discover the power of meaningful activity
TRANSCRIPT
Discover The Power Of
Meaningful Activity
Barbara Speedling Quality of Life Specialist
LANY – Webinar 2021

The Birth of Culture ChangeCMS 2007 Action Plan for Nursing Home Quality
o “Culture Change principles echo OBRA principles of knowing and
respecting each nursing home resident in order to provide
individualized care that best enhances each person’s quality of life.”
o “The concept of Culture Change encourages facilities to change
outdated practices to allow residents more input into their own care
and encourages staff to serve as a team that responds to what each
person wants and needs.”

The Intent of Culture Change
o The “culture change” movement aims to transition
nursing homes from institutions to homes for
residents that improve the quality of care and quality
of life of residents.
o The philosophy of the culture change movement
embraces the person-centered concept, while also
supporting the improvement of work conditions for
staff.

The Intent of Culture Change
Key principles of the culture change movement include:
o Resident-directed care and activities;
o Home environment;
o Relationships with staff, family, residents, and community;
o Staff empowerment;
o Collaborative and decentralized management; and
o Measurement-based continuous quality improvement (CQI)
process

Person-Centered Care
“…a framework for health and social care
assessment, including risk assessment,
within a comprehensive, person centered,
multi-disciplinary care planning process.’
(Thiru et al., 2002, p. 11)

F675 Quality of life
Definition: “Quality of Life”
•An individual’s “sense of well-being, level of
satisfaction with life and feeling of self-worth and
self-esteem.
•For nursing home residents, this includes a basic sense
of satisfaction with oneself, the environment, the care
received, the accomplishments of desired goals, and
control over one’s life.”

The Woodstock Generation
THEN NOW
Drug Abuse and
Mental Health Issues
A 2011 study by the Substance Abuse and Mental
Health Services Administration found:
• Baby Boomers who came of age in the ‘60s and ‘70s
when drug experimentation was pervasive, are far
more likely to use illicit drugs;
• Among adults 50-59, current illicit drug use increased
to 6.3 percent in 2011 from 2.7 percent in 2002;
• The most commonly abused drugs were opiates,
cocaine and marijuana.
Drug Abuse and
Mental Health Issues
2010: An estimated six to eight million older Americans – almost 20 % of the elderly population – had one or more substance abuse or mental health disorders.
2030: Adults 65 and older is projected to increase to 73 million from 40 million between 2010 and 2030.
http://newoldage.blogs.nytimes.com/2013/04/29/a-rising-tide-of-mental-distress/

Increased Numbers of Disabled Young Adults
• The number of children and young adults with disabilities is increasing.
• Life-saving and life-prolonging medical care and new technologies have increased the survival of seriously ill younger people.
• These children, teens and young adults will need long-term care to assist them in their homes or in nursing homes and residential facilities.
LTC Panel Report 2009
F838 FACILITY ASSESSMENT
• The facility must conduct and document a facility-wide assessment to determine
what resources are necessary to care for its residents competently during both
day-to-day operations and emergencies.
– Review and update at least annually, whenever there is, or the facility plans for, any
change that would require a substantial modification to any part of this assessment;
– Must address or include a facility-based and community-based risk assessment,
utilizing an all-hazards approach;
– The results of the facility assessment must be used, in part, to establish and update
the IPCP, its policies and/or protocols to include a system for preventing, identifying,
reporting, investigating, and controlling infections and communicable diseases for
residents, staff, and visitors.
• Note: a community-based risk assessment should include review for risk of
infections (e.g., Multidrug-resistant organisms- MDROS) and communicable
diseases such as tuberculosis and influenza. Appropriate resident tuberculosis
screening should be performed based on state requirements.

What Keeps Us from Better Behavior?
“When you don’t get what you want (or need),
you get an attitude.”
-Regina, (57), Brooklyn, NY
Nursing Home Resident

Living in Retrograde
“I want what I had”

What is Grief?
Whenever we face loss, we experience grief. Everyone grieves
differently, yet there are some common responses you might expect.
Source: https://hospicefoundation.org/Grief-(1)/What-to-Expect

What is Grief?
• Grief is a reaction to loss.
• People may have different “styles” of grieving.
• There is no timetable to grief.
– Over time the pain lessens, and we return to similar—sometimes
better--levels of functioning.

