dnr/dni in the or where are we now? milla muller, c.r.n.a., msn massachusetts general hospital...
TRANSCRIPT
DNR/DNI in the ORWhere are we now?
Milla Muller, C.R.N.A., MSNMassachusetts General Hospital
Department of Anesthesia, Critical Care and Pain Management
Objectives
Review the history of patient autonomy and informed consent
Understand the expectations of the patients and family
Review the ethical, medicolegal and regulatory issues related to the care of patients with active DNR orders.
Foster discussion about optimal care practices of DNR patients perioperatively
ContentWhat is the dilemma related to the care of patients
with active DNR orders perioperatively?What are the current perspectives on end of life
care and perioperative code status?How is this issue effecting our operating rooms?What are the guidelines supported by professional
anesthesia and surgical organizations?What constitutes informed consent during code
discussion?How can this discussion be better optimized and
where do we go from here?
Case 70 yo male Presenting for an angiogram PMH of PVD, MI, HTN, COPD DNR- code status not addressed prior to procedure MAC Pt has an allergic reaction to IV contrast Requires CPR and undergoes prolonged period of
rehabilitation Sues the hospital while in rehab for “wrongful
prolongation of life”
Case
73 yo male presents for a left BKA PMH : severe CAD, PVD, stroke Active DNR order; no intraoperative CPR Spinal anesthetic and sedation After 20 minutes, the patient complains of weakness in
his arms, and difficulty breathing. Within 3 minutes, his blood pressure and heart rate fall, and he abruptly arrests.
In every house where I come I will enter only for the good of my patients, keeping myself far from all intentional ill-doing and…
Beneficence
Autonomy
Nonmaleficence
Justice
Ethical Issues
HISTORY 1960: Development of CPR by closed-chest massage
1974: AMA recognizes that DNR wishes should be documented and communicated to all attending staff
1976: First DNR case to be litigated
1983: CPR became the standard; becoming the only treatment that required and order to be withheld.
1988 : JCAHO requires hospitals to implement policies on resuscitative efforts and end of life care.
1990 Patient Determination Act
1990: AANA publishes guidelines supporting “required reconsideration” of DNR orders
