discussion document - saavi home · discussion document ... 2.4. voluntariness and freedom from...
TRANSCRIPT

Page -1-
DISCUSSION DOCUMENT
Guidelines for the development of culturally sensitive approaches to obtaining informed consent for participation in HIV vaccine-related trials
Linda M Richter Graham C Lindegger
Quarraisha Abdool Karim* Nolwazi Gasa*
School of Psychology, University of Natal, Private Bag X01, SCOTTSVILLE, South Africa
[email protected] Phone: 09-27-331-2605016; Fax: 09-27-331-2605809
* Medical Research Council (Durban)
Commissioned by UNAIDS
Submitted February 1999 Revised May 1999

Page -2-
CONTENTS
PRE-AMBLE......................................................................................................................................3
PART 1: OVERVIEW .....................................................................................................................3 1.1. INTRODUCTION: ...........................................................................................................3 1.2. LITERATURE REVIEW:..................................................................................................4 1.3. CONCEPTUAL FRAMEWORK FOR PROCEDURES TO OBTAIN INFORMED CONSENT ..................................................................................................................................12 1.4. REFERENCES ...........................................................................................................14
PART 2: PRACTICAL GUIDE .....................................................................................................23 2.1. PREPARATION FOR INFORMED CONSENT: ...........................................................23 2.2. INFORMED CONSENT MATERIAL PREPARATION: ................................................24 2.3. UNDERSTANDING AND DECISION MAKING: .........................................................26 2.4. VOLUNTARINESS AND FREEDOM FROM COERCION:..........................................29 2.5. CONSENT ......................................................................................................................29 2.6. EVALUATION OF THE CONSENT PROCESS AND CONDITIONS: .........................32 2.7. PROTOCOL FOR IMPLEMENTING A CULTURALLY SENSITIVE INFORMED CONSENT PROCESS ................................................................................................................32 2.8. TASKS AND RESPONSIBILITIES FOR IMPLEMENTATION OF INFORMED CONSENT PROCEDURES: ......................................................................................................37 2.9. TIME LINE: ...................................................................................................................40 2.10. FLOW CHART OF ACCOUNTABILITY AND ANSWERABILITY............................41 2.11. BUDGET....................................................................................................................42
PART 3: PROCEEDINGS OF UNAIDS MEETING.....................................................................43
Page -3-
PRE-AMBLE. The document, which follows, is an attempt to set out some recommended guidelines for the development of culturally sensitive approaches to obtaining informed consent for participation in HIV vaccine trials. These guidelines are set out especially against the background of populations likely to be involved in HIV vaccines trials in developing countries, especially in Africa, Latin America and Asia. However, the authors have also attempted to bear in mind that vaccine trials are already under way in developed countries such as the USA, and to consider the application of principles of informed consent in these countries as well. The authors are aware that the guidelines for the ethics of HIV vaccine trials in developing countries will not always be the same as those in developed countries, and that the guiding principles may, at times, not be universally applicable. It would seem to us that this is in the very nature of “culturally sensitive” approaches to ethical issues such as informed consent. In essence, the authors have suggested that it is the “spirit of informed consent” which needs to be understood, implemented and honoured throughout HIV vaccine trials. It is argued that ethics is an integral part of medical research, rather than an add-on quality, and should be considered at every stage of research planning, implementation and evaluation. It is also argued that ethical considerations should apply to all role players in vaccine trials, including funders, scientific team, community advisory board and participants. These guidelines attempt to first identify some of the major ethical principles governing informed consent in HIV vaccine trials and to then proceed to develop a series of practical guidelines for each aspect of informed consent, based on these principles. Whilst the authors have attempted to develop a series of specific recommendations for the implementation of informed consent, they are aware that the exact form of the informed consent procedures and the way in which these are implemented will vary a great deal, dependent on local norms and customs as well as the medico-legal framework for the implementation of such medical trials. Throughout, it is the “spirit of informed consent” which the authors have attempted to emphasize and encourage. PART 1: OVERVIEW 1.1. INTRODUCTION: This paper, Approaches to obtain informed consent, is one of three documents commissioned by UNAIDS to address some specific ethical, social and behavioural implications of HIV vaccine-related trials, with particular reference to potential study populations in Africa, Latin America and Asia. The other two documents are Monitoring risk behaviour in HIV vaccine trials and Explore willingness to participate in trials. The latter papers are preceded by other UNAIDS initiatives to address these implications, including a working document by Dr MJ Paris Spink entitled Social and behavioural dimensions of HIV vaccine trials, and regional workshops in Ouro Pretro, Bangkok and Entebbe to discuss ethical issues in preventive HIV vaccine trials.
Page -4-
1.2. LITERATURE REVIEW: ...ethical systems do not exist in order to eliminate ethical discourse, they provide a framework for such discourse. Christakis (1992, p.108)
1.2.1. INFORMED CONSENT IN THE CONTEXT OF BIOMEDICAL ETHICS Informed consent cannot be discussed in isolation from ethics in general, nor from other ethical issues in vaccine-related trials. This is because the informed consent document is an expression of a larger contract governing the relationship between science and society, and embodied in the relationship between the scientific team and the volunteer1. As a result, obtaining written informed consent cannot compensate for comprises to the principles of respect for persons, beneficence, and justice in other respects of a trial. One of the problems with current approaches to informed consent is that consent has been reduced to a technical issue, often removed from wider ethical considerations. The history of informed consent is well documented (Katz, 1972). Landmarks in its development from the time of its formulation in the 1947 Nuremberg Code are: the International Covenant on Civil and Political Rights (Article 7) adopted by the United Nations General Assembly in 1966; the Belmont Report Ethical Principles and Guidelines for the Protection of Human Subjects of Research (1979); the World Medical Association Declaration of Helsinki (most recently revised in 1989); and the 1993 International Ethical Guidelines for Biomedical Research Involving Human Subjects proposed by the Council for International Organizations of Medical Sciences (CIOMS) and the World Health Organization (Beauchamp & Childress, 1983), a further revision of which was initiated in 1998. The Belmont Report outlined three principles to guide the conduct of research - informed consent (embodying the ethical precept of respect for persons), the assessment of risks and benefits (beneficence and nonmaleficence), and the selection of subjects (justice). The report conceptualised informed consent as consisting of three elements: information, comprehension and voluntariness. Informed consent procedures in many senses thus represent the ethical stance adopted by scientists towards volunteers in a trial. It is from this perspective that we argue that the technicalities of informed consent are not separable from the conditions created in the trial to give meaning to the principles of respect for persons, beneficence and justice. For example, the access volunteers will have to treatments, compensation for research-related injuries, provisions for trial participants once the trial is completed, and the steps taken to counteract the stigma and discrimination that may be consequent on trial participation. The early documents were based on an assumption of the universal applicability of the requirements to respect persons and protect their individual rights. And, while current requirements for consent continue to stress individual autonomy, understanding and freedom from coercion, there is a
1 The terms “scientific team” and volunteer” remind us of the reality of roles in trials. In most clinical trials, and
certainly in vaccine-related trials, there will be a scientific team, headed by a director, rather than an individual physician-scientist. This influences the locus and nature of responsibilities for scientific and ethical issues. In turn, persons who enter trials are volunteers, not subjects which, as Stark (1998) asserts, carries unacceptable connotations of objectification.
Page -5-
growing tendency to regard research in developing countries2 as presenting a set of special circumstances requiring difficult ethical interpretation and application. The prospect of large-scale vaccine trials to control HIV/AIDS, designed for implementation among vulnerable groups, has increased debate around the issues of if, when and how deviations from standard requirements for informed consent are justified. The Belmont Report emphasised the importance of consent requirements when research involved vulnerable persons, including minorities and economically disadvantaged groups. The CIOMS Guidelines pay particular attention to vulnerability, defined as the incapacity to protect one’s own interests (for a number of reasons including unfamiliarity with modern medical concepts), as well as to research involving persons in underdeveloped communities (Guideline 8). This guideline reiterates that every effort should be made “to secure the ethical imperative that the consent of individual subjects be informed (p. 25), and advises researchers to “respect the ethical standards of their own countries and the cultural expectations of the societies in which research is undertaken” (p. 26). Other aspects of the guideline stress: the need for research to be responsive to the health needs of local communities, the reasonable availability to the community of tested products, the need for intermediaries to assist people to give informed consent when required, and the need for ethical review by persons with a thorough understanding of a community’s customs and traditions. ... only the “authenticity of volunteering overcomes the depersonalizing effect of being treated as a token or sample in an experiment” Jonas (1969, in Mackillop & Johnston, 1986; p. 181)
1.2.2. THE INTERDEPENDENCE OF SCIENCE AND ETHICS Instead of seeing science and ethics being as separate and even opposing, a more sophisticated understanding recognises their essential interdependence. Firstly, it is appreciated that poor science is unethical. It is unethical to ask people to participate in studies that have little or no likelihood, because of poor conceptualisation and/or design, of producing meaningful results or furthering scientific knowledge. Secondly, inadequate attention to respect for persons, beneficence, and justice, can affect the scientific viability and validity of research. For example, conditions governing participation in trials affects recruitment, attrition, adherence and compliance, in ways that can introduce serious confounding, as well as threats to the internal and external validity of the data collected (Leventhal, 1991; Verheggen & van Wijmen., 1996). Research conducted by humans on, or amongst, other humans is an essentially social activity. This necessitates responsibility for integrity in research relationships, as well as awareness that there are always social consequences to research and that there are always impacts on a personal level (Mackillop & Johnston, 1986).
2 There is no agreed upon terminology for what are called “developed” and “developing” countries, but these terms
are recognised to refer to the division between rich countries, largely in the northern hemisphere, and poor countries, largely in the southern hemisphere.
Page -6-
1.2.3. THE LEGAL AND MORAL FOUNDATIONS OF INFORMED CONSENT Informed consent and related ethical requirements governing biomedical research have their origins in morality and in a shared revulsion towards the degeneracy of Nazi experimentation. However, subsequent developments in informed consent requirements have been strongly influenced by the litigious milieu in the United States of America and the necessity to develop legal criteria for consideration in criminal and civil cases (Alfidi, 1971; Hertz, Looman & Lewis, 1992; Kaufman, 1983; Meisel & Roth, 1983). This legal history and context has, in the opinion of many authors, diminished the concept of informed consent. Informed consent is often, it is claimed, treated as a mere legalism (Baum, 1986; Finkelstein, Smith & Faden, 1993); a rite rather than a right; “... no more than an elaborate ritual, a device that, when the subject is uneducated and uncomprehending, confers no more than the semblance of propriety on human experimentation” (Ingelfinger, 1972). This is one sense in which the claim is made that informed consent does not work. The scientists obliged to conform to informed consent requirements have to be convinced, as a scientific team, of both the moral right of human beings to decide what is to be done to them in research studies, and the scientific sense of not treating human beings as inert specimens. Otherwise, ethical requirements for informed consent can be manipulated into a cookbook approach to conform to the minimum bottom line. Rules can proliferate in an attempt to cover all possible gaps, yet still fail to achieve the purpose that concrete actions must be taken to demonstrate respect for persons by ensuring their autonomy.
