disclosures / conflicts of interest alfred k. cheung, m.d. none relevant to this topic
TRANSCRIPT
Disclosures / Conflicts of Interest
Alfred K. Cheung, M.D.
None relevant to this topic


Lipid Control Is it really needed in the ESRD
patient?
ESRD: STATE OF THE ART AND CHARTING THE CHALLENGES FOR THE FUTURE
April 23-26, 2009
Alfred K. Cheung, M.D.

Lipid Control Is it really needed in the ESRD
patient?
I don’t know

Unconventional Relationship with Clinical Outcomes in HD
Patients
• Blood pressure
• Hemoglobin
• Blood glucose
Is Dialysis World round or flat?

Serum Cholesterol and CHD Death Rate in MRFIT (N=361,662)
Martin, Lancet 1986

Can LDL-C be too low?(Atorvastatin 80 mg in PROVE-IT with achieved LDL <100 mg/dl)
Wiviott , 2005Wiviott , 2005
Target 70-100
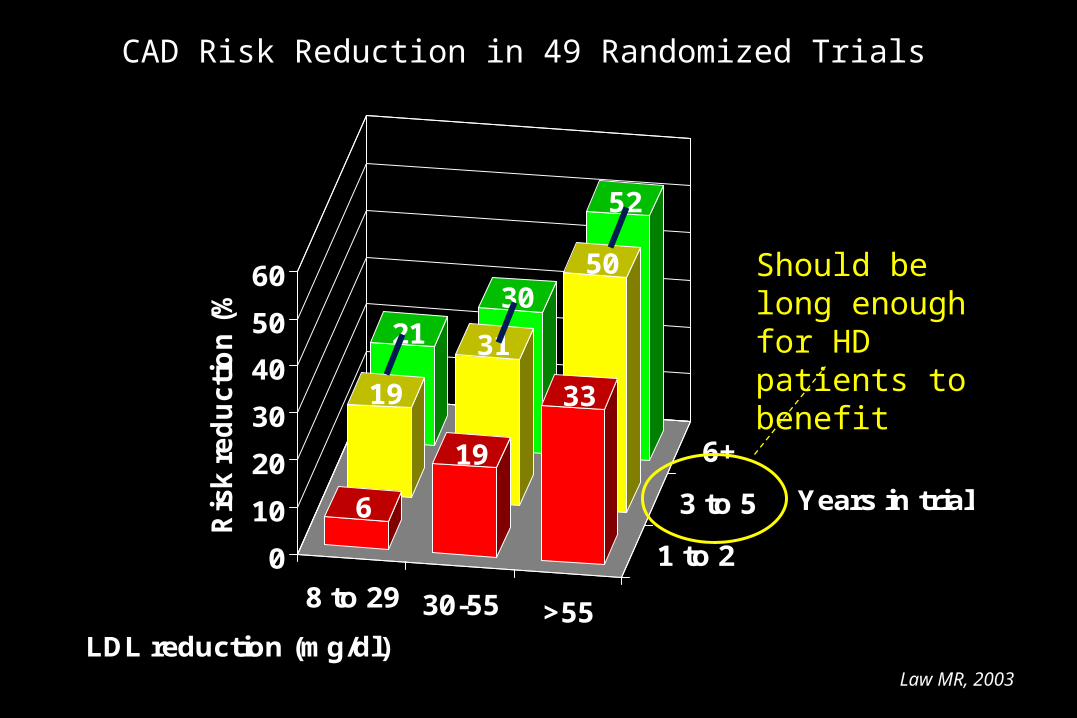
CAD Risk Reduction in 49 Randomized Trials
8 to 29 30-55 >55
1 to 2
3 to 5
6+
2130
52
19
31
50
6
19
33
0
10
20
30
40
50
60
Ris
k r
ed
ucti
on
(%
)
LDL reduction (mg/dl)
Years in trial
Law MR, 2003Law MR, 2003
Should be long enough for HD patients to benefit

0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
LT 100 100-150 150-200 200-250 250-300 300-350 GE 350
Re
lativ
e D
ea
th R
isk
Total Cholesterol (mg/dL)
N = 13,535
Lowrie, 2002
Hemodialysis Patients

Liu, CHOICE, 2004
Inflammation / Malnutrition
n = 206 213 130 85 43 65 52 29
Total cholesterol

Total Mortality
0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Simvastatin Better
Simvastatin Worse
eGFR < 75
eGFR ≥ 75
eGFR < 75
eGFR ≥ 75
Major coronary events
eGFR < 75
eGFR ≥ 75
CHD death or nonfatal MI
CABG or PTCA eGFR < 75 eGFR ≥ 75
eGFR < 75 eGFR ≥ 75
Stroke
Effect in Simvastatin on Total Mortality in Mild CKD
Chonchol AJKD, 2007
● 4S post-hoc analysis4S post-hoc analysis
● 4444 patients with CHD4444 patients with CHD
● 2314 (52%) CKD2314 (52%) CKD

Prospective, randomized double-blind study with type II DM
Atorvastatin 20 mg QDAtorvastatin 20 mg QD
PlaceboPlacebo
12551255patientspatientsPlaceboPlacebo
Die Deutsche Diabetes Dialyse Studie4D Study: Effects of Statins on HD Patients
Wanner, NEJM. 2005;
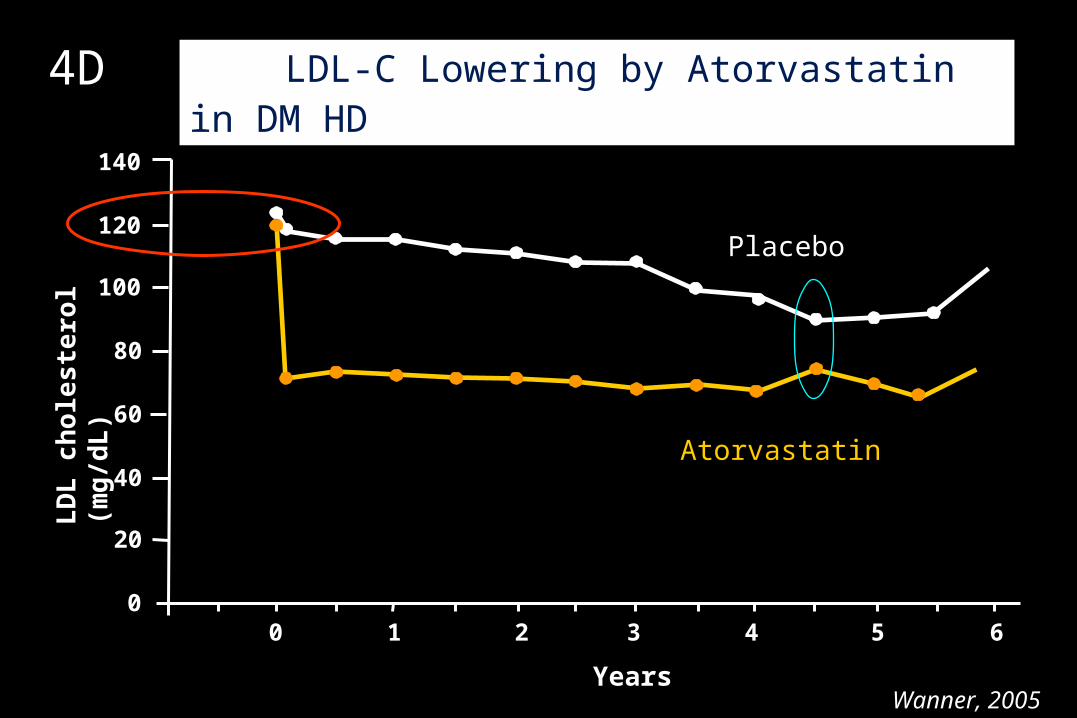
LDL-C Lowering by Atorvastatin in DM HD
Placebo
0
20
40
60
80
100
120
140
Atorvastatin
40 1 2 3 5 6
Years
LD
L c
ho
les
tero
l (m
g/d
L)
Wanner, 2005
4D

