doh guidelines for covid-19 infection related maternity
TRANSCRIPT
DOH GUIDELINES FOR COVID-19 INFECTION RELATED MATERNITY AND NEONATAL CARE
June 2020
Page 2 of 20
Document Title: DOH Guideline For COVID-19 Infection related Maternity and Neonatal Care
Document Ref. Number:
DOH/Guideline/ COVID-19 Infection related Maternity and Neonatal Care
Version 0.9
For Further Advice Contact:
Healthcare Quality Division
Applies To: All Healthcare Providers and Professionals licensed by DOH and engaged in the management of maternity patients in the Emirate of Abu Dhabi
Classification:
Public
Document Owner/ Control
This document shall be reviewed and updated by Healthcare Quality Division
* This guidelines is designed for regulatory procedures and should not be used as content for media publication”
Page 3 of 20
Table of Contents: 1. Introduction .............................................................................................................................. 4
2. About this Guideline .................................................................................................................. 4
3. Purpose .................................................................................................................................... 4
4. Scope ....................................................................................................................................... 5
5. Abbreviations and Definitions ................................................................................................... 5
6. General Approach for Outpatient and Inpatient Maternity Care: ............................................... 6
7. Emergency Management: ......................................................................................................... 9
8. Women who develop new symptoms of COVID-19 during admission (antenatal, intrapartum or postnatal) ............................................................................................................................... 10
9. Intrapartum Care for Women with suspected or confirmed COVID-19 .................................... 10
10. Newborn Care ......................................................................................................................... 12
11. Postnatal Management ........................................................................................................... 12
12. Reviewers: .............................................................................................................................. 15
13. Appendices ............................................................................................................................. 16
14. Bibliography ............................................................................................................................ 20
Page 4 of 20
1. Introduction
Unlike other viral infections (including previous coronaviruses and influenza), pregnant women with COVID-19 are not any more likely to have serious morbidity and complications than the general population based on age and gender. Vertical transmission is possible, although the proportion of pregnancies affected is uncertain and likely to be very low, with minimal or no effect on the neonate. The highest risk factor from Coronavirus in pregnancy is in women with significant heart disease (congenital or acquired), followed by the other well-known risk factors affecting the general population. Symptoms & effect on mother The large majority of women will experience only mild or moderate cold/flu like symptoms. Cough, fever and shortness of breath are other relevant symptoms. Pregnant women, due to changes to their immune system, may be associated with more severe symptoms particularly towards the end of pregnancy. Effect on the fetus There are currently no data suggesting an increased risk of miscarriage or early pregnancy loss or teratogenicity in relation to COVID-19. Risk of vertical transmission is reported but rare to date. Risk of preterm birth, fetal compromise and pre-labor preterm rupture of membranes are reported in common with general infections.
2. About this Guideline
This Guideline is based on a review of international guidelines on maternity and newborn care during COVID-19 pandemic. In addition, local technical/expert advice has largely contributed in the development of this guideline within the context of best practices for COVID-19 screening and management of maternal patients and newborns. The Guideline covers the following:
Maternity care for the woman under different situations.
Care for the newborn (intrapartum and postnatal management).
It addresses the recommended preventive and management practices under different care needs. However, as COVID-19 infection is an evolving situation the guidelines may need regular updates as new evidence emerges.
3. Purpose
This Guideline is designed to serve as a basic reference for the screening and management of mothers with suspected or confirmed COVID-19 infection and newborns in the Emirate of Abu Dhabi. This information combined with clinical judgment should lead to more appropriate
Page 5 of 20
testing and treatment to reduce transmission to pregnant women and their newborns & to provide safe care to women with suspected or confirmed COVID-19 and to newborns.
4. Scope
4.1 This guideline can be used by all healthcare providers and professionals licensed by DOH and engaged in the management of maternity patients in the Emirate of Abu Dhabi.
4.2 It applies to all patients seeking maternal care. 4.3 This guideline pertains to the screening and management of mothers with suspected or
confirmed COVID -19 infection.
5. Abbreviations and Definitions
Category Definition
CRP C-reactive Protein CT Computerized tomography CTG Cardiotocograph HDU High Dependency Unit HEPA High Efficiency Particulate Air
IPC Infection Prevention and Control IV Intravenous LMWH Low Molecular Weight Heparin NICU Neonatal Intensive Care Unit PPE Personal Protective Equipment UC Urgent Care URTI Upper Respiratory Tract Infection VTE Venous Thromboembolism
Page 6 of 20
6. General Approach for Outpatient and Inpatient Maternity Care:
Maternity care is essential, and studies have shown that if women do not attend antenatal services then they are at increased risk of maternal death, stillbirth, and other adverse perinatal outcomes. Women should therefore be encouraged to attend scheduled antenatal care although maternity care units should seek to adopt teleconferencing and videoconferencing capability where possible.