1.2.4. DIFFERENCES BETWEEN TREATMENT AND RESEARCH The Belmont Report distinguished between biomedical research and therapy on the basis that research involves greater risks for the patient-volunteer, and on the basis of the different intentions and motivations of the health professionals involved. The clinician is obliged to render “personal care” (Fried, 1974); care based entirely on considerations of the wellbeing of the patient. In contrast, the researcher is immediately intent on developing or testing new knowledge, even though the long-term goal of such investigations is to benefit patients. The altered intention of the investigator-physician potentiates a conflict of interests because the patient-volunteer becomes a means to an end (Lantos, 1993; Tuthill, 1997). In this situation, the interests of the investigator-physician and patient-volunteer may no longer be congruent. This conflict between the wellbeing of the patient and the goals of the investigating physician is illustrated, for example, by placebos which are not meant to benefit the individual patient, and by randomisation which may conflict with clinical judgement about how to achieve maximum benefit available (Appelbaum, Lidz & Meisel, 1987). Kaufman has argued that the distinction between therapy and research is simplistic, particularly when considered in the light of innovative or experimental therapy. However, it may also be simplistic when considered from the perspective of the patient-volunteer. Several studies, including in our local environment have found that one of the primary motivations for volunteering for participation in research is the belief that better care, better treatment, or other health benefits will accrue (Abdool Karim et al, 1997; Appelbaum et al, 1987; Tuthill, 1997). In many settings, but
Page -7-
particularly in resource-poor environments, the same health professionals may function in respect of the community as both physicians and investigators. If the role of the health professional as an investigator is not made plain to the patient as a volunteer, the resulting role confusion, in the mind of the patient-volunteer, may constitute one of the most fundamental obstacles to voluntary entry into trials and thereby to informed consent. The problematic nature of this situation was well-recognised in the Belmont Report - “A continuum of such influencing factors exists, however, and it is impossible to state precisely where justifiable persuasion ends and undue influence begins”
1.2.5. OBSTACLES TO INFORMED CONSENT There is a comprehensive literature on informed consent. Over 1 000 references are listed in Medline since 1989 in which informed consent is the focus of the paper (Kent, 1996). A good part of this literature, in one way or another, refers to or documents difficulties in obtaining informed consent. This is as true in the United States of America and the United Kingdom, as anywhere else in the world (Alfidi, 1971). It is hard to imagine that it could be otherwise. As Beecher (1966, p. 1355) noted, more than 30 years ago, “all so-called codes are based on the bland assumption that meaningful or informed consent is readily available for the asking”. The difficulties in obtaining informed consent include: 1. The problems lay people have in remembering and understanding the details of scientific design and biomedical treatment comparisons (Cassileth et al, 1980); 2. Defensive psychological forgetting of threatening information, especially about risks (Verheggen & van Wijmen, 1996); 3. Barriers to communication emerging from cultural and class differences; these include illiteracy, language differences, competing models of disease, presumed differences in the construction of personhood, etc (Schoepf, 1991); 4. Situational pressures, including a feeling of obligation, as volunteers get caught up in several processes with different people, so that they can no longer distinguish between treatment and research, nor do they feel able to exert their right to withdraw (Meisel & Roth, 1983); 5. Implicit forms of coercion which threaten voluntariness and the right to withdraw (Abdool Karim et al, 1997; Levine, 1991), and 6. The resistance of health professionals which arises from the challenge that informed consent requirements pose to their assumed beneficence (Kaufman, 1983; Lidz et al, 1983; Meisel & Kuczewiski, 1996; Taylor & Kelner, 1987). Informed consent is by all accounts an ideal not easily accomplished. This is the second sense in which the criticism is heard that informed consent does not work. However, the fact that informed consent is difficult to attain, in no way justifies dispensing with it or relegating it to a formality. Formalistic consent requirements can become a way of delegating the entire burden of medical decisions to the patient, thus isolating him or her from physician and family support and limiting medical responsibility. (Gostin, 1995; p. 845)
Page -8-
1.2.6. THE ROLE OF CULTURE IN INFORMED CONSENT A lengthy debate has been waged concerning the role of cultural differences in significantly altering either the requirements or methods for obtaining informed consent from individual volunteers. This debate is summarised by the opposing accusations of “ethical imperialism” on the one hand, and advocating “double standards” on the other (Angell, 1992; Barry, 1992; Benatar, 1998; Ijsselmuiden & Faden, 1992; Olivier, 1995). Sometimes the question is formulated as to whether American ethical standards should be everywhere applied? This question involves several complex issues and the arguments can be interpreted in different ways. Another way the debate is approached is by asking whether ethical principles are relative or universal, and whether informed individual consent, based on notions of individual autonomy, should be imposed by Western researchers on collectivist cultures as occur, for example, in parts of Africa and Asia, and which are assumed to place little value on personal autonomy. It stands to reason that because morals are social constructions, that ethical standards, in general, are likely to differ from culture to culture and are in this sense, relative (Christakis, 1992). However, this does not mean that the ethical principles generated specifically to govern the conduct of biomedical research are relative and therefore amenable to adjustment or compromise. Ethical principles were articulated to restrain biomedical research regardless of where it occurs. Therefore, the ethical principles under discussion are specific to the activity (biomedical research) and not determined by the setting (for example, a society based on collectivist values) (Christakis, 1992; Gostin, 1995). In addition, the anthropological literature articulating differences between societies characterised by collectivist and individualist values, does not support the conclusion that collectivist societies are uniformly devoid of concepts relating to individuality and personal autonomy, and that individuality is unconditionally rejected (Gasa, 1999; Ijsselmuiden & Faden, (1992). There is almost no support in the literature for the idea that individual informed consent can be replaced by the proxy consent of local leaders, government officials, husbands, fathers or other traditional male authorities. In fact, cogent arguments have been advanced by several authors (Adityanjee, 1986; Angell, 1992; Barry, 1992; Benatar, 1998; Ijsselmuiden & Faden, 1992; Olivier, 1995) for strict adherence to the requirement that individual volunteers give informed consent for their participation in clinical trials. Among other things, there are no guarantees that proxy authorities have the best interests of all potential participants in mind with respect to a particular endeavour; in addition to which, their decisions are likely to replicate and entrench traditional age, gender and status differentials to the detriment of individual rights.

Page -9-
The uncompromising adherence to the principle of informed consent does not exclude sensitivity to local customs and expectations. It is polite and anticipated that any major research endeavour, such an HIV vaccine-related trial, will make contact with local authorities and seek their consent and cooperation before approaching citizens to volunteer for a study with potential personal, economic and political ramifications for the society. This is not a custom peculiar to Africa, Asia or Latin America - it would be as much expected and appreciated in Cambridge, Massachusetts. Undue interpretations of differences between societies can function to objectify others, and care should be taken not to see all cultural differences as indicating extreme incompatibilities between social values and practices. Similarly, the notion that an individual approached for recruitment into a trial, especially a trial with considerable personal ramifications, might want to discuss the issue with family and friends is not unusual (Nelson, 1992). However, the consent of such people cannot replace the individual informed consent of the volunteer (Gostin, 1995). Rather than seeking the proxy consent of such people, scientific teams should ensure that recruits and volunteers feel free to share decisions with their families or not, depending on the idiosyncratic circumstances of each potential volunteer. The idea that people in resource-poor countries - who are likely to be culturally distant from Western researchers and also technocratic elites from their own society - cannot understand the basics of research design or biomedical treatment options because they have little education, speak languages devoid of the technical terms of biomedical research, or have different views about health and illness, appears to be exaggerated. It may be difficult to communicate the purposes, conditions and risks of research, but the difficulty of doing so should not be used to detract from the importance of obtaining individual informed consent. In any case, several researchers (Abdool Karim et al, 1997; Preziosi et al, 1997) have recounted experiences to indicate that, with sufficient care, acceptable levels of understanding can be communicated to volunteers in Africa. In our own research (Gasa, 1999), for example, we have found that largely illiterate rural people can understand randomization when illustrated with coins; but, like Westerners, they seem to show defensive denial when the idea of randomisation is personalised The foregoing arguments for the necessity of obtaining individual informed consent do not invalidate the assertion that important social and cultural differences are likely to exist between scientific teams and volunteers, whether the scientific teams are foreign or local. Sometimes what are called cultural differences reflect also differences in power, prestige and resources. For example, we have found (Gasa, 1999) that largely illiterate rural women find it extremely difficult to respond to questions with an Agree or Disagree format. It is very difficult for them to engage in a personalised discourse of conflict or disagreement with people they consider to be authorities or in a superior position. On a macro level, issues raised in connection with culture are frequently associated with two assumptions: firstly, that vaccine trials will involve a binational or international agreement where a more resourced country from the North will finance and provide intellectual leadership for the conduct of the HIV vaccine trial based on a product developed in the North; and secondly, that the host country involvement and contribution occurs only at the stage of an efficacy trial. Developments during the last year have radically altered this model of assumed vaccine development and testing. Several governments from the South (including China, Cuba, India, South Africa and Pakistan) have made a commitment to and become actively involved in vaccine development. This shift in initiative places new imperatives on the need to understand and come to
Page -10-
grips with the interplay between culture and power. There may be an unwarranted assumption that the role of cultural differences will be negligible and therefore also the threats to understanding and voluntariness when the product and trial are conducted by local researchers involving local participants. Power differentials between researcher elites and local communities will continue to exert effects previously attributed also to the influence of cultural differences.
1.2.7. RISKS IN HIV VACCINE-RELATED TRIALS It is obvious that research which carries significant risks as the cost for yielding important benefits is likely to pose the most complex ethical problems. HIV vaccine-related trials fall into this category. No one can deny the significant medical and social risks that these trials present for potential volunteers (Porter et al, 1989). Firstly, such trials need to be conducted in regions of the world where large numbers of suitable participants, that is, individuals at high risk for HIV infection, are available, and where antiretroviral drugs which could interfere with the assessment of vaccine efficacy, are not widely available (Bloom, 1998). These individuals are, by definition, vulnerable to exploitation and stigmatisation. Currently, most of these individuals are in resource-poor countries which themselves are vulnerable to exploitative relationships with funding agencies and research groups from the West and from within their own countries (Barry, 1992; Benatar, 1998; Ijsselmuiden & Faden, 1992). Secondly, participation in trials carry significant social risks for participants, including those that arise from vaccine-induced seropositivity. Social risks include confidentiality issues, stigma, violence and abandonment, occupational and social constraints, among others. Thirdly, exposure to a vaccine may enhance disease if the individual is subsequently exposed to HIV, and may affect a participant’s capacity, through immune tolerance, to receive a vaccine developed in the future. In addition, the risk-benefit ratio may be distorted by the type of vaccine being tested in particular community or amongst a particular group of volunteers. While the vaccinological implications of the different subtypes of HIV remain uncertain, there has been increasing concern about the ethics of testing a product that has been developed against a sub-type that is not prevalent in the population where the product is proposed to be tested. The rationale that high incidence rates justify such trials distorts the principle of justice - in that the risks and benefits are not equal for the host and donor countries or their citizens. Of equal importance in cost-benefit evaluations is the choice of vaccine design. The emphasis to date has been on designs that emphasise safety at the expense of immunogenicity, which has retarded the vaccine development agenda, thereby depriving potential beneficiaries earlier access to protection from developing products. Informed consent procedures need to make risks clear to recruits, at the same time as indicating the potential benefits to society of producing an effective vaccine, together with any other benefits specific to a particular trial. This, together with the need to communicate the nature of the experimental design, creates a considerable communication challenge. It is likely that strong motivations on the part of volunteers will drive participation in vaccine trials, particularly the desire to avoid infection and/or seek treatment. These motivations will themselves complicate volunteers’ interpretation of the purposes and methods of the trial. In order to understand the social processes governing recruitment and adherence, it will be necessary to have some understanding of volunteer motivations.
Page -11-
Several questions recur in the literature with respect to informed consent, among which are the following: 1. How can consent be truly informed when many laypersons cannot comprehend complex medical and scientific information? 2. How much disclosure of information is necessary and beneficial to informed decision-making, and how much is harmful to the well being of volunteers? 3. How can an investigator know how a volunteer interprets information about an experiment? 4. Is the consent form the appropriate instrument through which researchers may fulfil their obligations not to treat volunteers merely as a means to an end? 6. Are individuals free to participate under conditions of limited health care resources, which coincide with research sites? No clear answers exist to these questions. Christakis (1992) argues that final and transcendent resolution of ethical issues is not possible, apart from decisions made in particular local settings in which the problems are framed. We return to the assertion that the dilemmas of obtaining informed consent in any particular setting cannot be separated from the design and ethical intentions of the scientific team. It may be advisable, in addition to the requirement for signed informed consent by volunteers, for scientific teams to write ethical justifications for all aspects of the research design in terms of the fundamental principles of respect for persons, beneficence and justice.
