digital healthcare strategy - nhs croydon · pdf filecroydon clinical commissioning group...
TRANSCRIPT
Digital Healthcare Strategy 2015 - 2020
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-20
Amendment history:
Version Date Amendment
V0.1 12/10/2015 Outline document created
V0.2 17/11/2015 Document populated
V0.3 18/11/2015 Internal HRC review and update
Approvals:
Name Lead Date of Review Date of sign-
off
Version
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
1
Contents
1. Executive Summary ....................................................................................................................................... 3
2. Introduction ................................................................................................................................................... 5
2.1. Purpose of this document ...................................................................................................................... 5
2.2. Process used for the development of this strategy ................................................................................ 5
3. Strategic Context ........................................................................................................................................... 6
3.1. National context ..................................................................................................................................... 6
3.1.1. The Five Year Forward View (FYFV) and the role of IM&T .............................................................. 6
3.1.2. Implementing the Five Year Forward View – Local Digital Roadmaps ............................................ 7
3.1.3. Local Digital Roadmaps .................................................................................................................... 7
3.1.4. Outcome Based Commissioning (OBC) ............................................................................................ 8
3.1.5. Integrated care and population health ........................................................................................... 9
3.2. Local context ........................................................................................................................................... 9
3.2.1. Croydon Clinical Commissioning Group .......................................................................................... 9
3.2.2. Croydon’s Population .................................................................................................................... 11
3.2.3. Commissioning .............................................................................................................................. 11
3.2.4. General Practice ............................................................................................................................ 12
3.3. Local and regional integrated care initiatives ...................................................................................... 13
4. Stakeholder Analysis .................................................................................................................................... 14
5. Current IM&T Environment ......................................................................................................................... 16
5.1. Commissioning Support Service (CSU) ................................................................................................. 16
5.1.1. CSU services ................................................................................................................................... 16
5.1.2. Business Intelligence ..................................................................................................................... 16
5.2. Primary Care ......................................................................................................................................... 17
5.2.1. Primary Care Systems .................................................................................................................... 17
5.2.2. Medicines Optimisation and Variation Teams .............................................................................. 18
5.2.3. Mobile and remote access ............................................................................................................ 19
5.2.4. Infrastructure and hardware ......................................................................................................... 19
5.3. CCG IM&T environment ....................................................................................................................... 19
5.4. IM&T in the local healthcare economy ................................................................................................ 20
5.5. Summary of current IM&T environment .............................................................................................. 21
6. Vision and strategic objectives .................................................................................................................... 22
6.1. Vision and Mission ................................................................................................................................ 22
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
2
6.2. IM&T strategic objectives ..................................................................................................................... 22
6.2.1. Objective one - Utilising IM&T to improve integration and quality of care across the health
economy .................................................................................................................................................. 23
6.2.2. Objective two - Sharing of patient information across provider organisations ............................ 23
6.2.3. Objective three - Technology to promote wellness and engage and empower the people of
Croydon ................................................................................................................................................... 26
6.2.4. Objective four – Business Intelligence to understand population needs, and manage contracts 27
6.2.5. Objective five – Provision of robust infrastructure and IM&T support ......................................... 28
6.2.6. Objective six – Optimise, standardise and integrate GP software to support clinical knowledge
and decision making ................................................................................................................................ 29
6.2.7. Objective seven - Improving the satisfaction and productivity of the workforce through
information and digital technology ......................................................................................................... 30
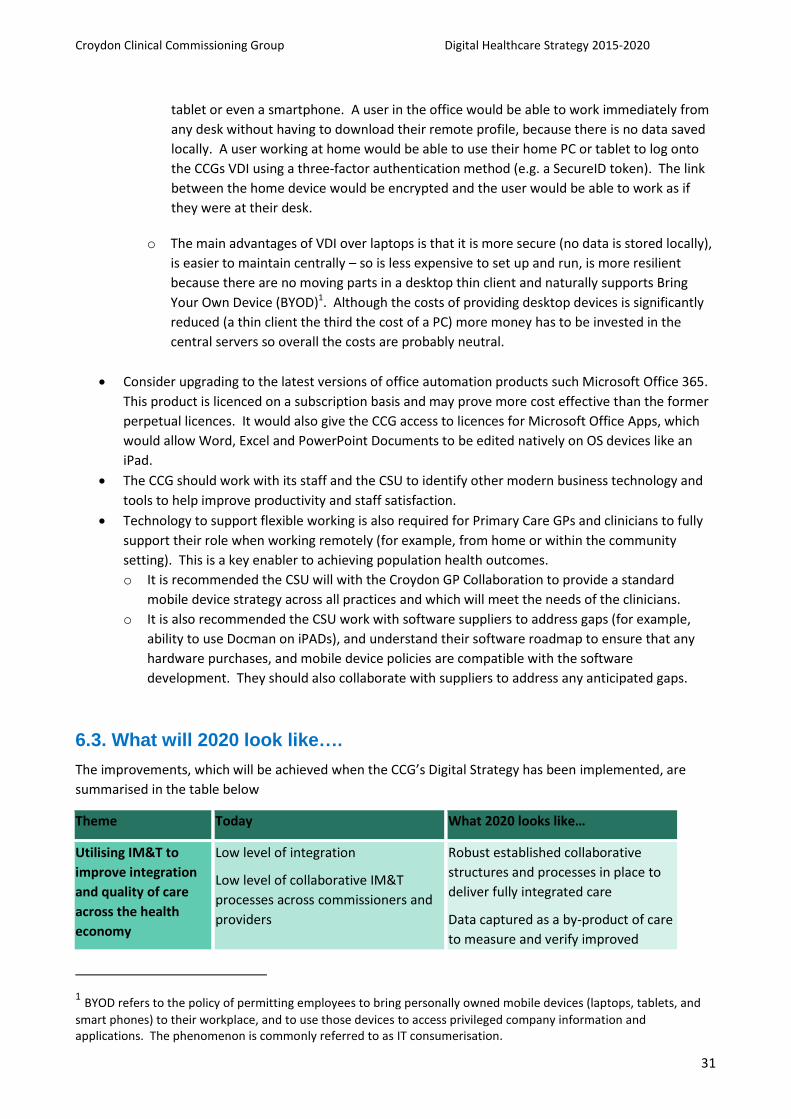
6.3. What will 2020 look like…. .................................................................................................................... 31
7. Action and implementation plan ................................................................................................................. 34
8. Conclusion ................................................................................................................................................... 35
Appendix A – Governance ............................................................................................................................... 36
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
3
1. Executive Summary
The Croydon Clinical Commissioning Group (CCG) was established in 2013 and provides services for a large
and diverse population in south west London. The CCG represents 57 practices and six GP networks
providing the clinical leadership which is instrumental in achieving the goals of the CCG, GPs, and their
provider partners.