6.1 Outpatient Settings:
For women who are confirmed or suspected to be positive with scheduled antenatal appointments may be deferred until 7-14 days after the start of symptoms but only after review of the clinical circumstances by an obstetric physician. It is important that care is available to ensure continued support for women with multiple complex needs and individualized plans for women requiring frequent review may be necessary. As evidence continues to emerge regarding the effects of confirmed COVID-19 in pregnancy, recent reports suggest possible placental changes secondary to the viral infection, although these were not associated with clinical complications. It is therefore recommended to monitor women recovered from COVID-19 for signs of fetal growth restriction during the remainder of the pregnancy with a growth scan in the second trimester and serial growth scans during the third trimester. Visitor restrictions, including in outpatient settings are in place in all hospitals. Patients should attend outpatient appointments without escorts unless special consideration is required in rare complex cases.
6.2 Inpatient Setting:
During the pandemic period, all maternity patients who are admitted to hospital from the community shall be screened for COVID-19 at admission whether they have symptoms or not.
6.3 Appointments for Elective birth:
6.3.1 Women with suspected or confirmed COVID-19 with scheduled appointments for pre-operative care and elective caesarean birth should have individual assessments made to determine whether it is safe to delay the appointment to minimize the risk of infectious transmission to other women, healthcare workers and postnatally to the infants.
6.3.2 The same applies for induction of labor.
Page 7 of 20
6.4 COVID-19 Management:
6.4.1 In cases of uncertainty, providers should investigate and treat as suspected COVID-19 any maternity patients who are admitted to the hospital from the community until a negative test result is obtained. (Appendix for PPEs for COVID-19). All women with epidemiologic history of contact should be carefully monitored.
6.4.2 Pregnant women with a suspected, probable or confirmed COVID-19 infection, including women who may need to spend time in isolation should have access to woman-centered specialized care (hospital).
6.4.3 Appropriate IPC measures and prevention of complications, also apply to pregnant and recently pregnant women including those with miscarriage, late pregnancy fetal loss and postpartum/post abortion women
6.4.4 Mode of birth should be individualized based on obstetric indications and the woman’s preferences (hospital)
6.4.5 Recently pregnant women with COVID-19 or who have recovered from COVID-19 should be provided with necessary information and counselling on safe infant feeding and appropriate IPC measures to prevent COVID-19 transmission.
6.4.6 All pregnant women undergoing or recovering from COVID-19 should be provided with counselling and necessary information related to the potential risk of adverse pregnancy outcomes.
Page 8 of 20
6.5 Recommended Investigations: 6.5.1 PCR Test for COVID-19
o For inpatients, PCR test should be repeated every 72 hours* until negative. 6.5.2 Blood for full blood count, urea & electrolytes, liver function test & CRP. 6.5.3 Chest X-ray / Chest CT if indicated. 6.5.4 Other investigations for routine obstetric management e.g. CTG, ultrasound.
6.6 Ultrasound:
If ultrasound is required, it should be performed in the patient’s room. Ultrasound equipment used should be decontaminated after use in line with standard guidance.
*This may change as the epidemiology of the virus and more scientific data is available regarding the virus. Professionals should follow the updated
National Guidelines from DOH as they develop.