1993: ASA publishes guidelines against automatic suspension of DNR orders
1995: "Physician Orders for Life-Sustaining Treatment" (POLST) form released in Oregon
2008: Massachusetts Acts of 2008 mandates a "POLST Paradigm" demonstration program
February 2010: Implementation of “MOLST” and use of Comfort Care/DNR form for out of hospital arrests.
© 2003 Lippincott Williams & Wilkins, Inc. 2
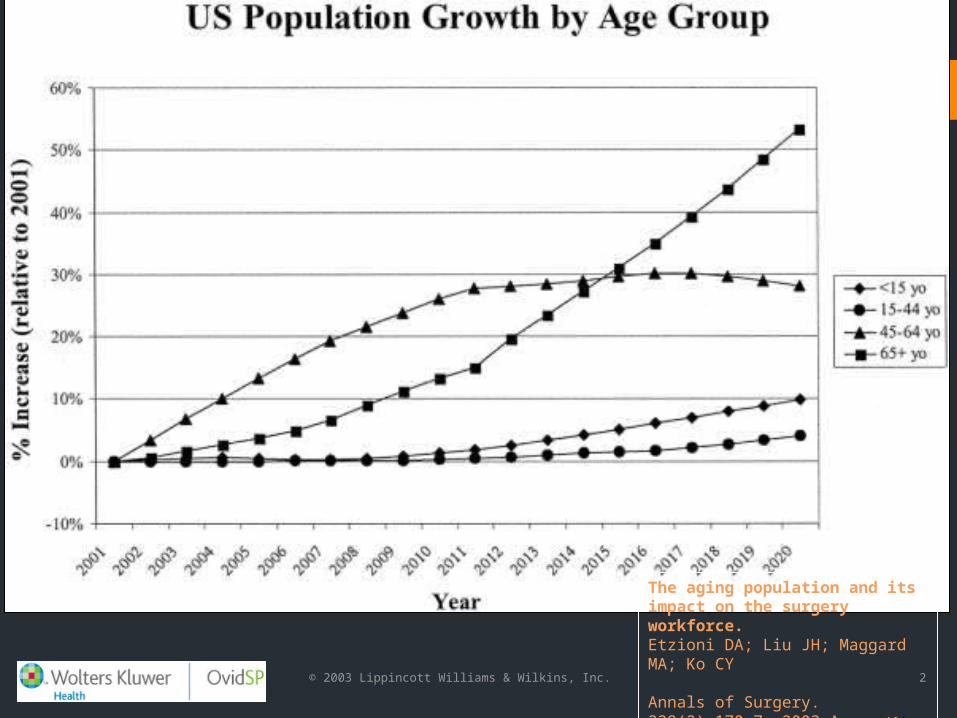
The aging population and its impact on the surgery workforce.Etzioni DA; Liu JH; Maggard MA; Ko CY
Annals of Surgery. 238(2):170-7, 2003 Au g. (1)
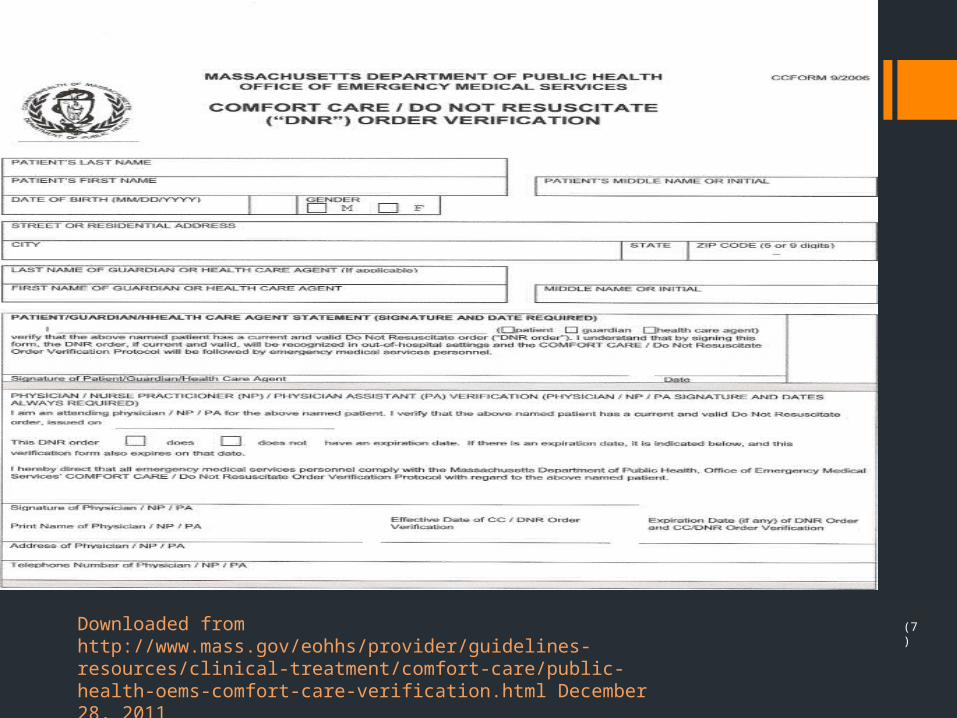
(7)Downloaded from http://www.mass.gov/eohhs/provider/guidelines-resources/clinical-treatment/comfort-care/public-health-oems-comfort-care-verification.html December 28, 2011

The Confusion
Does routine anesthetic management inherently imply resuscitation?
Does automatic suspension of DNR/DNI code status constitute breach of duty or negligence on the part of the anesthetist?
Who has the perioperative code discussion and makes the final decision?
Do anesthesia providers have the right not to take care of a patient with an active DNR order?
What constitutes liability in failing to uphold a DNR order and/or provide informed consent?
Anesthesia is the partial or complete loss of sensation, with or without loss of consciousness as a result of disease, injury or the use of a drug or gas……
Patient Demographics 10-15% of hospitalized patients have a DNR order entered
in house (2)(17)
8-10 % of patients requiring surgery have DNR/DNI orders
(2)(8) with a mean age is approximately 68-79 (5)
In hospital mortality rates for DNR/DNI patients are approximately 3-4x the mortality rate in non-DNR patients (4)
DNR/DNI patients have a 30-50% in hospital mortality rate and an 80% mortality within 2 years of discharge (3) (4)
The percentage of the patient population with DNR/DNI orders is increasing.
DNR in the operating room
Procedures for DNR patients are usually palliative in nature
Surgical risks are weighed against the possibility of improving one’s quality of life
DNR patients have a significantly higher mortality rate within 30 days surgery(2)(5)
Active DNR order: an independent predictor of postoperative mortality vs. sign of confounding comorbidity
Date of download: 1/6/2013Copyright © 2012 American Medical
Association. All rights reserved.
