disease state primer: ovarian cancer - lumleian...
TRANSCRIPT

Q1 2012 Update
Disease State Primer: Ovarian Cancer
http://www.mayoclinic.com/images/image_popup/c7_ovarian_cancer.jpg

2
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on ovarian cancer?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is ovarian cancer?
• Epidemiology by geography and risk factors
• Presentation, diagnosis, classification
• Current care paradigm and clinical evidence
• Emerging care paradigm
11 • 12
• 13
• 14
• 15 - 20
• 21
III. Clinical Development Pipeline • Clinical development pipeline mapping
• Traditional chemotherapies
• Anti-Angiogenesis agents
• Kinase Inhibitors
• Folate Receptor Targeting Agents
• Ovarian Cancer Vaccines
23 • 24 – 29
• 30 - 31
• 32 – 36
• 37 – 38
• 39 – 41
• 42 – 43
IV. Commercial Landscape • Estimated use in ovarian cancer of branded therapies
• Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
45 • 46
• 47 - 50
• 51
• 52
• 53 – 56
V. Appendix • Table of Acronyms
• More about Lumleian
• 58
• 59 – 61

3
Lumleian offers the requisite scale and depth of life science expertise required for our client’s
most critical investment decisions; We offer universal information and real time knowledge.
• Data Mining
- Regulatory filings
- Scientific literature
- Patent filings
- Company filings
and press releases
• Secondary Data
- Industry pipelines
- Wall Street analysis
- US TRx, pricing,
promotional spend
• Primary Research
- Key opinion leaders
- Practicing physicians
- Reimbursement
Expertise Based
Teams
• Experience
- Academic faculty
- Bio-pharmaceutical
- Equity research
- Strategy consulting
• Expertise
- 30+ clinicians
and Ph.D. scientists
• Analytics
- 5 Ph.D. economists
and statisticians
Universal
Information
Real-Time
Knowledge
• Disease State Primers
- Disease overview
and care paradigm
- Clinical development pipeline
- Commercial landscape
• Functional Drill Downs
- In licensing assessments
- Early and late stage
- Preliminary due dilligence
- Real-time clinical data
• Proprietary Analytics
- Asset valuation
- Epidemiologic forecasts
- Industry benchmarks
• Drug Development
and commercial
- Patient segment valuations
- Promotional response models
• Healthcare professional
and direct to consumer
• Academic and
Research Institutions
- Portfolio optimization
• Early stage
- Out licensing strategy
• Asset valuation
• Transaction support
• Royalty monetization
• Bio-pharmaceutical Companies
- Asset valuation
- Clinical strategy
- In licensing strategy
• Early and late stage
- Portfolio optimization
• Early and late stage
- Preliminary due dilligence
• Life Science Investors
- Asset valuation
- Clinical strategy
- In licensing strategy
Life Science
Client Base
Decision
Support

4
Notes: 1These are a representative sub-set of the publicly available data sources
To ensure real-time knowledge, across disease states, our team of 30+ clinicians and Ph.D.
scientists maintain a comprehensive knowledge management platform, leveraging novel data
mining technology and proprietary analytics.
Data Mining
and Analytics
• Company presentations
• Earnings announcements
• Equity research coverage
• Investor relations transcripts
• Clinical trials
• Conference presentations
• Gene ontology
• Industry pipeline databases
• NIH grants
• Scientific literature & citations
• Business development transactions
• Venture capital investments
• Disease profiles
• Industry publications
• Sales and Rx data
• Treatment algorithms
• Advisory committee transcripts
• FDA and EMA filings
Scientific
& Clinical:
Financial:
Academic
Tech Transfer:
Competitive
Landscape:
• Early stage technologies
• Intellectual property filings
Business
Development:
Regulatory:
• Leverage data mining
technology to access
novel data sources
• Standardize, collate,
and link data sources
• Execute Lumleian’s
proprietary analytical
models
Universe of Public
Information1
• 30+ clinicians and
Ph.D. scientists
- Focused by area
of expertise
• 5 Ph.D. economists
and statisticians
Expert Validation
and Decision Support

5
Our efficient platform and our expertise based teams enable us to both deliver the highest
quality product and tailor our offer, to specific client needs: Either custom decision support or
more standardized research and analytics, e.g. disease state primers.
Decision
Support
• Clinical strategy
• Portfolio optimization
- Pre-Clinical
- Clinical
• Transaction support
- In licensing
- Out licensing Disease
State Primers
Proprietary
Analytics
• Asset valuation
• Epidemiologic forecasts
• Industry benchmarks
- Commercial
- Clinical Development
• Patient segment
valuations
• Promotional
response models
- Healthcare professional
- Direct to consumer
• Royalty monetization
Functional
Drill Downs
• Real-time clinical
data
- Trial strategies
- Results
• In licensing
assessments
- Pre-clinical
- Clinical
• Preliminary
due dilligence
- Scientific
- Clinical
- Commercial
• Disease overview
and care paradigm
• Clinical development
pipeline
• Commercial
landscape Customized
Standardized

6
What information is included in a disease state primer?
• Lumleian’s objective and fact based perspective on the relative attractiveness of investing in a given disease state
• Disease overview and care paradigm - Etiology, Diagnosis and patient segmentation, Global epidemiology, Treatment algorithm, Clinical evidence, Emerging care paradigm
• Clinical Development Pipeline - Validated industry pipeline for all assets in clinical development, Select mechanism of action profiles, trial designs and evidence
• Commercial landscape - Global, US, EU, Japan market and brand revenue, Pipeline forecasts, US growth decomposition, Promotional spend and messaging
What disease states are planned for 2012? • Autoimmune: Inflammatory Bowel Disease, Lupus, Multiple Sclerosis, Psoriasis, Rheumatoid Arthritis
• Cardiovascular: Hyperlipidemia
• Central Nervous System: Alzheimer’s Disease, Depression, Pain, Schizophrenia
• Endocrine: Type II Diabetes, Obesity
• Infectious Disease: Gram Negative Bacteria, Hepatitis C Virus
• Oncology: Breast, Colorectal, Leukemia(s), Lung, Lymphoma(s), Melanoma, Ovarian, Pancreatic, Prostate
• Pulmonary: Chronic Obstructive Pulmonary Disease, Idiopathic Pulmonary Fibrosis
Can we create custom disease state primers for customers? • Yes, based on the expertise of our team of 30+ clinicians and Ph.D. scientists, 5 Ph.D. economists and statisticians we can create a
sustome primer in appoximately 3 to 4 weeks
• We can supplement the primers with deeper analysis to help customers reach a deeper understanding of critical issues e.g. KOL
interviews, Financial Models, Survey Conduction and Analysis, Pre-Clinical Asset Assessment
• We are also developing deep drills by function, e.g. Discovery, Clinical development, Business development, Commercial
Why did we create our disease state primers? • We were frustrated by having to repeatedly validate, standardize, and collate pipeline and commercial data
• Portfolio optimization requires a standard framework to compare “apples to apples” investment decisions across disease states
• Our primers began as a training tool; We require every decision scientist create one from scratch before supporting clients
What is a Lumleian’s disease state primer?

7
Disease
Overview and
Care Paradigm
• Ovarian cancer is an aggressive gynecologic cancer with a high mortality rate, and an overall 5-year survival rate of
45%; ~15K patients die annually in the US from ovarian cancer
• Due to the lack of early-stage symptoms and a corresponding delay in diagnosis, ovarian cancer is the fifth most
common cause of cancer death in women
• All ovarian cancer patients undergo the same surgical procedure, which involves the removal of the uterus, ovaries,
and fallopian tubes
• Ovarian cancer is a highly chemo-sensitive cancer, and is typically treated aggressively in all stages, usually starting
with an IV regimen of paclitaxel and carboplatin/cisplatin
Clinical
Development
Pipeline
• As of Q1 2012, Lumleian validated 81 assets in development for ovarian cancer
• The vast majority of the ovarian cancer pipeline is comprised of next-generation chemotherapeutic agents - DNA binders, microtubule destabilizers, and topoisomerase inhibitors are all validated classes of agents that dominate the
ovarian cancer pipeline, owing to the chemo-sensitive nature of this tumor
• A number of novel, targeted drug classes are being pursued, including anti-angiogenesis agents, kinase inhibitors,
tumor vaccines and immunotherapies - Numerous vascular-targeting agents are in development, including Roche’s Trebananib, Sanofi’s Aflibercept,Takeda’s
Ramucirumab, ImClone’s Vargatef, and Exelixis’ XL999
- Despite early positive data supporting Roche’s Avastin, disappointing Phase III survival data paired with significant side effects
have drawn into question whether anti-VEGF approaches will be a viable approach for ovarian cancer
- Several clinical-stage programs are directed at intracellular kinases involved in cell signaling, proliferation, and cell cycle
transcription factors, including Roche’s Tarceva and AstraZeneca’s Iressa; clinical trials are underway and it remains to be seen
if these will provide a significant advantage over existing chemotherapy regimens
Commercial
Landscape
• Systemic chemotherapy dominates the treatment paradigm for both early- and late-stage ovarian cancer
• Lilly’s Gemzar and Sanofi’s Taxotere are the key branded drugs for the treatment of both early- and late-stage
disease; additionally, BMS’ Taxol (paclitaxel) is still used despite the availability of generics
• Generic formulations of carboplatin, cisplatin, and doxorubicin are widely used in chemo regimens
Source: www.clinicaltrials.gov, Evaluate Pharma, BioPharm Insight, American Cancer Society: Cancer Facts and Figures 2011. Atlanta, Ga,
American Cancer Society, 2011, S.A. Cannistra, R.C. Bast Jr., J.S. Berek et al. Progress in the management of gynecologic cancer: consensus
summary statement. J Clin Oncol, 21 (Suppl. 10) (2003), pp. 129–132
Executive Summary: Ovarian cancer refers to a malignant growth that arises in the ovaries, most
often in the epithelial layer; this malignancy commonly goes undiagnosed until later stages,
resulting in aggressive chemotherapeutic treatment and a high mortality rate.

8
Source: www.clinicaltrials.gov, http://www.cancer.gov/cancertopics/types/ovarian, Company press releases, Cannistra SA, et al. Progress in the
management of gynecologic cancer: consensus summary statement. J Clin Oncol, 21:10 (2003), Lutz AM, et al. Early diagnosis of ovarian
carcinoma: is a solution in sight? Radiology 259:2(2011),
Key Questions
• Will agents currently in development provide distinct clinical benefits over the generic drugs that have become
entrenched as first-line therapies? - Novel formulations of established therapies, such as conjugation of chemotherapies to molecules which specifically target
tumor cells, may demonstrate greater efficacy while reducing overall toxicity; promising examples include EC-145 and
Abraxane
• Will mechanistic understanding of an agent’s effects in other tumor types be transferable to ovarian cancer?
• Can molecular diagnostic screening tools facilitate the selection and treatment of patients with specific
biochemical profiles? - To date, the kinase inhibitors which have revolutionized the treatment of other cancer indications have not affected
ovarian cancer treatment; this may change as the molecular basis of ovarian cancer becomes better understood, and the
selection of targeted agents becomes more disease-specific
- Established links between specific mutations and the therapeutic efficacy of targeted agents will lead to increased
sequencing of tumors as part of the treatment selection process
Lumleian’s
Perspective
• Ovarian cancer will remain an enduring unmet need, predominantly due to the lack of routine diagnostics with
the ability to detect the disease at an early stage - Although levels of tumor antigens such as CA-125 and OVA can be reliable indicators of therapy effectiveness and tumor
progression, these antigens are poor diagnostic tools for the detection of early-stage ovarian cancer
- Development of a reliable test for early-stage ovarian cancer could significantly change the treatment paradigm by shifting
the market in ovarian cancer treatment to different agents, and by increasing our understanding of ovarian cancer
development
• Due to the depth of the current development pipeline, the treatment paradigm is likely to evolve over the next
five to ten years, based on next-generation chemotherapeutics, as well as the probable launch of novel
approaches to treat the disease - Current approaches to treating ovarian cancer have severe side effects, adversely impacting the quality of life; novel
formulations of chemotherapies may increase efficacy while decreasing the toxicity of systemic treatments
- Insights from other cancer indications, such as the link between specific mutations and treatment efficacy, may inform
future ovarian cancer trials and treatments
• As evidenced by Roche’s Avastin, targeted therapies may encounter difficulty demonstrating a clinically
meaningful benefit in this patient population - Due to the late diagnosis of most ovarian cancers, these tumors are difficult to treat
- Significant advances in ovarian cancer treatment are most likely to come from development of diagnostics and better
understanding of ovarian tumor pathology
What are the key questions for 2012?

