reduction of overall treatment time in patients irradiated for more than three brain metastases
TRANSCRIPT

Int. J. Radiation Oncology Biol. Phys., Vol. 69, No. 5, pp. 1509–1513, 2007Copyright � 2007 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/07/$–see front matter
doi:10.1016/j.ijrobp.2007.05.014
CLINICAL INVESTIGATION Brain
REDUCTION OF OVERALL TREATMENT TIME IN PATIENTS IRRADIATED FORMORE THAN THREE BRAIN METASTASES
DIRK RADES, M.D.,*y SUSANNE KIECKEBUSCH, M.D.,* RADKA LOHYNSKA, M.D.,z THEO VENINGA, M.D.,x
LUKAS J. A. STALPERS, M.D.,k JUERGEN DUNST, M.D.,* AND STEVEN E. SCHILD, M.D.{
*Department of Radiation Oncology, University Hospital Schleswig-Holstein, Luebeck, Germany; yDepartment of RadiationOncology, University Hospital Hamburg-Eppendorf, Hamburg, Germany; zDepartment of Radiation Oncology, University Hospital,Prague, Czech Republic; xDepartment of Radiotherapy, Dr. Bernard Verbeeten Institute, Tilburg, The Netherlands; kDepartment of
Radiotherapy, Academic Medical Center, Amsterdam, The Netherlands; and {Department of Radiation Oncology,Mayo Clinic Scottsdale, Scottsdale, AZ
Purpose: Patients with multiple brain metastases usually receive whole brain radiotherapy (WBRT). A dose of 30Gy in 10 fractions (10� 3 Gy) in 2 weeks is the standard treatment in many centers. Regarding the poor survival ofthese patients, a shorter RT regimen would be preferable if it provides a similar outcome as that with 10 � 3 Gy.This study compared 20 Gy in five fractions (5 � 4 Gy) within 5 days to 10 � 3 Gy.Methods and Materials: Data from 442 patients treated with WBRT for multiple brain metastases were retrospec-tively analyzed. Survival and local control within the brain of 232 patients treated with 5 � 4 Gy were comparedwith the survival and local control within the brain of 210 patients treated with 10 � 3 Gy. Seven additional po-tential prognostic factors were investigated: age, gender, Karnofsky performance score, tumor type, intervalfrom tumor diagnosis to RT, extracranial metastases, and recursive partitioning analysis class.Results: On univariate analysis, the WBRT program was not associated with survival (p = 0.29) or local control(p = 0.07). On multivariate analyses, improved survival was associated with a lower recursive partitioning analysisclass (p < 0.001), age #60 years (p = 0.001), Karnofsky performance score $70 (p = 0.015), and the absence ofextracranial metastases (p = 0.005). Improved local control was associated with a lower recursive partitioninganalysis class (p < 0.001), Karnofsky performance score $70 (p < 0.001), and breast cancer (p = 0.043). Grade3 acute toxicity rates were not significantly different between 5 � 4 Gy and 10 � 3 Gy.Conclusions: Shorter course WBRT with 5 � 4 Gy was associated with similar survival and local control as‘‘standard’’ WBRT with 10 � 3 Gy in patients with more than three brain metastases. The 5 � 4-Gy regimenappears preferable for most of these patients, because it is less time consuming and more convenient for patientsthan the 10 � 3-Gy regimen. � 2007 Elsevier Inc.
Multiple brain metastases, Shorter course radiotherapy, Overall treatment time, Survival.
