
1
Anti-Anxiety Agents and Sedative-Hypnotics
CNS CNS DEPRESSANTSDEPRESSANTS

INTRODUCTION• Anxiety is an unpleasant state of tension,
apprehension or uneasiness from an unknown source.
• Symptoms are similar to those of fear and is due to sympathetic activation
• Symptoms of Chronic, severe, debilitating anxiety requires treatment
• Hypnosis simply means sleep inducing • All antianxiety drugs cause sedation, and can
also function as anxiolytic and hypnotic agents. 2

3
• A sedative drug decreases activity, moderates excitement, and calms the recipient.
• B. A hypnotic drug produces drowsiness and facilitates the onset and maintenance of a state of sleep that resembles natural sleep, and from which the patient can be easily aroused.
• C. An anxiolytic drug reduces anxiety.

4

5
CLASSIFICATION
• Barbiturates• Benzodiazepines• Are the two major categories of sedative-
hypnotics • Other anxiolytic drugs• Nonbarbiturate sedatives

BENZODIAZEPINES (BDZs)
• Are the most widely used anxiolytic drugs• Have replaced barbiturates in the treatment of
anxiety cos are more effective and safer.
6

Mech of action
• GABA-A receptors is the target for BDZs.• It binds to a site on GABA-A called BDZ receptors• Binding of GABA to its receptor opens the chloride
channel causing hyperpolarization.• MOA: binding of BDZs to a site on GABA-A
receptor potentiates the effect of GABA by ↑ing the frequency of opening of chloride channel.
7

8

Benzodiazepines • DIAZEPAM• ALPRAZOLAM• LORAZEPAM• CLONAZEPAM• FLURAZEPAM• TEMAZEPAM• QUAZEPAM• MIDAZOLAM• ESTAZOLAM• TRIAZOLAM
9

ACTIONS• Reduction of anxiety: at low doses and acts via
enhancing the effects of GABA by binding to GABA-A receptors.
• Sedative and hypnotic: at higher doses via binding to GABA-A and enhancing the effect of GABA
• Anterograde amnesia: causes temporary impairment of memory by binding to GABA-A receptors.
• Anticonvulsant: used to treat epilepsy•
10

• Muscle relaxant: at high doses• All BDZs have neither anesthetic nor analgesic
property
11

Therapeutic uses• Anxiety disorders: that accompanies
depression and schizophrenia.• Panic disorder, phobias: alprazolam• Muscular disorder: diazepam• Amnesia• Seizures: clonazepam, diazepam(grand mal and
status epilepticus)• Clorazepate, chlordiazepoxide, diazepam,
oxazepam and lorazepam useful for treatment of alcohol withdrawal 12

continuation
• Sleep disorders:• Flurazepam: ↑es duration of sleep, ↓es
number of awakenings and its long acting
• Temazepam: used in pts who experience freq wakening
• Triazolam: used to induce sleep in pts with insomnia.
13

PHARMACOKINETICS
• BDZs are rapidly and completely absorbed after oral administration.
• Duration of action: • Long acting BDZs (1-3days):clorazepate,
chlordiazepoxide, diazepam, flurazepam and quazepam• Intermediate acting(10-20 hours): alprazolam,
estazolam, lorazepam, temazepam• Short-acting (3-8 hours): oxazepam, triazolam
14

Fate of BDZs
• Most are metabolized by the hepatic P450 system to compunds that are also active.
• Their effects are terminated by excretion or redistribution.
• All BDZs cross the placenta
15

16
PRECAUTIONS• LIVER FAILURE (most BDZs).• Some are not metabolized by the liver and so can
be given to pts with liver disease. It includesOxazepam, Temazepam, Lorazepam. These drugs are
not metabolized in liver. ( remember the first letters OTL – Outside The Liver)
• Alcohol and other CNS depressants enhance the sedative-hypnotic effects of BDZs
• Should be avoided in pts with narrow angle glaucoma

17
ADVERSE EFFECTS• DROWSINESS, CONFUSION• ATAXIA• Cognitive impairment
• DEPENDENCE : PSYCHOLOGICAL, PHYSICAL
WITHDRAWAL :• ANXIETY, TENSION,CONFUSION,
restlessness, REBOUND INSOMNIA (Triazolam)

18
Benzodiazepine antagonist
FLUMAZENIL• GABA receptor antagonist• Rapidly Reverses the effect of benzodiazepines.• I.V. route only.• Used for treatment of BDZs poisoning
SE:• Nausea, vomiting, agitation and dizziness.