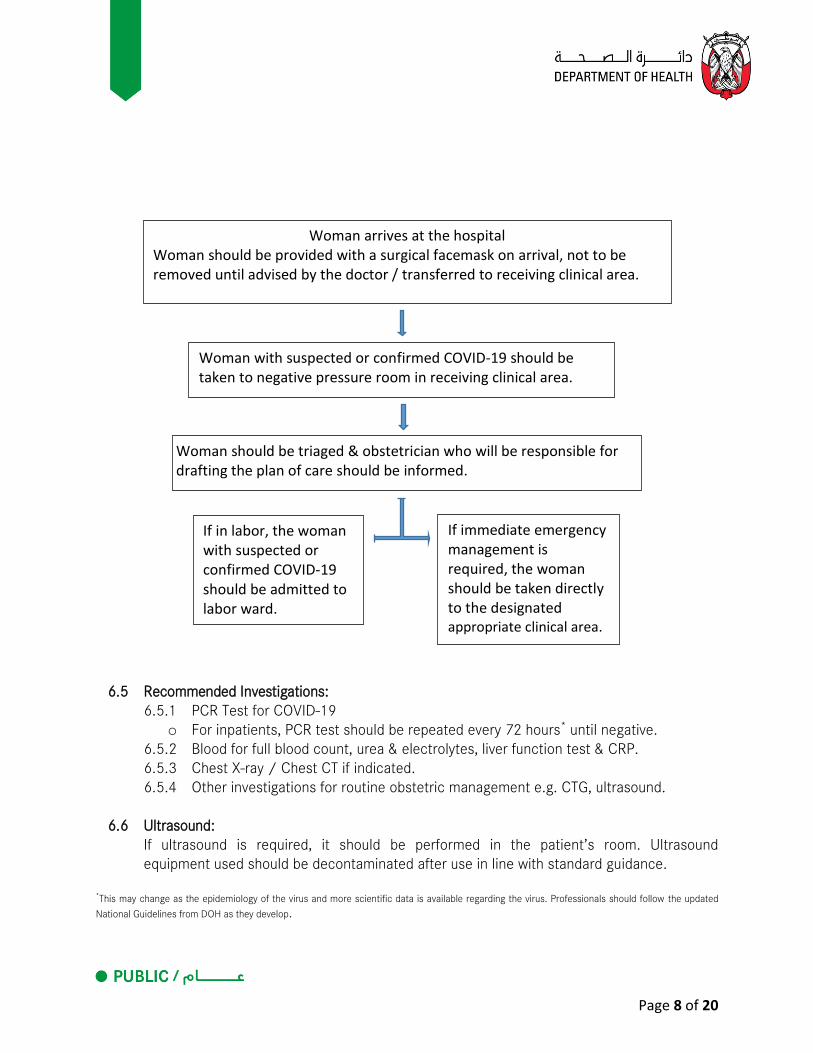
Woman arrives at the hospital Woman should be provided with a surgical facemask on arrival, not to be removed until advised by the doctor / transferred to receiving clinical area.
If in labor, the woman with suspected or confirmed COVID-19 should be admitted to labor ward.
Woman should be triaged & obstetrician who will be responsible for drafting the plan of care should be informed.
If immediate emergency management is required, the woman should be taken directly to the designated appropriate clinical area.
Woman with suspected or confirmed COVID-19 should be taken to negative pressure room in receiving clinical area.
Page 9 of 20
6.7 Therapeutic Options*:
6.7.1 Medications may include Hydroxychloroquine in addition to Lopinavir/Ritonavir as below. These medications may have a place in early therapy to reduce time to clinical improvement. Remdesevir and interferon therapy are additional options in severe cases. Clinicians should follow the updated National Guidelines for Clinical Management & treatment of Covid-19 for details of therapeutic options available.
Disease Severity Medication Duration
Asymptomatic without radiological evidence of pneumonia
No treatment required Monitor for symptoms
14 days
Mild URTI without radiological evidence of pneumonia
No treatment required Monitor for symptoms
14 days
1) Asymptomatic with radiological evidence of pneumonia
2) Mild URTI with risk factors
Lopinivir-Ritonavir (200/50mg) 2 tablets PO BID
7 days
Symptomatic + Pneumonia Use above regimen 10 days
* The medication options will be updated regularly as further studies are available and new medications emerge. Professionals should follow the updated National Guidelines from DOH as they develop.
6.7.2 Bacterial infection should be considered if the white cell count is raised (lymphocytes usually normal or low with COVID-19) and antibiotics should be started.
6.7.3 LMWH should be added on admission and 14 days post transfer or discharge. 6.7.4 Consultation with Intensive Care and Infectious Disease Consultants for coordinated
case by case care of more severe cases. 7. Emergency Management:
7.1 Non-obstetric Emergency When a woman is admitted to hospital with deterioration in symptoms and suspected/confirmed COVID-19 infection, the following recommendations apply:
7.1.1 A multi-disciplinary discussion should be arranged as soon as possible following admission.
7.1.2 The priority for medical care should be to stabilize the woman’s condition with standard supportive care therapies.
Page 10 of 20
7.1.3 COVID-19 care set should be available including labs, radiological investigation, ECG & medications.
7.2 Obstetric Emergency
In the event of obstetric emergency and being suspected or confirmed to have COVID-19, maternity staff must first follow infection prevention and control (IPC) guidance. Once IPC measures are in place, the obstetric emergency should be dealt with as the priority.