Primary composite end point(Cardiac death / MI / stroke)
RR reduction = 8% (0.77-1.10)
Cu
mu
lati
ve i
nci
den
ce (
%)
0
10
20
30
40
50
60
1 2 3 4 50 5.5 years
Placebo
Atorvastatin
Years from Randomization
Wanner, 2005
2X fatal stroke (13 vs. 27 events, p=0.04) 32% in cardiac events
4D

A study to evaluate the Use of Rosuvastatin in subjects on Regular hemodialysis: an
Assessment of survival and CV events (AURORA)
• 280 centers in 25 countries
• 2,776 HD patients (age 50-80 yrs)
~40% history of CVD
~25% DM (vs. 4D)
• Rosuvastatin (10 mg vs. placebo)
• ACM and CV events
Fellstrom, 2009
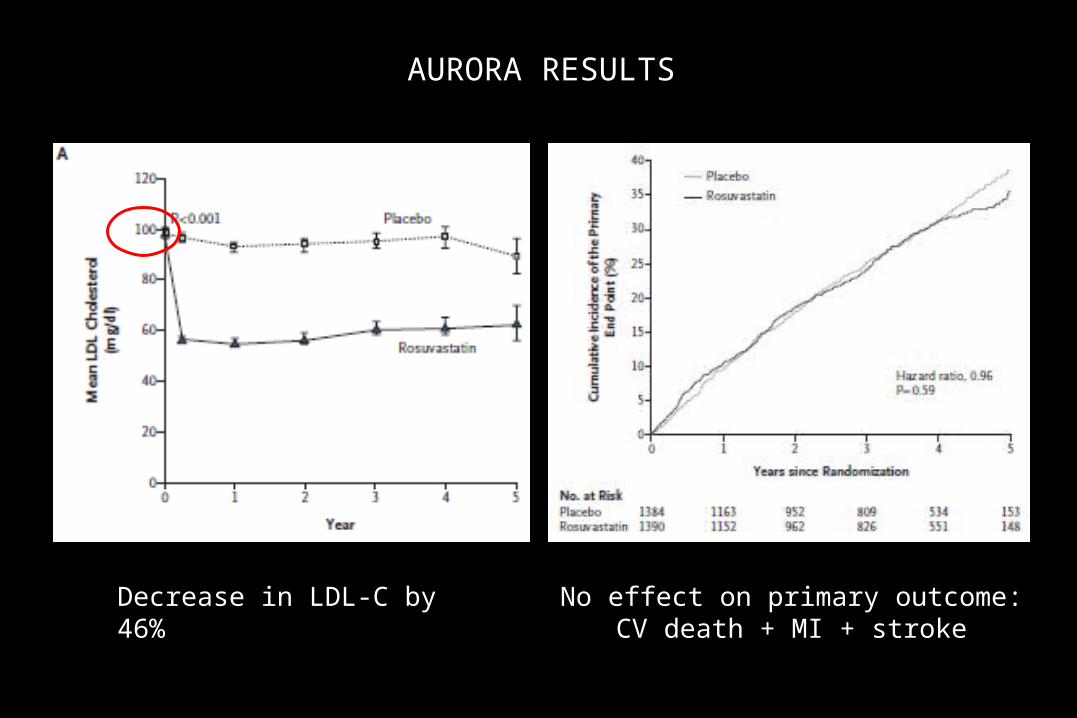
AURORA RESULTS
Decrease in LDL-C by 46% No effect on primary outcome:CV death + MI + stroke
Study of Heart and Renal Protection
• ~9,000 patients (~6000 CKD + ~3000 HD/PD)
• No lipid criteria (statin not obviously indicated)
• 19% DM (vs. 100% in 4D)
• No prior MI or coronary revascularization
• Simvastatin (20 mg) + ezetimibe (10 mg)
• Results?
• It is very difficult to prophesize, especially about the future
Why is lowering LDL-cholesterol
ineffective in improving clinical
outcomes
in dialysis patients?

It is too late to treat !!

Hypothesis:
Atherosclerosis is not a major problem in dialysis
patients
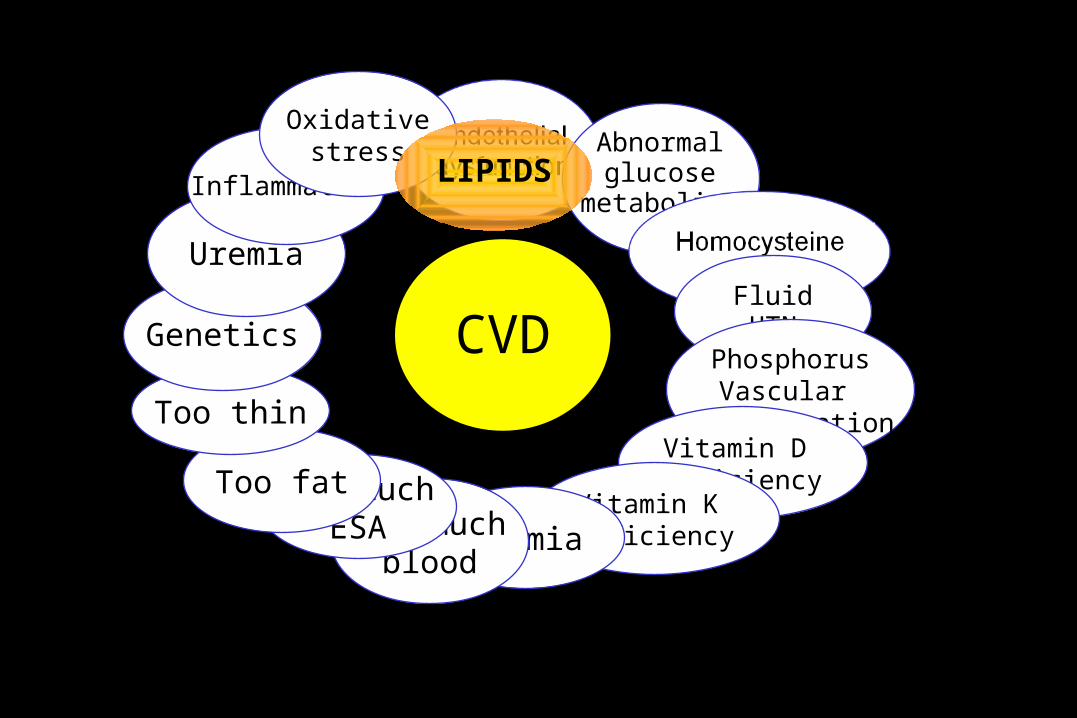
Abnormalglucose
metabolism
CVDFluidHTN
PhosphorusVascular
calcificationVitamin D deficiency
Vitamin K deficiencyAnemiaToo much
blood
Too muchESA
Too fat
Too thin
Genetics
Uremia
Inflammation
Oxidativestress
LIPIDS