The Relationship Between Trauma and Grief
Trauma is an event.
•It can be any event that causes psychological, physical, emotional or
mental harm; such as a death or abuse.
•A traumatic event could also be called a loss event. If someone dies,
that’s a loss. If someone was abused, that too is a loss. A loss of trust.
•The result of a traumatic event is grief.
Source: https://www.griefrecoverymethod.com/blog/2015/02/what-difference-between-trauma-and-grief

The Relationship Between Trauma and Grief
Grief is the normal and natural response to loss.
•It’s the conflicting emotions that result in the end of, or
change in, a familiar pattern or behavior.
•Grief is the feeling of wishing things would have ended
different, better, or more.
•Grief is the normal and natural feelings after a trauma.
Source: https://www.griefrecoverymethod.com/blog/2015/02/what-difference-between-trauma-and-grief
F699
Trauma-Informed care
§483.25(m) Trauma-informed care
The facility must ensure that residents who are trauma survivors
receive culturally competent, trauma-informed care in
accordance with professional standards of practice and
accounting for residents’ experiences and preferences in order to
eliminate or mitigate triggers that may cause re-traumatization of
the resident.
What is Cultural Competency?
• Cultural competence is the ability to understand, communicate with and effectively interact with people across cultures.
• Cultural competence encompasses. being aware of one's own world view. developing positive attitudes towards cultural differences, gaining knowledge of different cultural practices and world views.
Source: makeitourbusiness.ca/blog/what-does-it-mean-be-culturally-competent

What is Trauma-Informed Care?
Trauma-Informed Care understands and
considers the pervasive nature of trauma and
promotes environments of healing and recovery
rather than practices and services that may
inadvertently re-traumatize.
2019 Coronavirus Pandemic
Trauma can be defined as a psychological,
emotional response to an event or an experience
that is deeply distressing or disturbing.
2019 Coronavirus Pandemic
What is Traumatic about COVID-19?
•Fear of life-threatening illness
•Being separated from friends and family
•Giving up your customary routine for an indefinite
period of time
•Unable to work or travel
•Financial instability
•Loneliness

The Five Principles of Trauma-Informed Care
• The Five Guiding Principles are; – Safety;
– Choice;
– Collaboration;
– Trustworthiness; and
– Empowerment.
• Ensuring that the physical and emotional safety of an individual is addressed is the first important step to providing Trauma-Informed Care.
http://socialwork.buffalo.edu/social-research/institutes-centers/institute-on-trauma-and-trauma-informed-care/what-is-trauma-informed-care.html

AssessmentWhen, Where, and How…

THE GLOBAL
DETERIORATION
SCALE
Assessing The Degree
Of Dementia

Communication
Language Disturbance
Aphasia
Apraxia of Speech
AgnosiaVision Deficits
Motion
Depth
Color

Evaluate Existing Medications
• Consider the following issues:
– Drug induced cognitive impairment
• Anticholinergic Load
– Medication induced electrolyte disturbance
– Recent medication additions that may alter
metabolism of a drug that the person has been
taking for a while
– Withdrawal reaction to a recently discontinued
medication
27
What to Ask
Significant social/personality information:
• How do you feel about being in large groups of people?
• Are there any specific things that turn you off about other
people?
• How do you express yourself when you are angry, frustrated or
upset?
• What things do you do to comfort yourself at times when you
feel this way?