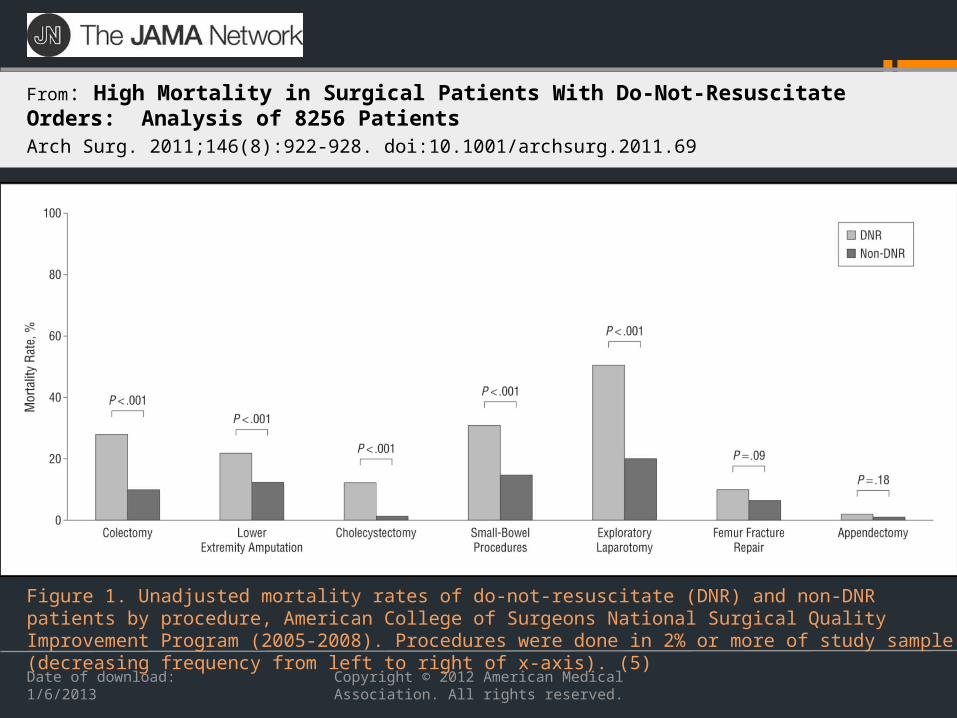
From: High Mortality in Surgical Patients With Do-Not-Resuscitate Orders: Analysis of 8256 PatientsArch Surg. 2011;146(8):922-928. doi:10.1001/archsurg.2011.69
Figure 1. Unadjusted mortality rates of do-not-resuscitate (DNR) and non-DNR patients by procedure, American College of Surgeons National Surgical Quality Improvement Program (2005-2008). Procedures were done in 2% or more of study sample (decreasing frequency from left to right of x-axis). (5)
Figure Legend:
The DNR/DNI code status in the OR: Automatically Suspended?
The nature of the anesthetic requires airway manipulation and inherently implies that the patient will be intubated.
Being under anesthesia implies the need to be resuscitated since it causes cardiopulmonary depression (21).
During a critical event it is difficult to decide if the patient’s arrest is due to iatrogenic or intrinsic causes related to the patient’s comorbidities.
Assuming that the proximate cause (anesthesia) caused the arrest is the safest alternative (15)
Therefore, resuscitation of an arrest due to iatrogenic causes does not fall within the scope of the DNR / DNI order.
Surveys of Anesthesiologists and Surgeons
Anesthesiologists assume DNR/DNI 50-60% of the time (11) 0
Surgeons assume suspension 40% of the time (11)
Recent national survey of cardiothoracic, neurosurgical and vascular surgeons reveals that over 50% would refuse or be reluctant to operate on a patient with a preoperative request to limit life supporting treatments (26)
Both groups are more likely to override DNR orders if the cause of the arrest was iatrogenic or due to “physician error” .
CRNA Perspectives
50% are unsure of departmental policies or if a policy exists
Approximately 67% indicate a policy of automatic DNR suspension
20% have a policy of reconsideration54% favored a policy or reviewing DNR ordersMore than 90% indicated that they would discuss
DNR orders with the patient before surgery40% would resuscitate a patient with a DNR order
Legal Risks
The right of a competent adult patient to refuse medical treatment has its origins in the constitutional right of privacy….and is in the “penumbra” of rights guaranteed by the Fifth and Ninth Amendments to the United States Constitution.
-California Appellate Court, Bartling et al v The Superior Court of Los Angeles County, 1984
Negligence
Plaintiff must prove that the health care provider breached the standard of care
Requires proofs of duty, breach of duty, causation and damages
Battery
Plaintiff must prove intentional and nonconsensual physical contact.
In some states, must prove resulting damages.
