district rotation - gcpsgcps.edu.gh/wp-content/uploads/2014/07/newsletter-vol.-2-no.-2.pdfdistrict...
TRANSCRIPT
DistrictRotation
A "Consultative Workshop" took place at the Georgia Hotel in Kumasi from Wednesday the15th to Friday the 17th of November 2006. The participants were members of the ExecutiveBoard of the Ghana College of Physicians and Surgeons (GCPS), some teachers of residentsfrom the Regional and District hospitals and a selection of Fellows of the College. The purposeof the Workshop was primarily to determine the need for and nature of any modification (s) tothe overall programme of postgraduate professional training of the residents by the GCPS. Thedeliberations at the Workshop included:
i) the review of the curricula of all the faculties of the College,ii) brief reports from the teachers of the residents posted to the Regional and District
hospitals and comments on these reports,iii) fine-tuning of the examinations for the Parts I and 2 of the Membership Programme andiv) defining the Fellowship programmes of all the faculties.
Other topics which were discussed included the perennial problem of accommodation for theresidents and the selection of new Training Centres.
The workshop was a great success overall. It was able to highlight areas of the programme thatneed to be modified to improve the training of the residents. It was emphasized by some of theteachers of the residents in the Regional and District Hospitals in particular that changes inattitude in some residents would be desirable to ensure that, on completion of their training, theresidents would become not only well-trained specialists in terms knowledge and acquiredskills but in ethics as well. Other problems mentioned included failure to transfer in a timelymanner the salaries of residents from the teaching hospitals to the Regional and DistrictHospitals. This often led to several days to weeks lost for training by residents who traveled tothe Teaching Hospitals to collect their salaries. This provided opportunities for some residentsto stay way from their new stations using, falsely, the same excuse.
The overall impression of all participants at the workshop was that the system of training of theresidents for a period in stations outside of the teaching hospitals has been beneficial to bothtrainees and trainers and should continue.
Some faculties preferred that their residents should be posted to the outstations after two yearsof training in the Teaching Hospitals and others preferred that the second of the three-yearprogram should be the time when the residents should be posted outside of the TeachingHospitals. Whichever practice was adopted had problems relating to accommodation for theresidents who were returning to the Teaching Hospitals from the Regional and DistrictHospitals.
A similar Consultative Workshop took place at the Georgia Hotel almost five years ago, inJanuary 2002, to determine whether there was a need for a GCPS. The lobby that supportedthe idea carried the day. A lot has obviously happened since that momentous decision wastaken to establish the College. Clearly the continuing need for the newly established Collegewould be "to find solutions by first defining precisely the problems encountered and thoseanticipated. "
This issue of College News has published information on the nature of "Family Medicine"which is taught by a faculty of the same name in the College. It is hoped that this faculty willgrow and provide training for many residents for years to come.
Prof. Alexander Bruce-Tagoe, FRCPath. FWACP, FGCP.Editor.
CPD'sRevision Course in PaediatricsThe Faculties of Child Health of the Ghana College of Physicians and Surgeons (GCPS) andthe West African College of Physicians (W ACP) jointly organized a revision course under thetheme "Revision Course in Paediatrics." The course, which ran from 5th
- 9th June 2006 at theKorle Bu Teaching Hospital, attracted 25 Residents from- both the Ghana College and the WestAfrican College. Lectures delivered included Genetics, Common Renal Diseases, Malaria,Childhood Malignancy, Childhood Tuberculosis, Sickle-cell Disease, Cerebral Palsy andIntellectual Disability, Seizure Disorders, Congenital Heart Diseases, Acquired Heart Disease,Protein Energy Malnutrition and Hepato-biliary Diseases, Paediatric AIDS Management,among others. Participants were also taken through a bedside teaching on N eurodevelopmentalExamination. The facilitators were Profs. S. H. Annobil, Jennifer Welbeck, Bamenla Goka,
-Onike Rodrigues, C. Enweronu-Laryea and Drs. E. Badoe, E. Addo-Yobo, V. Adabayeri, S.Peprah-Douse, N. Adjaye, Theresa Rettig, S. Antwi, A. Edwin and Lorna Renner.