1.2.8. VOLUNTARINESS AND FREEDOM FROM COERCION Financial and other benefits offered to trial participants are regarded as inducements that impair voluntariness and act to influence participation. For example, Adityanjee (1982) argues that money offered to pay for transport for examinations and other procedures can function as an inducement in poor communities. He advocates that no benefits or potential benefits should be discussed until consent has been given. On the other hand, it must be acknowledged that the communities likely to be targeted for trials, particularly in southern hemisphere countries, are generally poor. Individuals and families will not be easily persuaded to cover transport costs for visits to health centres with no apparent benefit to themselves, especially when they have other very pressing financial priorities. In addition, work and especially women’s work in households has economic value. Many women spend hours collecting water and fuel, washing clothes, preparing food, and caring for small children and dependent others. Time spent out of the household to attend to trial examinations is a spent resource, and other capital has to be found to compensate for them. Research teams will have to struggle with issues concerned with compensation and benefits for trial participants. Simplistic either-or dichotomies, while morally comfortable, are not going to be adequate to deal with the complexities of motivations and expectations that potential trial participants bring to the informed consent process. Ethical dilemmas, by their very nature, are often not amenable to solutions, which can be shown to be unequivocally and substantively correct. (Benatar, 1988; p. 222)
Page -12-
1.2.9. SUMMARY In the preceding sections, a conceptual framework was created for the consideration of informed consent. This framework informs understanding of informed consent in the following ways: 1. Informed consent should not be seen merely as a technical requirement of ethical oversight bodies. Instead, informed consent procedures express researchers’ commitment to respect for persons and the principle of autonomy. 2. HIV vaccine-related trials will have to transcend technical approaches to informed consent and grapple with thorny issues of risks and benefits. 3. Culture is a complex concept that overlaps also with class and other power differentials. Considerable sensitivity is required both to accommodate cultural differences while at the same time recognising the fundamental nature of the ethical principles of biomedical research. 4. The ethical issues facing HIV vaccine-related trials will require that scientific teams create mechanisms for public discussion and debate amongst themselves on ethical issues to resolve matters concerning design as well as benefits for participants. 1.3. CONCEPTUAL FRAMEWORK FOR PROCEDURES TO OBTAIN INFORMED CONSENT The procedures recommended to obtain informed consent laid out in Part 2 of this document are based on the notion of informed consent as a shared decision making process between researcher and volunteer, aimed at optimizing the process of making this decision in the best interest of the volunteer. The following considerations form the basis of the approach to informed consent adopted in these guidelines.
1.3.1. THE DECISION MAKING PROCESS One of the most important issues in informed consent is the question of how prospective participants come to make the decision whether or not to participate in a trial, and why they remain in the study. Essentially, the informed consent process is concerned with assisting the volunteer to make a decision, which is “truly” in their own best interest. Many of the standard procedures regarding informed consent are based on the assumption that the decision to participate in a research study is a rational decision made on the basis of the information presented to prospective participants. Yet a considerable proportion of the available research suggests that the information transmitted to potential research subjects has little impact on their decision to participate, and that the decision is often made before or independently of the technical information provided to participants (Faden & Beauchamp, 1980). There is evidence that personal and cultural values play a major role in coming to a decision about whether or not to participate in research (Parker, 1995; Weil, 1996), and that the decision making process involves cognitive, emotional, motivational and value-based components (Faden & Beauchamp, 1980; Kent, 1996; Weil, 1996). In developing the protocol proposed in this
Page -13-
document, we have attempted to take account of the complexity of the decision making process, and to facilitate this process by incorporating the various factors likely to affect decisions.
1.3.2. SOCIAL DESIRABILITY Social desirability refers to the tendency for research participants to behave in what they deem to be socially acceptable ways in order to win the favour, or avoid the displeasure, of the researcher. It is likely that social desirability has a very strong influence on various aspects of biomedical research studies, as well as the informed consent process itself. The importance of social desirability becomes even more apparent when one considers the significant power and status differentials between medical researchers and research participants, especially in resource poor settings. Therefore, for the informed consent process to be truly ethical, the issue of social desirability needs to be carefully considered, including the issue of dependency of potential participants on health care provided through or alongside the research effort. In designing the protocol outlined in Part 2 of this document, the authors have attempted to consider ways in which the issue of social desirability may be addressed in the informed consent process. In the main, we recommend that advocacy-support staff be employed to assist volunteers in identifying and voicing their concerns.
1.3.3. UNDERSTANDING Another central issue in considerations of informed consent is the question of understanding or comprehension. While it may be relatively easy to assess the adequacy of information disclosed and imparted, it is far more difficult to assessed whether the information is understood. This means that the legal requirement of disclosure of information may be satisfied, while the moral requirement of understanding in order to make decisions in one’s own best interest may not. Further, expressed understanding on the part of research participants is not necessarily the same as true understanding (Meisel & Roth, 1983), so that opinions of participants regarding their understanding cannot be taken at face value. The most common check on the adequacy of the understanding of the technical elements of a study is in the form of an information test for participants after the transmission of information, or at different stages of the research. However, there are a number of complications with such tests of understanding or comprehension. Numerous studies indicate that relatively few participants recall a large portion of information conveyed by researchers. But more important, such tests are actually assessments of short-term verbal memory rather than of understanding. Further, the culturally or personally based value systems that enable prospective participants to evaluate information given to them with respect to its personal implications are largely unrecognized or ignored (Parker, 1995). To achieve understanding (as opposed to the repetition of facts following some delay) entails incorporating a recognition of these value systems. Finally, if informed consent is accepted to be a process of shared decision making, then understanding should always be a two way process. The researcher should comprehend the needs, values and motivations of the recruit, and how best to optimize their participation in the research study (Meisel & Kuczewski, 1996).

Page -14-
In the light if these considerations, a number of decisions have to be made in setting up the procedures for informed consent in a study: What kinds of information should be given to potential participants to optimize their understanding? For example, is it necessary for participants to understand the elements of randomization? How should this information be given so as to best facilitate an optimum decision-making process? And how can personal understanding of this information and its implications best be facilitated and assessed? In preparing this protocol, the authors have operated from the assumption that for understanding to operate as an ethical and psychologically sound part of the informed consent process, it is essential that understanding is taken to be more than the short-term memory of technical facts. It is acknowledged that participants may require an understanding of certain basic technical issues (objective understanding) in order to indemnify the researchers. However, for informed consent by persons to be attained it is more important that participants understand the personal implications of participation in research (subjective understanding).
1.3.4. FREEDOM FROM COERCION An essential component of the informed consent process is respect for the autonomy of volunteers and their right to decide about their participation in research studies without coercion of any sort. The research team needs to be especially aware of subtle coercive pressures arising from various sources. The issue of social desirability is again relevant here, as the significant power differential between researchers and volunteers in resource poor settings may exert considerable social pressure on volunteers to conform to the wishes of services providers and health care professionals. In addition, the research team needs to give careful attention to understanding the motivations of volunteers for participating in research trials as these may, at times, exert pressures to participate. This is especially important if the volunteer’s motivations are based on misunderstanding or assumed benefits. 1.4. REFERENCES Abdool Karim, Q., Abdool Karim, S., Coovadia, H. & Susser, M. (1998). Informed consent for HIV testing in a South African hospital: Is it truly informed and truly voluntary? American Journal of Public Health, 88, 537- Adityanjee, Dr. (1986). Informed consent: Issues involved for developing countries. Medical and Scientific Law, 26, 305-307. Alfidi, R. (1971). Informed consent: A study of patient reaction. Journal of the American Medical Association, 24, 1325-1329. Angell, M. (1992). Ethical imperialism? Ethics in international collaborative clinical research. The New England Journal of Medicine, 319, 1081-1083 Appelbaum, P. & Grisso, T. (1988). Assessing patient’s capacities to consent to treatment. The New England Journal of Medicine, 319, 1635-1638.
Page -15-
Appelbaum, P., Lidz, C. & Meisel, A. (1987). Informed consent: Legal theory and clinical practice. New York: Oxford University Press. Appelbaum, P., Roth, L., Lidz, C., Benson, P. & Winslade, W. (1987). False hopes and best data: Consent to research and the therapeutic misconception. Hastings Center Report, April, 20-24. Askew, G., Pearson, K. & Cryer, D. (1990). Informed consent: Can we educate patients? Journal of the Royal College of Surgeons, Edinburgh, 35, 308-310. Barber, B. (1976). The ethics of experimentation with human subjects. Scientific American, 234, 25-31. Barry, M. (1992). Ethical considerations of human investigation in developing countries: The AIDS dilemma. The New England Journal of Medicine, 319, 1083-1085. Baum, M. (1986). Do we need informed consent? The Lancet, October 18, 911-912. Baum, M., Zilkha, J. & Houghton, J. (1989). Ethics of clinical research: Lessons for the future. British Medical Journal, 299, 251-253. Beauchamp, T. & Childress, J. (Eds), Principles of biomedical ethics. Oxford: Oxford University Press. Beecher, H. (1966). Ethics and clinical research. The New England Journal of Medicine, 274, 1354-1360. Belmont Report (1979). Ethical principles and guidelines for the protection of human subjects of biomedical and behavioral research (www.hunger.brown.edu/Administration/Research_Ad ministration/belmont/belmont.html). Benatar, S. (1992). Informed consent in Africa. South African Medical Journal, 81, 489. Benatar, S. (1998). Imperialism, researth ethics and global health. Journal of Medical Ethics, 24, 221-222. Bergler, J., Pennington, C., Metcalfe, M. & Freis, E. (1980). Commentary. Informed consent: How much does the patient understand? Clinical Pharmacology and Therapeutics, 27, 435-440. Blackhall, L., Murphy, S., Frank, G., Michel, V. & Azen, S. (1995). Ethnicity and attitudes towards autonomy. Journal of the American Medical Association, 274, 820-825. Bloom, B. (1998). The highest attainable standard: Ethical issues in AIDS vaccines. Science, 279, 186-188. Blustein, J. (1993). The family in medical decisionmaking. Hastings Center Report, May-June, 6-13. Byrne, D., Napier, A. & Cuschieri, A. (1988). How informed is signed consent? British Medical
Page -16-
Journal, 296, 839-840. Cassileth, B., Zupkis, R., Sutton-Smith, K. & March, V. (1980). Informed consent - Why are its goals imperfectly realised? The New England Journal of Medicine, 302, 896-900. Chesney, M., Lurie, P. & Coates, T. (1995). Strategies for addressing the social and behavioral challenges for prophylactic HIV vaccine trials. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology, 9, 30-35. Christakis, N. (1988). The ethical design of an AIDS vaccine trial in Africa. Hastings Center Report, 18, 31-37. Christakis, N. (1992). Ethics are local: Engaging cross-cultural variations in the ethics for clinical research. Social Science and Medicine, 35, 1079-1091. Council for International Organizations of Medical Sciences (CIOMS) in collaboration with the World Health Organization (WHO) (1993). International Guidelines for Biomedical Research Involving Human Subjects. CIOMS: Geneva. Dawes, P., O’Keefe, L. & Adcock, S. (1992). Informed consent: The assessment of two structured interview approaches compared to the current approach. The Journal of Laryngology and Otology, 106, 420-424. DeCock, K, Shaffer, N., Wiktor, S., Simonds, R., Rogers, M. (1997). Lancet, 350, 154647. Del Rio, C. (1997). Ethics, economic realities and medical research in developing countries. www.ucian.ac.uk/facs/ethics/azt.htm. Dorn, L., Susman, E. & Fletcher, J. (1995). Informed consent in children and adolescents: Age maturation and psychological state. Journal of Adolescent Health, 16, 185-190. Dudley, H. (1991). Informed consent - issues for the 1990's. British Journal of Urology, 68, 561-564. Durojaiye, M. (1979). Ethics of cross-cultural research viewed from a Third World perspective. International Journal of Psychology, 14, 137-141. Dyer, A. (1997). The ethics of human genome intervention: A postmodern perspective. Experimental Neurology, 144, 168-172. Ekunwe, E. & Kessel, R. (1984). Informed consent in the developing world. Hastings Center Report, 14, 22-24. Epstein, L. & Lasagna, L. (1969). Obtaining informed consent: Form or substance. Archives of Internal Medicine, 123, 682-688. Faden, R. & Beauchamp, T. (1980). Decision-making and informed consent: A study of the impact of disclosed information. Social Indicators Research, 7, 313-336.