VLDLr
Lecitin cholesterol acyl-transferase
Cholesterol ester transfer protein
torcetrapib

Dyslipidemia in Dialysis Patients
• Hypertriglyceridemia – in lipoprotein remnants– Total TG ~265 mg/dL in 4D; ~155 mg/dL in AURORA
• Low HDL and impaired anti-oxidant activity of HDL
• Abnormal LDL– modified (oxidized, glycated, carbamylated)
Not responsive to statins

Triglycerides and HDL-C are Independent CAD Risk Factors
<30 30-39 40-49 50+
<200
200-299
300+
17.2
4.36.7 7.9
6.1
3.1 3.7
1.1
5.7
2.21.3
1.00
5
10
15
20
Od
ds
Rat
io
HDL Cholesterol (mg/dL)
Triglycerides (mg/dL)
Hopkins , JACC, 2005Hopkins , JACC, 2005

0
2
4
6
8
10
12
14
16
TG <200 TG 200+ TG <200 TG 200+
HDL-C 40+ mg/dl HDL-C <40 mg/dl
New
car
dia
c ev
ents
(p
er 1
000
per
son
-yea
rs)
Placebo
Gemfibrozil
Manninen, Circulation, 1992.
Fasting TG, HDL and Risk for CHDThe Helsinki Heart Study
nsnsnsns nsns
67% reduction67% reduction

LDL-cholesterol

Tentative Practice Guidelines for Dyslipidemia in HD Patients
• Would not discontinue statins; consider initiating statin for LDL-C >130 mg/dL (reduce lovastatin dose by 50%)
• For total TG >500 mg/dL– -3 FA 3-4 gm QD – gemfibrozil 600 mg QD (beware of fenofibrate)
• Niacin is a reasonable alternative– decrease TG– increase HDL-C– decrease small dense LDL
Conclusions in ESRD Patients
• Serum total and LDL-cholesterol levels are not usually high
• Despite lowering of LDL-cholesterol levels, there is no convincing evidence for benefits or harm associated with statin use
• There are other dyslipidemia that may be more atherogenic in uremia (e.g., hypertriglyceridemia associated with retention of lipoprotein remnants; low HDL levels and activities as result of uremic modifications)
• Future clinical research should concentrate on these other dyslipidemic states

Lipid Control Is it really needed in the ESRD
patient?
CANNOT SAY “YES” IN 2009NOT total cholesterol or LDL-cholesterol


ADA/ACC 2008 Consensus Statement:Treatment Goals in Patients With
Cardiometabolic Risk
Brunzell JD, et al. JACC 2008; 51:1512.
GoalsGoals
LDL-C LDL-C NonNon––HDLHDL-C-C Apo BApo B
Highest-Risk PatientsHighest-Risk Patients♥ Known CVDKnown CVD
♥ Diabetes plus Diabetes plus ≥1 additional major ≥1 additional major CVD risk factorCVD risk factor
<70 mg/dL<70 mg/dL <100 mg/dL<100 mg/dL <80 mg/dL<80 mg/dL
High-Risk PatientsHigh-Risk Patients♥ ≥≥2 major CVD risk factors, no 2 major CVD risk factors, no
diabetes or known CVD but diabetes or known CVD but
♥ Diabetes but no other major CVD Diabetes but no other major CVD risk factorsrisk factors
<100 mg/dL<100 mg/dL <130 mg/dL<130 mg/dL <90 mg/dL<90 mg/dL
“In individuals on statin therapy who continue to have low HDL-C or elevated non–HDL-C, especially if Apo B levels remain elevated, combination therapy is recommended. The preferred agent to use in combination with a statin is nicotinic acid…”

ADA and ACC Consensus StatementTreatment Recomendations
• A statin is the initial drug of choice.• If LDL goal not reached consider adding:
– ezetimibe– bile acid sequestrants (can raise TG)– niacin
• Low HDL-C or elevated non-HDL-C, especially if apoB remains elevated:– combination therapy is recommended– niacin first choice
Brunzell JD, et al. JACC 2008; 51:1512.

ADA and ACC Consensus StatementTreatment Recomendations
• Fibrates have been shown to reduce CVD events in some studies but not total mortality
• N-3 fatty acid therapy– CVD outcome data are lacking for hypertriglyceridemic patients
– Clear reduction in CV risk in other studies
• Severe hypertriglyceridemia : – fat restriction– fibrate– niacin– high-dose n-3 FA (4 g / day)
Brunzell JD, et al. JACC 2008; 51:1512.
ADA and ACC Consensus StatementTreatment Recommendations:
Niacin
• Niacin decreased CVD in the Coronary Drug Project and total mortality in an extended follow up
• Niacin in combination with bile-acid sequestrants or statin was associated with regression of atherosclerosis and CVD events in several studies– FATS, HATS, ARBITER 2, CLAS
• In diabetes the use of low dose niacin (1500 mg/day) does not significantly increase A1C levels
Brunzell JD, et al. JACC 2008; 51:1512.
Potential Mechanism of Statin Benefit in Kidney Disease
• Inhibit mesangial proliferation• Inhibit induction of TGF- and increase in extracellular matrix
• Inhibition of induction of MCP-1• Decrease in inflammation and oxidative stress• Ameliorate podocyte damage• Hemodynamic effects on endothelial function and vasodilation
• Ameliorate renal vascular disease
Fried L, et al. Kidney Int. 2008;74:571-576.

