donor lymphocyte infusion: dr. chenhua yan
TRANSCRIPT

CHENHUA YAN, MDChina
• Associate Professor, Peking University Institute of Hematology
• Dr. Yan completed her residency from the Peking University People’s Hospital an dcurrently serves as an associate professor at the same institute. Her interests are in hematologic malignancies and clinical trials.

Peking University People’s Hospital & Institute of Hematology
Beijing Key Laboratory of HSCT, Beijing, P.R.China
Chen-hua Yan M.D
Modified donor Lymphocyte Infusion for Relapse of Hematologic Malignancies after Haploidentical
Hematopoietic Stem Cell Transplantation
Content
Establishment of modified donor lymphocyte infusion
Modified donor lymphocyte infusion for the treatment of relapse
1
2
Modified donor lymphocyte infusion for the prevention of relapse3
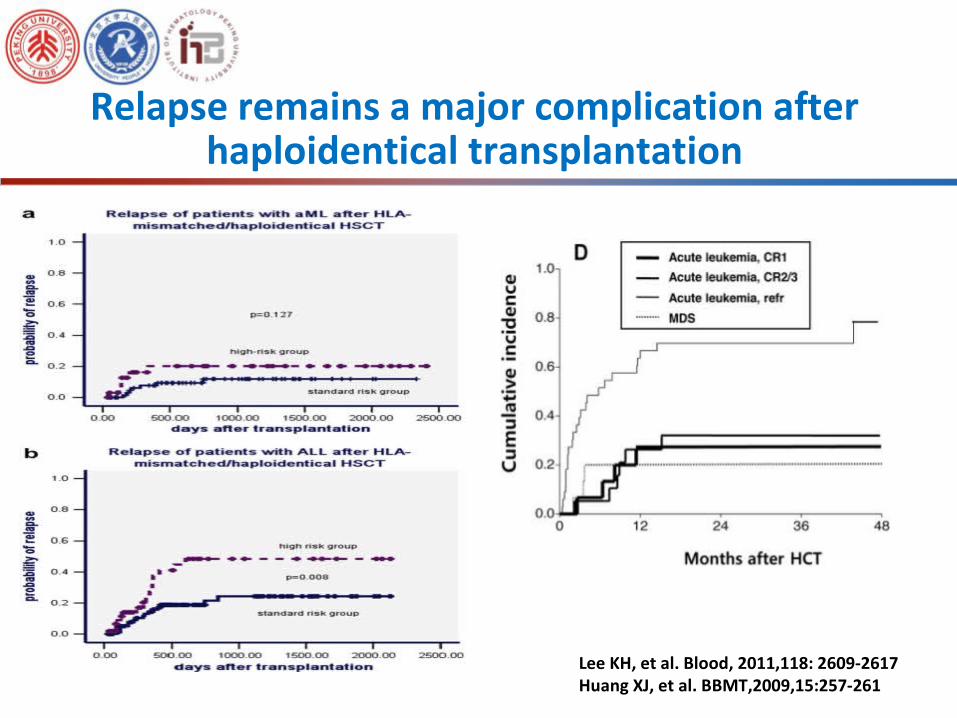
Relapse remains a major complication after haploidentical transplantation
Lee KH, et al. Blood, 2011,118: 2609-2617Huang XJ, et al. BBMT,2009,15:257-261

Limited efficacy of DLI in the treatment of relapse
Levine JE, et al. BMT. 2008, 42: 201-205Schmid, et al. J Clin Oncol,2007,25:4938-45
Patients receiving DLI (n=228) 21% Patients not receiving DLI (n=171) 9%
P< 0.0001

One probable reason for the limited efficacy of DLI
• Higher incidence of severe acute GVHD after DLI
Marks DI, et al. Blood 2002; 100: 3108.Collins Jr RH, et al. J Clin Oncol 1997; 15: 433.Chalandon , et al. BMT 2010; 45: 558.
33%28%
15%
33%
26%
60%
46.40%
22.40%
60.70%
32.10%34%
21.60%
12.50%
25%
15.20%
0%
10%
20%
30%
40%
50%
60%
70%
acute GvHD grade 2-4 acute GvHD
grade 3-4 acute GvHD
chronic GvHD extensive chronic GvHD
RIC-sibling donor
MA-sibling and unrelated
MA-sibling and unrelated

Methods to minimize severe GVHD after DLI
Yan CH, et al. clinical transplant. 2012; 26: 868-876
• Escalating dose of DLI
• CD8+ T cell depleted DLI
• Modified DLI

Part 1
Establishment of modified DLI

• G-CSF could modulate the polarization of T cells from a Th1 to a Th2 phenotype
• G-CSF could indirectly induce T-cell hypo-responsiveness through the selective increase of DC2 cells and monocytes and the down-regulation of the CD28/B7 co-stimulatory signal.
• G-CSF could augment NK-T-cell–dependent CD8+ cytotoxicity
G-CSF moblized peripheral blood stem cell for Infusion
G-CSF maybe separates GVHD and GVL effects
Huang XJ,et al. Haematologica. 2004; 89: 1517-1524Huang XJ, et al. Transpl Immunol. 2007; 17: 193-197.Morris ES, et al. J Clin Invest. 2005; 115: 3093-3103.