9
0
1
2
3
4
5
Level of Unmet Need Likelihood of Technical Success Regulatory Impetus Commerical Attractiveness Required Investment
Sources: Bharwani et al. Ovarian Cancer Management: the role of imaging and diagnostic challenges. Eur J Radiol (2011), www.seer.cancer.gov,
Schorge et al. SGO White Paper on ovarian cancer: etiology, screening and surveillance. Gynecologic Cncology 119:1 (2010)
Greenfield investment in clinical development for ovarian cancer is a high risk vs. moderate
rewards proposition; probability of technical success is low, and the market is small (though
growing), but there is high unmet need, potential Orphan Drug status and strong patient advocacy.
Average
Ovarian Cancer: Relative Attractiveness of Greenfield Investment in Late Stage Clinical Development
High
Low
Required
Investment
Phase III Investment
- Phase III trials require
at least a 1000 patient
trial
- Expensive monitoring
costs during trial
Commercial Spend
- Modest commercial
spend; highly data
driven
- Focused audience of
gyn-oncs and medical
oncologists
Phase IV Investment
- Limited requirements
(monitoring adverse
events)
- Ability to obtain
institutional
sponsorship of
additional trials
Level of
Unmet Need
Clinical Unmet Need
- High, few drugs are
approved
- Due to late diagnosis,
disease progresses rapidly,
leading to high mortality
Global Epidemiology
- 190,000 new diagnoses
and 125,000 deaths each
year worldwide
Disease Burden
- 21,550 new diagnoses/yr.
(US)
- 14,600 deaths/yr. (US)
- 177,578 women alive with
history of OC (US)
- Lifetime risk: 1.4 %
- Median age of diagnosis:
63 (US)
A Cause of Mortality
- Highly lethal
Commercial
Attractiveness
Market Size
- OC market is under $1B;
potential for dramatic growth
in aging populations
Global Epidemiology
- 190,000 new diagnoses &
125,000 deaths each year
worldwide
Market Expansion
- Limited opportunity due to
widespread use of low cost
generics
Generic Penetration
- Highly generic market
dominated by legacy chemo
agents (>95%)
Competitive Launches
- No significant launches
anticipated near-term
- Robust, competitive pipeline
(80+ agents)
Likelihood of
Technical Success
Poorly Understood Etiology
- Cell of origin is unclear
- Multiple etiology hypotheses:
incessant ovulation,
gonadotropin stimulation,
hormonal stimulation,
inflammation
Historic Ph. III /IIIB Failures
- Avastin (RHHBY)
- Phenoxodiol (Marshall
Edwards)
- Pemtumomab (Antisoma/
RHHBY)
- Pautipilone (NVS)
Statistical Challenges
- Late-stage diagnosis results in
more advanced and intractable
disease
Target Patient Populations
- Postmenopausal women
- Women with BRCA mutations
- Women with Lynch syndrome
Regulatory
Environment
Clinical Unmet Need
- High, few drugs are
approved
- Due to late diagnosis,
disease progresses rapidly,
leading to high mortality
Historical Precedents
- Ovarian Cancer National
Alliance
Advocacy
- Ovarian Cancer National
Alliance
- National Ovarian Cancer
Coalition
- Ovarian Cancer Research
Fund

10
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on ovarian cancer?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is ovarian cancer?
• Epidemiology by geography and risk factors
• Presentation, diagnosis, classification
• Current care paradigm and clinical evidence
• Emerging care paradigm
11 • 12
• 13
• 14
• 15 - 20
• 21
III. Clinical Development Pipeline • Clinical development pipeline mapping
• Traditional chemotherapies
• Anti-Angiogenesis agents
• Kinase Inhibitors
• Folate Receptor Targeting Agents
• Ovarian Cancer Vaccines
23 • 24 – 29
• 30 - 31
• 32 – 36
• 37 – 38
• 39 – 41
• 42 – 43
IV. Commercial Landscape • Estimated use in ovarian cancer of branded therapies
• Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
45 • 46
• 47 - 50
• 51
• 52
• 53 – 56
V. Appendix • Table of Acronyms
• More about Lumleian
• 58
• 59 – 61
11
What is Ovarian
Cancer?
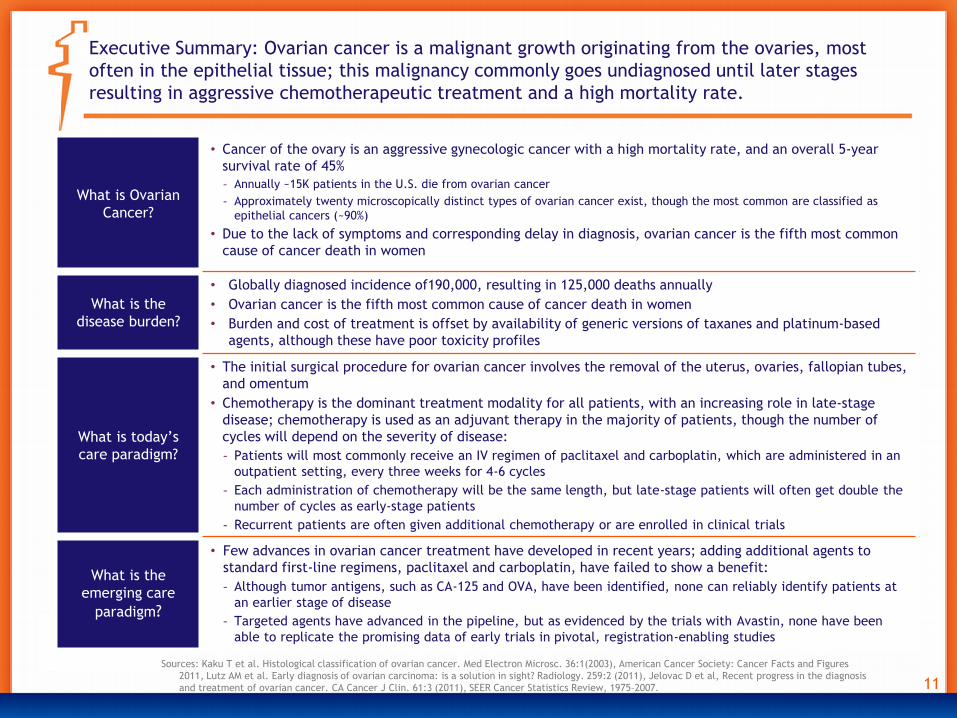
• Cancer of the ovary is an aggressive gynecologic cancer with a high mortality rate, and an overall 5-year
survival rate of 45%
- Annually ~15K patients in the U.S. die from ovarian cancer
- Approximately twenty microscopically distinct types of ovarian cancer exist, though the most common are classified as
epithelial cancers (~90%)
• Due to the lack of symptoms and corresponding delay in diagnosis, ovarian cancer is the fifth most common
cause of cancer death in women
What is the
disease burden?
• Globally diagnosed incidence of190,000, resulting in 125,000 deaths annually
• Ovarian cancer is the fifth most common cause of cancer death in women
• Burden and cost of treatment is offset by availability of generic versions of taxanes and platinum-based
agents, although these have poor toxicity profiles
What is today’s
care paradigm?
• The initial surgical procedure for ovarian cancer involves the removal of the uterus, ovaries, fallopian tubes,
and omentum
• Chemotherapy is the dominant treatment modality for all patients, with an increasing role in late-stage
disease; chemotherapy is used as an adjuvant therapy in the majority of patients, though the number of
cycles will depend on the severity of disease:
- Patients will most commonly receive an IV regimen of paclitaxel and carboplatin, which are administered in an
outpatient setting, every three weeks for 4-6 cycles
- Each administration of chemotherapy will be the same length, but late-stage patients will often get double the
number of cycles as early-stage patients
- Recurrent patients are often given additional chemotherapy or are enrolled in clinical trials
What is the
emerging care
paradigm?
• Few advances in ovarian cancer treatment have developed in recent years; adding additional agents to
standard first-line regimens, paclitaxel and carboplatin, have failed to show a benefit:
- Although tumor antigens, such as CA-125 and OVA, have been identified, none can reliably identify patients at
an earlier stage of disease
- Targeted agents have advanced in the pipeline, but as evidenced by the trials with Avastin, none have been
able to replicate the promising data of early trials in pivotal, registration-enabling studies
Sources: Kaku T et al. Histological classification of ovarian cancer. Med Electron Microsc. 36:1(2003), American Cancer Society: Cancer Facts and Figures
2011, Lutz AM et al. Early diagnosis of ovarian carcinoma: is a solution in sight? Radiology. 259:2 (2011), Jelovac D et al, Recent progress in the diagnosis
and treatment of ovarian cancer. CA Cancer J Clin. 61:3 (2011), SEER Cancer Statistics Review, 1975–2007.
Executive Summary: Ovarian cancer is a malignant growth originating from the ovaries, most
often in the epithelial tissue; this malignancy commonly goes undiagnosed until later stages
resulting in aggressive chemotherapeutic treatment and a high mortality rate.

12
Description
• Ovarian cancer is a malignant growth that arises in the ovaries, most often
from epithelial tissue
• Most ovarian cancer patients are post-menopausal women
• Ovarian cancer is subdivided into epithelial cancers, germ cell tumors, and
tumors of low malignant potential; the epithelial subtype is the most
dominant (90% of cases)
Etiology & Risk
Factors
• Women who have BRCA1/2 mutations or with hereditary non-polyposis
colorectal cancer have the highest risk, but account for only 10% of patients
• Risk is inversely proportional to number of lifetime ovulations; pregnancies,
lactation, oral contraceptives, tubal ligation and hysterectomy decrease risk
• Nulliparity, early menarche/ late menopause, hormone replacement therapy
and endometriosis increase risk
Diagnosis &
Symptom
Progression
• Screening tests, such as those which exist for the CA-125 and OVA-1 antigens,
do not improve outcome
• Early symptoms are non-specific, resulting in late-stage diagnosis; tumors
spread to the pelvis and upper abdomen, cause pelvic/abdominal pain,
swelling; weight loss, pain, bowel or ureteral obstruction are symptoms of
advanced disease
• Diagnosis: palpation of adnexal mass during pelvic examination, ultrasound, CA
125 & OVA-1 assessment, laparoscopy/laparotomy
Disease
Burden
• Estimated new cases: 21,990 (US, 2011)
• Estimated deaths: 15,460 (US, 2011)
• Lifetime incidence: 1 in 72 (1.39%); lifetime risk: 1 in 96 (1.04%) (US)
• Median age at diagnosis: 63 years. Age-adjusted incidence rate 12.9/100,000
Sources: Kaku T et al. Histological classification of ovarian cancer. Med Electron Microsc. 36:1(2003), American Cancer Society: Cancer Facts and Figures
2011, Lutz AM et al. Early diagnosis of ovarian carcinoma: is a solution in sight? Radiology. 259:2 (2011), Jelovac D et al, Recent progress in the diagnosis
and treatment of ovarian cancer. CA Cancer J Clin. 61:3 (2011), SEER Cancer Statistics Review, 1975–2007.
What is ovarian cancer?
Yes: Women No
2. Is ovarian cancer a primary cause of mortality?
7. Where is ovarian cancer treated?
Yes No
Out
Patient
Inpatient
Hospital
Long Term
Care
Symptom
Relief
Disease
Treatment
Disease
Cure
3. Is ovarian cancer an acute or chronic disease?
Acute Chronic
6. Which specialties treat ovarian cancer?
5. What is ovarian cancer’s treatment goal?
8. Who pays for ovarian cancer (Rx)?
3rd party Cash CMS
Gynecologist Gyn-
Oncologist
Medical
Oncologist
4. Is ovarian cancer a communicable disease?
Yes No
Yes No
9. Does ovarian cancer impact a special
population?
1. Is ovarian cancer etiology well understood?

13
Sources: www.seer.cancer.gov, GloboCan 2008: World Cancer Report 2008, IARC 2010, PDQ Cancer Information Summary, NCI. Genetics of Breast
and Ovarian Cancer
Global ovarian cancer incidence was 190K in 2010, with an estimated 22K new cases in the US;
the incident patient population will grow at a rate consistent with the aging population.
• BRCA1 or BRCA2 mutations (increases lifetime risk from 1.4%
in general population to 15-40% with a harmful mutation of
BRCA 1/2)
• Hereditary non-polyposis colorectal cancer (increases lifetime
risk from 1.4% to 10%)
High-Risk Factors Risk Factors
• Post-menopausal women are more likely to develop OC
• Risk is inversely proportional to number of lifetime
ovulations: pregnancies, lactation, oral contraceptives, tubal
ligation and hysterectomy decrease risk; nulliparity, early
menarche/late menopause and hormone replacement therapy
increase risk
• Endometriosis (increased inflammation) increases the risk
• 190,000 new diagnoses each year
• 125,000 deaths each year
Global Incidence
• Because 50% of ovarian cancer cases occur in women over the
age of 65, the incident patient population will grow at a rate
consistent with the aging population
US Incidence
• 21,990 new diagnoses each year
• 15,460 deaths each year
• Lifetime risk 1.4 %
• Median age of diagnosis: 63
• Age-adjusted incidence rate: 12.9 per 100,000 women
• 177, 578 women alive with a history of OC

14
Clinicians segment patients based initially on clinical stage, though tumor grade is also
considered to inform treatment; more than half of cases are diagnosed in Stage III or IV, which
contributes to the relatively high mortality rate.
Stage I Stage II Stage III Stage IV
% of presentations • 15% • 17% • 69%
Dia
gnosi
s Criteria
• Disease confined to
ovaries
• Dissemination confined
to pelvis
• Dissemination to
peritoneum
• Dissemination to liver
parenchyma, lung,
pleura, other sites
Presenting
Symptoms
• Non-specific
symptoms
• Pelvic pain • Abdominal pain;
Swelling
• Weight loss; Pain;
Bowel or ureteral
obstruction
Treatm
ent
1st line
• Debulking surgery, including, for well-differentiated Stage I & II tumors, total abdominal hysterectomy and
bilateral salpingo-oophorectomy with omentectomy for Stage III & IV disease
• The primary chemotherapy regimen is IV paclitaxel/carboplatin that is administered as adjuvant on an
outpatient basis once every three weeks, for a total of 4-6 cycles
Outcome of 1rst line
therapy
determines 2nd and
3rd line therapy
• Platinum-resistant—progressive disease during platinum therapy or within 6 months of last platinum
treatment; these patients can only expect a13% to 19% chance of response to further chemotherapy
- Platinum-resistant patients are treated with paclitaxel, pegylated liposomal doxirubicin, gemcitabine,
topotegan, cyclophosphamide or other non-platinum agents in 2nd and 3rd line therapy
• Platinum partially sensitive—progressive disease 6–12 months from last platinum therapy; patients can
expect to have a 27% chance of response to further chemotherapy
- Platinum-sensitive patients are treated with a combination of carboplatin and a non-platinum agent, such as
paclitaxel, gemcitabine and pegylated liposomal doxirubicin
• Patients with advanced disease that recur often cycle through various chemotherapy regimens and may be
enrolled in clinical trials
5 year survival rate • 93.8% • 72.8% • 28.2%
Sources: http://www.cancer.gov/cancertopics/types/ovarian, Kaku T et al. Histological classification of ovarian cancer. Med Electron Microsc.
36:1(2003), American Cancer Society: Cancer Facts and Figures 2011

15
Carboplatin
(Paraplat, Paraplatin, Paraplatin-AQ)
Cisplatin
(Platinol, Platinol-AQ)
MoA • DNA binder/crosslinking agent – Platinum • DNA binder/crosslinking agent – Platinum
Sponsor • Widely available as generic
• Paraplatin is sold by BMS
• Widely available as generic
• Platinol is sold by BMS
Formulation
(Generic)
• Aqueous solution • Aqueous solution
Dosing • 300-360 mg/m2 IV every 4 weeks or target AUC 5-7.5
every 3 weeks (4-10 cycles)
• May be administered IP in ovarian cancer; a typical
regimen for intra-peritoneal infusion is 200-650
mg/m2
• IV; 75 mg/m2
• May be administered IP in ovarian cancer
Indications • OC that has recurred after cisplatin, or is advanced
and has never been treated; also used for palliative
treatment of OC that has recurred after earlier
chemotherapy
• OC that is advanced, or has metastasized in patients
whose disease has not gotten better with other types
of treatment or chemotherapy
Adverse Events
(Discontinuation)
• Severe side-effects include infusion reactions,
gastrointestinal toxicity (nausea/vomiting),
nephrotoxicity, myelo-suppression, peripheral
sensory neuropathy
• Severe side-effects include infusion reactions,
gastrointestinal toxicity (nausea/vomiting),
nephrotoxicity, myelo-suppression, peripheral
sensory neuropathy
Lumleian
Commentary
• Carboplatin is the preferred platinum agent to cisplatin for platinum-sensitive ovarian cancer, owing to the
belief that carboplatin is significantly less toxic, although does not confer an efficacy advantage; this
demonstrates that an improved side effect profile can govern uptake as standard of care
Sources: www.carboplatin.org, www.cisplatin.org, Sakaeda et al., Adverse event profiles of platinum agents: data mining of the public version of
the FDA adverse event reporting system, AERS, and reproducibility of clinical observations. Int J Med Sci 8:6 (2011)
The first-line, post-surgical chemotherapy regimen for ovarian cancer consists of a platinum-
based agent, generic carboplatin or cisplatin, usually in combination with generic paclitaxel; in
most markets, this combination is considered the SoC therapy.

