discharge and transfer of care
TRANSCRIPT
Version 1.2 July 2018
Discharge and Transfer of Care
Target Audience
Who Should Read This Policy
All Clinical Staff
Discharge and Transfer of Care Policy
Version 1.2 July 2018
2
Ref. Contents Page
1.0 Introduction 5
2.0 Purpose 5
3.0 Objectives 5
4.0 Process for Discharges 5
5.0 Procedures connected to this Policy 14
6.0 Links to Relevant Legislation 14
6.1 Links to Relevant National Standards 15
6.2 Links to other Key Policies 17
6.3 References 18
7.0 Roles and Responsibilities for this Policy 19
8.0 Training 20
9.0 Equality Impact Assessment 20
10.0 Data Protection and Freedom of Information 20
11.0 Monitoring this Policy is Working in Practice 22
Appendices
1.0 Inpatient Discharge Checklist for Mental Health 25
2.0 Community Mental Health Team 26
3.0 Admission & Discharge Checklist – Learning Disabilities 28
4.0 Simple or Complex Discharge Flowchart 34
5.0 Child and Adolescent Mental Health Service 35
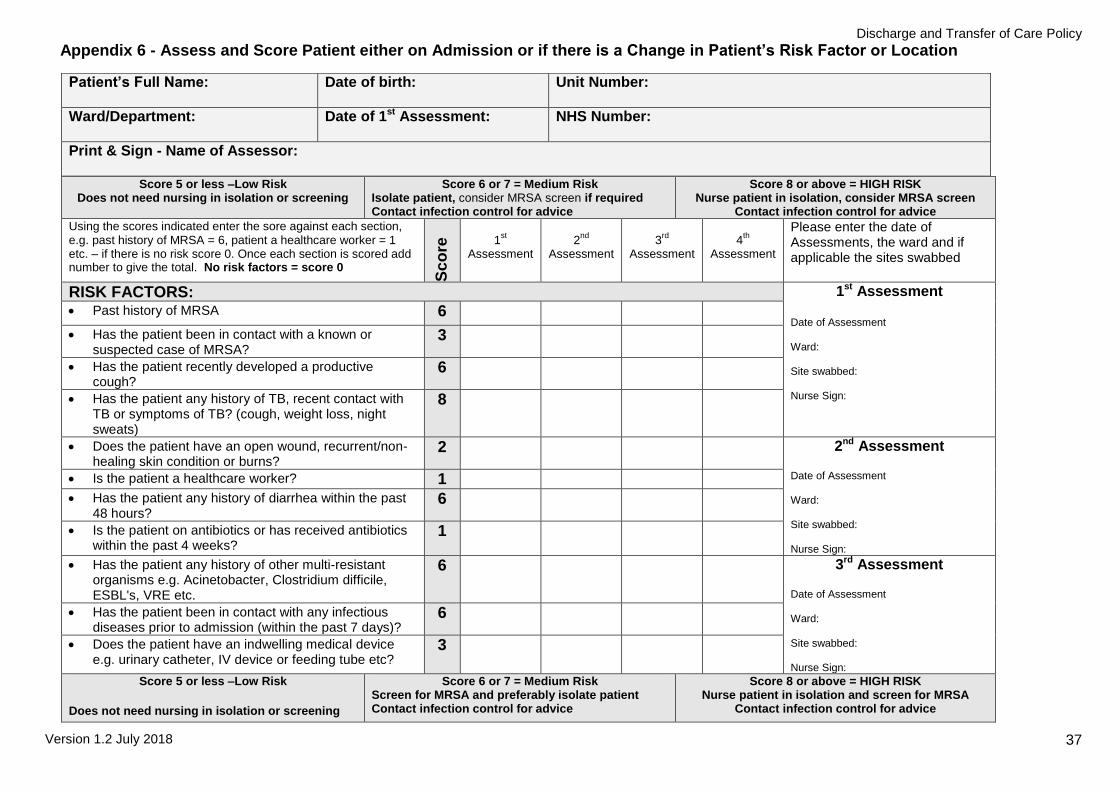
6.0 Appendix 6 - Assess and Score Patient either on Admission or if there is a
Change in Patient’s Risk Factor or Location 37
7.0 Delayed Discharge 39
Discharge and Transfer of Care Policy
Version 1.2 July 2018
3
Explanation of terms used in this policy
Care Programme Approach (CPA) - The term Care Programme Approach (CPA) has been used
since 1990 to describe the framework that supports and co-ordinates effective mental health care for
people with severe mental health problems in secondary mental health services
Common Assessment Framework (CAF) - The adoption of a common framework based on the experience to date from implementing the Care Programme Approach (CPA) for Mental Health, the
Single Assessment Process (SAP) for Older People, and Person Centred Planning for People with
Learning Disabilities. The aim of adopting a common framework is to remove the artificial boundary of 'older age', and provide continuity of a person centred approach
Delayed transfer - A delayed transfer of care occurs when a patient is ready for transfer from once
service area to another, or from one team to another but is still occupying a bed or placement
designated for the original care.
Discharge from Inpatient Care - When a service user is discharged from a ward or inpatient unit and their care is very often transferred to a community team within the Trust involving a transfer
between teams.
Discharge from section - This applies to those detained under the Mental Health Act 1983 when
they are discharged from detention under the Act. They may however remain in hospital informally or continue treatment within the community, sometimes under Section 25 (or from 1.10.08, a
Community Treatment Order under Section 17A of the Mental Health Act 2007).
Discharge from the Trust - When a service user is discharged entirely from the care and treatment
of the Trust. They could be discharged back to their GP or have ongoing specialist treatment outside the Trust involving a transfer of care.
Independent Mental Health Advocate - A specialist mental health advocate who helps to provide
and explain information about mental health legislation, regarding conditions, restrictions and rights
Multi-disciplinary team (MDT) - Includes doctors, nurses, psychologists, social workers,
pharmacists, occupational therapists, speech and language therapists, dieticians and occupational therapists and any other health and social care professionals caring for that patient
PALS - Patient Advisory and Liaison Service (PALS) is a trust based-service which offers independent
advice and support to service users and carers regarding any concerns they may have about the
service they have received
Person-centred Planning (PCP) - Putting the person at the centre of planning for their lives by listening to and learning about what they want from their lives and helping them to think about what
they want now and in the future
Service User - The term is used generically and covers, patients, clients or any person who uses
services managed by Black Country Partnership NHS Foundation Trust
7 Day Follow-up form - The arrangements made to ensure follow-up within 7 days for service users following discharge from an inpatient unit. The form is a single page document forwarded before the
date of discharge, by the ward
Single Assessment Process (SAP) - Multi-professional person centred assessment process
primarily for older people but increasingly used as a framework for delivering services to other adult groups requiring care
Transfer - A patient is ready for transfer when a multi-disciplinary team decision has been made that the patient is ready for transfer and the patient is safe for discharge/transfer

Discharge and Transfer of Care Policy
Version 1.2 July 2018
4
Transfer between teams - This refers to when service users are transferred from one clinical team
to another within the Trust. This could, for example, involve their discharge from inpatient care to a
community team or to be followed up in an outpatient setting. It could also involve a transfer to a specialist team within the Trust or the admission to hospital of a service user previously cared for by a
community team.
Transfer of Care - This refers to when a service user’s ongoing treatment is moved to services
outside the Trust and they are discharged from the care of the Trust.
TTOs - Tablets to take out
Discharge and Transfer of Care Policy
Version 1.2 July 2018
5
1.0 Introduction It is an essential requirement of good patient care that discharge and transfer of care is planned and co-ordinated on a multi-disciplinary and multi-agency basis and that patients and carers are involved in making decisions and kept informed of their discharge or transfer plans. Early discharge planning with patients and carers through multi-disciplinary co-operation will promote flexibility and accessibility of services whilst supporting the individual’s choice. Discharge or transfer of care should be managed as a process and not an isolated event. All discharges or transfers of care should involve the development and implementation of a plan to progress towards the transfer of an individual from hospital to their home or to a more appropriate setting. The individuals concerned and their carers should be fully involved in this process and kept fully informed by regular reviews and updates of their care plans and estimated date of discharge or transfer. This policy recognises that many people need ongoing support whether they are leaving hospital, or are referred to different services and continuity of the right care in the right place is what matters most to them. Admission, discharge and other associated processes should now all be viewed are as a ‘transfer of care’ process. Therefore this policy has been developed to help all staff, across all services to improve their localised discharge and transfer of care processes and practices. It provides the overall framework; within set principles, that ensures staff have the support and guidance they need to achieve good and safe discharge and transfer of care practices.
2.0 Purpose The purpose of this policy is to ensure that discharge or transfer from services managed by the Black Country Partnership NHS Foundation Trust is effective, consistent and organised around the needs of individual service users and carers.
3.0 Objectives To set out the roles and responsibilities of staff involved with discharge or
transfer from services To provide continuous information sharing and communication with service
users and carers regarding their needs To ensure early and effective discharge planning facilitated by a co-ordinated
multi-agency approach is embedded in the delivery of services To work with other providers, agencies and organisations proactively, to
improve early and effective discharge planning and transfer of care Any individual’s care that would be optimised by using a service that is not
designated for their age group or they have needs that fall into more than one service should be able to have appropriate access to it irrespective of where their care is being managed
Transition is to be viewed by staff as a continuous process rather than a series of assessments, interviews and reviews
4.0 Process for Discharges
4.1 Discharge Requirements for all Patients Protocols and procedures for discharge within all services must be based as far as possible on common assessment and planning frameworks and methodologies e.g.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
6
Single Assessment Process (SAP) Care Programme Approach (CPA) and incorporate the following steps:
Start thinking and planning for discharge before, on and during admission
Identify whether the patient has simple or complex discharge planning needs, always involving the patient and carer in your decision making processes
Develop an initial care plan and complete initial risk assessment screening tool (Sainsburys) for every patient within 24 hours of inpatient admission to the service
Co-ordinate the discharge process through effective leadership and handover of responsibilities at ward level/ team level e.g. SAP/CPA/care plan review
Set an expected date of discharge, ideally within three days of admission for acute care cases or for more complex cases, as soon as it becomes clinically appropriate to do so and discuss with the patient and carer
Ensure care planning review/CPA/SAP review is undertaken within the review period as stated on the SAP/CPA/care plan documentation. Ensure actions are taken with updates/progress made to towards the discharge and is clearly recorded within the SAP/CPA/Care Planning documentation
Involve patients and carers so that they can make informed decisions and choices that deliver a personalised care pathway and maximise their independence
Develop a care plan for those patients not in inpatient areas and are community based
Ensure section 117 after care is in place and recorded as appropriate
Plan discharges to take place within an agreed period of time, e.g. three days, seven days, two weeks etc. dependant on circumstances, in order to deliver continuity of care for the patient
Wherever possible use the appropriate discharge checklist (Appendix 2 and Appendix 3) completing the list 24 - 48 hours prior to discharge
Ensure SAP/CPA/Care Planning documentation is up to date, signed, dated, with copies given to service user and clinical team in the community
Ensure that patients GP is informed by way of discharge follow up letter of the discharge plan within 48 hours of discharge
Please refer to Appendix 1 (MH inpatient), Appendix 2 (MH community) and Appendix 3 (LD) Discharge Checklist (utilise references from service clinical information systems, i.e. oasis, care notes etc.)
4.1.1 Excess Winter Deaths and Illness and the Health Risks Associated with Cold Homes NICE Clinical Guideline NG6 is for commissioners, managers and health, social care and voluntary sector practitioners who deal with vulnerable people who may have health problems caused, or exacerbated, by living in a cold home. This guideline makes recommendations on how to reduce the risk of death and ill health associated with living in a cold home. On discharging patients to their own homes the Trust must receive assurance that the home is appropriately heated.
4.2 Simple Discharge Process A simple discharge is one that:
Will involve minimal disturbance to the patient’s activities of daily living
Facilitates a patient’s return to their usual place of residence
Discharge and Transfer of Care Policy
Version 1.2 July 2018
7
Will not require a significant change in support offered to the patient or their carer in the community
Have simple ongoing care needs that do not require complex planning and delivery
Please see Appendix 4
4.3 Complex Discharge Process Complex discharges occur when there are significant changes in the care needs of a patient since admission resulting in the patient being unable to return to their usual place of residence or requiring increased input from community based health or social care providers on discharge. Such complexities will be picked up, actioned and recorded through 16 week care pathway (LD) or CPA review as part of the Mental Capacity Act. Please see Appendix 4 4.4 Delayed Discharge within LD Once the patients agreed health outcomes for admission have been met but no discharge package or date has been finalised, the MDM will decide if the discharge is considered to be delayed. Correspondence will be sent to the named social workers. For the first two months letters A and B will be sent from the unit manager (see Appendix 5). Following this letter C will be sent from the service managers on a monthly basis until a discharge package and date is agreed. This information is collated by LD Operational and Performance Team. Please see Appendix 7 4.5 Unplanned Discharge Unplanned discharges should only be undertaken within working hours to ensure full MDT involvement to support decision making processes and should be clinically led. Any unplanned discharges outside of working hours should only be undertaken in exceptional circumstances and should be formally raised as a Datix incident. Unplanned discharges must evidence consideration of:
Engagement of MDT liaising with other relevant agencies involved
Environmental factors – home environment accommodation etc.
Previous risk factors
Current risk factors
Clear plan in place including medication and treatment regime, follow up plan etc.
Ongoing police restrictions
Patient and carer engagement in discharge process
Full supporting documentation
4.5.1 Discharge out of Hours Out of Hours is the time period between 17:00 hours and 09:00 hours Monday to Friday and for the entire duration of weekends and bank holidays. This policy seeks to ensure that all patients, including those with complex needs, are discharged or transferred safely with a planned, timely and appropriate care
Discharge and Transfer of Care Policy
Version 1.2 July 2018
8
package. Therefore, wherever possible, discharges and transfer of care should be made during the normal working day. The Trust does not expect discharge or transfers to take place outside the normal working day except in exceptional circumstances as there is only limited availability of staff and of community based services. Decisions about the appropriateness of discharges or transfers should consider the need for assessment of and provision for patient’s needs i.e. the age of patient, their home circumstances, the level of support required post discharge as well as an appropriate timeframe for this assessment and provision. Where there are compelling reasons for a discharge or transfer of care to be made out of hour’s staff must ensure that the patients’ electronic or paper health care records are fully completed and remain on site. The information to be offered to the patient and to be sent to the receiving Health Care Professional, will remain consistent with the in hours approach to patient discharge or transfer. The Trust encourages and allows patient identifiable data to be sent by fax or email as long as the data is sent securely. In practice this means that:
Any discharge or transfer information that is faxed should be sent from and to a safe haven fax i.e. the sender remains at the fax and then seeks confirmation that it has been received
Any discharge letter that is emailed should be sent from an NHS Net account to an NHS Net account e.g. [email protected] to [email protected]
Under no circumstances should a discharge or transfer information be sent from an unsecure Trust email account to another organisations unsecure email account e.g. [email protected] to [email protected]
For further information please see the Information Sharing Policy 4.5.2 Self-Discharge Patients, who wish to self-discharge, could potentially be at risk. Staff should record that they have informed the patient of the risks in order for the patient to make an informed choice. It is essential that the patient has capacity to make this decision when assessing the risk of a ‘Self-Discharge’.