INTRODUCTION
Most patients with multiple brain metastases are treated with
whole brain radiotherapy (WBRT) alone. The optimal dose
fractionation of WBRT is still controversial. A total dose of
30 Gy in 10 fractions (10 � 3 Gy) with an overall treatment
time of 2 weeks is considered the standard schedule in most
countries, worldwide. Patients with multiple brain metastases
have an extraordinarily poor survival prognosis. The median
survival of untreated patients is about 1 month (1). Even with
treatment, most patients with multiple brain metastases have
a median life expectancy of only 3–5 months (2). For these
patients, a radiation schedule with a shorter overall treatment
time such as 20 Gy in five fractions (5� 4 Gy) with an overall
Reprint requests to: Dirk Rades, M.D., Department of RadiationOncology, University Hospital Schleswig-Holstein, Campus Lue-beck, Ratzeburger Allee 160, Luebeck D-23538 Germany. Tel:(++49) 451-500-6661; Fax: (++49) 451-500-3324; E-mail: [email protected]
15
treatment time of 5 days would be preferable, because it
would be more convenient for these often-debilitated pa-
tients. Longer palliative RT programs increase the cost of
therapy and often provide similar results to shorter RT pro-
grams, as has been demonstrated for other palliative situa-
tions such as bone metastases (3). However, such a shorter
course program could only be recommended if it provided
similar outcomes as those with 10 � 3 Gy.
Only a few studies have compared ‘‘standard’’ treatment
with 10 � 3 Gy to shorter course programs such as 1 � 10
Gy, 2 � 6 Gy, and 5 � 4 Gy for survival (4–7). One study
suggested a slightly better survival with 10� 3 Gy compared
with 2 � 6 Gy (5), although the other three studies did not
observe a significant difference in survival between 10 � 3
Conflict of interest: none.Received Feb 5, 2007, and in revised form April 16, 2007.
Accepted for publication May 5, 2007.
09
1510 I. J. Radiation Oncology d Biology d Physics Volume 69, Number 5, 2007
Gy and shorter programs (4, 6, 7). Only two studies were
identified that compared 10 � 3 Gy and 5 � 4 Gy, as was
done in the present study (6, 7). However, Borgelt et al. (6)
also included patients who received 40 Gy in 15 fractions.
Chatani et al. (7) presented a series of 70 lung cancer patients
with elevated lactate dehydrogenase. Thus, few studies have
compared 10� 3 Gy and 5� 4 Gy in terms of survival. Also,
we could not identify any study that compared 10� 3 Gy and
shorter course programs regarding local control within the
brain. The present study compared 10 � 3 Gy and 5 � 4 Gy
in a series of 442 patients with more than three brain metas-
tases regarding survival and local control within the brain to
evaluate the outcome of treatment and further refine our
understanding of the prognostic factors.
METHODS AND MATERIALS
A total of 442 patients, who were treated with WBRT alone for
more than three brain metastases between 2001 and 2005, were in-
cluded in this retrospective analysis. The criteria for inclusion were
the presence of more than three brain metastases treated with WBRT
alone (lateral opposed fields), no previous RT to the brain, confirma-
tion of metastases by computed tomography or magnetic resonance
imaging, and administration of dexamethasone during RT. Dexa-
methasone was started at 12–32 mg/d, depending on the symptoms
at presentation. The daily dose was increased if symptoms such as
headache and nausea persisted or occurred. The data were obtained
from the patients, their general practitioners, the treating oncolo-
gists, and the patient files. The patient characteristics are summa-
rized in Table 1.
The survival and local control within the brain of 232 patients
who received 5 � 4 Gy were compared with those of 210 patients
who received 10 � 3 Gy. The time to death and local failure were
measured from the completion of RT. Local failure was confirmed
by computed tomography or magnetic resonance imaging. The
patients treated in The Netherlands received 5 � 4 Gy, and those
treated in Germany or the Czech Republic received 10 � 3 Gy.
Thus, each series from a contributing center represented an unse-
lected series of patients with more than three brain metastases
treated within a certain period.
In addition to the RT schedule, the following potential prognostic
factors were evaluated: age (#60 vs. $61 years; median age, 60),
gender, Karnofsky performance score (<70 vs. $70), primary tumor
type (breast cancer vs. lung cancer vs. other), extracranial metastases
at RT, interval between tumor diagnosis and RT (#8 vs. >8 months,
median interval, 8), and recursive partitioning analysis (RPA) class
(1 vs. 2 vs. 3) (8).