What to Ask
• Dislikes with regard to other people
• How do you feel about needing help with your
personal care?
• Things the resident finds stressful
• Resident’s feelings about noise and sharing
living space
• Things the resident finds comforting
• Current life goals and aspirations How do you
feel about needing help with your personal
care? How do you feel about needing help
What to Ask
• Are you sexually active?
• Is there anything about your sexual needs or
preferences that you want to share?
• Do you need education on safe sexual
practices or infection control?
• Do you require private time with a spouse or
significant other?
Preadmission Screening and Resident Review
(PASARR)
• Preadmission Screening and Resident Review (PASARR) is a
federal requirement to help ensure that individuals are not
inappropriately placed in nursing homes for long term care.
PASARR requires that:
• All applicants to a Medicaid-certified nursing facility be evaluated
for mental illness and/or intellectual disability;
• Be offered the most appropriate setting for their needs (in the
community, a nursing facility, or acute care settings); and
• Receive the services they need in those settings.
Preadmission Screening and Resident Review
(PASARR)
• PASARR process requires that all applicants to
Medicaid-certified Nursing Facilities be given a
preliminary assessment to determine whether they
might have MI or MR.
• This is called a "Level I screen." Those individuals who test
positive at Level I are then evaluated in depth, called "Level
II" PASARR.
• The results of this evaluation result in a determination of
need, determination of appropriate setting, and a set of
recommendations for services to inform the individual's plan
of care.
PASARR
F645 Coordination
Incorporating the recommendations from the
PASARR level II determination and the PASARR
evaluation report into a resident’s assessment, care
planning, and transitions of care.
F679 Activities
Recommendations for Behavioral Interventions
For the resident who exhibits behavior that require a less stimulating
environment to discontinue behaviors not welcomed by others sharing their
social space:
• Offering activities in which the resident can succeed, that are broken into
simple steps, that involve small groups or are one-to-one activities such as
using the computer, that are short and repetitive, and that are stopped if the
resident becomes overwhelmed (reducing excessive noise such as from the
television);
• Involving in familiar occupation-related activities. (A resident, if they
desire, can do paid or volunteer work and the type of work would be
included in the resident’s plan of care, such as working outside the facility,
sorting supplies, delivering resident mail, passing juice and snacks.
(§483.10(e)(8) Resident Right to Work);

F679 Activities
Recommendations for Behavioral Interventions
• Involving in physical activities such as walking, exercise or dancing, games
or projects requiring strategy, planning, and concentration, such as model
building, and creative programs such as music, art, dance or physically
resistive activities, such as kneading clay, hammering, scrubbing, sanding,
using a punching bag, using stretch bands, or lifting weights; and
• Slow exercises (e.g., slow tapping, clapping or drumming); rocking or
swinging motions (including a rocking chair).

F679 Activities
Recommendations for Behavioral Interventions
For the resident who goes through others’ belongings:
• Using normalizing life activities such as stacking canned food
onto shelves, folding laundry; offering sorting activities (e.g.,
sorting socks, ties or buttons); involving in organizing tasks
(e.g., putting activity supplies away); providing rummage
areas in plain sight, such as a dresser; and
• Using non-entry cues, such as “Do not disturb” signs or
removable sashes, at the doors of other residents’ rooms;
providing locks to secure other resident’s belongings (if
requested).

F679 Activities
Recommendations for Behavioral Interventions
For the resident who has withdrawn from previous
activity interests/customary routines and isolates self in
room/bed most of the day:
• Providing activities just before or after meal time and
where the meal is being served (out of the room);
• Providing in-room volunteer visits, music or videos
of choice;
F679 Activities
Recommendations for Behavioral Interventions
• Encouraging volunteer-type work that begins in the room and
needs to be completed outside of the room, or a small group
activity in the resident’s room, if the resident agrees; working
on failure-free activities, such as simple structured crafts or
other activity with a friend; having the resident assist another
person;
• Inviting to special events with a trusted peer or family/friend;
• Engaging in activities that give the resident a sense of value
(e.g., intergenerational activities that emphasize the resident's
oral history knowledge);

F679 Activities
Recommendations for Behavioral Interventions
• Inviting resident to participate on facility
committees;
• Inviting the resident outdoors; and
• Involving in gross motor exercises (e.g.,
aerobics, light weight training) to increase
energy and uplift mood.

