disaster - health management and leadership portal
TRANSCRIPT

ICUMANAGEMENTT H E O F F I C I A L M A N AG E M E N T A N D P R AC T I C E J O U R N A L V O L U M E 9 - I S S U E 3 - A U T U M N 2009
EARLY MOBILISATION OF CRITICALLY ILL PATIENTS: SERIES - PART ONE
FROM CARDIAC TO THORACIC – THE OTHER COMPARTMENT SYNDROMES
EXPERIENCE FROM THE INFLUENZA OUTBREAK IN MEXICO
TRANSFORMING CARE IN THE INTENSIVE CARE UNIT
TRANSPORT EQUIPMENT: CREATING THE ULTIMATE MOBILE ICU
SURGE CAPACITY IN A COST-EFFECTIVE HEALTHCARE SYSTEM
ARE YOU PREPARED?DISASTER:
PLUS:
ICU_V9_I3_Cover10_with_correct_ads:ICU 29/09/09 09:55 Page 2

ICU_V9_I3_Cover10_with_correct_ads:ICU 29/09/09 09:55 Page 3

DISASTER: A heading that covers a myriad of problems,reactions, plans that have failed to come to fruition,sometimes natural, uncontrollable- other times pur-poseful and deliberate. Whether it be a natural event-hurricane, earthquake, flood or wild fire; an accident-plane crash, bridge collapse, ferry capsizing; or an in-tentional act- bomb explosion, arson, mass shooting,biological warfare, the result and the manner of re-sponse should and must remain the same. Respondersmust act quickly, in an organised and well-planned fash-ion in an attempt to utilise resources and ultimatelysave the lives of as many as possible in what may wellbecome a mass casualty situation.
ARE YOU PREPARED? Even carefully laid plans madeby emergency departments and intensive care units orthose based on national or international guidelines cansometimes fail to suffice in the heart of a mass casual-ty event. As recent events have shown, governments andfederal agencies are not always in control of the actu-al implementation of these plans, and it often falls tothose in the front-lines: on the scene, in the ER / trau-ma bay and ICU. In this issue of ICU Management, weattempt to delve into issues of planning at a hospitallevel and touch on a number of techniques used inemergency rooms, trauma centres and intensive careunits around the world.
In this issue, paramedics Mike Clumpner and JimMobley discuss front-line planning for a range of dis-asters and remind us of recent events and lessonslearned. Prof. Weiss brings his experiences from a lev-el one trauma centre in Israel to an article on the im-portance of process control in mass casualty events.Professors Amir Khorram-Manesh and Martin Wahlfrom Sweden discuss disaster preparedness given thecurrent ongoing challenges (economic and resource-based) in our hospitals, and management of a pandem-ic in our ICUs, respectively. In the management sec-tion, Prof. Örtenwall pushes further on the topic, bydelving into the value of surge capacity in a cost-effec-tive healthcare system.
Within the Matrix, you will find a number of enlight-ening articles - from the conclusion of Dr. Malbrain’s
article on the polycompartment syndrome to MaryKay Bader’s detailed description of the positive resultsof utilising nurse-directed protocols in the ICU. Weare also pleased to bring you the first in a three-partseries on early mobilisation of critically ill patients.In this article, Radha Korupolu and her team fromJohns Hopkins will discuss patient screening and safe-ty issues.
We feature Mexico in our Country Focus this issue - asomewhat timely choice given the cover story of thisissue and the country’s recent management of the out-break of the H1N1 virus. In addition to the usualoverview of healthcare and intensive care in his coun-try, Prof. Vazquez de Anda has kindly agreed to sharehis first hand experiences with the influenza epidem-ic in his country.
It has been oft said “To fail to plan is to plan to fail”,and undoubtedly in these uncertain times of both glob-al economic strife and political unease, we in the health-care realm must assuredly make plans for events whichare in most cases unpredictable and unexpected.
Jean-Louis Vincent
ICU Management 3-2009
EDITORIAL1
Jean-Louis Vincent
Editor-in-ChiefICU Management
Head Department
of Intensive CareErasme Hospital FreeUniversity of Brussels
Brussels, Belgium
DISASTER: ARE YOU PREPARED?
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 1

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 2

3
TABLE OF CONTENTS
EDITORIAL
DISASTER: ARE YOU PREPARED? (J.-L. Vincent)
NEWS
COVER STORY: DISASTER: ARE YOU PREPARED?
HOSPITAL DISASTER RESPONSE: ARE YOU REALLY PREPARED?
(M. Clumpner, J. Mobley)
PROCESS CONTROL IN MULTIPLE CASUALTY EVENTS
(Y. G. Weiss, Y. Weiss)
IMPACT OF HOSPITAL-RELATED DISTURBANCES ON DISASTER
PREPAREDNESS (A. Khorram-Manesh, M. Wahl, A. Hedelin, P. Örtenwall)
PANDEMIC IN THE ICU
(M. Wahl, P. Örtenwall, A. Hedelin, A. Khorram-Manesh)
MATRIX FEATURES
THE POLYCOMPARTMENT SYNDROME - PART TWO: FROM CARDIAC
TO THORACIC – THE OTHER COMPARTMENT SYNDROMES (M. Malbrain)
TRANSPORT EQUIPMENT: CREATING THE ULTIMATE MOBILE ICU
(J. Mobley, M. Clumpner)
SERIES ON EARLY MOBILISATION OF CRITICALLY ILL PATIENTS
PART ONE: SCREENING AND SAFETY ISSUES
(R. Korupolu, S. Chandolu, D. Needham)
TRANSFORMING CARE IN THE INTENSIVE CARE UNIT
THE USE OF NURSE DRIVEN PROTOCOLS (M.K. Bader)
PRODUCT COMPARISION: TRANSPORT VENTILATORS
TRANSPORT VENTILATORS: PURCHASE CONSIDERATIONS (ECRI Europe)
PRODUCT COMPARISON CHART (ECRI Europe)
MANAGEMENT
SURGE CAPACITY IN A COST-EFFECTIVE HEALTHCARE SYSTEM
(P. Örtenwall, A. Hedelin, M. Wahl, A. Khorram-Manesh)
COUNTRY FOCUS: MEXICO
THE MEXICAN HEALTHCARE SYSTEM:
THE PRACTICE OF CRITICAL CARE MEDICINE (G. F. Vazquez de Anda)
EXPERIENCE FROM THE INFLUENZA OUTBREAK IN MEXICO
(G. F. Vazquez de Anda)
CONGRESS REVIEW
EUROANAESTHESIA 2009 (I. Moppett)
AGENDA
ICU Management
is the Official Managementand Practice Journal of theInternational Symposium onIntensive Care and emer-gency Medicine and waspreviously published asHospital Critical Care.
Editor-in-ChiefProf. Jean-Louis VincentBelgium
Editorial Board
Prof. Antonio ArtigasSpain
Dr. Richard BealeUnited Kingdom
Prof. Julian BionUnited Kingdom
Dr. Todd DormanUnited States
Prof. Hans Kristian FlaattenNorway
Prof. Luciano Gattinoni Italy
Prof. Armand Girbes Netherlands
Prof. Jeff LipmanAustralia
Prof. Paolo PelosiItaly
Prof. Peter PronovostUnited States
Prof. Konrad Reinhart Germany
Prof. Jukka Takala Switzerland
CorrespondentsDr. Maurizia CapuzzoItaly
Nathalie DanjouxCanada
Prof. David EdbrookeUnited Kingdom
Dr. Dominique VandijckBelgium
ICU Management 3-2009
1
4
6
8
13
16
18
20
27
31
2223
34
36
39
4648
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 3

WORLDHospital Infections In Australia Cost $1 Billion In Lost Bed Days
A recent study by The New England Journal of Medicine found pneumonia to be the second most common cause of rehospi-talisation within 30 days after surgery.1 It’s this kind of real-world need that drives our search for relevant innovations—inno-vations like the Mallinckrodt™ TaperGuard™ endotracheal tube, shown to reduce microaspiration an average of 90% com-pared with our own Mallinckrodt™ Hi-Lo™ cuff.2 To learn more about the Mallinckrodt™ TaperGuard™ endotracheal tube,visit respiratorysolutions.covidien.com.
1 Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 360(14): 1418-1420.2 FDA 510(k) clearance.
INDUSTRYWe all know endotracheal tubes leak.The question is: What does that mean?
Infections caught in hospital are costing theAustralian healthcare system more than850,000 lost bed days, according to a newstudy by Queensland University of Technology.
Associate Professor Nick Graves, from QUT'sInstitute of Health and Biomedical Innovation,said there were 175,153 cases where patients hadacquired an infection during their hospital stay.
"If rates were reduced by just one per cent,then 150,158 bed days would be released foralternative uses, allowing an estimated 38,500additional admissions annually," he said.
The results, which have been published in theAustralian journal Healthcare Infection, cal-culate the economic consequences of health-care-acquired-infections arising among ad-missions to Australian acute care hospitals.
"Healthcare-acquired infection rates are aboutfive per cent of all admissions at the momentand with bed days valued at 1005 AUD each,the total economic burden is close to 1 bil-lion AUD per annum," he said. ProfessorGraves said the bulk of the costs were facedby the most populous states of New SouthWales, Queensland and Victoria.
He said a national programme was being un-dertaken to encourage healthcare workers towash their hands before and after touching everypatient, which had the potential of being effec-tive at reducing infection and cost-effective.
Queensland University of Technology (2009,September 2). Hospital Infections In AustraliaCost $1 Billion In Lost Bed Days. ScienceDaily.
WORLDNew WHO Data Underscores Global Threat Of World's Leading Child Killer: Pneumonia
New World Health Organisation data published in the Lancet will shed new lighton two leading causes of pneumonia, the world's leading killer of children un-der age 5, both globally and within specific countries. The results, which are thefirst ever available at the country level, are expected to serve as a clarion call todeveloping country governments to invest in pneumonia prevention programmes.
According to the studies, Streptococcus pneumoniae and Haemophilus in-fluenzae type b [Hib] infections take the lives of an estimated 1.2 million chil-dren under age 5 each year. Safe and effective vaccines exist to provide pro-tection against both diseases. However, use of Hib vaccine has only recentlyexpanded to low-income countries and pneumococcal vaccine is not yet in-cluded in national immunisation programmes in the developing world, wherechildren bear the highest risk for pneumonia and where most pneumonia-re-lated child deaths occur.
For more information and country-specific estimates, visitwww.who.int/immunization_monitoring/burden/en/.
Adapted from materials provided by GAVI's PneumoADIP, via EurekAlert!, a service of AAAS. www.sciencedaily.com
EUROPECall for Proposals for Marie Curie Initial TrainingNetworks Launched
The European Commission's Directorate-General for Research is calling forproposals for Marie Curie Initial Training Networks (ITNs). In support of train-ing and career development for researchers, the action addresses joint researchtraining networks in the form of either multi- or mono-partner ITNs. Multi-partner ITNs require at least three participants from three different MemberStates or Associated Countries. Mono-partner ITNs, on the other hand, arecomposed of just one single participant in a Member State or Associated Countryand a network of associated partners. The indicative budget of this call for pro-posals amounts to EUR 243.79 million. The deadline for submitting propos-al is 22 December 2009.
Full details of the call are available at: www.cordis.europa.eu/fp7/calls/
NEWSICU Management 3-2009
4
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 4

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 5
In the United States, there has been a large emphasis placedon disaster response training since 2001. Following September11th 2001, hospitals everywhere reviewed their disaster re-sponse plans to include scenarios that seemed so unthink-able that they once would only be thought of as a plot in aHollywood movie. Disaster plans must now address situa-tions such as state-sponsored terrorism, weapons of mass de-struction including chemical, biological radiological, nuclearand explosive agents, and cyber terrorism. In 2005, HurricaneKatrina struck the United States Gulf Coast and severely test-ed hospital disaster plans. Katrina proved that many hospi-tals could in fact handle a large-scale disaster, but only foran extremely short period of time. Most hospital disasterplans assumed that help would arrive within 12-24 hoursfollowing the incident. Katrina showed that help could bedays, if not weeks away.
Disasters are not just limited to the United States. The report-ed frequency of mass casualty disaster incidents has increasedsignificantly over the past 50 years. In the last ten years, over2 billion people worldwide have been affected by disasters(Campbell 2005).
Since 2002, many hospitals have made dramatic strides towardsincreasing their ability to respond to disasters. However, a re-cent report from the Center of Biosecurity states “The nation’shealthcare system still remains largely unprepared to respondto large-scale catastrophic emergencies” (Toner et al. 2009).
A research study conducted by the United States Departmentof Health and Human Services Agency for Healthcare Researchand Quality assessed hospital training and mock responsesto mass casualty incidents. Their research found several keypoints that were common to most all hospitals:• Internal and external communications are the key to effective disaster response
• There must be a well-defined incident command center to reduce confusion
• Conference calls are an inefficient way to manage disaster response
• An accurate and frequently updated list of phone numbers for key personnel is essential
(Hsu et al. 2004)
All Hazards Planning
An all hazards plan is an integrated planning approach to anyrealistic threat to an organisation including natural disasters,terrorist attacks, and any other incidents that could threatenthe operational capacity of a hospital. When an all hazardsplan is produced, it needs to address the following:• Preparedness- Development of plan and procedures- Increase response capabilities
• Incident mitigation and response- Sustaining critical mission operations- Protection of personnel
COVER STORY: DISASTER: ARE YOU PREPARED?
Is your hospital prepared for the next disaster? This article is designed to generate dis-cussion into the adequacy of your hospital’s current emergency response plan. Hoursupon hours of work go into creating a hospital’s emergency response plan that isdesigned to respond to a myriad of disasters. As with any large-scale plan, it mayappear flawless on paper, but may fall well short during actual performance. To para-phrase a famous quote, every battle plan works perfectly until first engagement. Thisarticle is designed to review some of the basics of hospital disaster plans, and offer top-ics for hospital administrative personnel to discuss with their staff.
HOSPITAL DISASTER RESPONSE: ARE YOU REALLY PREPARED?
6
Mike Clumpner, MBA, NREMT-P
AFire Captain/ParamedicCharlotte (NC, USA) Fire DepartmentFlight Paramedic, Regional One Air Medical Service/Med-Trans Corporation Spartanburg, South Carolina, USA
Jim Mobley, RN, BSN, NREMT-P
Program Director/Chief Flight NurseRegional One Air Medical Service/Med-Trans Corporation Spartanburg, South Carolina, USA
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 6

ICU Management 3-2009 7
• Recovery - Restoration of organisational functions
How up to date is your all hazards plan? Does it address cur-rent threats? One of the most devastating threats will arrivewith very little fanfare. A cyber attack on a critical govern-ment infrastructure can absolutely cripple a community. Wehave become so dependent on computers that they affect al-most every facet of our lives. How dependent on computersis your facility? What kind of impact would there be if youcould not use a computer for an hour, a day, or a week? Doesyour disaster plan prepare for cyber attacks on your facility?This is a very realistic threat with a high level of operationalimpact that must be considered.
Communication
The Achilles’ heel of disaster management has historically beencommunication. Hospitals need to have multiple redundanciesbuilt into their communication plan. When performing a ba-sic critical infrastructure vulnerability analysis, communication
is frequently one of the most critical vulnerabilities. Hospitalshave to work in tandem with local communication providersto harden the communication infrastructure. Does your hospi-tal all hazards plan take into account a complete and total com-munications failure? Imagine the potential for destruction if aterrorist organisation could eliminate all phone, Internet andintranet communication at your facility! Most hospitals havegone to a total paperless system for charting, ordering proce-dures, and countless other treatment modalities. Loss of com-munication in any infrastructure can prove to be crippling.Although most every hospital would be severely hampered bylosing communication, would your facility be able to compen-sate? One of the greatest hurdles faced in the first 24 – 48 hoursfollowing Hurricane Katrina was the inability to communicateto any outside agency. Every hospital in essence became an is-land for several days. Is your hospital prepared to be complete-ly self-sufficient for at least 48 – 72 hours? Do you maintain astockpile of the paper forms that your hospital used to use pri-or to going paperless? These forms may prove absolutely invalu-able if there was a total loss of computer communication.
Experts in intensive care and anaesthesia have predicted that thecurrent swine flu pandemic could overwhelm critical care bedsand ventilators in England, with hospitals on the South EastCoast, and in the South West, East of England and East Midlands,being worst hit.
The research suggests that demand for critical care beds couldoutstrip supply by up to 130 per cent, with up to 20 per cent excessdemand for ventilators in some regions.
“Any predictions need to be based on the most accurate informationavailable at the time and we recognise that we are in the earlystages of the pandemic” says Dr. Ari Ercole, a member of theresearch group led by Professor David Menon from theUniversity of Cambridge.
However, based on figures provided by the ten regional healthauthorities and using the FLUSURGE model developed by theCentres for Disease Control and Prevention in the USA, we can seethat hospitals would face massive excess demand even if the pan-demic lasted an optimistic twelve weeks.
“One of the main problems is that these beds already run at highoccupancy rates and even delaying elective surgery to create addi-tional ventilated beds would not meet demand”, explains Dr. Ercole.
Dr. Jonathan Handy, a consultant intensivist and anaesthetist fromthe Chelsea and Westminster Hospital, London, says that theresults of the study are alarming. “The best case estimates predict
that capacity could be significantly increased from baseline, whilethe worst case could exceed current capacity by an order of mag-nitude” he says in an accompanying editorial.
“All acute trusts should have already developed local flu plans toinclude a 100% increase in critical care capacity. However, some maybe more comprehensive (and optimistic) than others.”
He adds that the predicted demand levels suggest that immediateaction is needed to ensure that practical measures are in place,from stockpiling supplies to looking at how medical students couldplay an active role in patient care.
Dr. Handy argues that if the worst-case scenario fails to emergethe work carried out to expand critical care capacity will never bewasted, in a world where terrorism and environmental and man-made disasters are omnipresent.
Journal references:
Ercole A, Taylor B L, Rhodes A and Menon D K. Modelling theimpact of an influenza A/H1N1 pandemic on critical caredemand from early pathogenicity data: the case for sentinelreporting. Anaesthesia, July 2009
Handy et al. Critical care bed capacity during the flu pandemic:implications for anaesthetic and critical care departments.Anaesthesia, July 2009; DOI: http://dx.doi.org/10.1111/j.1365-2044.2009.06069.x"10.1111/j.1365-2044.2009.06069.x
Pandemic Could Overwhelm Critical Care Beds In England, Especially Children’s Units NEWS
Continued on page 43
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 7