NHS England’s Five Year Forward View highlights the role digital and information technology will play in
transforming the NHS to meet the challenges ahead. CCGs nationally have been handed the responsibility
of coordinating and driving forward Local Digital Roadmaps. Croydon CCG has a significant task, and a
strong opportunity in undertaking this role.
This is the first Digital Healthcare Strategy produced by the CCG. The executive leadership and board
members recognise the important role IM&T will play in ensuring success of the borough’s integrated care,
and outcomes based commissioning goals. This strategy sets out to deliver against these ambitious goals.
This Digital Healthcare Strategy demonstrates the role information and digital technology will play in the
delivery of improved population health outcomes for the people of Croydon for the next five years. The
strategy explores both the national and local strategic context for IM&T and also engages with the needs
and aspirations of partners and stakeholders.
Croydon’s strategic vision for IM&T is to:
use the power of intelligent information and digital technology
to achieve:
Longer healthier lives for all the people in Croydon
Through an ambitious programme of innovation and by working together with the
diverse communities of Croydon and with our partners, we will use resources wisely to
transform healthcare to help people look after themselves, and when people do need
care they will be able to access high quality services
The strategy outlines seven key strategic objectives to meet this vision. The first is an overarching goal for
IM&T to support the CCG’s integrated care, quality and health outcome goals. The remaining six provide
core objectives to support and enable this objective to be achieved. The seven objectives are:
Overarching goal:
1. Utilising IM&T to improve integration and quality of care across the health economy
Core supporting objectives to achieve this goal are:
2. Sharing of patient information across provider organisations
3. Technology to promote wellness and engage and empower the people of Croydon
4. Business intelligence to understand population needs, and manage contracts
Enabling objectives:
5. Provision of robust infrastructure and IM&T support
6. Optimise, standardise and integrate GP software to support clinical knowledge and
decision making

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
4
7. Improving the satisfaction and productivity of the workforce through information and
digital technology
An action plan is set out in section seven which outlines key developments over the next five years to
deliver the structures and processes required to implement the strategy. The CCG will be required to
rapidly put in place the foundations of this strategy in order to meet Digital Roadmap and Outcome Based
Commissioning timelines.
In conclusion, this strategy aims to ensure that CCG has the appropriate structures in place as they embark
on a progressive integrated care and commissioning programme. The strategy aims to achieve the
population health goals of Croydon while also aligning with the goals of local, regional and national
initiatives.
The importance of communication, intelligent data, and digital technology to support these collaborative
goals cannot be understated. The strategy strongly recommends that the CCG invests in and drives forward
additional structures and roles to support the successful delivery of this Digital Healthcare Strategy. It is
also recommends that the strategy is refreshed on annual basis over the next five years to reflect the fast
changing pace of technology and healthcare.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
5
2. Introduction
Croydon CCG is responsible for commissioning the health services for a diverse, growing and challenging
population. It supports one of the largest number of GP practices of any CCG in London, while continuing to
manage the significant shortfall it inherited at its inception in 2013. The CCG, along with its provider
partners, has recently adopted new and forward thinking commissioning goals by moving to an Outcome
Based Commissioning approach for people aged over 65.
This is the first IM&T strategy produced by the CCG. Existing IM&T initiatives have focused on provision of
technology and information to support GPs in their practices. This strategy aims to build on this base and
create a solid environment for supporting the integration and quality improvement goals of the CCG.
2.1. Purpose of this document
This documents sets out NHS Croydon CCG’s high-level vision for the future of IT for health and social care
across Croydon for the next five years. It identifies the strategic objectives to be achieved in order to fulfil
that vision. The document will inform the CCG’s Digital Roadmap for the local health economy which is
required to be submitted to NHS England in April 2016. It will also inform the organisation’s Strategic and
Operational plans.
The IM&T Strategic Vision illustrates how digital technology can help support the CCG in its commissioning
goals, and as an enabler of transformational change in service delivery over the next five years.
The target audience for the document includes the CCG’s senior management, CGG governing board
members, and senior primary and secondary care clinicians within Croydon.
2.2. Process used for the development of this strategy
The strategy has been produced based on the following inputs:
National policy and guidance in relation to healthcare IM&T
Strategic documentation produced by the CCG and local healthcare economy
Interviews conducted with over twenty local individual stakeholders
A Strategic vision and objectives workshop with senior primary care and CCG personnel
The process used for the development of this strategy is summarised in the diagram below:
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
6
3. Strategic Context
This section describes the context in which the CCG operates and identifies the key strategic drivers at a
national, regional and local level.
3.1. National context
3.1.1. The Five Year Forward View (FYFV) and the role of IM&T
In October 2014, NHS England produced Five Year Forward View (FYFV). This sets out a clear view of the
challenges ahead, why change is needed, and what change might look like. It outlines a vision to address
the challenges facing the NHS, and to drive better patient outcomes.
