Download - A Child With Wheeze

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 1/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 2/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 3/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 4/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 5/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 6/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 7/53
What structural aspects must be consideredin the process of respiration?
• Trachea• Primary bronchi• Secondary bronchi• Tertiary bronchi• Bronchioles• Terminal bronchioles•
Respiratory bronchioles withstart of alveoli outpouches• Alveolar ducts with outpouchings
of alveoli
conductiveportion
exchangeportion

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 8/53
ExternalRespiration
InternalRespiration

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 9/53
Anatomy of Immune System

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 10/53
Physiology of Immune SystemTo discriminate self form non-self and to eliminate the
foreign substanceTo protect the host against foreign antigen
8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 11/53
Definition of WheezePolyphonic(multiple pitch) noise coming from theairways believed to represent many airways of differentdimensions vibrating from abnormal narrowing.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 12/53
eren a agnoses oConditions that can cause
WheezingTransient early wheezing Atopic asthma
Non-atopic asthmaRecurrent aspiration of feedsInhaled foreign bodyCystic fibrosisRecurrent anaphylaxis in a child with food allergiesCongenital abnormality of lung, airway or heartIdiopathic

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 13/53
Asthma

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 14/53
Definition of Asthma
• Chronic airway inflammation leading to increaseairway responsiveness that leads to recurrent episodesof wheezing, breathlessness, chest tightness andcoughing particularly at night or early morning.
• Often associated with widespread but variable airflowobstruction that is often reversible eitherspontaneously or with treatment.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 15/53
• Reversible and variable airflow limitation asevidenced by >15% improvement in PEFR (PeakExpiratory Flow Rate), in response to administration ofa bronchodilator.
8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 16/53
Recommendations to define pre-
school wheezing2 main categories:• Episodic (viral) wheeze.
only wheeze with viral infections and are well betweenepisodes.• Multiple trigger wheezers
have discrete exacerbations and symptoms in betweenthese episodes. Triggers are smoke, allergens, crying,laughing and exercise.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 17/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 18/53
Pathophysiology of asthma

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 19/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 20/53
Clinical Features of AsthmaSymptoms worse at night and in the early morningSymptoms that triggers (eg: exercise, pets, dust, coldair, emotions, laughter)Intervals symptoms (between acute exacerbation)Personal or family history of an atopic diseasePositive response to asthma therapy.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 21/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 22/53
Harrison’s sulciDepression at the base ofthe thorax with muscularinsertion of the diaphragmare called Harrison’s sulci,and are associated withchronic obstructive airwaysdisease such as asthmaduring childhood.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 23/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 24/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 25/53
Management Aim of management-- To allow the child to lead a normal life by controllingthe symptoms and preventing exacerbations,optimising pulmonary function, while minimizingtreatment and side effects.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 26/53
Outcome of AsthmaMajority has a good prognosis.Those more severe, persistent asthma cases , developlongitudinal changes in lung function. ( impaired lungfunction in childhood and decline in lung function inadulthood)Early intervention of anti-inflammatory therapy may
improve the short-term outcome of asthma.Disease progression to nonreversible airflowobstrcution may be observed in minority.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 27/53
EpidemiologyEstimated prevalence of asthma in Malaysia is4.2%. (The Star, May 2011)
International Studies on Asthma and Allergy(ISAAC) has shown the prevalence of asthmaamong school children is 10%. (Protocol Ed3)
Among children up to 14 yrs old has aprevalence rate of 4.5% and age 15 years andabove is 4.1%. (The Star, May 2011)