• Twenty patients were enrolled. Unstimulate donor lymphocyte infusion (n=11, hematological relapse=5), GPBSCs infusion (n=9, hematological relapse=9).
• DLI: MNC > 1×108/Kg• Acute GVHD after DLI: GPBSCs 5/9 vs. lymphocytes 10/11
(P>0.05)• Grade 3 - 4 acute GVHD after DLI: GPBSCs 0/9 vs. lymphocytes
2/11 (P>0.05)• CR rate after DLI: GPBSCs 7/9 vs. lymphocytes 3/5 (P<0.01)
GPBSCs Infusion vs. unstimulate lymphocytes ifusion
Huang XJ,et al. Chin Med J (Engl). 2003; 116 (5):736-741.
GPBSCs infusion: G-CSF mobilized peripheral blood stem cell infusion

Application of immunosuppressive agents after GPBSCs infusion reduces severe acute GVHD
Huang XJ, et al. Hematologica 2007,92:414-417
In haploidentical DLI: application of immunosuppressive agents after GPBSCs infusion could reduce severe GVHD
Grade 3 - 4 acute GVHD: (P=0.013)•no prophylaxis: 5/9 •with prophylaxis: 1/11
Question?---What is the appropriate duration of immunosuppressive
agents after haploidentical GPBSCs infusion?
Acute GVHD
no prophylaxis
with prophylaxis

Application of immunosuppressive agents after GPBSCs infusion reduces acute GVHD
Yan CH, et al. clinical transplant. 2012; 26: 868-876
49.5%
31.6%
14.4%
9.3%
In haploidentical DLI: prophylaxis 6 - 8 weeks reduced incidence of grade 3 - 4 acute GVHD

Application of immunosuppressive agents after GPBSCs infusion
Problems?
reducing DLI-associated acute GVHD
preserving GVL effects?

Application of immunosuppressive agents for 6 - 8 weeks reduced acute GVHD after haploidentical DLI
67.7%
39.0%
63.6%
32.7%32.9%
8.2%
Yan CH, et al. Chin Med J (Engl) 2014: 127: 3602-3609.
acute GVHDGrade 2 - 4 acute
GVHDGrade 3 - 4 acute
GVHD
prophylaxis <6w prophylaxis <6w
prophylaxis <6w
prophylaxis 6 - 8w
prophylaxis 6 - 8wprophylaxis 6 - 8w
P=0.020 P=0.012 P=0.005
prophylaxis for 6 - 8 w (n=52)prophylaxis <6 w (n=51)

Application of immunosuppressive agents for 6 - 8 weeks did not influence relapse rate after haploidentical DLI
Total patients (n=103) Hematological relapsed (n=54)
MRD-positive (n=49)
69.0%
26.6%
80.0%
55.6% 51.5%
17.3%
Yan CH, et al. Chin Med J (Engl) 2014: 127: 3602-3609.
prophylaxis for 6 - 8 w (n=52)prophylaxis <6 w (n=51)

Yan CH, et al. Chin Med J (Engl) 2014: 127: 3602-3609.
Application of immunosuppressive agents for 6 - 8 weeks improved survival after haploidentical DLI
Total patients (n=103) Hematological relapsed (n=54)
MRD-positive (n=49)
prophylaxis for 6 - 8 w (n=52)prophylaxis <6 w (n=51)
Establishment of modified donor lymphocyte infusion (mDLI)
G-CSF mobilized peripheral blood stem cells (GPBSCs) infusion
Application of immuno-suppressive agents for 6 - 8 weeks after
haploidentical GPBSCs infusion
mDLI

Part 1.2
Modified DLI for the treatment of relapsed hematological malignancies after haploidentical HSCT

Poor results of DLI alone for relapsed acute leukemia after HSCT
Probable reason: A heavier burdens of leukemic cells in relapsed acute leukemia
Schmid C, et al. J Clin Oncol. 2007; 25: 4938-4945.

Choi SJ, et al. Leukemia. 2004; 18 (11): 1789-1797.Huang, et al. Haematologica,2007,92(3):414-417
Chemotherapy followed by DLI could increase CR rate and improve survival in patients with relapsed acute leukemia
◆ 16 AML patients were enrolled. chemotherapy
followed by GPBSCs infusion
◆ CR after DLI: 10/16 (62.5%) patients
◆ OS at 2-year after DLI: 31%.
◆ 20 patients were enrolled. chemotherapy followed by GPBSCs
infusion
◆ CR after DLI: 13/20 (65.0%)
◆ LFS at 2-year after DLI: 40%.