8. Women who develop new symptoms of COVID-19 during admission (antenatal, intrapartum or
postnatal) There is an estimated incubation period of 0-14 days (mean 5-6 days); an infected woman may therefore present asymptomatically and develop symptoms later during an admission. In the event of new onset of respiratory symptoms or unexplained fever of or above 37.8 degrees following admission, the woman should be isolated, screened for COVID-19 and appropriate infection control precautions initiated.
9. Intrapartum Care for Women with suspected or confirmed COVID-19
9.1 The woman should be admitted to a designated labor / delivery room.
9.2 A full maternal and fetal assessment should be conducted by a multi-disciplinary team including an obstetric physician, obstetric consultant, charge midwife, anesthetist & neonatologist and should include: 9.2.1 Maternal observations including temperature, respiratory rate and oxygen
saturations. 9.2.2 Confirmation of the onset of labor, as per standard care. 9.2.3 Electronic fetal monitoring using cardiotocograph (CTG) above 26 weeks gestation.
9.3 Efforts should be made to minimize the number of staff members entering the room.
9.4 Maternal observations and assessment should be continued as per standard practice.
9.5 The aim should be to keep oxygen saturation >94%, titrating oxygen therapy accordingly.
9.6 Preparation for Delivery:
9.6.1 Steroids should be given to mothers anticipating preterm delivery where indicated and urgent delivery should not be delayed for their administration (as normal practice).
Page 11 of 20
9.6.2 Magnesium sulfate should be considered for neuroprotection of infants < 32 weeks’ gestation as per current guidance. In severe cases, weigh benefits and risks of magnesium sulfate given the risk of maternal respiratory depression.
9.6.3 The neonatal team should be informed as soon as possible of such admissions. 9.6.4 The resuscitaire (including a dedicated pulse oximeter) and room equipment should
be checked before the mother enters the room. 9.6.5 Commonly used equipment for neonatal resuscitation and stabilization should be
readily available, stored in disposable plastic boxes, stored outside the designated room to avoid taking the full resuscitation trolley into the room.
9.6.6 Only essential staff should be present in the delivery room/theatre. A designated member of the neonatal team should be assigned to attend suspected/confirmed COVID-19 deliveries.
9.7 Partners: 9.7.1 Asymptomatic/COVID-19 negative partners of suspected/confirmed COVID-19
women – mask and hand hygiene of partner in labor. 9.7.2 Symptomatic partners and COVID-19 positive partners of suspected/confirmed
COVID-19 women must not be allowed in hospital.
9.8 Mode of Delivery for suspected or confirmed COVID-19 obstetric cases: 9.8.1 There is currently no evidence to favor one mode of birth over another and,
therefore, the mode of birth should be discussed with the woman taking into consideration her preferences and any obstetric indications for intervention.
9.8.2 The mode of birth should not be influenced by the presence of COVID-19, unless the woman’s respiratory condition demands urgent delivery. Performance of C-Section in women with respiratory failure is a complex situation that requires a multidisciplinary team, availability of high dependency unit and advanced anesthesia and should not be undertaken without all of the above fully available.
9.8.3 Use of birthing pool is contra-indicated for all women with suspected/confirmed Covid-19.
9.9 Analgesia/Anesthesia for suspected or confirmed COVID-19 obstetric cases
9.9.1 Epidural or spinal analgesia or anesthesia is not contraindicated in the presence of SARS-Cov-2. Epidural analgesia could, therefore, be recommended in labor to women with suspected/confirmed COVID-19 to minimize the need for general anesthesia if urgent delivery is needed.
9.9.2 There is no evidence that the use of Entonox is an aerosol-generating procedure (AGP) and therefore its use should be allowed in labor.
9.10 Length of Delivery for suspected or confirmed COVID-19 obstetric cases:
9.10.1 For emergency caesarean section, donning PPE is time consuming & may impact on the decision to delivery interval but it must be done. Women and their families should be told about this possible delay.
Page 12 of 20
9.10.2 An individualized decision should be made regarding shortening the length of the second stage of labor with elective instrumental birth in a symptomatic woman who is becoming exhausted or hypoxic.
9.10.3 Delayed cord clamping is still recommended following birth, provided there are no other contraindications.
10. Newborn Care*
10.1 The baby can be cleaned and dried as normal, while the cord is still intact - or in the case of a preterm baby, standard thermoregulatory measures including the use of a plastic bag should be applied.
10.2 Skin to skin contact should be discouraged immediately after delivery within the delivery room as the latter is considered an aerosol generating environment. The risks of skin to skin care in the context of COVID-19 is unknown at this point in time but are considered to be minimal and outweighed by its benefits. Therefore, it should not be discouraged later in a normal room environment – with mother using a mask and good hand hygiene (see below regarding breast-feeding).