COVER STORY: DISASTER: ARE YOU PREPARED? 8
Background
A decade ago, Jerusalem was the site of recurrent MCEs relat-ed to the Israeli-Palestinian conflict. As the single level I trau-ma centre in greater Jerusalem, this gave us a rare opportuni-ty to examine the effectiveness of our preparedness and processcontrol in such events. We quickly realised the importance ofprocess control and open communications. This was especial-ly evident with communications between those running theemergency room / trauma bay and those responsible for thefunctioning of the operating rooms, imaging (specifically CTand angiography) and intensive care units. Clear communica-tion protocols between these important areas are of key impor-tance for the smooth processing of a multitude of severely in-jured patients and their successful outcomes.
Importance of Key Personnel
Our experience and subsequent analysis taught us the importanceof having the most senior ICU manager present in the traumabay/emergency room. Several reasons supported this decision.
The ICU representative can provide:
• A direct and unbiased assessment of patient quantity andseverity. Of key importance is the direct impression on themagnitude of injury and problems faced by each patient. Thisis of key importance because much information may get lostin the chaotic phase of an MCE.
• Important input in triage decisions on the placement ofthese patients in the ICU, intermediate unit or regularwards. Some patients may present with only minor injuries,but their mechanism of injury and current complaint maysignal only the tip of an iceberg of problems to follow with-in minutes, hours or days.
Importance of Information Process
The information gathered or supervised by the senior ICUmanager in the trauma bay bears directly on the subsequentmovement of not only the patient in question but the reor-ganisation of other patient's placement in the ICU.
In fact, this information impacts the discharge policy of cur-rently admitted patients to other ICUs or regular wards. It isimportant to realise that some patients being first directed tothe operating rooms may arrive at the ICU several hours lat-er, providing an extended time window for patient dischargeor re-organisation.
Key senior personnel can also assist in decision-making re-garding necessary interventions and serve to direct patientload between different parts of the ICU or other ICU's(Cardiothoracic, Neurosurgical, Medical) based on the acu-ity and the level of required interventions and treatments.Equally distributing patients based on these criteria is ofkey importance for nursing to be able to adequately care forall patients.
There are few places which could be considered immune to man-made or natural disas-ters, culminating in a Multiple/mass Casualty Event (MCE). Much has been written onthe importance of preparedness for a MCE. However, a relatively neglected aspect in theMCE literature is that of in-hospital process control from patient admission to the trau-ma bay until their final admission to the ICU.
PROCESS CONTROLIN MULTIPLE CASUALTY EVENTS
Yoram G. Weiss, MD, MBA, FCCM
DirectorCenter for Surgical Critical Care MedicineHadassah Ein Kerem University HospitalAssociate Professor in Anesthesia and Critical Care MedicineHadassah Hebrew University Medical School, Jerusalem, Israel.
Yuval Weiss, MD
DirectorHadassah Ein Kerem University HospitalJerusalem, Israel
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 8

NETWORKINGAWARDS 2009NETWORKINGAWARDS 2009
WINNING PROJECTGETS EXTENSIVE
PRESSCOVERAGEAND €5,000 CASH
More information on www.hitm.eu
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 9

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 10

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:58 Page 11

COVER STORY: DISASTER: ARE YOU PREPARED? 12
Patient Flow
To analyse patient flow we used two terms in relationship tothe patient admission stage:• The latent phase - the time from the occurrence of an MCE to the admission of the first injured at the trauma bay/ER.
• The chaotic phase - the time from first injured admission to the final clearance of the trauma bay/ER following an MCE.
Patient flow in the hospital during the chaotic phase is of ma-jor importance. During the latent phase a quick decision, basedon official sources (police, fire brigade, etc.) and the media,must be made with regards to the magnitude of the MCE. Thiswill reflect on the policy for ER and ICU evacuation. However,as the chaotic phase starts, the flow of patients is uni-direction-al in restricted areas (Figure 1). Injured patients never return tothe ER/trauma bay after imaging or any other procedure. It isof key importance not to clog the ER / trauma bay with patientsespecially when, in many cases, a second wave of transfers willarrive, soon after the first wave, from secondary ERs in the area.Hence, patient flow is directed from the ER/trauma bay to im-aging and from there to the OR, ICU or ward (Figure 1).
Furthermore, it is of key importance to identify, prepare andstaff a-priori an area for the management of those patients thatrequire augmented care but do not meet criteria for ICU ad-mission. Preferentially, this area should be controlled or co-di-
rected by ICU specialists and be in close proximity to the ICU.A possible option is utilising the post-anaesthesia care unit(PACU), as the nursing staff is amply trained for the care of un-stable critically ill patients.
Conclusions
In any MCE, there is a massive influx of trauma patients fol-lowed shortly thereafter by a second wave of patients. This in-flux of patients is accompanied by a plethora of information(both vital and insignificant), which requires efficient pro-cessing and prioritising. In our experiences in a level I traumacentre, we have encountered a number of these events andamassed a great deal of knowledge on best practices. Of coreimportance is proper process control, which is ideally man-aged by a senior ICU manager who can assess the prioritiesand smooth transfer of patients and assist when necessary.Continuous communication is also a crucial element withinthe departments and facilitates the efficient flow of patientsfrom the ER / trauma bay through imaging, the OR and ontothe ICU. The set-up and utilisation of an area for patients whoneed additional care outside of the ICU also assists in improv-ing the uni-directional patient flow from the trauma bay. WhileMCEs can test the strengths of any hospitals’ resources and or-ganisational structure, the adherence to these simple processcontrol guidelines can positively impact the outcome of thepatients involved.
References
Aschkenasy-Steuer G, Shamir M, Rivkind A, Mosheiff R, Shushan Y,Rosenthal G, Mintz Y, Weissman C, Sprung CL, Weiss YG. The Israeliexperience: conventional terrorism and critical care. J. "http://web-spirs.ziur.co.il/webspirs/doLS.ws?ss=Crit-Care+in+SO" \t "wsr" -Crit Care 2005, 9(5): 490-499.
Shamir MY, Weiss YG, Willner D, Mintz Y, Sprung CL, Weissman C (2004).Multiple casualty terror events: the anaesthesiologist's perspective.Anaesth. Analg. 2004, 98:1746–1752.
Shamir MY, Rivkind A, Weissman C, Sprung CL, Weiss YG. Conventionalterrorist bomb incidents and the intensive care unit. Curr Opin CritCare, 2005, 11(6):580-584.
Trauma Unit / Emergency Room
Operating rooms
Patient Floors Medical ICUs
Computerized Tomography Suite
Surgical Intensive Care Units
Angiography Suite
Post-Anesthesia Care Unit
Uni-directional for traumaBi-Directional for traumaUni-Directional for non-traumaFigure 1. Patient flow
in the chaotic phase.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 12

Amir Khorram-Manesh, MD, PhD
Co-Medical DirectorPrehospital and Disaster Medicine Centre,Gothenburg, Sweden
Martin Wahl MD, PhD / Annika H.E. Hedelin, RN, / Per Örtenwall, MD, PhD,
Prehospital and Disaster Medicine Centre,Gothenburg, Sweden
IMPACT OF HOSPITAL-RELATED DISTURBANCESON DISASTER PREPAREDNESS
13ICU Management 3-2009
There is a need for adaptation and expansion of healthcare sys-tems to mobilise its resources at the time of disasters. Therefore,every country should have or create its own regional, nation-al, as well as, international plans to use all necessary resourcesto cope with qualitative and quantitative outcomes of a disas-ter. Such a plan should not only provide the theoretical back-ground, but also physical facilities needed to combat a disas-ter. In this context the capacity and preparedness of prehospitalservices, emergency departments, intensive care units, radio-logical institutions and operation theatres are of special impor-tance (Arnold 2002; Wenzel 2007).
In a recent publication we could show that hospital-related in-cidents might jeopardise the regional preparedness due to insuf-ficient capacities within the emergency institutions (Khorram-Manesh et al. 2009). The lack of hospital beds and overcrowdingof emergency departments were the major causes of such a short-coming in this study. However, it also pointed out the shortageof hospital beds and respirators in intensive care units along withambulance diversions as other important sources of failure. Eventhough the regional healthcare coverage in this study was wellenough to take care of the publics’ healthcare needs (around 150primary healthcare centres and ten emergency hospitals), hos-pital-related incidents created such regional disturbances that re-sulted in a shortcoming of the ordinary healthcare system, ques-tioning its ability to cope with an extraordinary event or disaster.Regarding intensive care units, the lack of capacity for adapta-tion, and expansion was obvious. Closure of an emergency de-partment or lack of operation theatres at another hospital led tooverloading of the nearest hospital, which in addition receivedeven more patients at its emergency department. Bed shortagein intensive care units could either be due to high inflow of op-erated patients or high admission of critically ill patients in needof assisted ventilation. The higher rate of operated patients wasdirectly related to higher number of planned operations and si-
multaneous increasing in amount of emergency cases. These num-bers changed in 2008 to 35% and 65% for bed and respiratorsshortage, respectively. In such a situation a regional coordinat-ing centre to assume command and control on a regional(“gold”) level was inevitable (Khorram-Manesh et al. 2009).
The current economic crisis within most healthcare systems hasresulted in local, regional and national plans to reduce econom-ic deficits, mostly by increasing the healthcare systems effec-tiveness through reduction of hospital beds and staff numbers,minimising reserve materials, increasing inter-institutional co-operation and expansion of out-patients departments. Althoughthese measures have proven to result in shorter length of hos-pital stay, higher number of out-patient treatments and tempo-rary cost reductions, they also challenge the mode of operationat other emergency institutions by causing overcrowded emer-gency departments, and intensive care units, ambulance diver-sions, increased morbidity and mortality (Wenzel 2007; Epleyet al. 2006; Lee et al. 2006; Fatovich et al 2003; Sun et al 2006).
Although these measures might be comprehended as logical stepstaken to improve healthcare effectiveness and reduce costs, they alsoinfluence our disaster preparedness in a negative way. Hospitals surgecapacity is influenced by three essential elements: staff; supplies/equip-ment; and structure (Guss et al. 1989; West et al. 1979). Structurerefers to both locations for patients and the organisational infrastruc-ture. ED (emergency department) overcrowding is associated withboth space and staff shortage. Hospital beds occupancy of > 90% iscorrelated with a blocked access to the wards, defined as patientswaiting in the ED for more than 8 hours when the decision has beenmade to admit them. For severely ill patients this consequently leadsto initiation of extra measures e.g. multiple testing, interventions andadministration of drugs during their prolonged stay in the ED (Kleineet al. 2007; Fatovitch et al. 2003; Sun et al. 2006; Khorram-Maneshet al. 2009). This even includes patients in need of beds in the in-
In response to the current economic constrains within the healthcare systems, differentaction plans and reforms, including tax increases, have been deployed to decrease thecosts and to increase healthcare’s effectiveness. It is, however, the time to realise thatthese measures are not enough and prioritisation might be the only way to cure thischronic condition.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 13
COVER STORY: DISASTER: ARE YOU PREPARED? 14
tensive care units. In such situations, the ED serves as a holding areafor admitted patients, sometimes remaining for more than 24 hours,which may also result in establishing observation areas in the ED(Klein et al. 2007). Earlier reports show that the average waiting timefor an inpatient acute or critical care bed in American EDs has near-ly doubled (> 6 hr) in hospitals with consistently overcrowded EDs.Delays of > 6 hours in bringing ED patients in critical condition tointensive care units has also shown to increase hospital LOS (lengthof stay) and result in higher ICU and hospital mortality (Sun et al.2006). The results, besides missed diagnoses, poor outcomes, pro-longed pain and suffering, long waiting times, patient dissatisfac-
tion, more ambulance diversions, lower physician and staff produc-tivity and higher levels of frustration among medical staffs, are high-er hospital costs and longer LOS (Wenzel 2007; Lee et al. 2006;Khorram-Manesh et al. 2009).
Disasters seldom occur, but if they do strike, a fast and effective re-sponse from healthcare services is expected. There are an increas-ing number of reports of incidents when emergency hospitals, fordifferent reasons, cannot operate at their normal capacity.This is aserious matter of concern for patient safety as well as disaster re-sponse preparedness.
A large attack on a major metropolitan area with airborne anthraxcould affect more than a million people, necessitating their treat-ment with powerful antibiotics. A new study finds that in order fora response to be effective, quick detection and treatment areessential, and any delay beyond three days would overwhelm hos-pitals with critically ill people.
"No matter how well-organised and prolonged a treatment pro-gramme is, it must be quickly implemented. In fact, our analysisshows that time-to-treatment is roughly twice as important as theduration of the distribution programme," says lead author Dr.Nathaniel Hupert, associate professor of public health and medi-cine at Weill Cornell Medical College.
"Crucial to rapidly implementing a treatment programme is earlydetection, including thorough use of advanced biosurveillancetechnologies and live, person-to-person communication," contin-ues Dr. Hupert, who is also director of the new PreparednessModeling Unit at the U.S. Centers for Disease Control andPrevention (CDC). "But most important of all are multilateral diplo-matic efforts to prevent bioterrorist attacks from ever happening."
The study predicts that a campaign initiated two days after expo-sure would protect as many as 87 percent of exposed individualsfrom illness - a rate considered successful by the CDC. Eachadditional day needed to complete the campaign would result inan average of up to 2.9 percent more hospitalisations in theexposed population. And each extra day of delay to the start ofthe programme beyond two days would result in up to 6.5 per-cent more hospitalisations.
Anthrax attack scenarios typically involve the release of onekilogram of weaponised anthrax from a small airplane flyingover a major city. The invisible powder could be inhaled by thou-sands or hundreds of thousands, who would start becomingsick anywhere from 24 hours to a week or more after theattack. With appropriate and timely administration of an antibi-otic treatment programme, exposed individuals would bespared from developing inhalational anthrax infection.
Adapted from materials provided by www.med.cornell.eduNewYork- Presbyterian Hospital/Weill Cornell Medical Center/WeillCornell Medical College. www.sciencedaily.com
Early Detection And Quick Response Are Key To Defense Against Anthrax Attack NEWS
References
Arnold JL: Disaster medicine in the 21st Century: Future hazards, vul-nerabilities, and risks. Prehosp Disast Med 2002, 17:3–11
Epley EE, Stewart RM, Love P, Jenkins D, Siegworth GM, Baskin TW,Flaherty S, Cocke R: A regional Medical operations center improvesdisaster response and inter-hospital trauma transfers. Am J Surg 2006,192: 853-859
Fatovich DM, Hirsch RL: Entry overload, emergency department over-crowding, and ambulance bypass. Emerg Med J 2003, 20: 406-409
Guss DA, Meyer FT, Neuman TS, Baxt WG, Dunford JV Jr, Griffith LD,Guber SL: The impact of a regionalized trauma system on trauma carein San Diego County. Ann Emerg Med 1989, 18: 1141–5
Khorram-Manesh A, Hedelin A, Örtenwall P: Hospital-related incidentsand its impact on disaster preparedness and prehospital organizations.Scand J Trauma Resusc Emerg Med 2009, 17: 26
Kleine KR, Nagel NE: Mass medical evacuation: Hurricane Katrina andnursing experiences at the New Orleans airport. Disaster ManagResponse 2007, 5: 56-61
Lee VJ, Low E: Coordination and Resource Maximization during DisasterRelief Efforts. Prehosp Disast Med 2006, 21: 8-12
Sun BC, Mohanty SA, Weiss R, Tadeo R, Hasbrouck M, Koenig W, MeyerC, Asch S: Effects of Hospital Closure and Hospital Characteristics onEmergency Department Ambulance Diversion, Los Angeles County,1988 to 2004. Ann Emerg Med 2006, 47: 309-316
Wenzel GW: Organizational aspects of disaster preparedness and re-sponse. JAVMA 2007, 230: 1634-1637
West JG, Trunkey DD, Lim RC: Systems of trauma care: a study of twocounties. Arch Surg 1979, 114: 455– 460
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 14

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 15

COVER STORY: DISASTER: ARE YOU PREPARED? 16
A new influenza A virus variant (H1N1)v has spread rapidlyglobally since its first appearance in April 2009 (Swine influen-za A, MMWR 2009). The World Health Organisation (WHO)raised the level of pandemic alert from phase five to phase 6/6in June 2009, indicating that an influenza named “pandemic(H1N1) 2009” is under way (ProMed-mail 2009; statementWHO Director-General 2009). This is the first pandemic in 41years and has spread more rapidly than before possibly due tointernational travel, which has eased the geographical spreadof the new virus throughout the world (New influenza A, WHOweekly 2009; Khan et al 2009).
Today, the medical society and institutions are better pre-pared to tackle the impacts of a widespread pandemic thanever before owing to better knowledge about influenza epi-demiology, diagnostic methods, surveillance systems, an-tiviral medications, antibiotics, improved influenza vaccineand vaccine production. Simultaneously, healthcare systemsworldwide are struggling with higher costs and demands ofbecoming more cost-effective. Having a capacity for adap-tion and expansion is one important factor for national/re-gional preparedness, which in combination with planningmust be crucial for the exceptional situation such as a pan-demic. Without an ongoing influenza pandemic, hospital-related incidents could jeopardise such preparedness due toinsufficient capacities within the emergency institutions(Khorram-Manesh et al 2009). Thus, there should be a con-cern how the situation will become when the pandemicstrikes hard?
During a pandemic, medical care is one of the few areas ofthe society that definitely will experience an increased de-mand and work load. Such an increase in demand cannotmerely be met through planning only; prioritisation will soonbecome the lead theme due to scarcity in many areas. The
planning in the ICU setting for an extraordinary incidence,like a pandemic has in many senses the same ingredients asin the rest of the society, but also several peculiarities, whichneed special consideration, most of all, again: scarcity espe-cially of:• ICU-beds and at least in the beginning of the epidemic, beds with possibilities for isolation or later on in the pandemic, for cohort care;
• Trained staff; • Equipment, especially for assisted ventilation;• Pharmaceutical agents (Antibiotics, antiviral, influenza-vaccine), and
• All the above but mainly in a paediatric setting depending on how the pandemic evolves.
Bed shortage at intensive care units will most likely be due tohigh admission of critically ill patients in need of assisted ven-tilation. In such a situation a regional coordinating centre toassume command and control on a regional (“gold”) levelcan be inevitable (Cowan et al. 2005, Khorram-Manesh et al.2009). Other possible ways of increasing numbers of beds oralternative technical set-ups needs to be considered alreadyin the pre-pandemic period. Scarcity of skilled staff, trainednot only for ICU activities, but also trained and comfortablewith hygienic procedures including practical skills and expe-rience from working in personal or individual protectiveequipment (PPE/IPE), can be avoided through well in-ad-vance run recruiting and training procedures. Such traininghas most probably to be extended far beyond the staff of theindividual ICU.
Scarcity in so many aspects will eventually, whether we want itor not, lead to increased needs for making priorities among pa-tients, possibly on grounds that we might not be used to orcomfortable with. Pre-planning is thus crucial also in this con-
Martin Wahl, MD, PhD
Co-Medical DirectorPrehospital and Disaster Medicine CentreRegionens HusGothenburg, Sweden
PANDEMIC IN THE ICUPer Örtenwall, MD, PhD / Annika H.E. Hedelin, RN / Amir Khorram-Manesh, MD, PhD
Prehospital and Disaster Medicine Centre,Gothenburg, Sweden
The new world, new technology and new means of transport not only make global coop-eration easier, but also the distribution of new diseases. The new influenza A virus vari-ant (H1N1)v, which has rapidly spread worldwide, offers new possibilities for coopera-tion and an unique opportunity to plan a mutual tactic against the pandemic.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 16