Page -17-
Faden, R. & Beauchamp, T. (1986). A history and theory of informed consent. Oxford: Oxford University Press. Feinleib, M. (1991). The epidemiologist’s responsibilities to study participants. Journal of Clinical Epidemiology, 44, 73S-79S. Finkelstein, D., Smith, M. & Faden, R. (1993). Informed consent and medical ethics. Archives of Opthalmology, 111, 324-326. Fried, C. (1974). Medical experimentation: Personal integrity and social policy. New Year: American Elsevier Publishing Co. Gasa, N. (1999). Cultural conceptions of culture and informed consent. Unpublished Master’s dissertation, University of Natal, Pietermaritzburg. Geertz, C. (1983). Local knowledge: fact and law in comparative perspective. In Local knowledge: Further essays in interpretive anthropology. New York: Basic Books. Gordon, D. & Paci, E. (1997). Disclosure practices and cultural narratives: Understanding concealment and silence around cancer in Tuscany, Italy. Social Science and Medicine, 44, 1433-1452. Gostin, L. (1991). Ethical principles for the conduct of human subject research: Population-based research and ethics. Law, Medicine and Health Care, 19, 191-201. Gostin, L. (1995). Informed consent, cultural sensitivity, and respect for persons. Journal of the American Medical Association, 274, 844-845. Grady, C. (1999). Grappling with global concerns in the search for an HIV vaccine. Journal of the Association of Nurses in AIDS Care, 10, 17. Gray, B. (1982). The regulatory context of social and behavioral research. In T. Beauchamp, R. Faden., R. Wallace & L. Walters (Eds), Ethical issues in social science research. Baltimore: John Hopkins University Press. Gray, J., Lyons, P. & Melton, G. (1995). Ethical and legal issues in AIDS research. Baltimore: The John Hopkins University Press. Hancock, G. (1989). Lords of poverty. London: Mandarin. Hardwig, J. (1990). What about the family?. Hastings Center Report, 10, 5-10. Hein, K. (1997). Annotation: Adolescent HIV testing - Who says who signs? American Journal of Public Health, 87, 1277-1278. Henley, L., Benatar, S., Robertson, B. & Ensink, K. (1995). Informed consent - a survey of doctors’ practices in South Africa. South African Medical Journal, 85, 1273-1278. Herz, D., Looman, J. & lewis, S. (1992). Informed consent: Is it a myth? Neurosurgery, 30, 453-
Page -18-
458. Ho, V. (1995). Marginal capacity: The dilemmas faced in assessment and declaration. Canadian Medical Association Journal, 152, 259-263. Howard, J., DeMets, D. and the Bhat Research Group (1981). How informed is informed consent? The Bhat experience. Controlled Clinical Trials, 2, 287-303. Howard-Jones, N. (1982). Human experimentation in historical and ethical perspectives. Social Science and Medicine, 16, 1429-1448. Ikuenobe, P. (1998). Moral education and moral reasoning in traditional African cultures. The Journal of Value Inquiry, 22, 17-36. Ijsselmuiden, C. & Faden, R. (1992). Research and informed consent in Africa - another look. The New England Journal of Medicine, 326, 830-834. Ingelfinger, F. (1972). Informed (but uneducated) consent. The New England Journal of Medicine, 287, 465-466. Katz, J. (1972). Experimentation with human beings. New York: Russell Sage Foundation. Kaufman, C. (1983). Informed consent and patient decision making: Two decades of research. Social Science and Medicine, 17, 1657-1664. Kent, G. (1996). Shared understandings for informed consent: The relevance of psychological research on the provision of information. Social Science and Medicine, 43, 1517-1523. Kerrigan, D., Thevasagayam, R., Woods, T., Welch, I., Thomas, W., Shorthouse, A. & Dennison, A. (1993). Who’s afraid of informed consent? British Medical Journal, 306, 298-300.
Page -19-
Kimmel, A. (1996). Ethical issues in behavioral research: A survey. Cambridge, Ma: Blackwell. Kirby, M. (1983). Informed consent: What does it mean? Journal of Medical Ethics, 9, 69-75. Kunstadter, P. (1980). Medical ethics in cross-cultural and multi-cultural perspectives. Social Science and Medicine, 14B, 289-296. Laforet, E. (1976). The fiction of informed consent. Journal of the American Medical Association, 235, 1579-1585. Lancet. Editorial (1984). Consent: How informed? Lancet, II, 1445. Lantos, J. (1993). Informed consent: The whole truth for patients? Cancer, 72, 2811-2815. Lavelle-Jones, C., Byrne, D., Rice, P. & Cuschieri, A. (1993). Factors affecting quality of informed consent. British Medical Journal, 306, 885-890. Lesko, L., Dermatis, H., Penman, D. & Holland, J. (1989). Patients’, parents’, and oncologists’ perceptions of informed consent for bone marrow transplantation. Medical and Pediatric Oncology, 17, 181-187. Leventhal, H., Nerenz, D., Leventhal, E., Love, R. & Bendena, L. (1991). The behavioral dynamics of clinical trials. Preventive Medicine, 20, 132-146. Levine, C. (1991). AIDS and the ethics of human subjects research. In F. Reamer (Ed), AIDS and ethics (pp 77-104). New York: Columbia University Press. Levine, R. (1988). Ethics and regulation of clinical research. New Haven: Yale University Press. Levine, R. (1991). Informed consent: Some challenges to the universal validity of the Western model. Law and Medical Health Care, 19, 207-213. Levine, R. (1996). International codes and guidelines for research ethics: A critical appraisal. In H. Vanderpool (Ed), The ethics of research involving human subjects: Facing the 21st century (pp 235-259). Frederick, MD: University Publishing Group. Lidz, C., Meisel, A., Osterweis, M., Holden, J., Marx, J. & Munetz, M. (1983). Barriers to informed consent. Annals of Internal Medicine, 99, 539-543. Light, D. (1979). Uncertainty and control in professional training. Journal of Health and Social Behaviour, 310, 2979. Lord, R. (1995). Informed consent in Australia. Australian and New Zealand Journal of Surgery, 65, 224-228. Lurie, P. & Wolfe, S. (1997). Unethical trials of interventions to reduce perinatal transmission of the human immunodeficiency virus in developing countries. The New England Journal of Medicine, 337, 85356.
Page -20-
Lynoe, N., Sandlund, M., Dahlqvist, G. & Jacobsson, L. (1991). Informed consent: Study of quality of information given to participants in a clinical trial. British Medical Journal, 303, 610-613. Mackillop, W. & Johnston, P. (1986). Ethical problems in clinical research: The need for empirical studies of the clinical trials process. Journal of Chronic Diseases, 39, 177-188. McLean, G. & Jenkins, T. (1994). HIV Testing and informed consent - ethical considerations. South African Medican Journal, 84, 669-674. Meisel, A. (1979). The “exceptions” to the informed consent doctrine: Striking a balance between competing values in medical decision-making. Wisconsin Law Review, 413, 413-418 Meisel, A. & Kuczewski, M. (1996). Legal and ethical myths about informed consent. Archives of Internal Medicine, 156, 2521-2526. Meisel, A. & Roth, L. (1983). Toward an informed discussion of informed consent: A review and critique of the empirical studies. University of Arizona College of Law, 25, 265-346. Melton, G., Levine, R., Koocher, G., Rosenthal, R. & Thompson, W. (1988). Community consultation in socially sensitive research: Lessons from clinical trials of treatment for AIDS. American Psychologist, 43, 573-581. Morrow, G., Bennett, J. & Carpenter, P. (1983). Informed consent to treatment in clinical trials. Biomedicine & Pharmacotherapy, 37, 10-13. Morrow, G., Gootnick, J. & Schmale, A. (1978). A simple technique for increasing cancer patients’ knowledge of informed consent to treatment. Cancer, 42, 793-799. Murray, T. (1994). Individualism and the community: The contested terrain of autonomy. Hastings Center Report, 24, 32-35. Muss, H., White, D., Michielutte, R., Richards, F., Cooper, M., Williams, S., Stuart, J. & Spurr, C. (1979). Written informed consent in patients with breast cancer. Cancer, 43, 1549-1556. Nelson, J. (1992). Taking families seriously. Hastings Center Report, 22, 6-12. Novick, A. (1986). Why burdensome knowledge need not be imposed. Hastings Center Report, September/October, 46-47 Ogbonnaya, A. (1994). Person as community: An African understanding of the person as an interpretive community. Journal of Black Psychology, 20, 75-88. Olivier, S. (1995). Informed consent and transcultural research. South African Medical Research, 85, 984-985. Parker, L. (1995). Ethical concerns in the research and treatment of complex disease. TIG, 11, 520-523
Page -21-
Penman, D., Holland, J., Bahna, G., Morrow, G., Schmale, A., Derogatis, L., Carnrike, C. & Cherry, R. (1984). Informed consent for investigational chemotherapy: Patients’ and physicans’ perceptions. Journal of Clinical Oncology, 2, 849-855. Philipson, S., Doyle, M., Gabram, S., Nightingale, C. & Philipson, E. (1995). Informed consent for research: A study to evaluate readability and processability to effect change. Journal of Investigative Medicine, 43, 459-467. Porter, J., Glass, M. & Koff, W. (1989). Ethical considerations in AIDS vaccine testing. Hastings Center Report, May/June, 163-166. Preziosi, M-P., Yam, A., Ndiaye, M., Simaga, A. & Simondon, F. (1997). Practical experiences in obtaining informed consent for a vaccine trial in rural Africa. The New England Journal of Medicine, 336, 370-373. Resnick, J. & Schwartz, T. (1973). Ethical standards as an independent variable in psychological research. American Psychologist, 28, 134-139. Roman, J. (1974). Reflections on informed consent. Archives of General Psychiatry, 30, 129-135. Rosnow, R. & Rosenthal, R. (1997). People studying people: Artifacts and ethics in behavioral research. New York: WH Freeman & Co. Roth, L., Lidz, C., Meisel, A., Soloff, P., Kaufman, K., Spiker, D. & Foster, F. (1982). Competency to decide about treatment or research: An overview of some empirical data. International Journal of Law and Psychiatry, 5, 29-50. Schoepf, B. (1991). Ethical, methodological and political issues of AIDS research in central Africa. Social Science and Medicine, 33, 749-763. Silva, M. & Sorrell, J. (1984). Factors influencing comprehension of information for informed consent: Ethical implications for nursing research. International Journal of Nursing Studies, 21, 233-240. Silverman, W. (1989). The myth of informed consent in daily practice and in clinical trials. Journal of Medical Ethics, 15, 6-11. Simes, R., Tattersall, M., Coates, A., Raghavan, D., Solomon, H. & Smart, H. (1986). Randomized comparison of procedures for obtaining informed consent in clinical trials of treatment for cancer. British Medical Journal, 293, 1065-1068. Simpson, J. (1981). Informed consent: A medical viewpoint. Medical Journal of Australia, 1, 169-171. Skovlund, E. (1991). Should we tell trial patients that they might receive a placebo? The Lancet, 337, 1041. Snowdon, C., Garcia, J. & Elbourne, D. (1997). Making sense of randomization: Responses of
Page -22-
parents of critically ill babies to random allocation of treatment in a clinical trial. Social Science & Medicine, 45, 1337-1355. Stark, C. (1998). Ethics in the research context: Misinterpretation and misplaced misgivings. Canadian Psychology, 39, 202-211. Strull, W. Lo, B. & Charles, G. (1984). Do patients want to participate in medical decision making? Journal of the American Medical Association, 252, 2990-2994. Surbone, A. (1992). Truth telling to the patient. Journal of the American Medical Association, 13, 1661-1662. Taylor, K. & Kelner, M. (1987). Informed consent: The physician’s perspective. Social Science and Medicine, 24, 135-143. Truog, R., Robinson, W., Randolph, A. & Morris, A. (1999). Is informed consent always necessary for randomised controlled trials? New England Journal of Medicine, 340, 804-807. Tuthill, K. (1997). Human experimentation: Protecting patient autonomy through informed consent. Journal of Legal Medicine, 18, 221-250. Ubel, P. & Loewenstein, G. (1997). The role of decision analysis in informed consent: Choosing between intuition and systematicity. Social Science and Medicine, 44, 647-656. Valdiserri, R., Tama, G. & Ho, M (1988). The role of community advisory committees in clinical trials of Anti-HIV agents. Hastings Center Report, July/August, 149-151. Veatch, R. (1995). Abandoning informed consent. Hastings Center Report, March/April, 5-12. Verheggen, F. & van Wijmen, F. (1996). Informed consent in clinical trials. Health Policy, 36, 131-153. Verhoef, H. & Michel, C. (1997). Studying morality within the African context: A model of moral analysis and construction. Journal of Moral Education, 26, 389-407. Weil, W. (1996). Abandoning informed consent? Hastings Centre Report, January-February, 2-3. White, W. (1983). Informed consent: Ambiguity in theory and practice. Journal of Health Policy and the Law, 8, 99-119.