Management of LabourThe Faculty of Obstetrics and Gynaecology organized a Continuing Professional DevelopmentProgramme on "Management of Labour" on 15th and 16th June 2006 at the College Secretariat.Forty-two postgraduate Residents in Obstetrics and Gynaecology and Midwives attended theprogramme. The topics discussed were Physiology of labour, Diagnosis of and fetalmonitoring in labour, Management of 1st stage of labour / partograph (1), Management of 1st
stage of labour / partograph (II), Episiotomy in labour, Pain relief in labour, Management ofthe 2nd stage of labour, Management of the 3rd stage of labour and CPD and obstructed labour.There was also a practical session on Partograph. It was facilitated by Prof. E. Kwawukume,Drs. K. Nkyekyer, J. B. Wilson, S. A. Obed, F. Ahiaku, K. Danso, C. A. Turpin, N. Damaleand Kwame-Aryee.
Update Course in Dermatology and Infectious DiseasesThe Faculties of Internal Medicine of GCPS and W ACP organized an update course in"Dermatology and Infectious Diseases". The three-day programme for postgraduate Residentsand doctors in the health sector was held at the College Secretariat from 26th to 28th June 2006.Among the topics discussed were Atopic. Eczema, Psoriasis, Acne, Dermatology Cancers:Cutaneous T cell lymphomas and Kaposi's Sarcoma, Dermatological manifestations ofSystemic Disorders, Paediatric Dermatology, Skin Diseases associated with pregnancy,Diseases of the Oral Mucosa, Dermatological Treatment, Leishmaniasis, Update onManagement of Malaria, SARS, Diagnosis of Tuberculosis, Avian Influenza, Management ofChronic Hepatitis, Haemorrhagic Fevers and Infections of CNS. Forty-two (42) participantssubscribed to the course. The facilitators were Profs. H. Addo, J. H. Addy, J. Mingle, N. O.Nartey, Drs. M. Lartey, E. Amable, A. Forson, L. Ahadzie, K. Nkrumah and A. Akpalu. Theywere supported by Dr. D. C. Hansen, Associate Professor of Dermatology and D. L. Powell,Assistant Professor of Dermatology, all from the University of Utah School of Medicine, SaltLake City, USA.
Quality Assurance in Laboratory MedicineThe Faculty of Laboratory Medicine has organized a workshop on the theme "QualityAssurance in Laboratory Medicine (Anatomic Pathology & Microbiology)". he one-dayprogramme for postgraduate residents in Laboratory Medicine and Laboratory Teehnicians &Technologists was held on 30th August 2006 at the College Secretariat. Seventeen participantsattended the workshop. Lectures were delivered on Quality Assurance - Media Preparation &Sensitivity Testing, Specimen Collection, Interpretation of Results, Quality As ra ce inAnatomic Pathology - Prospective & Retrospective, and Quality Assurance in Cytopat ology.There were also sessions for practical demonstration. It was facilitated by Prof. T. D. Osafo,M. Newman, Twum Danso, Y. Tettey, E. Wiredu and Dr. R. Gyasi.

, "
Co ege Sets up Endowment FundThe Council of the College is in the process of setting up an Endowment Fund. The object ofthe Endowment Fund will be to augment the resources of the College to further theprofessional and educational training of physicians and surgeons in promoting:
Specialist training in medicine, surgery and related disciplinesContinuous professional developmentResearch and the formulation of health policies
Colleges of this nature are established mainly to raise the expertise of doctors to safeguard thequality of health care given to patients, and to do medical research relevant to health caredelivery. They are independent of official political establishment. This independence makesthem serve only the needs of medicine, and is one reason for setting up an Endowment Fund.There is a board of trustees with the ultimate responsibility for running the fund. The membersof the Board of Trustees are:
Mr. Ato Ampiah (Chairman) M.D., Crystal Auto LimitedMr. Albert Essien Regional Head ofEcobank, W.A.M.Z.Mr. Osei Kwame Agyeman Architect, Casa AssociatiMs. Joyce R. Aryee C.E.O., Ghana Chamber of MinesMr. Edward Addo M.D., Unimax Macmillian LimitedNr. Komla Afeke Dumor Journalist, B.B.C.Mrs. Elizabeth 1. Villars M.D., Camelot Gh. LtdNana Oye-Mansa Yeboaa Dompiahene of AkuapemMr. D.S. Quarcoopome C.E.O., 'Q' Farms LimitedMr. Akenten Appiah-Menka Exec. Chairman, Appiah-Menka ComplexAlhaji Asoma Abu Banda Chairman, Antrak Group of CompaniesDr. H.A. Wemah M.D., Agrovets Limited
The details of the formal inauguration of the Endowment Fund are being worked out.