16
Paclitaxel
(Taxol)
MoA • Microtubule inhibitor/tubulin binder
Sponsor • Paclitaxel is sold by BMS
Formulation
(Generic)
• Solution for injection
Dosing • For previously untreated patients one of the following recommended regimens may be given every 3 weeks: 1)
over 3 hours at a dose of 175 mg/m2 followed by cisplatin at a dose of 75 mg/m2 or 2) over 24 hours at a dose of
135 mg/m2 followed by cisplatin at a dose of 75 mg/m2
• In patients previously treated with chemotherapy, paclitaxel injection has been used at several doses and
schedules; although, the optimal regimen is not yet clear, the current recommended regimen is injection 135
mg/m2 or 175 mg/m2 administered intravenously over 3 hours every 3 weeks
Indications • Frequently used in combination with platinum therapy in platinum-sensitive recurrences
• Single-agent use in platinum-refractory or platinum-resistant ovarian cancer
Adverse Events
(Discontinuations)
• Severe side-effects include myelosuppression, hypersensitivity, neurotoxicity, nausea/vomiting,
myalgia/arthralgia, diarrhea, asthenia, peripheral neuropathy
Lumleian
Commentary
• Widespread availability of low cost generic versions of Taxol have supported adoption into first-line regimens in
the majority of markets, despite conflicting data supporting use first-line
• Novel, solvent-free formulations of paclitaxel are in Phase III clinical trial in ovarian cancer: Paclical (Oasmia
Pharmaceutical) is nano particle-bound paclitaxel, Abraxane (Abraxis/Celgene) is albumin-bound paclitaxel,
and Opaxio (paclitaxel poliglumex; Cell Therapeutics) is amino acid-bound paclitaxel
Sources: www.cancer.gov, Taxol drug label, www.clinicaltrials.gov
The microtubule inhibitor, Taxol, continues to be used as standard-of-care; however, data from
the ICON3 trial has showed that the addition of Taxol to platinum-based monotherapy does not
confer a survival benefit.

17
Doxorubicin Hydrochloride
(Adriamycin, Evacet/DOXIL/Dox-SL/LipoDox liposomes)
MoA • Microtubule inhibitor/tubulin binder – Anthracycline
Sponsor • Liposomal formulation (DOXIL) sold by Johnson and Johnson (Centocor)
Formulation
(Generic)
• Powder must be dissolved for IV administration (Adriamycin)
• Liposomal formulation approved by FDA in 1995, solution (DOXIL)
Dosing • Liposomal formulation (DOXIL): 50 mg/m2 IV every 4 weeks for 4 courses minimum
Indications • Liposomal formulation (DOXIL): single-agent use in platinum-refractory or platinum-resistant OC
• Frequently used in combination with platinum therapy in platinum-sensitive recurrences
Adverse Events
(Discontinuations)
• Severe side-effects include infusion reactions, myelo-suppression, cardio-toxicity, Hand-Foot syndrome
Lumleian
Commentary
• Liposomal doxorubicin alleviates the cardio-toxicity and neurotoxicity associated with doxorubicin and
provides a longer half-life of the molecule, although the Doxil provides only a modest benefit (12%
response rates; 11-month median overall survival) in recurrent disease setting
• Data from the ICON 5 trial demonstrated that adding a third cytotoxic agent in the first-line setting did not
improve progression-free survival, limiting the agent’s ability to penetrate earlier treatment lines
Sources: DOXIL drug label, Journal of Clinical Oncology, 2006 ASCO Annual Meeting Proceedings Part I. Vol 24, No. 18S, 2006
The anthracycline, liposomal doxorubicin, is a component of regimens targeting patients with
platinum-resistant disease, although clinicians will often re-treat with the initial combination
after a first relapse before moving on to second-line agents.

18
Cyclophosphamide
(Clafen/Cytoxan/Neosar)
MoA • DNA binder/alkylating agent
Sponsor • Powder for injection sold by Baxter Healthcare
• Tablets for oral use sold by Roxane
Formulation
(Generic)
• Powder for injection
• Tablets for oral use
Dosing • When used as the only oncolytic drug therapy, the initial course of cytoxan for patients with no hematologic
deficiency usually consists of 40 to 50 mg/kg given intravenously in divided doses over a period of 2 to 5 days;
other intravenous regimens include 10 to 15 mg/kg given every 7 to 10 days or 3 to 5 mg/kg twice weekly
• Oral cytoxan dosing is usually in the range of 1 to 5 mg/kg/day for both initial and maintenance dosing
Indications • Recurrent OC
• Frequently used in combination with platinum therapy in platinum-sensitive recurrences
Adverse Events
(Discontinuations)
• Severe side-effects include myelosuppression, gastrointestinal toxicity, pulmonary toxicity, cardiotoxicity,
hypersensitivity and secondary neoplasias
Lumleian
Commentary
• Cyclophosphamide is commonly used in relapse patients although other agents, such as liposomal doxorubicin,
are preferable due to toxicity issues, leading to a decline in use over the past years
Sources: www.fda.gov, www.drugs.com, Cytoxan prescribing information
Cyclophosphamide once was a core component of first-line regimen CAP, but has now been
supplanted by the more effective taxanes.

19
Topotecan hydrochloride
(Hycamtin)
MoA • Topoisomerase inhibitor
Sponsor • GSK
Formulation
(Generic)
• Solution for injection
Dosing • 1.5 mg/m2 by intravenous infusion over 30 minutes daily for 5 consecutive days, starting on day 1 of a 21 day
course. In the absence of tumor progression, a minimum of 4 courses is recommended because tumor response
may be delayed
Indications • Single-agent use in platinum-refractory or platinum-resistant OC
Adverse Events
(Discontinuations)
• Severe side-effects include myelosuppression, nausea, vomiting, alopecia and asthenia
Lumleian
Commentary
• Hycamtin’s utility is further constrained in the second-line setting, due to the fact that recurrent patients
who have Hycamtin-resistant or Paclitaxel-resistant disease have little chance of responding to the other
drug
• Similarly, the negative results of the ICON 5 trial, paired with a poor toxicity profile, has relegated
Hycamtin to a third-line option for most patients
Sources: www.cancer.gov, www.fda.gov, Hycamtin prescribing information
Severe hematological toxicities are observed with Hycamtin when it is used as triple therapy in
combination with paclitaxel and carboplatin, limiting the agent’s ability to penetrate the first-
line setting.

20
Gemcitabine Hydrochloride
(Gemzar)
MoA • Antimetabolite/pyrimidine analog
Sponsor • Generic formulations widely available since Q4 2010
• Eli Lilly
Formulation
(Generic)
• Solution for injection
Dosing • Intravenously at a dose of 1000 mg/m2 over 30 minutes on Days 1 and 8 of each 21-day cycle
Indications • Single-agent use in platinum-refractory or platinum-resistant OC
• Frequently used in combination with platinum therapy in platinum-sensitive recurrences
• Responses have been observed in paclitaxel-refractory OC
Adverse Events
(Discontinuations)
• Severe side-effects include myelosuppression, cardiotoxicity, vascular toxicity, hepatotoxicity, pulmonary
toxicity, renal toxicity
Lumleian
Commentary
• As with other agents, Gemzar failed to demonstrate an efficacy benefit as first-line triple therapy in the
ICON 5 trial
• However, Gemzar is well tolerated and produces relatively mild side effects, such as minor
myelosuppression, so the agent is used frequently as mono-therapy in the second-line setting
Sources: www.drugs.com, Gemzar drug label
Lilly’s Gemzar has been approved for ovarian cancer for patients that have had a relapse of at
least six months after failure of a platinum-based regimen; however, the agent is now subject to
generic competition after loss of patent exclusivity at the end of 2010.

21
• Ovarian cancer has a poor treatment response profile and high mortality, primarily due to lack of specific
symptoms and the resulting late-stage diagnosis
• Numerous blood markers and protein profiles are being evaluated, though success is not expected in the
near-term
- Markers, such as CA125 and OVA, though performing well as indicators of treatment success and disease
progression, do not achieve the level of sensitivity that would be required for a molecular diagnostic tool in
the clinic
- Antigens which are being tested for early-stage diagnosis of ovarian cancer include SPAG9, OY-TES-1, Piwil2,
LAGE-1, NY-ESO-1, Sp17, SSX, AKAP-3, SCP-1
• Treatment selection in late stage ovarian cancer would be significantly improved by the discovery and
development of biomarkers predictive of tumor resistance to platinum-based regimens
Sources: www.clinicaltrials.gov, EvaluatePharma, Lutz AM, et al. Early diagnosis of ovarian carcinoma: is a solution in sight? Radiology
259:2(2011), Mirandola L et al., Cancer test antigens: novel biomarkers and targetable proteins for ovarian cancer. Int Rev Immunol. 30:2-3
(2011)
None of the late-stage assets are likely to transform the treatment paradigm; the most likely
changes will be in platinum-resistant patients, with only incremental improvements in efficacy.
Future
Diagnosis
Future
Treatment
• Novel formulations of established chemotherapies, such as conjugation of chemotherapies to molecules
which specifically target tumor cells, may demonstrate greater efficacy while reducing overall toxicity;
promising examples include EC-145 and Abraxane
• In addition to new generation cytotoxic agents, novel targeted therapies are undergoing clinical testing;
late-phase (III-IV) emerging therapies include new-generation topoisomerase inhibitors, DNA binders and
microtubule inhibitors as well as immunotherapy, epigenetic therapy, vascular-targeting therapy and
kinase inhibitors
- Insights from other cancer indications, such as the link between specific mutations and treatment efficacy,
may inform future ovarian cancer trials and treatments
- Established links between specific mutations and the therapeutic efficacy of targeted agents will lead to
increased sequencing of tumors as part of the treatment selection process
• Combination therapy, personalized medicine, prediction and monitoring of treatment responses by
biomarkers are foreseen as part of the future standard of care
22
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on ovarian cancer?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is ovarian cancer?
• Epidemiology by geography and risk factors
• Presentation, diagnosis, classification
• Current care paradigm and clinical evidence
• Emerging care paradigm
11 • 12
• 13
• 14
• 15 - 20
• 21
III. Clinical Development Pipeline • Clinical development pipeline mapping
• Traditional chemotherapies
• Anti-Angiogenesis agents
• Kinase Inhibitors
• Folate Receptor Targeting Agents
• Ovarian Cancer Vaccines
23 • 24 – 29
• 30 - 31
• 32 – 36
• 37 – 38
• 39 – 41
• 42 – 43
IV. Commercial Landscape • Estimated use in ovarian cancer of branded therapies
• Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
45 • 46
• 47 - 50
• 51
• 52
• 53 – 56
V. Appendix • Table of Acronyms
• More about Lumleian
• 58
• 59 – 61

23
Source: Lumleian perspective
Executive Summary: Clinical Development Pipeline
What is in the
industry’s
clinical
development
pipeline?
• As of Q1 2012, Lumleian validated 81 assets in development for ovarian cancer
• The vast majority of the ovarian cancer pipeline is comprised of next-generation as well as novel
chemotherapeutic agents
- DNA binders, microtubule destabilizers, and topoisomerase inhibitors are all validated classes of agents that
dominate the ovarian cancer pipeline, owing to the chemo-sensitive nature of this tumor
• A number of novel, targeted drug classes are being pursued, including monoclonal antibodies, anti-
vascular approaches, agents targeting kinases, and immunotherapy
- Numerous anti-angiogenesis agents are in development, including Roche’s Trebananib, Sanofi’s
Aflibercept,Takeda’s Ramucirumab, ImClone’s Vargatef, and Exelixis’ XL999
- Despite early positive data supporting Roche’s Avastin, disappointing Phase III survival data paired with
significant side effects have drawn into question whether anti-VEGF approaches will be a viable approach for
ovarian cancer
- Several clinical-stage programs are directed at intracellular kinases involved in cell signaling, proliferation,
and cell cycle transcription factors
What is the
evidence for late
stage assets?
• Although the overall pipeline contains numerous assets in development, the vast majority are at a pre-
proof of concept stage in ovarian cancer and lack data showing tumor-specific efficacy
• Roche’s Avastin has been moderately successful in targeting the VEGF pathway in other oncology
indications; Phase III data has demonstrated minimal benefit over existing therapy, with significant
adverse effects
- Assets with any proof-of-concept data are likely to become used following paclitaxel/carboplatin, as few
agents provide any benefit in this high unmet need setting