If after all appropriate personnel have been informed and have spoken to the patient, and the patient still wishes to leave, the patient should be asked to sign a ‘Discharge against Medical Advice’ form.
Patients wishing to self-discharge should be advised to contact their GP Practice as they may need services or treatment in the community.
The doctor will, as with regular discharges, send a discharge letter to the GP and should contact the GP by phone if they have any immediate concerns. Nursing staff should inform any appropriate community staff or relatives/carers and the matron/manager on call
If the patient is under sixteen or deemed to be an ‘adult at risk’ and wishes to leave against advice, the nurse should inform the parent or carer, the senior nurse on duty, the doctor and the police.
All actions should be accurately documented in the patients’ records.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
9
If a patient wishes to discharge him or herself because they have a concern or complaint, all efforts need to be made to resolve the problem in order to allow their care to continue. Further information on dealing with complaints can be sought by contacting the Patient Experience and Involvement Team. 4.6 Did Not Attend (DNA) For information and guidance regarding discharging patients who repeatedly fail to attend appointments, please refer to: Did Not Attend / No Access Visit Adult Safeguarding Policy or Did Not Attend/No Access Visit Policy – CYPF as appropriate.
4.7 Seven Day Follow up After Discharge from Mental Health Inpatient Units In Mental Health services there are national requirements regarding community follow up of service users discharged from inpatient wards. The Trust must ensure that all vulnerable service users have access to face to face follow up as the first contact in the community within a maximum of 7 days following discharge. This includes those who take their own discharge. Service users who are identified as particularly vulnerable or at risk should be followed up within 48 hours; this decision is to be taken in consultation with the ward MDT, crisis and home treatment team, service user and their family/ carers.
4.8 Planning Transfers The default position for transition to all services will be age. Transfers should be made by 18th and 65th birthday. Consideration of transfer, where there is an enduring or episodic mental illness, should commence 6 months before the person’s 18th or 65th birthday. This will require a comprehensive review of their health and social care needs, and should be completed at least 3 months before the relevant birthday. If the review concludes that transfer is necessary, a clear process for the practicalities of transfer should also be agreed. It is the responsibility of the transferring service to trigger the process of transfer, adopting the usual referral process. The existing service will retain responsibility until transfer is confirmed. 4.9 Exceptions Where someone has a learning disability the default position will be that they receive services in the learning disability services for adults and children with a learning disability. Where the person has early onset dementia and is younger than 65, responsibility for treatment and care will be with the older people's services. Referrals should be to the general adult service unless there is a clearly established diagnosis of early onset dementia. People meeting the criteria for the Early Intervention Service, first psychotic episode, should be referred to that service. 4.10 Decision in Respect of People not Previously Known to the Service
Access to secondary care mental health services should be via a known (referred) single point directly to the service. For example:
Discharge and Transfer of Care Policy
Version 1.2 July 2018
10
Child and Adolescent Mental Health Services Point of Access Service (0-18th birthday) (see Appendix 5)
Adult Mental Health Point of Access Service (18-65th birthday) Older Adults Mental Health Services Point of Access (After 65th birthday) Learning Disabilities Point of Access ( Learning Disabilities for Adults) Children with Learning Disabilities, to be directed as follows:
- Mild learning disabilities please refer to CAMHS - Severe learning disabilities please refer to Adult Learning Disability Services - Moderate learning disabilities decision to be jointly agreed by CAMHS and
Adult Learning Disabilities to provide the best service (see Appendix 5) Gerry Simon Clinic referrals to be made to NHS England for gate keeping assessment to low secure. The Larches and Assessment and Treatment services referrals to be made from consultant to consultant, admission clinical treatment review (CTR) must have been completed. Referrals to services should be made on the basis of age, except for Learning Disabilities where referrals should be directly to the service areas if the presenting issue is predominantly Learning Disabilities. 4.11 Decisions in Respect of People Currently Known to Services Where people are known to services and known to have ongoing needs, they can continue in children’s services or adult services if it is deemed clinically appropriate and has been agreed by the responsible clinician, service, and the user. In this event, reviews should continue to consider the option of transfer, and initiate this once deemed clinically appropriate. 4.12 Out of Area Transfers (Incoming) - All Services Documentation Requirements The process for receiving service users from outside the area is as follows:
i. Requests for transfer of care must be made in writing to the receiving Consultant. Verbal requests cannot be accepted. Ensure letters have included patient details and current team contacts
ii. Copies of ‘request for transfer of care’ letters must be sent immediately to the Team Leader of the relevant team/service
iii. The Team Leader will then contact the manager of the referrer's respective team and initiate the process of a full CPA handover where all agencies involved in the care of the patient are present
iv. CPA handovers of care must include: CPA documents that are current, up to date and correctly completed, full risk assessment details, copies of individualised care plans, GP details and any other aftercare arrangements
v. For inpatient services - complete all admission documentation
4.13 Transfers Out of Area (Outgoing) - All Services The process for referring patients/service users outside the area reverses the above stated protocol as follows:
i. Consultants must refer to receiving teams in writing. The letter requesting transfer of care needs to include patient details and team contacts
ii. A copy of the letter requesting transfer of care to an out of area team needs to be sent to the team leader of the patients existing team/service. The Team leader can then ensure current CPA documentation, individual care plans and any other relevant documentation is prepared in anticipation of the full meeting. The Team Leader, or, where relevant care coordinator, is to alert
Discharge and Transfer of Care Policy
Version 1.2 July 2018
11
the multi-disciplinary and any other agencies involved with care that a full CPA meeting is due
iii. Upon receiving contact from the receiving team, the Team Leader or, if relevant, care co-ordinator is to arrange a full CPA meeting in accordance with normal CPA practices
In either scenario, the referring consultant should always retain the clinical responsibility of the concerned patient until the CPA handover is completed, after care arrangements are made explicit, the referral is formally accepted and the patient is offered an outpatient appointment in the new area of residence.
4.14 Transfer between Services i. The Team Leader/person in charge/responsible clinician, whichever is
relevant, will contact the manager/appropriate member of the respective team and initiate the process of a full CPA handover where the patient and all agencies involved in the care of the patient are present
ii. CPA handovers of care must include: CPA documents that are current, up to date and correctly completed, full risk assessment details, copies of individualised care plans, GP details and any other aftercare arrangements
iii. For inpatient/residential services - complete the infection control assessment upon arrival
4.15 Transfers between General/Acute/Medical Care Services i. The person in charge to complete an assessment of individual needs and risk.
Where needed, specialist mental health /learning disability care needs, in agreement with the host site, to be in place during period of admission/ treatment
ii. Complete the 'patient/service user transfer form' and the 'transfer checklist', clinical details will be provided by medics. There is no need to remove health and social care records from Trust premises (see Information Sharing Policy)
4.16 Transfer or Discharge of Service Users Reducing Routes of Cross Infection The prevention and management of infectious diseases is a high priority in all health care organisations. The transfer/discharge of service users known to have an infection can put both the service user and others at risk. Therefore infection prevention and control procedures must be followed in all decision making when planning transfer of a service user. All patients must have an up to date infection risk assessment completed prior to transfer. Sharing of essential information related to a patients infectious status when transferring them internally between units or to another organisation ensures any risks are minimised (see IPC SOP 16 Sharing information with other health and social care providers in relation to patients with a known or suspected infection) - see Appendix 6 4.17 Information to be Given to the Receiving Healthcare Professional For transfers of specialist care outside the Trust the following records should be sent as a minimum:
Assessment of current health and social care needs
Up-to-date clinical risk assessment
Up-to-date care plan which includes crisis and contingency arrangements
Discharge and Transfer of Care Policy
Version 1.2 July 2018
12
Current/ongoing medication
Legal status and CPA level as applicable
For those detained under the Mental Health Act, relevant section papers
Safeguarding Adult issues
Safeguarding Children issues
Any other supporting written information In the case of discharge from the Trust to the GP, it is also required that appropriate discharge information including medication needs should be provided. 4.18 Information to be Given to the Patient when they are Discharged or Transferred a) The service user must be offered a copy of their written care plan and be
supported to understand its contents b) The service user must be offered a copy of the service user pack containing
standard information and information specific to their individual needs c) Where appropriate the carer should also have access to and a copy of this
information d) The service user should be informed that they will receive follow-up within 7 days
of discharge and which service will be delivering that.
Ensure continuity of information. Every effort must be made to ensure consistency and continuity of information from different people. Information leaflets about the receiving service/team or discharge arrangements will ensure the patient understands what is happening. Contact the receiving service for a copy of their leaflet prior to transfer/ discharge. The provision of information and discharge folders can be helpful. The patient and carer can have their own safe place to keep their care plans, a record of events, correspondence and future plans. Information folders enable patients to look through the information at their own pace, ask questions later and raise their concerns
Where patients cannot represent themselves, the next of kin, carer, relative or an independent mental capacity advocate (IMCA) must be involved. An IMCA’s role is to represent the patient’s interest, and to challenge any decision that does not appear to be in the best interest of the patient. A referral is to be made on admission if applicable (see Mental Capacity Act Policy). 4.19 Medication Service users and or carers/relatives should receive clear discharge and post discharge medication information. The discharge prescription chart, should be sent to, or collected by, pharmacy in good time and preferably at least 24hrs before discharge. In particular, patients who require a monitored dosage system (e.g. NOMAD ®) will need more input and time to dispense and organise the appropriate arrangements by liaising with the relevant community pharmacy. Discharge prescriptions for patients who are being started for the first time on a monitored dosage system should ideally be written 48 hours before discharge to give sufficient time for arrangements to be made.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
13
Nurses must never supply drugs from ward stock to patients going home. Patients should not be discharged from the ward without the appropriate drugs and a copy of the TTO. In general, prescriptions for inpatients who are being discharged should be for a 14 and 28 days’ supply respectively, unless a shorter/longer course is indicated, or it is appropriate, at the pharmacist's discretion, to supply the manufacturer's original pack. Medication taken from a ‘one-stop’ dispensing ward, authorised by pharmacy, will be a minimum of fourteen days’ supply. If a patient being discharged is at risk of self poisoning/ misuse of medicines, they should only be provided with a small supply of medicine e.g. for a day, a few days or a week. This should be discussed with the pharmacy team as necessary. Please refer to the Medicines Policies for more detailed information and guidance. 4.20 How the Organisation Records the Information Given to the Receiving Healthcare Professional and the Patient when they are discharged
4.20.1 Internal Transfers Discharge plans and record of discussions will be documented in the appropriate format on the electronic system and a copy retained in the healthcare record in accordance with the professional standard for record keeping and the Trust’s Records Management Policy.
A copy of the agreed plan will be given to each service user.
Discharge and contingency plans are recorded as part of the existing assessment & care planning process and included in integrated care pathways where used. Discharge checklists may be used for further guidance and evidence of completed actions, such documents may be included in the integrated care pathway documentation or local documents. Such documents must provide clear details of personal information, location of discharge, actions taken and clear accountability for completion (see Appendix 1 for MH inpatients, Appendix 2 for MH community and Appendix 3 for LD Discharge check lists). Utilise references from service clinical information systems, i.e. oasis, care notes etc. 4.20.2 Discharges to/from other Providers If a transfer or discharge from a team or inpatient unit occurs to an organisation or Trust outside of the Trust, including to an acute hospital setting, the healthcare record remains the property of the Trust at all times. Service user consent must be sought before copies of relevant parts of the record are shared with the new organisation. If the service user refuses, a decision must be made based on any risks identified of not sharing the information. If the service user does not have capacity to give consent to share information, the Responsible Clinician or Care Co-ordinator/lead professional will apply best interest rules (please refer to Mental Capacity Act Policy). Information that indicates a child or adult may be suffering, or at risk of suffering significant harm must be shared in line with the Trusts’ information sharing protocols. Any decisions relating to consent, confidentiality and sharing information must be documented in the healthcare record and the Transfer of Care to another provider form completed. Examples could include risk assessment, health and social care
Discharge and Transfer of Care Policy
Version 1.2 July 2018
14
assessment, discharge letter, care plan, pre-discharge review summary. This must include any section117 aftercare entitlements (please refer to Mental Health Act Policy). If a service user is received into the care of a team or inpatient unit from outside the Trust, it is the responsibility of the receiving team to contact the referrer and ensure that photocopies of any relevant healthcare records are requested. Examples could include risk assessment, health and social care assessment, discharge letter, care plan, pre-discharge review summary. These records should then be incorporated into a trust healthcare record. Black Country Partnership NHS Foundation Trust patient healthcare records must remain in the possession of the Trust. 4.21 Incident Reporting Staffs need to complete a Trust Incident Form via DATIX if the standards for managing the quality of discharges or transfer of care in this policy are not upheld. This could include when an error or anomaly is identified within a record they are handling e.g. an error in recording patient identification details or health care information inserted into the wrong health records. The aim of reporting incidents is to make timely improvements to the discharge and transfer of care processes by providing a record of issues that can be addressed.
5.0 Procedures connected to this Policy
Discharge and Transfer of Care - SOP 01 -Planned Care Community
Discharge and Transfer of Care - SOP 02 - 7 day Follow up.
