positioning an iris-clip iol with an anterior loop stitch
TRANSCRIPT
PRETERCAPSULAR CATARACT EXTRACTION WITH CAPSULAR ENCLOSED IMPLANT
To the Editor: I wish to propose a new cataract extraction technique
that can be performed whether or not an intraocular lens (IOL) is implanted. I have termed the technique pretercapsular cataract extraction (PCCE). In Latin, preter means "except."
In PCCE the capsules remain in situ and only the nucleus and cortex are removed. It is thus possible to obtain a virtually completely closed capsular bag in which to enclose an IOL that cannot contact the surrounding intraocular structures.
The surgical technique begins with topical application of phenylephrine, cyclopentolate, and indomethacin to achieve a maximally dilated pupil.
After preparing a superior fornix-based peritomy, a 12-mm scleral groove is made 1.0-1.5 mm posterior to the surgical limbus with a diamond knife.
The anterior capsulotomy is performed under sodium hyaluronate (Healon ®) using a diamond knife. The curvilinear incision, extending about 120-140 degrees, is made peripherally, as near to the lens equator as possible.
A fine spatula is introduced through the capsulotomy incision to separate the anterior capsule from the underlying cortex. With the same spatula the nucleus is separated from the posterior cortex.
After removing the nucleus, a coaxial cannula is introduced into the capsular bag, and the cortex is stripped and removed without aspiration, using a maneuver similar to Simcoe's microerisiphake.
Healon ® is injected into the capsular bag to separate the leaflets. Air should be avoided since it compresses the capsules.
A posterior chamber IOL (Sheets, Shearing short model, Galand, Simcoe short model, Binkhorst mustache) is inserted through the capsular incision and rotated to a horizontal position.
The gupil is constricted with acetylcholine. The Healon in the capsular bag is not evacuated and an iridectomy is not generally performed.
The advantages of PCCE include the following: 1. Surgical maneuvers are performed within a
complete capsular bag, which protects the corneal endothelium, the iris, and the iridocorneal angle.
2. Whether or not a lens is implanted, both capsules remain smooth and lack the folds that could reduce visual acuity.
3. During implant insertion the corneal endothelium is protected by the capsule. Since the loops are securely positioned within the capsular bag, they avoid contact with the ciliary body or the posterior iris surface, and the possibility of synechias between iris and IOL is significantly reduced.
4. The IOL is safely centered. Pupil capture, iris sphincter damage, dislocation, and pseudophacodonesis are unlikely occurrences.
5. Should IOL removal become necessary, an intracapsular extraction using enzymatic zonulysis would be possible.
6. The IOL could possibly have accommodation by moving ahead with ciliary muscle contraction.
Gaetano Alfano, M.D. Avellino, Italy
POSITIONING AN IRIS-CUP IOL WITH AN ANTERIOR LOOP STITCH
To the Editor: I would like to suggest a simple way of positioning an
iris-clip implant (Severin, Shamrock, Boberg-Ans, or similar ones) following a routine intracapsular lens extraction, and show the insertion of an anterior loop stitch.
The aim is to have minimal handling of the cornea by lifting and thus prevent endothelial folding and cell damage. Routine preoperative intravenous mannitol 20%, 20 ml, if there is no contraindication, helps to keep the eye soft.
1. The limbal peritomy and corneal incision is preferred to avoid washing out blood in the anterior chamber. The absence of a conjunctival flap keeps the view of the anterior chamber very clear.