24
Sources: : Lumleian perspective
Drug sponsors have numerous entry points in advanced ovarian cancer (Stage IIb-IV), when
developing a clinical development strategic plan; although each market segment presents
unique opportunities, each segment also poses unique development issues.
Neoadjuvant
Adjuvant
(First-Line)
Active Comparator Opportunity Key Issues
• Paclitaxel + Carboplatin
• Standard of care provides limited
tumor reduction; opportunity to
increase magnitude of response
• Ability to obtain institutional
sponsorship for such a study
• Neoadjuvant protocols are only
applicable to a subset of patients
with Stage III-IV disease
• Chemo generally administered for
only 3 cycles; limited duration of
treatment
• Paclitaxel + Carboplatin
• Given the limited survival benefit,
new agents may be tested first-line
by showing a benefit in addition to
SOC chemotherapy
• Efficacy benefit would result in
rapid uptake by clinicians
• Avastin was unable to improve PFS
in large, pivotal trial, despite
promising data
• ICON 5 trial showed that adding a
third chemo to SOC did not improve
SOC
Relapse
(Second-Line) • Gemzar, Doxorubicin,
Cyclophosphamide
• Relapse and treatment refractory
rates remain very high in this tumor
• Limited efficacy of available
second-line agents
• Ability to gain approval based on
PFS endpoint
• Difficult population to treat;
median progression-free survival of
3-5 months
• Challenging to differentiate
resistant and refractory patients
Patient Segment
Novel agents have an opportunity to penetrate the first-line treatment setting initially;
however, no agents have been able to demonstrate a significant improvement in overall
survival in pivotal trials to date

25
OC Pipeline: Current (N= 81) Phase III
(N = 16)
Phase II
(N = 42)
Phase I
(N = 23)
DNA binders (6)
Alkylating agent (4) 1 2 1
DNA intercalation agent (1) - 1 -
Hypomethylation agent (1) - 1 -
Apoptosis Induction (10)
Antibody-mediated (1) - - 1
Antimetabolite (1) - 1 -
Gene therapy (1) - 1 -
Lytic Peptide (1) - 1 -
PARP Inhibitor (3) - 3 -
Other (3) 1 2 -
Mitosis Disruptors (14)
G2 disrupter (2) - 1 1
HDAC inhibitor (1) - - 1
Microtubule Disruptor (5) 2 1 2
Topoisomerase Inhibitor (6) 2 2 2
Anti-Angiogenesis agents (11)
Angiopoetin antagonist (1) 1 - -
Anti-PIGF (1) - - 1
VEGFR inhibitor (5) 4 1 -
Other (4) 1 2 1
Kinase Inhibitors (11) Akt, Aurora A Kinase, BRAF, c-MET, EGFR,
Her2, IGF1R, BDGFR, Ras 1 9 2
Immunomodulation (7) T-cell, B-cell, NK cell activation - 5 2
Vaccines (12) 1 8 3
Folate-Targeting Agents (3) 2 - 1
Other (6) HSP inhibitors, viral therapy, etc. - 1 5
Sources: www.clinicaltrials.gov, EvaluatePharma
The ovarian cancer pipeline is comprised of next-generation cytotoxic agents with potential for
incremental improvement, as well as novel, targeted agents with transformational potential,
but which require validation, as little is known about signaling mechanisms in ovarian cancer.

26
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
pipeline presentations, analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; CenterWatch
As of Q1 Lumleian validated 81 assets in ‘active’ clinical development for OC: 23 in Phase III, 42
in Phase II, and 16 in Phase I; leading oncology companies hold multiple assets, while the
pipeline is dominated by smaller biotech companies with an interest in cancer.
OC Assets in ‘Active’ Clinical Development
Phase III (N = 23) Phase II (N =42) Phase I (N = 16)
1 1 1 1 1 1 1
3
1
5 2
1 1
1 1 1
1
1
5
1
1
1
1
2
1 1
1 2
0
5
10

27
Traditional chemotherapeutics, such as mitosis disruptors, apoptosis induction agents and DNA
binders are under investigation due to the chemo-sensitive nature of ovarian cancer; however,
pipeline agents are likely to provide only incremental improvement over current SoC.
Mechanism of Action Phase III (N = 6) Phase II (N = 16) Phase I (N = 8)
DN
A
bin
ders
(10)
Alkylating agent (4) • Eloxatine (SNY) • Irofulven
• Prolindac (ACCP)
• Picoplatin (PARD)
DNA intercalation agent (1) • Zoptarelin Doxorubicin (AEZS)
Hypomethylation agent (1) • Dacogen (ESALY)
Apopto
sis
Inducti
on (
10)
Antibody-mediated (1) • GT-Mab 2.5 GEX (Glycotope)
Antimetabolite (1) • Alimta (LLY)
Gene therapy (1) • BC-819 (BICL)
Lytic Peptide (1) • EP-100 (Esperance
Pharmaceuticals)
PARP Inhibitor (3)
• Iniparib (SNY) • Olaparib (AZN) • Rucaparib (CLVS)
Other (3) • Canfosfamide (TELK) • Tasisulam (LLY)
• Tirapazamine
Mit
osi
s D
isru
pto
rs
(14)
G2 disrupter (2) • Ispinesib (CYTK) • CBP-501 (CanBas)
HDAC inhibitor (1) • Belinostat (TPTGF)
Microtubule Disruptor (5) • Opaxio (CTIC) • Paclical (Oasmia)
• Abraxane (CELG) • Lorvotuzumab (IMGN) • SAR-566658 (IMGN)
Topoisomerase Inhibitor (6)
• Hycamtin (GSK) • Karenitecin (BioNumerik)
• Quinamed (ChemGenex) • Vosaroxin (SNSS)
• Brakiva (TLON) • Pegylated Irinotecan (PFE)
Sources: www.clinicaltrials.gov, EvaluatePharma

28
Mechanism of Action Phase III (N = 6) Phase II (N = 3) Phase I (N = 2)
Anti
-angio
genesi
s agents
(11)
Angiopoetin
Antagonist (1)
• Trebananib (Takeda
Pharmaceuticals)
Anti-PIGF (1)
• RO5323441 (RHHBY)
VEGF inhibitors (5)
• Votrient (GSK) • Zaltrap (SNY) • Avastin (RHBY) • Vargatef (Boehringer Ingelheim)
• Ramucirumab (LLY)
Other (4)
• Thalomid (CELG) • Panzem (ENMD) • Zybrestat (OXGN)
• Vadimezan (NVS)
Anti-angiogenesis agents target several pathways involved in vascular development; VEGF
pathway inhibition dominates the anti-angiogenesis landscape.
Sources: www.clinicaltrials.gov, EvaluatePharma

29
Numerous kinase-targeting strategies are being pursued in treatment of ovarian cancer, in hopes
of replicating the dramatic success of some kinase inhibitors in different oncology indications;
however, to date kinase inhibition has not demonstrated significant improvement on SoC.
Mechanism of Action Phase III (N = 1) Phase II (N = 8) Phase I (N = 2)
Kin
ase
Inhib
itors
(11)
Akt inhibitors (1) • VQD-002
Aurora A Kinase inhibitors (1) • Alisertib (Takeda Pharmaceuticals)
BRAF inhibitors (2) • Nexavar (BAYN)
• Selumetinib (AZN)
c-MET inhibitors (1) • Cabozantinib (EXEL)
EGFR inhibitors (2) • Tarceva (RHHBY) • Erbitux (BMY/LLY/MRK)
Her2 inhibitors (1) • Omnitarg (RHHBY)
IGF-1R inhibitors (1) • Linsitinib (Astellas Pharma, Inc.)
PDGFR inhibitors (1) • Olaratumab (LLY)
Ras inhibitors (1) • TLN-4601 (TLN)
Sources: www.clinicaltrials.gov, EvaluatePharma

30 Sources: Bio-Pharma Insight; Clinical Trials.gov. http://chemweb.bham.ac.uk
Telcyta and Eloxitine are two of the most advanced traditional chemotherapeutics attempting
to provide improvements over existing standard of care, however, the currently available low-
cost and well-know therapies present a significant hurdle to commercial success.
Physiology • Unimpeded DNA synthesis and segregation is
required for cell division
Pathophysiology • Cancer cells divide at a faster rate than normal
cells and fail to respond to normal mitosis
inhibition signals
Hypothesized
Mechanism
• Interference with DNA structure leads to inhibition
of DNA and protein synthesis, stopping cell division
and even causing cell death
• DNA binding is a well-established MOA for cancer
treatment, and is the basis of many traditional
chemotherapies
• Impeding other mechanisms of mitosis, such as
disruption of microtubules or inhibition of
topoisomerase are other mechanisms of traditional
chemotherapy
Pipeline
2 doxorubicin molecules
bound to DNA
Phase III (6) • Eloxatine (SNY) • Telcyta (TELK)
• Paclical (Oasmia) • Hycamtin (GSK)
• Karenitecin (BioNumerik) • Opaxio (CTIC)
Phase II (16) • Irofulven • Prolindao (ACCP) • Zoptarelin Doxiorubicin (AEZS) • Dacogen (ESALY) • Alimta (LLY)
• EP-100 (Esperance) • Iniparib (SNY) • Olapanib (AZN) • Rucaparib (CLVS) • Tasisulam (LLY)
• BC-819 (BICL) • Tirapazmine, Ispinesib (CYTK) • Abraxane (CELG) • Quinamed (ChemGenex) • Vosaroxin (SNSS)
Phase I (8) • Picoplatin (PARD) • GT-Mab 2.5 GEX (Glycotope)
• CBP-501 (CanBas) • Belinostat (TPTGF) • Lorvotuzumab (IMGN)
• SAR-566658 (IMGN) • Brakiva (TLON), Pegylated • Irinotecan (PFE)

31
Sources:www.clinicaltrials.gov, Vergote, I et al. Randomized Phase III study of canfosfamide in combination with pegylated liposomal doxorubicin
compared with pegylated liposomal doxorubicin alone in platinum-resistant ovarian cancer. Int J Gynecol Cancer. 20:5 (2010)
Telcyta/Canfosfamide (TELK), a glutathione s-transferase-activated cytotoxic pro-drug, has
shown promise by increasing survival with the drawback of accompanied increased toxicity;
further clinical evaluation is expected.
Telcyta (Canfosfamide)
Efficacy: Phase III results of combination study of canfosfamide + pegylated liposomal doxorubicin (PLD) published in 2010:
• PFS Canfosfamide + PLD: 5.6 months (n=65)
• PFS PLD alone: 2.9 months (n=60)
Safety: • Hematologic adverse events: 66% for canfosfamide + PLD vs 44% for PLD alone
• Palmar-plantar erythrodysesthesia and stomatitis incidence: 23% and 31% for canfosfamide + PLD vs 39% and 49%
for PLD alone
Lumleian Commentary: • Clinical trials of Telcyta have demonstrated that increased PFS was obtained with increased hematological
toxicity; further clinical evaluation of Telcyta is expected in ovarian cancer
Phase III (Completed)
Patient Segment: • Platinum-resistant ovarian cancer
Stratification: • Randomized, open-label
Studies:
(Target Enrollment)
• N = 244, N = 125, N = 440
Comparator: • PLD alone
Dosing: • 1000 mg/m2 canfosfamide; 50 mg/m2; IV; day 1 and every 28 days
• Dose until progression or unacceptable toxicity
Duration: • 60 months
Primary End-Points: • Primary: PFS
• Secondary: Objective Response
• Secondary: Tolerance/Toxicity

32
Physiology • Tumors secrete angiogenic factors that promote the
formation of blood vessels;
– Vascular endothelial growth factor (VEGF), basic
fibroblast growth factor (bFGF), platelet-derived
growth factor (PDGF), placental growth factor
(PlGF) and angiopoietins play a role in blood
vessel formation
Hypothesized
Mechanism • Normal cells cannot live past the diffusion limit of
oxygen and nutrients, and therefore depend on the
proximity of blood vessels; therefore, tumors
cannot grow unless they secure their own blood
supply by promoting the growth of nearby
vasculature in a process called angiogenesis
• Two main classes of therapeutic agents target
tumor vasculature: angiogenesis inhibitors and
vascular-disrupting agents (VDA)
Phase III (6) • Avastin (RHHBY) • Trebananib (Millenium/Takeda)
• Vargatef (Boehringer Ingelheim) • Zaltrap (Regeneron)
• Votrient (GSK) • Thalomid (CELG)
Phase II (3) • Ramucirumab (LLY) • Panzem (ENMD)
• Zybrestat (OXGN)
Phase I (2) • Vadimezan (NVS) • RO5323441 (RHHBY)
Sources: Bio-Pharma Insight, www.clinicaltrials.gov, http://www2.nau.edu, Hall M, et al. Recurrent ovarian cancer: when and how to treat. Curr
Oncol Rep. 13:6 (2011)
Pipeline
Avastin and trebananib are the most advanced vascular-targeting agents, with Avastin showing a
modest efficacy benefit in pivotal trials; although FDA approval is unlikely, Avastin is likely to be
used widely in this difficult-to-treat tumor type.