F679 Activities
Recommendations for Behavioral Interventions
For the resident who has delusional and hallucinatory behavior that is stressful
to her/him:
• Focusing the resident on activities that decrease stress and increase
awareness of actual surroundings, such as familiar activities and physical
activities;
• Offering verbal reassurance, especially in terms of keeping the resident
safe; and
• Acknowledging that the resident’s experience is real to her/him.
The outcome for the resident, the decrease or elimination of the behavior,
either validates the activity intervention or suggests the need for a new
approach.
Activities for a New Age
• Diversify therapeutic activity offerings to include education, self-help,
and support programs;
• Collaborate with community addiction services;
• Promote positive self-esteem through meaningful socialization and
therapeutic activity;
• Collaborate with community vocational services organizations in
discharge planning;
• Foster opportunities for volunteerism.
CREATIVE, ARTISTIC, AND
EXPRESSIVE THERAPIES FOR PTSD
A number of non-traditional
creative/expressive therapies has demonstrated
at least preliminary effectiveness in reducing
PTSD symptoms, reducing the severity of
depression (which often accompanies PTSD),
and/or improving quality of life.
CREATIVE, ARTISTIC, AND
EXPRESSIVE THERAPIES FOR PTSD
•Expressive Writing: is a brief intervention that instructs individuals to write about their
deepest thoughts and feelings about a stressful event without regard to the structure of the
writing
•Dance and Body Movement Therapies: propose that one’s negative, emotion-laden
experiences are represented in the body in the form of tension and pain.
•Art Therapy: involves residents using some medium (e.g., painting, drawing, collage) to
represent their feelings or emotions related to their trauma;
•Music Therapy: engages residents to use music in a variety of ways (e.g., playing music,
beating a drum, listening to and sharing songs) to encourage emotional expression in a non-
threatening environment.

CREATIVE, ARTISTIC, AND
EXPRESSIVE THERAPIES FOR PTSD
• Drama Therapy: creates safe, playful environments where patients are
able to act out anxieties or conflicts due to their trauma
• Nature Therapy: involves a set of related activities that utilize a mix of
relaxation and creative approaches involving nature.
• Mindfulness Therapies: focus primarily on observing one’s internal and
external states and accepting one’s past experiences, so as to better
tolerate the distress associated with trauma reminders
Source: Creative, Artistic, and Expressive Therapies for PTSD
By Joshua Smyth, PhD and Jeremy Nobel, MD, MPH
Benefit of Conversation
University of Exeter:
"One Social Hour a Week in Dementia Care
Improves Lives and Saves Money: Person-
centered activities combined with just one hour a
week of social interaction can improve quality of
life and reduce agitation for people with
dementia living in care homes, while saving
money." ScienceDaily, 16 July 2017

LIFE SKILLS PROGRAMMING:
CHRONIC MENTAL HEALTH
• Life skills programs encourages independent
living and enhances quality of life.
• Life skills often have several components:
– Communication and talking;
– Financial awareness and money management; domestic
tasks (such as cooking, washing‐ up dishes, hoovering,
doing the laundry and running a home); and
– Personal self‐care (such as washing, bathing, cleaning
teeth, shaving, combing hair and getting dressed).
LIFE SKILLS PROGRAMMING:
CHRONIC MENTAL HEALTH
• Other life skills include training on:
– Coping with stress
– Shopping for and eating healthy food,
– Knowing the time,
– Taking medication,
– Improving social skills,
– Using transport; and
– Forward planning

Procedural Memory
• A part of the long-term memory that is responsible
for knowing how to do things, also known as motor
skills.
• Procedural memory stores information on how to
perform certain procedures, such as walking, talking
and riding a bike.
• Delving into something in your procedural memory
does not involve conscious thought.
http://www.livescience.com/43595-procedural-memory.html#sthash.sgerS8rA.dpuf
Cognition and Memory
“The motor component of a task is believed to make it more memorable, as it enriches the encoding experience and often involves the manipulation of concrete objects. There is further evidence that people with dementia are able to maintain or relearn activities of daily living (e.g. setting the table, preparing a meal) with appropriate environmental support and active regular practice.”
Pachana, Nancy, “Memory and Communication Support in Dementia: Research-Based Strategies For Caregivers” Cambridge Univ Press: Jan 1, 2011