19
OTHER ANXIOLYTIC DRUGS
• BUSPIRONE
• HYDROXYZINE
• ZOLPIDEM
• ZALEPLON

20
OTHER ANXIOLYTICS - BUSPIRONE
• Site of action: binds to 5-HT1A receptor subtype. • No anticonvulsant activity. • No interaction with benzodiazepine binding sites • No muscle relaxant properties and causes
minimal sedation• Minimal adverse effects • USED FOR GAD Generalized Anxiety Disorders• Slow onset of action

21
ZOLPIDEM• ACTS ON BENZODIAZEPINE RECEPTORS though not a
BDZ.• HYPNOTIC• NO ANTI CONVULSANT• NO MUSCLE RELAXTION• MINIMAL REBOUND INSOMNIA
• ONSET OF ACTION – FAST• METABOLIZED BY P450 TO INACTIVE COMPOUND• HALF LIFE – SHORT ( 3 HOURS)• SE: NIGHTMARES, GI UPSET, DAYTIME DROWSINESS

ZALEPLON
• Similar to zolpidem in its hypnotic actions but causes fewer side effects compared to zolpidem or BDZs.
• Has a half life of < 1hour• Metabolized by cyt P450 system.
22

Barbiturates
• Were formerly the mainstay of treatment used to sedate the patient or to induce and maintain sleep.
• Have been replaced by BDZs cos they induce tolerance, physical dependence, severe withdrawal symptoms and coma in toxic doses.
23

24
DRUGS
• PHENOBARBITAL – LONG ACTING• PENTOBARBITAL• SECOBARBITAL• Both are short acting• THIOPENTAL – ULTRA SHORT ACTING
( 20 MIN)

25
BARBITURATES
MECH OF ACTION :• Bind to GABA-A receptors potentiating the effect
of GABA by prolonging the duration of chloride channel opening.

Actions
• Anesthesia• Treatment of seizures• Sedative(low dose) and hypnotic agents(high doses)• Depression of CNS and can lead to coma and death.• Respiratory depression• Induces P450 in the liver• No analgesic action
26

Therapeutic uses
• Anesthesia: thiopental an ultra-short acting barbiturate is used intravenously to induce anesthesia.
• Anticonvulsant: phenobarbital used in the long term management of tonic-clonic seizures, status epilepticus
• Anxiety: used as sedatives to relieve anxiety, nervous tension, insomnia at low doses
27

pharmacokinetics
• Readily cross the placenta and can depress the fetus.
• Are metabolized by the liver except phenobarbital
• Excreted in urine• Barbiturate + alcohol = bad combination
28

29
ADVERSE EFFECTS
• Drowsiness• CNS: Impaired concentration, sluggishness• HANG OVER: Hynoptic doses
• METABOLISED IN LIVER• CI : ACUTE INTERMITTENT PORPHYRIA
• DEPENDENCE:• WITHDRAWAL SEVERE: MAY CAUSE DEATH

Barbiturate poisoning
• Severe depression of respiration• CVS depression• Shock• Treatment: artificial respiration,gastic lavage,
hemodialysis, alkalinzation of urine.• No specific barbiturate antagonist available
30

NONBARBITURATE SEDATIVES• Chloral hydrate• Antihistamine• ethanol
31

32
OTHER SEDATIVES
• ANTIHISTAMINES : diphenhydramine, doxylamine are effective in treating mild types of insomnia
CHLORAL HYDRATE• SEDATIVE AND HYPNOTIC• SE: GI UPSET• TASTE CHANGES• PREFERRED ROUTE : PER RECTAL

33

ETHANOL
• Is a CNS depressant at high doses• Anxiolytic • Produces sedation • Hypnosis with increasing dosage.• Crosses the placenta• Metabolized in the liver first to acetaldehyde by
alcohol dehydrogenase and then to acetate by acetaldehyde dehydrogenase
34