Statins for Improving Renal Outcomes: Meta-analysis
39,704 participants (27 studies) 21 studies with data for eGFR and 20 for albuminuria or proteinuria
Change in mean differences for eGFR was significant: 1.22 ml/min per yr slower in statin recipients
Subgroup analysis: benefit of statin was significant in studies of participants with CVD but not in populations with diabetic or hypertensive kidney disease or glomerulonephritis
Reduction in albuminuria or proteinuria as a result of statin therapy was also significant: 0.58 Units of SD greater decrease in statin recipients
Sandhu S, et al. JASN. 2006;17:2006-2016.
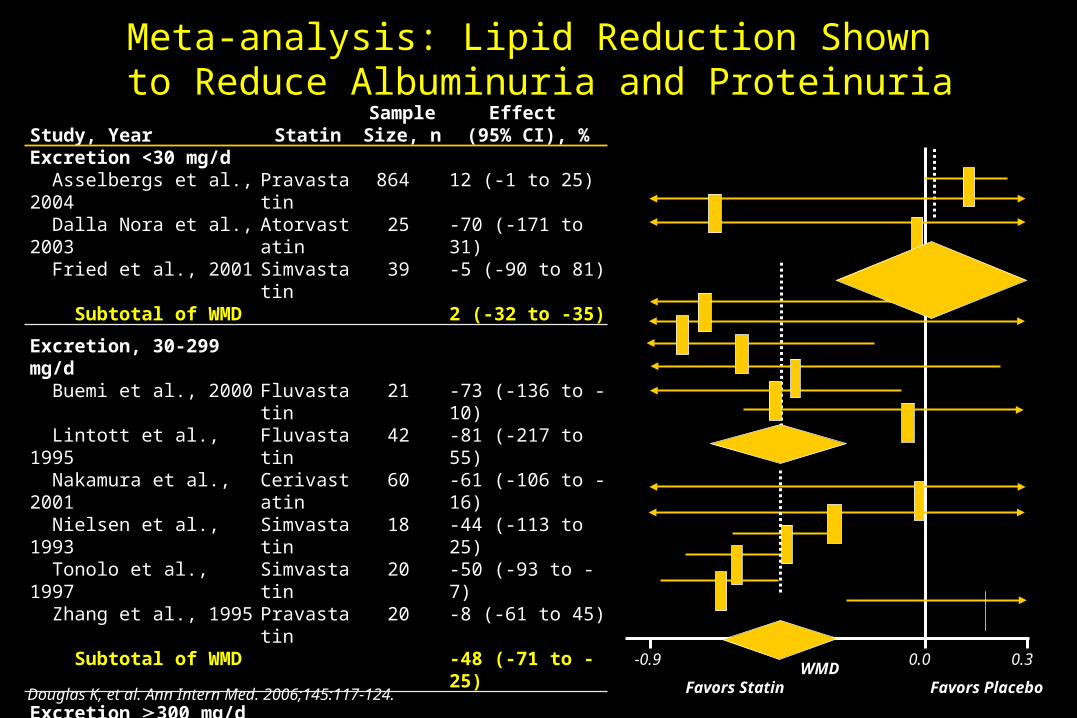
Douglas K, et al. Ann Intern Med. 2006;145:117-124.
Meta-analysis: Lipid Reduction Shown to Reduce Albuminuria and Proteinuria
Study, YearStudy, Year StatinStatinSample Sample Size, nSize, n
Effect Effect (95% CI), %(95% CI), %
Excretion <30 mg/dExcretion <30 mg/d Asselbergs et al., 2004 Asselbergs et al., 2004 PravastatinPravastatin 864864 12 (-1 to 25)12 (-1 to 25) Dalla Nora et al., 2003 Dalla Nora et al., 2003 AtorvastatinAtorvastatin 2525 -70 (-171 to 31)-70 (-171 to 31) Fried et al., 2001 Fried et al., 2001 SimvastatinSimvastatin 3939 -5 (-90 to 81)-5 (-90 to 81) Subtotal of WMDSubtotal of WMD 2 (-32 to -35)2 (-32 to -35)
Excretion, 30-299 mg/dExcretion, 30-299 mg/d Buemi et al., 2000 Buemi et al., 2000 FluvastatinFluvastatin 2121 -73 (-136 to -10)-73 (-136 to -10) Lintott et al., 1995 Lintott et al., 1995 FluvastatinFluvastatin 4242 -81 (-217 to 55)-81 (-217 to 55) Nakamura et al., 2001 Nakamura et al., 2001 CerivastatinCerivastatin 6060 -61 (-106 to -16)-61 (-106 to -16) Nielsen et al., 1993 Nielsen et al., 1993 SimvastatinSimvastatin 1818 -44 (-113 to 25)-44 (-113 to 25) Tonolo et al., 1997 Tonolo et al., 1997 SimvastatinSimvastatin 2020 -50 (-93 to -7)-50 (-93 to -7) Zhang et al., 1995 Zhang et al., 1995 PravastatinPravastatin 2020 -8 (-61 to 45)-8 (-61 to 45) Subtotal of WMDSubtotal of WMD -48 (-71 to -25)-48 (-71 to -25)
Excretion Excretion 300 mg/d300 mg/d Hommei et al., 1992 Hommei et al., 1992 SimvastatinSimvastatin 2121 -5 (-137 to 128)-5 (-137 to 128) Lam et al., 1995 Lam et al., 1995 LovastatinLovastatin 3636 -32 (-102 to 38)-32 (-102 to 38) Lee et al., 2002 Lee et al., 2002 PravastatinPravastatin 6666 -47 (-64 to -29)-47 (-64 to -29) Lee et al., 2005Lee et al., 2005 PravastatinPravastatin 8282 -62 (-79 to -45)-62 (-79 to -45) Nakamura et al., 2002 Nakamura et al., 2002 CerivastatinCerivastatin 4040 -67 (-87 to -48)-67 (-87 to -48) Thomas et al., 1993 Thomas et al., 1993 SimvastatinSimvastatin 3030 20 (-28 to 67)20 (-28 to 67) Subtotal of WMDSubtotal of WMD -47 (-67 to -26)-47 (-67 to -26)
0.30.0-0.9WMD
Favors Statin Favors Placebo

Rubins HB, et al. N Engl J Med. 1999;341:410-418.Rubins HB, et al. N Engl J Med. 1999;341:410-418.
0
5
10
15
20
25
0 1 2 3 4 5 6
Cum
ulat
ive
Inci
denc
e, %
Year
Placebo
Gemfibrozil
VA-HIT: Cumulative Incidence of CHD Death and Nonfatal MI

Statins decreases CV events in Patients with normal LDL-C
• JUPITER• Comparative Atorvastatin Pleiotropic Effects
• However, no effect in HD patients (11% decrease in CRP in AURORA, not ine 4D)
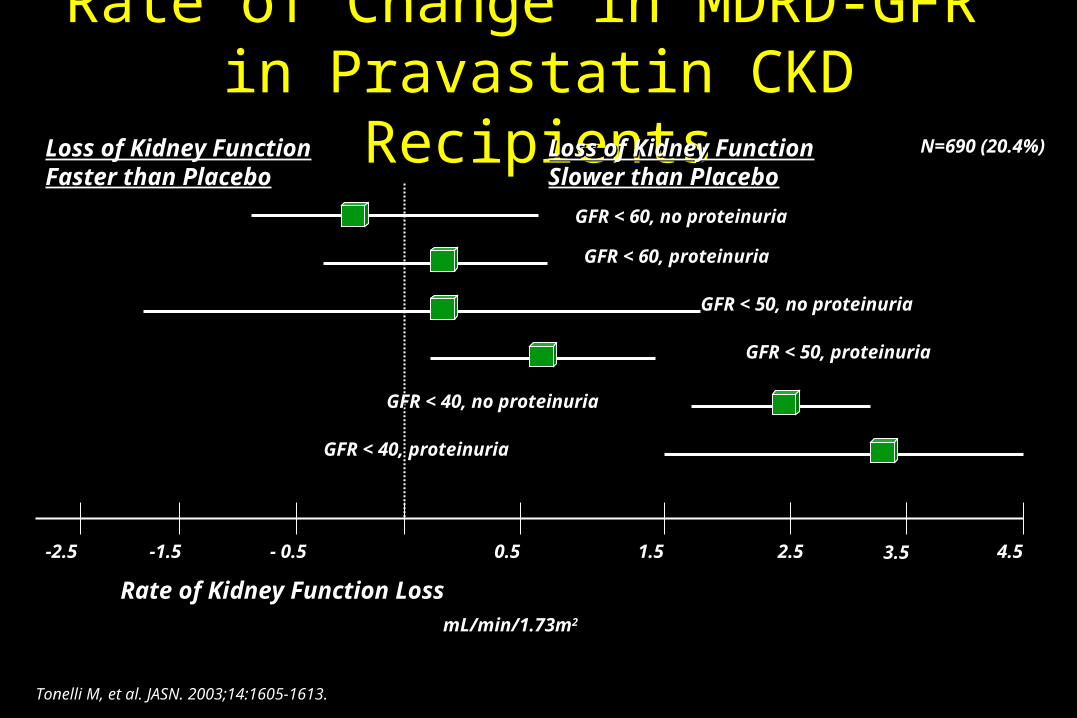
Rate of Change in MDRD-GFR
in Pravastatin CKD Recipients
2.51.50.5- 0.5-1.5
Rate of Kidney Function LossRate of Kidney Function Loss
GFR < 60, no proteinuriaGFR < 60, no proteinuria
Loss of Kidney Function Loss of Kidney Function Faster than PlaceboFaster than Placebo
Loss of Kidney Function Loss of Kidney Function Slower than PlaceboSlower than Placebo
GFR < 60, proteinuriaGFR < 60, proteinuria
GFR < 50, no proteinuriaGFR < 50, no proteinuria
GFR < 50, proteinuriaGFR < 50, proteinuria
GFR < 40, no proteinuriaGFR < 40, no proteinuria
Tonelli M, et al. JASN. 2003;14:1605-1613.
4.5-2.5
GFR < 40, proteinuriaGFR < 40, proteinuria
3.5
N=690 (20.4%)
mL/min/1.73m2