The Impact Of Music On
MEMORY AND LANGUAGE
Researchers have found that “musical training has a profound
impact on other skills including speech and language, memory
and attention, and even the ability to convey emotions vocally. S.L.Baker, “Music Benefits the Brain Research Reveals, circa 2010,”
NaturalNews.com, http://www.naturalnews.com/029324_music_brain.html
For people with cognitive and memory deficits, medical research
shows us that music affects the brain in ways that can promote
language and understanding beyond the spoken word. New
research also shows that music has a significant impact on
reducing depression and agitation in people with dementia.Laird Harrison, “Music Therapy May Help Dementia Patients Especially,”
Caring for the Ages, Vol.12, No.7 (July 2011): 1

Music Helps Dementia Patients
Recall Memories and Emotions
A recent study shows that dementia and Alzheimer’s
patients can recall memories and emotions, and
have enhanced mental performance after singing
classic hits and show tunes from movies and
musicals — a breakthrough in understanding how
music affects those with dementia and Alzheimer’s.
Source: https://www.alzheimers.net/why-music-boosts-brain-activity-in-dementia-patients/
Music Helps Dementia Patients
Recall Memories and Emotions
• Researchers determined the effect music has on dementia
patients, by leading half of the participants through selected
songs while the other half listened to the music being played.
• After the musical treatment, all participants took cognitive
ability and life satisfaction tests which showed how
participants scored significantly better when being lead
through songs, rather than only listening.

Singing is Engaging
• The singing sessions in the study engaged more than just the brain and the area related to singing.
• As singing activated the left side of the brain, listening to music sparked activity in the right and watching the class activated visual areas of the brain.
• With so much of the brain being stimulated, the patients were exercising more mind power than usual.
Source: https://www.alzheimers.net/why-music-boosts-brain-activity-in-dementia-patients/
Non-pharmacological Interventions
• Increasing the amount of resident exercise;
• Reducing underlying causes of distressed behavior such as
boredom and pain;
• Improving sleep hygiene;
• Accommodating the resident’s behavior and needs by
supporting and encouraging activities reminiscent of lifelong
work or activity patterns;
• Using massage, hot/warm or cold compresses to address a
resident’s pain or discomfort; and
• Enhancing the dining experience.

Personalized Activity
Example #1• Facts: Middle-aged woman, brain injured, comatose,
vent dependent: known to collect butterflies, loved
the smell of lilacs in the spring, enjoyed music by the
Beatles.
– Activity intervention: butterfly mural painted on the
ceiling tiles over the resident’s bed; aroma of fresh lilacs
used in room; Beatles music on as scheduled (not to be
played continuously and variety is maintained).

Personalized Activity
Example #2
• Facts: 93 y/o man with moderate dementia: He says
that he would go fishing on his boat, that he loves
being on the water and the smell of the sea. He says
he feels free and peaceful when he’s fishing,
especially if he goes out alone. His family fills in the
details of where he fished and about his boat because
these are details he no longer remembers.
Personalized Activity
Example #3
• Facts: 78 y/o alert, oriented woman who was admitted for short term rehab,
but was unable to return home due to lack of ambulation/AD L support: owned
a successful real estate firm until two years ago when she sold the business and
retired; is known to be smart, strong, persuasive and aggressive in getting what
she wants; loves all things cultured – the ballet, the opera, the annual
fundraising gala for Lincoln Center. Says that she loves being in the city, loves
the “pulse” of New York. Expresses frustration over being “pinned down” as
she perceives it. Sees herself as intellectually superior to her peers.

“Sheltered Workshops"
JOURNALING
101 ACTIVITIES
ANYONE CAN DO
1. Listen to music
2. Make homemade lemonade
3. Count trading cards
4. Clip Coupons
5. Sort poker chips
6. Rake leaves
7. Write a poem together
8. Make a fresh fruit salad…
Source: Alzheimer’s Association Web Site – www.alz.org

Combining ADL, Leisure and Therapeutic
Activity
The simplest way to begin improving the manner in which meaningful activity is made available to residents is by redefining what “meaningful” is.
Find ways to turn ADL activity into activity that occurs between leisure and therapeutic groups. Consider all the disciplines that could contribute real and valuable programming to the day. There may be more resources than you think.
There are hundreds of tasks that make up a person’s daily routine. Evaluate what already happens in your environment with regard to common sense ADL and leisure tasks.

