Herpertz et al., 2001b). Addi-
tionally, physiologic unresponsiveness found in aportion (e.g., 30–40%) of subjects in past studies of
PTSD (see Orr and Roth, 2000) might be explained by
present-state dissociation.
Limitations of this study should be noted. First,
sample size is small and stage of menstrual cycle was not
assessed. This is a possible confound in the current
study. A clinical comparison group was not studied yet,
therefore it remains unclear whether these findings arespecific for BPD. Another remaining question is why
enhanced startle response and a detectable influence of
dissociation were only evident in the EMG. This may be
explained by relatively independent pathways of the
three physiological parameters (Dawson et al., 2000).
Since enhanced acoustic startle response is a common
finding in patients with PTSD, one might argue that the
enhanced startle response in the current study is relatedto PTSD symptomatology. However, this seems un-
likely, since the diagnosis of PTSD did not account
significantly for the variance in the multiple regression
analyses. Furthermore, post hoc analyses showed that
BPD patients with comorbid PTSD did not show dif-
ferences in EMG response compared to the group of
BPD patients without comorbid PTSD (t ¼ 0:31;df ¼ 19; p ¼ 0:759). Furthermore, no effect of stateanxiety on startle response was detected. This is sur-
prising given the vast literature on the effects of fear-
induced startle (Lang et al., 1990, 1998). We suppose
that the limited sample size may have obscured such a
potential relationship. Finally, the current study was
based on a relatively new measure of present-state dis-
sociation (DSS; Stiglmayr et al., 2001). Although initial
psychometric data on the measure are strong, furtherstudies on the reliability and validity of the measure are
needed.
We would like to suggest implications for both
psychotherapy and basic research. With regard to the
former, we would like to make a daring comparison
between ASR as a simple learning process – in terms
of learning not to react to an aversive stimuli – and
exposure therapy, as a much more complex learningprocess. Jaycox and colleagues (1998) postulates two
necessary conditions for successful exposure therapy:
high initial emotional engagement and habituation.

U.W. Ebner-Priemer et al. / Journal of Psychiatric Research 39 (2005) 85–92 91
The results of the current study suggest that exposure
therapy in patients with BPD might be hampered by
both: patients experiencing low levels of dissociation
may reveal prolonged habituation (at least in the
TTC), whereas patients with high dissociation mayshow attenuated initial emotional activation (Fig. 1).
A treatment-outcome study of patients with panic
disorder could already confirm, that dissociative be-
havior led to poorer outcomes in exposure therapy
(Michelson et al., 1998). However, the finding of al-
tered habituation (TTC) should be interpreted care-
fully because it is inherently confounded with the level
of startle reactivity.With regard to basic research, the present findings
highlight the importance of assessing present-state dis-
sociation, in investigations of psychophysiology, neu-
ropsychology and neuroimaging in BPD as well as other
disorders with comorbid dissociative behavior.
Our findings, of course, require replication in order to
determine the strength and stability of the present
findings. Additional studies examining the extent ofemotion dysregulation in individuals with BPD to a
range of stimuli as well as the role of present-state dis-
sociation in emotional reactivity among individuals with
BPD are needed to fully understand the nature of
emotion dysregulation in this population.
Acknowledgements
This research was supported by a grant (Bo 1487/3-1)
from the German Research Society (DFG) and the
Borderline Personality Disorder Research Foundation
(BPDRF). The authors thank J. Fahrenberg, F. Foer-
ster, P. H€uttner, and V. H€oppner from the Psycho-
physiology Research Unit, University of Freiburg for all
methodological, technical and statistical support, andthe patients and control probands for their participation
in the study.
References
Beck AT, Ward CH, MendelsonM, Mock H, Erbaugh J. An inventory
for measuring depression. Archives of General Psychiatry
1961;4:561–71.
Berg WK, Balaban MT. Startle elicitation: stimulus parameters,
recording techniques, and quantification. In: Dawson ME, Schell
AM, B€ohmelt AH, editors. Startle modification: implications for
neuroscience, cognitive science, and clinical science. New York:
Cambridge University Press; 1999. p. 21–50.