6.0 Links to Relevant Legislation Human Rights Act 1998 One of the main laws protecting human rights in the UK, it contains a list of 16 rights (called articles) which belong to all people in the UK, and outlines several ways that these rights should be protected. These rights are drawn from the European Convention on Human Rights, which were developed by the UK and others in the aftermath of World War II. The Human Rights Act may be used by every person resident in the United Kingdom regardless of whether or not they are a British citizen or a foreign national, a child or an adult, a prisoner or a member of the public. The Human Rights Act has two main aims, to promote a ‘culture of human rights’ by making sure that basic human rights underpin the workings of government at the national and local level and enabling access to human rights here at home, instead of only being able to go to the European Court of Human Rights It does this by placing a legal duty on all public authorities, including NHS organisations and staff and mental health tribunals carrying out public functions, to respect and protect human rights in everything that they do. This means that public authorities have legal responsibilities for respecting, protecting and fulfilling human rights. This duty is important in everyday situations because it enables individuals to challenge poor treatment and to negotiate better solutions.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
15
Data Protection Act 1998 The Data Protection Act 1998 became law in March 2000. It sets standards that must be satisfied when obtaining, recording, holding, using or disposing of personal data. The law applies to data held on computers or any sort of storage system, including paper records. There are 8 enforceable principles of good practice. Data should be:
Fairly and lawfully processed
Processed for limited purposes
Adequate, relevant and not excessive
Accurate
Not kept longer than necessary
Processed in accordance with the data subject's rights
Secure
Not transferred to countries outside the European Economic Area (EEA), without adequate protection
Freedom of Information Act 2000 The Freedom of Information (FOI) Act gives a general right of access to all types of recorded information held by public authorities, including NHS Trusts. The Act also sets out exemptions to that right and places certain obligations on public authorities. In addition to providing information when asked to do so, FOI also requires public authorities to be proactive in the release of information. Every public authority is required to adopt and maintain a publication scheme setting out how it intends to publish the different classes of information it holds, and whether there is to be a charge for the information disclosed. The Trust’s FOI publication scheme is regularly updated and has been approved by the Information Commissioner. 6.1 Links to Relevant National Standards CQC Regulation 9: Person-Centred Care The intention of this regulation is to make sure that people using a service have care or treatment that is personalised specifically for them. This regulation describes the action that providers must take to make sure that each person receives appropriate person-centred care and treatment that is based on an assessment of their needs and preferences. Providers must work in partnership with the person, make any reasonable adjustments and provide support to help them understand and make informed decisions about their care and treatment options, including the extent to which they may wish to manage these options themselves. Providers must make sure that they take into account people's capacity and ability to consent, and that either they, or a person lawfully acting on their behalf, must be involved in the planning, management and review of their care and treatment. Providers must make sure that decisions are made by those with the legal authority or responsibility to do so, but they must work within the requirements of the Mental
Discharge and Transfer of Care Policy
Version 1.2 July 2018
16
Capacity Act 2005, which includes the duty to consult others such as carers, families and/or advocates where appropriate. CQC Regulation 11: Need for Consent The intention of this regulation is to make sure that all people using the service, and those lawfully acting on their behalf, have given consent before any care or treatment is provided. Providers must make sure that they obtain the consent lawfully and that the person who obtains the consent has the necessary knowledge and understanding of the care and/or treatment that they are asking consent for. Consent is an important aspect of providing care and treatment, but in some cases, acting strictly in accordance with consent will mean that some of the other regulations cannot be met. For example, this might apply with regard to nutrition and person-centred care. However, providers must not provide unsafe or inappropriate care just because someone has consented to care or treatment that would be unsafe. See the glossary for the definition of 'relevant person' in relation to Regulation 11. CQC Regulation 12: Safe Care and Treatment The intention of this regulation is to prevent people from receiving unsafe care and treatment and prevent avoidable harm or risk of harm. Providers must assess the risks to people's health and safety during any care or treatment and make sure that staffs have the qualifications, competence, skills and experience to keep people safe. Providers must make sure that the premises and any equipment used is safe and where applicable, available in sufficient quantities. Medicines must be supplied in sufficient quantities, managed safely and administered appropriately to make sure people are safe. Providers must prevent and control the spread of infection. Where the responsibility for care and treatment is shared, care planning must be timely to maintain people's health, safety and welfare. CQC understands that there may be inherent risks in carrying out care and treatment, and we will not consider it to be unsafe if providers can demonstrate that they have NICE Clinical Guideline NG6 - Excess Winter Deaths and Illness and the Health Risks Associated with Cold Homes The guideline is for commissioners, managers and health, social care and voluntary sector practitioners who deal with vulnerable people who may have health problems caused, or exacerbated, by living in a cold home. This guideline makes recommendations on how to reduce the risk of death and ill health associated with living in a cold home. On discharging patients to their own homes the Trust must receive assurance that the home is appropriately heated. NICE Clinical Guideline NG27 – Transition between Inpatient Hospital Settings and Community or Care Home Settings for Adults with Social Care Needs This guideline covers the transition between inpatient hospital settings and
community or care homes for adults with social care needs. It aims to improve
people's experience of admission to, and discharge from, hospital by better
coordination of health and social care services.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
17
NICE Clinical Guideline NG43 - Transition from Children’s to Adults’ Services for Young People Using Health or Social Care Services This guideline covers the period before, during and after a young person moves from children's to adults' services. It aims to help young people and their carers have a better experience of transition by improving the way it’s planned and carried out. It covers both health and social care. NICE Clinical Guideline NG53 - Transition between Inpatient Mental Health Settings and Community or Care Home Settings This guideline covers the period before, during and after a person is admitted to, and discharged from, a mental health hospital. It aims to help people who use mental health services, and their families and carers, to have a better experience of transition by improving the way it’s planned and carried out.
6.2 Links to other Key Policies Health Records Policy This policy is intended to be a comprehensive guide to all staff involved in the handling of health records and the associated documentation providing a framework for consistent and effective record management enabling the Trust to ensure that there is a systematic and planned approach to the management of health records, from the moment the record is created until their ultimate disposal. Care Programme Approach Policy The purpose of this policy is to set out a clear CPA framework. This is intended to create an environment in which recovery is enabled. Involvement is fundamental to everyday practice and the approach to care is one which maximises the safety and well-being of all as a priority. It is the foundation for excellent service provision and high quality patient experience provided through a multi-disciplinary and inter-agency approach. Mental Capacity Act Policy The purpose of this policy is to underpin the implementation of the MCA within the Trust by outlining the procedures to assess mental capacity, make decisions in the best interests of patients including patients who appear to have no family or friends to consult, use restraint, and follow valid and applicable advanced decisions. The Trust takes its responsibility for the care and treatment of patients seriously and aims to ensure compliance with legislation, statutory instruments and guidance. Clinical Record Keeping Standards Policy The aim of this policy is to provide direction and guidance to staff on how to meet the standards required for the recording of information within health care records. Clinical Risk Management Policy This policy is intended to guide practitioners who work with service users to manage the risk of harm. It sets out the principles and standards required that should underpin best practice across all health settings. Did Not Attend / No Access Visit Adult Safeguarding Policy To provide a clear process for all staff working within the Black Country Partnership NHS Foundation Trust on how to apply safeguarding procedures to the following situations :
non-attendance at pre-arranged appointments;
Discharge and Transfer of Care Policy
Version 1.2 July 2018
18
no access visits where community staff are unable to make contact or gain access to a person’s place of residence;
appointments cancelled in advance by people;
those occasions when appointments need to be cancelled by the Trust Did Not Attend/No Access Visit Policy – CYPF This policy applies to all CYP who through identification and follow up do not attend for health appointments or who are unavailable for home visits. The purpose of this policy is to:
Provide practitioners with information about the potential consequences for CYP in families who disengage from health services
Provide a clear process for managing non-attendance at health appointments and no access visits
Ensure that the process ensures early intervention and prevention when disengagement is a feature as this is the key to safeguarding children and young people
Support effective communication both inter-agency and multi- agency in order to raise awareness when defaulted appointments, no access visits occur
Violence and Aggression Policy The purpose of this policy is to detail the Trust’s strategy and legislative compliance in tackling violence and aggression against patients and staff. Information Sharing Policy This policy provides clarity and guidance for staff to comply with the many different rules in relation to the release of patient information for requests to access any other types of information, please refer to the Trust’s Freedom of Information Policy.
6.3 References Department of Health (2010) Ready to go? Planning the discharge and transfer
of patients from hospital and intermediate care Royal Pharmaceutical Society (2011) Keeping patients safe when they transfer
between care providers - getting the medicines right Pharmaceutical Services Negotiating Committee (2008) Moving patients,
Moving medicines, Moving safely: Guidance on Discharge and Transfer Planning
Discharge and Transfer of Care Policy
Version 1.2 July 2018
19
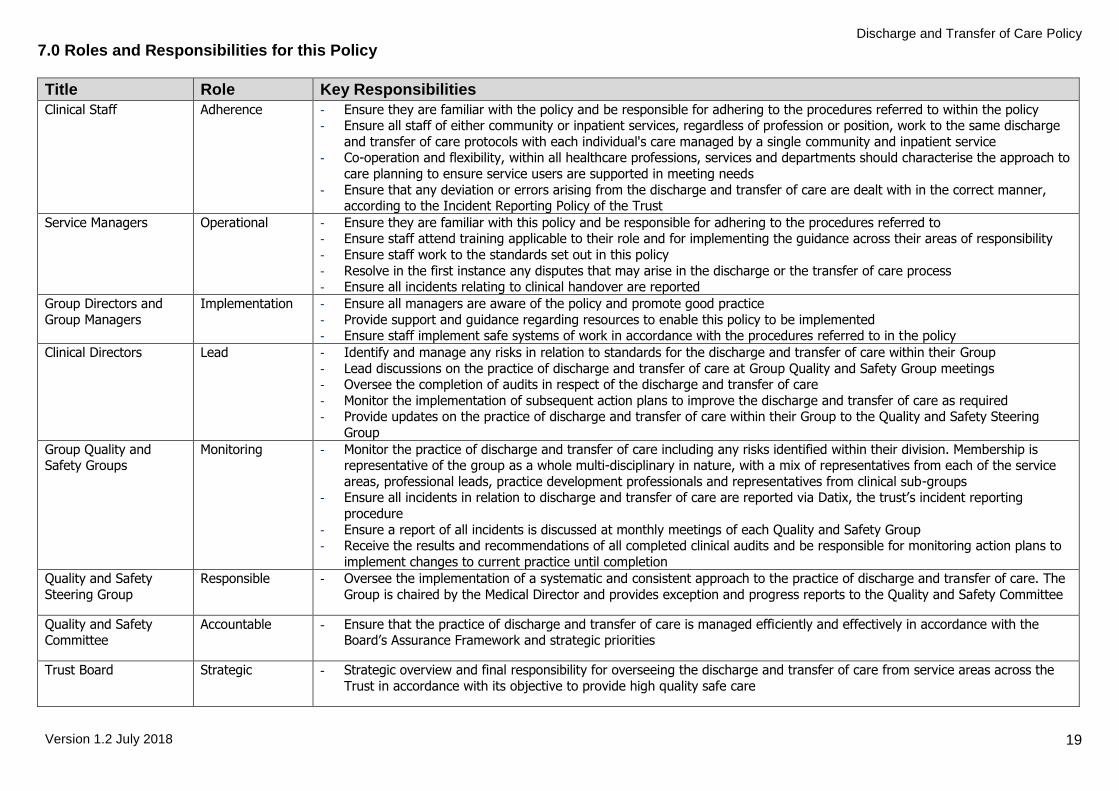
7.0 Roles and Responsibilities for this Policy
Title Role Key Responsibilities
Clinical Staff Adherence - Ensure they are familiar with the policy and be responsible for adhering to the procedures referred to within the policy - Ensure all staff of either community or inpatient services, regardless of profession or position, work to the same discharge
and transfer of care protocols with each individual's care managed by a single community and inpatient service - Co-operation and flexibility, within all healthcare professions, services and departments should characterise the approach to
care planning to ensure service users are supported in meeting needs
- Ensure that any deviation or errors arising from the discharge and transfer of care are dealt with in the correct manner, according to the Incident Reporting Policy of the Trust
Service Managers Operational - Ensure they are familiar with this policy and be responsible for adhering to the procedures referred to - Ensure staff attend training applicable to their role and for implementing the guidance across their areas of responsibility
- Ensure staff work to the standards set out in this policy
- Resolve in the first instance any disputes that may arise in the discharge or the transfer of care process - Ensure all incidents relating to clinical handover are reported
Group Directors and
Group Managers
Implementation - Ensure all managers are aware of the policy and promote good practice
- Provide support and guidance regarding resources to enable this policy to be implemented - Ensure staff implement safe systems of work in accordance with the procedures referred to in the policy
Clinical Directors Lead - Identify and manage any risks in relation to standards for the discharge and transfer of care within their Group
- Lead discussions on the practice of discharge and transfer of care at Group Quality and Safety Group meetings - Oversee the completion of audits in respect of the discharge and transfer of care
- Monitor the implementation of subsequent action plans to improve the discharge and transfer of care as required - Provide updates on the practice of discharge and transfer of care within their Group to the Quality and Safety Steering
Group
Group Quality and Safety Groups
Monitoring - Monitor the practice of discharge and transfer of care including any risks identified within their division. Membership is representative of the group as a whole multi-disciplinary in nature, with a mix of representatives from each of the service
areas, professional leads, practice development professionals and representatives from clinical sub-groups - Ensure all incidents in relation to discharge and transfer of care are reported via Datix, the trust’s incident reporting
procedure
- Ensure a report of all incidents is discussed at monthly meetings of each Quality and Safety Group - Receive the results and recommendations of all completed clinical audits and be responsible for monitoring action plans to
implement changes to current practice until completion
Quality and Safety
Steering Group
Responsible - Oversee the implementation of a systematic and consistent approach to the practice of discharge and transfer of care. The
Group is chaired by the Medical Director and provides exception and progress reports to the Quality and Safety Committee
Quality and Safety Committee
Accountable - Ensure that the practice of discharge and transfer of care is managed efficiently and effectively in accordance with the Board’s Assurance Framework and strategic priorities
Trust Board Strategic - Strategic overview and final responsibility for overseeing the discharge and transfer of care from service areas across the
Trust in accordance with its objective to provide high quality safe care
Discharge and Transfer of Care Policy
Version 1.2 July 2018
20
Title Role Key Responsibilities
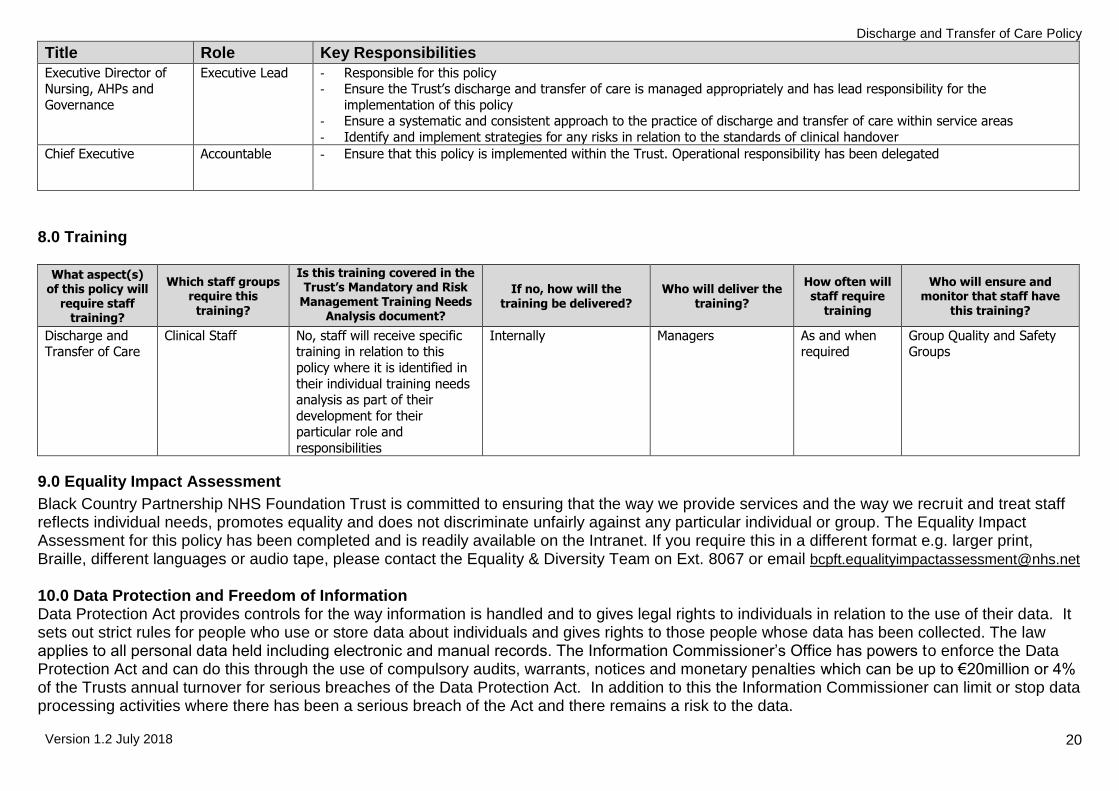
Executive Director of Nursing, AHPs and
Governance
Executive Lead - Responsible for this policy - Ensure the Trust’s discharge and transfer of care is managed appropriately and has lead responsibility for the
implementation of this policy - Ensure a systematic and consistent approach to the practice of discharge and transfer of care within service areas
- Identify and implement strategies for any risks in relation to the standards of clinical handover
Chief Executive Accountable - Ensure that this policy is implemented within the Trust. Operational responsibility has been delegated
8.0 Training
What aspect(s) of this policy will
require staff training?