Effect of Atorvastatin on Inflammation in Patients with Type 2 Diabetes Mellitus on Hemodialysis
Krane V, et al. Kidney Int 2008.
p=0.001 p=0.71
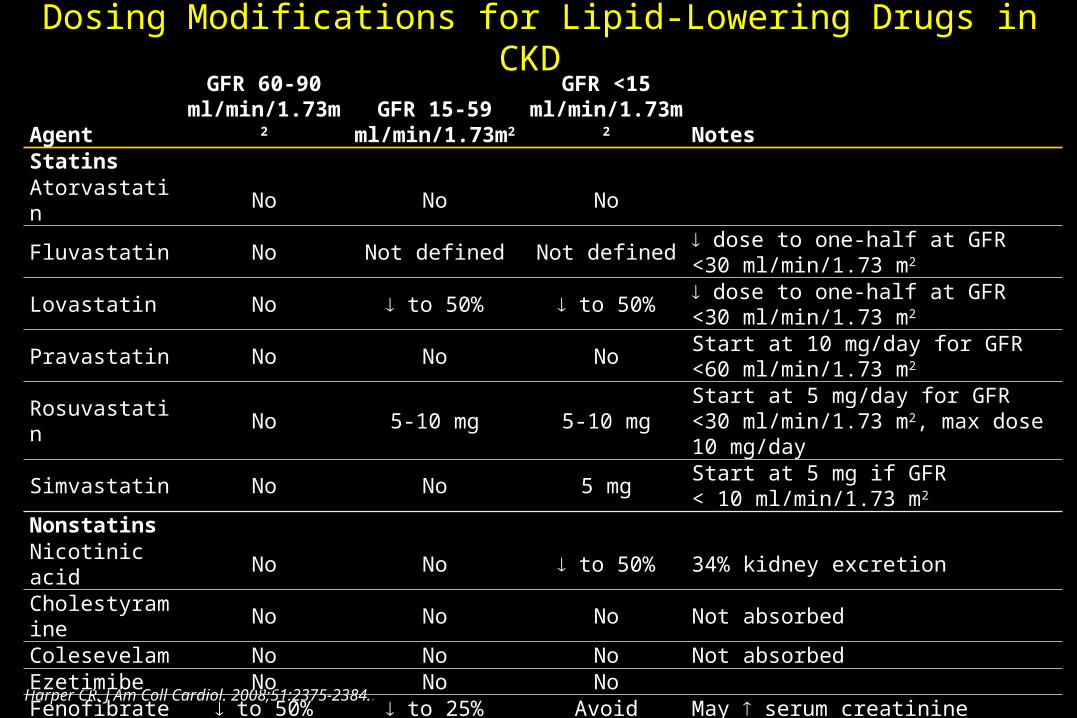
Dosing Modifications for Lipid-Lowering Drugs in CKD
Harper CR. J Am Coll Cardiol. 2008;51:2375-2384..
AgentAgentGFR 60-90GFR 60-90
ml/min/1.73mml/min/1.73m22
GFR 15-59 GFR 15-59 ml/min/1.73mml/min/1.73m22
GFR <15GFR <15ml/min/1.73mml/min/1.73m22 NotesNotes
StatinsStatinsAtorvastatinAtorvastatin NoNo NoNo NoNo
FluvastatinFluvastatin NoNo Not definedNot defined Not definedNot defined dose to one-half at GFR dose to one-half at GFR <30 ml/min/1.73 m<30 ml/min/1.73 m22
LovastatinLovastatin NoNo to 50%to 50% to 50%to 50% dose to one-half at GFR dose to one-half at GFR <30 ml/min/1.73 m<30 ml/min/1.73 m22
PravastatinPravastatin NoNo NoNo NoNo Start at 10 mg/day for GFR <60 ml/min/1.73 mStart at 10 mg/day for GFR <60 ml/min/1.73 m22
RosuvastatinRosuvastatin NoNo 5-10 mg5-10 mg 5-10 mg5-10 mg Start at 5 mg/day for GFR Start at 5 mg/day for GFR <30 ml/min/1.73 m<30 ml/min/1.73 m22, max dose 10 mg/day, max dose 10 mg/day
SimvastatinSimvastatin NoNo NoNo 5 mg5 mg Start at 5 mg if GFR Start at 5 mg if GFR < 10 ml/min/1.73 m< 10 ml/min/1.73 m22
NonstatinsNonstatinsNicotinic acidNicotinic acid NoNo NoNo to 50%to 50% 34% kidney excretion34% kidney excretionCholestyramineCholestyramine NoNo NoNo NoNo Not absorbedNot absorbedColesevelamColesevelam NoNo NoNo NoNo Not absorbedNot absorbedEzetimibeEzetimibe NoNo NoNo NoNoFenofibrateFenofibrate to 50%to 50% to 25%to 25% AvoidAvoid May May serum creatinine serum creatinine
GemfibrozilGemfibrozil NoNo NoNo NoNo NLA recommends a dose of 600 mg/day for NLA recommends a dose of 600 mg/day for GFR 15-59 ml/min/1.73mGFR 15-59 ml/min/1.73m22
Omega-3 FAsOmega-3 FAs NoNo NoNo NoNo