text and must include psycho-social considerations. Risk strat-ification of patients with influenza related pneumonia and find-ing appropriate and well-communicated methods for it, is onlyone aspect that needs to be considered in this planning con-text. Risk stratification methods also need to be transferred intosimple, agreed and well-communicated treatment protocols.Capabilities must of course include more than a list of staff andequipment available, but also a clear comprehension of howfast the resources can be achieved and for how long they canbe sustained. Communicating all the reasons for scarcity, the
necessary actions taken and priorities made, is all together prob-ably the most intricate issue.
The medical society has never before in history been able toplan so many aspects of the upcoming and unavoidable influen-za pandemic. This time we have a unique opportunity to avoiddisappointing those expectations we have for our hospitals anddepartments in this aspect. The ultimate hope is that the old(yet valid) expression from disaster medicine “To fail to planis to plan to fail” will not be realised.
ICU Management 3-2009 17
PANDEMIC IN THE ICUWhile the job of a clinician in a dis-aster scenario is to save lives with-out regard for the cause or ration-ale for the injury, medical andemergency professionals whounderstand the diverse aspects ofa disaster are better equipped torespond effectively. Giving emer-gency personnel the tools theyneed to perform in catastrophicsituations, Med ical DisasterResponse: A Survival Guide forHospitals in Mass Casualty Events
addresses the critical planning and response issues sur-rounding a mass casualty disaster before, during, and afterthe event.
The book presents the fundamental components of a com-prehensive medical disaster management plan that providesreaders with a framework for developing individual policies tosuit their particular institution. It examines natural, man-made, and terrorist disasters, and offers insight into the dif-ferent strategies required for distinct scenarios, as well as theneed to be prepared for the cascade effect of secondaryevents resulting from the original disaster.
This volume provides a powerful and unique case examplethrough a chronology of the events of September 11th,offering a firsthand account and insight into the quintes-sential test case for disaster response effectiveness. It alsoprofiles other notorious events—including HurricaneKatrina, the Madrid bombings, the SARS outbreak in 2004,and the sarin gas attack in Tokyo in 2005—as seen throughthe eyes of the expert contributors who witnessed andresponded to these tragedies.
The book presents the lessons learned from these events bythe contributing authors who acted on the front lines of themedical disaster response. It is a valuable reference manualfor emergency planning, response, and healthcare profes-sionals to confront future disasters and help prevent and mit-igate destruction and unnecessary casualties.
Dr. David Goldschmitt became the director of emergencymedicine at NYU Downtown Hospital in 1996. One of his firstduties was to reorganise the department for disaster pre-paredness. At the time of 9/11, the hospital, which received1200 casualties in three hours, had a fully operational incidentcommand structure. Since September 11, Dr. Goldschmitt haslectured in the U.S., Canada, and Israel on disaster-manage-ment strategies.
Medical Disaster Response: A Survival Guide for Hospitals in Mass Casualty Events (Hardcover)David Goldschmitt and Robert Bonvino
BOOKSin review
References
Cowan R, Trzeciak S: Clinical re-
view: Emergency department
overcrowding and the poten-
tial impact on the critically ill.
Critical care 2005, 9: 291-5
Influenza A (HlNl) – worldwide
(86): official nomenclature.
International Society for
Infectious Diseases, Pro MED-
mail, Archive number
20090706.2430 (Available at
www.promedmail.org
Khan K, Arino J, Hu W, Raposo P,
Sears J, Calderon F,
Heidebrecht C, Macdonald M,
Liauw J, Chan A, Gardam M.
Spread of a Novel Influenza A
(HlNl) Virus via Global
Airline Transportation. N
Engl J Med Jun 2009;
[Epub ahead of print]
Khorram-Manesh A, Hedelin A,
Ortenwall P. Hospital-related in-
cidents; causes and its impact on
disaster preparedness and prehos-
pital organisations. Scand J Trauma
Resusc Emerg Med. 2009; 17: 26.
New influenza A (HlNl) virus: glob-
al epidemiological situation, Jun
2009. WHO Weekly Epidemiolo -
gical Record 19 June 2009, No.
25, 2009, 84, 249-260 [edited]
Statement to the press by WHO
Director-General Dr Margaret
Chan, 11 June 2009 (Available at:
www.who.int/mediacentre/news
/statements/2009/h1n1_pande -
mic_phase6_20090611/en/in-
dex.html>; accessed June 2009).
Swine influenza A (HlNl) infection
in 2 children—Southern Cali -
fornia. MMWR Morb Mortal
Wkly Rep. 2009; 58: 400-2.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 17

Manu Malbrain, MD, PhD
ICU DirectorIntensive Care UnitZiekenhuisNetwerk AntwerpenZNA StuivenbergAntwerpen, Belgium
Inneke De laet
IntensivistIntensive Care UnitZiekenhuisNetwerk AntwerpenZNA StuivenbergAntwerpen, Belgium
THE POLYCOMPARTMENT SYNDROMEMATRIX
18
Orbital Compartment Syndrome – OCSAcute orbital compartment syndrome is a rare but treatablecomplication of increased pressure within the confined or-bital space, intra-ocular pressure (IOP). The increased IOP maycause pressure-related decreased ocular perfusion pressure(OPP) similar to that caused by mass lesions or Graves dis-ease. The condition presents with recognisable physical find-ings (eye pain, reduced ocular motility, pro-optosis, diplop-ia) and progressive visual deficit. Recognition and prompttreatment may prevent blindness. A recent study in burn pa-tients showed that increased IOP was significantly (p= 0.015)associated with the amount of fluids given during the first 24hours (37.2 ± 14.4 L vs 24.6 ± 12.3 L) and with the pres-ence of periocular burns. Emergent orbital decompression re-sulted in a drop in IOP from 59.4 ± 15.9 mmHg to 28.6 ±8.2 mmHg. Conditions that can be associated with OCS areinfection, inflammation, spinal surgery, optic nerve sheathcompression (tumour or meningeoma), vascular problemswith ophthalmic artery or retinal vein occlusion, traumaticasphyxia syndrome, bleeding diathesis or even after orbitalextravasation of X-ray contrast material.
Intracranial Compartment Syndrome – ICSA unique feature of the brain is that the intracranial contents areconfined within a rigid bony cage. Because the volume of thecranial cavity is limited by its bony casing, any change in thesize of any intracranial compartment leads to a reciprocal changein the size of the remaining compartments leading to alterationsin cerebral perfusion pressure (CPP) and intracranial pressure(ICP). Many studies have been published regarding the best treat-ment options for ICH either focusing on lowering ICP (by di-uretics or evacuation) or raising CPP (by maintaining correct
MAP with fluids or vasopressors). However fluid therapy usedto support CPP may cause retroperitoneal and visceral oedema,ascites accumulation and increased IAP, which in turn can fur-ther increase ICP. Therefore in patients with severe traumaticbrain injury, treatment decisions may result in a vicious cyclethat increases pressures in various compartments.
The effects of IAP and ITP on ICP have not been extensivelystudied to date, and remain a challenging area for laborato-ry and clinical investigators. In the study by Scalea, 78 pa-tients had an ICS and underwent a decompressive craniecto-my (DC), resulting in a significant decrease in ICP from 24to 14 mmHg. The other 24 patients had a multiple CS andunderwent both a decompressive craniectomy and a decom-pressive laparotomy (DL). The combination of DC and DL inthese 24 patients led to a decrease in ICP from around 32 to14 mmHg after DC and from 28 to 19 mmHg after DL (theeffect being different depending on whether DC or DL wasperformed first). After DL, the IAP decreased from 28 toaround 18 mmHg and so did mean airway pressure from 37to 27 cm H2O. The authors concluded that increased ICP canresult from primary traumatic brain injury as well as fromincreased IAP, which has been documented before. Patientswith PolyCS received significantly more fluids during thefirst 7 days of ICU stay, around 63 ± 21 L vs 40 ± 13 L (p<0.001). They also stayed longer in the ICU, about 25 ± 13days vs 17 ± 12 days (p= 0.01) and in the hospital, 29 ± 16days vs 21 ± 14 days (p= 0.05). While there was a trend to-wards higher mortality in these patients (42% vs. 31%), itdid not reach statistical significance. PolyCS should thereforebe considered in multiple injured patients with increased ICPthat does not respond to therapy.
PART TWO: FROM CARDIAC TO THORACIC – THE OTHER COMPARTMENT SYNDROMES
In the last issue of ICU Management, we featured PART ONE of this article, which dis-cussed Pelvic Compartment Syndrome, Abdominal Compartment Syndrome (ACS) andintra-abdominal pressure measurement. In the second part of this article, we will fo-cus on the remaining compartment syndromes –Orbital (OCS), Intracranial (ICS), Thoracic(TCS), Cardiac (CCS), Limb or extremity (ECS), Hepatic (HCS), and Renal (RCS), as wellas their interactions.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 18

19ICU Management 3-2009
Thoracic Compartment Syndrome – TCSThoracic compartment syndrome has traditionally been describedin adult and paediatric patients undergoing cardiac surgical pro-cedures. In the setting of substantial myocardial oedema, acuteventricular dilatation, mediastinal haematoma or noncardiogenicpulmonary oedema, sternal closure may precipitate cardiac tam-ponade physiology leading to haemodynamic instability or col-lapse. Theoretically TCS could also occur in patients with trau-ma, however is rarely seen due to the limited survival of patientswhose injuries were significant enough to result in massive tis-sue oedema after resuscitation from thoracic trauma. In the ICU,increased ITP is seen most commonly in relation to sepsis, cap-illary leak, fluid resuscitation, positive pressure ventilation withhigh PEEP or dynamic hyperinflation, pneumothorax, COPDwith auto-PEEP, diminished chest wall compliance (e.g. morbidobesity or eschars), lung fibrosis and ARDS. The most importantstrategy to prevent TCS or decrease the ITP and to facilitate clo-sure is the limitation of resuscitation fluid therapy through theuse of hypertonic saline or colloid solutions. The rising ITP, meanor peak inspiratory pressure during thoracic wall closure mayserve as an early warning that the patient is at risk for TCS. Theincreased ITP (normal < 5–7 mmHg) can be measured via aballoon-tipped catheter positioned in the lower third of the oe-sophagus will exert its effect on the lungs, the heart and the brain(by limiting venous return). Since increased ITP is most com-monly related to futile fluid resuscitation, IAP and ITP go handin hand. Some key-issues to remember are:
• Best PEEP should be set to counteract ITP and IAP whilst inthe same time avoiding over-inflation of already well-aeratedlung regions
- Best PEEP (cmH2O) = IAP (mmHg)
• During lung protective ventilation, the plateau pressuresshould be limited to transmural plateau pressures below35cmH2O
- Pplattm = Pplat – ITP = Pplat – IAP/2 < 35 cm H2O
• Increased ITP and IAP increase lung edema, within this concept monitoring of extravascular lung water index(EVLWi) seems warranted
Cardiac Compartment Syndrome – CCSWithin the thorax, the heart can develop an isolated CS also calledcardiac tamponade. Cardiac tamponade occurs when there is ac-cumulation of fluid or air in the pericardium caused by trauma,haemorrhage, infection or tumour causing impaired filling ofthe ventricles and decreased cardiac output (CO). As little as 250mL of fluid can cause acute cardiac tamponade whereas underchronic conditions greater amounts of fluid can accumulate asthe cardiovascular system can slowly adjust. The same effect onthe heart can occur via transmission of increased ITP either di-rectly as seen with TCS or indirectly as seen with ACS, due to thecephalad movement of the diaphragm. In case of increased ITPor IAP coronary perfusion pressure (CoPP) is lowered: CoPP =DBP – PAOP = DBP – ITP. The increase in ITP will also result in adifficult preload assessment because traditional filling pressures
will be erroneously increased. When ITP or IAP rise above 10-12 mmHg CO drops due to an increase in afterload (systemicvascular resistance) and a decrease in preload and left ventricu-lar compliance. Tachycardia may develop, mean arterial bloodpressure will decrease and a pulsus paradoxus may occur.Cardiovascular dysfunction and failure (low CO, high SVR) arecommon in conditions of increased ITP or IAP. Finally, he-patomegaly (backward failure) may develop in chronic cases, sothat cardiac tamponade may have a distant effect on other organs.
Some key-issues to remember are:
• Our understanding of traditional haemodynamic monitor-ing techniques and parameters, however, must be re-evaluat-ed in conditions of increased ITP or IAP since pressure-based or “barometric” estimates of intravascular volume as pulmonary artery occlusion pressure (PAOP) and centralvenous pressure (CVP) are erroneously increased.- The clinician must be aware of the interactions between ITP, IAP, PEEP, and intracardiac filling pressures- Misinterpretation of the patient’s minute-to-minute cardiac status may result in the institution of inappropriate and potentially detrimental therapy- Transmural (tm) filling pressures, calculated as the endexpiration value (ee) minus the ITP better reflect preload:
- CVPtm= CVPee – ITP- PAOPtm = PAOPee – ITP
- A quick estimate of transmural filling pressures can also be obtained by subtracting half of the IAP from the end-expiratory filling pressure
- CVPtm = CVPee – IAP/2- PAOPtm = PAOPee – IAP/2
• “Volumetric” estimates of preload status such as right ven-tricular end diastolic volume index (RVEDVi) or global enddiastolic volume index (GEDVi), are especially useful inconditions of the changing ventricular compliance due toelevated ITP.
• The cardiovascular effects are aggravated by hypovolemiaand the application of PEEP, whereas hypervolemia has atemporary protective effect.
Limb or Extremity Compartment Syndrome – ECSThe ECS is a condition in which the CP within the closed mus-cle compartment increases to a level that reduces capillary bloodperfusion below the level necessary for tissue viability. Permanentloss of function and contracture may occur. The extremity CPcan be measured via a needle connected to a fluid-filled pres-sure transducer system. Normal CP should be below 20 mmHgand should be used to guide the need for surgical intervention.
- Tissue PP = capillary pressure – extremity CP
The clinical findings are characterised by the 5 Ps: Pain, Pressure(tension on muscles), Paraesthesia, Paresis and Peripheral pulsealterations (diminished or prolonged capillary refill above 5
Continued on page 42
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 19

20
Mike Clumpner, BS, MBA
Fire Captain/Paramedic, Charlotte Fire Department Flight Paramedic Regional One Air Medical Services Spartanburg, South Carolina USA
Jim Mobley, RN, BSN
Program Director/Chief Flight NurseRegional One Air Medical Services Spartanburg, South Carolina USA
TRANSPORT EQUIPMENT:CREATING THE ULTIMATE MOBILE ICU
MATRIX
Equipment used on board transport vehicles whether air, sea, orland, must be both durable and functional. The rigors of the trans-port environment necessitate that the equipment be reinforcedto withstand drops, vibration, and other stressors that are nottypically seen in the in hospital environment. Battery life, ease ofuse, and other factors also play a large role in equipment choice.
Many items are used in the transport environment. In this arti-cle we will focus specifically on ventilators and patient moni-toring devices, as these are often two of the most costly pur-chases that must be made when outfitting a transport vehiclewith medical equipment.
In recent years, the available choices of both ventilators andmonitors have increased drastically. Gone are the days of onemanufacturer who dominates the market. Decision makers mustspend countless hours doing due diligence to ensure that pur-chases will allow the transport crew to be well prepared for yearsto come. A hasty purchase today may result in the acquisitionof an outdated or obsolete system. It is common knowledge thattechnology changes from day to day. Today’s cutting edge prod-uct can be tomorrow’s antiquated dinosaur.
The transport ventilator has made great progress since its in-ception. Gone are the days of having a machine that just usespressure to push air into the lungs at an oxygen concentrationof 21 percent or 100 percent. Today, many ventilators allow forprecise delivery of a prescribed oxygen concentration. This isof particular interest to transport providers that transport pa-tients that have been “weaned” from 100% oxygen down to
the lowest percentage of oxygen possible while maintaininghaemodynamic stability. Having a ventilator that will exactlymimic the hospital’s settings can mean a great deal to the pa-tients wellbeing. In fact, placing a patient on a higher concen-tration of oxygen than required simply because of ventilatorlimitations, can result in the patient having a longer hospitalstay due to the “loss of ground” that potentially occurs whenoxygen settings are manipulated unnecessarily.
Oxygen concentration is not the only differentiator when evalu-ating possible options. Weight, oxygen consumption and batterylife are also three important factors. In particular these can be-come a huge issue when transport distances are long or the trans-port vehicle has limited space. Additionally of great importanceare the operating modes of the ventilator. Is the ventilator pow-ered by gas, electricity, or both? Can it deliver positive end expi-ratory pressure (PEEP) and pressure support? Is it capable of de-livering continuous positive airway pressure (CPAP)? Ventilatorsthat can also do non-invasive ventilation may actually save a trans-port provider from buying a CPAP unit and a ventilator. Choosingan “all in one” ventilator will cover both uses with one purchase.
There are numerous ventilators to choose from in the currentECRI product comparison chart, ranging widely in price de-pending on the features that are included. Some are very ad-vanced, offering many modes to choose, while others are morebasic. Some of the ventilators are uniquely suited for the trans-port environment, touting long battery life, low oxygen con-sumption, and ease of use as selling points.
The average intensive care unit (ICU) room is approximately 400 square feet. This space oftenseems quite small when filled with monitoring devices, beds, ventilators, and pumps neces-sary for proper patient care. In the transport environment, space is often a fraction of that ofa hospital. Ambulances of all types must be configured to transport patients that require all ofthe devices that are being used in the ICU, but in a much smaller space. The limited space re-quires transport agencies to seek equipment that is compact, lightweight, and capable of per-forming the required functions that are necessary based on mission type and patient acuity.
Continued on page 35
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 20