Which staff groups require this
training?
Is this training covered in the Trust’s Mandatory and Risk
Management Training Needs Analysis document?
If no, how will the training be delivered?
Who will deliver the training?
How often will staff require
training
Who will ensure and monitor that staff have
this training?
Discharge and Transfer of Care
Clinical Staff No, staff will receive specific training in relation to this
policy where it is identified in
their individual training needs analysis as part of their
development for their particular role and
responsibilities
Internally Managers As and when required
Group Quality and Safety Groups
9.0 Equality Impact Assessment
Black Country Partnership NHS Foundation Trust is committed to ensuring that the way we provide services and the way we recruit and treat staff reflects individual needs, promotes equality and does not discriminate unfairly against any particular individual or group. The Equality Impact Assessment for this policy has been completed and is readily available on the Intranet. If you require this in a different format e.g. larger print, Braille, different languages or audio tape, please contact the Equality & Diversity Team on Ext. 8067 or email [email protected]
10.0 Data Protection and Freedom of Information Data Protection Act provides controls for the way information is handled and to gives legal rights to individuals in relation to the use of their data. It sets out strict rules for people who use or store data about individuals and gives rights to those people whose data has been collected. The law applies to all personal data held including electronic and manual records. The Information Commissioner’s Office has powers to enforce the Data Protection Act and can do this through the use of compulsory audits, warrants, notices and monetary penalties which can be up to €20million or 4% of the Trusts annual turnover for serious breaches of the Data Protection Act. In addition to this the Information Commissioner can limit or stop data processing activities where there has been a serious breach of the Act and there remains a risk to the data.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
21
The Freedom of Information Act provides public access to information held by public authorities. The main principle behind freedom of information legislation is that people have a right to know about the activities of public authorities, unless there is a good reason for them not to. The Freedom of Information Act applies to corporate data and personal data generally cannot be released under this Act. All staffs have a responsibility to ensure that they do not disclose information about the Trust’s activities; this includes information about service users in its care, staff members and corporate documentation to unauthorised individuals. This responsibility applies whether you are currently employed or after your employment ends and in certain aspects of your personal life e.g. use of social networking sites etc. The Trust seeks to ensure a high level of transparency in all its business activities but reserves the right not to disclose information where relevant legislation applies. The Information Governance Team provides a central point for release of information under Data Protection and Freedom of Information following formal requests for information; any queries about the disclosure of information can be forwarded to the Information Governance Team.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
22
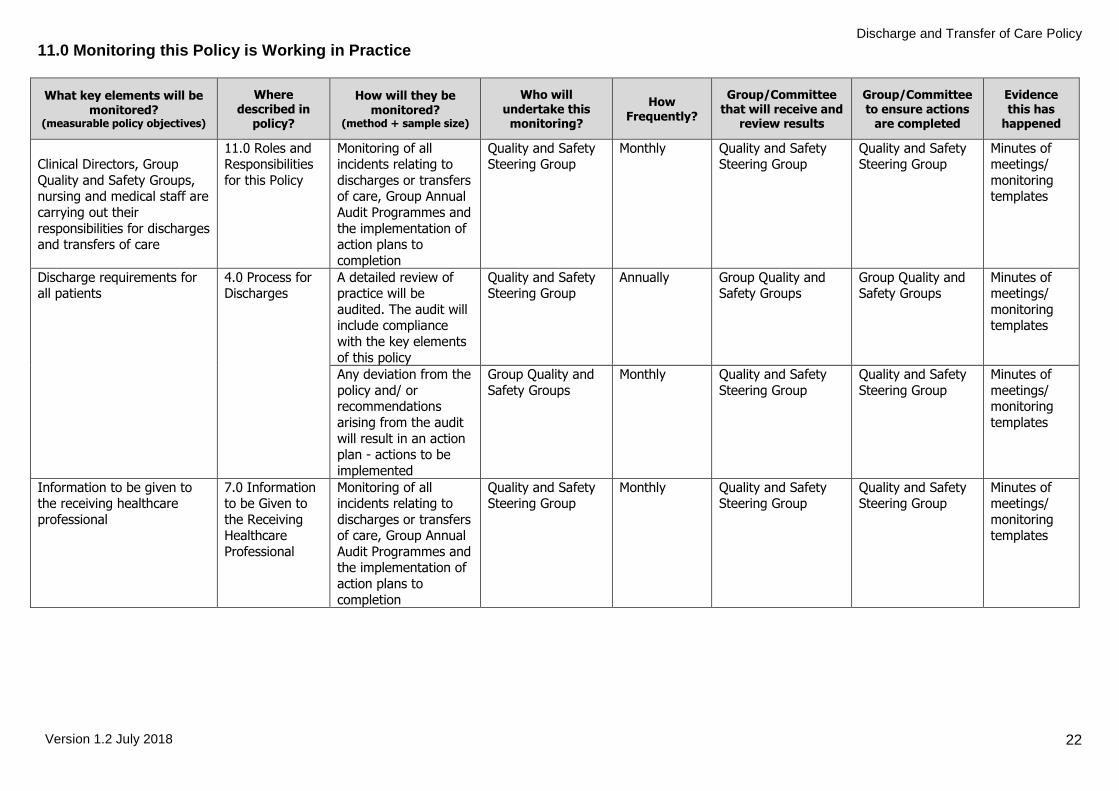
11.0 Monitoring this Policy is Working in Practice
What key elements will be monitored?
(measurable policy objectives)
Where described in
policy?
How will they be monitored?
(method + sample size)
Who will undertake this
monitoring?
How Frequently?
Group/Committee that will receive and
review results
Group/Committee to ensure actions
are completed
Evidence this has
happened
Clinical Directors, Group
Quality and Safety Groups, nursing and medical staff are
carrying out their
responsibilities for discharges and transfers of care
11.0 Roles and Responsibilities
for this Policy
Monitoring of all incidents relating to
discharges or transfers of care, Group Annual
Audit Programmes and
the implementation of action plans to
completion
Quality and Safety Steering Group
Monthly Quality and Safety Steering Group
Quality and Safety Steering Group
Minutes of meetings/
monitoring templates
Discharge requirements for all patients
4.0 Process for Discharges
A detailed review of practice will be
audited. The audit will include compliance
with the key elements
of this policy
Quality and Safety Steering Group
Annually Group Quality and Safety Groups
Group Quality and Safety Groups
Minutes of meetings/
monitoring templates
Any deviation from the
policy and/ or recommendations
arising from the audit
will result in an action plan - actions to be
implemented
Group Quality and
Safety Groups
Monthly Quality and Safety
Steering Group
Quality and Safety
Steering Group
Minutes of
meetings/ monitoring
templates
Information to be given to the receiving healthcare
professional
7.0 Information to be Given to
the Receiving Healthcare
Professional
Monitoring of all incidents relating to
discharges or transfers of care, Group Annual
Audit Programmes and the implementation of
action plans to
completion
Quality and Safety Steering Group
Monthly Quality and Safety Steering Group
Quality and Safety Steering Group
Minutes of meetings/
monitoring templates
Discharge and Transfer of Care Policy
Version 1.2 July 2018
23
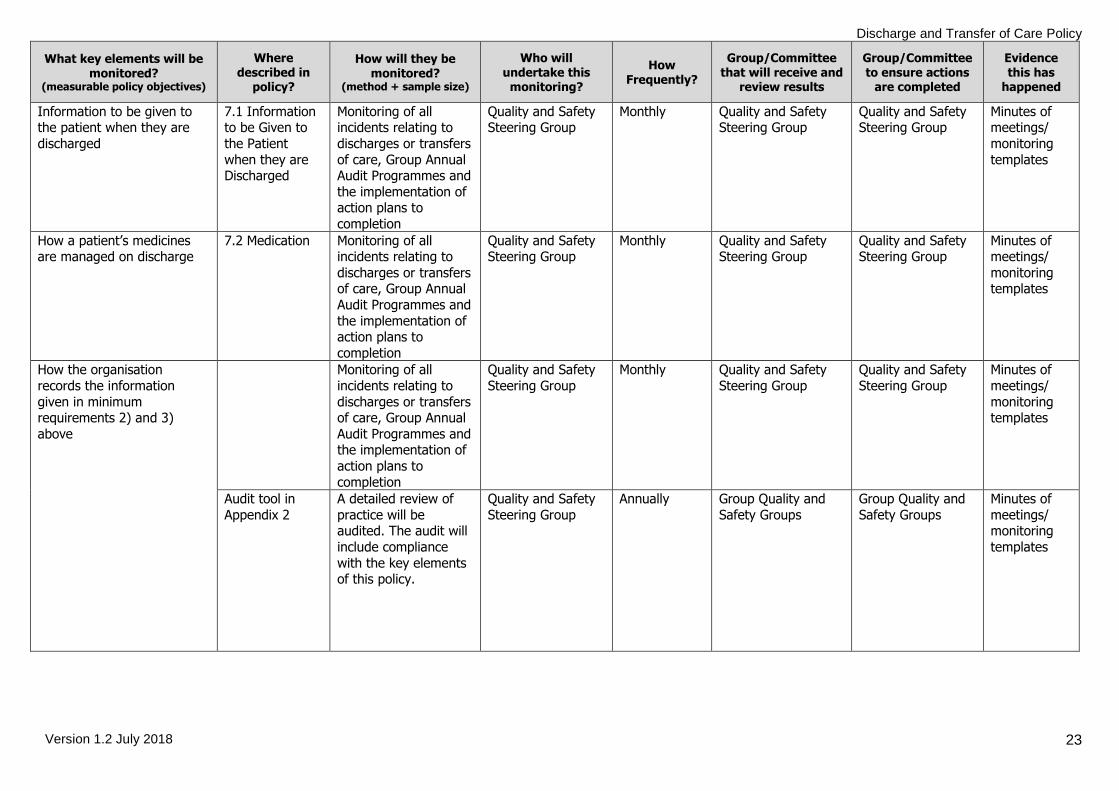
What key elements will be monitored?
(measurable policy objectives)
Where described in
policy?
How will they be monitored?
(method + sample size)
Who will undertake this
monitoring?
How Frequently?
Group/Committee that will receive and
review results
Group/Committee to ensure actions
are completed
Evidence this has
happened
Information to be given to the patient when they are
discharged
7.1 Information to be Given to
the Patient
when they are Discharged
Monitoring of all incidents relating to
discharges or transfers
of care, Group Annual Audit Programmes and
the implementation of action plans to
completion
Quality and Safety Steering Group
Monthly Quality and Safety Steering Group
Quality and Safety Steering Group
Minutes of meetings/
monitoring
templates
How a patient’s medicines are managed on discharge
7.2 Medication Monitoring of all incidents relating to
discharges or transfers of care, Group Annual
Audit Programmes and
the implementation of action plans to
completion
Quality and Safety Steering Group
Monthly Quality and Safety Steering Group
Quality and Safety Steering Group
Minutes of meetings/
monitoring templates
How the organisation
records the information
given in minimum requirements 2) and 3)
above
Monitoring of all
incidents relating to
discharges or transfers of care, Group Annual
Audit Programmes and the implementation of
action plans to
completion
Quality and Safety
Steering Group
Monthly Quality and Safety
Steering Group
Quality and Safety
Steering Group
Minutes of
meetings/
monitoring templates
Audit tool in
Appendix 2
A detailed review of
practice will be audited. The audit will
include compliance
with the key elements of this policy.
Quality and Safety
Steering Group
Annually Group Quality and
Safety Groups
Group Quality and
Safety Groups
Minutes of
meetings/ monitoring
templates
Discharge and Transfer of Care Policy
Version 1.2 July 2018
24
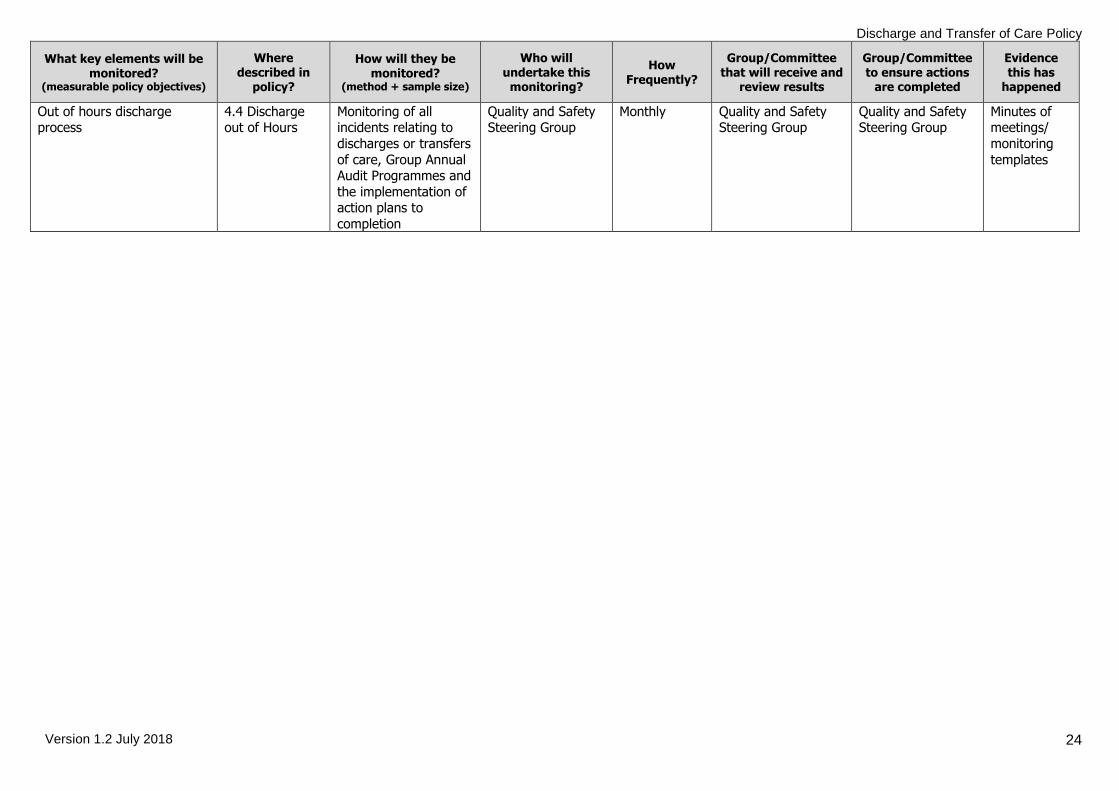
What key elements will be monitored?