o oured ·0 al wardsCeremonyThe President of the Republic of Ghana, H. E. John Agyekum Kufuor, has authorized theinstitution of a National Medals Awards Day to honour distinguished and deservingGhanaians in the various Disciplines, Professions and Trades. The list of beneficiaries forawards in the various categories for this year included some Fellows of the College. Theywere:
Prof. E Evans-AnfomProf. F T SaiProf. E A BadoeProf. E Q ArchampongProf. K Frimpong Boateng
Prof. A B AkosaProf J 0 M PobeeProf. Francis NkrumahDr. E N Gyader
The Coordinated Applied Basic Sciences (CABS) Revision Course for the Part I MembershipExaminations of the College was held at the Conference Room of the Ghana MedicalAssociation, Korle Bu, from 31st July to 31 st August 2006. The revision covered areas inAnatomy, Biochemistry, Physiology, Haematology, Chemical Pathology, Pathology,Microbiology, and Pharmacology.
esi en s end training in Re i na. Distri t H s i a.sThe first batch of residents posted to Regional and District hospitals for part of their residencytraining have successfully completed their training' and returned to the teaching hospitals. Thisfalls in line with the College's philosophy that part of the training of residents, for at least oneyear, should take place outside the teaching hospitals. The residents were in the Regional andDi ict hospitals from October. 2005 to September 2006. Another batch of residents left for the
, al and District hospitals in October 2006 and are expected back in the teaching hospitalsin Sctp ember 2007.
" ."
What is Family MedicineBy Dr. De-Anne Martey-Marbell, Chairperson, Faculty of Family MedicineFamily medicine is governed by the concept of "Family Dynamics in Health and Disease"which holds that the family influences the causation of acute and chronic diseases and plays acrucial role in therapeutic success or failure.
The concept of Family Dynamics is derived from the "General System Theory" which positsthat there is a Supra System or a Biosphere made up of society1- community, culture andfamily and a Sub-System made up of the person - personality-organ-organelles - molecules-sub molecules-atoms and sub atoms that constitute the genetic make-up of the individual.
Both the Supra and Sub Systems are forces that impact positively and negatively on theindividual and an imbalance in these forces may provoke a disturbance in the homeostasisprocess of the individual causing a ripple that may pervade the whole system.
The family is defined as a mutually interacting system acting as an emotional unit so that the"Family Relational System" carries more importance towards the solution to a problem thanthe individual input.
On account of all of the above, the unit of care in the discipline is the family rather than theindividual patient. Also the Ethnomedico-cultural model for patient care, which emphasizescultural concepts relevant to health and illness, is fundamental in Family Practice to ensurecomprehensive care for individual patient.
The spectrum of Family Medicine cuts across the various twists and turns of the family lifecycle i.e. from the cradle of the baby to the rocker of the aged and beyond.
Family Practice necessarily has to provide continuing, co-coordinated and comprehensivehealth care for the individual in a holistic manner within the context of his family, environmentand community. The domain of the discipline therefore transcends all specialties, integratingthem into a "new whole".
To be able to provide quality and comprehensive health care across this spectrum of familymedicine, the family physician is trained to be highly skilled and competent over a wide rangeof medical care so that he/she will be able to manage the host of medical problems thatconfront him/her as a first contact and General Duty Medical Specialist. Some of the skillsrequired of the Family Physician include Frontline Diagnostic Skills, Preventive, Therapeutic,Resource Management and Practice Research Skills.
The Family Genogram and Family Circle are examples of, assessment tools which providegeographical information about the family life cycle, risk factors and socio-economic problemsof an index family and help the family physician to gain insight into the task of management.
The Family Physician is therefore the physician who is primarily responsible for providingcomprehensive health care to every individual seeking medical care, and arranging for otherhealth personnel to provide services when necessary, thereby combining breadth of practicewith depth of expertise.
..