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 21

Purchase Considerations
Included in the accompanying comparison chart are ECRIInstitute’s recommendations for minimum performancerequirements for transport ventilators. The recommendationshave been separated into two categories—basic and compre-hensive. The comprehensive recommendations are for facilitiesthat want additional features (e.g., pressure control, pressuresupport) so that ventilator strategies, similar to those offeredby an ICU ventilator, can be provided during intra-hospitaltransport. Transport ventilators should offer, at a minimum,the control mode of ventilation. In the control mode, the ven-tilator provides mandatory breaths at preset intervals and doesnot allow the patient to breathe spontaneously. They may alsoinclude other modes, such as SIMV for both volume and pres-sure breaths. Although these modes are optional for basicunits, they are preferred for intra-hospital transport applica-tions. At minimum, both visual and audible alarms should beavailable for high and low pressures, low battery power level,loss of power, and loss of supply gases. Depending on sophis-tication, the unit may have few or numerous alarms. All alarmsshould be distinct and easily identified. In addition, if alarmvolume is adjustable, it should not be possible to turn the vol-ume down to an inaudible level. The alarm silence featuremust reactivate automatically if the condition is not corrected.If an alarm is silenced, a visual display should clearly indicatewhich alarm is disabled. The delivered O2 should be monitoredwith an O2 analyser that includes an alarm for concentrationsoutside acceptable ranges. The analyser should either be
included with the ventilator or purchased separately andshould be placed in line with the breathing circuit. The con-trols (i.e., switches and knobs) should be visible and clearlyidentified, and their functions should be self-evident. Thedesign should prevent misinterpretation of displays and con-trol settings. Controls should be protected against accidentalsetting changes (e.g., due to someone brushing against thepanel) and should be sealed against fluid penetration. Patientand operator safety and system performance should not beadversely affected by fluid spills.
Other Considerations
When a purchase decision is being made, the ease with whichthe ventilator can be carried or transported must be considered.The ventilator should be small and lightweight, resistant to tip-ping over, and easily mounted in different orientations. Thesefeatures are especially useful because users may need to maneu-ver the ventilator to gain access to the controls or to accommo-date space constraints. Another important consideration is thelength of time the unit can operate on internal battery power.
Users should select ventilators that are easy to operate, which isespecially important in emergencies. The primary controls should
TRANSPORT VENTILATORS ECRI INSTITUTE RECOMMENDATIONS
HEALTHCARE PRODUCT COMPARISON SYSTEM : 22
TRANSPORT VENTILATORS
Drager MedicalOxylog 3000 plus
CovidienSupportair
Drager MedicalOxylog 2000 plus
GE HealthcareiVent 201
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 22
23ICU Management 3-2009
Contact
ECRI Institute EuropeWeltech Centre, Ridgeway Welwyn Garden City, Herts AL7 2AA, United KingdomTel. +44 (0)1707 871511 Fax. +44 (0)1707 [email protected] www.ecri.org.uk
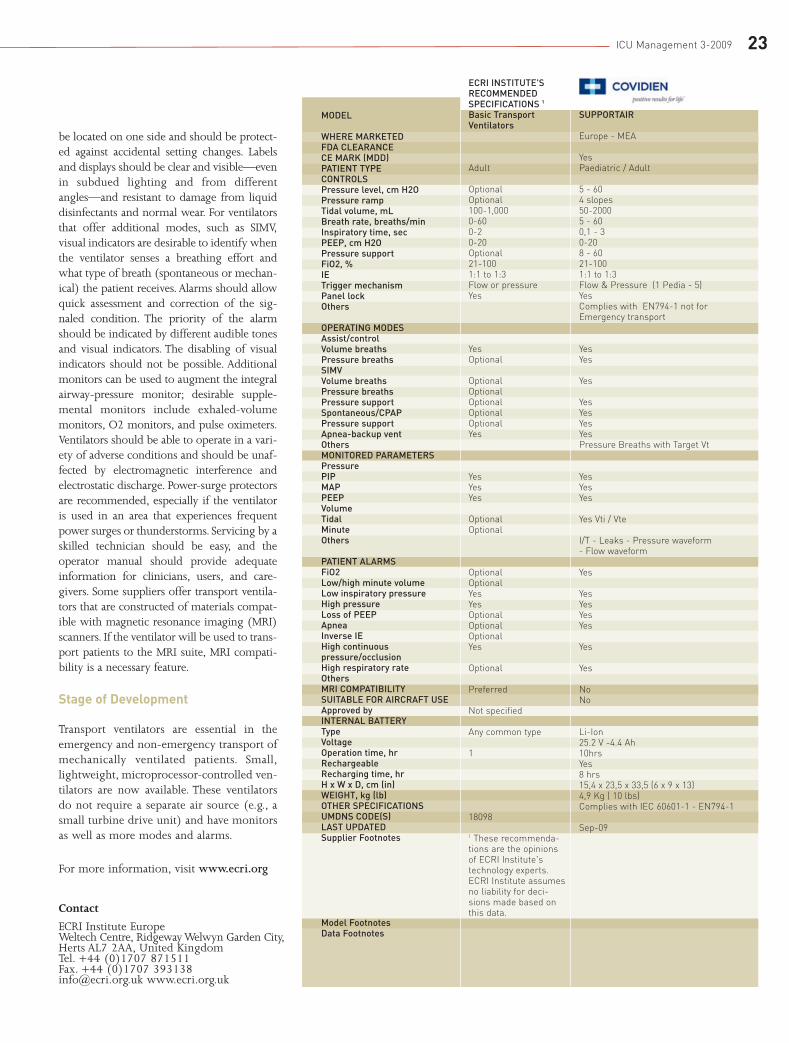
be located on one side and should be protect-ed against accidental setting changes. Labelsand displays should be clear and visible—evenin subdued lighting and from differentangles—and resistant to damage from liquiddisinfectants and normal wear. For ventilatorsthat offer additional modes, such as SIMV,visual indicators are desirable to identify whenthe ventilator senses a breathing effort andwhat type of breath (spontaneous or mechan-ical) the patient receives. Alarms should allowquick assessment and correction of the sig-naled condition. The priority of the alarmshould be indicated by different audible tonesand visual indicators. The disabling of visualindicators should not be possible. Additionalmonitors can be used to augment the integralairway-pressure monitor; desirable supple-mental monitors include exhaled-volumemonitors, O2 monitors, and pulse oximeters.Ventilators should be able to operate in a vari-ety of adverse conditions and should be unaf-fected by electromagnetic interference andelectrostatic discharge. Power-surge protectorsare recommended, especially if the ventilatoris used in an area that experiences frequentpower surges or thunderstorms. Servicing by askilled technician should be easy, and theoperator manual should provide adequateinformation for clinicians, users, and care-givers. Some suppliers offer transport ventila-tors that are constructed of materials compat-ible with magnetic resonance imaging (MRI)scanners. If the ventilator will be used to trans-port patients to the MRI suite, MRI compati-bility is a necessary feature.
Stage of Development
Transport ventilators are essential in theemergency and non-emergency transport ofmechanically ventilated patients. Small,lightweight, microprocessor-controlled ven-tilators are now available. These ventilatorsdo not require a separate air source (e.g., asmall turbine drive unit) and have monitorsas well as more modes and alarms.
For more information, visit www.ecri.org
MODEL
WHERE MARKETED FDA CLEARANCE CE MARK (MDD) PATIENT TYPE CONTROLS Pressure level, cm H2O Pressure ramp Tidal volume, mL Breath rate, breaths/min Inspiratory time, sec PEEP, cm H2O Pressure support FiO2, % IE Trigger mechanism Panel lock Others
OPERATING MODES Assist/control Volume breaths Pressure breaths SIMV Volume breaths Pressure breaths Pressure support Spontaneous/CPAP Pressure support Apnea-backup vent Others MONITORED PARAMETERS Pressure PIP MAP PEEP Volume Tidal Minute Others
PATIENT ALARMS FiO2 Low/high minute volume Low inspiratory pressure High pressure Loss of PEEP Apnea Inverse IE High continuous pressure/occlusion High respiratory rate Others MRI COMPATIBILITY SUITABLE FOR AIRCRAFT USE Approved by INTERNAL BATTERY Type Voltage Operation time, hr Rechargeable Recharging time, hr H x W x D, cm (in) WEIGHT, kg (lb) OTHER SPECIFICATIONS UMDNS CODE(S) LAST UPDATED Supplier Footnotes
Model Footnotes Data Footnotes
SUPPORTAIR
Europe - MEA
YesPaediatric / Adult
5 - 604 slopes50-2000 5 - 600,1 - 3 0-20 8 - 6021-100 1:1 to 1:3 Flow & Pressure (1 Pedia - 5)Yes Complies with EN794-1 not forEmergency transport
Yes Yes
Yes
Yes Yes Yes Yes Pressure Breaths with Target Vt
Yes Yes Yes
Yes Vti / Vte
I/T - Leaks - Pressure waveform - Flow waveform
Yes
Yes Yes Yes Yes
Yes
Yes
NoNo
Li-Ion25.2 V -4.4 Ah10hrs Yes8 hrs15,4 x 23,5 x 33,5 (6 x 9 x 13)4,9 Kg ( 10 lbs)Complies with IEC 60601-1 - EN794-1
Sep-09
ECRI INSTITUTE'SRECOMMENDEDSPECIFICATIONS 1
Basic TransportVentilators
Adult
Optional Optional 100-1,000 0-60 0-2 0-20 Optional 21-100 1:1 to 1:3 Flow or pressure Yes
Yes Optional
Optional Optional Optional Optional Optional Yes
Yes Yes Yes
Optional Optional
Optional Optional Yes Yes Optional Optional Optional Yes
Optional
Preferred
Not specified
Any common type
1
18098
1 These recommenda-tions are the opinionsof ECRI Institute'stechnology experts.ECRI Institute assumesno liability for deci-sions made based onthis data.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 23

HEALTHCARE PRODUCT COMPARISON SYSTEM : 24
TRANSPORT VENTILATORS
MODEL
WHERE MARKETED FDA CLEARANCE CE MARK (MDD) PATIENT TYPE
CONTROLS Pressure level, cm H2O Pressure ramp Tidal volume, mL Breath rate, breaths/min Inspiratory time, sec PEEP, cm H2O Pressure support FiO2, % IE Trigger mechanism Panel lock Others
OPERATING MODES Assist/control Volume breaths Pressure breaths SIMV Volume breaths Pressure breaths Pressure support Spontaneous/CPAP Pressure support Apnea-backup vent
Others MONITORED PARAMETERS Pressure PIP MAP PEEP Volume Tidal Minute Others
PATIENT ALARMS FiO2 Low/high minute volume Low inspiratory pressure High pressure Loss of PEEP Apnea Inverse IE High continuous pressure/occlusion High respiratory rate Others
MRI COMPATIBILITY SUITABLE FOR AIRCRAFT USE Approved by
INTERNAL BATTERY Type Voltage Operation time, hr
Rechargeable Recharging time, hr H x W x D, cm (in) WEIGHT, kg (lb) OTHER SPECIFICATIONS
UMDNS CODE(S) LAST UPDATED
LTV 1000
Worldwide YesYesAdult, pediatric
1 to 99Rise time 1-9 50-2,000 0-80 0.3-9.9 0-20 Off, 1-60 cm H2O 21-100 1:4 to 4:1 Flow Yes Pressure control, sensitivity, inspiratory/expiratory hold
Yes Yes
YesYesYes Yes Yes Yes
NPPV
Yes Yes Yes
YesYesStatic compliance, autoPEEP, calculated peak flow, patient effort
Yes YesYes Yes Not specified Yes No No
Yes None specified
NoYesAir Force (C-17, C-21A, C-130EH, C-130J, KC-10, KC-135 & WC-130J),Army (H-60 medevac H-60 helicopter) YesSealed lead-acid Not specified 1
YesNot specified 8 x 25 x 30 (3.1 x 9.8 x 11.8) 6.5 (14.5) O2 cylinder calculation feature, vari-able rise time, variable terminationcriteria for pressure support andpressure-controlled breaths. Meetsrequirements of cETL, IEC 60601-2-12, and ISO 13485.
18098Sep-09
LTV 1200
Worldwide YesYesAdult, pediatric, infant. All patients greater than 5 kg.
1 to 99Rise time 1-9 50-20000-80 0.3-9.9 0-20 Off, 1-60 cm H2O 21-100 1:4 to 4:1 FlowYes Pressure control, sensitivity, inspiratory/expiratory hold
YesYes YesYesYesYesYes Yes Yes Yes
NPPV
YesYes Yes Yes YesYesYesStatic compliance, autoPEEP, calculated peak flow, patient effort, SBT f/Vt, SBT f
No YesYes Yes Yes Yes NoNo
YesLow PEEP, SBT high f/Vt, SBT low f/Vt, SBT high f, SBT low f MR Conditional System available.YesArmy (H-60 medevac H-60 helicopter)
YesSealed lead-acid Not specified 1
Yes8 hours8 x 25 x 30 (3.1 x 9.8 x 11.8) 6.5 (14.5) Patient presets, spontaneous breathing trial (SBT), O2flush, O2 cylinder duration, variable rise time, andvariable termination criteria for pressure support andpressure-controlled breaths. Meets requirements ofcETL, IEC 60601-2-12, and ISO 13485.
18098Sep-09
iVent 201 IC-AB
Worldwide YesYesAdult, pediatric
5- 80 Adjustable rise/auto rise 50-2,000 1 - 800.2-3, adaptive time 0-40 0-60 cm H2O 21-100 Adjustable Pressure, flow, dual Confirm required for all changesAdaptive flow, adaptive I-time, easyexhale, Esens, Phigh, Plow
YesYes
YesYesYes Yes Yes Yes
Adaptive bilevel (NIV)
Yes Yes Yes
YesYesPlateau pressure, autoPEEP, time con-stant, compliance, resistance, Rt/Vt,trending (14 parameters for 72 hr), pres-sure and flow over time curves, eventlog, optional SpO2
Adjustable Adjustable Adjustable Adjustable Yes Adjustable YesYes
Adjustable Leak, low tidal volume delivered
Yes, conditional YesNot specified
YesSealed lead-acid 12, 7.8 A-hr Up to 2, depending on settings; optional up to 4Yes~Twice battery duration 33 x 24 x 26 (13 x 9.4 x 10.2) 10.9 (24) Rotational control knob interface; VGAoutput for secondary screen option; inte-gral O2 sensor; battery backup; softwareupgrades via PC; optional integral pulseoximetry with pleth waveform. Meetsrequirements of CSA, IEC 60601, and UL.
18098Sep-09
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 24

25ICU Management 3-2009
Oxylog 3000
WorldwideYesYesAdult & Pediatric
3 - 553 levels50-20002 - 600.2 - 100 - 200 - 35 mbar40% - 100%1:4 to 3:1 FlowNoCentral rotary knob, EL display
Yes Yes
YesYes (BIPAP & Pressure Support)Yes
Yes Yes Non-Invasive ventilation
Yes Yes Yes
YesYesRRspon., Pplat, MVspon.,Actual O2 consumption, Paw & Flow curves
NoYes/YesYes Yes NoYes NoYes
Yes
NoYes
YesLithium ion11,1 Volt4 hrs
Yes4-5 hrs184 x 285 x 1755,4 Kg (11,9 lb) incl. Battery
Sep-09
Oxylog 2000 plus
WorldwideYesYesAdult
0 - 35 3 levels100-20002 - 600.2 - 100 - 200 - 35 mbar40% or 100%1:4 to 3:1 FlowNoCentral rotary knob, EL display
Yes No
YesYes (Pressure Support)Yes
Yes Yes Non-Invasive ventilation
Yes Yes Yes
YesYesRRspon., Pplat, MVspon.,Actual O2 consumption,.Paw bar graph
NoYes/YesYes Yes NoYes NoYes
Yes
NoYes
YesLithium ion11,1 Volt4 hrs
Yes4-5 hrs184 x 285 x 1755,4 Kg (11,9 lb) incl. BatterySupplier Footnotes:Options: Pressure Support& NIV
Sep-09
Oxylog 3000 plus
WorldwidePendingYesAdult & Pediatric
3 - 553 levels50-20002 - 600.2 - 100 - 200 - 35 mbar40% - 100%1:100 to 50:1FlowNoCentral rotary knob, EL display
Yes, AutoFlow®Yes
Yes, AutoFlow®Yes (BIPAP & Pressure Support)Yes
Yes Yes AutoFlow®, Non-Invasive ventilation
Yes Yes Yes
Yes Vti / Vte
etCO2, RRspon., Pplat, MVspon., Actual O2 consumption, Paw & Flow & CO2 curves
NoYes/YesYes Yes NoYes NoYes
Yes Low & High etCO2
NoYes
YesLithium ion11,1 Volt4 hrs
Yes4-5 hrs184 x 290 x 1755,8 Kg (12,8 lb) incl. BatteryComplies with IEC 60601-1 - EN794-8
Supplier Footnotes: Oxylog 3000 plusreplaces the Oxylog 3000. Options:AutoFlow®, Capnography, Real-time-DataExport, Remote Servicing.
Sep-09
Servo-i (Adult : Infant : Universal Basic : Universal Extended)WorldwideYesYesAdult, pediatric, neonatal
0-120Rise time100-2,000 : 2-350 : 2-4,000 : 2-4,0000-1500.1-5 (infant)0-50Yes21-1001:10 to 4:1Pressure, flow, neuralYesInspiratory cycle off
YesYes
YesYesYesYesYesYesPRVC, Volume Support, NIV, NCPAP, automode, BiVent, Heliox, NAVA1
YesYesYes
YesYesTi/Ttot, Tc, WOB, RSBI, Edi, ETCO2, R, C, P0.1
YesYesYesYesYesYesYesYes
YesLow Resp rate, High/Low EtCO2, Technical alarms
YesYesFRM, Linköping, Sweden
YesNi-MH121-3 (based on 2-6 battery modules, at least 30 min/module)Yes3 per battery41.5 x 30 x 20.5 (16.3 x 11.8 x 8.1) patient unit15 (33) patient unitCan be used for treatment with Heliox (80-20, 79-21, 78-22 mixtures can be used), both invasively andnoninvasively and in any mode of ventilation offered.Meets requirements of IEC 60601-1 and ISO 10651-1.
Supplier Footnotes: 1 NAVA stands for NeurallyAdjusted Ventilatory Assist.18098Aug-09
MAQUET
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 25