(measurable policy objectives)
Where described in
policy?
How will they be monitored?
(method + sample size)
Who will undertake this
monitoring?
How Frequently?
Group/Committee that will receive and
review results
Group/Committee to ensure actions
are completed
Evidence this has
happened
Out of hours discharge process
4.4 Discharge out of Hours
Monitoring of all incidents relating to
discharges or transfers
of care, Group Annual Audit Programmes and
the implementation of action plans to
completion
Quality and Safety Steering Group
Monthly Quality and Safety Steering Group
Quality and Safety Steering Group
Minutes of meetings/
monitoring
templates
Discharge and Transfer of Care Policy
Version 1.2 July 2018
25
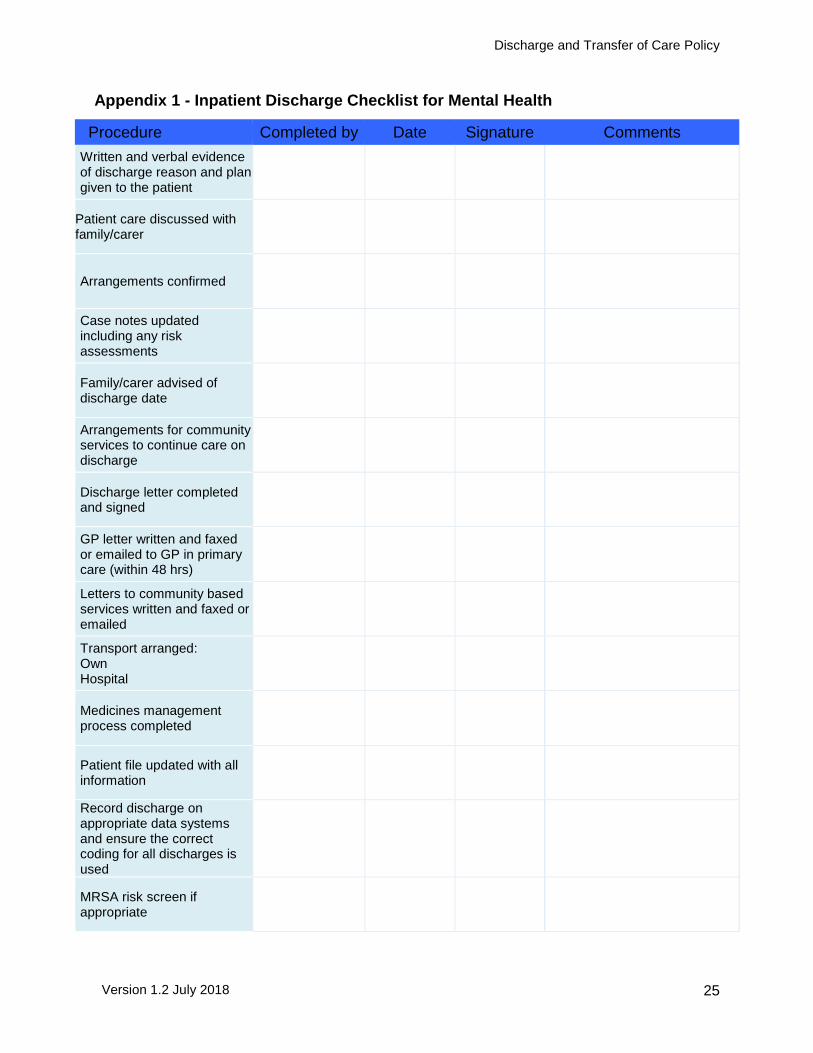
Appendix 1 - Inpatient Discharge Checklist for Mental Health
Procedure Completed by Date Signature Comments
Written and verbal evidence of discharge reason and plan given to the patient
Patient care discussed with family/carer
Arrangements confirmed
Case notes updated including any risk assessments
Family/carer advised of discharge date
Arrangements for community services to continue care on discharge
Discharge letter completed and signed
GP letter written and faxed or emailed to GP in primary care (within 48 hrs)
Letters to community based services written and faxed or emailed
Transport arranged: Own Hospital
Medicines management process completed
Patient file updated with all information
Record discharge on appropriate data systems and ensure the correct coding for all discharges is used
MRSA risk screen if appropriate
Discharge and Transfer of Care Policy
Version 1.2 July 2018
26
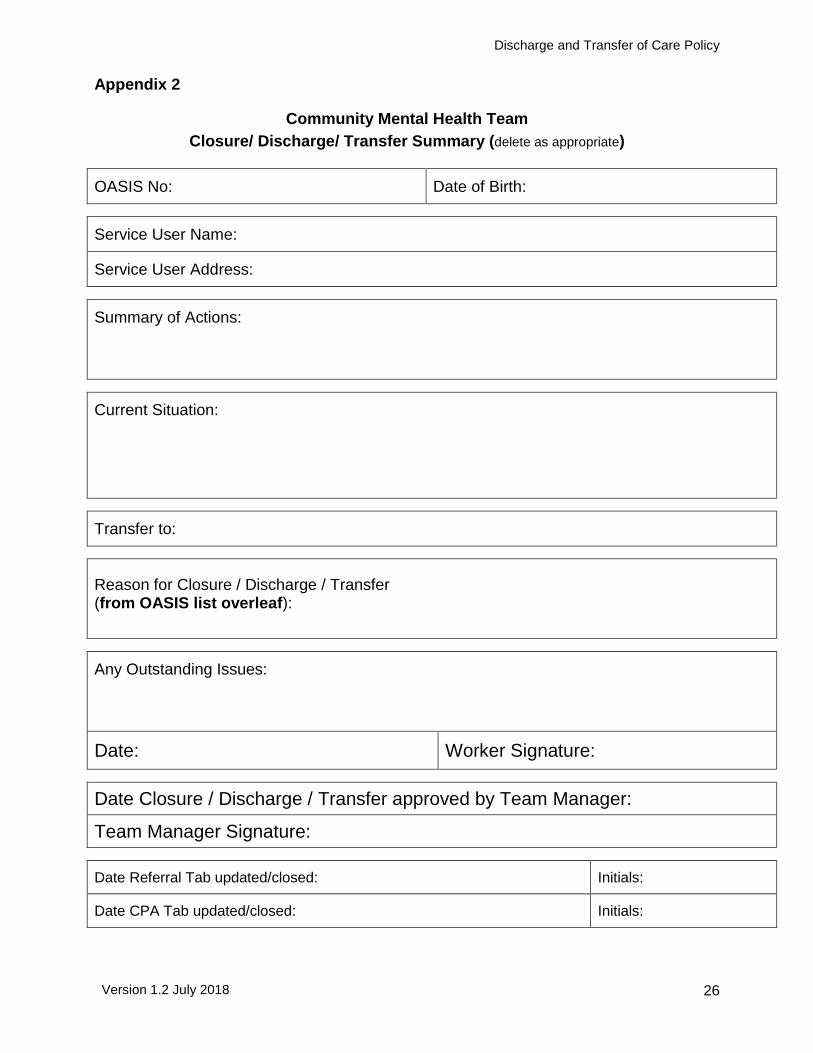
Appendix 2
Community Mental Health Team
Closure/ Discharge/ Transfer Summary (delete as appropriate)
OASIS No: Date of Birth:
Service User Name:
Service User Address:
Summary of Actions:
Current Situation:
Transfer to:
Reason for Closure / Discharge / Transfer (from OASIS list overleaf):
Any Outstanding Issues:
Date: Worker Signature:
Date Closure / Discharge / Transfer approved by Team Manager:
Team Manager Signature:
Date Referral Tab updated/closed: Initials:
Date CPA Tab updated/closed: Initials:
Discharge and Transfer of Care Policy
Version 1.2 July 2018
27
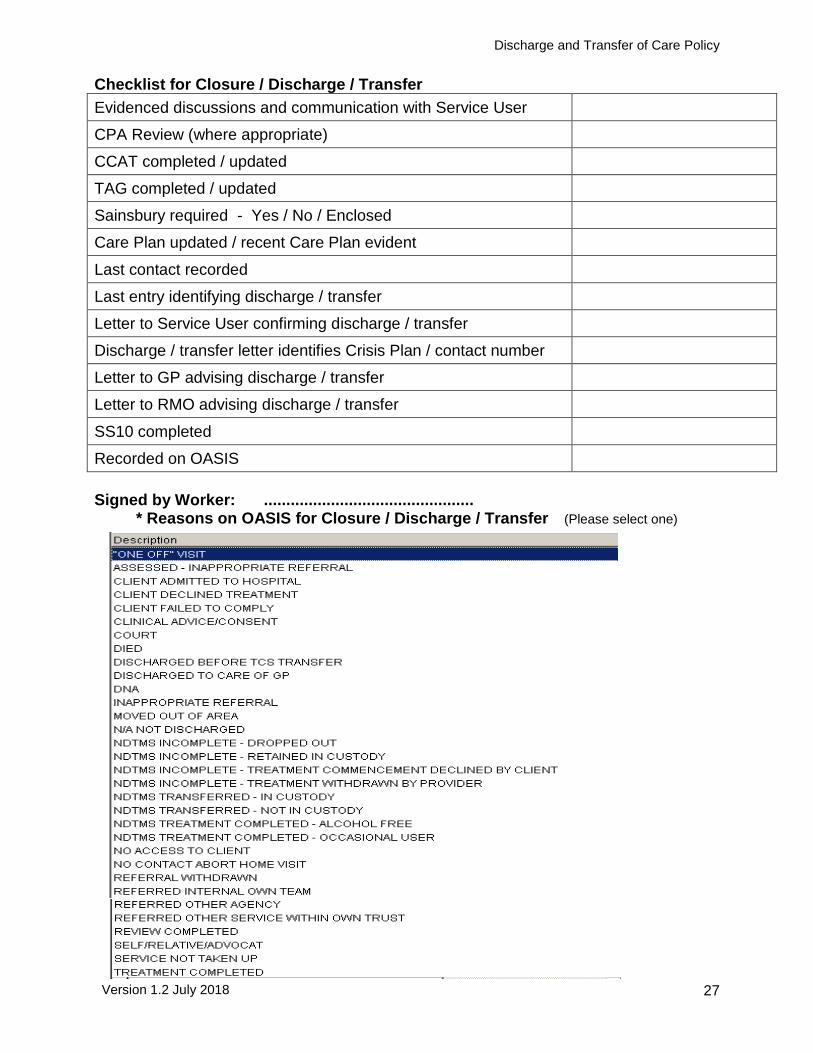
Checklist for Closure / Discharge / Transfer
Evidenced discussions and communication with Service User
CPA Review (where appropriate)
CCAT completed / updated
TAG completed / updated
Sainsbury required - Yes / No / Enclosed
Care Plan updated / recent Care Plan evident
Last contact recorded
Last entry identifying discharge / transfer
Letter to Service User confirming discharge / transfer
Discharge / transfer letter identifies Crisis Plan / contact number
Letter to GP advising discharge / transfer
Letter to RMO advising discharge / transfer
SS10 completed
Recorded on OASIS
Signed by Worker: ...............................................
* Reasons on OASIS for Closure / Discharge / Transfer (Please select one)
Discharge and Transfer of Care Policy
Version 1.2 July 2018
28
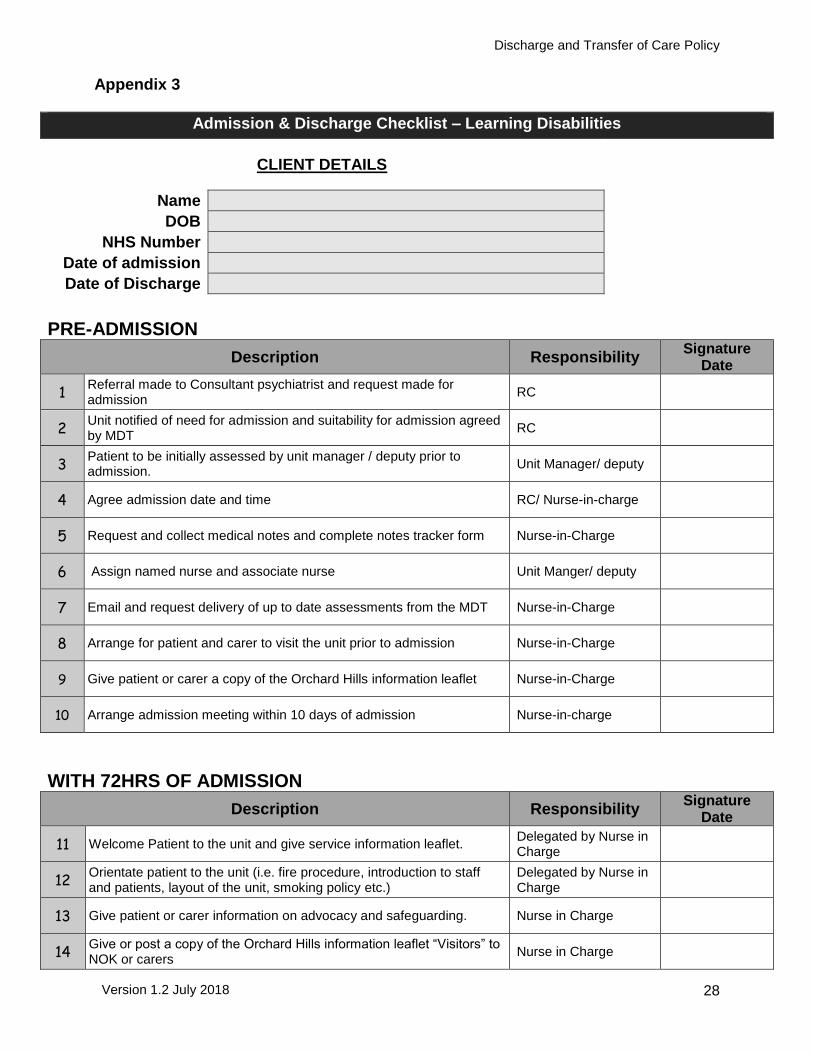
Appendix 3
Admission & Discharge Checklist – Learning Disabilities
CLIENT DETAILS
Name
DOB
NHS Number
Date of admission
Date of Discharge
PRE-ADMISSION
Description Responsibility Signature
Date
1 Referral made to Consultant psychiatrist and request made for admission
RC
2 Unit notified of need for admission and suitability for admission agreed by MDT
RC
3 Patient to be initially assessed by unit manager / deputy prior to admission.
Unit Manager/ deputy
4 Agree admission date and time RC/ Nurse-in-charge
5 Request and collect medical notes and complete notes tracker form Nurse-in-Charge
6 Assign named nurse and associate nurse Unit Manger/ deputy
7 Email and request delivery of up to date assessments from the MDT Nurse-in-Charge
8 Arrange for patient and carer to visit the unit prior to admission Nurse-in-Charge
9 Give patient or carer a copy of the Orchard Hills information leaflet Nurse-in-Charge
10 Arrange admission meeting within 10 days of admission Nurse-in-charge
WITH 72HRS OF ADMISSION
Description Responsibility Signature
Date
11 Welcome Patient to the unit and give service information leaflet. Delegated by Nurse in Charge
12 Orientate patient to the unit (i.e. fire procedure, introduction to staff and patients, layout of the unit, smoking policy etc.)