*As more information from scientific research related to this becomes available, the recommendations may change. Therefore, professionals should follow the updates to the National Guidelines from DOH as they become available.
11. Postnatal Management* 11.1 General
11.1.1 Given the current limited evidence and the established benefits, women and healthy infants, not otherwise requiring neonatal care, may be kept together in the immediate post-partum period (subject to the severity of the disease in the mother).
11.1.2 The confirmed/suspected COVID-19 positive mother should go back to an isolation room and managed as per routine care (routine post-natal care set, medications and VTE assessment and appropriated COVID-19 care).
11.1.3 Baby can be roomed with mother if allowed by clinical status, with stringent droplet precautions as below.
11.1.4 If there is limitation in the availability of a negative pressure rooms, mother and baby should be cared for in a room with the option of a portable HEPA filter
11.1.5 Breast-feeding is allowed as benefits outweigh the risks. Nonetheless, good respiratory hygiene and infection control measures (including washing hands and nipples before feeding and the use of mask by mother) should be observed.
11.1.6 In case of transfer to another facility for ICU/HDU care, ambulance transfer should be as per DOH guideline, early arrangement & notification to receiving ICU is required.
Page 13 of 20
11.1.7 If the mother is acutely unwell, an alternative non-quarantined carer/relative should be identified to provide care for the baby at home or in the designated room.
11.1.8 Where appropriate, the baby should be discharged at the earliest possible with the mother or the carer with advice and education to return promptly if the child becomes unwell.
11.1.9 From the limited literature on newborns presenting with any symptoms due to SARS-COV-2, most of them present within 48 hours. Hence, it is prudent to observe infants born to COVID-19 positive mothers for 48 hours in hospital with 4 hourly observations.
11.1.10 Babies requiring admission to the NICU should be transported in a closed incubator by the nurse and doctor wearing appropriate PPE and minimize the number of staff involved.
*These recommendations are subject to change as more scientific research becomes available. Professionals should follow updates of the National Guidelines from DOH.
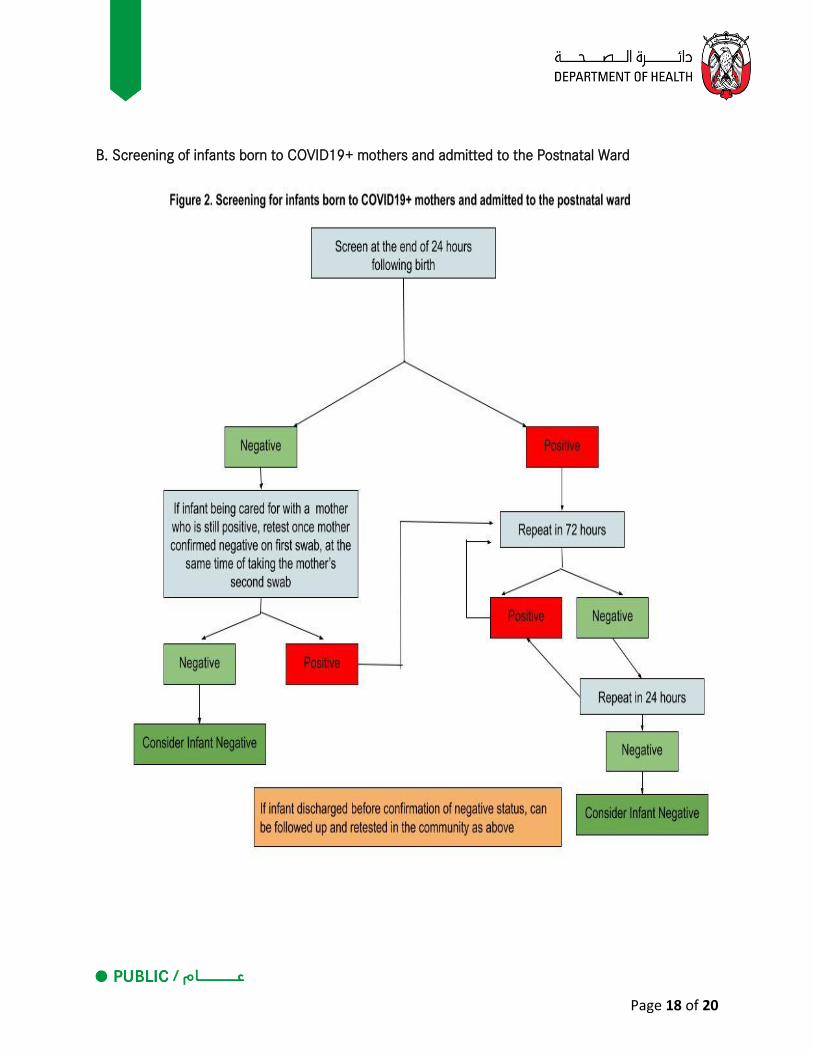
11.2 Testing of Newborns for COVID 19
All infants born to mothers who are positive should be tested for COVID-19 at 24 hours of age; this is to exclude false positives from surface contamination (Appendix).