33
Sources: www.clinicaltrials.gov, Perren et al. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med 365:26 (2011), Hall M, et al. Recurrent
ovarian cancer: when and how to treat. Curr Oncol Rep. 13:6 (2011), Aghajanian C, et al. OCEANS: A Randomized, Double-Blind, Placebo-Controlled
Phase III Trial of Chemotherapy With or Without Bevacizumab in Patients with Platinum-Sensitive Recurrent Epithelial Ovarian, Primary Peritoneal or
Fallopian Tube Cancer. J Clin Oncol. (2012)
Although Avastin showed promise in Phase II studies, the pivotal trials (ICON7 and Oceans) led to
a modest efficacy benefit with increases in the development of fistulae and GI perforations that
raise the patients’ risk factors; FDA approval is unlikely.
Avastin
Efficacy: • In the ICON7 trial, patients treated with carboplatin + paclitaxel had a mean PFS of 22.4 months, while the
carboplatin + paclitaxel + Avastin arm had a mean PFS of 24.1 months
- In patients at high risk for progression, PFS was 14.5 months with standard therapy and 18.1 months with
Avastin, while median OS was 28.8 months in the control group and 36.6 months with Avastin
• In the OCEANS trial, patients with relapsed, platinum-sensitive disease treated with carboplatin + gemcitabine had a
PFS of 8.4 months, while patients given carboplatin + gemcitabine + Avastin had a PFS of 12.4 months
- Overall survival was 35.2 months in patient receiving no Avastin and 33.3 months in Avastin-treated patients
Safety: • Avastin treatment is associated with serious toxicities , including hypertension, gastrointestinal perforations and
inracereberal hemorrhage
Lumleian
Commentary:
• Avastin has demonstrated positive data in advanced ovarian cancer (ICON7) and early-stage patients with multiple risk
factors; however, the efficacy benefit is modest and unlikely to support FDA approval given the increase in adverse
events
Phase III Program (Completed) Phase III Program (Completed)
Patient Segment: • ICON7: Advanced Ovarian Cancer (Stage IIB or greater) • OCEANS: Recurrent, platinum-sensitive ovarian cancer
Stratification: • Randomized, two arm trial (N=1528) • Randomized, double-blinded (N=484)
Comparator: • Standard of care, carboplatin and paclitaxel • Control: Carboplatin and gemcitabine + placebo
• Research: Carboplatin and gemcitabine + Avastin
Dosing: • 6 cycles, 1 Avastin for 6 cycles and then Avastin alone
for a further 12 cycles
• 6, 21-day treatment cycles; research arm followed by
Avastin as a single agent until disease progression
Duration: • Control: 18 weeks; Research: 54 weeks • Control: 18 weeks; Follow-up to 24 months
Primary End-Points: • Primary: Progression-free survival
• Secondary: Objective Response; Overall survival
• Primary: Progression-free survival
• Secondary: Objective Response; Overall survival

34
Sources: www.Clinicaltrials.gov, Karlan BY et al., Randomized, double-blind, placebo-controlled phase II study ofAMG 386 combined with weekly
paclitaxel in patients with recurrent ovarian cancer. J Clin Oncol. 30:4 (2012)
Millenium/Takeda’s vascular-targeting agent lead asset trebananib has been advanced to Phase
3 trials in Australia, Canada, and Europe for recurrent ovarian cancer patients.
Trebananib (AMG 386)
Efficacy: • Prolongation of PFS in Phase II in combination with weekly paclitaxel from 4.6 to 7.2 months; may not dramatically
extend survival in terminal patients, but shows promise in recurrent patient population not pursued by Avastin
Safety: • Side effects included edema, hypertension, thromboembolic events
Lumleian
Commentary:
• Trebananib could renew promise for vascular-targeting agents if Phase III data is positive, although the mechanistic
similarity to Avastin makes those results uncertain; the side effect profile looks distinct from other VEGF inhibitors
Phase II (Completed) TRINOVA-1, TRINOVA-3 Phase III (Ongoing)
Patient Segment: • Recurrent ovarian cancer • Recurrent ovarian cancer
Stratification: • Randomized, double-blind • Global multicenter, randomized, double-blind trial of
paclitaxel plus trebananib or placebo
Studies:
(Target Enrollment)
• N = 161 • N = 900
Comparator: • Trebananib plus paclitaxel vs. placebo • Trebananib plus paclitaxel vs. placebo
Dosing: • Paclitaxel at 80 mg/m2 IV QW (3 on/1 off) plus
Trebananib at 10 mg/kg (Arm A), 3 mg/kg (Arm B) or
placebo (Arm C) IV QW
• Experimental: Weekly Intravenous (IV) Trebananib 15
mg/kg plus IV paclitaxel 80 mg/m2 weekly (3 on / 1
off); Control: Weekly Intravenous (IV) placebo plus IV
paclitaxel 80 mg/m2 weekly (3 on / 1 off)
Duration: • Disease progression or unacceptable toxicity • Primary data: July 2013; study completion: April 2017
Primary End-Points: • Primary: Progression-free survival
• Primary: Progression-free survival
• Secondary: Overall survival, objective response rate

35
Sources: www.clinicaltrials.gov, Ledermann JA et al. Randomized phase II placebo-controlled trial of maintenance therapy using the oral triple
angiokinase inhibitor BIBF 1120 after chemotherapy for relapsed ovariancancer. J Clin Oncol. 29:28 (2011), Bousquet G et al. Phase I study
of BIBF 1120 with docetaxel and prednisone in metastatic chemo-naive hormone-refractory prostate cancer patients.. Br J Cancer. 105:11 (2011)
Boehringer Ingelheim’s Vargatef is a novel triple angiokinase inhibitor that inhibits VEGFR, FGFR
and PDGFR; Phase II data in relapse patients is promising.
Vargatef (BIBF 1120)
Efficacy: • 14.3% of patients in the active arm were progression-free at 9 months, compared to just 5% progression-free in the
placebo arm of the trial
Safety: • Generally well tolerated; no significant hypertension
Lumleian
Commentary:
• Vargatef has shown promise in relapse patients who have already undergone treatment with chemotherapy in order to
delay the time to relapse; study was not powered to show significance but trends in efficacy looked favorable, but BI
has not announced plans for a Phase III maintenance trial
• A Phase III clinical trial is in progress for first-line treatment of primary disease
Phase II (Completed) LUME-Ovar 1 Phase III (Ongoing)
Patient Segment: • Continuous Maintenance Treatment Following
Chemotherapy in Patients With Relapsed Ovarian Cancer
• First-line in Patients With Advanced Ovarian Cancer
Stratification: • Randomized Placebo-Controlled • Multicenter, Randomized, Double-blind
Studies:
(Target Enrollment)
• N = 84 • N = 1300
Comparator: • Placebo during maintenance phase • Combination with carboplatin and paclitaxel vs.
placebo, carboplatin and paclitaxel
Dosing: • Oral, BID dosing of active drug • Oral, BID dosing of active drug
Duration: • 9 months • 41 months
Primary End-Points: • Progression-free survival (PFS) • Progression-free survival (PFS)

36
Sources:www.clinicaltrials.gov, Friedlander M et al. A Phase II, open-label study evaluating pazopanib in patients with recurrent ovarian
cancer. Gynecol Oncol.119:1 (2010)
GSK has advanced its oral, vascular-targeting agent Votrient to the second stage of a Phase II
trial with promising biochemical response, but no data is available on the agent’s ability to
impact survival in a randomized, controlled study.
Votrient (Pazopanib)
Efficacy: • In Phase II clinical trials, Votrient monotherapy has demonstrated a biochemical response in 31% of recurrent
ovarian cancers; ORR was 18%
Safety: • Generally well tolerated; no significant hypertension
Lumleian Commentary: • Although Votrient has demonstrated a biochemical response in ovarian cancer patients, and is generally well-
tolerated, clinical trials have so far failed to demonstrate meaningful efficacy in treatment of ovarian cancer
• A Phase III trial is underway, but this trial has been designed to test Votrient as a maintenance therapy,
rather than a treatment for the primary disease
Phase II (Completed) Phase III (Ongoing)
Patient Segment: • First-line in Patients With Advanced Ovarian
Cancer
• Stage III/IV ovarian cancer which has not progressed after
first-line therapy
Stratification: • Multicenter, Randomized, Double-blind • Randomized, placebo-controlled, double-blind
Studies:
(Target Enrollment)
• N = 35, N = 12 • Target enrollment N = 900
Comparator: • None • Placebo
Dosing: • 800 mg daily, 800 mg daily w/carboplatin,
800 mg daily w/paclitaxel
• 800 mg daily
Duration: • Baseline to response after 3 years • Up to 8 years
Primary End-Points: • Primary: Best Biochemical Response
• Primary: Toxicity/Tolerance
• Secondary: Overall response
• Primary: PFS
• Secondary: OS
• Secondary: Toxicity/Tolerance

37
Sources: Faivre, Kroemer & Raymond. Current development of mTOR inhibitors as anticancer agents. Nature Reviews Drug Discovery. 5:8 (2006).
www. clinicaltrials.gov, EvaluatePharma
To date, non-VEGFR kinase inhibitors have failed to replicate the successes achieved in other
oncology indications; however, numerous clinical trials remain underway and results may
improve with a greater understanding of ovarian cancer etiology.
Physiology • The numerous kinase mediate cell growth,
proliferation and survival
Pathophysiology • Hyperactivation of these critical pathways can
result in inappropriate cell growth, proliferation
and survival
Hypothesized
Mechanism
• Inhibition of the kinase-mediated pathway can
abrogate the cell proliferation and survival signals
that tumors depend upon
Pipeline
Phase III • Tarceva (RHHBY)
Phase II • Alisertib (Takeda) • Nexavar (BAYN) • Selumetinib (AZN)
• Cabozantinib (EXEL) • Erbitux (BMY/LLY/MRK) • Omnitarg (RHHBY)
• Linsitinib (Astellas) • Olaratumamb (LLY)
Phase I • TLN-4601 (TLN)

38
Sources:www.clinicaltrials.gov, Gordon AN et al. Efficacy and safety of erlotinib HCl, an epidermal growth factor receptor (HER1/EGFR) tyrosine kinase
inhibitor, in patients with advanced ovarian carcinoma: results from a phase II multicenter study. Int J Gynecol Cancer. 15:5 (2005), H. Hirte et al.
phase II study of erlotinib (OSI-774) given in combination with carboplatin in patients with recurrent epithelial ovarian cancer (NCIC CTG IND.149).
Gynecologic Oncology. 118 (2010), Halla S. Nimeiri et al., Efficacy and safety of bevacizumab plus erlotinib for patients with recurrent ovarian, primary
peritoneal, and fallopian tube cancer. Gynecologic Oncology 110 (2008), Blank SV, Erlotinib added to carboplatin and paclitaxel as first-line treatment
of ovarian cancer: Gynecologic Oncology 119 (2010)
Tarceva (RHHBY/OSI) has disappointed as a second- and third-line treatment for ovarian cancer;
Tarceva is currently in Phase III clinical trials as a maintenance therapy for patients who have
demonstrated an objective response to platinum therapy.
Tarceva (erlotinib)
Efficacy: • Tarceva was found to have an ORR of 57% in platinum-sensitive and 7% in platinum-resistant tumors
• A Phase II combination trial found that Tarceva did not demonstrate clinical benefit over Avastin alone
Safety: • Tarceva was generally well-tolerated; the most frequent adverse events were rash and diarrhea
Lumleian
Commentary:
• Although Tarceva has performed disappointingly in ovarian cancer to date, it is currently in Phase III trials as a
maintenance therapy; the favorable toxicity profile may increase odds of approval if Phase III data is positive
Phase II (Completed) Phase III (Ongoing)
Patient Segment: • Refractory ovarian cancer, platinum-sensitive and
platinum-resistant
• Patients with no evidence of disease progression after
successful first-line platinum therapy
Stratification: • Open-label • Randomized, open-label
Studies:
(Target Enrollment)
• N = 34, N = 50, N = 13, N = 56 • Target enrollment N = 830
Comparator: • None, Avastin alone • Observation
Dosing: • 150 mg daily, 150 mg daily w/carboplatin or Avastin • Twice daily
Duration: • 12 months • Up to 24 months
Primary End-Points: • Primary: PFS
• Secondary: OS
• Secondary: Toxicity/Tolerance
• Primary: PFS
• Secondary: OS
• Secondary: Adverse events/Toxicity
• Secondary: Quality of life

39
Sources: EvaluatePharma, Company product information, Kalli KR et al., Folate receptor alpha as a tumor target in epithelial ovarian cancer. Gynecol Oncol. 108:3 (2008), Kelemen, LE. The role of folate receptor alpha in cancer development, progression and treatment: Cause, consequence or innocent bystander? Int. J. Cancer. 119 (2006).
Farletuzumab (MORAb-003) and vintafolide (EC-145) are the most advanced folate receptor
targeting agents, though it is currently unclear whether they will provide significant
improvement over SoC.
Physiology • Folate receptors bind and transport folate, a
critical component of cell metabolism and DNA
synthesis
Pathophysiology • Cancer cells require high levels of folate, due to
more rapid metabolism and frequent cell division;
loss of functioning folate receptors can seriously
inhibit tumor growth and activity
• Folate receptor is overexpressed in 72%-81% of all
ovarian cancers
Hypothesized
Mechanism
• Inhibition of folate receptors (by antibody or small
molecule) leads to impairment of cell metabolism
and DNA synthesis, halting mitotsis and leading to
cell death
• Alternatively, therapeutic agents are conjugated to
folate-like molecules and are transported
preferentially into cells with high levels of folate
receptor, such as ovarian cancer cells Pipeline
Phase III (2) • MORAb-003/farletuzumab (ESALY) • EC145 (BMY/ECYT)
Phase II (0)
Phase I (1) • IMGN-853 (IMGN)