Chemotherapy followed by mDLI vs. chemotherapy alone
Characteristics Chemo (n=32)
Chemo + DLI (n=50)
P
CR rate post-intervention (%) 4 (12.5) 32 (64.0) 0.000
Median time of onset of CR post-intervention (months) (range)
1.00 (0.70 - 1.00)
1.00 (0.50 - 4.90)
0.258
Duration of CR post-intervention (months) (range)
2.05 (2.00 - 3.00)
12.00 (1.00 - 109.90)
0.009
Yan CH, et al. Eur J Haematol. 2013; 91 (4): 304-314.

DFSP=0.000
chemo+DLI
chemo
chemo+DLI
chemoP=0.000
Chemotherapy followed by mDLI vs. chemotherapy alone
Yan CH, et al. Eur J Haematol. 2013; 91 (4): 304-314.
How to improve survival further?
Investigate the risk factors of relapse after chemotherapy followed by modified DLI

Multivariate analysis for higher relapse rate:Lack of chronic GVHD after DLI (P=0.039, OR=2.471) MRD (-) < 4 months after DLI (P=0.001, OR=40.342)
Risk-stratification
50 patients
No risk factors = 11
One of risk factor = 11
Two risk factors = 28
Low-risk
Intermediate-risk
High-risk
Risk factors of relapse for chemotherapy followed by mDLI
Yan CH, et al. Eur J Haematol. 2013; 91 (4): 304-314.

Relapse, OS, and DFS for low-risk, intermediate-risk and high-risk patients
Relapse OS DFS
Yan CH, et al. Eur J Haematol. 2013; 91 (4): 304-314.
How to improve survival further?
Repeated chemotherapy followed by modified DLI based on the status of MRD and GVHD post-DLI

Part 1.3.1
Modified DLI for the prevention of relapse: risk-stratification directed modified DLI in patients with positive status of MRD post-transplant

The levels of WT1 and LAIPs could predict relapse of acute leukemia
Huang XJ, et al. Ann Hematol. 2012;91:183-192.Huang XJ, et al. BMT. 2012;47:499-507

Patients with Leukemia
MRD monitoring
MRD (-) MRD (+)
Risk-stratification directed mDLI
Decrease relapse ?Improve survival ?
Hypothesis
after HSCT

Risk-stratification directed mDLI could reduce relapse
Total (n=814): 22.0% (95% CI 18.4-25.6%)
MRD (-) (n=709): 18.1% (95% CI 14.6-21.6%)
MRD (+)-IL-2 (n=49): 64.4%(95% CI 44.8-84.0%)
MRD (+)-DLI (n=56): 27.8% (95% CI 12.1-43.5%)Yan CH, et al. Blood,2012,119(14):3256-62
MRD (+) vs. MRD (-): P<0.001DLI vs. IL-2: P=0.001DLI vs. MRD (-): P=0.269

Yan CH, et al. Blood,2012,119(14):3256-62
Risk-stratification directed mDLI could improve survival
Risk-stratification directed mDLI could reduce relapse and improve survival after haploidentical HSCT
MRD (+) vs. MRD (-): P=0.041DLI vs. IL-2: P=0.002DLI vs. MRD (-): P=0.688
Part 1.3.2
Modified DLI for the prevention of relapse: prophylactic modified DLI in patients with relapsed/refractory acute leukemia at transplant

Prophylactic mDLI could reduce relapse and improve survival of patients with relapsed/refractory acute leukemia at haploidentical HSCT
Wang Yu, et al. BMT. 2012; 47 (8): 1099-104
Prophylactic mDLI could reduce relapse and improve survival

• Modified DLI could reduce incidence of acute GVHD, but did not compromise GVL Effects.
• Modified DLI was a potentially effective therapeutic option for relapsed acute leukemia after haploidentical HSCT and chemotherapy followed by modified DLI is superior to chemotherapy alone.
• Risk stratification-directed modified DLI could prevent relapse and improve survival after HSCT.
• Prophylactic modified DLI could prevent relapse and improve survival in patients with relapsed/refractory acute leukemia at haploidentical HSCT.
Summary

Questions remained?
• appropriate dose of CD3+ T cells in haploidentical
modified DLI
• appropriate drug used as immunosuppressive
agents after haploidentical modified DLI, such as
CSA or MTX
• appropriate time for prophylactic modified DLI

Acknowledgements
Stem cell collection centerHai-Yin ZhengHong XuQing ZhaoSu Wang
Department of bone marrow transplant Xiao-Jun Huang Kai-Yan Liu Dai-Hong Liu Lan-Ping XuHuan Chen Wei HanXiao-Hui Zhang Ying-Jun ChangYu-Hong Chen Feng-Rong Wang Jing-Zhi Wang Yu WangChen-Hua Yan Yuan-Yuan ZhangYu Ji Yu-Qian SunXiang-Yu Zhao Xiao-Su Zhao
Laboratory of PUIHDan LiYa-Zhen QinYan-Rong LiuYue-Yun Lai