11.3 Newborn screening and vaccination:
11.3.1 Newborn examination, critical congenital heart disease screening and blood spot screening should proceed as normal as per DOH Guidelines.
11.3.2 Any blood sample should be double bagged until the infant is declared clear of the infection.
11.3.3 Audiology screening – this should be deferred and the baby referred post discharge to an appropriate facility.
11.3.4 Asymptomatic infants should be vaccinated as per existing DOH Guidelines on immunization regardless of maternal COVID status.
11.4 Baby requiring NICU care 11.4.1 The infant should be cared for preferably in the negative pressure isolation room on
NICU. If a room is not is not available, then HEPA filter should be used in a single room.
11.4.2 The baby should be placed in a closed incubator. 11.4.3 Clinical investigations should be minimized whilst maintaining standards of care. 11.4.4 The following should be considered aerosol-generating procedures requiring full
PPE: Intubation, extubation, surfactant administration; CPAP, Bi-PAP, HFNC (flow equal or more than 2 liters/min), NIPPV, HFV,
HFJV; Nebulised therapy; Open airway suctioning.
Page 14 of 20
11.4.5 If the baby requires intubation, then it should be performed, if possible, while baby is in the incubator and the hood is closed (for models with elevatable hoods).
11.4.6 Clinical problems of the baby should be dealt with as per local protocols for babies without Covid-19.
11.5 Neonatal Transport 11.5.1 Transfers should be limited to the minimum. 11.5.2 Non-urgent intra- or inter-hospital transfers should be postponed until the infant is
declared clear of Covid-19.
11.6 Breastfeeding. 11.6.1 If a baby is admitted to NICU or there is temporary separation due to maternal
condition, mothers who intend to breastfeed should be encouraged to express their breast milk with proper hand hygiene to establish and maintain milk.
11.7 Parents and visitors 11.7.1 COVID-19 positive parents should not visit their baby in the NICU. 11.7.2 No visitors should be allowed for suspected or confirmed COVID-19 positive
mothers and babies who have been admitted to the post-natal ward. 11.7.3 Parents of infants admitted to NICU, who have been screened for COVID-19 due to
high risk factors (exposed to positive case, travel history), should not be permitted to visit their baby until they have been confirmed negative. As their initial screening tests may be negative, no visits should be allowed until the end of two weeks of exposure and the test by the end of incubation is negative.
11.8 Neonatal discharge and follow up: 11.8.1 Neonatal follow up through telephone/video consultations should be considered
where possible, to avoid vulnerable infants with chronic lung disease, etc., attending clinics.
Page 15 of 20
12. Reviewers:
Name of Reviewer Profession Organization
Dr. Paul Bosio Consultant SEHA
Jane Kelly Quality SEHA

Page 16 of 20
13. Appendices Appendix 1- Guideline for PPEs for COVID-19 PPEs for managing any patient in the hospital depends on where they are admitted and the results of screening
Red zone Amber Zone Green Zone
Area for admission for all highly suspected or Confirmed COVID 19 positive mothers and/or their infants
Area for admission for all screened asymptomatic mothers or/and their babies pending screening results
Area for admission of all screened asymptomatic patients whose screen is negative for COVID 19
PPE Routine Patient Care: Head Cover Shoe Cover Fluid Resistant gown Surgical Mask Face Shield Gloves Aerosol Generating Procedures and Nasopharyngeal swab collection Same as above but use N95
mask instead of surgical mask
PPE Routine Patient Care: Gown
Surgical Mask
Gloves Aerosol Generating Procedures and Nasopharyngeal swab collection Head Cover
Shoe Cover
Blue Fluid Resistant gown
N95
Face Shield
Gloves
PPE 1. Implement Standard precautions for all patient care. 2. Wear a surgical mask all the time in clinical area.