Bernstein EM, Putnam FW. Development, reliability, and validity of a
dissociation scale. Journal of Nervous and Mental Disease
1986;174:727–35.
Bohus M, Haaf B, Stiglmayr CE, Pohl U, Boehme R, Linehan MM.
Evaluation of inpatient dialectical-behavioral therapy for border-
line personality disorder – a prospective study. Behaviour Research
and Therapy 2000;38:875–87.
Boucsein W. Electrodermal activity. New York: Plenum Press; 1992.
Corrigan FMD, Davidson A, Heard HL. The role of dysregulated
amygdalic emotion in borderline personality disorder. Medical
Hypotheses 2000;54:574–9.
Davis M, Walker DL, Lee Y. Neurophysiology and neuropharmacol-
ogy of startle and its affective modulation. In: Dawson ME, Schell
AM, B€ohmelt AH, editors. Startle modification: implications for
neuroscience, cognitive science, and clinical science. Cambridge:
University Press; 1999. p. 95–114.
Dawson ME, Schell AM, Filion DL. The electrodermal system. In:
Cacioppo JT, Tassinary LG, Berntson GG, editors. Handbook of
psychophysiology. Cambridge: University Press; 2000. p. 200–23.
Dougherty DM, Bjork JM, Huckabee HCG, Moeller FG, Swann AC.
Laboratory measures of aggression and impulsivity in women with
borderline personality disorder. Psychiatry Research 1999;85:315–
26.
Driessen M, Herrmann J, Stahl K, Zwaan M, Meier S, Hill A,
Osterheider M, Petersen D. Magnetic resonance imaging volumes
of the hippocampus and the amygdala in women with borderline
personality disorder and early traumatization. Archives of General
Psychiatry 2000;57:1115–22.
First MB, Spitzer RL, Gibbon M, Williams JBW. User’s guide for the
Structured Clinical Interview for DSM-IV personality disorders
(SCID-II). Washington, DC: American Psychiatric Press; 1996.
First MB, Spitzer RL, Gibbon M, Williams JBW, Benjamin LS. User’s
guide for the Structured Clinical Interview for DSM-IV axis I
disorders (SCID-I) – clinical version. Washington, DC: American
Psychiatric Press; 1997.
Foa EB, Kozak MJ. Emotional processing of fear: exposure to
corrective information. Psychological Bulletin 1986;99:20–35.
Foerster F. Programm-Paket BIO (Computersoftware). Germany:
Psychophysiology Research Unit, University of Freiburg; 1998.
Fridlund AJ, Cacioppo JT. Guidelines for human electromyographic
research. Psychophysiology 1986;23:567–89.
Griffin MG, Resick PA, Mechanic MB. Objective assessment of
peritraumatic dissociation: psychophysiological indicators. Amer-
ican Journal of Psychiatry 1997;154:1081–8.
Herpertz SC, Dietrich TM, Wenning B, Krings T, Erberich SG,
Willmes K, Thron A, Sass H. Evidence of abnormal amygdala
functioning in borderline personality disorder: a functional MRI
study. Biological Psychiatry 2001;50:292–8.
Herpertz SC, Kunert HJ, Schwenger UB, Sass H. Affective
responsiveness in borderline personality disorder: a psycho-
physiological approach. American Journal of Psychiatry
1999;156:1550–6.
Herpertz SC, Werth U, Lukas G, Qunaibi M, Schuerkens A, Kunert
HJ, Mueller-Isberner R, Osterheider M, Sass H. Emotion in
criminal offenders with psychopathy and borderline personality
disorder. Archives of General Psychiatry 2001;58:737–45.
Jaycox LH, Foa EB, Morral AR. Influence of emotional engagement
and habituation on exposure therapy for PTSD. Journal of
Consulting and Clinical Psychology 1998;66:185–92.