40
Sources: www.clinicaltrials.gov, Armstrong, DK et al. Exploratory Phase II efficacy study of MORAb-003, a monoclonal antibody against folate
receptor alphha, in platinum-sensitive ovarian cancer in first relapse. 2008 ASCO Annual Meeting. (2008)
Farletuzumab (Morphotek/ESALY), a monoclonal antibody with anti-folate receptor activity, has
demonstrated a modest increase in response rate and overall survival in recurrent ovarian
cancer; data from a Phase III trial is expected in September 2012.
Farletuzumab (MORAb-003)
Efficacy: • In a Phase II clinical trial, patients treated with MorAb-003 in combination with paclitaxel and carboplatin
demonstrated a 6.8% CR, 63.6% PR and 20.5% SD, with an average PFS of 10.2 months
• MorAb-003 treatment alone resulted in a change in CA-125 levels in only 2/21 patients
Safety: • MorAb-003 was generally well-tolerated; the most common adverse events were fatigue, anemia, and nausea
Lumleian
Commentary:
• MorAb-003 has demonstrated a modest increase in response rate when compared to standard chemotherapies in
treatment of recurrent ovarian cancer; data from ongoing Phase III trials are due in September
Phase II (Completed) Phase III (Ongoing)
Patient Segment: • Recurrent ovarian cancer • Ovarian cancer, in first relapse
Stratification: • Non-randomized, open label • Randomized, double blind
Studies:
(Target Enrollment)
• Two Phase II trials (N = 111, N = 52) • Target enrollment N = 900
Comparator: • Intravenous MorAb-003 alone or MorAb-003 +
paclitaxel + carboplatin
• Carboplatin/cisplatin + taxane
Dosing: • 100 mg/m2 MorAb-003, or 100 mg/m2 MorAb-003 +
175 mg/m2 paclitaxel on
• IV dosing, two different dosages
Duration: • 60 months • 12-24 months
Primary End-Points: • Serologic Response (change in CA125 levels)
• PFS
• OS
• PFS
41
Sources:www.clinicaltrials.gov, Li, J et. al . “Clinical Pharmacokinetics and Exposure-Toxicity Relationship of a Folate-Vinca Alkaloid Conjugate
EC145 in Cancer Patients. J. Clinical Pharmacology. 49 (2009), Naumann et. al, Randomized Phase II trial comparing EC145 and pegylated
liposomal doxorubicin (PLD) in combination, versus alone, in subjects with platinum-resistant ovarian cancer. 2010 ASCO Annual Meeting.
(2010)
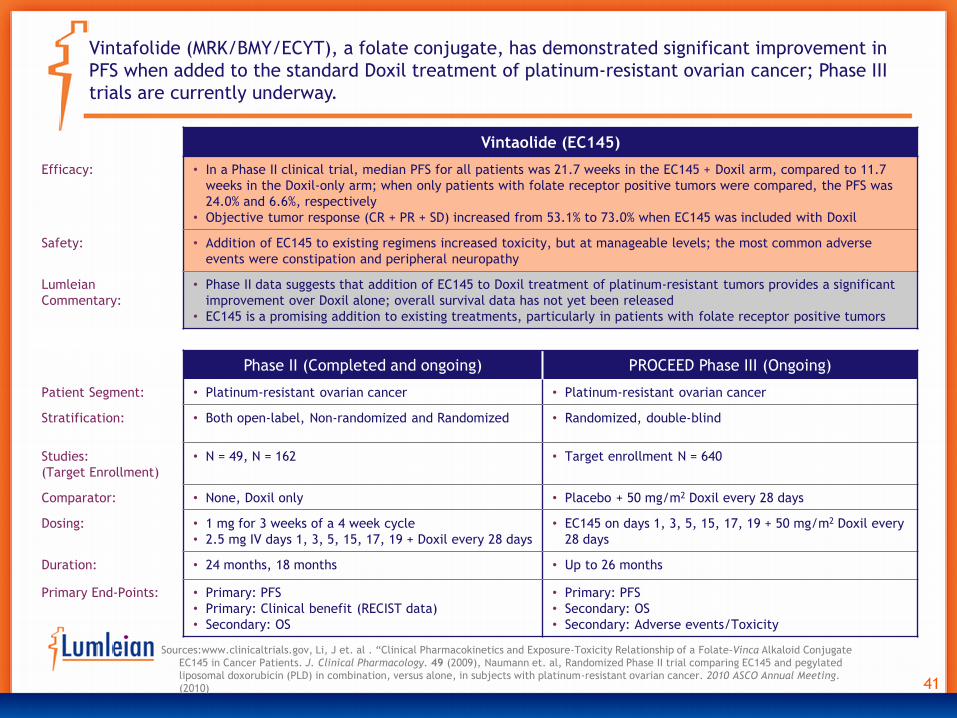
Vintafolide (MRK/BMY/ECYT), a folate conjugate, has demonstrated significant improvement in
PFS when added to the standard Doxil treatment of platinum-resistant ovarian cancer; Phase III
trials are currently underway.
Vintaolide (EC145)
Efficacy: • In a Phase II clinical trial, median PFS for all patients was 21.7 weeks in the EC145 + Doxil arm, compared to 11.7
weeks in the Doxil-only arm; when only patients with folate receptor positive tumors were compared, the PFS was
24.0% and 6.6%, respectively
• Objective tumor response (CR + PR + SD) increased from 53.1% to 73.0% when EC145 was included with Doxil
Safety: • Addition of EC145 to existing regimens increased toxicity, but at manageable levels; the most common adverse
events were constipation and peripheral neuropathy
Lumleian
Commentary:
• Phase II data suggests that addition of EC145 to Doxil treatment of platinum-resistant tumors provides a significant
improvement over Doxil alone; overall survival data has not yet been released
• EC145 is a promising addition to existing treatments, particularly in patients with folate receptor positive tumors
Phase II (Completed and ongoing) PROCEED Phase III (Ongoing)
Patient Segment: • Platinum-resistant ovarian cancer • Platinum-resistant ovarian cancer
Stratification: • Both open-label, Non-randomized and Randomized • Randomized, double-blind
Studies:
(Target Enrollment)
• N = 49, N = 162 • Target enrollment N = 640
Comparator: • None, Doxil only • Placebo + 50 mg/m2 Doxil every 28 days
Dosing: • 1 mg for 3 weeks of a 4 week cycle
• 2.5 mg IV days 1, 3, 5, 15, 17, 19 + Doxil every 28 days
• EC145 on days 1, 3, 5, 15, 17, 19 + 50 mg/m2 Doxil every
28 days
Duration: • 24 months, 18 months • Up to 26 months
Primary End-Points: • Primary: PFS
• Primary: Clinical benefit (RECIST data)
• Secondary: OS
• Primary: PFS
• Secondary: OS
• Secondary: Adverse events/Toxicity

42
Physiology • Ovarian cancer is associated with a variety of
proteins and peptides which could become
recognizable by the immune system
Pathophysiology • Because cancers arise from “self” tissue, the
immune system often does not attack tumor
tissues unless specifically stimulated to do so
Hypothesized
Mechanism
• Immunization against OC-specific peptides can
result in immune activity specifically against
melanoma tumor cells
• A number of different peptides are being tested,
alone and in combination, against OC
• The most advanced ovarian cancer vaccine is
CVac, which is likely to be approved if Phase III
trials replicate promising Phase II results
Phase III • CVac
Phase II • CTL-Vaccine (GNBT) • CDX-1401 (CDLX) • DPX-Survivac (IMV)
• FBP (GALE) • DepoVax (IMV) • P53-SLP (ISA Pharmaceuticals)
• FANG Vaccine (Gradalis) • O-Vax (AVXT)
Phase I • Alpha-Targeted Therapy (Vaxonco, Inc.) • Neuvenge (DNDN), V930/V932 (MRK)
Pipeline
Sources: EvaluatePharma, www.clinicaltrials.gov, http://www.bru.licr.org/brussels/research/iman/iman.html,
A variety of peptides and peptide combinations are currently in clinical trials for treatment of
ovarian cancer; CVac is currently the most advanced, and is likely to be approved due to
efficacy and low toxicity profile.

43 Sources:www.clinicaltrials.gov, “Developing the world’s first Ovarian Cancer Therapy Vaccine” RBC Capital Healthcare Conference (2011)
The MUC1 autologous dendritic cell vaccine CVac has shown promise in early Phase II trial and is
entering phase III as consolidation therapy for patients in primary or secondary remission.
Cvac
Efficacy: Phase IIa trial is completed:
• 21% of patients responded to therapy, 47% of patients had disease stabilization
• CA125 antigen demonstrates therapy response
• PFS: 127 days
Safety: • No therapy-related toxicity
Lumleian
Commentary:
• CVac has demonstrated some therapeutic response, with no toxicity; if Phase III trial data matches the success of
the Phase II trials, FDA approval is likely
• Phase III trials are currently underway, with the goal of maintenance therapy of ovarian cancer patients in primary
or secondary remission
Phase II (Ongoing) Phase III (Ongoing)
Patient Segment: • Patients with Stage III or IV OC who have had a
complete response after first- or second-line therapy
• Patients in CR following first-line therapy
Stratification: • Randomized, open-label • Randomized, double-blind
Studies:
(Target Enrollment)
• N = 60 • N = 750
Comparator: • Observation • Placebo
Dosing: • 10 intradermal vaccine administration
• Every 4 weeks x 7, then every 8 weeks x 3; 52 weeks
• Intradermal injection every 4 weeks for the first 3 doses,
then every 12 weeks for 3 additional doses
Duration: • Up to 60 months • 24 months
Primary End-Points: • PFS and OS
• Immunologic response
• Safety
• PFS
• OS

44
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on ovarian cancer?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is ovarian cancer?
• Epidemiology by geography and risk factors
• Presentation, diagnosis, classification
• Current care paradigm and clinical evidence
• Emerging care paradigm
11 • 12
• 13
• 14
• 15 - 20
• 21
III. Clinical Development Pipeline • Clinical development pipeline mapping
• Traditional chemotherapies
• Anti-Angiogenesis agents
• Kinase Inhibitors
• Folate Receptor Targeting Agents
• Ovarian Cancer Vaccines
23 • 24 – 29
• 30 - 31
• 32 – 36
• 37 – 38
• 39 – 41
• 42 – 43
IV. Commercial Landscape • Estimated use in ovarian cancer of branded therapies
• Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
45 • 46
• 47 - 50
• 51
• 52
• 53 – 56
V. Appendix • Table of Acronyms
• More about Lumleian
• 58
• 59 – 61

45
How large is
the global
market and what
growth
is forecast?
• Global ’11 brand revenue shrank by ~47% to ~$0.3B due to the patent expiration of Gemzar, Taxotere and
Hycamtin, while the supply shortage of Doxil is anticipated to keep the market declining this year; however,
global revenue will increase by ~51% annually to ~$0.7B between ’12 and ’15, largely driven by Avastin’s
approval in EU and new pipeline drug launches
• In the US, the loss of exclusivity of Gemzar, Hycamtin and Taxotere, combined with the effect of the Doxil
shortage, the brand revenue for ovarian cancer dropped ~70% in ’11 and is expected to decline another 68% in
’12; with the end of Doxil’s supply shortage and anticipated new launches, the market will recover to ~$0.3B by
’15 and the ovarian cancer patients are anticipated to grow rapidly due to the aging of “baby-boomers”
• The EU market shrank ~29% to ~$0.1B in ’11, but will recover faster than other regions due to Avastin’s approval
by the EMA
• The Japanese market is small, but promising assets from Takeda and Eisai will increase revenues from ovarian
cancer by ’14
• The rest of world market dropped ~17% in ’11, but will increase ~16% annually between ’12 and ’15, largely
driven by new drug launches
What are launch
forecasts?
• Wall Street consensus estimates forecast new product launches will increase the ’15 global market by ~$280M,
driven largely by anticipated launches for Takeda/Amgen’s TREBANANIB (’14), Eisai’s Farletuzumab (’14) and
Merck/Endocyte’s Vintafolide (’14)
What trends
are driving the
US market?
• Generic carboplatin and paclitaxel continue to dominate patient share, although Avastin has gained patient
share as use in first-line expanded; however, negative Phase III data will cap Avastin penetration
• In the three months ending Dec ’11, total promotional spend grew ~2.7%, with no direct-to-consumer (DTC)
spend observed; Doxil dominated the healthcare professional (HCP) spend by ~52%, though recent LoE of Gemzar
and Taxotere has resulted in a surge of commercial spend on generic chemotherapy drugs
• After the LoE in May ‘10, Gemzar reduced its promotional force; however, the producers of generics increased
commercial spend in Q4, emphasizing the availability of generic gemcitabine for cheaper oncology treatment
• Taxotere increased HCP spend in March ’11, 2 months before its LoE and started a ~0.1M campaign in November
to forestall generic penetration; however, Hospira increased journal advertisements for generic docetaxel
immediately after the LoE of Taxotere in May and June
• As the only chemotherapy drug with patent protection in ovarian treatment, Doxil’s promotional spend
dominated the market; the messaging emphasized the support by J&J for ovarian cancer patients
Executive Summary: Commercial Landscape

46
Sources: SDI (IMS) Oncology Tracker data
For the commercial analysis, we used the market share of each drug used in ovarian cancer patients, multiplied by that agent’s total revenue numbers, to derive the commercial value of the ovarian cancer market.
3.4%
4.4%
3.4%
33.9%
36.1%
3.9%
7.5%
7.4%
11.6%
12.4%
0 50 100 150 200
Paclitaxel Protei-bound
Vinorelbine
Cisplatin
Doxorubicin Liposomal
Topotecan
Docetaxel
Bevacizumab
Gemcitabine
Carboplatin
Paclitaxel
Patient (Thousands)
Other Cancer
Ovarian Cancer
Oncology drug uses for Ovarian Cancer based on patients treated in 2011 US
Noets: Revenues for each drug in ovarian cancer are calculated based on percentage of drug used in ovarian cancer as compared to other cancers.

47
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
Global ’11 brand revenue shrank by ~47% to ~$0.3B due to the patent expiration of Gemzar, Taxotere and Hycamtin, while the supply shortage of Doxil is anticipated to keep the market declining this year; however, global revenue will increase by ~51% annually to ~$0.7B between ’12 and ’15, largely driven by Avastin’s approval in EU and new pipeline drug launches.
’11 Sales ($B) ’10–’11A ’11-’12F ’12–’15F
CAGR
Global &
Pipeline $0.3 -47.3% -20.6% 51.1%
US $0.1 -70.5% -68.4% 138.0%
EU $0.1 -29.0% 7.6% 35.6%
JP $0.0 -16.3% -20.7% 18.1%
RW $0.0 -17.2% -19.1% 15.5%
Recent and Anticipated New Product Launches – Global
• Merck/Endocyte’s Vintafolide (’14)
• Eisai’s Farletuzumab (’14)
• Takeda/Amgen’s Trebananib (’14)
Recent and Anticipated Line Extensions
• EU: Avastin (approved for Ovarian Cancer 12/11)
Recent and Anticipated Loss of Exclusivity
• US: Gemzar (05/10), Taxotere (05/11), Hycamtin (05/11),
Doxil (10/09, extended to 05/14)
• EU: Taxotere (11/10)
• JP: Taxotere (06/12)
Ovarian Cancer’s Global Brand Revenue ($B)
Actual: Solid bars Consensus Wall Street Forecast: Hashed bars
$0.5 $0.5
$0.3 $0.2
$0.3
$0.6
$0.7
$0.0
$0.4
$0.8
09A 10A 11A 12F 13F 14F 15F
EU
US
JP RW
Updated: 05/30/12
Global
Pipeline
Notes: Branded sales excludes generic revenues; Pipeline includes: Merck/Endocyte’s Vintafolide (’14), Eisai’s Farletuzumab (’14) and
Takeda/Amgen’s Trebananib (’14)