How Should We Treat Them?
Harper CR. J Am Coll Cardiol. 2008;51:2375-2384.
Lipid DisorderLipid Disorder Therapeutic OptionTherapeutic OptionModerate to severe CKD, stages 3 to 4 (GFR 15-59 ml/min/1.73 mModerate to severe CKD, stages 3 to 4 (GFR 15-59 ml/min/1.73 m22))
Elevated LDL-CElevated LDL-C1.1. Atorvastatin, add ezetimibe if not at LDL-C goalAtorvastatin, add ezetimibe if not at LDL-C goal2.2. Fluvastatin, add ezetimibe if not at LDL-C goalFluvastatin, add ezetimibe if not at LDL-C goal
Mixed dyslipidemia Mixed dyslipidemia (not at non-HDL goal)(not at non-HDL goal)
1.1. Atorvastatin ofrfluvastatin + ezetimibeAtorvastatin ofrfluvastatin + ezetimibe2.2. Fluvastatin + gemfibrozil 600 mg/day + ezetimibe if not at non Fluvastatin + gemfibrozil 600 mg/day + ezetimibe if not at non
HDL goalHDL goal3.3. Statin + omega 3 fatty acids, add ezetimibe if not at non-HDL goalStatin + omega 3 fatty acids, add ezetimibe if not at non-HDL goal4.4. Statin + fenofibrate 48 mg/day, add ezetimibe if not at non-HDL goalStatin + fenofibrate 48 mg/day, add ezetimibe if not at non-HDL goal
Very high triglycerides (triglyceride Very high triglycerides (triglyceride 500 500 mg/dl)mg/dl)
1.1. Gemfibrozil 600 mg/dayGemfibrozil 600 mg/day2.2. Omega-3 fatty acids 3-4 g/dayOmega-3 fatty acids 3-4 g/day3. Fenofibrate 48 mg/day3. Fenofibrate 48 mg/day
CKD stage 5 (hemodialysis or GFR <15 ml/min/1.73 mCKD stage 5 (hemodialysis or GFR <15 ml/min/1.73 m22))
Elevated LDL-CElevated LDL-CAtorvastatin (10-80 mg/day) or fluvastatin 40 mg/day, add ezetimibe if not at LDL-C Atorvastatin (10-80 mg/day) or fluvastatin 40 mg/day, add ezetimibe if not at LDL-C goalgoal
Mixed dyslipidemiaMixed dyslipidemiaAtorvastatin or fluvastatin 40 mg/day, add ezetimibe 10 mg/day or Atorvastatin or fluvastatin 40 mg/day, add ezetimibe 10 mg/day or omega-3 fatty acids 3-4 g/day if not at non-HDL goalomega-3 fatty acids 3-4 g/day if not at non-HDL goal
Very high triglyceridesVery high triglycerides Omega-3 fatty acids 3-4 g/day or gemfibrozil 600 mg/dayOmega-3 fatty acids 3-4 g/day or gemfibrozil 600 mg/day
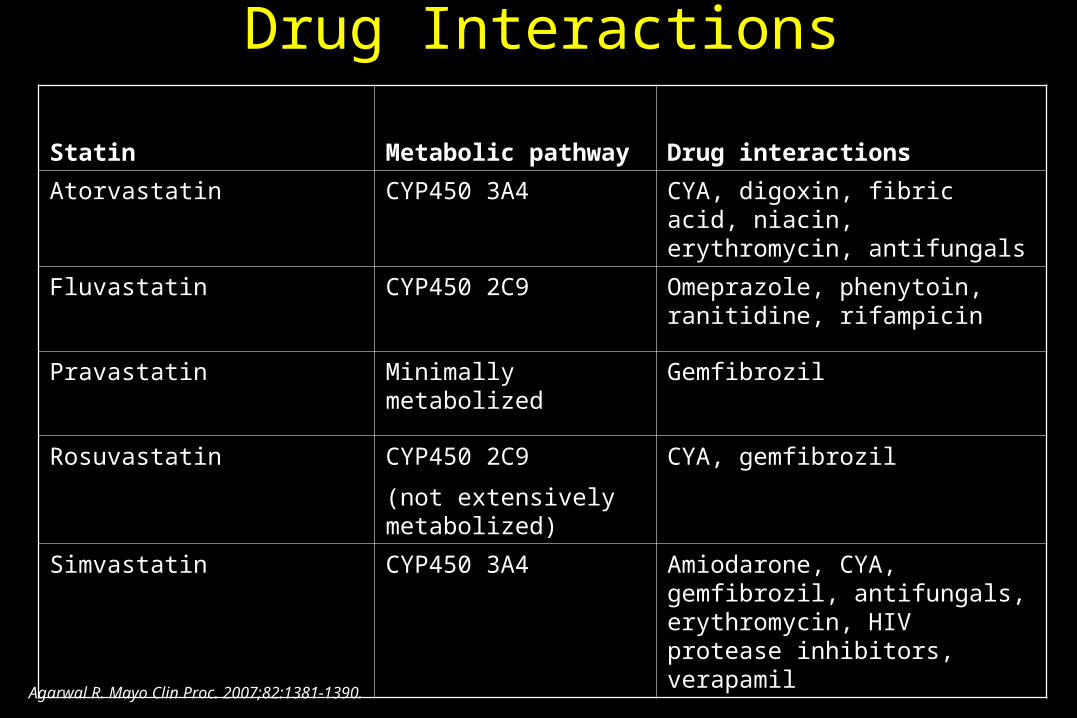
Drug Interactions
StatinStatin Metabolic pathwayMetabolic pathway Drug interactionsDrug interactions
AtorvastatinAtorvastatin CYP450 3A4CYP450 3A4 CYA, digoxin, fibric acid, niacin, CYA, digoxin, fibric acid, niacin, erythromycin, antifungalserythromycin, antifungals
FluvastatinFluvastatin CYP450 2C9CYP450 2C9 Omeprazole, phenytoin, ranitidine, Omeprazole, phenytoin, ranitidine, rifampicinrifampicin
PravastatinPravastatin Minimally metabolizedMinimally metabolized GemfibrozilGemfibrozil
RosuvastatinRosuvastatin CYP450 2C9CYP450 2C9
(not extensively (not extensively metabolized)metabolized)
CYA, gemfibrozilCYA, gemfibrozil
SimvastatinSimvastatin CYP450 3A4CYP450 3A4 Amiodarone, CYA, gemfibrozil, Amiodarone, CYA, gemfibrozil, antifungals, erythromycin, HIV antifungals, erythromycin, HIV protease inhibitors, verapamilprotease inhibitors, verapamil
Agarwal R. Mayo Clin Proc. 2007;82:1381-1390.

How Should We Treat Them?
Harper CR. J Am Coll Cardiol. 2008;51:2375-2384.
Lipid DisorderLipid Disorder Therapeutic OptionTherapeutic OptionModerate to severe CKD, stages 3 to 4 (GFR 15-59 ml/min/1.73 mModerate to severe CKD, stages 3 to 4 (GFR 15-59 ml/min/1.73 m22))
Elevated LDL-CElevated LDL-C1.1. Atorvastatin, add ezetimibe if not at LDL-C goalAtorvastatin, add ezetimibe if not at LDL-C goal2.2. Fluvastatin, add ezetimibe if not at LDL-C goalFluvastatin, add ezetimibe if not at LDL-C goal
Mixed dyslipidemia Mixed dyslipidemia (not at non-HDL goal)(not at non-HDL goal)
1.1. Atorvastatin ofrfluvastatin + ezetimibeAtorvastatin ofrfluvastatin + ezetimibe2.2. Fluvastatin + gemfibrozil 600 mg/day + ezetimibe if not at non Fluvastatin + gemfibrozil 600 mg/day + ezetimibe if not at non
HDL goalHDL goal3.3. Statin + omega 3 fatty acids, add ezetimibe if not at non-HDL goalStatin + omega 3 fatty acids, add ezetimibe if not at non-HDL goal4.4. Statin + fenofibrate 48 mg/day, add ezetimibe if not at non-HDL goalStatin + fenofibrate 48 mg/day, add ezetimibe if not at non-HDL goal
Very high triglycerides (triglyceride Very high triglycerides (triglyceride 500 500 mg/dl)mg/dl)
1.1. Gemfibrozil 600 mg/dayGemfibrozil 600 mg/day2.2. Omega-3 fatty acids 3-4 g/dayOmega-3 fatty acids 3-4 g/day3. Fenofibrate 48 mg/day3. Fenofibrate 48 mg/day
CKD stage 5 (hemodialysis or GFR <15 ml/min/1.73 mCKD stage 5 (hemodialysis or GFR <15 ml/min/1.73 m22))
Elevated LDL-CElevated LDL-CAtorvastatin (10-80 mg/day) or fluvastatin 40 mg/day, add ezetimibe if not at LDL-C Atorvastatin (10-80 mg/day) or fluvastatin 40 mg/day, add ezetimibe if not at LDL-C goalgoal
Mixed dyslipidemiaMixed dyslipidemiaAtorvastatin or fluvastatin 40 mg/day, add ezetimibe 10 mg/day or Atorvastatin or fluvastatin 40 mg/day, add ezetimibe 10 mg/day or omega-3 fatty acids 3-4 g/day if not at non-HDL goalomega-3 fatty acids 3-4 g/day if not at non-HDL goal
Very high triglyceridesVery high triglycerides Omega-3 fatty acids 3-4 g/day or gemfibrozil 600 mg/dayOmega-3 fatty acids 3-4 g/day or gemfibrozil 600 mg/day