Page -23-
PART 2: PRACTICAL GUIDE 2.1. PREPARATION FOR INFORMED CONSENT:
2.1.1. COMMUNITY PREPARATION It is suggested that all research trials should be jointly developed by researchers and the communities in which they are carried out, with volunteers as active participants rather than passively complying with institutional demands. All decisions regarding participation should be shared decisions of the research team and volunteers, and their representatives. In addition to broad education of the community regarding the nature of the research project, full consultation should take place with the community and with key informants in the community, in order to foster a sense of partnership with respect to the research project. Early in the research, the research team should establish a community advisory board (CAB), which can represent the interests of the community, and advise the research team on matters relating to cultural expectations and others issues of local importance, which need to be considered in setting up the research. These considerations apply also to trials being conducted in facilities in addition to communities.
2.1.2. PREPARATION OF THE SCIENTIFIC TEAM If informed consent is to be a mutual decision making process then it is essential that researchers and volunteers establish a relationship of mutual understanding before and during the introduction and execution of the study. The research team also needs to maintain an attitude of respect towards the notion of partnerships in research projects carried out in particular communities, as well as the active participation of the community in the research process. Further, researchers need to acquire information about the motivations and expectations of volunteers.
2.1.3. RESEARCHER UNDERSTANDING While the community and research participants will obviously need to be educated and informed about various elements of the research, it is as essential that the research team has an understanding of various issues affecting volunteers in the research project. Amongst the issues to be understood by the research team are: the socio-cultural and personal values which impact on the decision to participate in the research; the psychosocial implications of participating; and the expectations and motivations of volunteers. Community representatives and a community advisory board play a vital role in fostering this understanding early in the research process. It is suggested that once the research is underway there should be constant monitoring and feedback to the research team about the expectations, implications and effects of participation in the study. Given that informed consent is best enacted as a shared decision-making process, mutual understanding rather than unilateral understanding of the research by volunteers, is an essential pre-requisite

Page -24-
2.1.4. STAFF PREPARATION In order to foster the informed consent process, it is recommended that particular attention be given to the training and supervision of two types of participant counsellors: research counsellors and advocacy/support counsellors. Both types of participant counsellors should be thoroughly trained, supervised and monitored in basic counselling skills. The task of research counsellors is to counsel volunteers regarding the necessary technical and personal information in order to make the decision about participation in the project. These counsellors should be in a position to understand and counsel volunteers about personal concerns they might have. They would also be responsible for ongoing monitoring of the social and personal effects of participation and for providing feedback to the research team. These counsellors would effectively be part of the research team. In addition, it is recommended that advocacy/support counsellors be employed to assist volunteers in identifying issues of personal concern and in voicing these concerns from an advocacy perspective. Parallel to union representatives, these support counsellors would assume the responsibility of protecting the interests of volunteers (e.g. freedom from coercion), and would be primarily responsible to volunteers, CABs and other community representatives rather than to the research team. It is suggested that early on in the research process they be publically established with an advocacy role.
2.1.5. PREPARATION OF POTENTIAL VOLUNTEERS AND SIGNIFICANT OTHERS Especially in cultural contexts where the value of individual autonomy is balanced by the importance attached to community allegiance and interpersonal relationships, it is important that the research team give special attention to various people to whom potential volunteers are connected by blood relationship or community membership. Reference has already been made to the preparation of the broader community for participation in research trials. With the consent of potential volunteers, family and significant others need to be offered the possibility of active incorporation into the various stages and aspects of the informed consent process. Further reference to these components is made below. 2.2. INFORMED CONSENT MATERIAL PREPARATION:
2.2.1. PREPARATION OF INFORMATION FOR EDUCATION OF VOLUNTEERS Informed consent traditionally requires the transmission of information regarding the project’s aims, methods and procedures, and expected benefits or risks/hazards. Disclosure of all information is seen as an essential aspect of risk management for legal protection of researchers. But insofar as informed consent is driven by moral as well as legal concerns, careful attention needs to be given to the nature, amount and method of information disclosure and its effects on the decision making process (Lantos, 1993). We recommend that the research team also needs to consult with the community on the nature of information required by volunteers in order to decide in their own best interests whether to participate in the project or not. It is also recommended that rather than viewing information giving as a once-off activity, the research team should make ongoing counselling (incorporating information) available to all volunteers.
Page -25-
The following specific recommendations are made regarding preparation of information:
• All aspects of the study should be discussed with key community representatives, in order to decide on issues such as: what cultural values need to be considered in implementing the research; which information should be transmitted to participants; how could such information best be transmitted; who should share the information with potential participants; how can potential participants best be assisted in the decision process.
• Researchers should attempt to establish a network of participants, linking potential
participants with others already in the study (with the agreement of both parties) with similar demographic characteristics and values, in order to better understand the personal implications of participation.
• The research team should decide on the minimal technical information that is essential to be
given to participants for legal indemnity of researchers.
• Informational counselling sessions with participants should be repeated at different stages of the research.
• The right of volunteers to withdraw from the study at any stage should be emphasized
during initial and subsequent informational counselling sessions.
2.2.2. SELECTION AND TRAINING OF STAFF FOR EDUCATION AND COUNSELLING
Reference has already been made to the training of research counsellors for the transmission of information. These research counsellors should include people who share the values and world-view of potential research participants.
2.2.3. METHODS OF INFORMATION TRANSMISSION The research team, in collaboration with the community advisory board, should decide on the most effective and most acceptable medium of information transmission. It is recommended that videotaped presentations be prepared for transmission of information. These should also incorporate material relating to the personal implications of participation for volunteers.
2.2.4. INTERACTIONAL ASPECTS OF EDUCATION Careful attention should be given to the establishment of rapport between researchers and participants in order to facilitate an optimal emotional context for the transmission and understanding of information. In order to facilitate understanding through the asking of questions or discussion of personal concerns, research counsellors should attend to process aspects of information counselling. The following are important to achieving these aims:
• Ensure that all research assistants are trained to take account of the process/interactional aspects of information provision.
• Request volunteer evaluation of satisfaction with information-giving interviews. These
Page -26-
evaluations should not be conducted by researchers or persons who gave the information, but by a support/advocate staff member.
• Do a full assessment of a random sample of interviews recorded on audio- or videotape in order to assess the adequacy of the informed consent process using, for example, the Meerwein model. This model looks at three dimensions of information: i) the information dimension, concerned with the content and technique of disclosure; adequacy of description; technical terms and jargon used; appropriateness of information disclosed; ii) the emotional dimension, concerned with the rapport between researcher and subject; and iii) the interactional dimension, concerned with the capacity and willingness of the researcher to perceive and discuss the emotional needs, concerns and complaints of the subject, and to deal with these concerns.
• Test beliefs about volunteers’ perceptions of the trustworthiness of researchers, through the
support/advocate person.
2.2.5. ONGOING MONITORING OF INFORMATION PROVIDED There should be ongoing monitoring of information provided to volunteers. Regular feedback interviews with participants should be done by research counsellors in order to ascertain what kind of information participants would have found helpful at the start of the project which can be used for new recruits into the project; as well as what kinds of issues are emerging that participants would have liked to consider in deciding whether or not to participate in the project, and which they would like to now discuss. 2.3. UNDERSTANDING AND DECISION MAKING: Adequate understanding is an essential aspect of informed consent. It is recommended that this understanding goes beyond short-term recall of technical information. It should include understanding of personal implications of participation. Assessment of understanding should be an ongoing part of information counselling. To facilitate understanding it is recommended that:
• The videotape should include clips illustrating one participant explaining the research to another person, and telling the story of their participation.
• Following the screening of videotape as described above, allow interactive discussion to
improve and assess understanding.
• Researchers should apprise themselves of the life circumstances of potential participants, with the assistance of community representatives and a community advisory board, in order to identify which personal implications of participation it is important for participants to understand.
• That the right to withdraw from the study at any stage without prejudice is fully understood
by volunteers and ensured.
Page -27-
• An advocacy/support counsellor should assist volunteers in identifying desired benefits and potential risks, and in reminding volunteers of their right to withdraw.
• Follow-up visits should be scheduled at which participants can raise personal questions.
• Family and friends should be allowed and encouraged to attend a follow-up visit to raise questions.
• Time is allowed for further discussion of issues after talking with family, friends and
support persons.
2.3.1. ASSESSMENT OF UNDERSTANDING BY VOLUNTEERS In order to assess various facets of understanding, it is recommended that:
• The research team, in collaboration with the community advisory board, establish a list of essential technical issues, which require understanding, e.g., that the vaccine being tested cannot be assumed to provide protection.
• Understanding of these essential technical issues should be assessed through specific
questions, but also through discussion of typical scenarios from volunteers’ lives.
• Volunteers should be asked to explain in their own words what the research is about and its implications for themselves and significant others.
• Understanding should be checked at different stages of the study.
2.3.2. RESEARCH TEAM UNDERSTANDING OF VOLUNTEERS’ MOTIVATIONS From the outset, researchers should view the transmission of information as a two-way process, and set in place processes for researchers to obtain necessary information from the community and participants about the implications of participation in the project. Arrangements should be made for mutual informational exchange during the course of the research project, with the researchers viewed as recipients of information as much as potential participants. Research counsellors should provide constant feedback to researchers about the kind of information that they need in order to better comprehend the position of participants. Specific recommendations regarding research team understanding include:
• A sample of interviews with volunteers should be evaluated to assess the extent to which research counsellors understand the issues facing participants.
• Request ratings by volunteers, with the help of the advocacy/support counsellor, of
volunteers’ perceptions of researcher understanding.
• Research counsellors should monitor the ongoing experiences of participants. Regular feedback to researchers about experiences of participants should be arranged, in order that researchers can provide more helpful information to other participants.

Page -28-

Page -29-
2.4. VOLUNTARINESS AND FREEDOM FROM COERCION: An essential component of informed consent is the freedom to make the decision to participate or not, in one’s own best interest, without coercion of any nature. Specific recommendations to facilitate freedom from coercion are:
• Researchers need to explore potential recruits’ motivations to participate with the help of a community advisory group.
• The provision of information about expectations and motivations, and the extent to which
they will be met in the study or not, should be facilitated by an advocate/support person.
• Sufficient time should be allowed before participants are required to commit themselves to participation. This should be at least enough time to discuss the matter with people at home and in the community if they so choose.
• Require the advocacy/support counsellor to identify and voice any aspect of coercion to
participate. This counsellor can especially assist in overcoming obstacles created by social desirability pressures.
2.5. CONSENT Informed consent requires that participants have the capacity to decide about participation in research; that is, potential recruits have the legal status of adults and are not mentally impaired. It is assumed that participants are in a position to make decision for themselves. Consent refers to the autonomous and explicit agreement by individuals to participate in a research project based on their informed understanding of what it entails. In order to foster free consent the following recommendations are made:
• Advocacy/support counsellors should assist volunteers in identifying and voicing reservations about consent, to overcome social desirability pressures.
• Potential participants should be allowed time before requiring them to commit themselves to
participate, as well as a “cooling off” period before participation commences.