Page 17 of 20
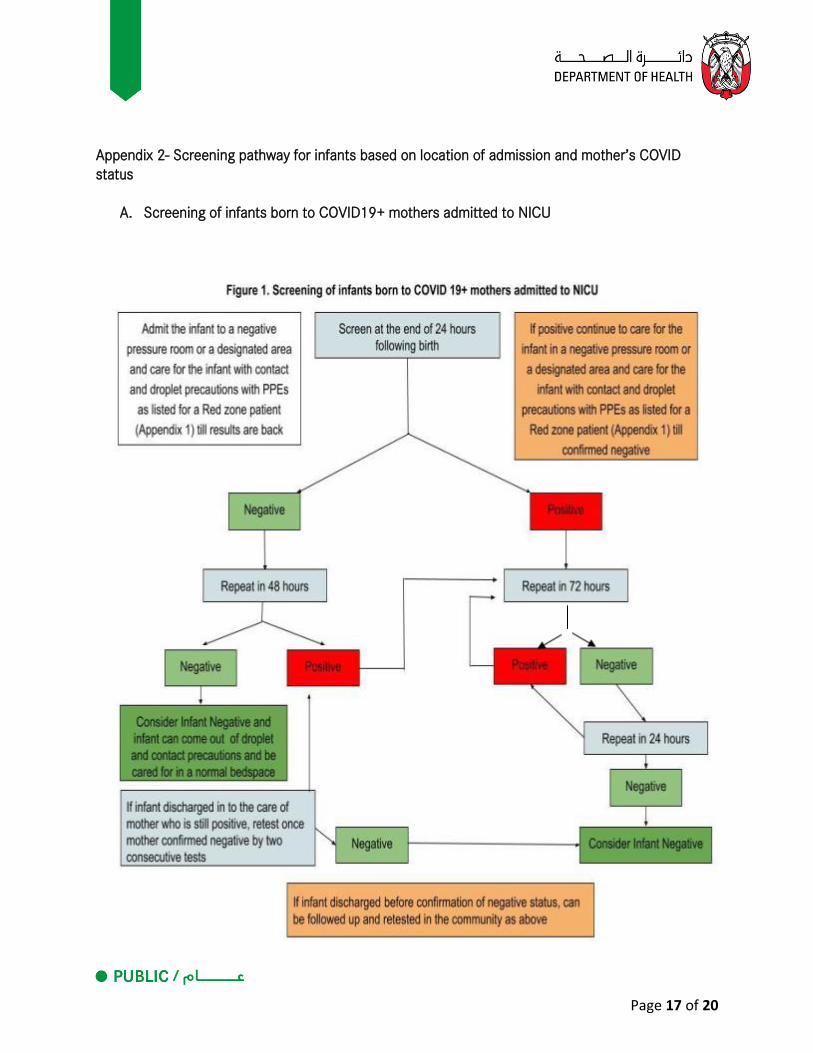
Appendix 2- Screening pathway for infants based on location of admission and mother’s COVID status
A. Screening of infants born to COVID19+ mothers admitted to NICU
Page 18 of 20
B. Screening of infants born to COVID19+ mothers and admitted to the Postnatal Ward
Page 19 of 20
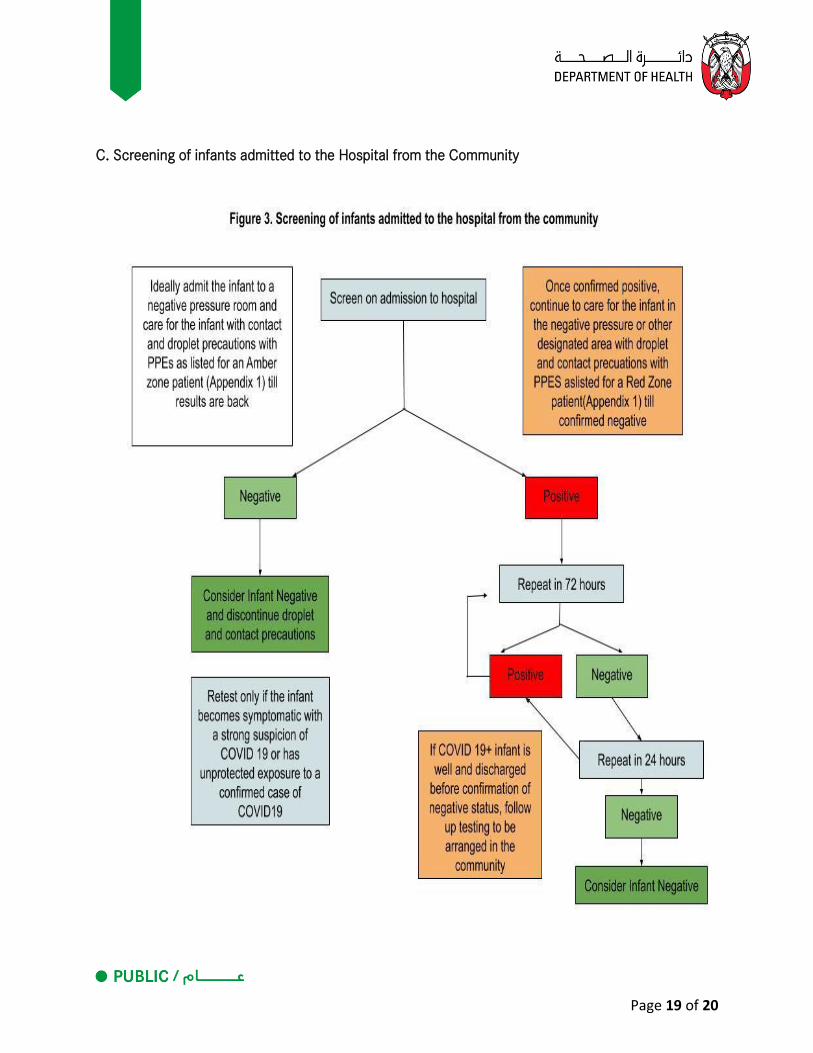
C. Screening of infants admitted to the Hospital from the Community
Page 20 of 20
14. Bibliography 1. National Guidelines for Clinical Management and Treatment of COVID-19. Version4.0: Updated 1st
June 2020. National Clinical Committee for COVID-19 Management. UAE Ministry of Health and
Prevention, Dubai Health Authority and Department of Health Abu Dhabi
2. Considerations for Inpatient Obstetric Healthcare Settings. Centers for Disease Control and
prevention.https://www.cdc.gov/coronavirus/2019-ncov/hcp/inpatient-obstetric-healthcare-
guidance.html
3. Coronavirus (COVID-19) Infection in Pregnancy. Version 10: updated Thursday 4th June 2020.
Guidance for healthcare professionals on coronavirus (COVID-19) infection in pregnancy published
by the RCOG, Royal College of Midwives, Royal College of Paediatrics and Child Health, Public
Health England and Public Health Scotland. https://www.rcog.org.uk/globalassets/documents/guidelines/2020-06-04-coronavirus-covid-19-
infection-in-pregnancy.pdf
4. Rasmussen SA, Jamieson DJ. Caring for Women Who Are Planning a Pregnancy, Pregnant, or
Postpartum During the COVID-19 Pandemic; JAMA. Published online June 5, 2020.
doi:10.1001/jama.2020.8883