The survival of patients with brain metastases is strongly associ-
ated with the RPA class, which was derived from an analysis of
three Radiation Therapy Oncology Group brain metastases trials
(8). Three RPA classes were defined, taking into account the KPS,
age, presence of extracranial metastases, and primary tumor status
(controlled vs. uncontrolled). RPA class 1 patients had a KPS of
$70 plus three other favorable prognostic factors: age <65 years,
no extracranial metastases, and a controlled primary tumor. RPA
class 2 patients had a KPS of $70, and at least one unfavorable
prognostic factor: age $65 years, extracranial metastases, or an un-
controlled primary tumor. RPA class 3 included all patients with
a KPS <70. The median survival stratified by the three RPA classes
was reported as 7.1, 4.2, and 2.3 months (8).
Patient survival and local control were calculated using the
Kaplan-Meier method (9). The differences between the Kaplan-
Meier curves were determined with the log–rank test (univariate
analysis). The prognostic factors found to be significant (p < 0.05)
or nearly significant (p # 0.06) were included in a multivariate anal-
ysis, which was performed with the Cox proportional hazards model.
The comparisons of the two dose groups (5 � 4 Gy vs. 10 � 3 Gy)
regarding the other potential prognostic factors (Table 1) and the
symptoms at presentation were performed with the chi-square test.
RESULTS
Both treatment groups (patients treated with 5 � 4 Gy vs.
those treated with 10 � 3 Gy) were well balanced for the
other investigated potential prognostic factors (Table 1).
Furthermore, no significant difference was observed between
the two groups (5� 4 Gy vs. 10� 3 Gy) regarding symptoms
at presentation. The most common symptoms were motor
dysfunction (57% vs. 60%, p = 0.76), severe headache
(50% vs. 46%, p = 0.61), nausea/vomiting (25% vs. 22%,
p = 0.57), dysarthria (24% vs. 21%, p = 0.48), severe neuro-
cognitive problems (22% vs. 19%, p = 0.63), seizures (9% vs.
12%, p = 0.35), and vision problems (10% vs. 8%, p = 0.63).
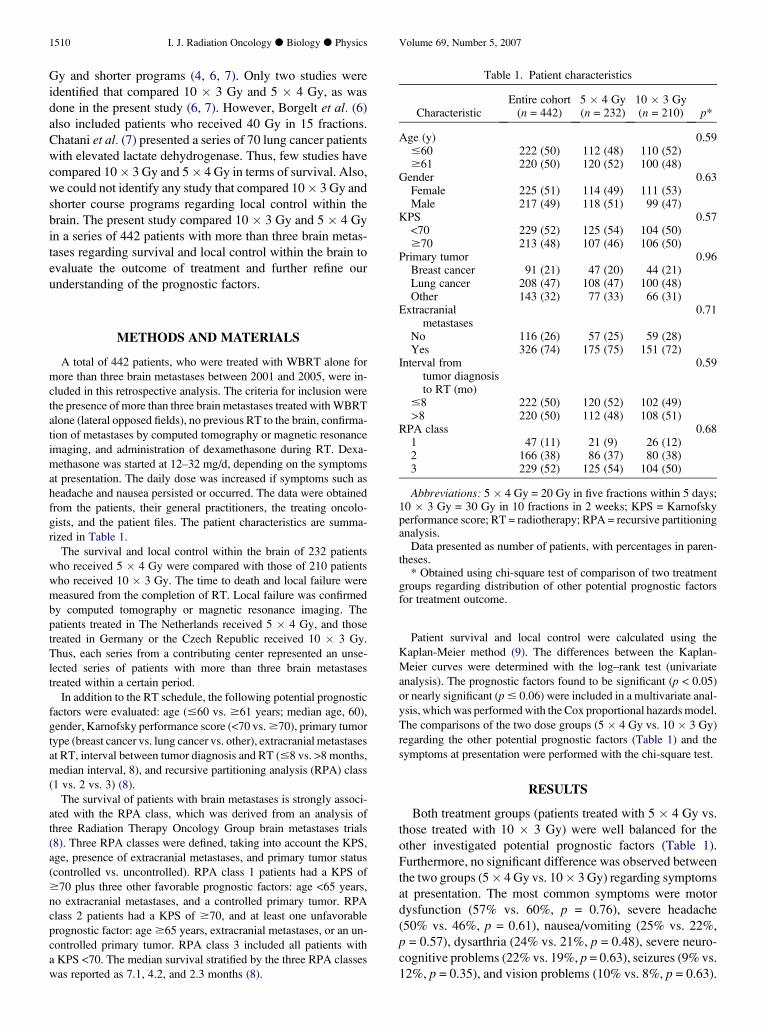
Table 1. Patient characteristics
CharacteristicEntire cohort
(n = 442)5 � 4 Gy(n = 232)
10 � 3 Gy(n = 210) p*
Age (y) 0.59#60 222 (50) 112 (48) 110 (52)$61 220 (50) 120 (52) 100 (48)
Gender 0.63Female 225 (51) 114 (49) 111 (53)Male 217 (49) 118 (51) 99 (47)