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 28/53
Prevalence of childhood asthma is 24%, particullarly inMalays and those living in urban areas. ( Selangor ,2011)
A study of symptom control and severity of Asiansunder 16 years old shows that 2.5% controlled while53.4% uncontrolled asthma.(MIMS, Jul 2014)
As for severity, 24.5% had moderate to severepersistent symptoms.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 29/53
Participants of uncontrolled asthma were the most
frequent users of anti-asthmatic medication andurgent healthcare services. (MIMS, Jul 2014)
Hospitalization was the most important factoraffecting life quality of Malaysian parents withasthmatic child.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 30/53
Grading of severity in asthma1. IntermittentDaylight symptoms less than once a week
Noctural symptoms less than once a monthNo exercise induced symptomsBrief, infrequent exacerbation not affecting sleep andactivityNormal lung function

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 31/53
2. Persistent
Criteria Mild Moderate Severe
DaylightSymptoms
>once a week Daily Daily
NocturalSymptoms
>2x a month >once a week Daily
Exercise inducedsymptom
Present Present Daily
Exacerbation(affecting sleepand activity)
> 1x/month >2x/month Frequently,>2x/month
PERF/FEV1 >80% 60% - 80% <60%
PEFR: Peak Expiratoty Flow Metre FEV1: Forced Expiratory Vol in 1 sec

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 32/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 33/53
Acute exacerbation Assessment of severity:i. Diagnosis: cough,wheezing, breathless
ii.Triggering factor: food, exercise, drugs
iii.Severity: RR, RE, consious lvl.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 34/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 35/53
Criteria for admissionFailure to respond to standard home treatment.Failure to respond to nebulised beta 2 agonist.
Relapse with 4 hours of nebulised beta 2 agonists.Severe acute asthma.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 36/53
DrugsBronchodilatorsBeta 2 Agonist (SABA, LABA) Anticholinergic (Ipratropium bromide)
Inhaled CorticosteroidsLeukotriene receptor agonist (oral)Theophylline
Prednisolone (Oral steroids) Anti-IgE injection (Omalizumab)

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 37/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 38/53
Mnemonics A - Adrenergics (Beta 2 Agonist)
- AlbuterolS - SteroidsT - TheophylineH - Hydration (IV)M - Mask O2 A - Anticholinergics
- Ipratropium bromide

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 39/53
Inhaler
N b li

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 40/53
Nebulizer
• Only used in acute asthma whereoxygen is needed in addition to inhaleddrugs.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 41/53

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 42/53
Allergic Disorders Allergy - an “altered state of reactivity” to commonenvironmental antigens.Most patients with allergy produce IgE antibodies to theantigens; familial predisposition to allergic diseases
Allergic rhinitis Allergic conjuntivitisEctopic eczema
Urticaria AnaphylaxisFood and drug allergyInsect bite hypersensitivity

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 43/53
8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 44/53
• Sudden onset• if the chest does not rise when ventilation is firstattempted.• The most serious complication is complete obstructionof the airway, recognized as sudden respiratory distressfollowed by inability to speak or cough.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 45/53
Three stages of symptoms:1. Initial event — violent paroxysms of coughing,
choking, gagging, and persistent monophonic wheeze.
2. Asymptomatic interval — the foreign bodybecomes lodged, reflexes fatigue, and the immediateirritating symptoms subside.
3. Complications — obstruction, erosion, or infection.
Complications include lung abcess, fever, cough,hemoptysis, pneumonia, and atelectasis .

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 46/53
Most airway foreign bodies lodge in a bronchus (rightbronchus in ≈58% of cases); laryngeal or tracheallocations occur in ≈10% of cases.Bronchoscopyx-rayCT or MRI