The estimated £30 billion gap in NHS funding predicted to appear by 2020-21 could be closed completely if
the health service develops new, more efficient care models. Digital and information technology is a key
enabler to deliver this transformed future for the benefit of every service user, carer, citizen and
professional.
The Five Year Forward View states that the biggest challenges the NHS is facing remains:
1. changes in patient health needs and personal preferences;
2. changes in treatments, technology and care delivery and the need to provide care that is genuinely
co-ordinated around what people need and want; and
3. changes to funding continued decline in funding growth.
Some key themes that need to be addressed to overcome these challenges are outlined below:
Quality – recent reports into quality of NHS care have all called for a truly patient focussed culture, greater
transparency and more rigorous management of standards. The FYFV continues the focus on quality
stating that NHS organisations must narrow the gap between the best and the worst whilst raising the bar
for all.
Prevention - As populations are living longer with more chronic health conditions, communities must work
toward reducing causes of preventable illness such as obesity and lifestyle risks. Organisations must
successfully incentivise and support healthier behaviours then we can prevent ill health and increasing
demands on healthcare. The FYFV focusses on targeted prevention, supporting a healthier workforce and
working across healthcare partners to enable local, democratic leadership.
CCGs have been asked to work with local government partners to set goals to reduce local health and healthcare inequalities and improve outcomes for health and wellbeing. This includes specifying agreed actions, interventions and metrics, in line with NICE guidance, with respect to patient and staff lifestyle factors.
Patients and communities- The FYFV builds on the Government’s vision of an NHS that puts patients and
the public first, where “no decision about me, without me” is the norm. It states that patients must have
more access to their healthcare information, increased control over the care that is provided to them, and
more support in managing their own health. The wider community, including carers, third sector and
citizens, also play a vital role and must be engaged in new ways to support the challenges ahead.
New models of care - Over the next 5 years and beyond the NHS will increasingly need to flex its traditional
care boundaries to support truly integrated, patient centred care. The FYFV defines its own view of what
healthcare should look like over the next 5 years and introduces new organisational types and care models
including:
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
7
Leadership and workforce - Radical change, can only be achieved with the leadership and people to make
it happen. Greater support is needed to help mobilise leaders and workforces to work differently, develop
the newly needed skills, values, behaviours and numbers to deliver the improvements needed.
Efficiency and productivity - By 2015, the NHS needs to make savings of £20 billion with an additional £30
billion required by 2021. It has been estimated that funding growth will remain at 1.2% per annum, which
will be half of what is needed to fund future services. With the Better Care Fund shifting a significant
amount of NHS funding to Social Care in 2015/16, the financial future of the NHS is increasingly challenging.
Greater efficiency and productivity is key to delivering the NHS vision for the future as demand increases
and funding decreases.
Health innovation - The FYFV highlights the need for health innovation in relation to research, personalised care, accelerated innovation in ways of delivering clinical care such as apps and telemedicine.
Information and technology – The FYFV focusses heavily on the importance of information and technology in achieving the required changes the NHS has to make. It talks of a national focus on key systems that will provide the ‘electronic glue’ to enable different parts of the NHS to work better together. Key elements include:
comprehensive transparency of performance data;
expanding set of NHS accredited health apps to support digital inclusion;
fully interoperable electronic health records continuing the move towards paperless;
family Dr appointments and prescriptions online, everywhere;
better audit data;
increased focus on technology including smart phones; and
support to help build capacity and help those unwilling or unable to use technology.
3.1.2. Implementing the Five Year Forward View – Local Digital Roadmaps
NHS England has subsequently released guidance and frameworks for organisations to achieve the goals
outlined in the FYFV. The National Information Board (NIB) published a framework outlining proposals to
transform outcomes for patients and the wider population. The Board plans to issue a set of road maps
and standards which will provide a more detailed approach to transforming digital care. Key milestones
include:
from March 2015, all citizens will have online access to their GP records;
by 2017, 100,000 individual genomes will have been sequenced;
by 2018, clinicians in primary care, urgent and emergency care and other key transitions of care contexts will be operating without the use of paper records;
by 2020, all care records will be digital real-time and interoperable.
3.1.3. Local Digital Roadmaps
The NIB Framework for Action calls for CCGs to produce digital roadmaps outlining how their local health and care economies will achieve the ambition of being paper-free at the point of care by 2020. CCGs will be required to submit their plans in April 2016, as part of the annual Clinical Commissioning Group
planning process. Commissioners have been asked to take a lead on coordinating and collaborating with their neighbouring providers to dissolve the artificial barriers between care settings, and between healthcare professionals.
The local digital roadmaps will provide a means for the CCG to communicate plans to local stakeholders and inform local service transformation, commissioning and investment strategies. The most recently published timelines for digital roadmap activities are shown below but are regularly updated.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
8
3.1.4. Outcome Based Commissioning (OBC)
In answer to many of the challenges outlined above, commissioners are taking the opportunity to improve local health and care systems by developing new and innovative commissioning partnerships to support integrated care. Commissioners are moving away from traditional commissioning models towards an outcome based commissioning approach.
Traditional commissioning tends to focus on processes such as payment for activity or organisational performance. With outcome based commissioning, health and care services are paid for based on achieving outcomes that are important to service users.
OBC is interested in net productivity based on outcomes in relation to the resources used - an approach which aligns with the FYFV’s focus on efficiency gains. The King’s fund paper, Commissioning and Contracting for Integrated Care identifies some of the more common contractual outcomes including:
patient experience and satisfaction with services
early detection and intervention, to support people to recover and stay well
supporting people to manage their condition, and increasing patient involvement in decision-making
improved patient outcomes (including survival rates)
reducing emergency admissions to hospital
delivery of co-ordinated and patient-centred care, demonstrating joined-up working
effective information-sharing, including use of technology
It is clear from these examples that information management and technology will play a significant part in supporting organisations to achieve OBC. Identifying the supporting data elements, and technology platforms will need to play a key part in contract negotiations and redesign of services. The high level implications of OBC for IM&T are:
pooling of population, patient, service and finance data to measure outcomes and report against contracts;
health intelligence platforms to support the detection and early intervention of illness;
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
9
technology to support data collection across the continuum of care;
data sharing to support co-ordination of patient centred care;
business intelligence platforms to support benchmarking, data analysis, reporting and predictive modelling; and
innovative technology to engage and empower patients.