Care Plan LibraryPerson-Centered Care Plan
Mild Cognitive Impairment
Resident is uncomfortable in group
discussion due to mild memory
impairment; he will often leave the
activity for this reason
Resident will attend and participate in
small group discussion group
successfully with cues and assistance
x 90 days
o Meet with resident to discuss memory loss and
feelings of embarrassment
o Provide reassurance that successful participation
is possible with support
o Orient to activity groups that would be
appropriately modified for the resident’s level of
ability
o Provide cues to support successful participation
during programs
o Offer support and praise for participation
Resident has difficulty locating his room
and is embarrassed to ask for directions;
he sometimes becomes agitated when he
feels this way
Resident will be able to locate his
room independently x 90 days
o Meet with resident to discuss memory loss and
feelings of embarrassment
o Discuss identifiers that the resident feels he
would recognize
o Use familiar objects, photographs, word cues and
audible reminders to help resident locate his
room
o Meet with resident to discuss success and to
modify the identifiers as needed to accommodate
memory loss
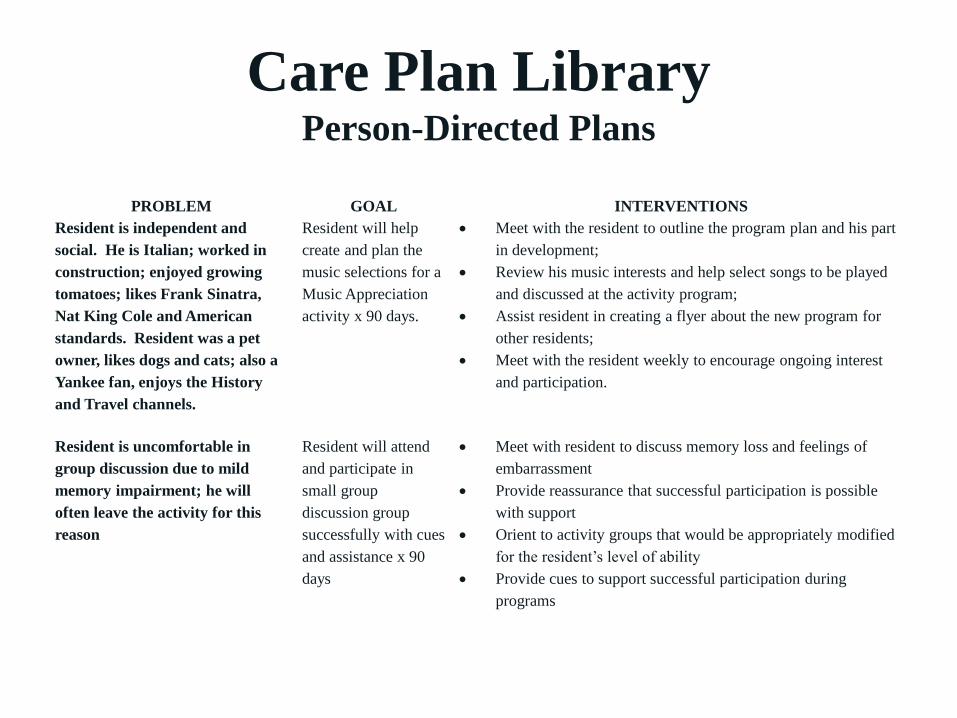
Care Plan LibraryPerson-Directed Plans
PROBLEM GOAL INTERVENTIONS
Resident is independent and
social. He is Italian; worked in
construction; enjoyed growing
tomatoes; likes Frank Sinatra,
Nat King Cole and American
standards. Resident was a pet
owner, likes dogs and cats; also a
Yankee fan, enjoys the History
and Travel channels.
Resident will help
create and plan the
music selections for a
Music Appreciation
activity x 90 days.
• Meet with the resident to outline the program plan and his part
in development;
• Review his music interests and help select songs to be played
and discussed at the activity program;
• Assist resident in creating a flyer about the new program for
other residents;
• Meet with the resident weekly to encourage ongoing interest
and participation.
Resident is uncomfortable in
group discussion due to mild
memory impairment; he will
often leave the activity for this