48
’11 Revenue
($B) ’10–’11A ’11-’12F
’12–’15F
CAGR
United States $0.1 -70.5% -68.4% 138.0%
Doxil $0.0 -50.0% -71.4% 91.3%
Gemzar $0.0 -90.2% -64.6% -26.3%
Hycamtin $0.0 -92.2% -10.0% -12.6%
Taxotere $0.0 -67.5% -74.9% -33.5%
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
The US loss of exclusivity of Gemzar, Hycamtin and Taxotere, combined with the effect of the
Doxil shortage, the US brand revenue for ovarian cancer dropped ~70% in ’11 and is expected to
decline another 68% in ’12; with the end of Doxil’s supply shortage and anticipated new
launches, the market will recover to ~$0.3B by ’15.
2012Q1
Revenue ($M) Q4A–Q3A Q4A–2012Q1A
United States $3.4 -19.2% -38.4%
Doxil $2.4 0.0% -30.0%
Gemzar $0.0 -59.5% -129.4%
Hycamtin $0.4 -33.3% -75.0%
Taxotere $0.6 -50.6% -20.5%
2011 Ovarian Cancer’s United States Brand Revenue ($M)
Actual: Solid bars Wall Street Consensus Forecast: Hashed bars Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
$0.2 $0.2
$0.1
$0.0 $0.1
$0.2
$0.3
$0.0
$0.2
$0.4
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
Updated: 05/30/12
$35
$22
$7 $5 $3
$0
$25
$50
Q1A Q2A Q3A Q4A 2012Q1A
Updated: 05/30/12
US
Pipeline
Ovarian Cancer’s United States Brand Revenue ($B)
Notes: Branded sales excludes generic revenues; Pipeline includes: Merck/Endocyte’s Vintafolide (’14), Eisai’s Farletuzumab (’14) and
Takeda/Amgen’s Trebananib (’14)
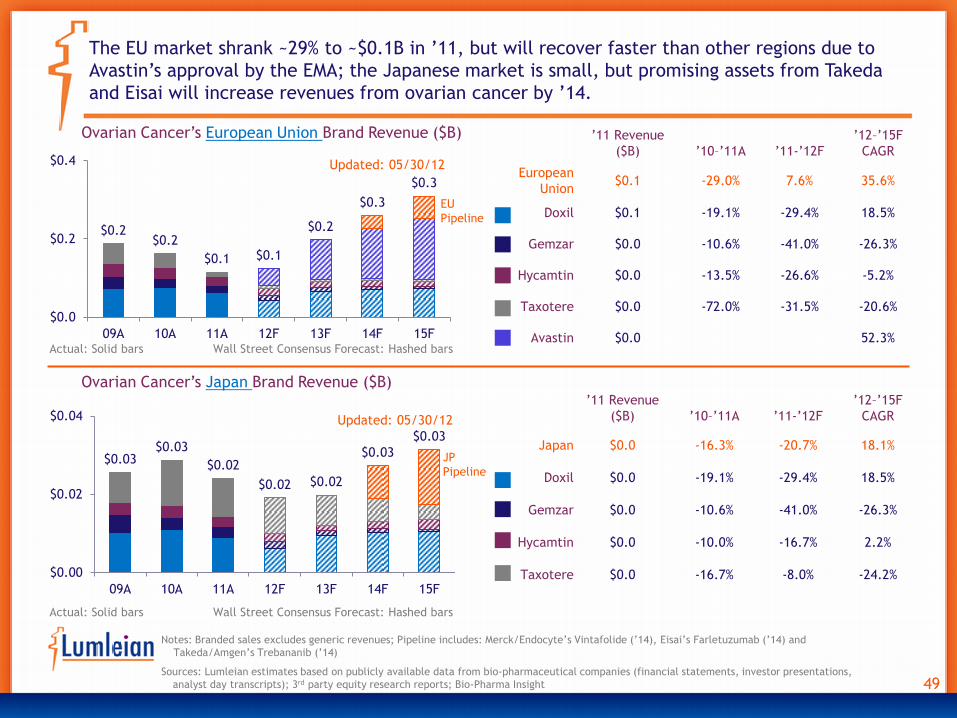
49
$0.2 $0.2
$0.1 $0.1
$0.2
$0.3
$0.3
$0.0
$0.2
$0.4
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
The EU market shrank ~29% to ~$0.1B in ’11, but will recover faster than other regions due to
Avastin’s approval by the EMA; the Japanese market is small, but promising assets from Takeda
and Eisai will increase revenues from ovarian cancer by ’14.
’11 Revenue
($B) ’10–’11A ’11-’12F
’12–’15F
CAGR
European
Union $0.1 -29.0% 7.6% 35.6%
Doxil $0.1 -19.1% -29.4% 18.5%
Gemzar $0.0 -10.6% -41.0% -26.3%
Hycamtin $0.0 -13.5% -26.6% -5.2%
Taxotere $0.0 -72.0% -31.5% -20.6%
Avastin $0.0 52.3% Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
Updated: 05/30/12
Updated: 05/30/12
EU
Pipeline
’11 Revenue
($B) ’10–’11A ’11-’12F
’12–’15F
CAGR
Japan $0.0 -16.3% -20.7% 18.1%
Doxil $0.0 -19.1% -29.4% 18.5%
Gemzar $0.0 -10.6% -41.0% -26.3%
Hycamtin $0.0 -10.0% -16.7% 2.2%
Taxotere $0.0 -16.7% -8.0% -24.2%
$0.03 $0.03
$0.02
$0.02 $0.02
$0.03
$0.03
$0.00
$0.02
$0.04
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
Ovarian Cancer’s European Union Brand Revenue ($B)
Ovarian Cancer’s Japan Brand Revenue ($B)
JP
Pipeline
Notes: Branded sales excludes generic revenues; Pipeline includes: Merck/Endocyte’s Vintafolide (’14), Eisai’s Farletuzumab (’14) and
Takeda/Amgen’s Trebananib (’14)

50
Updated: 05/30/12
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
The rest of world market dropped ~17% in ’11, but will increase ~16% annually between ’12 and
’15, largely driven by new drug launches.
Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
’11 Revenue
($B) ’10–’11A ’11-’12F
’12–’15F
CAGR
Rest of World $0.0 -17.2% -19.1% 15.5%
Doxil $0.0 -19.1% -29.4% 18.5%
Gemzar $0.0 -10.6% -41.0% -26.3%
Hycamtin $0.0 -10.0% -16.7% 2.2%
Taxotere $0.0 -18.6% -1.3% -2.7%
$0.05 $0.05
$0.04
$0.04 $0.04
$0.05
$0.06
$0.00
$0.03
$0.06
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
Ovarian Cancer’s Rest of World Brand Revenue ($B)
Notes: Branded sales excludes generic revenues; Pipeline includes: Merck/Endocyte’s Vintafolide (’14), Eisai’s Farletuzumab (’14) and
Takeda/Amgen’s Trebananib (’14)

51
$0.0
$0.2
$0.4
12F 13F 14F 15F
Thousa
nds
$0.0
$0.1
$0.2
12F 13F 14F 15F
Thousa
nds
$0.17
$0.28
$0.0
$0.1
$0.2
$0.3
$0.4
09A 10A 11A 12F 13F 14F 15F
Vintafolide
Trebananib
Farletuzumab
Sources: Consensus estimates based on publicly available equity research forecasts that have been updated in the past 12 months (since
02/15/11); Consensus estimate is the ‘straight line’ average with each bank’s forecast weighted equally
Notes: These forecasts are not representative of Lumleian’s viewpoint; Ad-hoc Lumleian develops its own forecasts for clients based on its
proprietary analytics and research
Global Pipeline Assets Wall Street Consensus Forecast ($B)
Wall Street consensus estimates forecast new product launches will increase the ’15 global
market by ~$280M, driven largely by anticipated launches for Takeda/Amgen’s Trebananib (’14),
Eisai’s Farletuzumab (’14) and Merck/Endocyte’s Vintafolide (’14).
Updated: 05/30/12
15F Consensus: $0.12B 15F Consensus: $0.13B
Wall Street Consensus Forecast: Hashed bars
Global Takeda/Amgen’s Trebananib
Equity Research Forecasts ($B)
Global Eisai’s Farletuzumab
Equity Research Forecasts ($B)

52
0%
50%
100%
Apr-
11
May-1
1
Jun-1
1
Jul-
11
Aug-1
1
Sep-1
1
Oct-
11
Nov-1
1
Dec-1
1
Jan-1
2
Feb-1
2
Mar-
12
Notes: Patient share includes both branded and generic products; Share Change compares the share for 03/12 vs. 1 month, 3 months, and 12
months ago; MAT(Moving Annual Total) growth compares the patient share for past 12 months vs. the patient share for previous 12 months;
QOQ(Ouarter on Quarter) growth compares the patient share for the 3 months 1/12-3/12 vs. the 3 months 1/11-3/11
Generic carboplatin and paclitaxel continue to dominate patient share, while doxorubicin loses
patient share due to a manufacturing shortage; although Avastin has gained patient share as a
first-line treatment, negative Phase III data will cap Avastin penetration.
Share Share Change
(% points) Growth Rate
Mar-12 1 mon 3 mon 12 mon QOQ MAT
Total TRx -1.6% -4.3%
doxorubicin
liposomal 4.3% 0.1 0.3 -8.0 -64.0% -47.9%
Gemcitabine 18.6% -0.6 0.0 4.7 27.5% 6.5%
Topotecan 7.7% -1.0 -5.2 -2.2 -14.8% 16.0%
Paclitaxel 19.6% -1.2 1.6 2.1 6.0% -8.5%
Docetaxel 6.4% -0.1 1.5 1.9 32.0% 1.7%
Bevacizumab 13.0% -2.0 -3.5 -0.3 8.0% 23.9%
Carboplatin 20.2% 4.5 4.7 1.3 -2.2% -9.7%
Cisplatin 3.1% 0.8 1.1 0.0 -17.1% -33.5%
OTHER 7.0% -0.4 -0.5 0.6 13.3% 10.3%
US Ovarian Cancer’s Patient Share by drug Updated: 05/30/12
Sources: SDI (IMS) Oncology Tracker data

53
0%
50%
100%
Apr-
11
May-1
1
Jun-1
1
Jul-
11
Aug-1
1
Sep-1
1
Oct-
11
Nov-1
1
Dec-1
1
Jan-1
2
Feb-1
2
Mar-
12
Notes: Patient share includes both branded and generic products; Share Change compares the share for 03/12 vs. 1 month, 3 months, and 12
months ago; MAT(Moving Annual Total) growth compares the patient share for past 12 months vs. the patient share for previous 12 months;
QOQ(Ouarter on Quarter) growth compares the patient share for the 3 months 1/12-3/12 vs. the 3 months 1/11-3/11
For 1st line treatment, the paclitaxel+carboplatin and gemcitabine+carboplatin combinations
dominate the treatment regeime; gemcitabine, topotecan and Avastin began to penetrate the
market as monotherapies within the last 12 months.
Share Share Change
(% points) Growth Rate
Mar-12 1 mon 3 mon 12 mon QOQ MAT
Total TRx 2.0% -0.9%
Doxorubicin 2.7% 1.2 1.4 -9.6 -83.1% -65.1%
+carboplatin 1.9% 0.3 0.7 -3.1 -58.5% -24.2%
Gemcitabine 12.6% -0.8 3.7 7.1 118.2% 54.3%
+carboplatin 14.2% -0.5 3.5 4.5 52.7% 8.3%
+cisplatin 1.6% -0.4 -0.1 -0.2 21.5% -11.1%
Topotecan 9.8% -1.2 -4.5 2.7 55.2% 41.5%
Docetaxel 0.0% -0.8 -0.9 -1.0 -52.3% 0.5%
+carboplatin 3.9% 0.9 0.3 0.8 6.6% -8.1%
Bevacizumab 7.5% -2.4 -1.9 2.7 134.8% 148.1%
+carboplatin
& paclitaxel 2.6% 0.1 0.0 -2.1 -34.8% 15.0%
Paclitaxel 1.6% 0.3 0.3 -0.2 -27.9% -25.1%
+carboplatin 23.4% 3.2 2.7 -1.8 -12.6% -21.6%
Carboplatin 0.9% -0.5 -0.9 0.4 114.4% 65.6%
Other 17.3% 0.4 -4.0 0.0 -5.8% 15.0%
US Ovarian Cancer’s Patient Share by
1st line treatment regimen Updated: 05/30/12
Sources: SDI (IMS) Oncology Tracker data

54
0%
50%
100%
Apr-
11
May-1
1
Jun-1
1
Jul-
11
Aug-1
1
Sep-1
1
Oct-
11
Nov-1
1
Dec-1
1
Jan-1
2
Feb-1
2
Mar-
12
Notes: Patient share includes both branded and generic products; Share Change compares the share for 03/12 vs. 1 month, 3 months, and 12
months ago; MAT(Moving Annual Total) growth compares the patient share for past 12 months vs. the patient share for previous 12 months;
QOQ(Ouarter on Quarter) growth compares the patient share for the 3 months 1/12-3/12 vs. the 3 months 1/11-3/11
Regimens containing gemcitabine and paclitaxel still lead the 2nd line treatment market;
paclitaxel+carboplatin have lost share to paclitaxel monotherapy.
Share Share Change
(% points) Growth Rate
Share
Change vs.
1st line
Mar-12 1 mon 3 mon 12 mon QOQ MAT MAT
Total TRx -9.1% -11.4%
doxorubicin 3.5% -0.1 0.6 -14.0 -83.7% -64.0% 1.6
+carboplatin 0.9% 0.6 0.9 -4.4 -86.6% -60.8% -1.4
gemcitabine 7.3% -2.6 -4.8 0.2 3.3% -11.9% -0.3
+carboplatin 11.0% 0.8 2.1 1.3 -3.5% -19.2% -2.9
+cisplatin 3.5% -0.6 -1.6 0.7 15.7% -2.5% 1.8
topotecan 7.8% -0.6 -4.4 -1.3 -27.2% -2.6% 0.2
docetaxel 3.2% -0.6 1.5 -0.6 18.9% -6.7% 2.2
+carboplatin 4.9% 0.9 2.7 1.5 6.0% -5.4% 0.8
bevacizumab 7.6% -0.5 2.1 4.4 145.4% 95.7% -1.4
+carboplatin
& paclitaxel 1.1% -0.7 -0.8 -1.4 -38.6% -4.7% -1.9
paclitaxel 13.5% 0.9 6.7 6.4 49.8% 10.7% 6.9
+carboplatin 8.3% 0.3 -1.4 -0.8 -17.1% -17.4% -12.0
carboplatin 4.7% 1.7 1.7 2.4 52.4% 72.3% 1.5
other 22.7% 0.4 -5.2 5.5 22.2% 5.4% 4.8
US Ovarian Cancer’s Patient Share by
2nd line treatment regimen Updated: 05/30/12
Sources: SDI (IMS) Oncology Tracker data