3.1.5. Integrated care and population health
Integrated care has become a central theme to health service reform in recent years due to the changing burden of disease and decreasing health and social care budgets outlined above. Integration of services through policy initiatives such as amendments to the Health and Social Care Bill, and the establishment of the Better Care Fund, have made some progress towards coordinating care of older people and those with complex needs.
Integrated care has seen benefits such as allowing people to live independently in their own home, and reducing use of hospital services. However, these efforts have not yet extended to the broader health of local populations.
Population health aims to achieve a wider co-ordination across a geographical population. It requires partnerships across many sectors to integrate investments and policies in order to improve the health of a total population.
Access to traditional health and services plays an important part in the health of a population, however evidence indicates that it is not as important as lifestyle, the influence of the local environment and the wider determinants of health. With population health, accountability is spread across the community and not just within the boundaries of health and care services.
The paper, Population Health Systems – Going Beyond Integrated Care, (The Kings Fund, February 2015) sees integrated care as part of a broader shift to population health and cites evidence such as the large and avoidable differences in health outcomes between social groups, increase in co-morbidity increasing with deprivation, and the clear link between morbidities and lifestyle.
A number of countries outside the UK have begun to make this shift from integrated care to population health and these all share similarities:
At the macro level organisations work together across systems to improve health outcomes across a whole population. Specific interventions target the most deprived group. In contrast integrated care models tend to target frequent service users.
At the meso level people with similar needs are grouped together and services and interventions are tailored accordingly. This requires population segmentation and risk stratification to identify the needs of different groups, and systems within systems to focus on the various groups.
At the micro level, population health systems deliver a range of interventions aimed at improving the health of individuals and involve a range of varied services. This includes integrated health records to co-ordinate peoples care services, “scaled up” primary care services to co-ordinate effectively with other services.
3.2. Local context
3.2.1. Croydon Clinical Commissioning Group
NHS Croydon Clinical Commissioning Group (Croydon CCG) was established in April 2013. The CCG inherited a
significant financial shortfall of £33.9m which is evident in the historical underinvestment in certain services and
infrastructure.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
10
The CCG’s vision for “longer healthier lives for all the people in Croydon” is being delivered by transforming
services that provide safe, effective, high quality, patient centred services through clinically-led, innovative re-
design.
In 2015 NHS Croydon CCG agreed the following aims:
develop as a mature membership organisation;
commission integrated safe, high quality services in the right place at the right time;
have collaborative relationships to ensure an integrated approach; and
achieve financial balance over five year.
The CCG has responsibility for planning, buying and monitoring most local health services, including:
outpatient appointments and planned operations (planned hospital care);
urgent and emergency care (including out of hours services);
rehabilitative care;
maternity services;
community health services (for example physiotherapy and district nursing);
mental health services;
services for people with disabilities; and
prescribing by member practices.
To ensure they make the best use of resources the CCG is embarking on a programme of transformational
change through:
prevention, self-care, shared decision making;
outcomes based commissioning;
transforming adult community services;
improve integration of care;
reducing unwarranted primary care variation; and
whole system redesign.
Some of the key local service providers are Croydon Health Services NHS Trust, St George’s Healthcare NHS
Trust, The Royal Marsden NHS Foundation Trust, South London and Maudsley NHS Foundation Trust, Care UK
and Virgin Care.
Priority outcomes
The CCG has identified the following priority outcomes based local service challenges and on population needs
identified through the Joint Strategic Needs Assessment:
Reducing potential years of life lost through disease;
Ensuring people are seen in the right place at the right time;
Children and young people reach their full potential;
Increased independence; and
Positive patient experience.
The CCG also focuses on the following long term needs of their population:
Cardiology;
Chronic Obstructive Pulmonary Disease (COPD);
Diabetes;
Cancer;
Mental Health including Dementia; and
Children and Young Adults.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
11
3.2.2. Croydon’s Population
Health and care services in Croydon face the challenge of a growing and diverse population. In addition to
the national trend of an aging population, Croydon also expects an increase in the number of young people
due to the high birth rate and the effects of immigration.
395,000 people are registered with a GP in Croydon and based on current projections; the population of
Croydon will increase by 9.2% over the next ten years, and by 16.8% over the next 20 years. The number of
people aged over 65 is expected to increase by around two-thirds by 2030.
Over half of the population of Croydon would identify themselves as being from an ethnic group other than
“White-British” and this rate is expected to increase. Over 100 languages are spoken as a first language by
patients registered with Croydon GPs.
Croydon also has a high number of care homes. Croydon has 144 care homes that are registered with the
Care Quality Commission (CQC), with a maximum capacity to care for 2,796 people.
Health of the population
The health of the population is complex and mixed when compared to the English average. For example:
Life expectancy is higher than average, but significantly lower for people in the most deprived area
of the borough.
Deprivation is lower than average, but growing at a higher rate than surrounding boroughs.
There is a higher need for mental health inpatient services than comparative boroughs and the
number of people with mental health support needs is increasing.
Lifestyle factors are a concern - an estimated 62% of adults are overweight or obese, and 17% of
residents are smokers.
The borough has a high number of looked after children including over 400 unaccompanied
asylum-seeking children.
The prevalence of diagnosed diabetes in Croydon is 6.5 % is significantly higher compared to the
rest of London or England.
Breast and cervical cancer screening rates are both significantly worse than the national average.
The transformation of healthcare services provided by the CCG reflect this current and evolving
demographic picture.
3.2.3. Commissioning
The CCG have been transforming local healthcare services for two years through clinically-led, innovative re-
design of services and are developing models of care planned and co-ordinated around the needs of patients
and their families.