• In the case where participants are illiterate they should at least provide the fingerprints as recorded evidence of consent.
• Every participant should have their signature or finger print recorded in the presence of
witnesses.
• The bilateral nature of consent should be recognized. The implicit hopes and expectations of individuals, families and community should be encouraged to be voiced, with a commitment, following negotiation, to meeting or not meeting these expectations on the part of the scientific team. It is the responsibility of the scientific team, through advocacy/support counsellors and the community advisory board, to introduce important
Page -30-
issues, such as provisions for participants at the end of the trial, as communities and volunteers may not have sufficient grasp of the implications of the trial to raise them.
• The willingness of people to continue to participate should be checked at different stages of
the project.
• Advocacy/support counsellors should assist in the drafting of consent forms, and assist volunteers in understanding and signing them.
• Family, friends and advocacy/support counsellors should be invited to witness the
consenting process (with the agreement of the volunteer), especially where volunteers are illiterate.
2.5.1. PHASED CONSENT The ongoing research project is likely to involve a series of distinct stages. Each stage of the volunteer’s participation should be spelled out, and explicit consent should be obtained for each stage, in addition to consent to participate in the project as a whole. For example, volunteers will need to consent to HIV-testing, to being vaccinated or to receive other treatment, to being examined, to give biological samples at various stages, and so on. It is also important that the consent of the community, via the community advisory board, be obtained for processes such as the public release of information derived from the study.
2.5.2. ONGOING RIGHT TO WITHDRAW The research team and volunteers need to bear in mind the ongoing right of volunteers to withdraw from the study. In this connection:
• Advocacy/support staff should frequently review with volunteers their right to withdraw from the study without prejudice.
• Researchers should regularly assess willingness for ongoing participation in the research
project, rather than assume that participants are aware of the right to withdraw at any time.
• Where possible, ambivalent participants should be introduced to other participants who have remained in the study, and to some who have chosen to withdraw from the study and have done so without prejudice. If, and where possible, incorporate an interview with such participants should be presented on videotape.
2.5.3. MULTI-PERSON CONSENT Most informed consent considerations are founded upon philosophical assumptions of rugged individualism, which may not be shared by all cultural groups and communities. Certain cultural views may define the meaning of persons in relationships with others, and this may affect how individual informed consent is understood. There may be explicit community norms regarding who should be consulted for agreement that any particular individual can be approached to participate in research trials; for example, parents, community leaders etc.
Page -31-
It is recommended that the principle of respect for individual autonomy is preserved as a universal principle in research trials, not being substituted by any other principle. But it is also important that the research team identify, understand and respect other cultural norms pertaining to individual participation in research trials. Therefore, it is recommended that in addition to always seeking individual consent, other family and community members should be incorporated into various stages and aspects of the informed consent process, but only with the explicit consent of the volunteer concerned. Specific recommendations regarding whose consent to seek include:
• Community partnerships on the project should be facilitates, and community groups should be consulted regarding general principles of who should be approached about consent procedures.
• All parties that need to be consulted and whose cooperation should be obtained in the case
of each potential participant should be identified. Participants should be invited and encouraged to involve these people in the informed consent process if they so choose, and such people should be invited to attend information sessions.
• Where participants decline opportunities for other family or community members to be
involved in their recruitment into the study, or where such involvement is difficult or inappropriate, the wishes of the individual person should be respected.
• Researchers should ascertain if there are any community-based constraints to particular
volunteers participating in the research.
2.5.4. AGREEMENT ABOUT COMPENSATION This document has recommended that research trials be seen as involving partnerships between researchers and the community participating in research. Further, it has been recommended that informed consent should always be seen as a mutual decision making process. Giving that there is always likely to be some degree of expectation from communities and individuals regarding the benefits to be derived from participation in research trials, it is recommended that consent should be seen as a two-way process. In addition to volunteers consenting to various aspects of participation in the research trial, it is recommended that researchers also indicate their explicit consent to meeting negotiated expectations of communities and volunteers. These may include expectations about employment and economic investment in the community, upgrading of health facilities, financial compensation for time lost to do household work, access to treatments, and so on. Other recommendations include:
• Specific expectations of community, volunteers and families should be identified early in the research trial.
• Motivations for participation should be identified with the help of the community advisory
board, advocacy/support counsellors and others.
• The research team should explicitly address expectations of the community and volunteers, by making clear which expectations can be met and to what extent.
Page -32-
• The motivations and expectations of individual volunteers should be carefully monitored by
research counsellors. Where these are substantially different from those negotiated and consented to with community representatives, they should be brought to the attention of the research team before acceptance of particular volunteers into the research trial.
2.6. EVALUATION OF THE CONSENT PROCESS AND CONDITIONS: It is recommended that there should be ongoing evaluation of the consent process and conditions in order to monitor and improve on various aspects of consent. Reference has already been made to various ongoing evaluation procedures and includes:
• Evaluation of the process/interactional aspects of informational counselling, through the application of evaluation measures, such as those of Meerwein, to samples of interviews observed or videotaped.
• With the assistance of advocacy/support staff, there should be ongoing evaluation of the
research team’s understanding of the situations and experiences of volunteers.
• There should be regular monitoring of the experience of volunteers and feedback to the research team in order to improve the quality of information and understanding early in the research trial.
• There should be ongoing monitoring and feedback regarding understanding of various issues
by volunteers at different stages of the research trial.
• Advocacy/support staff should be requested to monitor and offer regular feedback regarding protection of the autonomy of volunteers at different stages of the research trial, e.g. regarding the right to withdraw without prejudice or disadvantage.
2.7. PROTOCOL FOR IMPLEMENTING A CULTURALLY SENSITIVE INFORMED
CONSENT PROCESS
2.7.1. PRE-RECRUITMENT STAGE
• The scientific team needs to discuss and reach consensus on ethical issues implied by the research design. Commitments to uphold ethical standards with respect to all features of the study should be made explicit and incorporated into the training of all staff.
• Community leaders and representatives need to be identified.
• Explicit agreements should be reached regarding project collaboration between research
team and community, including terms and conditions.
Page -33-
• Advocacy/support counsellors to be selected and trained, and their conditions of operation
clarified.
• Facilitate the establishment of a community advisory board (CAB) consisting of people known for their leadership and independence.
• A strategy should be developed to ensure that all members of the scientific team are
acquainted with the necessary cultural knowledge of people in the community to be able to relate to them in culturally sensitive ways.
2.7.2. PREPARATION FOR INFORMED CONSENT
• Detailed and repeated discussions of the project need to be held with community leaders and the community advisory board to ensure that the purposes and methods of the study are understood.
• Ethnographic research needs to be conducted among potential volunteers in order to identify
attitudes towards the study and potential barriers and obstacles to participation. Attitudes to immunization practices in general may also provide important sources of valued information for HIV vaccine trials.
• Together the scientific team and the community advisory board need to identify the major
issues and values of likely concern to the community and potential participants regarding the project.
• The scientific team and the community advisory board need to identify the major
motivations, advantages and disadvantages of participation to community members.
• Expectations about individual and community benefits need to be made explicit as well as agreements regarding meeting expectations.
• The scientific team needs to identify major components of information about the study thought to be necessary for transmission to potential participants.
• These informational components should be discussed with community advisors in order to
decide what information potential participants should have in order to make an informed decision to participate in the study, who would best convey this information to potential participants, when, where and how.
• The scientific team and the community advisory group should establish a check list of
essential components to be understood for participation.
• The community advisory board should establish a list of essential issues about the local community that need to be understood and taken into account by the scientific team before commencing the research.
Page -34-
• Community education through meetings and via media should be undertaken to facilitate general understanding of the essential components identified;
• A videotape recording should be prepared, with the assistance of educational experts and
community representatives, conveying all the information identified, including hypothetical questions by participants and some case illustrations of different scenarios.
• Structures and functions for research counsellors and advocacy/support counsellors, as well
as lines of accountability, should be set in place.
• The informed consent form needs to be drafted and submitted for the approval of the IRB (or equivalent) and the CAB.
2.7.3. RECRUITMENT
• Initial contacts should be made with potential participants once significant progress has been made with community preparation.
• Following preliminary interest, research staff should arrange for a meeting and screening of
the videotape, followed by discussion and counselling around personal issues.
• The support/advocacy staff should meet independently with potential participants to explain their advocacy role and function.
• Individual interviews should be arranged with potential participants. In the interviews
attempts should be made to identify the person’s expectations of benefit from participation, as well as likely personal implications of participation.
• People, whose agreement is important to the potential participant, should be identified and
invited to see the video, if and when explicit agreement for this has been obtained from the participant.
• The possible participation of these people and their role in the informed consent process should be discussed.
• A further screening of the videotape and discussion of issues should be offered to family and
others whom the potential participant wishes to consult about involvement in the study.
• Advocacy/support counsellors should meet with volunteers and family/friends to identify and articulate possible concerns to be considered and discussed before deciding about participation.
• An information sheet and informed consent form, prepared with the help of educational
experts and advocacy counsellors, should be given to the potential participant to take home and discuss with significant others.
• The potential participant should be put in contact with other volunteers, or people already
Page -35-
participating in the study, as they become available.
2.7.4. EVALUATION OF RECRUITMENT PROCEDURES, INCLUDING UNDERSTANDING
• Potential participants who have been exposed to the initial contact procedures should be
interviewed by advocacy/support counsellors to evaluate the quality of the initial procedures using a multi-level model such as that of Meerwein, as well as their degree of satisfaction with these interviews and procedures.
• Advocacy/support counsellors should summarise potential participants’ fears and concerns
and report these to the scientific team.
• Strategies should be devised to address these concerns and fears.
• Random recordings or observation of initial interviews should be evaluated for process/interactive aspects of effective communication, and staff feedback and further training should follow.
• Potential participants should be interviewed to assess their understanding.
• In addition to assessment of the specific understanding of some of the core technical issues,
participants’ understanding of the personal implications of participation in the research should be assessed through discussion of vignettes.
• Specific questions should be addressed to participants to assess understanding of essential
technical issues.
• In interviews, potential participants should be asked to give their understanding of the aims and procedures of the research.
• Motivations, expectations and concerns of potential participants should be discussed.
• Individual descriptions and responses need to be evaluated according to criteria established
by the research team, to assess adequacy of understanding of key components identified to be essential to informed decision making. When required, remedial steps need to be taken to improve understanding.
• If desired by potential participants, the process should be repeated with family or friends.
• If requested by the potential participant, the advocacy/support counsellor should be present
to speak on behalf of the participant and to assist with the estimation of the level of understanding obtained.
• Assessment of understanding should be repeated at all identified stages of the research
process.
Page -36-
2.7.5. OBTAINING CONSENT
• Family and other people whose support or agreement is regarded as desirable should be identified with the volunteer, if s/he provides consent for this.
• Following exposure to information, videotape and discussion, a meeting should be held with
these people together with the potential participant.
• Opportunity should be provided for further questions or discussion about participation in the research.
• Expectations of the participant and family/community should be discussed and, where
necessary, corrected.
• An advocacy/support counsellor and/or a community representative may be present for the discussion if the participant prefers this.
• The volunteer is invited to sign the agreement or record finger print (if illiterate) in the
presence of witnesses.
• The IC form should contain the signatures of: the principal investigator or her/his representative, the research counselor, the participant, independent witness.
• Where family or community members have been involved in the informed consent process,
they are invited to indicate their support (as opposed to consent) for the person participating in the research process.
• A written copy of the obligations of the research team is made available to the volunteer.
• At any stage where particular steps are to be taken which may affect the community, e.g. the
public release of information from the research, this should only be with the written consent of the community advisory board.
2.7.6. ONGOING CONSENT, COUNSELLING AND EVALUATION
• At each stage where major procedures are implemented, specific informed consent procedures should be implemented. Obvious points at which IC must be obtained include: i) initial consent to be tested for HIV; ii) following testing and invitation to participate in study, specific consent to participate in the study.
• At regular intervals, research counsellors should approach participants to assess ongoing
willingness to participate in the research.