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 26

27ICU Management 3-2009MATRIX
Introduction
Patients in the intensive care unit (ICU) often receive heavy se-dation and bed rest, particularly while mechanically ventilated(Needham et al. 2007; Weinert & Calvin 2007; Winkelman etal. 2005). This immobility may contribute to ICU-acquiredneuromuscular weakness, which can be severe and long last-ing in some ICU survivors. (De Jonghe et al. 2002; Fletcher etal. 2003; Herridge et al. 2003). To improve this complicationof critical illness, there is growing interest in early mobilisa-tion of patients in the ICU setting (Herridge 2008; Korupoluet al. 2009; Needham 2008; Perme and Chandrashekar 2009).Existing studies indicate that early mobilisation is safe and as-sociated with improved physical function, shortened length ofstay, and improved weaning from mechanical ventilation. Inthis article, we discuss issues related to the safety and screen-ing of critically ill patients for early mobilisation.
Early Mobilisation in the ICU
Early mobilisation aims to reduce the deleterious effects of bedrest and post-ICU impairments in muscle strength, range ofmotion and physical functioning. In many ICUs, physical ther-apy (PT) and occupational therapy (OT) begin only once a pa-tient appears ready for weaning from mechanical ventilationand sedation is reduced, or once patients are extubated (Morriset al. 2008; Schweickert et al. 2009). This delay in rehabilita-tion therapy is associated with physical impairment after ICUdischarge (Korupolu et al. 2009; Schweickert et al 2009).
In contrast to this traditional approach to ICU care, an “earlymobilisation” programme starts from patients’ initial physio-logic stabilisation and continues throughout the entire ICU stay(Bailey et al. 2007). This approach minimises heavy sedationand introduces physical medicine and rehabilitation therapieseven while patients are receiving life support therapies, suchas mechanical ventilation and vasopressor infusions. Such pro-grammes frequently start within 48 hours of initiation of me-chanical ventilation (Morris et al. 2008; Schweickert et al. 2009).
Screening and Safety Issues
Early mobilisation of ICU patients presents challenges, includ-ing poor cardiopulmonary reserve, changes in mental status(e.g., sedation and delirium), and the need for medical devicesand equipment (e.g., lines, tubes, mechanical ventilator andmonitors). These challenges necessitate careful screening toensure patient safety during mobility activities. We discuss fourimportant publications which demonstrate screening and safe-ty issues related to early mobilisation in ICU patients (Baileyet al. 2007; Morris et al. 2008; Schweickert et al. 2009; Stilleret al. 2004).
The first study specifically evaluated the effect of mobilisationon the haemodynamic and respiratory status on acutely ill ICUpatients (Stiller et al. 2004). In this study, after a comprehen-sive screening process, 69 mobilisation activities were per-formed on 31 patients. The most frequently reported activitieswere sitting on the edge of the bed and standing. A total of 3(4%) sessions resulted in desaturation that responded to a tem-porary increase in the inspired fraction of oxygen.
The second study involved mechanically ventilated medical,surgical and trauma patients in a respiratory ICU. A total of1,449 activity events were performed on 103 patients includ-ing sitting on the edge of the bed, sitting in a chair, and am-bulation (Bailey et al. 2007). Of these activities, 41% were per-formed on intubated patients. Criteria for initiation of mobilitytherapy included patient response to verbal stimulation (neu-rologic criteria), FiO2 ≤0.6 and positive end-expiratory pres-sure (PEEP) ≤10 cm H2O (respiratory criteria), and the ab-sence of orthostatic hypotension and catecholamine drips(circulatory criteria). Adverse events were prospectively definedas: (1) fall to knees, (2) feeding tube removal, (3) systolic bloodpressure >200 or <90 mmHg, (4) oxygen saturation <80%,and (5) extubation. Such events occurred in <1% of all patientactivities with no extubation events recorded. All adverse eventswere immediately corrected with no need for additional ther-apy, cost, or length of stay.
Radha Korupolu, MBBS, MS
Division of Pulmonary/Critical Care MedicineJohns Hopkins Hospital
Satish Chandolu, MBBS, MHA
Division of Pulmonary/Critical Care MedicineJohns Hopkins Hospital
SERIES ON EARLY MOBILISATIONOF CRITICALLY ILL PATIENTSPART ONE: SCREENING AND SAFETY ISSUES
Dale M. Needham, MD, PhD
Medical DirectorDivision of Pulmonary/Critical Care MedicineJohns Hopkins HospitalBaltimore, Maryland, US
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 27

MATRIX 28
The third study is a non-randomised, controlled trial of med-ical ICU patients with acute respiratory failure (Morris et al.2008). In this study, an early mobility protocol was started with-in 48 hrs of mechanical ventilation. In the early mobility group,106 patients received graduated PT activities, including turn-ing, active resistance, sitting on the edge of the bed, and activetransfer from bed to chair. The criteria to limit or withhold mo-bilisation activities included hypoxia with frequent desatura-
tions below 88%, hypotension (mean arterial pressure <65mmHg), administration of a new vasopressor agent, new doc-umented myocardial infarction, dysrhythmia requiring the ad-dition of a new antiarrhythmic agent, an increase in the PEEPor a change to assist-control mode of ventilation once in a wean-ing mode. No events of death, near death, cardiopulmonary re-suscitation or removal of a medical device were reported dur-ing physical therapy in these patients.
Neurologic criteria: Opens eyes to verbal stimulation
Yes
No
No
Yes to 1 or more
Primary CNS etiology Reassess tomorrow
Sedation-related medication
Carefully evaluate regarding appropriateness of therapy
Discuss with ICU physician regardingappropriateness for therapy
Yes to 1 or moreNo
Respiratory criteria: • FiO2 >0.6• PEEP >10 cm H2OCirculatory criteria: • New or increased vasopressor dose within past 2 hrs• Continuous infusion of a vasodilator medication• Addition of a new anti-arrhythmic agent• New cardiac ischaemia
Attempt to decrease sedation via:• interrupting continuous infusion daily• changing from continuous infusion to “as needed” bolus doses
• using anti-psychotic medication for the treatment of hyperactive delirium
Consult therapist for rehabilitation
Other criteria: • Hypoxemia: Pulse oximetry <88%• Tachypnea: Respiratory rate >45 bpm• Acidosis: Arterial pH <7.25• Hypotension: Mean arterial pressure <55 mmHg• Hypertension: Mean arterial pressure >140 mmHg• New deep venous thrombosis
Carefully initiate activity
Abbreviations:CNS – central nervous system; FiO2 – fraction of inspired oxygen; PEEP – positive end expiratory pressure
From: Korupolu R, Gifford JM, Needham DM. Early mobilization of critically ill patients: reducing neuromuscular complications after intensive care. Contemporary Critical Care 2009 (Reproduced with the permission of Lippincott Williams)
Figure 1. A screening algorithm to evaluate patient appropriateness for rehabilitation therapy
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 28

ADVERTORIAL
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 29

MATRIX 30
Finally in a recently published randomised controlled trialof acute reparatory failure patients, 498 therapy sessions wereperformed on 104 patients in a medical ICU (Schweickert etal. 2009). Only one adverse event (desaturation <80%) wasreported in this study. Activity events included range of mo-tion exercises, bed mobility, sit to stand, transfer from bedto chair, and walking. The criteria to withhold therapy in-cluded MAP <65 or >110 mmHg, systolic blood pressure>200 mmHg, heart rate <40 or >130 beats per minute, res-piratory rate <5 or >40 breaths per minute, and oxygen sat-uration <88%.
Based on the above studies and experience with the CriticalCare Physical Medicine and Rehabilitation programme in ourmedical ICU at Johns Hopkins Hospital, we have proposed ascreening algorithm (Figure 1) for initiation of early mobilitytherapy (Korupolu et al. 2009). In general, active mobilisationactivities are deferred in patients who are deeply sedated or
comatose, and who have unstable blood pressure or require atleast moderate doses of infusions of vasoactive medications.
To maximise safety, it is important that mobilisation activitiesbe tailored to each patient’s individual circumstances. Clinicaljudgment is always required on the part of all ICU cliniciansand rehabilitation therapists involved in patient care since notall circumstances can be anticipated. Moreover, providing agraduated level of activity and carefully evaluating patients’ pri-or and current clinical response to each activity are vital for thesafety of early mobility therapy. Consequently, even patientswho do not fully meet circulatory and respiratory criteria maybe able to safely participate in mobilisation activities with closemonitoring (Bailey et al. 2007).
Conclusion
Early mobilisation and rehabilitation therapy may reduce thedeleterious effects of bed rest in the ICU. Existing studies andour clinical experience indicate that screening for patients’ lev-el of consciousness, haemodynamic and respiratory stability,and other relevant factors is key for safe delivery of mobilisa-tion activities in critically ill patients. Further research is requiredto study the physiological effects and outcomes of mobilisingcritically ill patients to continue the evolution of evidence-basedguidelines (Gosselink et al. 2008; Tan et al. 2009).
References
Bailey, P., Thomsen, G. E., Spuhler, V. J., Blair, R., Jewkes,J., Bezdjian, L., Veale, K., Rodriquez, L., & Hopkins,R. O. 2007, "Early activity is feasible and safe inrespiratory failure patients", Crit Care Med, vol.35, no. 1, pp. 139-145.
De Jonghe, B., Sharshar, T., Lefaucheur, J. P., Authier, F.J., Durand-Zaleski, I., Boussarsar, M., Cerf, C., Renaud,E., Mesrati, F., Carlet, J., Raphael, J. C., Outin, H., &Bastuji-Garin, S. 2002, "Paresis acquired in the in-tensive care unit: a prospective multicenter study",JAMA, vol. 288, no. 22, pp. 2859-2867.
Fletcher, S. N., Kennedy, D. D., Ghosh, I. R., Misra, V.P., Kiff, K., Coakley, J. H., & Hinds, C. J. 2003,"Persistent neuromuscular and neurophysiologicabnormalities in long-term survivors of prolongedcritical illness", Crit Care Med, vol. 31, no. 4, pp.1012-1016.
Gosselink, R., Bott, J., Johnson, M., Dean, E., Nava, S.,Norrenberg, M., Schonhofer, B., Stiller, K., van de,L. H., & Vincent, J. L. 2008, "Physiotherapy for adultpatients with critical illness: recommendations ofthe European Respiratory Society and EuropeanSociety of Intensive Care Medicine Task Force onPhysiotherapy for Critically Ill Patients", IntensiveCare Med, vol. 34, no. 7, pp. 1188-1199.
Herridge, M. S. 2008, "Mobile, awake and criticallyill", CMAJ., vol. 178, no. 6, pp. 725-726.
Herridge, M. S., Cheung, A. M., Tansey, C. M., Matte-Martyn, A., az-Granados, N., Al-Saidi, F., Cooper,A. B., Guest, C. B., Mazer, C. D., Mehta, S., Stewart,T. E., Barr, A., Cook, D., & Slutsky, A. S. 2003, "One-year outcomes in survivors of the acute respirato-ry distress syndrome", N.Engl.J.Med, vol. 348, no.8, pp. 683-693.
Korupolu, R., Gifford, J. M., & Needham, D. M. 2009,"Early mobilization of critically ill patients: reducingneuromuscular complications after intensive care",Contemporary Critical Care, vol. 6, no. 9, pp. 1-12.
Morris, P. E., Goad, A., Thompson, C., Taylor, K., Harry,B., Passmore, L., Ross, A., Anderson, L., Baker, S.,Sanchez, M., Penley, L., Howard, A., Dixon, L.,Leach, S., Small, R., Hite, R. D., & Haponik, E. 2008,"Early intensive care unit mobility therapy in thetreatment of acute respiratory failure", Crit CareMed, vol. 36, no. 8, pp. 2238-2243.
Needham, D. M. 2008, "Mobilizing patients in the in-tensive care unit: improving neuromuscular weak-ness and physical function", JAMA, vol. 300, no.14, pp. 1685-1690.
Needham, D. M., Wang, W., Desai, S. V., Mendez-Tellez,P. A., Dennison, C. R., Sevransky, J., Shanholtz, C.,Ciesla, N., Spillman, K., & Pronovost, P. J. 2007,"Intensive care unit exposures for long-term out-comes research: development and description ofexposures for 150 patients with acute lung injury",J.Crit Care, vol. 22, no. 4, pp. 275-284.
Perme C & Chandrashekar R 2009, "Early mobilityand walking program for patients in intensive careunits: creating a standard of care", Am J Crit Care.
Schweickert, W. D., Pohlman, M. C., Pohlman, A. S.,Nigos, C., Pawlik, A. J., Esbrook, C. L., Spears, L.,Miller, M., Franczyk, M., Deprizio, D., Schmidt, G.A., Bowman, A., Barr, R., McCallister, K. E., Hall, J.B., & Kress, J. P. 2009, "Early physical and occupa-tional therapy in mechanically ventilated, critical-ly ill patients: a randomised controlled trial", Lancet,vol. 373, no. 9678, pp. 1874-1882.
Stiller, K., Phillips, A., & Lambert, P. 2004, "The safe-ty of mobilisation and its effects on haemodynam-ics and respiratory status of intensive care patients.",Physiother.Theory.Pract., vol. 20, pp. 175-185.
Tan, T., Brett, S. J., & Stokes, T. 2009, "Rehabilitationafter critical illness: summary of NICE guidance",BMJ, vol. 338, p. b822.
Weinert, C. R. & Calvin, A. D. 2007, "Epidemiologyof sedation and sedation adequacy for mechani-cally ventilated patients in a medical and surgicalintensive care unit", Crit Care Med., vol. 35, no. 2,pp. 393-401.
Winkelman, C., Higgins, P. A., & Chen, Y. J. 2005,"Activity in the chronically critically ill", Dimens.CritCare Nurs., vol. 24, no. 6, pp. 281-290.
“All adverse events were immediately
corrected with no need for additional
therapy, cost, or length of stay.”
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 30

Mary Kay Bader, RN
Neuro/Critical Care Clinical Nurse Specialist Mission HospitalMission Viejo, California, US
TRANSFORMING CARE IN THE INTENSIVE CARE UNITTHE USE OF NURSE DRIVEN PROTOCOLS
31ICU Management 3-2009
Optimising the ICU nurse’s presence at the bedside with physi-cian ordered nurse-driven protocols enhance the power of the in-terdisciplinary team to achieve coordinated, collaborative patientcare leading to improved patient outcomes. In 1997, MissionHospital’s (Mission Viejo, California) Trauma/Neuro Surgical ICUteam acknowledged the need to change the practice environment.Outcomes for patients with severe traumatic brain injury (TBI)were less than optimal with a high mortality and morbidity inthis population (Palmer et al. 2001). Upon analysis of practicepatterns, there was great disparity amongst physician providersin delivering care and a lack of team guidelines based on the sci-entific literature. ICU nurses identified diverse practices for man-aging increased intracranial pressure (ICP) due to individual physi-cian preferences. This led to confusion amongst team membersand an inconsistent approach to a multitude of patient manage-ment issues. With the hiring of a Neuro/ICU advance practicenurse (APN), meetings were held to discuss changing the envi-ronment of care. The team focussed on creating a collaborativepractice team by unifying management strategies, translating ev-idence-based guidelines into hospital-based protocols, integrat-ing standardised physician order sets, and developing nurse driv-en protocols with critical thinking algorithms.
Transformation of Care
Following a retrospective review of 3 ½ years of severe TBI pa-tients and identification of a high mortality and morbidity, agroup of physicians, nurses, pharmacists, and respiratory ther-
apists met to review the Brain Trauma Foundation (BTF)“Guidelines for managing severe TBI” (Bullock et al. 1995).Consensus was obtained amongst the practitioners to translatethe BTF guidelines to practice and standardise care amongst allpractitioners. Neurosurgeons, trauma surgeons and intensivistsagreed on the major treatment goals for severe TBI. New tech-nology was introduced including monitoring oxygen levels inthe brain. Pre-printed physician order sets were created.Education of all team members occurred with 24/7 supportprovided by the Neuro/Critical Care APN. A TBI nurse compe-tency was developed by the nursing leadership team and nurs-es were selected based on the skill, ability to critically think andproblem solve. Physician ordered nurse-driven protocols wereimplemented. Critical thinking algorithms were developed,tested and implemented to enhance decision-making at thebedside. These algorithms are continually revised as new knowl-edge, technology, or changes in the EBL occur. Consultationwith the Neuro/Critical Care APN facilitated decision makingby the bedside nurse. Prospective data collection began in Juneof 1997 and is ongoing today. Results of this approach led toa statistically significant improvement in patient outcomes witha reduction in mortality (43% to 14%) and severe disability(30% to 14%) and an increase in good outcome/moderate dis-ability (27% to 72%) (Palmer et al. 2001; Bader et al. 2008).
The use of nurse driven protocols was expanded to other facetsof care in the neurosurgical population. The TBI protocol mandat-ed the maintenance of normothermia, core body temperature of
Practitioners in intensive care units (ICU) are challenged to deliver care to critically illpatients presenting with a wide variety of diagnoses and co-morbidities. Care in ICUsshould be based on the best evidence-based literature (EBL) available and delivered by acollaborative team of practitioners working from the same ‘framework’. This implies a uni-fied, consistent approach to patient management embedded in a work environment thatpromotes interdisciplinary respect and collaboration amongst all practitioners. ICU nurs-es are consistently present at the bedside of critically ill patients and are vital members ofthis interdisciplinary team. Their skills, clinical insight, and critical decision-making trans-form the evidence based protocols and physician orders from paper to practice.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 31

32
37 degrees Celsius, for the first seven days of the patient’s ICUstay. Temperature control was difficult due to technology short-comings as well as shivering. With the introduction of a pad basedwrap system to maintain temperature at a constant rate and adop-tion of a protocol from Columbia Hospital (New York, USA)(Badjatia et al. 2008; Mayer et al. 2004; Badjatia et al. 2007; Mayer2008), the nursing staff has been consistently successful in main-taining normothermia. The translation of the Columbia’s proto-col to Mission Hospital’s physician ordered nurse-driven shiver-ing protocol involved holding a consensus meeting withneurosurgeons, trauma surgeons, intensivists and nurses to agreeupon a step-by-step approach (see Figure 1) to physical and med-ication interventions to counter shivering and maintain normoth-ermia in the critically ill neuro patient population.
In the aneurysmal subarachnoid haemorrhage (SAH) population,a protocol was developed outlining major care issues and mon-itoring priorities. One of the most frequent potential complica-tions associated with aneurysmal SAH leading to increase mor-bidity and mortality is vasospasm (Bederson et al. 2009). Thecomplex management of these patients requires the interdiscipli-nary team to assess, monitor, intervene, and evaluate for vasospasm.Using the clinical exam in awake patients and invasive technolo-gy such as transcranial dopplers, ICP monitors, brain tissue oxy-gen monitors, and cerebral blood flow monitors in patients witha decrease level of consciousness requiring intubation for airwaysupport, the team outlined important components of an aneurys-mal SAH protocol. In order to assist with the translation to thebedside, critical thinking physician-ordered, nurse-driven algo-rithms were developed and implemented. This approach has ledto consistency in care and trouble shooting of clinical scenarios.
Discussion
The use of nurse-driven protocols in critical care has beenexplored in the literature. In 2003, researchers explored theuse of a nurse-driven protocol that allowed the nurse to se-lect and start age-appropriate interventions to control proce-dural pain in paediatric patients in the emergency department(Meunier-Sham and Ryan 2003). The researchers used a com-puterised pre-established order set, which was initiated by aphysician ordering “PainFree Measures per Protocol”. By pro-viding the nurses with the protocol and orders for PainFreePaediatric agents, the team was able to avoid delays in proce-dure start times by facilitating the achievement of a pain freeintervention (Meunier-Sham and Ryan 2003). McKendry etal. 2004 studied whether using a nurse delivered protocol tooptimise postoperative circulatory status in the early hoursfollowing cardiac surgery compared to standard periopera-tive care where the nurses would call for individual ordersdecreased ICU/hospital length of stay. The study results showeda trend towards fewer complications and lower ICU lengthof stay in the nurse delivered protocol group (McKendry etal. 2004).
In the mechanically ventilated patient population, there areseveral published studies on strategies using a nurse/thera-pist driven protocol for weaning patients from mechanicalventilation (Ely et al. 2001; Marelich et al. 2000; Dries et al.2004; Tonnelier et al. 2005). These studies have found nurse-driven protocols safe, reduced mechanical ventilation daysand ICU days, reduced ventilator associated pneumonia, anddecreased complications.
Studies exploring the use of a nurse-directed protocol with re-gards to controlling hyperglycemia in critical care resulted ingood control of elevated serum glucose with few hypoglycemicepisodes. Strategies included physician pre-printed orders withranges for treatment of elevated serum glucose with insulin aswell as computerised protocols with set ranges for treatment(Meynaar et al. 2007; Osburne et al. 2006).
These studies provided validation to the use of a well-construct-ed hospital based protocol that provides physician directed,nurse-driven interventions used in the ICU. Mission Hospital’sexperiences with the implementation of these strategies haveled to improved outcomes and increased nurse satisfaction.
Conclusion
Properly constructed, evidence based hospital protocols thatprovide ICU nurses with physician-ordered, nurse-driven in-terventions enhance the ability of the critical care team to de-liver optimal care to the ICU patient population. The interdis-ciplinary team of practitioners possesses the ability to transformcare in the ICU through collaboration and the translation ofthe scientific literature to practice.
To request full references please write to [email protected]
Figure 1. Nurse-Driven Normothermia/Shivering Protocol
I. Maintain patient’s temperature 37 degrees during first seven days of hospitalisationII. Assess patient using the Bedside Shivering Assessment Scale (BSAS) every hour. A. BSAS: (Badjatia et al. Stroke 2008) GOAL is BSAS < 1. Palpate masseter, pectoralis, deltoids and quadriceps muscles0 = No shivering1 = Mild shivering localised to neck and/or chest2 = Shivering involving neck and/or chest and arms3 = Intermittent generalised shivering involving all 4 extremities
II. Temperature > 37.5 Celsius during first 7days of admitA. Institute cooling measures (Medications: *Physician orders obtained per protocol)1. Remove excess blankets2. Maintain external environment cool3. Administer Acetamenophen 650 mg per rectum/feeding tube every 4 hours*
4. Start Buspirone 20 mg per feeding tube every 8 hours*B. If shivering present1. Apply Counterwarming (BAIR Hugger at 43 degrees C)2. *Physician orders obtained for shivering protocola. Non Sedating: Magnesium sulfate 0.5 – 1gram/hour IV (goal 3-4 mg/dL)
b. Sedating: Choose one of the following1) Meperidine 25 mg every 1 hour prn 2) Dexmedetomidine 0.2-1.5 mcg/kg/hour IV 3) Fentanyl 50-200 mcg/hour IV
c. Refractory shivering (must be mechnically ventilated)1) Propofol 20-100 mcg/kg/min IV titrated to reduce shivering2) Neuromuscular Blockade: Assure sedation/analgesia medications in place prior to starting
MATRIX
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 32

ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 33
MANAGEMENT
Worldwide, healthcare systems have been struggling with high-er costs and demands of becoming more cost-effective. Despiteour efforts diseases cannot be exterminated and treatments of cur-able diseases result in manifestation of new ones. For instance de-creasing neonatal mortality has been replaced with diseases amongaging population e.g. cancers, raising the need for new areas ofcompetency, treatment alternatives and technologies (Khorram-Manesh et al. 2004). The latter is considered to be the highest costincrease for today's and future healthcare – a desirable improve-ment of the healthcare quality, but at a cost, which has not beenincluded in our economical calculations (Culter 2001; Okunade2002; Baker 2005; Di Matteo 2005; Bodenheimer 2005).
The Swedish healthcare system has seen dramatic changes dur-ing the last two decades. An increasing elderly population com-bined with improvements in medical technology and treatmentfacilities has led to a situation with an ever-increasing demandof healthcare. In a healthcare system that is almost 100% fund-ed by taxpayers, and since Sweden has some of the highest in-come taxes in the world, increasing taxation rates has not beena viable political option. Instead these challenges have been metby several different measures: • A more “efficient” hospital system has been created, often using large manufacturing industries as a “blueprint”;
• The length of stay (LOS) has been reduced dramatically for all patient groups and more diseases and conditions are treated on an outpatient basis or in day-care surgery;
• Stockpiling of supplies has been replaced by systems of “same day delivery” (Carlsson 2007; OECD Health data 2008); and
• In the last 20 years, the number of hospital beds in Sweden has been reduced from around 100,000 to 26,000. Several emergency hospitals have closed or been converted to
facilities dealing only with elective cases (OECD Health data 2008; Khorram-Manesh et al. 2009).
These changes have obvious implications for the hospital surgecapacity in cases of major incidents or disasters – a fact that israrely openly discussed (Khorram-Manesh et al. 2009). Indisaster/armed conflict planning in the 1980’s, it was assumedthat 1/3 of all in-hospital patients in Sweden could be immedi-ately discharged should there be an influx of trauma patients. Suchan assumption would be completely unrealistic today! A majortask for many consultants on call in Swedish emergency hospitalsis to prioritise which patients must be discharged in order to makehospital beds accessible for newly admitted patients, a task some-times referred to as “reverse triage”. Overcrowding of hospitals isa common problem in many countries and often affects the ICUs.
From an economic point of view, the most efficient way of util-ising given resources is a 100% occupancy at all given times. Thiscan possibly be achieved in an ideal purely elective setting withmuch standardised care provided that none untoward events oc-cur. In emergency care such a perfect balance between given re-sources and demand is much more difficult to achieve and main-tain. In reality, certain key resources, e.g. ICU beds, are oftenover-utilised. However to have a preparedness that can deal witha sudden increase in demand for emergency care there must be acertain “reserve capacity” built into the system. This is what allemergency hospitals use on an everyday basis dealing with trau-ma alerts, myocardial infarctions or other potentially life-threat-ening conditions. Thus, medical preparedness - even for everydayemergencies - carries a cost and has to compete with other pri-orities within the healthcare system (Kohn 2000; Läkaresällskapet2001; Prioriteringar i hälso- och sjukvården 2007). Preparednessto increase the capability of a hospital or a hospital system beyond
SURGE CAPACITY IN A COST-EFFECTIVE HEALTHCARE SYSTEM
34
Increasing cost within the healthcare systems has enforced dramatic changes to pre-vent a disastrous outcome and to make it more efficient. Financial constraints are ob-vious in the generic planning phase for a real disaster. Economical restrictions have ahuge impact on disaster planning. It is now the time to decide which disasters we willsee in the future.
Per Örtenwall, MD, PhD
Medical DirectorPrehospital and Disaster Medicine CentreGothenburg, Sweden
Annika H.E. Hedelin, RN / Martin Wahl, MD, PhD / Amir Khorram-Manesh, MD, PhD
Prehospital and Disaster Medicine CentreGothenburg, Sweden
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 34

the everyday influx of emergencies in order to deal with a majorincident/disaster (“surge capacity”) will also draw resources.Perhaps there is positive aspect to the recent global terrorist ac-tions and the on-going pandemic of influenza (A/H1N1) in thatthe resulting media coverage has highlighted the need for everyhospital management to review their disaster plans.
The key question in attempting to increase the surge capacity iswhich costs can be justified in a sector that is under constant fi-nancial constraint? Decisions must be made based on estimatesof realistic predictions on which disasters we will see in the fu-ture (risk assessment). Climate changes and global warming are
additional hazards that might completely change both risks ofincidents as well as vulnerabilities within our societies. The com-plexity of these issues merits a multi-disciplinary approach, inwhich relevant hospital and pre-hospital preparedness must beassessed by experts on disaster medicine. Financial constraintsare obvious in the generic planning phase for a disaster, but of-ten seem to evaporate in the aftermath of an actual event. The re-sult is often costly actions with little or even counter-productiveeffects on the stricken society and population. It is time to re-alise that money spent on scientifically based generic plans onhow to increase healthcare surge capacity is the way forward. Itis time to get rid of the old myths regarding disasters!
References
Baker L, Birnbaum H, Geppert J, Mishol D and
Moneur E. “The Relationship Between
Technology Availability And Health Care
Spending,” Health Affairs, Web Exclusive 2005;
5: W3-537-W3-551
Bodenheimer T. High and Rising Health care Costs.
Technologic Innovation. Ann Intern Med 2005;
142: 932-937
Cutler DM and McClellan M. “Is Technological
Change In Medicine Worth It?” Health Affairs
2001; 20: 11-29
Di Matteo L. “The Macro Determinants of Health
Expenditure in the United State and Canada:
Assessing the Impact of Income, Age Distribution
and Time,” Health Policy 2005; 71: 23-42
Khorram-Manesh A, Ahlman H, Nilsson O, Odén
A, Jansson S. Mortality associated with
pheochromocytoma in a large Swedish cohort.
Eur J Surg Oncol 2004; 30:556-559
Khorram-Manesh A, Hedelin A, Örtenwall P.
Hospital-related incidents; causes and its im-
pact on disaster preparedness and prehospital
organisations. Scand J Trauma Resusc Emerg
Med. 2009; 17: 26.
Kohn LT. Organizing and managing care in a
changing health system. Health Serv Res.
2000; 35: 37-52
Läkaresällskapet. Prioriteringar – vad krävs för
underlag för att göra bra horisontella priori-
teringar 2001. "www.svls.se/cs-media-old
/SvLSPublikat30/xyz/000152109.pdf
OECD Health Data (2008). www.oecd.org
Okunade AA and Murthy VNR. “Technology as a
“Major Driver” of Health Care Costs: a Co-in-
tegration Analysis of the Newhouse Conjecture,”
J Health Econ 2002; 21: 147-159
Prioriteringar i hälso- och sjukvården.
Socialstyrelsen analys och slutsatser utifrån rap-
porten ”Vårdens alltför svåra val?” Artikelnr .
2007-103-4, www.socialstyrelse.se
35ICU Management 3-2009
As previously mentioned, ventilators and monitors are two of themost costly pieces of equipment to consider when outfitting anytype of transport vehicle. Monitors are unique, due in large partto their wide variance in capabilities. As with any purchase, themission profile of the agency must be evaluated prior to purchas-ing a monitor. Many monitors can be configured in an “a la carte”manner. This means that the external portion of the monitor maylook the same, but the internal part of the machine may not befully capable of performing all of the monitoring capabilities seenin a “fully loaded” or maximally configured device.
Some transport agencies have a mission profile that requiresbasic monitoring. Electrocardiogram (ECG) and non-invasiveblood pressure monitoring (NIBP) are two pieces of data re-quired by most agencies. This allows for monitoring of patientstatus by most any member of the transport team, from firstresponder to physician.
Specialty care transport agencies may require a monitoring devicethat is far more advanced. In addition to pulse oximetry, ECG andNIBP monitoring, the ability to monitor invasive pressures suchas central venous pressure (CVP), intra-cranial pressure (ICP), in-tra-arterial pressure (IA), and even pulmonary artery pressures(PA) may be necessary. In addition to these pressure readings, tem-perature, and the ability to acquire and transmit a 12 lead electro-cardiogram may be options that are required for patient care.
Manufacturers of both ventilators and monitors are constantlyresearching and evaluating ways to improve their ability to as-sist in the care of patients. As we look at devices, it is impera-tive that we not only look at what we need in a device today,but that we also look at our needs in the future. With due dili-gence in the evaluation and research stages, we can ensure thatwe make a well informed decision resulting in our patients re-ceiving the best possible care regardless of the environment.
Continued from page 20
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 35

COUNTRY FOCUS: MEXICO 36
The United Mexican States, better known as Mexico,is conformed by 32 states and the capital city isMexico City. Mexico has a total population of 103million people (www.inegi.gob.mx). Every Mexicanhas the right to receive health protection stated inthe 4th article of the “Constitución Politica de losEstados Unidos Mexicanos”. Despite this constitu-tional right, the Mexican Healthcare System is com-plex and unequally distributed. According to theOrganisation for Economic Co-operation andDevelopment (www.oecd.org), Mexico is placedon the tail of countries with lowest investment inhealth from the Gross National Income (GNI) with6.4%. Medical attention is mainly offered accord-ing to social level, 46.9 % of Mexicans have socialsecurity insurance, but nearly 50% of the popula-tion don’t have any kind of insurance to cover med-ical expenses and these expenses must be paid di-rectly from the consumers’ pocket.
Intensive Care Units (ICUs) in Mexico
Although critical care medicine has been practicedfor nearly 40 years in Mexico (www.ammcti. -org.mx) there are not clear rules about its’ prac-tice within either the public (Social Security) orprivate system. There is a norm utilised in the ba-sic design of an ICU, but it does not include spec-ifications for equipment and supplies or specifywho should lead the unit (intensivist or any oth-er physician). Critical care practice is traditional-ly divided into critical care medicine for adults,children, and neonates, with the latter two attend-ed by paediatricians and neonatologists. Mainlycardiologists attend specific cardiac ICUs or thosewith coronary units. Recently, the Health Secretaryintegrated a multitask force to develop the officialMexican norm in ICUs.
Social Security is available for the Labour class(~66.6% of population), the Federation workers(~14.0% of population), the Armed Forces, andemployees of parastatal companies like the Mexicanoil company PEMEX (~2.2% of population), andother governmental workers from the Mexican states(~6.1%). Recently a new programme called “Seguro
Popular” was introduced and is managed by theHealth Secretary (www.salud.gob.mx). This broad-er programme covers an additional ~11.1% ofMexico’s population.
Public hospitals are classified according to the lev-el of attention that is given. First Level includes pri-mary care; Second Level hospitals mainly includehospitals with four specialties: Surgery, InternalMedicine, Paediatrics and Gynaecology/Obstetricsand Third Level Hospitals include most other sub-specialties and are mainly referred to as “MedicalUnits of High Care”. There is close interaction be-tween first and second levels, as well as second andthird levels. Intensive Care Units are placed in sec-ond and third level hospitals.
In the public system, ICUs are mainly closed, whilein contrast, units in the private system are mainlyopen. Unfortunately, there is a shortage of inten-sivists in Mexico and as a result, ICUs are mainlyattended by specialists from other fields like inter-nal medicine, surgery, anaesthesiology and nephrol-ogy among others. There are highly specialised ICUslike trauma, gynaecology and obstetrics, neuroin-tensive care mainly in the public system from im-portant cities (Mexico City and capitals of eachstate). Three suburban hospitals (60 beds each) haverecently started working with telepresence in theirICUs. Using robots (RP7i) is being increasingly ac-cepted as a new and practical way of solving theshortage of intensivists in hospitals where there arenot specialists available 24/7.
The State of Mexico is leading this new practice inMexico offering high care specialists to ICUs lo-calised in distant cities. This “robotic programme”is focussed on protecting and serving those peoplewithout social security or “Seguro Popular” whoare situated in suburban cities.
Specialisation in Critical Care Medicine in Mexico
Several universities around Mexico offer a special-isation in Critical Care Medicine, which is taken
THE MEXICAN HEALTHCARE SYSTEM:THE PRACTICE OF CRITICAL CARE MEDICINE
Gilberto Felipe Vazquez de Anda, MD, PhDHead Critical Care Robotics Department Hospital Materno Perinatal “Mónica Pretelini”Instituto de Salud del Estado de MéxicoProfessor Centro de Investigaciónen Ciencias Médicas de laUniversidad Autónoma del Estado de MéxicoMéxico
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 36

37
at third level or high care affiliated hospitals. Thecritical care medicine programme for adults in-volves a minimum of four years of training. Thephysicians should have at least two years of a ba-sic specialty (internal medicine, anaesthesiology,surgery, gynaecology and obstetrics) and com-plete another two for Critical Care. However, it ispreferred and physicians are encouraged to havealready completed a first specialty before enter-ing critical care medicine.
After training, physicians receive a diploma fromthe affiliate hospital and the university where he orshe finished the specialisation course. Thereafter,specialists must take an examination given by theMexican Council of Critical Care Medicine in or-der to receive approval to practice in critical careand be certified by the National Academy ofMedicine of Mexico. Today there are 1039 certifiedspecialists in critical care medicine in Mexico andnearly 40% are located in Mexico City(www.conacem.anmm.org.mx). Finally, doctorshave to receive a registered license of specialist,which is given by the Public Education Secretary;this is the most important document to the prac-tice of critical care medicine.
Job Opportunities
In Mexico, after finishing their training, inten-sivists can work either in the public system (whichis the most important employer of specialists), inthe private system, at universities or within allthree. Salaries are fixed ~$ 25 000 US dollars peryear, which compared with incomes in othercountries in North America, Asia or Europe is rel-atively low. This is seen as one of the major flawsin the system as it forces intensivists to seek a sec-ond or even third job in addition to their primaryfull time position.
There are other options available within the privatesystem: One possibility is to work along with a mul-tidisciplinary team; another is to work directly fora hospital and be on the payroll (although the salaryis more or less the same as in public hospitals) anda third option is to practice on their own as spe-cialist (internal medicine, surgery, anaesthesiolo-gy). Universities often offer jobs to intensivists whoare interested in following an academic career inteaching and/or research.
Continual Education for Intensivists
The AMMCTI (Asociación Mexicana De MedicinaCritica y Terapia Intensiva), founded in 1972, is themost important association for intensivists inMexico and is the organisation, which looks aftercontinual education. Every year a national congress
is held in a major city in Mexico, where more thana thousand doctors and nurses unite and discussimportant topics in critical care along with highlyrecognised speakers from around the world. Also,there are monthly nation-wide sessions transmit-ted by internet (www.ammcti.org.mx). AMMCTIhas nineteen branches located in cities all aroundMexico and it is divided into three regions: Central,North and South. Additionally, AMMCTI has a peer-reviewed journal in Spanish, indexed to LatinAmerican indices, with printed and web versions.There are representative chairs in critical care med-icine at the most important Academies in Mexico,the National Academy of Medicine of Mexico(www.anmm.org.mx), Mexican Academy ofSciences (www.amc.unam.mx) and the MexicanAcademy of Surgery (www.amc.org.mx).
Research
Research in critical care in Mexico is still unde-veloped. This is due to the federal government in-vesting more in social care and medical assistancethan in research, only 0.33% of the GNI(www.amc.unam.mx). Despite that, there are sev-eral groups that publish their experiences inSpanish publications and contribute to local jour-nals. Additionally, groups of intensivists have par-ticipated in international multicentre trials (i.e.the EPIC II study, and others sponsored by thepharmaceutical industry).
The ICU Team
It is worth mentioning that there could not be a vi-able ICU team without critical care nurses and res-piratory care technicians- who are important care-givers for the critically ill patient. The ratio of carenurses to patients is 1 to 2 in most public and pri-vate ICUs. In Mexico, nursing is a professional ca-reer that requires five years of university.To obtain a
Mexico: Facts and Figures
Total population: 105,342,000Gross national income per capita (PPP international $): 11,990Life expectancy at birth m/f (years): 72/77Healthy life expectancy at birth m/f (years, 2003): 63/68Probability of dying under five (per 1 000 live births): 35Probability of dying between 15 and 60 years m/f (per 1 000 population): 155/89Total expenditure on health per capita (Intl $, 2006): 756Total expenditure on health as % of GDP (2006): 6.2
Figures are for 2006 unless indicated. Source: www.who.int/whosis/en/index.htmlWorld Health Statistics 2008
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 37