KPS 0.57<70 229 (52) 125 (54) 104 (50)$70 213 (48) 107 (46) 106 (50)
Primary tumor 0.96Breast cancer 91 (21) 47 (20) 44 (21)Lung cancer 208 (47) 108 (47) 100 (48)Other 143 (32) 77 (33) 66 (31)
Extracranialmetastases
0.71
No 116 (26) 57 (25) 59 (28)Yes 326 (74) 175 (75) 151 (72)
Interval fromtumor diagnosisto RT (mo)
0.59
#8 222 (50) 120 (52) 102 (49)>8 220 (50) 112 (48) 108 (51)
RPA class 0.681 47 (11) 21 (9) 26 (12)2 166 (38) 86 (37) 80 (38)3 229 (52) 125 (54) 104 (50)
Abbreviations: 5 � 4 Gy = 20 Gy in five fractions within 5 days;10 � 3 Gy = 30 Gy in 10 fractions in 2 weeks; KPS = Karnofskyperformance score; RT = radiotherapy; RPA = recursive partitioninganalysis.
Data presented as number of patients, with percentages in paren-theses.
* Obtained using chi-square test of comparison of two treatmentgroups regarding distribution of other potential prognostic factorsfor treatment outcome.

Reduction of RT time for more than three brain metastases d D. RADES et al. 1511
Progression of intracerebral disease and symptoms during
or directly after RT was observed in 20% and 19% of the pa-
tients, respectively (p = 0.91). Progression of metastatic dis-
ease was confirmed by computed tomography or magnetic
resonance imaging. In the group of patients in whom intrace-
rebral progression was not confirmed, the symptoms, such as
headache, nausea/vomiting, and deterioration of neurologic
function, that occurred during or shortly after RT were con-
sidered to be radiation related. The Grade 3 radiation-related
acute toxicity rate, according to the Common Toxicity Crite-
ria, version 2.0, was 9% in those who received 5 � 4 Gy and
6% in those who received 10� 3 Gy (p = 0.35). The patients
treated with 5 � 4 Gy received higher doses of dexametha-
sone than those treated with 10 � 3 Gy (median, 24 mg/d
vs. median, 20 mg/d).
Patients were followed until death or for 6–22 months
(median, 9 months) in those patients alive at the last follow-
up visit. During the follow-up period, 399 patients (90%) of
the entire cohort died. Of these, 211 (91%) had received 5
� 4 Gy and 188 (90%) had received 10 � 3 Gy. The rate of
patients who died secondary to brain metastases was 52%
(230 of 442) in the entire cohort, 50% (116 of 232) in the 5
� 4-Gy group, and 54% (114 of 210) in the 10� 3-Gy group
(p = 0.58).