2. A stay suture on the corneal lip is used to lift the cornea when needed.
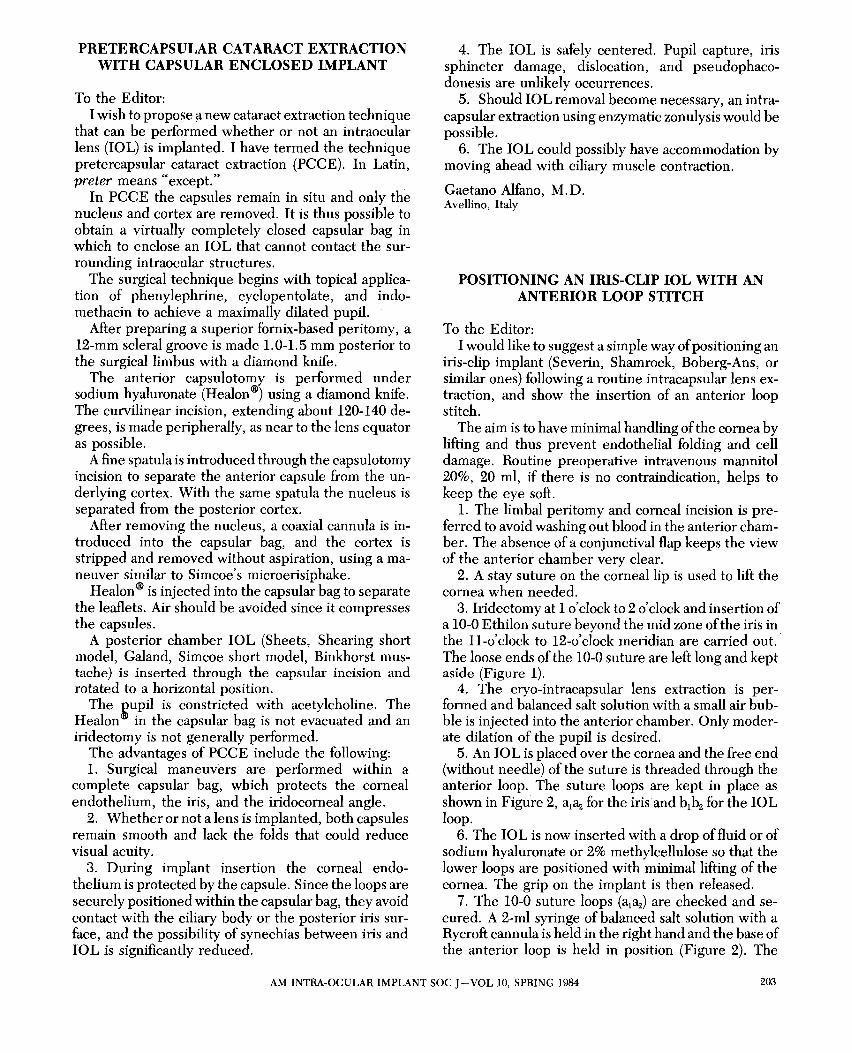
3. Iridectomy at 1 o'clock to 2 o'clock and insertion of a 10-0 Ethilon suture beyond the mid zone of the iris in the ll-o'clock to 12-0'clock meridian are carried out. The loose ends of the 10-0 suture are left long and kept aside (Figure 1).
4. The cryo-intracapsular lens extraction is performed and balanced salt solution with a small air bubble is injected into the anterior chamber. Only moderate dilation of the pupil is desired.
5. An IOL is placed over the cornea and the free end (without needle) of the suture is threaded through the anterior loop. The suture loops are kept in place as shown in Figure 2, al~ for the iris and b1b2 for the IOL loop.
6. The IOL is now inserted with a drop of fluid or of sodium hyaluronate or 2% methylcellulose so that the lower loops are positioned with minimal lifting of the cornea. The grip on the implant is then released.
7. The 10-0 suture loops (al~) are checked and secured. A 2-ml syringe of balanced salt solution with a Rycroft cannula is held in the right hand and the base of the anterior loop is held in position (Figure 2). The
AM INTRA-OCULAR IMPLANT SOC J - VOL 10, SPRING 1984 203
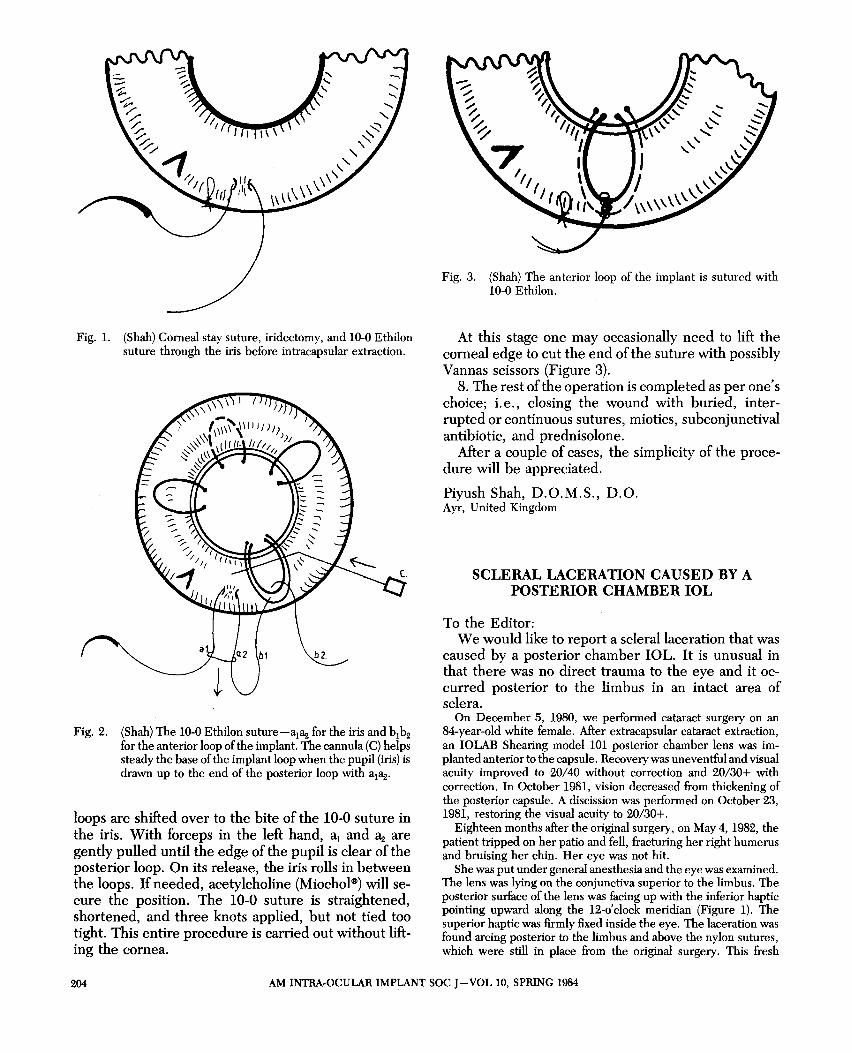
Fig. 1. (Shah) Corneal stay suture, iridectomy, and 10-0 Ethilon suture through the iris before intracapsular extraction.
Fig. 2. (Shah) The 10-0 Ethilon suture-al~ for the iris and b1b2 for the anterior loop of the implant. The cannula (C) helps steady the base of the implant loop when the pupil (iris) is drawn up to the end of the posterior loop with al~'
loops are shifted over to the bite of the 10-0 suture in the iris. With forceps in the left hand, a1 and ~ are gently pulled until the edge of the pupil is clear of the posterior loop. On its release, the iris rolls in between the loops. If needed, acetylcholine (Miochol(J) will secure the position. The 10-0 suture is straightened, shortened, and three knots applied, but not tied too tight. This entire procedure is carried out without lifting the cornea.