Informed Consent
No procedure may be performed on a patient without his or her consent
Consent is founded in the 4th and 14th Amendments to the Constitution and upheld by Common Law
Right to Privacy and Self DeterminationRequires full disclosure of risks Procedures performed without consent or against
expressed wishes of the patient constitute intentional tort of battery
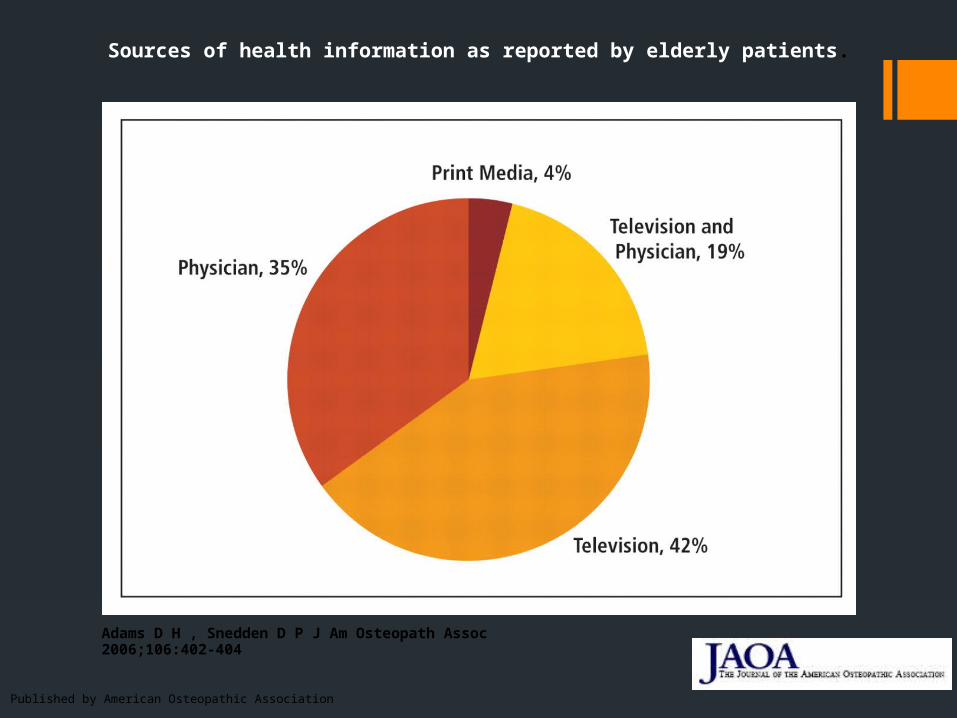
Sources of health information as reported by elderly patients.
Adams D H , Snedden D P J Am Osteopath Assoc 2006;106:402-404
Published by American Osteopathic Association
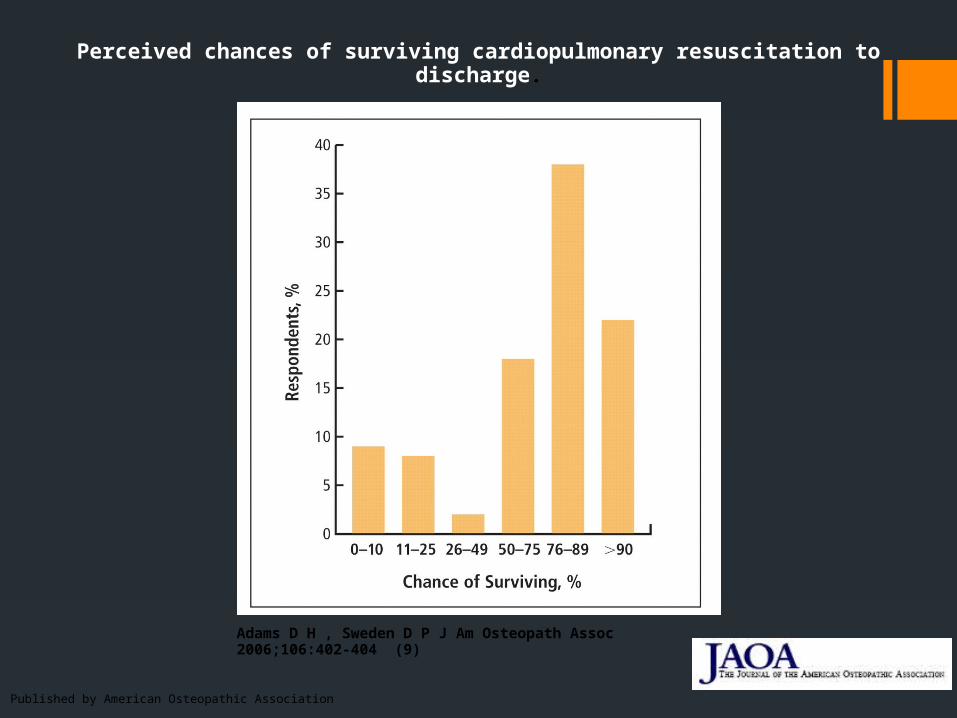
Perceived chances of surviving cardiopulmonary resuscitation to discharge.