49
• ↓ ApoA-1, ↓ ApoA-2
• ↓ ApoE
• ↓ Apo CII/CIII ratio
• ↑ ApoB
• ↑ LP(a)
Apolipoprotein abnormalities in CRF
50
• ↑ plasma VLDL, ↓ VLDL and CM clearance,
• ↑ plasma IDL and CM remnants
• ↑ plasma triglyceride
• ↓ adipose tissue triglyceride
• TG-enrichment of LDL and HDL
Triglycerides and TG-Rich LP Metabolism In CRF

51
Lipoprotein Lipase Deficiency (LPL)
• ↓ LPL expression and activity in muscle, myocardium and fat tissue (CRF rats)
(Vaziri, Liang, Kidney Int 50:1928-1935, 1996; Vaziri et al AJP 273:F929-930, 1997)
• Contributing factors: ↑ PTH, ↓ physical activity, uremic endocrinopathies, ↓ ApoC II/C III ratio,
↑ pre-B HDL, ↓ HDL-2, chronic heparin use, ?uremic inhibitor(s)
• Consequences: - deficient delipidation of VLDL and CM - ↓ fat tissue TG- ↑ plasma TG
- lipid fuel availability to muscles

52
VLDL Receptor Deficiency • ↓ VLDLr mRNA and protein in skeletal muscle
and fat tissue in CRF rats (Vaziri, Liang, Kidney Int 51:913-919, 1997)
• CRF-induced VLDLr deficiency is unrelated to ↑ PTH
(Liang, Oveisi, Vaziri, Kidney Int 53: 626-630, 1998)
• Consequences: - ↓ VLDL clearance- ↑ plasma VLDL
53
Hepatic Lipase Deficiency in CKD
• ↓ Hepatic lipase mRN and activity in CRF rats (Klin et al, JCI 97:2167-2173, 1996; Sato, Liang, Vaziri, KI 64:1780-1786, 2003)
• Deficiency linked to 2° hyperparathyroidism (Klin et al)
• Consequences: - ↑ IDL (↓ IDL→ LDL conversion), - ↑ LDL-TG, - ↑ HDL-TG

54
Downregulation of LDL Receptor-Related Protein (LRP) in CKD
• ↓ Hepatic LRP mRNA and protein abundance in CRF rats (Kim C, Vaziri ND. Kidney Int 67:1028-1032, 2003)
• Consequences:
- ↓ Clearance and ↑ plasma chylomicron remnants
(prolonged Post-prandial hyperlipidemia)

55
• ↓ HDL-3 maturation to HDL-2 • ↑ Pre-Beta HDL• ↓ HDL-cholesterol • ↑ HDL triglyceride• Impaired HDL function
HDL- Metabolism in CRF

56
1-Apo A-I and Apo A-II In CRF
• ↓ Plasma ApoA-I and -II in CRF humans and animals • ↓ Hepatic Apo A-I gene expression in CRF rats (Vaziri, Ding, Liang NDT 14:1462-1466, 1999)
• Consequence:
- ↓ plasma HDL

57
3- Lecithin Cholesterol Acyltransferase(LCAT)
-Made by liver, secreted in plasma LCAT --
Catalyzes extra-cellular:
A- Hydrolysis of sn-2 Fatty acid in phospholipids (phospholipase-2)
&
B- Esterification of free cholesterol
(acyltransferase activity)

58
Anti-atherogenic Actions of HDL
A- Reverse cholesterol - lipid transport
B- Antioxidant/anti-inflammatory actionsa. ApoA-I mediated extraction of oxidized phospholipids from lipoproteins and cell membrane
b. LCAT-mediated hydrolysis of proinflammatory oxidized phospholipids (AA at sn-2)
c. Prevention of LDL oxidation and destruction of oxidized phospholipids by paraoxonase-1 & GPX
d. Inactivation of PAF and PAF-like phospholipids by PAF acetyl hydrolase (anti-inflammatory / anti-thrombotic)
59
Conclusions (2/3)
• These abnormalities are compounded by concomitant proteinuria (or ? PD) which can raise plasma chol by up-regulating HMG-CoA reductase & lowering LDLr.
• Dysregulation of lipid metabolism and inflammation work in concert to promote atherosclerosis.
• Atherosclerosis in ESRD is primarily driven by inflammation which tends to lower plasma chol.
• Consequently, therapeutic strategies should be directed at amelioration of oxidative stress & inflammation & HDL and TG metabolism (as opposed to chol-lowering Rx).

Hypertriglyceridemia in ESRD
VLDL
CM
TG IDL
CMremnant
TG
FFA
LPL
LPL
Decreased LPL activity and VLDL receptor; therefore retain remnant particles, which are putatively highly atherogenic