Delegated by Nurse in Charge
13 Give patient or carer information on advocacy and safeguarding. Nurse in Charge
14 Give or post a copy of the Orchard Hills information leaflet “Visitors” to NOK or carers
Nurse in Charge
Discharge and Transfer of Care Policy
Version 1.2 July 2018
29
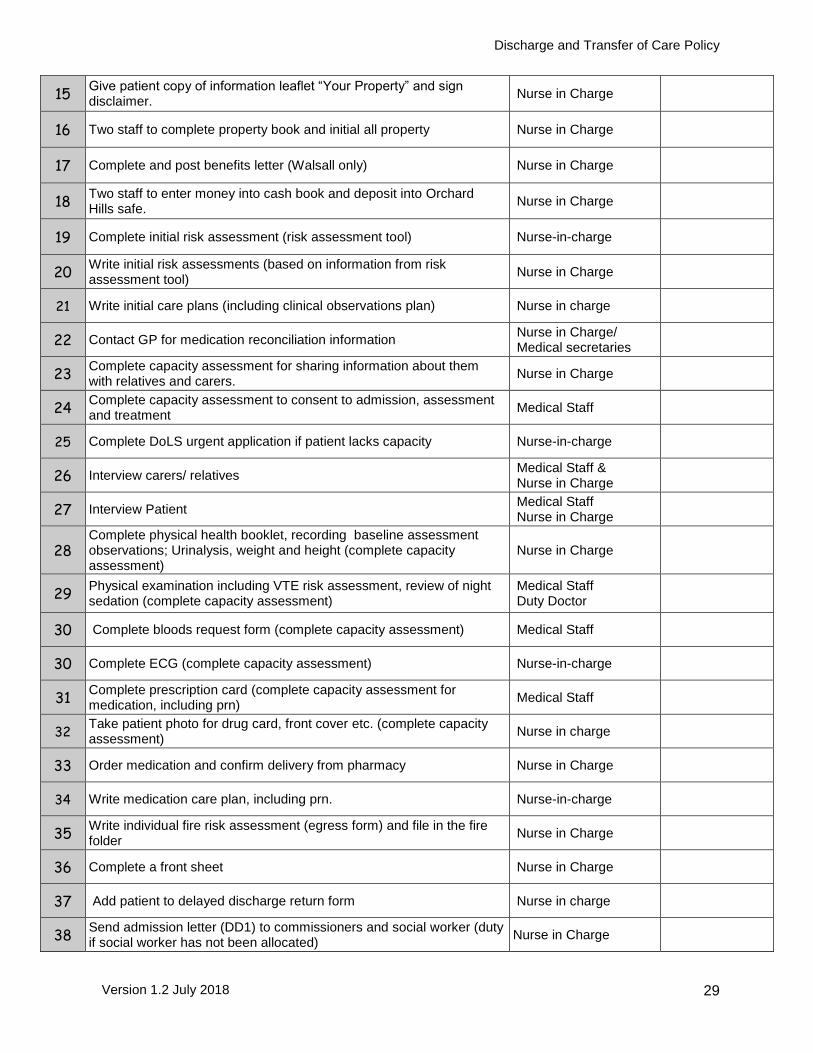
15 Give patient copy of information leaflet “Your Property” and sign disclaimer.
Nurse in Charge
16 Two staff to complete property book and initial all property Nurse in Charge
17 Complete and post benefits letter (Walsall only) Nurse in Charge
18 Two staff to enter money into cash book and deposit into Orchard Hills safe.
Nurse in Charge
19 Complete initial risk assessment (risk assessment tool) Nurse-in-charge
20 Write initial risk assessments (based on information from risk assessment tool)
Nurse in Charge
21 Write initial care plans (including clinical observations plan) Nurse in charge
22 Contact GP for medication reconciliation information Nurse in Charge/ Medical secretaries
23 Complete capacity assessment for sharing information about them with relatives and carers.
Nurse in Charge
24 Complete capacity assessment to consent to admission, assessment and treatment
Medical Staff
25 Complete DoLS urgent application if patient lacks capacity Nurse-in-charge
26 Interview carers/ relatives Medical Staff & Nurse in Charge
27 Interview Patient Medical Staff Nurse in Charge
28 Complete physical health booklet, recording baseline assessment observations; Urinalysis, weight and height (complete capacity assessment)
Nurse in Charge
29 Physical examination including VTE risk assessment, review of night sedation (complete capacity assessment)
Medical Staff Duty Doctor
30 Complete bloods request form (complete capacity assessment) Medical Staff
30 Complete ECG (complete capacity assessment) Nurse-in-charge
31 Complete prescription card (complete capacity assessment for medication, including prn)
Medical Staff
32 Take patient photo for drug card, front cover etc. (complete capacity assessment)
Nurse in charge
33 Order medication and confirm delivery from pharmacy Nurse in Charge
34 Write medication care plan, including prn. Nurse-in-charge
35 Write individual fire risk assessment (egress form) and file in the fire folder
Nurse in Charge
36 Complete a front sheet Nurse in Charge
37 Add patient to delayed discharge return form Nurse in charge
38 Send admission letter (DD1) to commissioners and social worker (duty if social worker has not been allocated)
Nurse in Charge
Discharge and Transfer of Care Policy
Version 1.2 July 2018
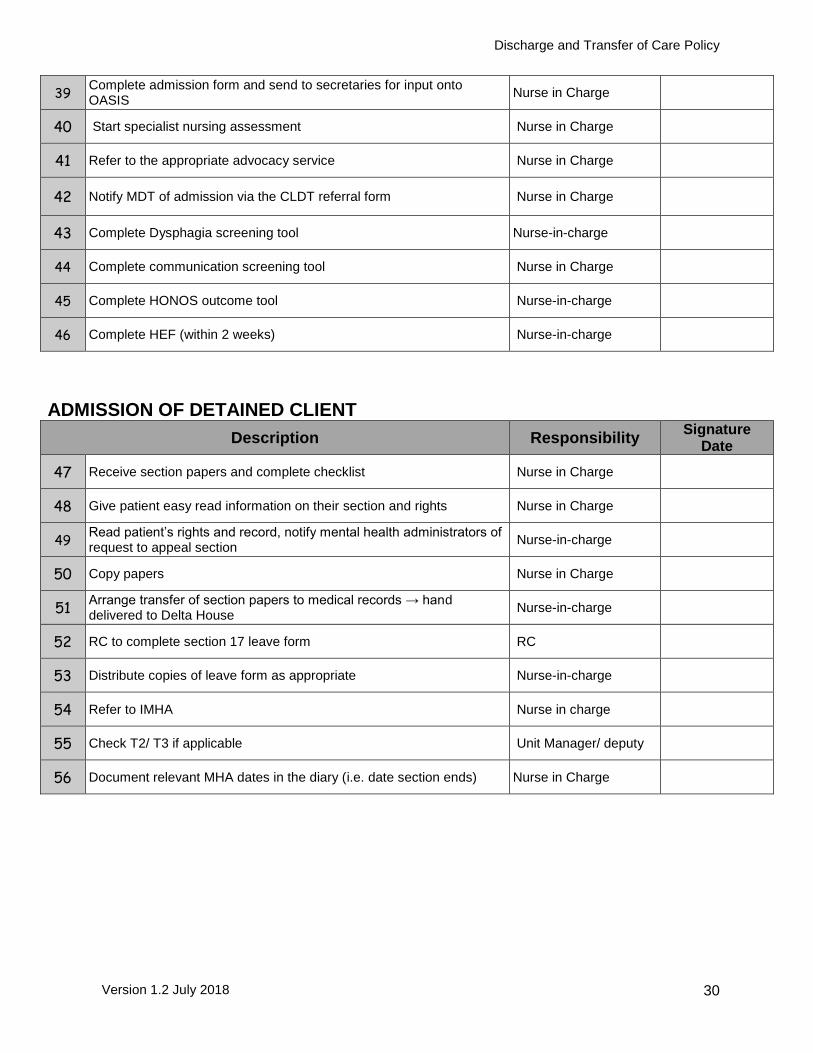
30
39 Complete admission form and send to secretaries for input onto OASIS
Nurse in Charge
40 Start specialist nursing assessment Nurse in Charge
41 Refer to the appropriate advocacy service Nurse in Charge
42 Notify MDT of admission via the CLDT referral form Nurse in Charge
43 Complete Dysphagia screening tool Nurse-in-charge
44 Complete communication screening tool Nurse in Charge
45 Complete HONOS outcome tool Nurse-in-charge
46 Complete HEF (within 2 weeks) Nurse-in-charge
ADMISSION OF DETAINED CLIENT
Description Responsibility Signature
Date
47 Receive section papers and complete checklist Nurse in Charge
48 Give patient easy read information on their section and rights Nurse in Charge
49 Read patient’s rights and record, notify mental health administrators of request to appeal section
Nurse-in-charge
50 Copy papers Nurse in Charge
51 Arrange transfer of section papers to medical records → hand delivered to Delta House
Nurse-in-charge
52 RC to complete section 17 leave form RC
53 Distribute copies of leave form as appropriate Nurse-in-charge
54 Refer to IMHA Nurse in charge
55 Check T2/ T3 if applicable Unit Manager/ deputy
56 Document relevant MHA dates in the diary (i.e. date section ends) Nurse in Charge
Discharge and Transfer of Care Policy
Version 1.2 July 2018
31
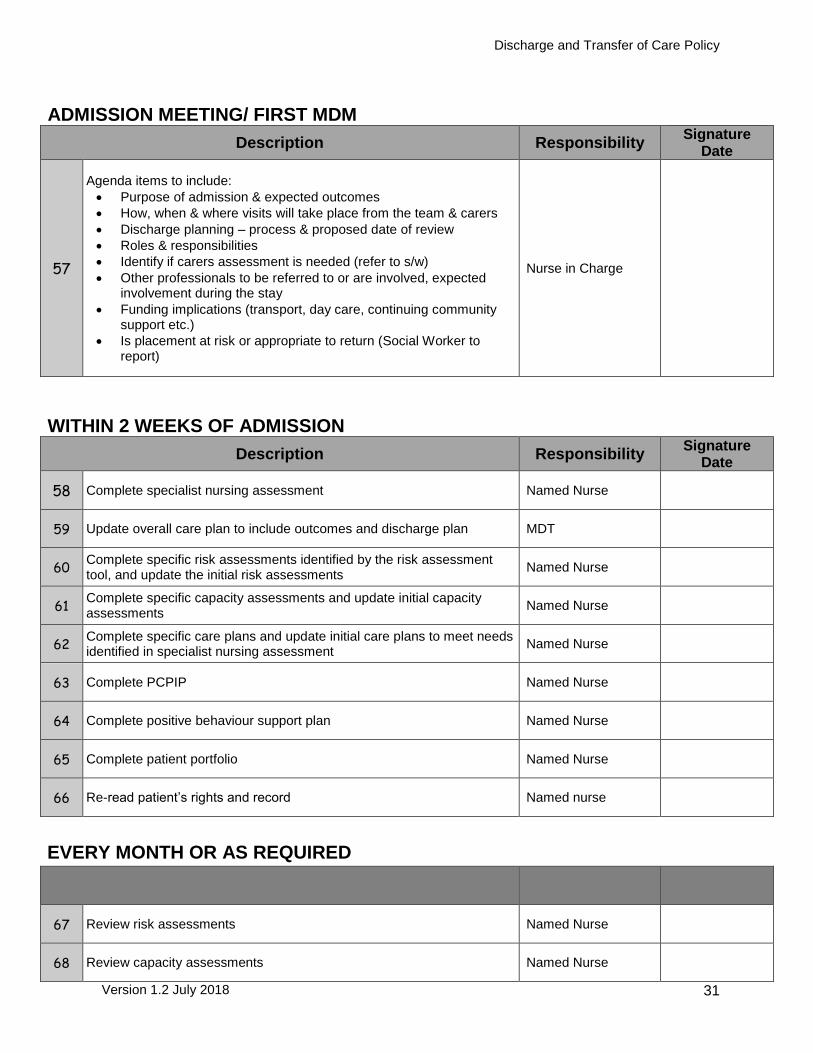
ADMISSION MEETING/ FIRST MDM
Description Responsibility Signature
Date
57
Agenda items to include:
Purpose of admission & expected outcomes
How, when & where visits will take place from the team & carers
Discharge planning – process & proposed date of review
Roles & responsibilities
Identify if carers assessment is needed (refer to s/w)
Other professionals to be referred to or are involved, expected involvement during the stay
Funding implications (transport, day care, continuing community support etc.)