ALCOHOL METAB
35

36
CNS
CHR. EFFECT•DEPRESSION, MEMORY LOSS•RISK FOR SEIZURES•WERNICKES – KORSAKOFFS ENCEPHALOPATHY•Metabolic effects: hypoglycemia, gout, lactic acidosis

37
CVS :• ACUTE : VASODILATION• HIGH DOSES : VASOCONSTRICTION IN
HEART• CHRONIC: MYOCARDIAL DEPRESSION
GIT : • ACUTE : STIMULATES ACID• HIGH : DIRECT IRRITATION• CHRONIC: DIARRHOEA / CONSTIPATION,,
PANCREATITIS

38
• LIVER :• CHR : CIRRHOSIS
• RESPIRATORY DEPRESSION
• CHRONIC :IMPOTENCE, TESTICULAR ATROPHY, GYNAECOMASTIA
• PREGNANCY : FETAL ALCOHOL SYN.• LOW IQ, MICROCEPHALY, FACIAL ABNORMAILITIES.

39
continuation
• Elimination: kidney(MC), lung• Alcohol withdrawal is treated with BDZs
40

Disulfiram
• Blocks the oxidation of acetaldehyde to acetate by inhibiting acetaldehyde dehydrogenase
• Results in the accum of acetaldehyde in the blood causing unpleasant symptoms such as flushing, tachycardia, hyperventilation, nausea
• Used in pts seriously desiring to stop alcohol ingestion.
41

42
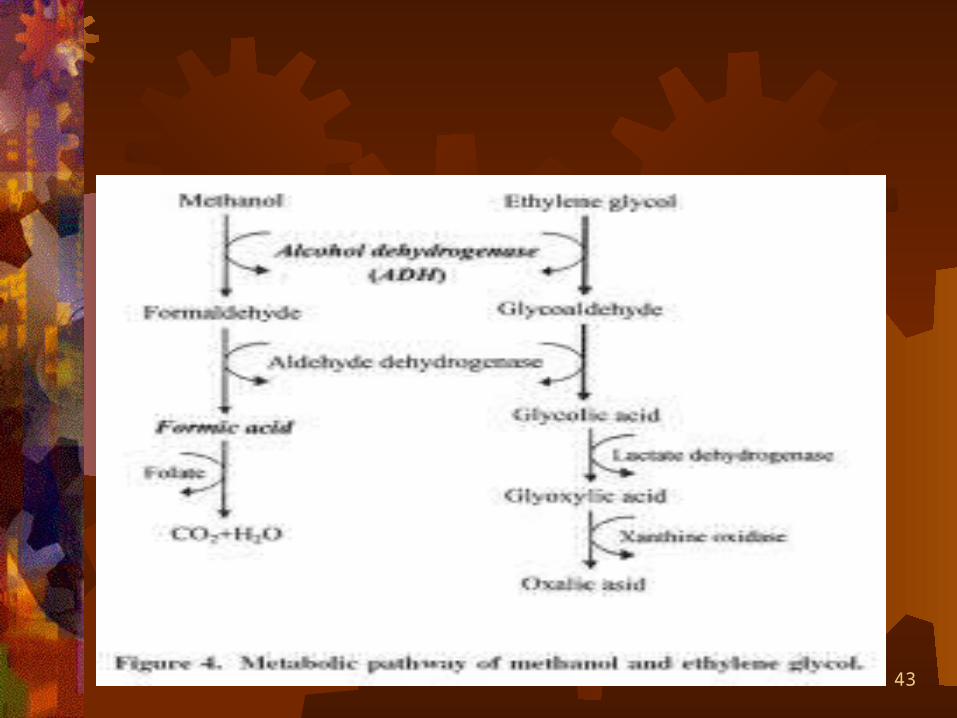
OTHER ALCOHOLS
METHANOL :• FORMS FORMIC ACID
• EFFECTS : BLINDNESS, SEVERE ACIDOSIS.. Respiratory failure…
• Ethylene glycol: forms OXALIC ACID• Side effect: acute tubular necrosis, CNS
depression, acidosis
43

Treatment for overdose
• Fomepizole: long acting inhibitor of alcohol dehydrogenase
• IV Ethanol: for methanol and ethylene glycol poisoning
44