The impact of the investigated potential prognostic factors,
including the radiation schedule, on survival is shown in
Table 2 (univariate analysis). The median survival was
9 months in RPA class 1 patients, 5 months in RPA class 2
patients, and 2 months in RPA class 3 patients (Fig. 1). On
univariate analysis, improved survival was significantly asso-
ciated with age #60 years (p < 0.001), KPS $70 (p < 0.001),
lack of extracranial metastases (p < 0.001), and lower RPA
class (p < 0.001). A trend was observed for female gender
(p = 0.06) and breast cancer (p = 0.052). The radiation sched-
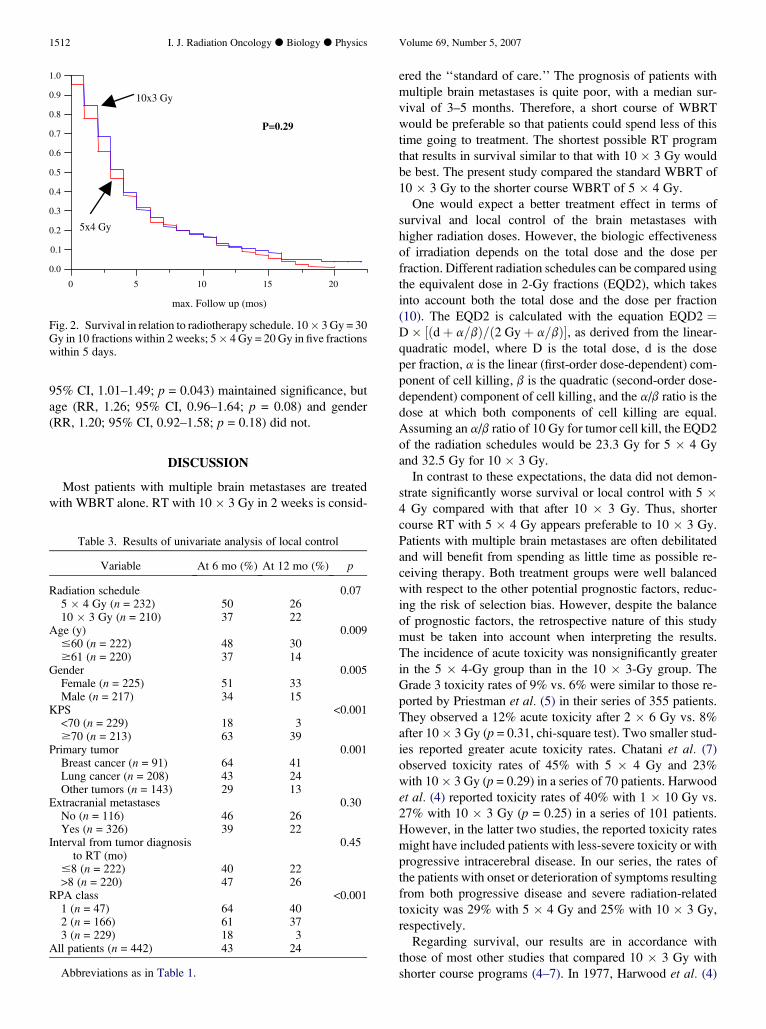
ule had no significant impact on survival (p = 0.29, Fig. 2).
The median survival after RT was 3 months for the entire co-
hort, 3 months after 5� 4 Gy, and 4 months after 10� 3 Gy.
The survival curves for these two dose levels are superim-
posable.
The multivariate analysis of survival included all prog-
nostic factors that were significant or nearly significant
on univariate analysis, but only the RPA class maintained
significance (relative risk [RR], 2.36; 95% confidence in-
terval [CI], 2.00–2.81; p < 0.001). To avoid confounding var-
iables, a second multivariate analysis was performed without
the RPA class. In this second multivariate analysis, age (RR,
1.42; 95% CI, 1.16–1.77; p = 0.001), KPS (RR, 2.13; 95%
CI, 1.15–3.83; p = 0.015), and lack of extracranial metastases
(RR, 1.48; 95% CI, 1.12–1.99; p = 0.005) maintained signif-
icance. Gender (RR, 1.14; 95% CI, 0.91–1.41; p = 0.26) and
tumor type (RR, 1.01; 95% CI, 0.87–1.18; p = 0.91) did not
achieve significance.