Croydon’s Outcomes Based Commissioning approach
Croydon CCG and Croydon Council have jointly developed an ‘Outcomes Based Commissioning’ approach to
buying health and social care services for people of Croydon over the age of 65. The capitated payment
mechanism allows both organisations to jointly buy services in a way that incentivises preventative and
proactive care and keeps people, and improves outcomes for the population.
The scope of the OBC includes people aged 65 and over registered with a Croydon GP. The contract will initially
focus on planned and unplanned acute care, community, out of hospital services, continuing care, prescribing
and older people mental health services, but to achieve the outcomes envisioned, the providers will need to
work collaboratively across health and social care services.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
12
Providers have together formed a legal entity called the Accountable Provider Alliance (APA) to meet this need.
The APA consists of:
Age UK (Croydon);
Croydon Council (Social Care);
Croydon Health Services NHS Trust;
GP Federation; and
South London and Maudsley NHS Foundation Trust.
3.2.4. General Practice
The Croydon CCG consists of 57 GP practices across Croydon. There are six geographically based networks of
practices are each led by a GP Clinical Lead and supported by network co-ordinators. These networks are:
East Croydon Network
Mayday Network
New Addington/Selsdon Network
Purley Network
Thornton Heath Network
Woodside/Shirley Network
In addition to this the Clinical Leadership Group (CLG) provides clinical and corporate support to the CCG’s
Governing Body, by driving key development and implementation of plans.
The Croydon GP Collaborative
GPs in Croydon have recently converged under a new organisation to provide services at a greater scale
than is often possible at individual GP practice level. This move has been driven by the strategic need for to

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
13
ensure that GPs have the capacity to meet current and future demand and deliver a comprehensive, high
quality service for the whole Croydon population. In addition, GPs need to ensure they are in position to
meet commissioning requirements, GPSoC Standards and LMA obligations.
3.3. Local and regional integrated care initiatives
Better Health for London
Better Health for London aims to work toward London becoming the world’s healthiest major city. It consists of
the joint partnership of The Mayor of London, NHS England, Public Health England, London Councils and the 32
GP-led clinical commissioning groups. Partners will align the objectives and aims of health and wellbeing
strategies to achieve a common goal.
South West London Collaborative Commissioning
The six south west London CCGs (Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth) and NHS
England, came together in April 2014 to work under the umbrella name of South West London Collaborative
Commissioning (SWLCC). The CCGs are working together as SWLCC on a long-term plan to improve the quality
of care in South West London for the benefit of patients and people of the area, and jointly developed
commissioning intentions for 2015/16. This focusses on the priority work areas outlined in the five year
strategy. Developing an IM&T Strategy to support this shared goal has been a key aim of the collaborative.
Integrated commissioning unit (ICU)
The CCG launched the ICU in partnership with Croydon Council in April 2014. The ICU has brought together
commissioning support functions in relation to services for children, mental health, learning disabilities and
vulnerable older people. The joint approach aims to improve the quality of local services, and to achieve results
more efficiently whilst combining commissioning resources. The Better Care Fund will build on this joint working
to achieve its goals and aims, and will provide Croydon will total £21.5m for 2015-16.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
14
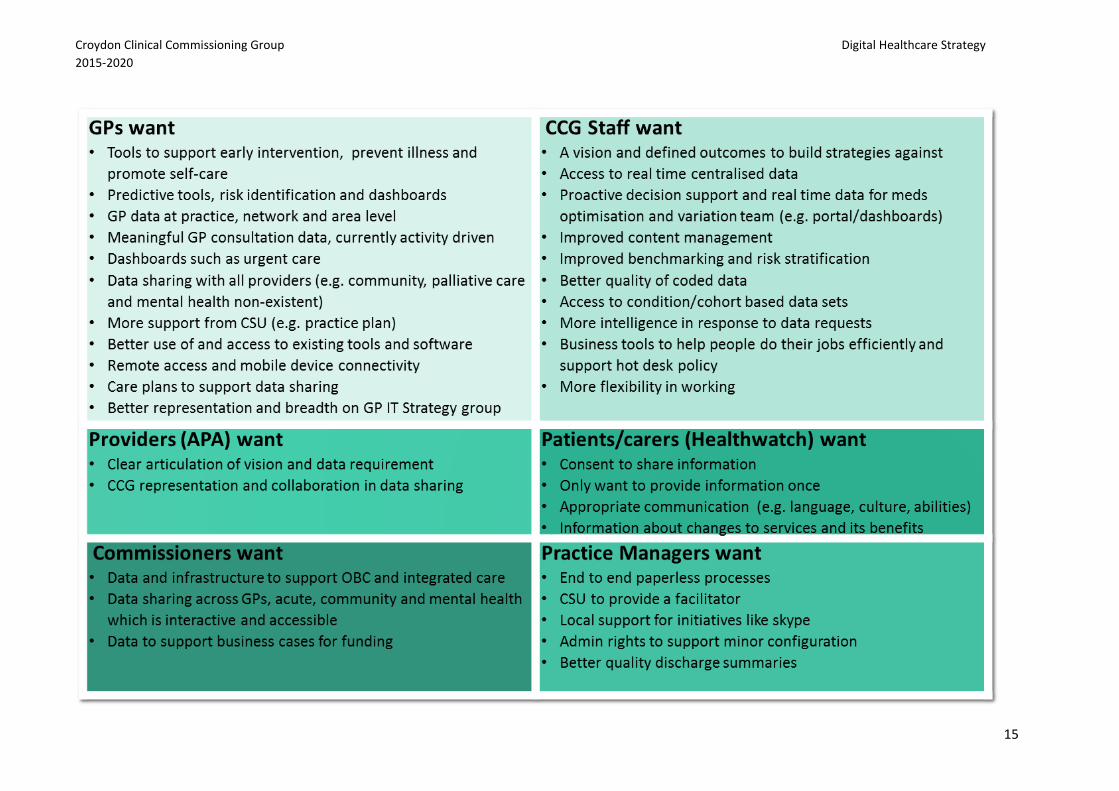
4. Stakeholder Analysis
Stakeholder engagement interviews were held with local stakeholder groups to ensure all perspectives
were considered during development of the strategy and to understand key strategic themes.