Elections 2005Elections for representation on Council and Vice Presidents of the Divisions were held duringthe 2nd Annual General and Scientific Meeting. The following Fellows were elected to thefollowing positions:Council MembersProf. S. Ofosu-AmaahProf. C. C. AdomakohProf. E. D. YeboahProf. E. Q. Archampong
OmmisionOn the back page of the June 2006 issue (Volume 2 Number 1) of College News, the names ofFellows elected to serve on Council from 2005 to 2007 should have included Prof. S. Ofosu-Amaah and Prof. E. D. Yeboah. The Editorial Board of College News sincerely ap logizes WProf•. Ofo.u-Amuh and Yeboah tOf Any distressOf embAffA8§mwt ~im~dby tM OOlj§ .
Vice PresidentsDivision of Physicians - Prof. S. K. OwuDivision of Surgeons - Prof. D. nii-Am
:~ ~ __ ~b'~'~' ~~ ~~ _
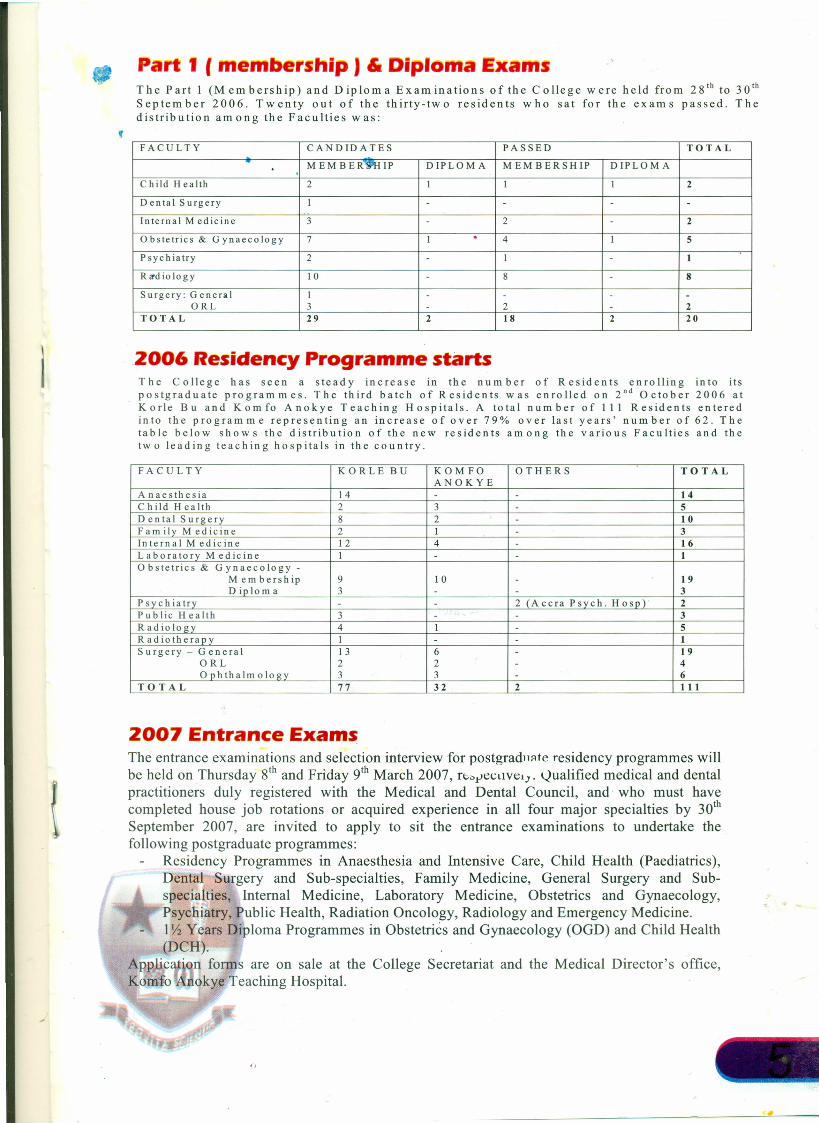
Par 1 Imemb rship) & Diploma ExamThe Part 1 (Membership) and Diploma Examinations of the College were held from zs" to 30th
September 2006. Twenty out of the thirty-two residents who sat for the exams passed. Thedistribution among the Faculties was:,FACULTY CANDIDATES PASSED TOTAL
MEMBER"WHIP DIPLOMA MEMBERSHIP DIPLOMA.Child Health 2 I I I 2
Dental Surgery I - - - -Internal Medicine 3 - 2 - 2
Obstetrics & Gynaecology 7 I . 4 I 5
Psychiatry 2 - I - 1
Raodiology 10 - 8 - 8Surgery: General I - - - -
ORL 3 - 2 - 2TOTAL 29 2 18 2 20
2006 ResidencyProgramme startsThe College has seen a steady increase in the num ber of Residents enrolling into itspostgraduate programmes. The third batch of Residents was enrolled on 2nd October 2006 atKorle Bu and Komfo Anokye Teaching Hospitals. A total number of 111 Residents enteredinto the programme representing an increase of over 79% over last years' number of 62. Thetable below shows the distribution of the new residents among the various Faculties and thetwo leading teaching hospitals in the country.