Kaufman ML, Kimble MO, Kaloupek DG, McTeague LM, Bachrach
P, Forti AM, Keune TM. Peritraumatic Dissociation and Physi-
ological Response to Trauma Relevant Stimuli in Vietnam Combat
Veterans with Posttraumatic Stress Disorder. Journal of Nervous
and Mental Disease 2002;190:167–74.
Ladwig K-H, Marten-Mittag B, Deisenhofer I, Hofmann B, Schap-
perer J, Weyerbrock S, Erazo N, Schmiff C. Psychophysiological
Correlates of Peritraumatic Dissociative Responses in Survivors
of Life-Threatening Cardiac Events. Psychopathology 2002;35:
241–8.
Lang PJ, Bradley MM, Cuthbert BN. Emotion, attention, and the
startle reflex. Psychological Review 1990;97:377–95.
Lang PJ, Bradley MM, Cuthbert BN. Emotion, motivation, and
anxiety: brain mechanisms and psychophysiology. Biological
Psychiatry 1998;44:1248–63.
92 U.W. Ebner-Priemer et al. / Journal of Psychiatric Research 39 (2005) 85–92
Lanius RA, Williamson PC, Boksman K, Densmore M, Gupta M,
Neufeld RWJ, Gati JS, Menon RS. Brain activation during script-
driven imagery induced dissociative response in PTSD: a functional
magnetic resonance imaging investigation. Biological Psychiatry
2002;52:305–11.
Levine D, Marziali E, Hood J. Emotion processing in borderline
personality disorders. Journal of Nervous and Mental Disease
1997;185:240–6.
Linehan MM. Cognitive-behavioral treatment of borderline personal-
ity disorder. New York: The Guildford Press; 1993.
Lykken DT, Iacono WG, Haroian K, McGue M, Bouchard TJ.
Habituation of the skin conductance response to strong stimuli: a
twin study. Psychophysiology 1988;25:4–15.
Maldonado JR, Spiegel D. Trauma, dissociation, and hypnotizability.
In: Bremner JD, Marmar CR, editors. Trauma, memory and
dissociation. Washington, DC: American Psychiatric Association;
1998. p. 57–106.
Metzger LJ, Orr SP, Berry NJ, Ahern CE, Lasko NB, Pitman RK.
Physiologic reactivity to startling tones in women with posttrau-
matic stress disorder. Journal of Abnormal Psychology
1999;108:347–52.
Michelson L, Vives A, Testa S, Marchione N, June K. The role of
trauma and dissociation in cognitive-behavioral psychotherapy
outcome and maintenance for panic disorder with agoraphobia.
Behaviour Research and Therapy 1998;36:1011–50.
Nijenhuis ERS, Spinhoven P, Van Dyck R, van der Hart O. The
development and psychometric characteristics of the Somatoform
Dissociation Questionnaire (SDQ-20). Journal of Nervous and
Mental Disease 1996;184:688–94.
Ornitz EM, Russell AT, Yuan H, Liu M. Autonomic, electroenceph-
alographic, and myogenic activity accompanying startle and its
habituation during mid-childhood. Psychophysiology 1996;33:507–
13.
Orr SP, Roth WT. Psychophysiological assessment: clinical applica-
tions for PTSD. Journal of Affective Disorders 2000;61:225–40.
Rauch SL, Whalen PJ, Shin LM, McInerney SC, Macklin ML, Lasko
NB, Orr SP, Pitman RK. Exaggerated amygdala response to
masked facial stimuli in posttraumatic stress disorder: a functional
MRI study. Biological Psychiatry 2000;47:769–76.
Rosen JB, Davis M. Enhancement of acoustic startle by electrical
stimulation of the amygdala. Behavioral Neuroscience
1988;102:195–202.
Rosen JB, Hitchcock JM, Sananes CB, Miserendino MJ. A direct
projection from the central nucleus of the amygdala to the acoustic
startle pathway: anterograde and retrograde tracing studies.
Behavioral Neuroscience 1991;105:817–25.