On univariate analysis (Table 3), improved local control
was significantly associated with a lower RPA class
(p < 0.001), age #60 years (p = 0.009), female gender
(p = 0.005), KPS $70 (p < 0.001), and breast cancer (p =
0.001). The radiation schedule had no significant impact on
local control (p = 0.07). The median time to recurrence after
RT was 5 months for the entire cohort and 6 months after 5�4 Gy and 4 months after 10 � 3 Gy. Repeat irradiation was
performed in 4 patients initially treated with 5 � 4 Gy and
in no patient initially treated with 10 � 3 Gy. On the multi-
variate analyses performed for local control, RPA class
(RR, 2.27; 95% CI, 1.84–2.84; p < 0.001), KPS (RR, 3.28;
95% CI, 2.48–4.35; p < 0.001), and tumor type (RR, 1.23;
Table 2. Results of the univariate analysis of survival
Variable At 6 mo (%) At 12 mo (%) p
Radiation schedule 0.295 � 4 Gy (n = 232) 24 1110 � 3 Gy (n = 210) 27 12
Age (y) <0.001#60 (n = 222) 32 17$61 (n = 220) 18 4
Gender 0.06Female (n = 225) 29 15Male (n = 217) 21 8
KPS <0.001<70 (n = 229) 6 2$70 (n = 213) 46 22
Primary tumor 0.052Breast cancer (n = 91) 35 18Lung cancer (n = 208) 24 12Other (n = 143) 21 5
Extracranial metastases <0.001No (n = 116) 42 20Yes (n = 326) 19 8
Interval from tumordiagnosis toRT (mo)
0.52
#8 (n = 222) 26 13>8 (n = 220) 24 10
RPA class <0.0011 (n = 47) 70 432 (n = 166) 39 163 (n = 229) 6 2
All patients (n = 442) 25 11
Abbreviations as in Table 1.
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 5 10 15 20
max. Follow up (mos)
P<0.001
RPA 3
RPA 2 RPA 1
Fig. 1. Survival in relation to three recursive partitioning analysisclasses.
1512 I. J. Radiation Oncology d Biology d Physics Volume 69, Number 5, 2007
95% CI, 1.01–1.49; p = 0.043) maintained significance, but
age (RR, 1.26; 95% CI, 0.96–1.64; p = 0.08) and gender
(RR, 1.20; 95% CI, 0.92–1.58; p = 0.18) did not.
DISCUSSION
Most patients with multiple brain metastases are treated
with WBRT alone. RT with 10 � 3 Gy in 2 weeks is consid-
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 5 10 15 20
max. Follow up (mos)
10x3 Gy
5x4 Gy
P=0.29
Fig. 2. Survival in relation to radiotherapy schedule. 10� 3 Gy = 30Gy in 10 fractions within 2 weeks; 5� 4 Gy = 20 Gy in five fractionswithin 5 days.
Table 3. Results of univariate analysis of local control
Variable At 6 mo (%) At 12 mo (%) p
Radiation schedule 0.075 � 4 Gy (n = 232) 50 2610 � 3 Gy (n = 210) 37 22
Age (y) 0.009#60 (n = 222) 48 30$61 (n = 220) 37 14
Gender 0.005Female (n = 225) 51 33Male (n = 217) 34 15
KPS <0.001<70 (n = 229) 18 3$70 (n = 213) 63 39
Primary tumor 0.001Breast cancer (n = 91) 64 41Lung cancer (n = 208) 43 24Other tumors (n = 143) 29 13
Extracranial metastases 0.30No (n = 116) 46 26Yes (n = 326) 39 22
Interval from tumor diagnosisto RT (mo)
0.45
#8 (n = 222) 40 22>8 (n = 220) 47 26
RPA class <0.0011 (n = 47) 64 402 (n = 166) 61 373 (n = 229) 18 3
All patients (n = 442) 43 24
Abbreviations as in Table 1.
ered the ‘‘standard of care.’’ The prognosis of patients with
multiple brain metastases is quite poor, with a median sur-
vival of 3–5 months. Therefore, a short course of WBRT
would be preferable so that patients could spend less of this
time going to treatment. The shortest possible RT program
that results in survival similar to that with 10 � 3 Gy would
be best. The present study compared the standard WBRT of
10 � 3 Gy to the shorter course WBRT of 5 � 4 Gy.