38
ContentArticles may focus on any managementor practice issue in intensive care relat-ed to economics, quality of care or pa-tient outcome. We only accept scientificpapers with a clear connection to man-agement and practise issues. We alsoinvite viewpoints for pu blication in ourForum section, which can be personalopinions of the author and/or reactionsto articles published in prior issues.These are published at the discretion ofthe Editors. Sub missions may not havebeen published previously or be current-ly submitted for publication elsewhere.Articles must be written by independentauthorities and any sponsors for re-search must be named. If manufactur-ers are named in an article, the text mustpresent an unbiased view, not in supportof any particular company.
Submission GuidelinesAuthors are responsible for all state-ments made in their work, includingchanges made by the editor and autho-rised by the submitting author. The textshould be provided as a word documentvia e-mail to [email protected]. Please provide a contact e-mail address for correspondence. Fol -lowing review, a revised version, whichincludes the editors’ comments andrecommendations, is returned to theauthor (at the contact e-mail address)for authorisation.
Length• Articles: maximum 1000 words (less if figures or tables are included)
• Viewpoints: maximum 700 words• News/research/product updates: maximum 200 words
Please note that contributions longerthan the specified number of wordsmay not be accepted.
StructureArticle texts must contain:• Title
• Names of authors with abbreviations for the highest academic degree
• Affiliation: Department and institution, city and country
• Main authors are requested to supply a portrait photo (see specifications below)
• Summary of one or two sentences (no more than 30 words) describing the content
• Contact name for correspondence and an e-mail address which may be published with the article
• Website, if appropriate• Acknowledgements of any connections with a company or financial sponsor
• Introduction, main text and summary/ conclusion, with subheadings as appropriate
• Authors are encouraged to include checklists and/or guidelines, which summarise findings or recommendations
• References or sources, if appropriate, as specified below
Writing StyleArticles must be written in UK/BritishEnglish (e.g. organisation, not organiza-tion), with short sentences, a clear struc -ture (see above) and no bias. Full stopsin numbers may only be used to indicatea decimal place; otherwise use commasas separators.
ImagesMain authors are invited to supply a portrait photo for publication with theirarticle. This and any other relevant im-ages for publication with an article shouldbe sent by e-mail as separate files (onlyhigh resolution images with 300dpi) andtheir order of placement in the articlemust be clearly indicated. Only the elec-tronic formats “.tif” or “.jpg” can be usedfor images, i.e. not Microsoft Word orPower Point. Images must be no small-er than 9cm x 9cm at 100% scale. Onlyimages meeting these specifications canbe published. If an image has been pub-lished before, permission to reproducethe material must be obtained by the au-thor from the copyright holder and the
original source acknowledged in the text,e.g. © 2009 Sherry Scharff.
Format for ReferencesAny references that are deemed impor-tant to understanding of the articleshould be cited in concise form withinthe article. Please use the Harvard ref-erence system. Citations within the textfor a single author reference should in-clude the author surname and year ofpublication; for a citation with two au-thors include both author surnames andyear of publication; for more than twoauthors, include the first author sur-name followed by "et al." and the yearof publication. Multiple citations shouldbe separated by a semicolon, and listedin alphabetical order.
Example of within text citation: (Edwards2004; Edwards and Miller 2002; Milleret al. 2003).
Reference lists should be alphabetisedby lead author and included at the con-clusion of the submission.
Example of standard journal reference:Sydow Campbell, K. (1999) "Collectinginformation; qualitative research meth-ods for solving workplace problems",Technical communication, 46 (4) 532-544.
Authors are responsible for the accuracyof the references they cite.
AcceptanceIt is always at the discretion of our edi-torial board to accept or refuse submis-sions. We will respond to submissionswithin 8 weeks of receipt. We reserve theright to revise the article or request theauthor to edit the contents, and to pub-lish all texts in any EMC ConsultingGroup journal, on the Internet and to listthem in online literature databases.
Thank you,The ICU Management Editorial [email protected]
AUTHOR GUIDELINESICUMANAGEMENT
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 38
39COUNTRY FOCUS: MEXICO
specialisation in intensive care, nurses haveto take another year of training. With a pro-fessional career, nurses can work towards amaster’s degree and/or doctorate in thesame manner as physicians. Also, theyshould have a registered license from thePublic Education Secretary (www.sep. -gob.mx). In Mexico, nurses have theirMexican Nurses Association in IntensiveCare Medicine (AMMENCTI, from theirmeaning in Spanish) and hold their annu-al congress along with the AMMCTI at the
same days and places. The respiratory caretechnicians have a three years course recog-nised by the Public Education Secretary anda registered license for practicing respira-tory care (www. conalep.edu.mx).
The Future
New opportunities are emerging for in-tensivists to practice: echocardiography,telepresence with robots in remote ICUs,sub specialisations in obstetrics, neurolog-
ical critical care and recently, the practiceof rapid response teams, as well as pursuitof further master’s degrees and doctorates.There are opportunities for improvementin quality of care and safety in the futurein ICUs in Mexico, and there are figuresexcluded from our system, which pointto the inclusion of a pharmacist and a spe-cialist in rehabilitation within the ICU.Every day we work to promote our spe-cialty as well as to increase the standard ofsafety and care to international levels.
Background: Natural Disasters
Mexico has suffered from more than its’fair share of disasters. In 1985, an earth-quake struck Mexico City killing morethan 10 000 inhabitants and destroyingor disabling the most important high carehospitals. Following the earthquake,Mexican society showed a deep sense ofhumanity, solidarity and awareness aboutthe importance of being prepared for dis-asters. New laws and rules were createdwith regards to the design of hospitalsand skyscrapers in high risk zones, theCivil Protection Secretary was created andspecial education, “disaster teams” forfirst aid were introduced, evacuationroutes for every building and simulationswere planned to protect the populationin case of a new treat of earthquake, fireor flood. A sonar system was installed atthe pacific shore as to send an alarm 40seconds before an earthquake would hitMexico City. In 1988, another natural dis-aster occurred – hurricane Gilberto struckMexico twice, first in the Yucatan penin-sula in the city of Cancun and then at theother site of the Gulf of Mexico in thenorthern city of Monterrey, leaving hun-dreds of deaths and economic losses ofmillions of dollars in its wake. However,despite these recent natural disasters, andthe preparation that resulted, we werenot prepared for an epidemical or bio-logical disaster.
Outbreak
The Influenza outbreak observed fromMarch to May 2009 in several cities ofMexico mainly affected the fragile inten-sive care system and the health system ingeneral, showing deep flaws and a generallack of knowledge of how to act and reactin case of an epidemical event. It took near-ly a month to fit all the pieces together andto see that we were facing an outbreak witha serious threat for the population at largeand given our lack of experience in thistype of case, we did not know what to do.Additionally, there were concerns with re-gards to the health workers, they were high-ly exposed to the virus due to their inex-perience and insufficient protectionequipment and supplies. Mexican healthauthorities sent an epidemiological alertabout the known cases of influenza on April16th, 2009. The same day, the MexicanAssociation of Critical Care Medicine(AMMCTI) held its monthly session, atwhich an important subject was discussed:The increasing number of cases of severepneumonia in younger people. These cas-es were invading intensive care units (ICUs)across the country and were associated withhigh acute respiratory failure, multi organfailure and high mortality. A common pat-tern was observed: All patients in these cas-es were below 65 years, obese, with severehypoxemia and there were difficulties toventilate them. Also, it was apparent that
health workers were becoming infected bypatients despite taking the usual precau-tions. Of course, the highest numbers ofcases of infected health workers were ob-served in the first days of the outbreak, inMarch and April. Those professionals whoparticipated in this session were very con-cerned and motivated to rectify the issuesand change our current course. A majorconcern was in our minds – we were fac-ing an outbreak of influenza, which wewere not prepared for, and had no plan atall to deal with a biological disaster like theone that was facing us. Our highly demand-ed ICUs, which most of the time are full ofpatients, might be under further demandfrom patients suffering from the epidem-ic- our primary concern at that time wasthe knowledge that there were not enoughventilators available for all patients whowould require ventilatory support.Additionally, ICUs were not designed withnegative pressure rooms, doctors and nurs-es were not trained to attend patients withhighly transmissible infections, and therewas not proper safety equipment to pro-tect them during patient care in the ICU.There was a high probability, given theseproblems, of this epidemic causing the to-tal failure of the healthcare system.
Organisation and Planning
Members of the AMMCTI agreed to startorganising ourselves to make an action
EXPERIENCE FROM THE INFLUENZAOUTBREAK IN MEXICO Gilberto Felipe Vazquez de Anda, MD, PhD
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 39

COUNTRY FOCUS: MEXICO40
plan for an eventful outbreak of influen-za. Colleagues from Mexico City and fromall over Mexico were informed about theepidemic, and advised on how to treat pa-tients and how to protect doctors, nursesand other health workers, as well as pre-pare for the number of patients whichwere admitted in their units with se-vere pneumonia. We were acutelyaware that the impact of the outbreakwould be on ICUs.
By April 21, we sent a call for help tosome colleagues, mainly those whohad previous experience with SARS, inan attempt to get specific recommen-dations on appropriate measures ofprotection, and the supplies and equip-ment that we would require. Membersof the AMMCTI became involved incommittees organised by the federalHealth Secretary and the more localisedhealth system from the states. We werejust three days ahead of the official an-nouncement of the new virus causingthe infection in Mexico when we re-ceived the first responses to our call for help.The responders, Randy Wax from Universityof Toronto and Edgar Jimenez from Universityof Florida, took immediate action and sched-uled a series of web talks about protectionfrom the spread of infection in cases of bio-logical disasters. Also the AMMCTI designeda specific web page with information aboutinfluenza, primary care and informationabout how to avoid transmission.
International Response
Exactly one week after our meeting, thePresident of Mexico announced that Méxicowas facing an outbreak of a new type of virusof influenza, the swine origin flu AH1N1,and for that reason schools, universities andpublic buildings had to be closed the verynext day in order to cut down the transmis-sion of the virus in a city of nearly 20 mil-lion people. For the three weeks that fol-lowed, Mexico was immersed in what severalcalled the first pandemic of the new era.People started wearing facemasks in publicsettings, rapidly depleting stocks of theseproducts even in hardware stores. In hospi-tals, especially within ICUs and ERs therewere insufficient supplies to attend to the de-mand of patients with flu, and there was alack of diagnostic tests and antiviral treat-ments. Mexican health authorities took dras-
tic measures to efficiently control the epi-demic; and a special budget was authorisedto buy supplies, equipment, diagnostic testsand treatment with antivirals. However, inthe first days of the outbreak, there was anoverwhelming feeling of fear and hopelesswhen patients crowded the ER and there
were mass transfers into ICUs. The web talksthat were given by Dr. Edgar Jimenez and Dr.Randy Wax were well attended by doctors,nurses, and administrators from several hos-pitals in Mexico City and in other cities. TheCritical Care Society web page provided in-formation about influenza, and there werenumerous other examples of solidarity, likethe letters to members of the AMMCTI sentby the president of the SCCM and colleaguesfrom all over the world (Canada, USA, China,Spain, and Germany, among others).
The health secretary, the federal governmentand the government of states involved in theoutbreak gave supplies for protection, diag-nosis and treatment. Members of the AMM-CTI designed a decision making chart for treat-ment of acute respiratory failure secondary tosevere pneumonia, and were involved in mostof the committees during the outbreak.
Despite the fact that influenza virus AH1N1was virulent, the associated mortality wasrelatively low, but the economic impactwas quite high. The epidemic has spreadrapidly all over the world and has reachedthe level of pandemic according to WHO.Now we are preparing the second strikefor this coming winter and schools, uni-versities, public buildings, federal and lo-cal governments are working intensively
to prepare people for the potential reoc-currance of the outbreak.
What we learned from the epidemic was thatwe have to have a plan for biological disas-ters, that mother nature can strike at any mo-ment and most of the time is not so benev-
olent. For that reason the Secretary ofHealth together with a multidiscipli-nary team is working to map out di-rectives on the minimal equipmentand supplies needed for ICUs to guar-antee medical attention for severelyill patients under these extreme cir-cumstances. Also, there is a nation-wide campaign underway to showthe population how to act in case ofan epidemic, and how to preventtransmission. In the State of Mexicothere is a telepresence programmewhich utilises robots and the inter-net to treat patients in distant cities.
Since the outbreak, we have returnedsomewhat to what we call normality,but we are mindful of the immediate
need to prepare for the potential reappear-ance of influenza this coming winter. Thehealth system is preparing the populationwith information about how to prevent in-fluenza, primary care measures to avoid trans-mission of the virus, a daily count of new cas-es, mortality, statistics, improvement ofequipment and supplies, symposiums, etc.
Conclusion
With the initial phase of this epidemic near-ing completion in our area, we are able tofinally reflect on our state of preparednessfor disasters. It has become clear that it is apriority to plan for the possibility of all typesof disaster, not just the predictable eventssuch as hurricanes or earthquakes, in everyICU of Mexico. Of crucial importance withregards specifically to biological threats isthe improvement of efficient medical atten-tion for critically ill patients, the protectionof health workers from highly virulentviruses and/or bacteria and the decrease ofmortality by careful monitoring of vulner-able patient populations during outbreaks.At this point, we feel relatively confident ofour position should we face an outbreak inthe future, however we must challenge our-selves to act in an even more organised andrapid way to save more lives than we did inour recent showdown with AH1N1.
Mexico deserves global gratitude for itsforceful, costly, courageous and timely response to the flu. The national shut-down in Mexico, which caused Cuba andArgentina to cancel flights to the country,helped slow the initial spread of the virus.
"Mexico gave the world an early warn-ing, and it also gave the world a modelof rapid and transparent reporting, ag-gressive control measures, and gener-ous sharing of data and samples,"said World Health Organisation Director-General Dr. Margaret Chan.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 40

FAX BACK: +32 2 286 8508TRANSFER TO: BE2973501603 2064 KREDBEBB
* If you attend ISICEM, a one year subscription is included in the congress free
ICUMANAGEMENT
Subscribe now!
•Transfer the correct amount to the following bank account:
ICU Management, 28 rue de la Loi, B-1040 Brussels
IBAN BE29 7350 1603 2064 Swift: KREDBEBB
(in Belgium: 735-01603 20-64) Note: Charges to the principal;
Name:
Institution:
Address:
Postcode & Town:
Country:
Telephone:
E-mail:
Two years subscription One year subscription
Subscription Rates
One year: Europe now only 53 € Overseas now only 68 €Two years: Europe now only 89 € Overseas now only 105 €
Subscription online:WWW.ICU-MANAGEMENT.ORG/INDEX.PHP?ID=SUBSCRIBE
HOW TO SUBSCRIBE:
•Complete the form below and fax it to +32 2 286 8508 or post it to:ICU Management, 28 rue de la Loi, B-1040 Brussels.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 41

42
seconds). A crush injury can be caused by the patient’s ownweight in case of unconsciousness related to poisoning, drugoverdose, strenuous exercise or during prolonged anaesthesia,especially if the patient has a high body mass index (BMI).External causes of increased extremity CP are mainly related totrauma with fractures (especially of the tibia) and tight plastercasts, muscle contusions, bleeding disorders, burns (with es-chars), venous obstruction, arterial occlusion with post ischaemicswelling, all causing muscle compression and further crush in-jury. This will result in muscle compression and rhabdomyoly-sis, which may cause hypovolemia, acute kidney injury and fail-ure, coagulopathy, acute lung injury (ALI) and shock. Hence theincreased extremity CP may have a distant effect on other or-gans. Besides aggressive fluid resuscitation, the only definitivetreatment if CP rises above 30 mmHg is decompressive fascioto-my with muscle debridement in case of necrosis. Increased IAPrelated to ACS or Pelvic CS can have an effect on extremity CPdue to the diminished venous return from the extremities to thecentral circulation causing further limb swelling.
Hepatic Compartment Syndrome – HCSWithin the capsule of the liver itself, local haematoma forma-tion caused by trauma or bleeding diathesis (e.g. oral anticoag-ulants, liver cirrhosis,…) may have an adverse affect on tissueperfusion causing a local hepatic compartment syndrome. Theliver appears to be particularly susceptible to injury in the pres-ence of elevated surrounding pressures, thus especially in caseof IAH or ACS. Animal and human studies have shown impair-ment of hepatic cell function and liver perfusion even with onlymoderately elevated IAP of 10 mmHg. Furthermore, acute liverfailure, decompensated chronic liver disease and liver transplan-tation are frequently complicated by IAH and ACS. Close moni-toring and early recognition of IAH, followed by aggressive treat-ment may confer an outcome benefit in patients with liver disease.In the management of these patients it might be useful to mon-itor the plasma disappearance rate (PDR) for indocyaninegreen(ICG) as this correlates not only with liver function and perfu-sion but also with IAP. Since cytochrome P450 function may bealtered in case of IAH/ACS, medication doses should be adapt-ed accordingly. With increasing IAP, there is decreased hepaticarterial flow, decreased venous portal flow and an increase in theportacollateral circulation, which all exerts physiological effectswith decreased lactate clearance, altered glucose metabolism andaltered mitochondrial function.
Renal Compartment Syndrome – RCSIntra-abdominal hypertension (IAH) has been associated withrenal impairment for over 150 years. It is only recently howev-er that a clinically recognised relationship has been found. ElevatedIAP significantly decreases renal artery blood flow and compress-es the renal vein leading to renal dysfunction and failure. Oliguriadevelops at an IAP of 15 mmHg and anuria at 25 mmHg in thepresence of normovolemia and at lower levels of IAP in the pa-tient with hypovolemia or sepsis. Renal perfusion pressure (RPP)and renal filtration gradient (FG) have been proposed as key fac-tors in the development of IAP-induced renal failure.
- RPP = MAP – RVP- Where RVP = renal vein pressure
- FG = GFP – PTP = RPP – PTP = (MAP – RVP) – RVP = MAP – 2*RVP
- Where GFP = glomerular filtration pressure- And PTP = proximal tubular pressure
In conditions of increased IAP, the RVP may be substituted byIAP, or thus:- RPP = MAP – IAP- FG = MAP – 2*IAP
- Thus, changes in IAP have a greater impact upon renal func-tion and urine production than will changes in MAP. Itshould not be surprising, therefore, that decreased renalfunction, as evidenced by development of oliguria, is oneof the first visible signs of IAH. An increasing number oflarge clinical studies have identified that IAH (³15mmHg)is independently associated with renal impairment and in-creased mortality. The etiology of these changes is not en-tirely well established, however it may be multifactorial:Reduced renal perfusion, reduced cardiac output and in-creased systemic vascular resistance and alterations in humer-al and neurogenic factors. Within the capsule of the kidneyitself, local haematoma formation (caused by trauma orbleeding diathesis) may have an adverse affect on tissue per-fusion causing a local renal compartment syndrome.
Conclusions
First suggested in 2007, the polycompartment syndrome is aconstellation of the physiologic sequelae of increased compart-ment pressures, be it ICP, ITP or IAP. Recent observations sug-gest an increasing frequency of this complication in all types ofpatients and increased compartment pressures are independent-ly associated with morbidity and mortality. Even chronic eleva-tions of CP seem to affect the various organ systems in the body.In spite of this, the syndrome is still in its infant stage and re-mains poorly recognised and thus poorly treated in some cases.The diagnosis relies largely on CP measurement. Within the poly-compartment syndrome the abdomen plays a central role andthe effect of IAH on different organ systems has been described,along with recommendations to compensate for these effects.The ultimate goal of treatment is not only to decrease the CP, butalso to improve organ function and to decrease mortality.Decompressive craniectomy, sternotomy, fasciotomy and laparo-tomy are the only treatment options that have been shown toreach most of these goals today. However, some less invasive tech-niques and some medical treatment strategies have shown prom-ise in achieving CP reduction as well as organ function improve-ment. The bottom line is that futile crystalloid over-resuscitationmay cause (iatrogenic) secondary ACS, while the cautious ad-ministration of colloids not only seems to decrease the incidenceof ACS in burn and trauma patients but also the ACS associatedcomplications and mortality as well as the complications relat-ed to increased pressures in other compartments.
To request full references please write to [email protected]
Continued from page 19
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 42