CCG management and board members;
General Practitioners and practice staff;
CCG staff;
Patient advocacy group, Healthwatch;
Accountable Care Provider (APA) representatives including NHS Croydon Health Services;
Local Health Authority;
Commissioning Support Unit (CSU);
Croydon GP Collaboration; and
South West London Commissioning Collaboration.
Findings of the interviews are summarised in the table below (not listed in any order):
Croydon Clinical Commissioning Group Digital Healthcare Strategy
2015-2020
15

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
16
5. Current IM&T Environment
This section describes the current status of the CCGs IM&T environment, capacity and capabilities. This
information has primarily been sourced from stakeholder interviews.
5.1. Commissioning Support Service (CSU)
Currently all IM&T services for Croydon CCG and Primary Care IM&T are outsourced to the South East
Commissioning Support Unit (CSU). There are no IM&T services or functions provided in-house apart from
an oversight role through the CCG’s Director of Quality and Governance.
This review also found that prior to development of this strategy there has been no IM&T strategy or
strategy function in place for either the GPs or the CCG.
5.1.1. CSU services
The CSU provides a wide range of IM&T services including:
service desk support (hardware and software);
infrastructure;
software and hardware licencing;
information governance (IG) guidance and support;
telephony;
procurement and supplier management;
business intelligence (BI); and
transformation and redesign.
The CCG relies on the CSU for a range of services. The CCG most recent large project provided by the CSU
was to upgrade GP practices to Microsoft Windows 7.
Satisfaction with help desk services from the CSU is variable but most stakeholders felt that there were
opportunities for improvement. The CCG is committed to outsourcing their IM&T and there is a desire to
create a successful technology partnership with the CSU.
5.1.2. Business Intelligence
Business Intelligence is a critical service for the CCG. They are dependent on analytics to understand the
health needs of their population, and to manage and monitor contracts – both core functions of their
business. The CCG has a contract in place to receive additional services from the CSU’s BI team. A
dedicated team of data analysts provide data and analytics based on CCG requests for data. CCG staff also
have access to data cubes to analyse data themselves.
Feedback from the stakeholder interviews raised a number of gaps in relation to provision of Business
Intelligence. These included:
misalignment between CCG and BI team understanding of priorities and output of BI requests;
underutilisation of the Data Cube query tool by CCG staff;
lack of standardised and centralised primary care data;
breadth of data – data is primary and secondary care focused with very little mental health or
community data and these cannot currently be linked (for example, for purpose of tracking
outcomes);
GP and secondary data is activity based (for example, QOF and CDS), not meaningful or outcomes
based
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
17
ability to derive cohorts or registers of data is limited;
benchmarking data is available but not utilised fully;
more agile development of real-time dashboards is needed for clinicians and managers; and
data analytics requirements are lacking for OBC.
5.2. Primary Care
Croydon GPs have been moving towards use of a single primary care system, EMIS, across the borough as a
result of individual practice choice. However, even across practices using EMIS, there are non-standardised
workflows and utilisation producing variation in outputs (for example, data and coding). This variation is
greater between EMIS and non-EMIS practices. Non-standardisation in the use of systems has contributed
to some of the variations found in benchmarking and performance data.
Historical underinvestment in IM&T strategy has meant that there is not a single strategic approach to the
selection and purchasing of IM&T solutions. This has led to issues with the deployment and adoption of
some GP software solutions. They are not perceived to be fully meeting the needs of the GPs, or value for
money.
5.2.1. Primary Care Systems
The following clinical systems are currently in use:
GP Clinical Systems – Through the national General Practice Systems of Choice (GPSoC) scheme
Croydon’s GPs can choose which clinical system the wish to use. An increasing number of practices
(approximately 90%) are using EMIS Web and the remaining practices using InPractice Systems
(InPS). It is believed that more practices will move to an EMIS as the practices organise themselves
to deliver services seven days a week and look for other opportunities to exploit economies of
scale.
Docman - Docman is a document management system, which integrates with the GP clinical
systems. It is used for receiving, editing, sharing, storing and viewing documents, including
electronic letters and discharge summaries from secondary care. The workflow also encompasses
automatic patient identification, filing and a coding tool. Docman is regarded positively by GPs and
practice staff but is not used consistently across Croydon practices.
GPs and practice staff have indicated dissatisfaction with quality of discharge summaries as one
reason for disengagement with Docman. However, feedback also indicated that discharge
summaries are improving, and there are opportunities for this to improve further now that
Croydon Health Services are released from the National Program for IT (NPfIT).
Sunquest ICE – ICE is used for pathology requesting and has recently been extended to requesting 2
week wait cancer referrals. This has not been well received by GPs due to lack of consultation,
duplication of data entry and deviation from existing workflows and data flows.
National Systems - The National e-Referral and Electronic Prescription Services are in use at most
practices.
Clinical Decision Support – The CCG has recently implemented DXS, a point of care Clinical Decision
Support System (CDSS) which allows CCGs to manage and distribute decision support information
to primary care users. The software is designed to equip with GPs with support information aligned
to local pathways and CCG clinical, policy and business objectives. Context is shared between DXS
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
18
and GP system, so that patient information pre-populates the form avoiding duplication of data
entry and transcription error. However, decision support information is only available to GPs when
they access a patient record and cannot be used as a resource to access ad-hoc information. There
are no other on-line knowledge content systems available to GPs apart from prescribing protocols
stored on the intranet and maintained by the CCG Medicines Optimisation team.