reason
Resident will attend
and participate in
small group
discussion group
successfully with cues
and assistance x 90
days
• Meet with resident to discuss memory loss and feelings of
embarrassment
• Provide reassurance that successful participation is possible
with support
• Orient to activity groups that would be appropriately modified
for the resident’s level of ability
• Provide cues to support successful participation during
programs
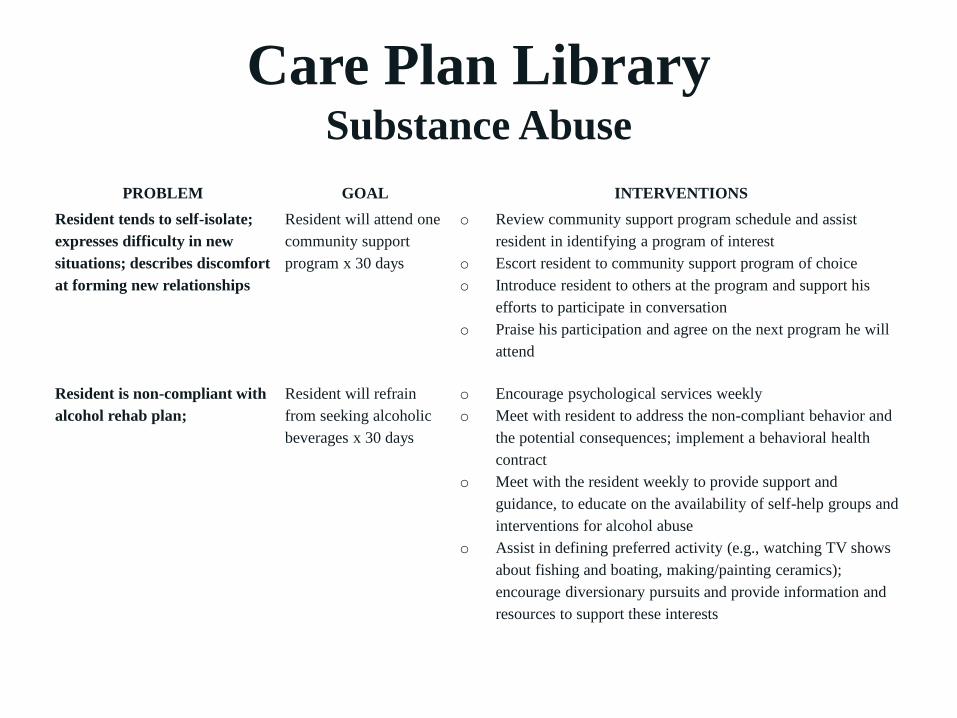
Care Plan LibrarySubstance Abuse
PROBLEM GOAL INTERVENTIONS
Resident tends to self-isolate;
expresses difficulty in new
situations; describes discomfort
at forming new relationships
Resident will attend one
community support
program x 30 days
o Review community support program schedule and assist
resident in identifying a program of interest
o Escort resident to community support program of choice
o Introduce resident to others at the program and support his
efforts to participate in conversation
o Praise his participation and agree on the next program he will
attend
Resident is non-compliant with
alcohol rehab plan;
Resident will refrain
from seeking alcoholic
beverages x 30 days
o Encourage psychological services weekly
o Meet with resident to address the non-compliant behavior and
the potential consequences; implement a behavioral health
contract
o Meet with the resident weekly to provide support and
guidance, to educate on the availability of self-help groups and
interventions for alcohol abuse
o Assist in defining preferred activity (e.g., watching TV shows
about fishing and boating, making/painting ceramics);
encourage diversionary pursuits and provide information and
resources to support these interests

Care Plan Evaluations
Evaluation is required:
✓Following an accident or incident, whether or not
it results in injury;
✓Following a significant change in function or
treatment;
✓Following determination of a new or revised
diagnosis;
✓Upon transfer/discharge; and
✓Upon readmission.

Barbara SpeedlingQuality of Life Specialist
917.754.6282
www.barbaraspeedling.com
Creating Meaningful, Satisfying Lives One Person at a Time