Fig. 3. (Shah) The anterior loop of the implant is sutured with 10-0 Ethilon.
At this stage one may occasionally need to lift the corneal edge to cut the end of the suture with possibly Vannas scissors (Figure 3).
8. The rest of the operation is completed as per one's choice; i. e., closing the wound with buried, interrupted or continuous sutures, miotics, subconjunctival antibiotic, and prednisolone.
After a couple of cases, the simplicity of the procedure will be appreciated.
Piyush Shah, D.O.M.S., D.O. Ayr, United Kingdom
SCLERAL LACERATION CAUSED BY A POSTERIOR CHAMBER IOL
To the Editor: We would like to report a scleral laceration that was
caused by a posterior chamber IOL. It is unusual in that there was no direct trauma to the eye and it occurred posterior to the limbus in an intact area of sclera.
On December 5, 1980, we performed cataract surgery on an 84-year-old white female. After extracapsular cataract extraction, an IOLAB Shearing model 101 posterior chamber lens was implanted anterior to the capsule. Recovery was uneventful and visual acuity improved to 20/40 without correction and 20/30+ with correction. In October 1981, vision decreased from thickening of the posterior capsule. A discission was performed on October 23, 1981, restoring the visual acuity to 20/30+.
Eighteen months after the original surgery, on May 4, 1982, the patient tripped on her patio and fell, fracturing her right humerus and bruising her chin. Her eye was not hit.
She was put under general anesthesia and the eye was examined. The lens was lying on the conjunctiva superior to the limbus. The posterior surface of the lens was facing up with the inferior haptic pointing upward along the 12-0' clock meridian (Figure 1). The superior haptic was firmly fixed inside the eye. The laceration was found arcing posterior to the limbus and above the nylon sutures, which were still in place from the original surgery. This fresh
204 AM INTRA-OCULAR IMPLANT SOGJ-VOL 10, SPRING 1984