Note: Healthcare Professional (HCP) spend includes marketing to physicians, nurse practitioners, physician assistants through marketing & event promotions,
journals, and online promotions; Direct to Consumer (DTC) includes marketing channels in television, radio, newspapers, magazines, outdoor advertisements,
and internet; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11
Sources: SDI (IMS) Promotion Audits, Kantar Media Research 2010 - 2011
In the three months ending Dec ’11, total promotional spend grew ~2.7%, with no direct-to-
consumer (DTC) spend observed; Doxil dominated HCP spend by ~52%, though the recent LoE of
Gemzar and Taxotere resulted in a surge of commercial spend on generic chemotherapy drugs.
$0.0
$0.2
$0.4
J F M A M J J A S O N D
2011 Healthcare Professional (HCP) Spend ($M)
Updated: 05/30/12
Share of Wallet Growth Rate
2011 3MR
HCP 100.0% 2.7%
DTC - -
Share of Voice CAGR
HCP 2011 3MR
Gemcitabine 3.1% -13.7%
Gemzar 7.9% -
Docetaxel 8.9% -44.7%
Taxotere 13.8% -
Topotecan 14.2% -
Doxil 52.0% -51.7%

0
0.09
0.18
J F M A M J J A S O N D
2011 Total Promotional Spend ($M) Gemzar
Gemcitabine HCl
Share of
voice
HCP 0.7% 49.1% - - - - - - 82.3% 8.7% 10.4% -
DTC - - - - - - - - - - - -
Notes: Updated: 05/30/12
Sources: SDI Promotion Audits, Kantar Media Research
After the LoE in May ’10, Gemzar reduced its promotional force; however, the
producers of generics increased commercial spend in Q4, emphasizing the
availability of generic gemcitabine for cheaper oncology treatment.
11/11
Hospira Inc
One for all. As
the complexity of
healthcare
evolves, Hospira
Gemcitabine
injection delivers
one solution for
all. GEMCITABINE
HCL
09/11
App Pharma
Expanding APP's
leading oncology
portfolio:
Gemcitabine
200mg, 1 gram,
and 2 gram. A
broad spectrum
of multisource
oncology
therapeutics.
GEMCITABINE
HCL
09/11
Sagent Phar
The new rock
stars.
Introducing
Gemcitabine
for injection,
USP.
GEMCITABINE
HCL
Total Growth
2011 3MR
HCP $0.18M -13.7%
DTC - -
Generic Gemcitabine Penetration
09/11
Teva
Now available
from Teva...
Gemcitabine for
injection, USP.
AP Rated to
Gemzar for
injection.
GEMCITABINE
HCL

0
0.1
0.2
J F M A M J J A S O N D
2011 Total Promotional Spend ($M)
Taxotere-HCP
Docetaxel-HCP
Share of
voice
HCP - 9.8% 67.4% - 48.6% 4.1% 22.2% - 17.7% - 89.6% -
DTC - - - - - - - - - - - -
Notes: Updated: 05/30/12
Sources: SDI Promotion Audits, Kantar Media Research
Taxotere increased HCP spend in March ’11, 2 months before its LoE and started a
~$0.1M campaign in November to forestall generic penetration; however, Hospira
increased journal advertisements for generic docetaxel immediately after the LoE
of Taxotere in May and June.
Total Growth
2011 3MR
HCP $0.4M 851.9%
DTC - -
Generic Docetaxel Penetration
06/11
Hospira Inc
Single vial Docetaxel
injection. Multidose
vials. DOCETAXEL
05/11
Hospira Inc
Single vial Docetaxel
injection. Multidose
vials. DOCETAXEL

0
0.15
0.3
J F M A M J J A S O N D
Millions
2011 Total Promotional Spend ($M)
Share of
voice
HCP 55.8% - 32.6% 100.0% 51.4% 95.9% 77.8% 100.0% - 91.3% - -
DTC - - - - - - - - - - - -
Notes: Updated: 05/30/12
Sources: SDI Promotion Audits, Kantar Media Research
As the only chemotherapy drug with patent protection in ovarian treatment, Doxil’s
promotional spend dominated the market; the messaging emphasized the support
by J&J for ovarian cancer patients.
HCP
For your patients receiving
or about to start
treatment with Doxil for
recurrent ovarian cancer
or relapsed/refractory
multiple myeloma... DOXIL
HCP
For your patients receiving or
about to start treatment with
Doxil for recurrent ovarian
cancer or relapsed/refractory
multiple myeloma, Doxil
C.A.R.E.S. provides help and
support. DOXIL
HCP
Total Growth
2011 3MR
HCP $0.9M -51.7%
DTC - -

59
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on ovarian cancer?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is ovarian cancer?
• Epidemiology by geography and risk factors
• Presentation, diagnosis, classification
• Current care paradigm and clinical evidence
• Emerging care paradigm
11 • 12
• 13
• 14
• 15 - 20
• 21
III. Clinical Development Pipeline • Clinical development pipeline mapping
• Traditional chemotherapies
• Anti-Angiogenesis agents
• Kinase Inhibitors
• Folate Receptor Targeting Agents
• Ovarian Cancer Vaccines
23 • 24 – 29
• 30 - 31
• 32 – 36
• 37 – 38
• 39 – 41
• 42 – 43
IV. Commercial Landscape • Estimated use in ovarian cancer of branded therapies
• Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
45 • 46
• 47 - 50
• 51
• 52
• 53 – 56
V. Appendix • Table of Acronyms
• More about Lumleian
• 58
• 59 – 61

60
Table of Acronyms
AEZS Aeterna Zentaris
AMG Amgen
ARRY Array Biopharma
AVXT AVAX Technologies
AZN AstraZeneca
BAYN Bayer
bFGF Basic Fibroblast Growth Factor
BI Boerhinger-Ingelheim
BMY Bristol-Myers Squibb
BRCA1/2 Breast Cancer 1/2
CA-125 Cancer Antigen 125
CELG Celgene
CLVS Clovis Technology, Inc
CTIC Cell Therapeutics, Inc.
CYTK Cytokinetics, Inc.
DNDN Dendreon Corporation
DTC Direct to Consumer
EGFR Epidermal Growth Factor Receptor
ENMD EntreMed, Inc.
EU European Union
EXEL Exelexis, Inc
FDA Food and Drug Administration
FT Fallopian Tubes
GALE Galena Biopharma
GSK GlaxoSmithKline
HSP Heat Shock Protein
IMGN ImmunoGen, Inc.
IMV ImmunoVaccine Technologies
INFI Inifinity Pharmaceuticals
INO Inovio Pharmaceuticals
IP Intraperitoneal
IV intraveneous
JNJ Johnson and Johnson
JP Japan
K thousand
kg Kilogram
LLY Eli Lilly
LoE Loss o Exclusivity
LOR Lorus Therapeutics, Inc.
M Millions
MAb monoclonal antibody
mcg microgram
mg Milligrams
MoA Mechanism of Action
MRK Merck
NDA New Drug Application
NVLT Novelos Therapeutics
NVS Novartis
OC Ovarian Cancer
OGXI OncoGene X
ONCY Oncolytics Biotech, Inc.
ORR Overall Response Rate
OS Overall Survival
OXGN OXiGENE
OSI OSI Pharmaceuticals
PARD Poniard Pharmaceuticals
PDGF Platelet Dervied Growth Factor
PFS Progression-Free Survival
Ph.D. Doctor of Philosophy
PlGF Placental Growth Factor
PLD Pegylated liposoma doxorubicin
Q1 First Quarter
Q2 Second Quarter
Q3 Third Quarter
Q4 Fourth Quarter
QD Quaque Die (Once Daily)
REGN Regeneron Pharmaceuticals
RHHBY Roche
ROI Return on Investment
RW Rest of World
SNSS Sunesis Pharmaceuticals, Inc.
SNTA Synta Pharmaceuticals Corp.
SNY Sanofi
TLN Thallion Pharmaceuticals
VEGF Vascular Endothelial Growth Factor

61
• Frank Deane, Ph.D. is a Director of Decision Science and Founder of Lumleian. Frank has over ten years experience
working with life science companies and concurrently holds an appointment in the department of strategy at the
Carroll School of Management, Boston College, where he teaches ‘Strategic Issues in Pharma and Bio-Tech,’ to MBA
students. Prior to founding Lumleian, Frank was a director with Leerink Swann and a case team leader with Bain,
where he gained substantial operational experience growing and operating a diverse set of businesses. Frank
entered consulting after spending three years in the bio-pharmaceutical industry with Eli Lilly, supporting portfolio
optimization and business unit strategic planning. He began his career, as a quantitative risk analyst working at
BlackRock. Frank earned a Ph.D. in econometrics from the Krannert School of Management at Purdue University,
where his dissertation focused on applying game theory and statistical modeling to optimize pharmaceutical sales
and marketing resources. Frank has a bachelor of arts in economics from Princeton University.
As a leadership team, we designed Lumleian’s business model based on our collective
experience in: academic R&D, bio-pharmaceutical industry, equity research and strategy
consulting …
• Mark Hochstetler, MBA is a Director of Decision Science at Lumleian. Mark has over ten years experience working
with life science companies. Prior to joining Lumleian, Mark served as the CFO at OPK Biotech, which focuses on
developing oxygen therapeutics for the treatment of anemia, ischemia, and trauma. Before segueing to industry,
Mark spent 5 years as a strategy consultant and equity research analyst at Leerink Swann, where he covered:
Array, Arqule, Ariad, Celgene, Chelsea, Cougar, Cubist, Genentech, GTx, Hana, Idenix, InterMune, Kosan,
Millennium, MGI Pharma, Onyx, Poniard and Vertex. Mark earned an MBA from Duke University’s Fuqua School of
Business with a concentration in health sector management. Mark has a bachelor of arts in political science from
Stanford University.
• Sarah Haigh Molina, Ph.D. is a Manager of Decision Science at Lumleian, where she leads the Academia and Non-
profit practice. Sarah has over ten years experience working and researching in the life sciences. Prior to joining
Lumleian, Sarah was an Assistant Professor of Medicine at Boston University School of Medicine where she served
as the Director of High-throughput Screening. Before returning to academia, Sarah was US Operations Manager at
Molecular Cytomics. Sarah earned a Ph.D. in biology from York University, an MBA from Boston University with a
concentration in entrepreneurship, and a bachelors of science in biochemistry from Dundee University.

62
… Having lived the client experience, we know quality is paramount, and pioneered our
approach with quality and process efficiency as dual mantras.
• Jean Kung, M.Eng., MBA as Manager of Process Efficiency and Quality Control oversees day-to-day operations and
finances at Lumleian and has over five years experience working in the life sciences. Jean designed the process
by which Lumleian efficiently and effectively creates and quarterly updates its disease state primers and serves as
the final point of quality control. Prior to joining Lumleian, Jean served as a contract project manager to various
life science clients. Before entrepreneurship, Jean was a clinical research associate at Health Policy Associates
and a researcher at the Harris Orthopedic Biomaterials and Biomechanics Laboratory, Massachusetts General
Hospital. Jean earned a masters of science in biological engineering from Cornell University and an MBA in the
Health Sector Management Program from Boston University with a concentration in operations and technology
management. Jean has a bachelor of science in biological engineering, also from Cornell University.
• Morgen Caroll, MBA as Manager of the Customer Experience at Lumleian, aspires to provide Lumleian's clients with
superior care and service based on their particular needs. Morgen brings over five years life science experience
and has a background in Marketing, Sales, and Public Relations. Prior to joining Lumleian, Morgen worked at
GlaxoSmithKline, with responsibility for the company’s flagship cardiology and endocrinology products. At
GlaxoSmithKline, Morgen was a primary care and specialty care sales representative while serving as a liaison
between product management teams and field sales. As a representative, Morgen consistently ranked in the top
10% of GSK’s sales force, despite working in an inner city territory with significant access challenges. Prior to
entering the life sciences Morgen worked on the sales and marketing staff at Philadelphia Magazine and Food &
Wine Magazine. Morgen earned an MBA from the Villanova School of Business with a concentration in marketing,
and a bachelor of arts in English from Gettysburg College.
• Qingwei Sun, M.Eng., MS as a Decision Science Analyst oversees secondary data collection, synthesis and analysis
and designed analytical methodologies fundamental to Lumleian’s knowledge management platform. KM
database. Using meta-analysis method, he aggregates the clinical and commercial data required to generate
Lumleian’s disease state primers. His work has wide application in product development, portfolio management,
and investment strategy for both large pharmaceutical companies and emerging bio-techs. Qingwei, who is fluent
in Chinese and Japanese, leads our work with Asian clients. Qingwei joined Lumleian after obtaining a Master of
Science degree from Harvard School of Public Health. He earned both Bachelor and Master of Engineering degrees
from Kyoto University, Japan, concentrating in materials science.

63
We recruit decision scientists explicitly for their expertise and relevant experience across
the gamut of major therapeutic areas and disease states.
• Whitney Amyot, Ph.D. as Decision Scientist focusing on infectious disease leverages her expertise in
scientific investigation and infectious disease to support primary and secondary research for strategic
decision making with biopharmaceutical clients and investors. She has more than ten years of experience in
scientific research, including positions at Atlanta’s Veteran Affairs hospital and in the pharmacology
department at Emory University School of Medicine. In her current role Whitney provides a broad knowledge
base to ensure Lumleian is up to date on current discovery and clinical trends. Whitney earned a Ph.D. in
Molecular Microbiology from Tufts University Sackler Graduate School of Biomedical Sciences where her
dissertation focused translocation in the becterium Legionella pneumophila. Whitney has a Bachelor of
Science degree in Biology from Emory University.
• Alice S. Kaanta, Ph.D. as Decision Scientist focusing on oncology is responsible for leading a team of decision
scientists in reviewing the scientific, clinical and regulatory landscape in numerous oncology indications.
Alice has over ten years of experience in scientific research, in both academia and industry, where her
primary focus has been on cancer research. Alice earned her Ph.D. in Biological and Biomedical Sciences
from Harvard University. At Harvard, Alice worked in the Brugge Lab studying the regulation of pro-
apoptotic Bcl-2 family member Bim in breast cancer progression and in the Neel lab where she identified and
characterized a novel multi-potent mammary progenitor with pregnancy-specific activity. Alice earned dual
bachelor of science degrees in Biology and Physics from the Massachusetts Institute of Technology.