Adams D H , Sweden D P J Am Osteopath Assoc 2006;106:402-404 (9)
Published by American Osteopathic Association
CPR Outcomes
Outcome of intraoperative CPR is significantly better for patients undergoing elective rather than emergent procedures (23)
Long term outcome data is variable: 30-40% rate of functional impairment and up to a 70% degree of neurological impairment (29)
Factors associated with poor prognosis: pre-op sepsis and hypotension, age>60, ASA class III or greater, pO2 <50, prolonged resuscitation >10 min , pneumonia, Class III CHF, metastatic
cancer. (19)(3)
Most patients discharged after cardiac arrest experience a reversible event and have no major underlying comorbidities (18)
CPR Outcomes
In hospital survival rate : 34-40%
hospital discharge rate of 14-17% (19) (23)
Intraoperative cardiac arrest averages: 4-8/10,000 (22)(23 (30))
Anesthesia related intraoperative cardiac arrest : 1/10,000 (30)
Intraoperative successful resuscitation rates considerably higher >60 % (23)(8)
Witnessed arrest
Iatrogenic Causes
Often of respiratory etiology
Patient Perspectives
Survey of patients > 60 yo Prior to knowing survival statistics, 41% wanted CPR After knowing the probability of survival, 17% opted for
CPR
Asked about arrest with a chronic illness when life expectancy was < 1 yr 11% wanted CPR After learning the probability of survival only 5% wanted
CPR
Informed Consent and the DNR Discussion
Was the patient competent?Was there full disclosure?Was there understanding?Was there mutual decision making?
“Is there a chance that you will die under the anesthetic? Well, that is the killer question “
AANA Position
The tradition of automatic rescission of an advance directive must be replaced with one of “required reconsideration”
This involves a discussion with the patient or his/her health care proxy
The discussion should be documented in the patient’s chart, including the summary of the agreed plan.
If the CRNA is unwilling to honor the patient’s choices, then transfer of care should be facilitated.
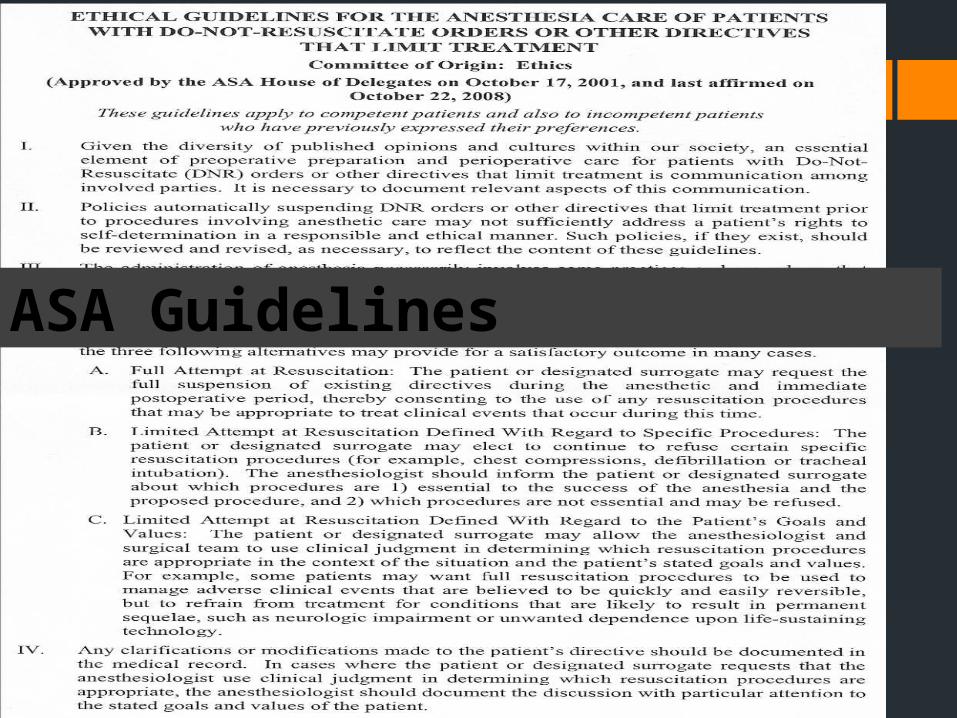
ASA Guidelines
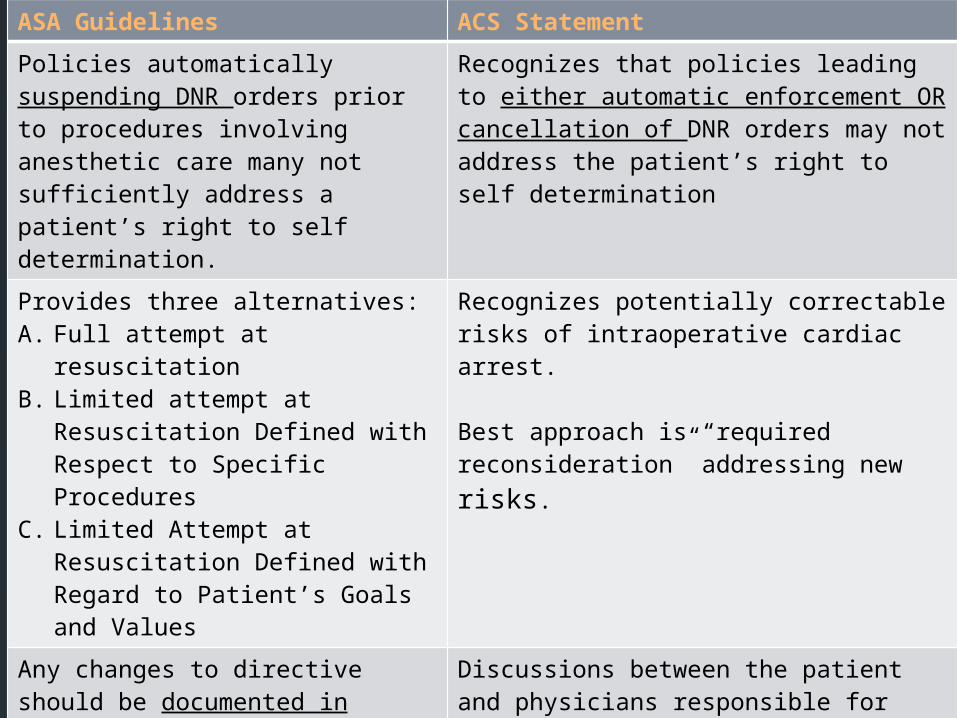
ASA Guidelines ACS Statement
Policies automatically suspending DNR orders prior to procedures involving anesthetic care many not sufficiently address a patient’s right to self determination.
Recognizes that policies leading to either automatic enforcement OR cancellation of DNR orders may not address the patient’s right to self determination
Provides three alternatives:A. Full attempt at resuscitationB. Limited attempt at Resuscitation
Defined with Respect to Specific Procedures
C. Limited Attempt at Resuscitation Defined with Regard to Patient’s Goals and Values
Recognizes potentially correctable risks of intraoperative cardiac arrest.
Best approach is “required reconsideration” addressing new risks.