FACULTY KORLE BU KOM FO OTHERS TOTALANOKYE
Anaesthesia 14 - - 14Child Health 2 3 - 5Dental Surgery 8 2 - 10Family Medicine 2 I - 3Internal Medicine 12 4 - 16Laboratory Medicine I - - 1Obstetrics & G ynaecology -
Membership 9 10 - 19Diploma 3 - - 3
Psychiatry - - 2 (Accra Psych. Hosp)· 2Public Health 3 - - 3Radiology 4 1 - 5Radiotherapy I - - 1Surgery - General 13 6 - 19
ORL 2 2 - 4Ophthalmology 3 3 - 6
TOTAL 77 32 2 111
2007 Entrance ExamsThe entrance examinations and selection interview for postgraduate residency programmes willbe held on Thursday s" and Friday 9th March 2007, rt,,,t'eCtlVely.Qualified medical and dentalpractitioners duly registered with the Medical and Dental Council, and who must havecompleted house job rotations or acquired experience in all four major specialties by 30th
September 2007, are invited to apply to sit the entrance examinations to undertake thefollowing postgraduate programmes:
Residency Programmes in Anaesthesia and Intensive Care, Child Health (Paediatrics),Dental Surgery and Sub-specialties, Family Medicine, General Surgery and Sub-specialties, Internal Medicine, Laboratory Medicine, Obstetrics and Gynaecology,Psychiatry, Public Health, Radiation Oncology, Radiology and Emergency Medicine.llh Years Diploma Programmes in Obstetrics and Gynaecology (OGD) and Child Health(DCH).
A plica ion forms are on sale at the College Secretariat and the Medical Director's office,Komfo ~nokye Teaching Hospital.
T e a owBy Prof E. Q. ArchampongPostgraduate medical education has been on the front burner for the past few years indiscussions on medical education in Ghana. It seems a far cry from the period of the early1970 's following the deliberations emanating from the Commonwealth Conference inMauritius that suggested the development of national medical colleges in West Africa. Thearrival of the Nigerian Postgraduate Medical College, the West African Postgraduate MedicalCollege and now the Ghana College of Physicians and Surgeons represent valuable imprints onthe sands of time.For us in Ghana these developments are so weighty that it is vital and profitable to have themental exercise of reviewing the recent incidents in the march of events in some detail. This inmy view has been the essence of the College-wide consultative workshop that took place inKumasi from the 15th to the 17th of November, 2006. In effect this was a revisit of theConsensus Gathering of professionals involved in postgraduate training that took place inKumasi in January 2002. <I , •
. ' ...The details of this extensive consultative exercise will no doubt be captured in the Collegereport that will be widely distributed. What is of captivating interest for the moment is thechanging professional attitudes and views attending the two meetings held in the same venue inthe city of Kumasi. The debate then was whether a national college was needed in order toadequately prosecute postgraduate medical education in the country. There was indeed muchuncertainty in the atmosphere and naturally this generated some anxiety and even tension inwell-meaning individuals who have been involved in postgraduate medical education for manyyears. There was no doubt that a national college could be more focused and directional in theapproach to solution of the national professional development problems. But there were theweighty concerns about sustainability and commitment of health and educational authorities.Well, volumes of water have tumbled down under the bridge; the torrents have abated andquieted down to ripples. The atmosphere has transformed from anxiety to expectations of hopefor now and the future. If there were sharp exchanges they were about detail, not principle;issues «f time duration of programmes and format of some examinations, not the essence ofcourses or examinations.