The deployment of DXS has had some issues which are still being resolved. Rollout of the pathways
has been slow and adoption has been low. However, this functionality will be an important means
to ensuring locally agreed pathways are met in an integrated care environment. The status of the
deployment is currently:
Total Forms = 127
Number sent to DXS = 105 (83%)
Number available on DXS = 77 (61%)
Dashboards – The only dashboard currently available to Croydon GPs is an Urgent Care Dashboard
provided by the CSU providing a static view of recent urgent care data within an excel format.
Urgent Care Dashboards support proactive care planning and case management as part of the
Avoiding Unplanned Admissions Directed Enhanced Service (AUPA ES). There is a strong demand
from the GPs for real-time data and this is being addressed. The CCG has recently submitted a
business case to provide a web based Clinical Dashboard with a daily refresh of data. It will provide
one location for practices and other assigned healthcare professionals to quickly access patient
level information about patient’s A&E attendances, emergency admissions, and other patient
contacts across local community, urgent care, mental health and social service providers. The
Clinical Dashboard will leverage the Sollis platform to link data to GP records.
Sollis – Sollis is a patient based data warehouse which captures NHS data sets for the delivery of
commissioning intelligence. It has the potential to support secondary care, primary care,
community, mental health and prescribing but currently focuses on primary care data. Sollis allows
the CCG, practices, and networks of practices to analyse practice data for the purpose of risk
stratification and analytics. Data is anonymised but records can be re-identified at the practice by
authorised users for person level case management. Since dissolution of the PCT Sollis has been
managed by the CSU. Stakeholders felt that the Sollis is currently not being utilised to its full extent
for a number of reasons including Information Governance (IG) policies, CSU ownership, and due to
the process involved in re-identifying patients at the practice level.
5.2.2. Medicines Optimisation and Variation Teams
The CCG’s Medicines Optimisation team work with GPs and provider organisations optimising use of
medicines to improve patient outcomes and reduce costs. The team provides guidance and information to
GPs to prescribe cost-effectively and optimise the use of drugs. The hospital also identifies patients who
require additional help with the drug compliance and management. This is currently a manual process
which has opportunity to be automated.
The Medicines Optimisation team use ScriptSwitch, a prescribing decision support solution for primary
care. ScriptSwitch integrates with GP systems to automatically display a recommendation, at the point at
which a drug is prescribed. They are currently planning to move to a web based tool, Eclipse Live, for risk
stratification in prescribing & screening. They use Primis software and audit tools to extract, analyse and
review data from patient records but are currently looking to replace this function with Eclipse.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
19
The Variation Team work directly with GPs and practices to standardise the quality of care and remove
significant variations across the borough. They use local risk stratification tools as well as the nationally
published data. They rely on local and national benchmarking and prescribing data which can be outdated
when published.
The teams can only access patient data when they are located at the GP practice. IG policy dictates that
data cannot be accessed centrally unless the user has a legitimate relationship with the patient, so data is
analysed practice by practice. They feel they have access to a lot of benchmarking and data but do not
have the tools to make best use of it.
5.2.3. Mobile and remote access
GPs and practice staff currently do not have a defined mobile device policy. Remote access to clinical
systems on mobile devices is variable depending on the practice, mobile device platform, and clinical
solution. For example, some GPs are able to access EMIS web from their iPAD but cannot access Docman.
Mobile and remote access is seen as a critical tool for flexible working, and providing care in the
community.
EMIS offer a product called EMIS Anywhere that runs across the N3 network on a dedicated Dell tablet with
an inbuilt Smartcard reader. This is marketed as being capable of supporting the remote viewing of patient
notes, appointments and medications, and when used with EMIS Mobile it can be used offline i.e. when
here is no network coverage. The GPs within Croydon are awaiting a demonstration of the EMIS Anywhere,
so that they can assess its suitable. However, there are concerns that remote access to Docman will still be
an issue.
5.2.4. Infrastructure and hardware
Feedback from stakeholders indicates that aspects of infrastructure and hardware are inadequate to fully
meet GP needs and support the planned goals of improved integration with local care providers. The
perception amongst some GP is that the centrally provided hardware conforms to the minimum
specification or is second hand and this contributes to the reliability and speed issues they experience.
Printer faults were also cited as being particularly disruptive, because a consulting room cannot be used if
the GP is unable to print out prescriptions. User satisfaction has also been affected since the Windows 7
upgrade. For example, Practice Manager’s administration rights were revoked adding additional barriers to
the resolving of printer issues.
The national NHS secure N3 network, is regarded to be slow and creates a barrier to integration with social
care as Local Authorities are currently unauthorised to access the network. A national outline business
case has recently been approved to replace N3 in 2017 when the current contract expires.
5.3. CCG IM&T environment
The CCG staff work within a ‘hot-desking’ environment. Roaming profiles allow staff to log on at any
workstation within the office. Many staff have found this unsatisfactory due to the lack of true hot desks,
and the time it takes to load a roaming profile onto a local PC. The result is that the majority of staff sit at
the same desk each day. This has some advantages i.e. teams are co-located and in an open planned space
teams which deal with sensitive data can be shielded from the rest of the CCG. However, there are some
disadvantages with this approach. For example visitors are increasingly finding it difficult to find a desk to

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
20
work at. As there is currently no flexible working policy in place the staff do not have an option of working
remotely to free up desk space. At times staff find an open plan workplace disruptive and need a
productive place to work for intensive assignments.
Staff also feel that they do not have access to modern business tools to optimise workplace efficiency and
productivity. For example, intranet and content management tools, on-line collaboration tools, mobile and
remote working. Staff who do have access to flexible or remote working are required to use security fobs
to access the CCG’s network which are currently purchased at a high cost to the CCG.
5.4. IM&T in the local healthcare economy
Sharing of data within the local healthcare economy is limited to:
referrals;
electronic prescribing;
hospital discharge summaries and letters; and
laboratory requesting and results.