Any changes to directive should be documented in medical record and plans for postop care should indicate if of when the original, pre-existent directive will be reinstated
Discussions between the patient and physicians responsible for patient’s care should address new risks and approach to life threatening problems should be documented.
Concurrence on these issues by the primary care physician or the surgeon and anesthesiologist is desirable.
Recognizes surgeon’s responsibility in guiding patients with decision making process
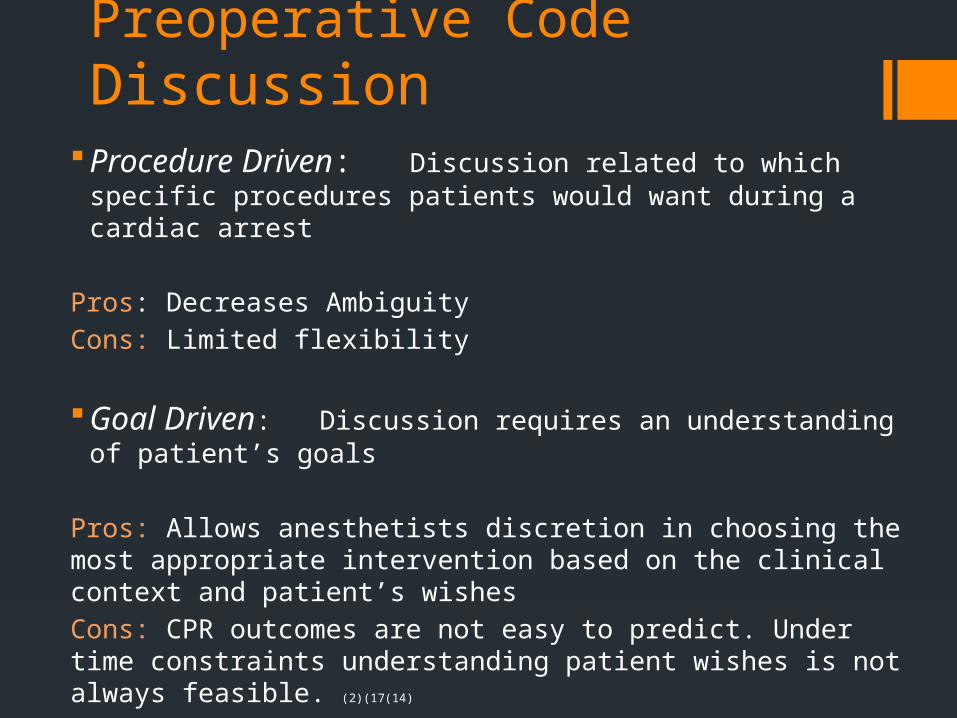
Preoperative Code DiscussionProcedure Driven: Discussion related to which specific
procedures patients would want during a cardiac arrest
Pros: Decreases Ambiguity
Cons: Limited flexibility
Goal Driven: Discussion requires an understanding of patient’s goals
Pros: Allows anesthetists discretion in choosing the most appropriate intervention based on the clinical context and patient’s wishes
Cons: CPR outcomes are not easy to predict. Under time constraints understanding patient wishes is not always feasible. (2)(17(14)
Plan Based on Individual Goals of Care
Procedure Driven Discussion
• Chest compressions
• Defibrillation or electrical cardioversion
• Implantable cardiac defibrillators
• VAD devices
• Endotracheal intubation
• Mechanical intubation
• Non-invasive ventilatory support
• Vasopressors
• Monitoring devices, etc.

Goal Driven Discussion
Requires a discussion between the anesthetist, patient and often family
Is driven by goals and likely outcomes of intervention
Is often a multidisciplinary approach
Documentation (14)
Document if there is a change in code statusDocument that risks vs. benefits have been addressed. Progress note signed by attending physicianDocument patient’s, family’s and surrogates goals and
wishes (14)
Document that the plan has been communicated to all members of care team.
Time limits: when should the order be reinstatedAvoid ambiguity: what and what would not be done
during a cardiac arrest (17)
Practices for Consideration
Understand patient wishes and expectations of their clinical outcome
Provide full disclosure and informed consent
Appreciate your own ethical and practice standards and understand department policies
Foster communication across specialties
DOCUMENT!
Practices for Consideration
Use of DNR directives is increasing
Patients need to understand the implications of a perioperative DNR order and we need to understand their goals and wishes
Discussion of perioperative code status requires multidisciplinary collaboration and documentation
Automatic suspension or continuation of code status disregards patient autonomy and prevents anesthetists from delivering quality care at the end of life.