5. COVID-19 - guidance for paediatric services. Royal College of Paediatrics and Child Health London.
https://www.rcpch.ac.uk/resources/covid-19-guidance-paediatric-services#working-in-neonatal-
settings. Last accessed 18/03/2020
6. Zeng L, Xia S, Yuan W et al. Neonatal Early-Onset Infection With SARS-CoV-2 in 33 Neonates Born
to Mothers With COVID-19 in Wuhan, China. JAMA Pediatr. 2020 Mar 26. doi:
10.1001/jamapediatrics.2020.0878. [Epub ahead of print]
7. Wang L, Shi Y, Xiao T, et al. Working Committee on Perinatal and Neonatal Management for the
Prevention and Control of the 2019 Novel Coronavirus Infection. Chinese expert consensus on the
perinatal and neonatal management for the prevention and control of the 2019 novel coronavirus
infection (First Edition). Ann Transl Med. 2020;8(3):47. doi:10.21037/atm.2020.02.20
8. Alberta health services neonatal management pathway for management of newborns at risk of
COVID 19 infection. https://www.albertahealthservices.ca/assets/info/ppih/if-ppih-covid-19-
neonatal-management-pathway.pdf. [Last accessed 13th April 2020]
9. American Academy of pediatrics. Initial Guidance: Management of Infants Born to Mothers with
COVID-19.
https://www.aappublications.org/news/2020/04/02/infantcovidguidanhttps://www.aappublicat
ions.org/news/2020/04/02/infantcovidguidance040220ce040220 [Last accessed 15th April
2020]
10. Elisheva Shanes, Leena Mithal, Sebastian Otero et al. Placental Pathology in Covid-19. American
Journal of Clinical Pathology. https://doi.org/10.1093/ajcp/aqaa089. Published 20th May 2020