Is placement at risk or appropriate to return (Social Worker to report)
Nurse in Charge
WITHIN 2 WEEKS OF ADMISSION
Description Responsibility Signature
Date
58 Complete specialist nursing assessment Named Nurse
59 Update overall care plan to include outcomes and discharge plan MDT
60 Complete specific risk assessments identified by the risk assessment tool, and update the initial risk assessments
Named Nurse
61 Complete specific capacity assessments and update initial capacity assessments
Named Nurse
62 Complete specific care plans and update initial care plans to meet needs identified in specialist nursing assessment
Named Nurse
63 Complete PCPIP Named Nurse
64 Complete positive behaviour support plan Named Nurse
65 Complete patient portfolio Named Nurse
66 Re-read patient’s rights and record Named nurse
EVERY MONTH OR AS REQUIRED
67 Review risk assessments Named Nurse
68 Review capacity assessments Named Nurse
Discharge and Transfer of Care Policy
Version 1.2 July 2018
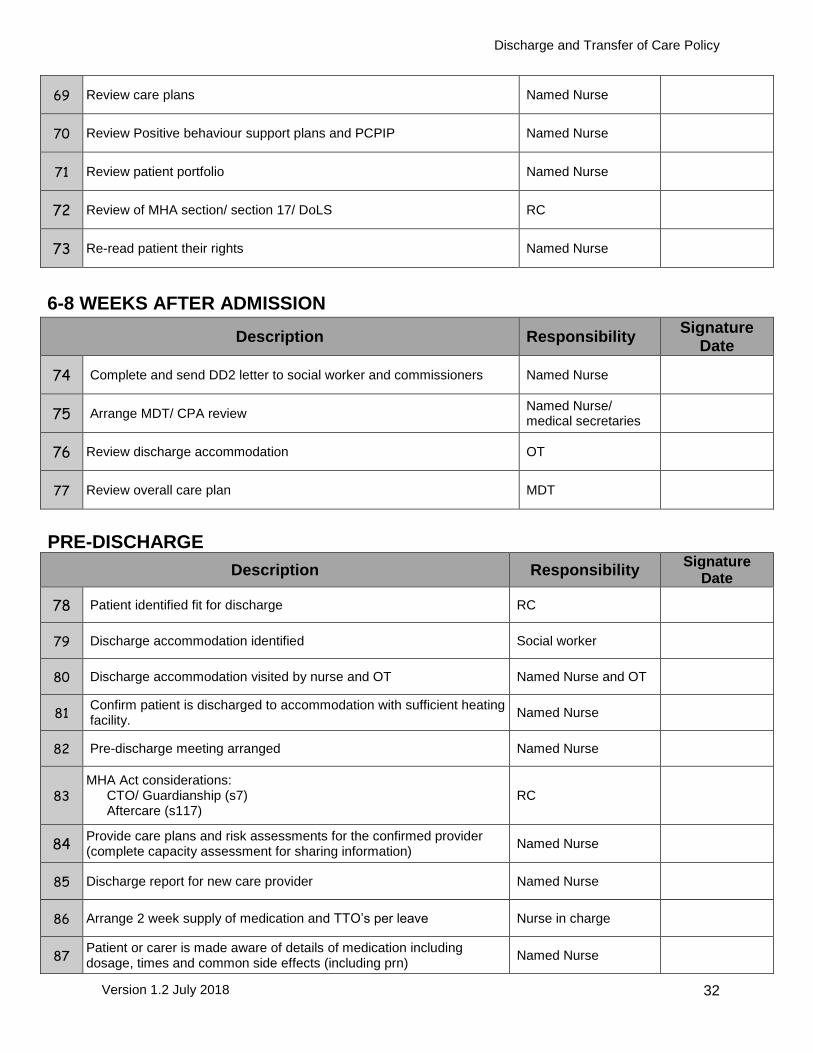
32
69 Review care plans Named Nurse
70 Review Positive behaviour support plans and PCPIP Named Nurse
71 Review patient portfolio Named Nurse
72 Review of MHA section/ section 17/ DoLS RC
73 Re-read patient their rights Named Nurse
6-8 WEEKS AFTER ADMISSION
Description Responsibility Signature
Date
74 Complete and send DD2 letter to social worker and commissioners Named Nurse
75 Arrange MDT/ CPA review Named Nurse/ medical secretaries
76 Review discharge accommodation OT
77 Review overall care plan MDT
PRE-DISCHARGE
Description Responsibility Signature
Date
78 Patient identified fit for discharge RC
79 Discharge accommodation identified Social worker
80 Discharge accommodation visited by nurse and OT Named Nurse and OT
81 Confirm patient is discharged to accommodation with sufficient heating facility.
Named Nurse
82 Pre-discharge meeting arranged Named Nurse
83 MHA Act considerations: CTO/ Guardianship (s7) Aftercare (s117)
RC
84 Provide care plans and risk assessments for the confirmed provider (complete capacity assessment for sharing information)
Named Nurse
85 Discharge report for new care provider Named Nurse
86 Arrange 2 week supply of medication and TTO’s per leave Nurse in charge
87 Patient or carer is made aware of details of medication including dosage, times and common side effects (including prn)
Named Nurse
Discharge and Transfer of Care Policy
Version 1.2 July 2018
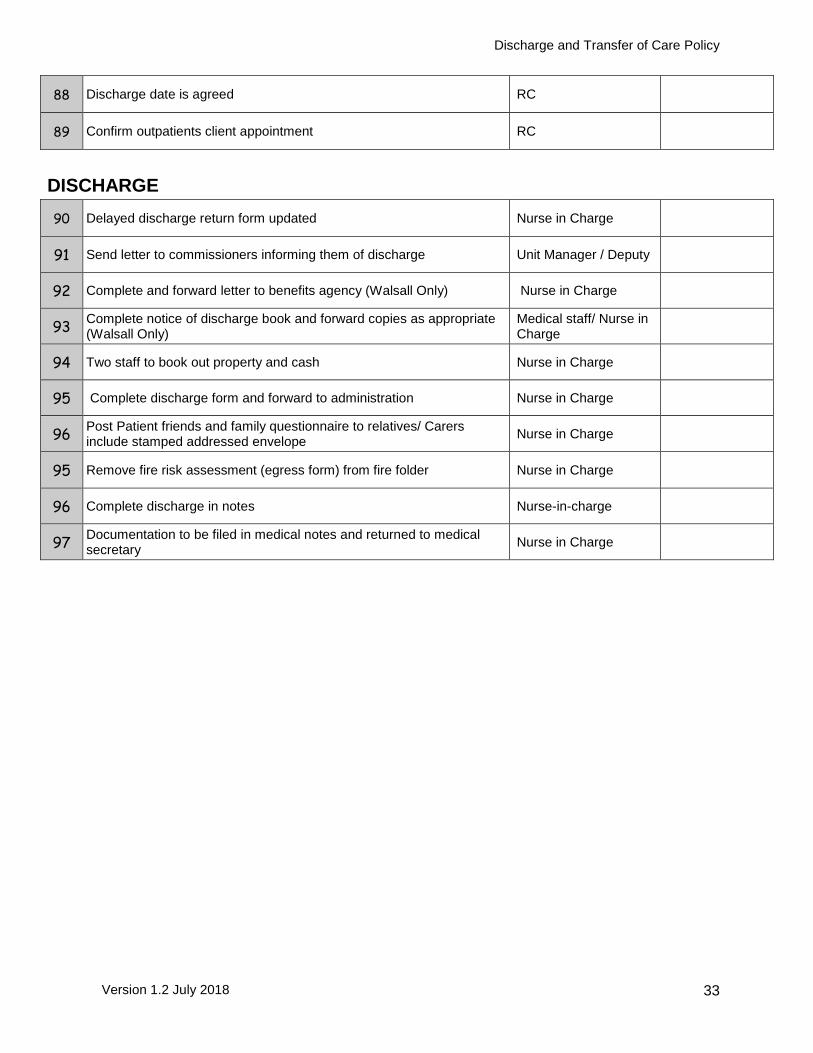
33
88 Discharge date is agreed RC
89 Confirm outpatients client appointment RC
DISCHARGE
90 Delayed discharge return form updated Nurse in Charge
91 Send letter to commissioners informing them of discharge Unit Manager / Deputy
92 Complete and forward letter to benefits agency (Walsall Only) Nurse in Charge
93 Complete notice of discharge book and forward copies as appropriate (Walsall Only)
Medical staff/ Nurse in Charge
94 Two staff to book out property and cash Nurse in Charge
95 Complete discharge form and forward to administration Nurse in Charge
96 Post Patient friends and family questionnaire to relatives/ Carers include stamped addressed envelope
Nurse in Charge
95 Remove fire risk assessment (egress form) from fire folder Nurse in Charge
96 Complete discharge in notes Nurse-in-charge
97 Documentation to be filed in medical notes and returned to medical secretary
Nurse in Charge
Discharge and Transfer of Care Policy
Version 1.2 July 2018
34
Appendix 4
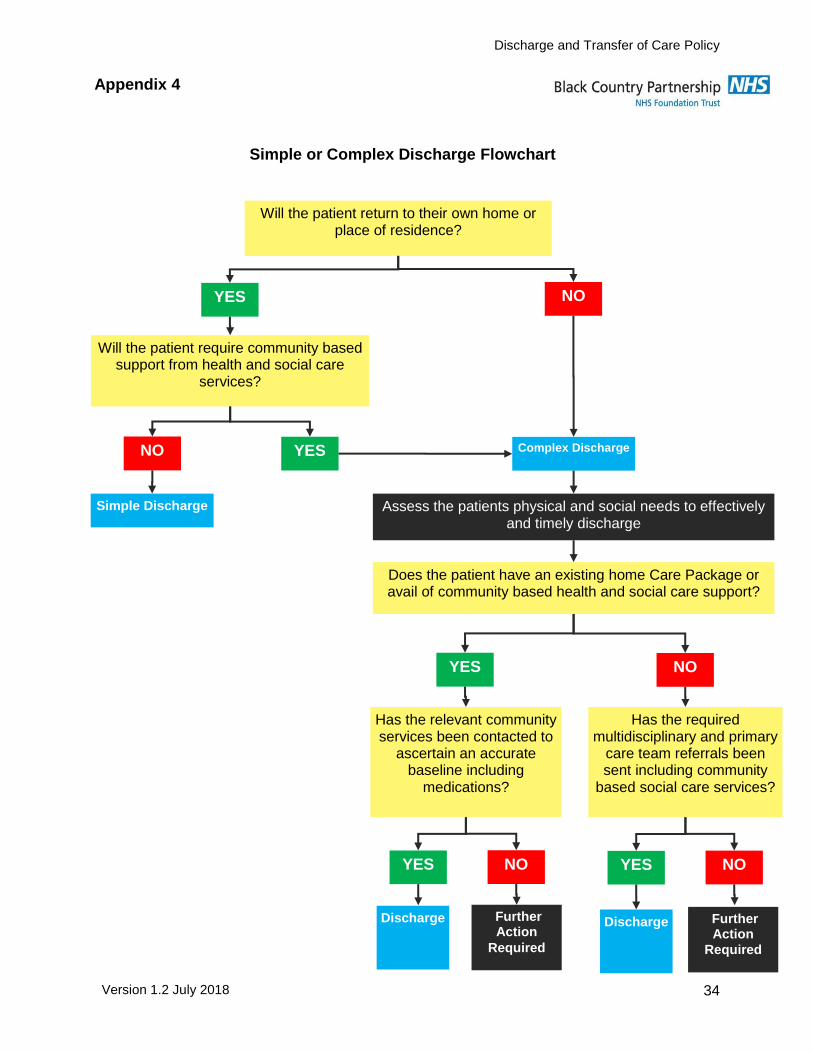
Simple or Complex Discharge Flowchart
Will the patient return to their own home or place of residence?
YES NO
Will the patient require community based support from health and social care
services?
YES NO
Simple Discharge
Complex Discharge
Assess the patients physical and social needs to effectively and timely discharge
Does the patient have an existing home Care Package or avail of community based health and social care support?
NO YES
Has the relevant community services been contacted to
ascertain an accurate baseline including
medications?
YES NO
Further Action
Required
Has the required multidisciplinary and primary
care team referrals been sent including community
based social care services?
YES NO
Further Action
Required
Discharge Discharge
Discharge and Transfer of Care Policy
Version 1.2 July 2018
35
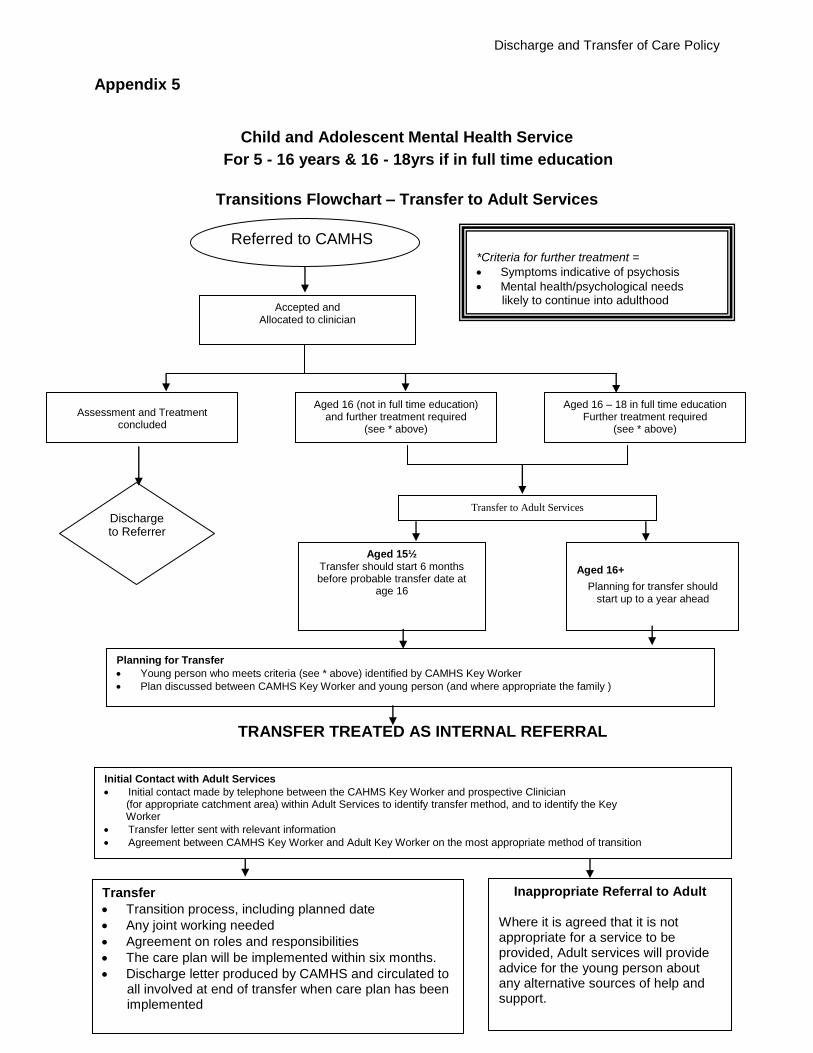
Appendix 5
Child and Adolescent Mental Health Service
For 5 - 16 years & 16 - 18yrs if in full time education
Transitions Flowchart – Transfer to Adult Services
TRANSFER TREATED AS INTERNAL REFERRAL
Accepted and Allocated to clinician
Referred to CAMHS
Assessment and Treatment concluded
Discharge to Referrer
Aged 16 (not in full time education) and further treatment required
(see * above)
Aged 16 – 18 in full time education Further treatment required
(see * above)
Aged 15½ Transfer should start 6 months before probable transfer date at
age 16
Aged 16+
Planning for transfer should start up to a year ahead
Planning for Transfer
Young person who meets criteria (see * above) identified by CAMHS Key Worker
Plan discussed between CAMHS Key Worker and young person (and where appropriate the family )
Transfer
Transition process, including planned date
Any joint working needed
Agreement on roles and responsibilities
The care plan will be implemented within six months.
Discharge letter produced by CAMHS and circulated to all involved at end of transfer when care plan has been implemented
*Criteria for further treatment =
Symptoms indicative of psychosis
Mental health/psychological needs likely to continue into adulthood
Enduring mental health problems
Transfer to Adult Services
Initial Contact with Adult Services
Initial contact made by telephone between the CAHMS Key Worker and prospective Clinician (for appropriate catchment area) within Adult Services to identify transfer method, and to identify the Key Worker
Transfer letter sent with relevant information
Agreement between CAMHS Key Worker and Adult Key Worker on the most appropriate method of transition
Inappropriate Referral to Adult
Where it is agreed that it is not appropriate for a service to be provided, Adult services will provide advice for the young person about any alternative sources of help and support.