References (1) Etzioni DA; Liu JH; Maggard MA; Ko CY The aging population and its impact on the surgery workforce. Annals of Surgery. 238(2):170-7, 2003 Aug
(2) Burns, J., et al : Do-not-resuscitate order after 25 years . Crit Care Med 2003 Vol 31, 5 1543-1150
(3) Wenger, N., Pearson, M., Desmond, K., et al. : Outcomes of Patients with Do-Not- Resuscitate Orders: Toward an Understanding of What Do-Not-Resuscitate Orders Mean and How they Affect Patients. Archives of Internal Medicine 155. 19 (October) 1995 2063-2068
(4) Wenger, NS et al Patients with DNR orders in the operating room: surgery, resuscitation, and outcomes. SUPPORT Investigators, Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. J Clin Ethics. Fall 1997; 8 (3): 250-7
(5) Kazaure, H., Roman, S., Sosa, J; High Mortality in Surgical Patients With Do-Not-Resuscitate Orders: Analysis of 8256 Patients. Archives of Surgery 2011; 148 (8): 922-928
(6) Berlin, L. Malpractice Issues in Radiology: Do Not Resuscitate AJR 2000;175 1513-1517
(7)Massachusetts Department of Public Health. Comfort Care/Do Not Resuscitate “DNR” Order Verification Form. Downloaded from http://www.mass.gov/eohhs/provider/guidelines-resources/clinical-treatment/comfort-care/public-health-oems-comfort-care-verification.html December 28, 2011
(8) Scott, T. Gavrin, J. Palliative Surgery in the Do-Not-Resuscitate Patient: Ethics and Practical Suggestions for Management Anesthesiology Clinics 2012 1 (1)
(9) Adams D H , Sweden D P J Am Osteopath Assoc 2006;106:402-404
(10) Morell, E, Brown, B., Qi, R et al The do-not resuscitate order: associations with advance directives, physician specialty and documentation of discussion 15 years after the Patient Self Determination Act . J Med Ethics 2008; 34; 642-647
(11)Clemency, M., Thompson, N., “Do Not Resuscitate” (DNR) Orders in the Perioperative Period-A Comparison of the Perspectives of Anesthesiologists, Internists, and Surgeons. Anesthesia Analgesia : 1994; 78; 651-658
Omnibus Budget Reconciliation Act 1990 Pub. L N. 101-508 (1990)
Cardiopulmonary resuscitation on television. Miracles and misinformation. N Engl J Med 1996; 334:1578-82
American Society of Anesthesiologists. Ethical guidelines for the anesthesia care of patients with do not resuscitate orders or other directives that limit treatment( approved by the House of Delegates on October 13, 1993.) Park Ridge (IL). American Society of Anesthesiologists, 1993
(12) Heyland, D., Frank, C., Groll, D. et al. Understanding Cardiopulmonary Resuscitation Decision Making: Perspectives of Seriously Ill Patients. CHEST 2006; 130 (2): 419-428
(13) Jones, K., Brewer, K,., Garrision H., Public Expectations of Survival Following Cardiopulmonary Resuscitation . Academic Emergency Medicine 2000, 7 (1) 48-53
(14) Weisel, D., et al Guidelines for perioperative do-not-resuscitate policies . Journal of Clinical Anesthesia. 2002 14(6):467-73.