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 47/53
8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 48/53
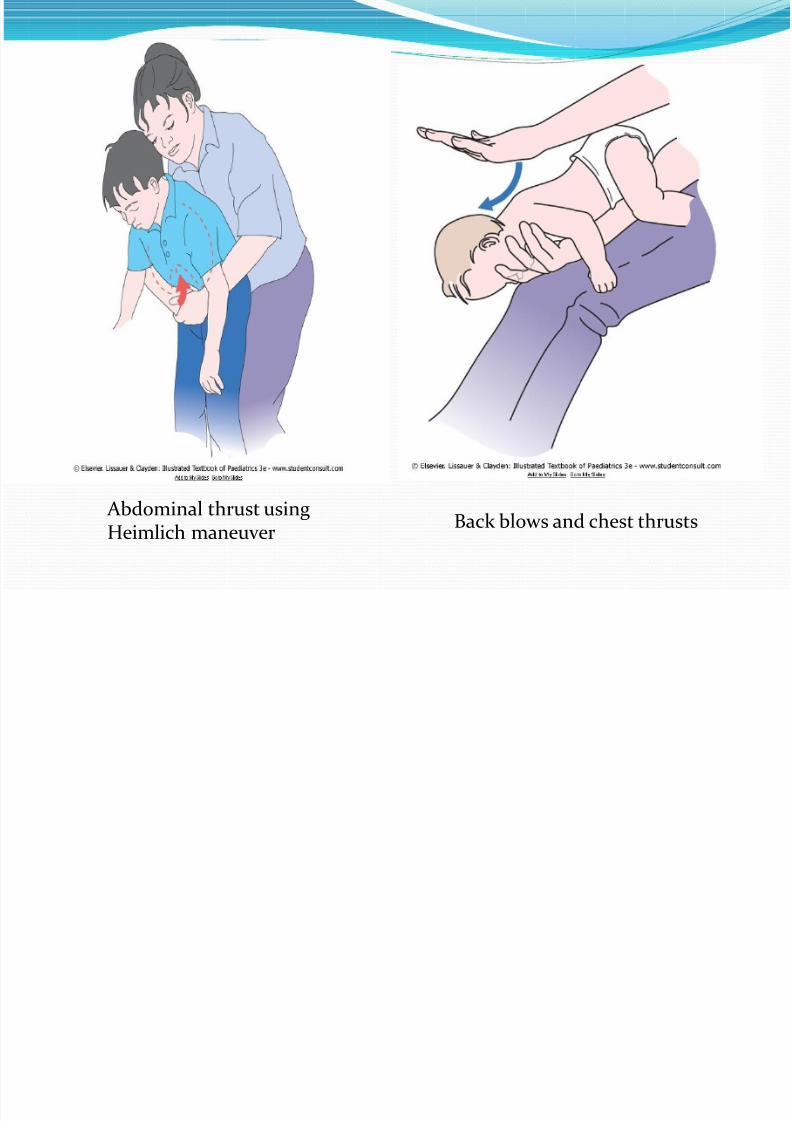
Abdominal thrust usingHeimlich maneuver Back blows and chest thrusts

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 49/53
Infant younger than 1 yr
Conscious child - permits to coughspontaneously until coughing is noteffective (or aphonic), respiratorydistress and stridor increaseUnconscious - the airway is opened with the head-tilt/chin-lift maneuver,and ventilation is attempted.
If there is still no chest rise, acombination of 5 back blows and 5chest thrusts is administered.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 50/53
Child older than 1 yr
A conscious child is administered a series of 5abdominal thrusts (Heimlich manoeuvre) with thechild standing or sitting.If the child is unconscious, this is done with the child
lying down.
1. Stand behind the patient2. Encircle arms around the upper part of the abdomen
just below the patient’s rib cage 3. Give a sharp, forceful squeeze, forcing the diaphragm
sharply into the thorax.

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 51/53
Obstructive emphysema (air trapping) and shiftof the mediastinum toward the opposite side.
8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 52/53
Clinical Approach to a Child with Wheeze AgeGradual or sudden onset, durationTransient early wheezing or persistent and recurrent
wheezingPreterm, maternal smoking Allergens (dust mites, pollens, pets etc), other allergicdisorders, family history of allergic disorder, asthmaFeeds

8/10/2019 A Child With Wheeze
http://slidepdf.com/reader/full/a-child-with-wheeze 53/53
ReferencesEuropean Respiratory Journals [Outcome of asthma :longitudinal changes in lung function]Illustrated Textbook of PaediatricsPaediatrics Protocols