ICU Management 3-2009 43
Security
Security is a vital link in disaster response. If your emergencydepartment has four shooting victims arrive from a gang shoot-ing, do you automatically “lock down” the emergency depart-ment? How difficult is it just to secure your emergency de-partment? Does your facility have the ability to completelysecure every entrance? How big is your security force?Historical data has shown that the majority of patients froma large-scale event will self-transport to the closest hospital.(Figure 1, below) Along with the concern of a large influx ofpatients, the United States Center for Disease Control has foundseveral problems for hospitals that are common when patientsself transport from a mass casualty scene. (Figure 2, page 44)
If a major event happened blocks from your hospital, wouldyou be able to completely lock down your hospital and pre-pare for the onslaught of patients? If there were an incidentat an elementary school which numerous injured children,could your hospital handle the influx of worried parents? Howmany security officers would it take to secure every entranceat your facility? If you gave the orders right now to lock downyour hospital, how long would it take? Could you secure yourfacility within five minutes? Odds are, in a real event, you willhave less than five minutes after notification to prepare for theonslaught of patients.
Security is vital in protecting the facility from the rush of in-jured patients and the “worried well”, but could your hospi-tal actually be a target of terrorist activity? The attacks by theAl-Qaeda trained Chechens in Georgia have shown that hos-pitals are often considered as targets by terrorists. Chechenrebels have attacked hospitals both as primary and secondarytargets. What better way to completely decimate a communi-ty then to injure people and destroy the place where theywould be treated?
One of the biggest threats is also one of the hardest to protectagainst. The use of car bombs has proven an effective weaponthat is difficult to prevent. Most hospitals are designed to al-low for vehicles to pull up close to the building to facilitateloading and unloading passengers. How easy would it be fora car bomb to pull into your emergency department? Oddsare, they would be able to park within 20 feet of the entranceto your facility. More and more high-threat buildings beingbuilt are having counter-measures designed and installed todeter car bombs. Unfortunately, convenience is the price thatis paid for increased security to minimise this threat.
Decontamination
When was the last time that your staff unpacked all of the pa-tient decontamination equipment and practiced with it? Wehave had the opportunity to teach disaster decontaminationat several hospitals. It is always disheartening to see staff openup equipment that is several years old and still in the originalpackage. Our history has shown us that over half of the par-ticipants in these disaster preparation classes have never seentheir hospital’s decontamination equipment prior to the class.However, each of the participants in the class was already as-signed an active role in their hospital’s disaster response plan.
All personnel who have an active role in the disaster plan thatis outside of their normal daily duties should have routine train-ing. The complexity of their role should dictate the frequencyof their training. Personnel who have a complex role (i.e. pa-tient decontamination) should train at least quarterly on theirduties. At Spartanburg Regional Medical Center in Spartanburg,South Carolina (United States), the hospital emergency responseteam (HERT) is comprised of personnel from all disciplines.These personnel train often and are ready to respond at a mo-ment’s notice to threats to the facility of any level.
Surge Capacity
Surge capacity is the hospital’s ability to rapidly expand serv-ices in order to accommodate an unanticipated influx of pa-tients in the event of a large-scale event. Hospitals through-out the world are faced with daily staffing shortages. In manyplaces, hospital personnel are already providing care at sub-optimal patient care ratios. Hospitals are staffed based on dai-ly, anticipated capacity, not for the unusual. A study of hospi-tals in the Los Angeles, California (United States) area foundthat out of 45 area hospitals, almost all operated all constantfull capacity with very little ability to handle surge capacity.
To stress this point, the problem of “patient parking” has be-come more common in the United States. Patient parking oc-curs when an emergency department is too full to accept apatient, and does not allow the ambulance to offload the pa-tient, but instead requires the crew to wait with the patientuntil a bed is available. Patient parking has often times result-
Continued from page 7
Virginia Tech Shooting04/16/09The first student who was shot walked onto a city bus and took it to the local hospital. This patient arrived andimmediately created a security nightmare in the smallemergency department.
New York City Terrorist Attack09/11/01911 patients were received at the two closest hospitals,with 85% self-transporting.
Tokyo Subway Sarin Gas AttackMarch 20, 19955500 injuries, with 85% self-transporting. All patientsrequired chemical decontamination upon arrival at the hospital.
Figure 1. Recent Mass Casualty Incidents withPatient Self-Transport
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 43

44
ed in an ambulance waiting hours with patients for a bed tobecome free. This obviously has a massive negative impacton the abilities and efficiency of the ambulance service.
What is your daily surge capacity at your facility? Do youshare information each day with other local hospitals to seethe availability of beds in the event of a large disaster? If youdo not want to share this information with competing hos-pitals, do you send the information to a neutral third partysuch as the emergency services provider? The person(s) inthe community with the responsibility to manage disastermust have bed capacity information provided to them daily.
Evidence-based disaster medicine shows that for every pa-tient who arrives to the hospital with physical injuries, fivemore will arrive with psychological injuries (Hankins 2009).Most patients will self-present at the hospital within one hourof the incident.
The optimal method for predicting and preparing for hospi-tal surge capacity is not yet known. However, hospitals shouldstrive to prepare for a myriad of incidents that can occur intheir community that would produce multiple patients. It isalso hard to predict the disaster that may exhaust specific re-sources such as surgical suites, ventilators, or burn beds.Literature from previous mass casualty disasters shows thatthe majority of patients will be discharged from the hospi-tal within 24 – 72 hours following admission (Einav-Bromikerand Schecter 2009).
Reliability on External Resources
When we have provided disaster training, we have had theopportunity to review multiple hospitals’ disaster plans. Anall hazard plan that relies on outside agencies or resources tomitigate a disaster is a set up for failure. Many hospitals areunder the false impression that the local emergency servicesagency will be able to assist with patient decontamination in
the event of a large incident. If there is a large hazardous ma-terials incident, the emergency service’s primary obligationis to mitigate the incident. Fire department and ambulanceresources cannot be dedicated to assisting hospitals with de-contamination. If resources are available, emergency serviceagencies would be more than willing to assist, but they can-not be counted on in the disaster plan. Hospitals must be asself-sufficient as possible, and designed to operate for at leastseven days before receiving outside help.
Relationships
When a hospital or community suffers from a disaster, it isimperative that in addition to being self-sufficient, they mustalso have a working relationship with other facilities in thearea. These relationships may be with direct competitors andfacilities that are not typically encountered on a daily basis.By developing relationships in advance of a disaster, the callfor assistance made by your hospital in the event of disasterwill not be made to a stranger. It has been proven time andtime again that relationships forged in advance of a disastercan pay dividends in the event an actual disaster.
Disaster Drills
The Joint Commission on Accreditation of HealthcareOrganisations (JCAHO) requires all hospitals in the UnitedStates to test their emergency plan twice a year, including onecommunity-wide drill. The authors recently were involved asinstructors in a large community disaster drill. Every hospi-tal in the community was asked to participate in the drill. Itwas rather disheartening to hear several of the hospitals de-cline to participate in the drill with each offering the sameexcuse: “We are under-staffed. We can’t afford to send any-one to the drill, nor can any of the mock patients come toour facility.” What better way to test your ability to respondto a disaster then when you are already short staffed! Disasterdrills should be realistic as possible, and under-staffed hos-pitals are a very realistic issue!
Conclusion
In closing, disaster planning should encompass all legitimatethreats. Hospitals must consider the possibility of being a pri-mary target in terrorist operations. In order to limit the impactof a large-scale disaster, hospitals must have multiple systemsof redundancy to back up their critical infrastructures. Hospitalsmust also limit their reliance on outside agencies to providesupport during disasters. Ideally, hospitals should be complete-ly self-sufficient for a minimum of seven days. Hospitals mustroutinely train and drill participants on their roles and respon-sibilities in a disaster. By emphasising these core componentsof disaster management, hospitals minimise the impact to theiroperational abilities during a large-scale disaster.
• Arrival of patients to the hospital with no prior notice;• Patients will converge on either the closest hospital, or the locally most renowned hospital;
• Arrival of patients to the hospital who have not been previously triaged;
• Arrival of patients without prior decontamination;• Patients are placed in hospital rooms without staff being aware that they are contaminated;
• The least injured patients will arrive first, tying up valuable resources;
• Secondary decontamination of hospital staff, and• A significant delay in the hospital learning what chemical(s) are involved in the attack.
Figure 2. Evidence-Based Problems with Patient Self-Transport in WMD Events
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 44

45ICU Management 3-2008 45ICU Management 3-2008
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 45
Euroanaesthesia 2009
EUROANAESTHESIA 2009
Over its four days, around 5,500 delegatesattended. Most participants pre-registered,but around 15% registered on the day.Euroanaesthesia has a similar format tomost major medical conferences, in thatthere is a large industrial exhibition, withalmost 100 industrial stands and scientif-ic and educational content comprised ofrefresher course lectures, scientific up-dates, hands-on workshops, interactivesessions and abstract presentations.
Euroanaesthesia is a general conference,which aims to provide a broad range anddepth of content, with something foreveryone from novice to expert. The sci-entific programme is planned by a seriesof subcommittees covering fields as di-verse as paediatrics, respiration, intensivecare and ethics. A new subcommittee thisyear now covers peri-operative manage-ment of the elderly – an increasingly im-portant cohort of patients.
The Milano Convention Centre providedan excellent, spacious venue for the con-gress. As delegates have come to expect,the standard of speakers was high. The ESAdeliberately seeks new speakers, ratherthan relying on purely the well known.The result is a mix of speakers, some areundoubtedly world experts, and othersare likely to become world experts in afew years time.
Many of the delegates are able to come toEuroanaesthesia by virtue of the reducedrates available to abstract presenters. Closeto 800 abstracts were presented in poster
format; around 67% of submitted abstractsare accepted. The standard of poster pre-sentations is generally high and reportedstudies include full-scale trials, basic sci-ence and cohort studies. With presentersfrom all around the world, there was theoccasional language problem, but withgood humour and patience these wereusually overcome. The best 6 abstracts werepresented orally, with prizes for the topthree. The winner this year was MalinJonsson Fagerlund (Sweden) with a paperentitled: “The functional affinity forpropofol is dramatically decreased in hu-man α1β2(N290M)γ2 and α2β3 -(N290M) γ2 mutant GABAA receptors”.
Aside from the scientific presentations,delegates spent time browsing the indus-trial exhibition. Despite the economicdownturn, around 100 companies cameto the congress, again covering the wholeof anaesthesia and intensive care relatedpharmacology and technology. One of theinteresting aspects of returning to the samecongress is observing the subtle, or not sosubtle, ways in which industry changesthe way products are marketed. Non-in-vasive monitoring of cardiac output wasone of the rising stars this year, with es-tablished and new products vying for del-egates’ attention.
As well as the science and industrial ex-hibitions, Euroanaesthesia includes aprize giving ceremony. Every year, suc-cessful candidates of the EuropeanDiploma of Anaesthesiology and In -tensive Care are awarded their diploma.
This year was a special year: it is 25 yearssince the Diploma was founded, and theESA was pleased to be able to honour thisachievement. The EDA is actually believedto be the oldest surviving Europeanmedical diploma.
The Dräger company have sponsored aprize for the last few years for the best pa-per published by a European group in thefield of intensive care. This year there wasstrong competition. Following a very rig-orous approval process, the Dräger prizewas awarded to Peter Radermacher andthe Universitätsklinik für Anästhesiologie,Ulm, Germany for their paper: Effects ofventilation with 100% oxygen during ear-ly hyperdynamic porcine fecal peritoni-tis. Barth E, Bassi G, Maybauer DM et al.Critical Care Medicine; 2008;36:495-503.
Outside of the congress, delegates had theopportunity to explore the renaissancewonders and fashion of Milan. Eating outwas a pleasure, with fine food and drinkavailable in a multitude of restaurants andbars. The networking evening was aRenaissance themed event in the groundsof at the beautiful main state university ofMilan “Università degli Studi di Milano”.Delicious Italian specialities were servedfrom the generous buffet tables with en-tertainment provided by renaissancesingers, dancers and jugglers.
Overall the congress was judged a success,both by delegates and by the ESA. The ESAlooks forward to welcoming people to its2010 congress in Helsinki.
Dr. Iain MoppettConsultant AnaesthetistQueen’s Medical CentreNottingham University HospitalsNottingham, UKNewsletter Editor European Society of Anaesthesiology
46
Euroanaesthesia 2009, the annual scientific meeting ofthe European Society of Anaesthesiology, took place atthe beginning of June in the Milano Convention Centre,the largest convention centre in Italy.
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 46
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 47

ICU Management 3-2008
In our Next Issue
ICU Management is the Official Management and Practice Journal of the International Symposium on Intensive Care and Emergency Medicine.
EDITOR-IN CHIEFJean-Louis Vincent, Head, Department of Intensive Care, Erasme Hospital, Free University of Brussels, Belgium [email protected]
EDITORIAL BOARDProf. Antonio Artigas (Spain) [email protected]. Richard Beale (United Kingdom) [email protected]. Julian Bion (United Kingdom) [email protected]. Todd Dorman (United States) [email protected]. Hans Kristian Flaatten (Norway) [email protected]. Luciano Gattinoni (Italy) [email protected]. Armand Girbes (Netherlands) [email protected]. Jeff Lipman (Australia) [email protected] Prof. Konrad Reinhart (Germany) [email protected]. Paolo Pelosi (Italy) [email protected]. Peter Pronovost (United States) [email protected]. Jukka Takala (Switzerland) [email protected]
NATIONAL CORRESPONDENTSDr. Maurizia Capuzzo (Italy) [email protected] Danjoux (Canada) [email protected]. David Edbrooke (United Kingdom) [email protected]. Dominique Vandijck (Belgium) [email protected]
MANAGING EDITORSherry Scharff [email protected]
SCIENTIFIC EDITORDr. Sonya Miller [email protected]
EDITORLee Campbell
EUROPEAN AFFAIRS EDITORSSonja Planitzer [email protected]
GUEST AUTHORSM.K. Bader, S. Chandolu, M. Clumpner, A. Hedelin, A. Khorram-Manesh, R. Korupolu, M. Malbrain, J. Mobley, I. Moppett, D. Needham, P. Örtenwall, G. F. Vazquez de Anda, M. Wahl, Y. G. Weiss, Y. Weiss
ICU MANAGEMENT IS PUBLISHED BYEMC Consulting Group28, rue de la Loi, B-1040 Bruxelles, BelgiumE-mail: [email protected]: www.icu-management.org
PUBLISHER AND CEOChristian Marolt [email protected]
MEDIA CONTACT, MARKETING, ADVERTISINGKatya Mitreva [email protected]
SUBSCRIPTION RATESOne year Europe 53 Euros
Overseas 68 EurosTwo years Europe 89 Euros
Overseas 105 Euros
Note: Participants of the International Symposium on Intensive Care and Emergency Medicine receive a one year subscription as part of their symposium fee.
ARTWORKAleksander Bugge [email protected]
PRODUCTION AND PRINTINGTotal circulation: 7,085 ISSN = 1377-7564
© ICU Management is published quarterly. The publisher is to be notified of cancellations six weeksbefore the end of the subscription. The reproduction of (parts of) articles without consent of the pub-lisher is prohibited. The publisher does not accept liability for unsolicited materials. The publisherretains the right to republish all contributions and submitted material via the Internet and other media.
LEGAL DISCLAIMERThe Publishers, Editor-in-Chief, Editorial Board, Correspondents and Editors make every effort to see thatno inaccurate or misleading data, opinion or statement appears in this publication. All data and opin-ions appearing in the articles and advertisements herein are the sole responsibility of the contributor oradvertiser concerned. Therefore the publishers, Editor-in-Chief, Editorial Board, Correspondents, Editorsand their respective employees accept no liability whatsoever for the consequences of any such inaccu-rate or misleading data, opinion or statement.
REFERENCESReferences cited in this journal are provided to EMC Consulting Group by the authors and areavailable on request at [email protected].
AGENDA
Letters to the Editor & Requests for References Cited in ICU [email protected]
NOVEMBER 2009
11-13 The Critical Care Canada Forum 2009 Toronto, Canadawww.cr iticalcarecanda.com
17-19 Echocardiography CourseBrussels, Belgiumwww.intensive.o rg
DECEMBER 2009
1-3 15th Postgraduate Refresher CourseBrussels, Belgiumwww.intensive.o rg
13-16 Update on Haemodynamic Monitoring Rome, Italywww.intensive.o rg
FEBRUARY 2010
5-6 15th International Symposium on Infections in the Critically Ill Patient Barcelona, Spainwww.infections-online.com
JANUARY 2010
9-13 Society of Critical Care Medicine’s (SCCM) 39th Critical Care CongressMiami Beach, Florida, USAwww.sccm.o rg
MARCH 2010
9-12 30th ISICEMBrussels, Belgium (Back to Brussels Congress Center: THE SQUARE)www.intensive.o rg
JUNE 2010
8-11 19th International Vicenza Course on Critical Care NephrologyVicenza, Italywww.nefro lo giav icenza.it
12-15 Euroanaesthesia 2010Helsinki, Finlandwww.euroanaesthesia.org
OCTOBER 2010
1-2 World Conference on Portable, Wearable and Miniaturized Dialysis Systems Vicenza, Italywww.nefro lo giav icenza.it
10-13 23rd Annual Congress ESICMBarcelona, Spainwww.esicm.o rg
Verified Circulationaccording to the standards of InternationalBusiness Press Audits
ICU Management is independently auditedby Accountskantoor Closset on behalf ofInternational Symposium on Intensive Careand Emergency Medicine
COVER STORY-OBESITY
THE MOBILITY SERIES: PART TWO
AUTOMATED HAND HYGIENE MONITORING
PRODUCT COMPARISON CHART-INTENSIVE CARE VENTILATORS
COUNTRY FOCUS -BELGIUM
CONGRESS PREVIEWS AND REVIEWS AND MUCH MORE…
ICU_V9_I3_Proof1:Layout 1 29/09/09 09:59 Page 48

ICU_V9_I3_Cover10_with_correct_ads:ICU 29/09/09 09:55 Page 4

ICU_V9_I3_Cover10_with_correct_ads:ICU 29/09/09 09:55 Page 1