(15) Grimaldo, D., Weiner-Kronish, J., et al A Randomized, Controlled Trial of Advance Care Planning Discussions during Preoperative Evaluations . Anesthesiology 2001 95(1): 43-509
(16) Bernat, J., Grabowski, E., Suspending Do-Not-Resuscitate Orders During Anesthesia and Surgery. Surgical Neurology 1993; 40: 7-9
(17) Troug, R., Waisel., D., Burns, J., DNR in the OR A goal directed approach. Anesthesiology 1999, 90: 289-95
(18)Mark, P.E., Craft, M., An Outcomes Analysis of In-Hospital Cardiopulmonary Resuscitation: The Futility Rationale for Do Not Resuscitate Orders. Journal of Critical Care Vol 12, No 3 (September), 1997: p 142-140
(19)Schultz, S.C., Cullinane, D., et al Predicting in-hospital mortality during cardiopulmonary resuscitation. Resuscitation 1996. Nov; 33(1) ; 13-7
(20)Schepardson, L., Younger S. et al Increased Risk of Death in Patients with Do-not- Resuscitate Orders Medical Care. 37(8) 1999 727-737
(21)Bernat, J., and Grabowski, E., Suspending Do-Not-Resuscitate Orders During Anesthesia and Surgery Surg Neurol 1993; 40:7-9
(22) Cohen, B, and Cohen, P. Do-Not-Resusciate Orders in the Operating Room New England Journal of Medicine 1991; 325: 1879-1882
(23) Juraj, S., Warner, M., et al Predictors of Survival following Cardiac Arrest in Patients Undergoing Non Cardiac Srugery: A Study of 518, 294 Patients at a Tertiary Referral Center Anesthesiology, 2003 99:2 259-269
(24) Becker, L, Aufderheide, T. et al. Primary Outcomes for Resuscitation Science Studies. A consensus statement from the American Heart Association. Circulation 2011. Downloaded January 15, 2012 from http://circ.ahajournals.org/content/early/2011/09/30/CIR.0b013e3182340239
(26) Schwarze, M., Redmann, A., et al Surgeons Expect Patients to Buy-In to Postoperative Life Support Preoperatively: Results of a National Survey Critical Care Medicine 2013 41:1 1-8
27) Pear, R., Medicare rule urges planning for end of life
Similar provision cut from overhaul of health system. The New York Times Dec 26, 2010 Downloaded on January 16, 2013 from http://www.boston.com/news/nation/washington/articles/2010/12/26/new_medicaid_rule_encourages_doctors_to_advise_patients_on_end_of_life_options/
(28) American College of Surgeons: Statement on advance directives by patients: “Do not resuscitate” in the operating room. Downloaded f January 29, 2012 rom http://www.facs.org/fellows_info/statements/st-19.html
(29) Loertscher, L., Reed, D., Cardiopulmonary Resuscitation and Do – Not-Resusciate Orders: A guide for clinicians. The American Journal of Medicine 2009.05.029
(30) Sprung, J., Warner, M., et al Predictors of Surival following Cardiac Arrest in Patients Undergoing Non Cardiac Surgery: A Study of 518,294 patients at a tertiary Referral Center Anesthesiology 2003 99:2. 259-269