One would expect a better treatment effect in terms of
survival and local control of the brain metastases with
higher radiation doses. However, the biologic effectiveness
of irradiation depends on the total dose and the dose per
fraction. Different radiation schedules can be compared using
the equivalent dose in 2-Gy fractions (EQD2), which takes
into account both the total dose and the dose per fraction
(10). The EQD2 is calculated with the equation EQD2 ¼D� ½ðdþ a=bÞ=ð2 Gyþ a=bÞ�, as derived from the linear-
quadratic model, where D is the total dose, d is the dose
per fraction, a is the linear (first-order dose-dependent) com-
ponent of cell killing, b is the quadratic (second-order dose-
dependent) component of cell killing, and the a/b ratio is the
dose at which both components of cell killing are equal.
Assuming an a/b ratio of 10 Gy for tumor cell kill, the EQD2
of the radiation schedules would be 23.3 Gy for 5 � 4 Gy
and 32.5 Gy for 10 � 3 Gy.
In contrast to these expectations, the data did not demon-
strate significantly worse survival or local control with 5 �4 Gy compared with that after 10 � 3 Gy. Thus, shorter
course RT with 5 � 4 Gy appears preferable to 10 � 3 Gy.
Patients with multiple brain metastases are often debilitated
and will benefit from spending as little time as possible re-
ceiving therapy. Both treatment groups were well balanced
with respect to the other potential prognostic factors, reduc-
ing the risk of selection bias. However, despite the balance
of prognostic factors, the retrospective nature of this study
must be taken into account when interpreting the results.
The incidence of acute toxicity was nonsignificantly greater
in the 5 � 4-Gy group than in the 10 � 3-Gy group. The
Grade 3 toxicity rates of 9% vs. 6% were similar to those re-
ported by Priestman et al. (5) in their series of 355 patients.
They observed a 12% acute toxicity after 2 � 6 Gy vs. 8%
after 10� 3 Gy (p = 0.31, chi-square test). Two smaller stud-
ies reported greater acute toxicity rates. Chatani et al. (7)
observed toxicity rates of 45% with 5 � 4 Gy and 23%
with 10� 3 Gy (p = 0.29) in a series of 70 patients. Harwood
et al. (4) reported toxicity rates of 40% with 1 � 10 Gy vs.
27% with 10 � 3 Gy (p = 0.25) in a series of 101 patients.
However, in the latter two studies, the reported toxicity rates
might have included patients with less-severe toxicity or with
progressive intracerebral disease. In our series, the rates of
the patients with onset or deterioration of symptoms resulting
from both progressive disease and severe radiation-related
toxicity was 29% with 5 � 4 Gy and 25% with 10 � 3 Gy,
respectively.
Regarding survival, our results are in accordance with
those of most other studies that compared 10 � 3 Gy with
shorter course programs (4–7). In 1977, Harwood et al. (4)

Reduction of RT time for more than three brain metastases d D. RADES et al. 1513
compared 10� 3 Gy and 1� 10 Gy in a series of 101 patients
and found no significant difference in median survival (4.4
vs. 4.0 months, p = 0.08). About 20 years later, Priestman
et al. (5) suggested a marginal advantage in median survival
after 10� 3 Gy than after 2� 6 Gy (84 vs. 77 days, p = 0.04)
in a series of 533 eligible patients with symptomatic brain
metastases. Two studies were identified that compared 10
� 3 Gy and 5 � 4 Gy, as was done in the present study
(6, 7). In the study by Borgelt et al. (6), the median survival
ranged from 2.3 to 3.5 months in patients treated with 30 Gy
in 10 fractions, 20 Gy in 5 fractions, or 40 Gy in 15 fractions
(p > 0.05). In the study by Chatani et al. (7), the median sur-
vival was 3.4 months after 10 � 3 Gy and 2.4 months after 5
� 4 Gy, and the 1-year survival rate was 6% and 4%, respec-
tively (p = 0.94). However, both studies that compared 10 �3 Gy and 5 � 4 Gy were different from our study. One study
included a cohort of patients treated with 40 Gy in 15 frac-
tions (6), and the other investigated only lung cancer patients
with elevated lactate dehydrogenase (7). Studies that com-
pared 10 � 3 Gy with shorter course programs regarding
local control within the brain could not be identified in
the available published studies.