Dyslipidemia in ESRD
Kwan BC, et al. J Am Soc Nephrol. 2007;18:1246-1261.
ParameterParameter HemodialysisHemodialysis
Total cholesterolTotal cholesterol
LDL cholesterolLDL cholesterol
HDL cholesterolHDL cholesterol
Non-HDL cholesterolNon-HDL cholesterol
TGTG
Lp(a)Lp(a)
ApoA-IApoA-I
ApoA-IVApoA-IV
ApoBApoB
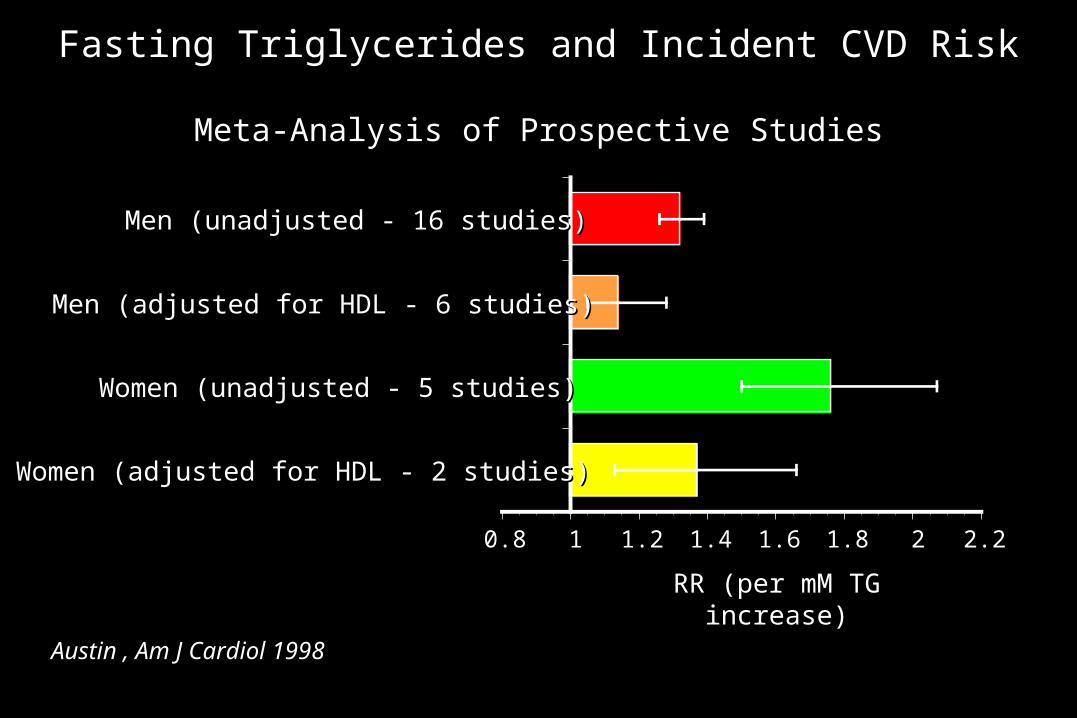
Fasting Triglycerides and Incident CVD Risk
Meta-Analysis of Prospective Studies
Women (adjusted for HDL - 2 studies)Women (adjusted for HDL - 2 studies)
Women (unadjusted - 5 studies)Women (unadjusted - 5 studies)
Men (adjusted for HDL - 6 studies)Men (adjusted for HDL - 6 studies)
Men (unadjusted - 16 studies)Men (unadjusted - 16 studies)
0.80.8 11 1.21.2 1.41.4 1.61.6 1.81.8 22 2.22.2
RR (per mM TG increase)RR (per mM TG increase)
Austin , Am J Cardiol 1998Austin , Am J Cardiol 1998
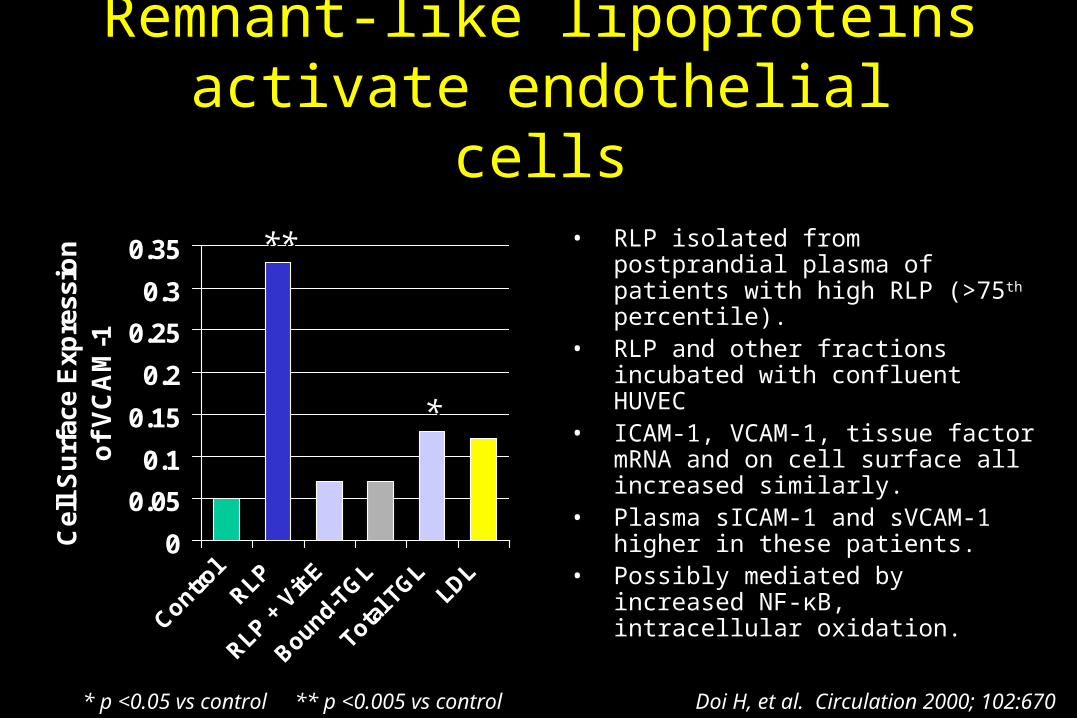
Remnant-like lipoproteins activate endothelial
cells
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Control
RLP
RLP + V
it E
Bound-TG
L
Total T
GLLDL
Cel
l S
urf
ace
Exp
ress
ion
o
f V
CA
M-1
• RLP isolated from postprandial plasma of patients with high RLP (>75th percentile).
• RLP and other fractions incubated with confluent HUVEC
• ICAM-1, VCAM-1, tissue factor mRNA and on cell surface all increased similarly.
• Plasma sICAM-1 and sVCAM-1 higher in these patients.
• Possibly mediated by increased NF-κB, intracellular oxidation.
Doi H, et al. Circulation 2000; 102:670Doi H, et al. Circulation 2000; 102:670
****
**
* p <0.05 vs control ** p <0.005 vs control* p <0.05 vs control ** p <0.005 vs control

The Fenofibrate Intervention and Event Lowering in Diabetes Trial
Lancet , 2005. Diabetic Care, 2009
N = 9.795 type II DMN = 9.795 type II DM
No clear indication for No clear indication for lipid-lowering drugslipid-lowering drugs
BaselinBaseline LDL-C = 119 e LDL-C = 119 mg/dL; TG = 154 mg/dLmg/dL; TG = 154 mg/dL
Fenofibrate 200 mg QDFenofibrate 200 mg QD
Subgroup TG >200 mg/dL: Subgroup TG >200 mg/dL: HR = 0.77 (p=0.01)HR = 0.77 (p=0.01)
Subgroup TG >200 mg/dL + Subgroup TG >200 mg/dL + low HDL-C: HR = 0.73 low HDL-C: HR = 0.73 (p=0.005)(p=0.005)
Unadj.Unadj. AdjustedAdjusted
for statinfor statin
Potential Caveats of AURORA
• Exclude patients on statins (who might need statins)
• Low event rates (selection bias against patients who needed statins)
• Age 50-80 yrs

SPACE (Secondary Prevention with Antioxidants of CVD in
ESRD)
• 196 HD patients with CVD • Vitamin E (800 IU/d) vs. placebo• Median F/U: 1.4 yrs• 1° endpoint: Composite of MI / unstable angina / ischemic stroke / PVD
• Vitamin E arm:– RR = 0.46 [0.27-0.78]; p=0.014 for 1° endpoint
• No difference in mortality or individual CVD
Boaz, Lancet, 2000

JUPITER
Ridker P, Lancet, 2009

N-Acetylcysteine (NAC) in Hemodialysis
• 134 HD patients (including DM + CVD)• NAC 600 mg BID vs. placebo• Median F/U 14.5 (1–24) months• 1° endpoint: Composite of CVD death / MI / coronary revascularization / ischemic stroke / PVD surgery
RESULTS:• 28% of NAC vs. 47% of placebo reached 1° endpoint (RR = 0.60 [0.38-0.95]; p=0.03)
• No difference in total mortality
Tepel, Circ, 2003