Much progress has been achieved. It was heart-warming and instructive to listen to theexperiences of teachers in the outstations, their enthusiasm, commitment and their concernsabout work ethics and their desire for greater involvement with residents and the main tertiarycentres.
There is already progression from instruction and examinations in the basic sciences in allFaculties to work in the clinical and laboratory sciences. It is remarkable that there are noreally serious dissensions in the format of training and assessment in so many Faculties. Thereis also a wide measure of general agreement in the post membership training leading tofellowships.It would be unrealistic to expect that the soaring problems of old would submerge anddisappear so soon. It is clear that with unity of purpose attention can be directed into facing upto these perennial challenges:i. training programmes in the basic sciences and mounting revision courses for all trainees in
face of limited or even dwindling instructional or Faculty capacity;ii. accommodation for residents at most training centres;11. details of subspecialty training at the Fellowship level; andv. the place of research and publications in the training programmes.
With respect to the last mentioned, it is a significant observation that Faculties are veering tothe consensus that while involvement in research and publication of ongoing research findingsby residents should be fostered, dedicated research leading to academic degrees the D/ MSshould be reserved for academic departments, thus releasing senior residents pursuin postmembership work to concentrate on the acquisition of the ever expanding range of skill in thevarious sub specialties. These are promising developments in postgraduate education in Ghana.
The most important challenge for the College still remains the issue of funding. So far theGovernment of the day has demonstrated its commitment through the enor ous capi ainvestment that has gone into the College building rapidly nearing completion. The stre th ofthe College resides in the activities of its Faculty. It is important to ensure that t s remainvigorous and that professional and financial motivation is commensurate.
The Ghana College District Rotation: towards s ill development and serviceto the communityCompiled by E. K. P. Kwarko
In September 2004, the Ghana College of Physicians and Surgeons admitted its first residentsto begin various Diploma and Membership programmes. A year after, a bold step was taken tosend residents out of their traditional training centres into the districts - a part of the design ofthe College training structure. Since this was the very first time it was being tried by theCollege, there were various expectations as well as uncertainties on the minds of residents andthe College.There is no longer any reason to keep guessing on this scheme because the first batch ofresidents, who were posted to accredited health facilities/ institutions, is back to the trainingcentres and their first hand experiences are now known. This piece is an attempt to give a fairidea of the various reports received from the returnee residents, and proceed therefrom to makesome suggestions and recommendations.The district experience can be described as having challenges and strengths that commonly runthrough most of the outposts; some of these will be discussed below .
. The Challengesi. Accommodation for residents - this, perhaps, was the most challenging area of residents'
.life. While a few residents were happy with their "transit quarters" offered them, manyothers had to make do with "make-shift rooms", poorly kept guest houses, and some evenhad to hire their own rooms (at their own expense) while others had to change districtsdue to lack of accommodation.
11. Integration difficulties - for some residents, integration into 'the system' of their newwork environment was either never achieved or it took too long to come. This resulted indifficulties like some allowances not paid to them; their inability to access facilities likelibraries, internet services, telephone exchange services, estate and maintenance services,supplementary feeding services during working hours, and some residents being turnedaway (on some occasions) from wards, theatres, and security gates. In fact, someresidents were treated as though they were "foreign staff'.
iii. Local Administration/ Management constraints - though this is a delicate area, it will beventured into somehow. Differences in management/ administrative style and sheer lackof resources often left some residents frustrated in their quest to deliver good qualityservice. Lack of basic drugs and working implements sometimes made it extremelydifficult to deliver any 'satisfactory' service at all. Other times, the difficulty arose out ofunwillingness to modify (not to change entirely) ways of doing things at the various unitsand even at the central administration level, in other to improve quality of care.
IV. Patient clinical carel management differences - some residents and their supervisorsoccasionally disagreed on clinical management approaches - especially as regards current'evidence-based' ways of patient care. My personal opinion here is that this challengecame about as a result of failure to reach a compromise between over enthusiasticresidents and supervisors who cannot tolerate varied opinion. In some cases somepersonal acrimony may have ensued.
v. Presence at post - while some supervisors were very happy leaving residents 'orphaned'to be in charge of units/ departments, some residents also often took advantage of the lackof proper co-ordination and time-tabling to be absent from their post.