In the present study, survival was significantly associated
with RPA class, age, KPS, and a lack of extracranial metas-
tases. These findings are in accordance with data regarding
the survival of patients with brain metastases presented by
Gaspar et al. (8). In that study, age, KPS, and a lack of extra-
cranial metastases were significant on both univariate analy-
sis and RPA. In the present series, RPA class and KPS were
also significantly associated with local control within the
brain. This finding is also in accordance with the survival
analysis reported by Gaspar et al. (8), because local control
is strongly associated with survival. In our series, every sec-
ond patient died secondary to brain metastases. That breast
cancer was associated with better local control than other tu-
mor types has been reported for other palliative situations,
such as bone metastases and metastatic spinal cord compres-
sion (11, 12).
CONCLUSIONS
No significant difference was found between the shorter
course WBRT with 5 � 4 Gy (overall treatment time, 5
days) and the ‘‘standard’’ WBRT with 10 � 3 Gy (overall
treatment time, 2 weeks) regarding survival or local control
within the brain in patients with more than three brain metas-
tases. Thus, 5 � 4 Gy appears preferable, in particular for
patients with a poor estimated survival (RPA class 2 and 3
patients), because it is less time consuming and more conve-
nient for the patients.
REFERENCES
1. Zimm S, Wampler GL, Stablein D, et al. Intracerebral metasta-ses in solid tumor patients: Natural history and results of treat-ment. Cancer 1981;48:384–394.
2. Sundstrom JT, Minn H, Lertola KK, et al. Prognosis of patientstreated for intracranial metastases with whole-brain irradiation.Ann Med 1998;30:296–299.
3. Van den Hout WB, Van der Linden YM, Steenland E, et al. Sin-gle- versus multiple-fraction radiotherapy in patients with pain-ful bone metastases: Cost-utility analysis based on a randomizedtrial. J Natl Cancer Inst 2003;95:222–229.
4. Harwood AR, Simpson WJ. Radiation therapy of cerebral me-tastases: A randomized prospective clinical trial. Int J RadiatOncol Biol Phys 1977;2:1091–1094.
5. Priestman TJ, Dunn J, Brada M, et al. Final results of the RoyalCollege of Radiologists trial comparing two different radiother-apy schedules in the treatment of cerebral metastases. ClinOncol 1996;8:308–315.
6. Borgelt B, Gelber R, Kramer S, et al. The palliation of brain me-tastases: Final results of the first two studies by the RadiationTherapy Oncology Group. Int J Radiat Oncol Biol Phys 1980;6:1–9.
7. Chatani M, Matayoshi Y, Masaki N, et al. Radiation therapy forbrain metastases from lung carcinoma: Prospective randomizedtrial according to the level of lactate dehydrogenase. Strah-lenther Onkol 1994;170:155–161.
8. Gaspar L, Scott C, Rotman M, et al. Recursive partitioning anal-ysis (RPA) of prognostic factors in three Radiation TherapyOncology Group (RTOG) brain metastases trials. Int J RadiatOncol Biol Phys 1997;37:745–751.
9. Kaplan EL, Meier P. Non parametric estimation from incom-plete observations. J Am Stat Assoc 1958;53:457–481.
10. Joiner MC, Van der Kogel AJ. The linear-quadratic approach tofractionation and calculation of isoeffect relationships. In:Steel GG, editor. Basic clinical radiobiology. New York:Oxford University Press; 1997. p. 106–112.
11. Steenland E, Leer J, van Houwelingen H, et al. The effect ofa single fraction compared to multiple fraction on painfulbone metastases: A global analysis of the Dutch BoneMetastasis Study. Radiother Oncol 1999;52:101–109.
12. Rades D, Fehlauer F, Schulte R, et al. Prognostic factors forlocal control and survival after radiotherapy of metastatic spinalcord compression. J Clin Oncol 2006;24:3388–3393.