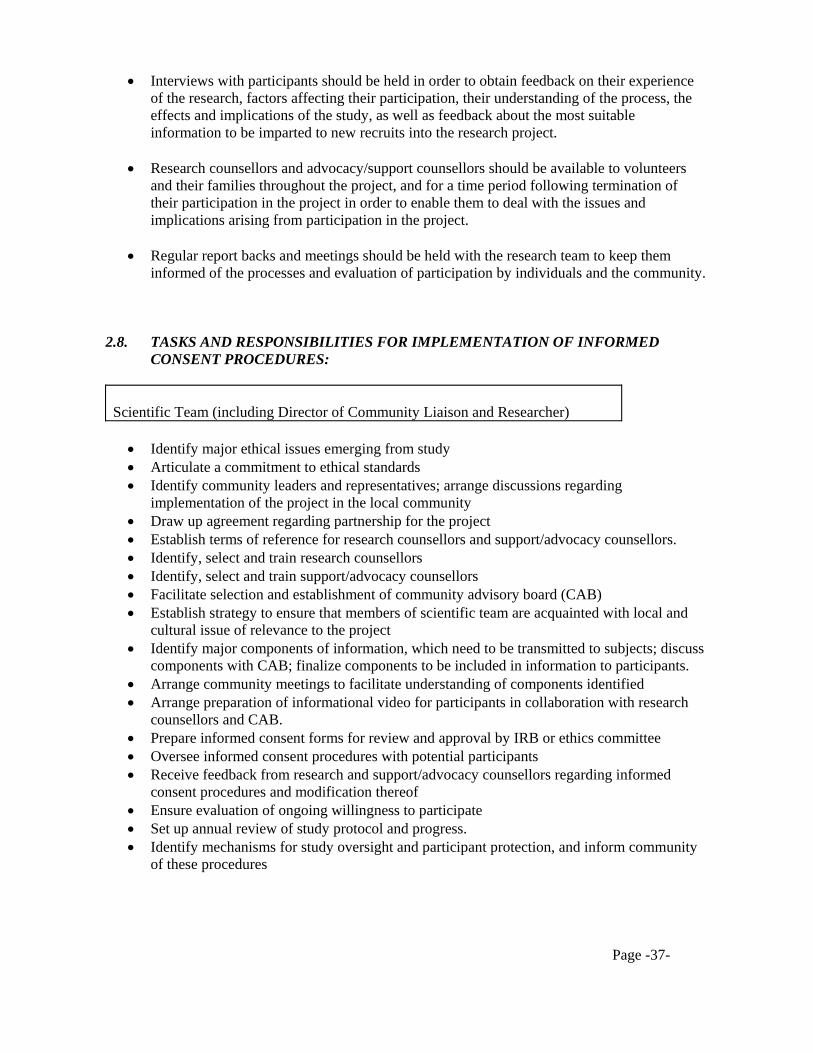
Page -37-
• Interviews with participants should be held in order to obtain feedback on their experience of the research, factors affecting their participation, their understanding of the process, the effects and implications of the study, as well as feedback about the most suitable information to be imparted to new recruits into the research project.
• Research counsellors and advocacy/support counsellors should be available to volunteers
and their families throughout the project, and for a time period following termination of their participation in the project in order to enable them to deal with the issues and implications arising from participation in the project.
• Regular report backs and meetings should be held with the research team to keep them
informed of the processes and evaluation of participation by individuals and the community. 2.8. TASKS AND RESPONSIBILITIES FOR IMPLEMENTATION OF INFORMED
CONSENT PROCEDURES: Scientific Team (including Director of Community Liaison and Researcher)
• Identify major ethical issues emerging from study • Articulate a commitment to ethical standards • Identify community leaders and representatives; arrange discussions regarding
implementation of the project in the local community • Draw up agreement regarding partnership for the project • Establish terms of reference for research counsellors and support/advocacy counsellors. • Identify, select and train research counsellors • Identify, select and train support/advocacy counsellors • Facilitate selection and establishment of community advisory board (CAB) • Establish strategy to ensure that members of scientific team are acquainted with local and
cultural issue of relevance to the project • Identify major components of information, which need to be transmitted to subjects; discuss
components with CAB; finalize components to be included in information to participants. • Arrange community meetings to facilitate understanding of components identified • Arrange preparation of informational video for participants in collaboration with research
counsellors and CAB. • Prepare informed consent forms for review and approval by IRB or ethics committee • Oversee informed consent procedures with potential participants • Receive feedback from research and support/advocacy counsellors regarding informed
consent procedures and modification thereof • Ensure evaluation of ongoing willingness to participate • Set up annual review of study protocol and progress. • Identify mechanisms for study oversight and participant protection, and inform community
of these procedures

Page -38-
Instutional Review Board - IRB
Not all countries have formal procedures or protocols for the establishment and functioning of IRB’s. Some countries may operate with structures such as Ethics Committees of medical schools or similar bodies. In each country the appropriate authority needs to be identified or established.
• Identify appropriate authority to oversee ethics of study. • Review and approve of IC forms • Review and approve of any modification to IC forms on basis of feedback from participants
Community Advisory Board: CAB
• Assist with identifying major issues affecting the local community • Assist with initial research into attitudes of potential participants to the study • Assist with identification of motivations and expectations of participants • Assist with identifying components of information which need to be transmitted to subjects
and how best to do this • Assist with the preparation of informed consent forms • Assume responsibility for establishing understanding of cultural and local issues by
scientific team • Provide ongoing commentary on the study
Research Counsellors
• Assist with research into attitudes of potential participants to the study • Assist with establishing motivations and expectations of participants • Assist with identifying components of information which need to be transmitted to subjects
and how best to do this • Identify major components of information which need to be transmitted to subjects; discuss
components with CAB; finalize components to be included in information to participants; establish checklist of items
• Assist with preparation of informed consent forms • Establish network of community links for referral, where necessary • Make preliminary contact with potential participants • Arrange screening of video recording • Arrange preliminary interviews with potential participants • Identify family/community members to be incorporated into informed consent procedures • Arrange to see family/community members, plus video screening • Arrange contact with other willing participants • Interview and assessment of understanding by participants, and follow up to improve
understanding, if necessary
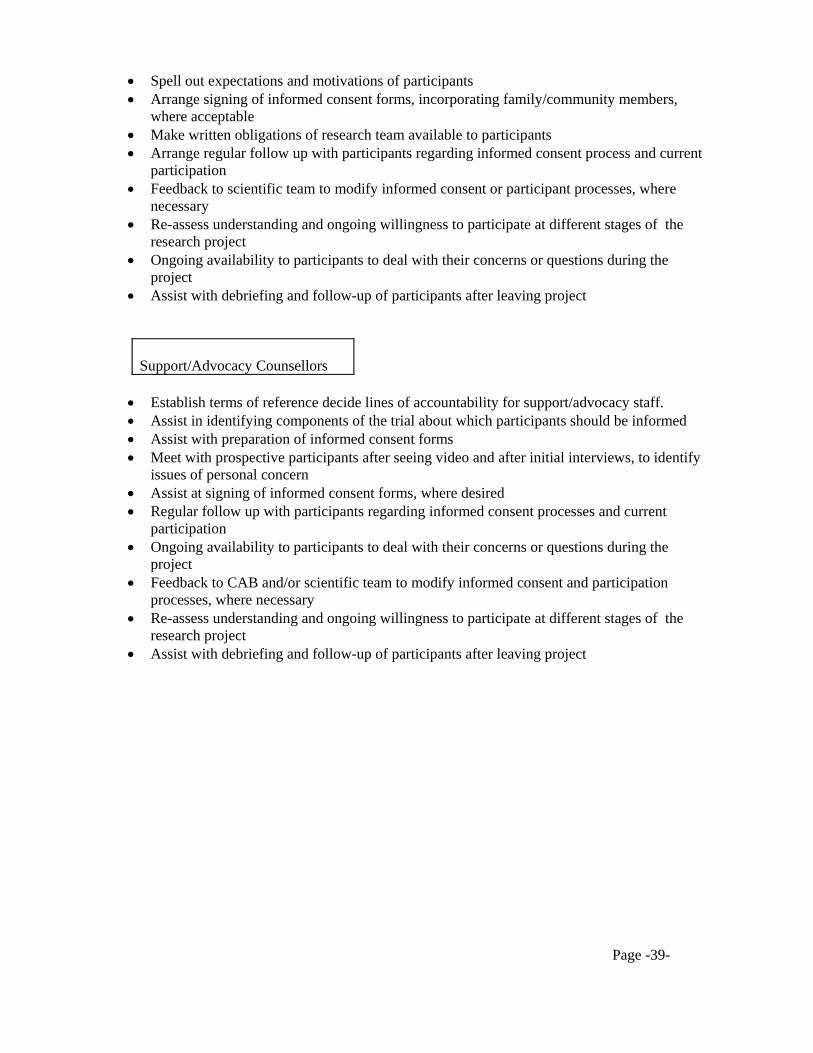
Page -39-
• Spell out expectations and motivations of participants • Arrange signing of informed consent forms, incorporating family/community members,
where acceptable • Make written obligations of research team available to participants • Arrange regular follow up with participants regarding informed consent process and current
participation • Feedback to scientific team to modify informed consent or participant processes, where
necessary • Re-assess understanding and ongoing willingness to participate at different stages of the
research project • Ongoing availability to participants to deal with their concerns or questions during the
project • Assist with debriefing and follow-up of participants after leaving project
Support/Advocacy Counsellors
• Establish terms of reference decide lines of accountability for support/advocacy staff. • Assist in identifying components of the trial about which participants should be informed • Assist with preparation of informed consent forms • Meet with prospective participants after seeing video and after initial interviews, to identify
issues of personal concern • Assist at signing of informed consent forms, where desired • Regular follow up with participants regarding informed consent processes and current
participation • Ongoing availability to participants to deal with their concerns or questions during the
project • Feedback to CAB and/or scientific team to modify informed consent and participation
processes, where necessary • Re-assess understanding and ongoing willingness to participate at different stages of the
research project • Assist with debriefing and follow-up of participants after leaving project

Page -40-
2.9. TIME LINE: The time line given below is a rough estimate of the time required to prepare a community or facility and obtain the necessary agreement and consent from all involved. Some procedures, such as recruitment, obtaining consent, and ongoing counselling and evaluation, will continue for the duration of the trial.