StrengthsI. Undoubtedly, the biggest strength of the district rotation comes from residents getting the
opportunity to try their hands at managing cases/ operating on cases that they wouldn ver have dreamt of handling in their own training centres. This has given a boost to the
.cal and management skills of residents and has elevated their level of confidence.This is one area of strength that the residents have never stopped talking about since theirreturn; and some actually wished they had had some more time to try some more things.
11. S II). ac redited facilities had taken on housemen! interns at the time of the residents'rotafo and these residents attest to the fact that they had benefited a lot from having toteach the house officers both "theory" and "practice".
III. Instead 0 100 ing at the cup as "half-empty", some residents did look at it as "half-full",and have lauded the fact that the district rotation has given them 'eye-openers'. Theycherish the experience of different ways of doing things - especially the opportunity tohave learnt to improvise in the face of genuine difficulty and lack.
RecommendationsThe district rotation has come to stay, and its strengths must be galvanized while its challengesmust be met squarely with pragmatic means.
Perhaps, one way to help the district posting is for the various District Coordinating Councils/District Directorate of Health Services and the Regional Coordinating Councils/ RegionalDirectorate of Health Services, as the case may be, to take part-ownership of the Districtposting programme. For starters, rented accommodation may be procured on standby forresidents so that, where it is difficult for the host facility to bear all the cost residents maysubsidize the rent cost. In the medium to the long term, RCC's/ DCC's and RDHSIDDHS mayput up transit accommodation for residents, even if it means on,cost recovery basis.
A good effort must be made to herald the coming of residents to the host facilities earlyenough, and their needs clearly specified in the rotation letters - so that integration into thedistrict system will be a bit smooth. Here, it may be prudent not to attempt to transfer residents'salaries from their training centres to the districts/ regions. Fuel allowances, however, may bepaid by the districts/ regions; and indeed any other due 'courtesies' must be extended to them.A terminal evaluation document may be prepared to evaluate residents at the end of theirdistrict posting. The content should be known to both' residents and supervisors and thegrading thereof discussed with residents (just like other postgraduate resident field researchevaluations). This may remove victimization and will help residents develop and exhibit theright attitudes while at post.Residents should endeavour to use more tactical ways of suggesting newer evidence-basedmanagement practices to their district supervisors; and they should refrain from showing off,with their acquired skills when they return from the district to their training institutions.Host facilities are encouraged to put in place strategies and incentives that will attractspecialists/ consultants/ supervisors to their service catchment areas, so that they can in turnattract residents and interns who will be of immense service to their service catchment areas.The possibilities of a token reward to district supervisors should be considered on annual basis,and a certificate of commendation to a supervisor may be a good innovation to take furthergood care of visiting residents.Ultimately the Ghana Health Service and the Ministry of Health should put in more effort atshowing 'tangible interest' in the district posting, so that some of the problems relating toaccommodation and transfer of specialists/ consultants/ supervisors to district! regionalfaculties could be tackled at a higher level.Finally, the College and the regional! district facilities must open themselves up to constructivesuggestions so that the district concept grows to meet the service gap between the trainingcentres and the peripheral facilities.The College of Physicians and Surgeons is here to stay; let us all help it to grow.
Fe. ow donates co p en to C
CongratulationsThe Editorial Board of College News congratulates:
Professors Yao Tettey, Department of Laboratory Medicine, and Bamenla Goka,Department of Child Health, on their promotion as associate Professors in the Universityof Ghana Medical School (UGMS).
Dr. Oheneba Boachie-Adjei, a Fellow ofthe GCPS, has donated five (5) usedcomputers to the College. The donationwas made to the Rector on Wednesday 22nd
November, 2006 at the College Secretariat.Dr. Boachie-Adjei is a Board Member ofthe West African Health Foundation in theUnited States and founder and Chairman ofthe Foundation of Orthopedics andComplex Spine (FOCOS).
The Rector in a handshake with Dr. Boachie-Adjei during thepresentation
June and ecember.