Sanislow CA, Grilo CM, Morey LC, Bender DS, Skodol AE,
Gunderson JG, Shea MT, Stout RL, Zanarini MC, McGlashan
TH. Confirmatory factor analysis of DSM-IV criteria for border-
line personality disorder: findings from the collaborative longitu-
dinal personality disorders study. American Journal of Psychiatry
2002;159:284–90.
Shalev AY, Peri T, Brandes D, Freedman S, Orr SP, Pitman RK.
Auditory startle response in trauma survivors with posttraumatic
stress disorder: a prospective study. American Journal of Psychi-
atry 2000;157:255–61.
Shalev AY, Peri T, Orr SP, Bonne OB, Pitman RK. Auditory startle
responses in help-seeking trauma survivors. Psychiatry Research
1997;69:1–7.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller
E, Hergueta T, Baker R, Dunbar GC. The Mini International
Neuropsychiatric Interview (M.I.N.I): the development and vali-
dation of a structured diagnostic psychiatric interview for DSM-IV
and ICD-10. Journal of Clinical Psychiatry 1998;59:22–33.
Sierra M, Berrios GE. Depersonalization: neurobiological perspec-
tives. Biological Psychiatry 1998;44:898–908.
Sierra M, Senior C, Dalton J, McDonough M, Bond A, Phillips ML,
O‘Dwyer AM, David AS. Autonomic response in depersonaliza-
tion disorder. Archives of General Psychiatry 2002;59:833–8.
Siever LJ, Torgersen S, Gunderson JG, Livesley WJ, Kendler KS. The
borderline diagnosis III: identifying endophenotypes for genetic
studies. Biological Psychiatry 2002;51:964–8.
Skodol AE, Gunderson JG, Pfohl B, Widiger TA, Livesley WJ, Siever
LJ. The borderline diagnosis I: psychopathology comorbidity, and
personaltity structure. Biological Psychiatry 2002;51:936–50.
Skodol AE, Siever LJ, Livesley WJ, Gunderson JG, Pfohl B, Widiger
TA. The borderline diagnosis II: biology, genetics, and clinical
course. Biological Psychiatry 2002;51:951–63.
Spielberger CD, Gorsuch RL, Lushene RE. STAI manual. Palo Alto:
Consulting Psychologists Press; 1970.
Stein KF. Affect instability in adults with a borderline personality
disorder. Archives of Psychiatric Nursing 1996;10:32–40.
Stiglmayr CE, Shapiro DA, Stieglitz RD, Limberger MF, Bohus M.
Experience of aversive tension and dissociation in female patients
with borderline personality disorder – a controlled study. Journal
of Psychiatric Research 2001;35:111–8.
Tassinary LG, Cacioppo JT. The skeletomotor system: surface
electromyogramm. In: Cacioppo JT, Tassinary LG, Berntson
GG, editors. Handbook of psychophysiology. 2nd ed. Cambridge:
University Press; 2000. p. 163–99.
Tebartz van Elst L, Thiel T, Hesslinger B, Henke M, Lieb K,
Bohus M, Henning J, Ebert D. Evidence of subtle prefrontal
neuropathology in patients with borderline personality disorder
as assessed by Short Echo 1H – magnetic resonance spectros-
copy study. Journal of Neuropsychiatry and Clinical Neuro-
science 2001;13:511–4.
Wagner AW, Linehan MM. Dissociation. In: Follette VM, Ruzek
JJ, Abueg FR, editors. Trauma in context: a cognitive-
behavioral approach. New York: Guildford Press; 1999. p.
191–225.
Zanarini MC, Gunderson JG, Frankenburg FR, Chauncey DL. The
revised diagnostic interview for borderlines: discriminating BPD
from other axis II disorders. Journal of Personality Disorders
1989;3:10–8.
Zanarini MC, Ruser TF, Frankenburg FR, Hennen J, Gunderson JG.
Risk factors associated with the dissociative experiences of
borderline patients. Journal of Nervous and Mental Disease
2000;188:26–30.