Activity outlined in protocol (2.7) Months ->
1
2
3
4
5
6
7
8
9
-
-
-
PRE-RECRUITMENT STAGE (2.7.1)
xxxx
xxxx
xxxx
xxxx
PREPARATION FOR INFORMED CONSENT (2.7.2)
xxxx
xxxx
xxxx
xxxx
RECRUITMENT (2.7.3)
xxxx
xxxx
xxxx
xxxx
->
->
-> EVALUATION OF RECRUITMENT PROCEDURES (2.7.4)
xxxx
xxxx
xxxx
xxxx
OBTAINING CONSENT (2.7.5)
xxxx
xxxx
xxxx
xxxx
xxxx
ONGOING COUNSELLING AND EVALUATION (2.7.6)
xxxx
xxxx
xxxx
xxxx
xxxx
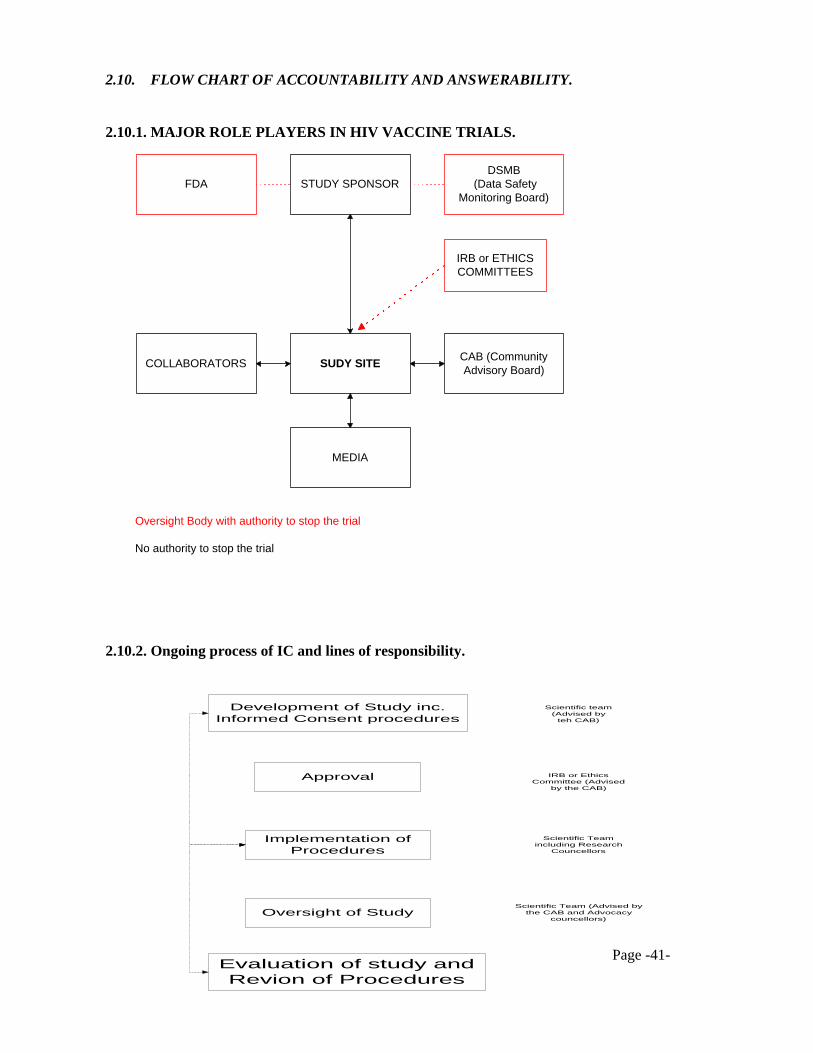
Page -41-
2.10. FLOW CHART OF ACCOUNTABILITY AND ANSWERABILITY.
2.10.1. MAJOR ROLE PLAYERS IN HIV VACCINE TRIALS.
2.10.2. Ongoing process of IC and lines of responsibility.
STUDY SPONSORFDADSMB
(Data SafetyMonitoring Board)
SUDY SITECOLLABORATORS
IRB or ETHICSCOMMITTEES
CAB (CommunityAdvisory Board)
MEDIA
Oversight Body with authority to stop the trial
No authority to stop the trial
Development of Study inc.Informed Consent procedures
Scientific team(Advised by
teh CAB)
Approval IRB or EthicsCommittee (Advised
by the CAB)
Implementation ofProcedures
Scientific Teamincluding Research
Councellors
Oversight of StudyScientific Team (Advised by
the CAB and Advocacycouncellors)
Evaluation of study andRevion of Procedures
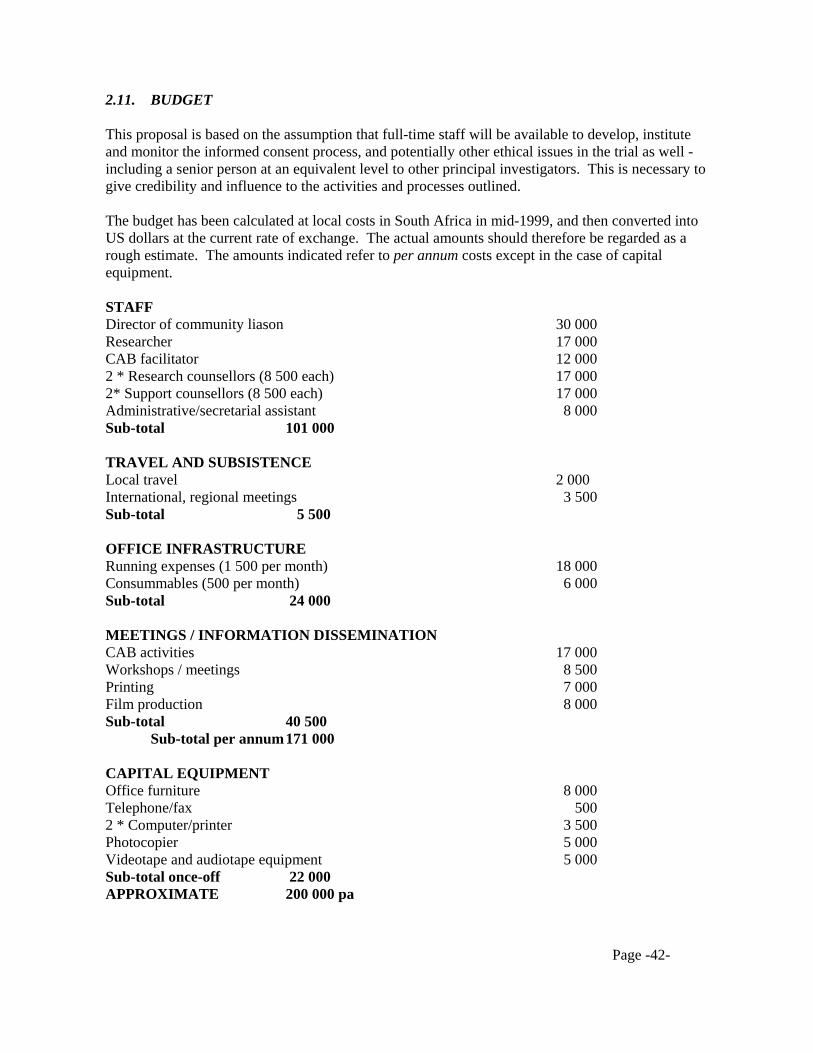
Page -42-
2.11. BUDGET This proposal is based on the assumption that full-time staff will be available to develop, institute and monitor the informed consent process, and potentially other ethical issues in the trial as well - including a senior person at an equivalent level to other principal investigators. This is necessary to give credibility and influence to the activities and processes outlined. The budget has been calculated at local costs in South Africa in mid-1999, and then converted into US dollars at the current rate of exchange. The actual amounts should therefore be regarded as a rough estimate. The amounts indicated refer to per annum costs except in the case of capital equipment. STAFF Director of community liason 30 000 Researcher 17 000 CAB facilitator 12 000 2 * Research counsellors (8 500 each) 17 000 2* Support counsellors (8 500 each) 17 000 Administrative/secretarial assistant 8 000 Sub-total 101 000 TRAVEL AND SUBSISTENCE Local travel 2 000 International, regional meetings 3 500 Sub-total 5 500 OFFICE INFRASTRUCTURE Running expenses (1 500 per month) 18 000 Consummables (500 per month) 6 000 Sub-total 24 000 MEETINGS / INFORMATION DISSEMINATION CAB activities 17 000 Workshops / meetings 8 500 Printing 7 000 Film production 8 000 Sub-total 40 500 Sub-total per annum 171 000 CAPITAL EQUIPMENT Office furniture 8 000 Telephone/fax 500 2 * Computer/printer 3 500 Photocopier 5 000 Videotape and audiotape equipment 5 000 Sub-total once-off 22 000 APPROXIMATE 200 000 pa
Page -43-
PART 3: PROCEEDINGS OF UNAIDS MEETING The protocol proposed in this document was presented and discussed at a special UNAIDS meeting 28-30 June 1999 to discuss social and behavioural aspects of HIV vaccine trials. The following is a summary of the issues, which emerged from the discussion of this document: 1.1. There was strong general support expressed for the assumptions, principles and procedures
in the document on culturally sensitive approaches to informed consent for HIV vaccine trials.
1.2. The largest portion of time in the discussion of this document was spent on the discussion of
the advocacy issue in HIV vaccine trials. 2.1. There was particular support expressed for the centrality of an advocacy function in order to
protect the rights, interests and well-being of participants in HIV vaccine trials, especially where these trials take place in developing countries. This was especially because of the recognized vulnerability, which characterizes typical populations likely to be involved in vaccine trials because of their high susceptibility to HIV infection.
2.2. But it was also recognized that the exact method of implementation of such advocacy
procedures would vary from one country and local context to another. 2.3. While the possible value of advocacy counsellors (as recommended in the document) was
acknowledged, there was concern expressed about a possible confusion in the mind of the participants, the community and the scientific team, about the relative roles and functions of the research counsellors as opposed to advocacy counsellors.
2.4. Further, the lines of accountability of the proposed advocacy counsellors was debated at
length. It was suggested that if the study donors were funding advocacy counsellors, then in effect it was to the study donors that these counsellors would be perceived as being accountable, potentially undermining their important and independent advocacy function. There was lengthy discussion on possible ways of implementing such advocacy functions in different contexts, including the use of para-legal NGO’s as possible bodies, which could assume the primary responsibility for the accountability of such advocacy counsellors. It was recognized that each country and local context would need to explore its own best method of implementation of advocacy functions in clinical trials.
2.5. The potential danger of a developing antagonism between scientific team and
community/participants (or between IRB and CAB) through advocacy procedures was acknowledged, and of the potential risk of a split between these role players recognized. The importance of a collaborative relationship and of maintaining the view of clinical trials as a scientific team/community partnership, alongside the protection of the rights of participants, was recognized and endorsed.
The lines of accountability and responsibility for various role players in HIV vaccine trials also involved a considerable amount of discussion. The need for clarity regarding lines of accountability was stressed.
Page -44-
3.1. Diagrams 2.10.1. and 2.10.2. above were developed in order to clarify the primary lines of
accountability in HIV vaccine trials. 3.2. It was agreed that the IRB or local equivalent in various countries, had the primary
responsibility for overseeing the ethical aspects of clinical trials, and was therefore ultimately responsible for the protection of participants. In particular the IRB was responsible for the approval of informed consent forms, including any and all changes to these forms. But IRB’s would be advised by CAB’s in the execution of this function.
3.3. In clarifying the respective roles and functions, the meeting acknowledged the central
importance of the CAB and of seeing clinical trials as operating from a partnership of scientific team and community. It was generally agreed, however, that the CAB should not be perceived as part of the research team, and therefore should be protected from being perceived as partially responsible for any negative effects of the research.
The importance of ethical considerations as opposed to indemnity considerations were discussed and endorsed by the meeting, although this distinction seemed more important to developing than to developed countries. 4.1. At the same time, it was stressed that the signing of the informed consent form in no ways
leads to a surrendering of legal rights on the part of participants. The importance of informed consent as an ongoing ethical process, rather than a once-off procedure was discussed and endorsed by the meeting. This led to the development of the flow chart in 2.10.2 above, indicating the relative responsibilities of different role players in the ongoing process. 5.1. A distinction was drawn between process and formal material in informed consent. The
importance of constantly monitoring and evaluating the IC process was endorsed by the meeting. It was agreed that the implementation of IC procedures might be modified in clinical trials as a result of monitoring and feedback, in order to better implement the spirit of IC. But, it was also stressed that informed consent forms may not be altered without the explicit approval of the IRB or equivalent.
5.2.1. The importance of recognizing the need for repeated consent at different stages was also
acknowledged by the meeting. However, there was concern expressed about the possible burden of administrative procedures with constant repetition of IC procedures at different stages. It was agreed that the major points of repeated consent needed to be clearly identified before the start of the clinical trial.
5.3. The meeting recognized the need for ongoing counselling of research participants. It was suggested that this counselling could be seen as part of the IC process, and different to the formal aspects of IC such as the consent form. It was agreed that through a process of ongoing feedback some of the process aspects of IC might by altered (e.g. the exact way in which information was explained to participants), while the actual IC form would remain the same.
6. There was some debate around the issue of consent forms as such. The meeting
acknowledged the importance of the consent form and its approval by the IRB. However, there was some discussion and debate about the relative importance of the form itself in
Page -45-
different and cultural contexts, with the recognition that in countries or cultures with primarily oral traditions these forms might be perceived as playing a less significant role.
7. The discussion also recognized the importance of prior research into vaccination and its
implications for HIV vaccine research. It was suggested that careful notice should be taken of the findings of studies on vaccination in various contexts, and especially of studying the perceptions and attitudes of local communities to vaccination, because of the potential implications for HIV vaccine trials.