Discharge and Transfer of Care Policy
Version 1.2 July 2018
36
Child and Adolescent Mental Health Service For 5 - 16 years & 16 - 18yrs if in full time education
Transitions Flowchart – Transfer to Learning Disabilities
TRANSFER TREATED AS INTERNAL REFERRAL
Accepted and Allocated to clinician
Referred to CAMHS
Assessment and Treatment concluded
Discharge to Referrer
Aged 16 (not in full time education) and further treatment required
(see * above)
Aged 16 – 18 in full time education Further treatment required
(see * above)
Aged 15½
Transfer should start 6 months before probable transfer date at
age 16
Aged 16+
Planning for transfer should
start up to a year ahead
Planning for Transfer
Young person who meets criteria (see * above) identified by CAMHS Key Worker
Plan discussed between CAMHS Key Worker and young person (and where appropriate the family )
Transfer Transition process, including planned date
Any joint working needed
Agreement on roles and responsibilities
The care plan will be implemented within six months.
Discharge letter produced by CAMHS and circulated to all involved at end of transfer when care plan has been implemented
*Criteria for further treatment =
Symptoms indicative of psychosis
Mental health/psychological needs likely to continue into adulthood
Enduring mental health problems
Transfer to Learning Disabilities
Initial Contact with Learning Disabilities
Initial contact made by telephone between the CAHMS Key Worker and prospective Clinician (for appropriate catchment area) within Learning Disabilities to identify transfer method, and to identify the Key Worker.
Transfer letter sent with relevant information
Agreement between CAMHS Key Worker and Learning Disabilities Key Worker on the most appropriate method of transition
Inappropriate Referral to Learning
Disabilities
Where it is agreed that it is not appropriate for a service to be provided, Learning Disabilities will provide advice
for the young person about any alternative sources of help and support
Discharge and Transfer of Care Policy
Version 1.2 July 2018
37
Appendix 6 - Assess and Score Patient either on Admission or if there is a Change in Patient’s Risk Factor or Location
Score 5 or less –Low Risk Does not need nursing in isolation or screening
Score 6 or 7 = Medium Risk Isolate patient, consider MRSA screen if required Contact infection control for advice
Score 8 or above = HIGH RISK Nurse patient in isolation, consider MRSA screen
Contact infection control for advice Using the scores indicated enter the sore against each section, e.g. past history of MRSA = 6, patient a healthcare worker = 1 etc. – if there is no risk score 0. Once each section is scored add number to give the total. No risk factors = score 0
Sc
ore
1
st
Assessment
2
nd
Assessment
3
rd
Assessment
4
th
Assessment
Please enter the date of Assessments, the ward and if applicable the sites swabbed
RISK FACTORS: 1st Assessment
Date of Assessment Ward: Site swabbed: Nurse Sign:
Past history of MRSA 6
Has the patient been in contact with a known or suspected case of MRSA?
3
Has the patient recently developed a productive cough?
6
Has the patient any history of TB, recent contact with TB or symptoms of TB? (cough, weight loss, night sweats)
8
Does the patient have an open wound, recurrent/non-healing skin condition or burns?
2 2nd Assessment
Date of Assessment Ward: Site swabbed: Nurse Sign:
Is the patient a healthcare worker? 1
Has the patient any history of diarrhea within the past 48 hours?
6
Is the patient on antibiotics or has received antibiotics within the past 4 weeks?
1
Has the patient any history of other multi-resistant organisms e.g. Acinetobacter, Clostridium difficile, ESBL's, VRE etc.
6 3rd Assessment
Date of Assessment Ward: Site swabbed: Nurse Sign:
Has the patient been in contact with any infectious diseases prior to admission (within the past 7 days)?
6
Does the patient have an indwelling medical device e.g. urinary catheter, IV device or feeding tube etc?
3
Score 5 or less –Low Risk
Does not need nursing in isolation or screening
Score 6 or 7 = Medium Risk Screen for MRSA and preferably isolate patient Contact infection control for advice
Score 8 or above = HIGH RISK Nurse patient in isolation and screen for MRSA
Contact infection control for advice
Patient’s Full Name: Date of birth: Unit Number:
Ward/Department: Date of 1st Assessment: NHS Number:
Print & Sign - Name of Assessor:
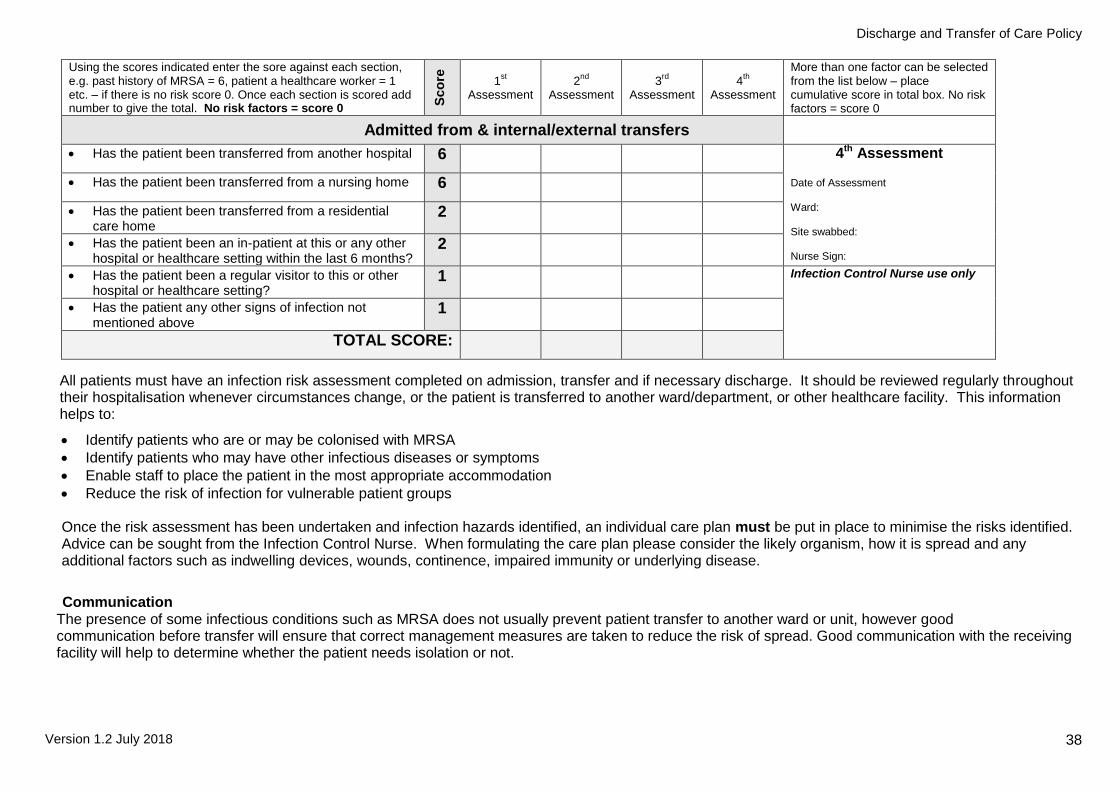
Discharge and Transfer of Care Policy
Version 1.2 July 2018
38
Using the scores indicated enter the sore against each section, e.g. past history of MRSA = 6, patient a healthcare worker = 1 etc. – if there is no risk score 0. Once each section is scored add number to give the total. No risk factors = score 0 S
co
re
1st
Assessment
2
nd
Assessment
3
rd
Assessment
4
th
Assessment
More than one factor can be selected from the list below – place cumulative score in total box. No risk factors = score 0
Admitted from & internal/external transfers
Has the patient been transferred from another hospital 6 4th Assessment
Date of Assessment Ward: Site swabbed: Nurse Sign:
Has the patient been transferred from a nursing home 6
Has the patient been transferred from a residential care home
2
Has the patient been an in-patient at this or any other hospital or healthcare setting within the last 6 months?
2
Has the patient been a regular visitor to this or other hospital or healthcare setting?
1 Infection Control Nurse use only
Has the patient any other signs of infection not mentioned above
1
TOTAL SCORE:
All patients must have an infection risk assessment completed on admission, transfer and if necessary discharge. It should be reviewed regularly throughout their hospitalisation whenever circumstances change, or the patient is transferred to another ward/department, or other healthcare facility. This information helps to:
Identify patients who are or may be colonised with MRSA
Identify patients who may have other infectious diseases or symptoms
Enable staff to place the patient in the most appropriate accommodation
Reduce the risk of infection for vulnerable patient groups
Once the risk assessment has been undertaken and infection hazards identified, an individual care plan must be put in place to minimise the risks identified. Advice can be sought from the Infection Control Nurse. When formulating the care plan please consider the likely organism, how it is spread and any additional factors such as indwelling devices, wounds, continence, impaired immunity or underlying disease.
Communication
The presence of some infectious conditions such as MRSA does not usually prevent patient transfer to another ward or unit, however good communication before transfer will ensure that correct management measures are taken to reduce the risk of spread. Good communication with the receiving facility will help to determine whether the patient needs isolation or not.
Discharge and Transfer of Care Policy
Version 1.2 July 2018
39
Appendix 7
Delayed Discharge
Letter A
Date xxxxx
Ward Address
Dear xxxxxx (named social worker)
Re: Patient xxxxxx
D.o.b xxxxxx
Date of admission xxxx
The health outcomes agreed for admission to the Assessment and Treatment Unit at
xxxxxx have now been met. However no discharge package or date has yet been
finalised. Therefore xxxxxxxxx discharge is now being delayed and will be added to
our delayed discharge submission under the following category.
Code xxxxxxxxx xxxxxxxxxxxx xxxxxxxxxxxxxxx
This submission is based on the principle that people with learning disabilities and/or
autism should not be living in hospitals. The purpose of this letter is to remind you of
the patient’s right to an ordinary life outside the hospital setting; where xxxxxxx is no
longer receiving any benefit from staying in an acute hospital unit. We believe
continued and prolonged stay in hospital is to her/his detriment, and timely discharge
is now required to ensure maximum value is gained from this admission.
Your ongoing support in resolving this delay is appreciated. The next case meeting to
discuss this is on xxxxxxxx at xxxxxxx Time: xxxxxxxxxxxxx.
Yours Sincerely,
Ward manager Cc Service manager Divisional Manager
Headquarters
Delta House
Delta Point
Greets Green Road
West Bromwich
B70 9PL
Tel: 0845 146 1800
Fax: 0121 612 8090
Web: www.bcpft.nhs.uk

Discharge and Transfer of Care Policy
Version 1.2 July 2018
40
Delayed Discharge - Letter B
Date xxxxx
Ward Address
Dear xxxxxx (named social worker)
Re: Patient xxxxxx
D.o.b xxxxxx
Date of admission xxxx
The health outcomes agreed for admission to the Assessment and Treatment Unit at
xxxxxx have now been met. However no discharge package or date has yet been
finalised. Therefore xxxxxxxxx discharge is now being delayed will be added to our
delayed discharge submission under the following category.
Code xxxxxxxxx xxxxxxxxxxxx xxxxxxxxxxxxxxx
This submission is based on the principle that people with learning disabilities and/or
autism should not be living in hospitals. The purpose of this letter is to remind you of
the patient’s right to an ordinary life outside the hospital setting; where xxxxxxx is no
longer receiving any benefit from staying in an acute hospital unit. We believe
continued and prolonged stay in hospital is to her/his detriment, and timely discharge
is now required to ensure maximum value is gained from this admission.
Your ongoing support in resolving this delay is appreciated. The next case meeting to
discuss this is on xxxxxxxx at xxxxxxx Time: xxxxxxxxxxxxx.
Yours Sincerely,
Ward manager Cc Service manager Divisional Managers
Headquarters
Delta House
Delta Point
Greets Green Road
West Bromwich
B70 9PL
Tel: 0845 146 1800
Fax: 0121 612 8090
Web: www.bcpft.nhs.uk
Discharge and Transfer of Care Policy
Version 1.2 July 2018
41
Delayed Discharge - Letter C
Date xxxxx
Ward Address
Dear xxxxxx (named social worker)
Re: Patient xxxxxx
D.o.b xxxxxx
Date of admission xxxx
The health outcomes agreed for admission to the Assessment and Treatment Unit at
xxxxxx have now been met. However no discharge package or date has yet been
finalised. Therefore xxxxxxxxx discharge is now being delayed will be added to our
delayed discharge submission under the following category.
Code xxxxxxxxx xxxxxxxxxxxx xxxxxxxxxxxxxxx
This submission is based on the principle that people with learning disabilities and/or
autism should not be living in hospital. The purpose of this letter is to remind you of
the patient’s right to an ordinary life outside the hospital setting; where xxxxxxx is no
longer receiving any benefit from staying in an acute hospital unit. We believe
continued and prolonged stay in hospital is to her/his detriment, and timely discharge
is now required to ensure maximum value is gained from this admission.
Furthermore, unless there is a clear rationale for assessment and treatment that
needs to take place in a hospital setting, people with learning disabilities and or
autism should not be there at all, in that ‘Hospital is not a home’. This is because
the hospital model is not the right one for many people whose behaviour is perceived
as challenging. (NHS England: CTR Policy &Guidance 2015).
Headquarters
Delta House
Delta Point
Greets Green Road
West Bromwich
B70 9PL
Tel: 0845 146 1800
Fax: 0121 612 8090
Web: www.bcpft.nhs.uk
Discharge and Transfer of Care Policy
Version 1.2 July 2018
42
A hospital setting can be experienced as an alien and challenging environment to be
in that we know at times can only serve to cause anxiety, separation from loved ones
and/or local communities, remove people’s choices and control over their lives and
lead to more distressed behaviour. This can result in more restrictive practices with
people becoming locked in a negative cycle.
Your ongoing support in resolving this delay is appreciated. The next case meeting to
discuss this is on xxxxxxxx at xxxxxxx at xxxxxxxxxxxxx.
Yours Sincerely,
Service manager Cc Ward manager Divisional Manager Hospital Directors
Discharge and Transfer of Care Policy
Version 1.2 July 2018
43
Policy Details
* For more information on the consultation process, implementation plan, equality impact assessment,
or archiving arrangements, please contact Corporate Governance
Review and Amendment History
Version Date Details of Change
1.2 Jul 2018 Reviewed with minor amendments
1.1 Nov 2016 New policy format and updated links to national standards
1.0 Nov 2012 New policy for BCPFT; Alignment of policies following TCS
Title of Policy Discharge and Transfer of Care Policy
Unique Identifier for this policy BCPFT-CLIN-POL-1112-057
State if policy is New or Revised Revised
Previous Policy Title where applicable n/a
Policy Category Clinical, HR, H&S, Infection Control etc.
Clinical
Executive Director whose portfolio this policy comes under
Executive Director of Nursing, AHPs and Governance
Policy Lead/Author Job titles only
Learning Disabilities Matron
Committee/Group responsible for the approval of this policy
Nursing Board
Month/year consultation process completed *
n/a
Month/year policy approved July 2018
Month/year policy ratified and issued July 2018
Next review date July 2021
Implementation Plan completed * Yes
Equality Impact Assessment completed * Yes
Previous version(s) archived * Yes
Disclosure status ‘B’ can be disclosed to patients and the public