An instance of Orion Portal is currently deployed for purposes of pathology messaging only.
Some local systems (for example, community) collect very limited data electronically, or have systems
which lack interoperability. Local health providers will be required to undertake a self-assessment of the
readiness, capabilities and infrastructure of their systems as part of NHS England’s Local Digital Roadmap
initiative. The systems currently in place within Croydon’s local health healthcare economy are listed in the
table below.
Organisation System
Croydon GP Practices EMIS (51) and Inpractice Systems Vision (6)
Croydon University Hospital – Acute
Croydon University Hospital – Community
Cerner Millennium
Ascribe EPEX
South London & Maudsley NHS Trust
(Mental Health)
RiO
Croydon LA – adults (Social Care)
Croydon LA – children (Social Care)
Integrated System (AIS)
Liquidlogic Children’s Social Care System
(LCS)
GPOOH: Virgin Healthcare
NHS 111
Adastra
St Christophers Palliative Care Co-ordinate My Care

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
21
5.5. Summary of current IM&T environment
The primary strengths, weaknesses, opportunities and threats of the current IM&T environment have been
identified and will provide key points to address in the strategies to follow.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
22
6. Vision and strategic objectives
This section aims to describe the vision for IM&T across the healthcare economy of Croydon, and to
identify the key strategic objectives for the CCG to achieve their vision.
6.1. Vision and Mission
Croydon CCG’s Vision is:
Longer healthier lives for all the people in Croydon
Through an ambitious programme of innovation and by working together with the diverse communities
of Croydon and with our partners, we will use resources wisely to transform healthcare to help people
look after themselves, and when people do need care they will be able to access high quality services
IM&T is one of the key enablers to realising this vision and strategy
The CCG’s IM&T vision is therefore to use the power of intelligent information and digital technology
The CCG’s IM&T mission or aim is:
To provide clinicians, patients and staff with accessible, insightful information and efficient technologies
to facilitate the sharing of knowledge, of health information across the care continuum, and to improve
the efficiencies of the organisation.
6.2. IM&T strategic objectives
The following set of objectives for IM&T focuses on building the foundations and capability which will
enable the CCG to succeed in achieving health outcome, care quality and integration goals over the next
five years. The strategy consists of seven key themes. The first is an overarching goal to reflect the
organisation’s IM&T vision, the remaining are core supporting, and enabling goals.
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
23
Overarching goal:
1. Utilising IM&T to improve integration and quality of care across the health economy
Core supporting objectives to achieve this goal are:
2. Sharing of patient information across provider organisations
3. Technology to promote wellness and engage and empower the people of Croydon
4. Business intelligence to understand population needs, and manage contracts
Enabling objectives:
5. Provision of robust infrastructure and IM&T support
6. Optimise, standardise and integrate GP software to support clinical knowledge and
decision making
7. Improving the satisfaction and productivity of the workforce through information and
digital technology
6.2.1. Objective one - Utilising IM&T to improve integration and quality of care across the health
economy
Fundamental to this Digital Healthcare Strategy is the need to provide the infrastructure, information and technology to underpin Croydon’s ambitious integration and commissioning plans. It is crucial that the fundamental foundation blocks are in place before deploying the necessary digital technology and architecture.
Under NHS England’s Local Digital Roadmap, the CCG are expected to co-ordinate and drive forward the digital integration plans for their local healthcare economy. In order to achieve this the CCG must address the following over the next three to six months:
Ensure healthcare vision, timelines and goals are understood and agreed across all stakeholder organisations.
Establish an intra-borough structure to support digital integration, data sharing and implementation of joint commissioning goals. The structure must represent all commissioning and provider stakeholders and drive the development and implementation of the Local Digital Roadmap. The CCG may consider proposing an independent Project Management Office (PMO) to manage the delivery of the digital roadmap.
Establish a cross-organisation Board to oversee this structure and the delivery of Croydon’s Digital Roadmap.
A forum must be in place for key managers and clinicians across both commissioners and providers to agree outcomes, indicators and data to be shared for purposes of improved quality of care, and outcome measurement.
The CCG will provide representation on the inter-borough digital roadmap lead by the South West London Commissioning Collaborative.
6.2.2. Objective two - Sharing of patient information across provider organisations
A patient centred approach to sharing information is crucial to delivering safe, efficient, co-ordinated care.
The SW London Commissioning Collaborative IM&T Strategy aims to achieve information sharing across SW
London Health and Social Care in in two phases:

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
24
Tactical Solution: within 1-2 years focuses on building on the existing systems
Strategic Solution: within 2-5 years including self management and prevention
Croydon is one of the few boroughs in SW London which currently is not sharing patient records across care
settings within the borough (for example, via a Clinical Portal, or Health Information Exchange). This is a
step which Croydon commissioners and providers should address prior to addressing the wider goals of
population health, or inter-borough record sharing is addressed.
However, it is recommended the CCG and providers explore record sharing options which can be deployed
quickly and cost effectively, and that energy is focused on the strategic vision of population management
and preventative healthcare. Given that the community and social care solutions are currently not capable
of sharing data, short term emphasis should be placed on access records between GPs and Acute. Sharing
of records will also alleviate some of the current issues in handover of care such as quality of discharge
summaries.
The following goals need to be achieved to ensure this objective is met.
Over the next 3-6 months:
Assessment of current capabilities of provider systems and barriers to sharing information
(undertaken through the Local Digital Roadmap Initiative).
Agree data sets for sharing information which align with health outcome and CCG care quality goals
Identify and evaluate short-term options for sharing patient records across General Practice and
acute settings, learning from the experiences of neighbouring CCGs.
Over the next 6-12 moths:
Identify and evaluate medium to longer-term options for sharing records including community,
mental health and social care settings. These options may take into consideration population
health and preventative care goals. Some of the differences between a Portal or Health
Information Exchange (HIE) solution and a Population Health Management solutions are explained
in the table below.
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
25
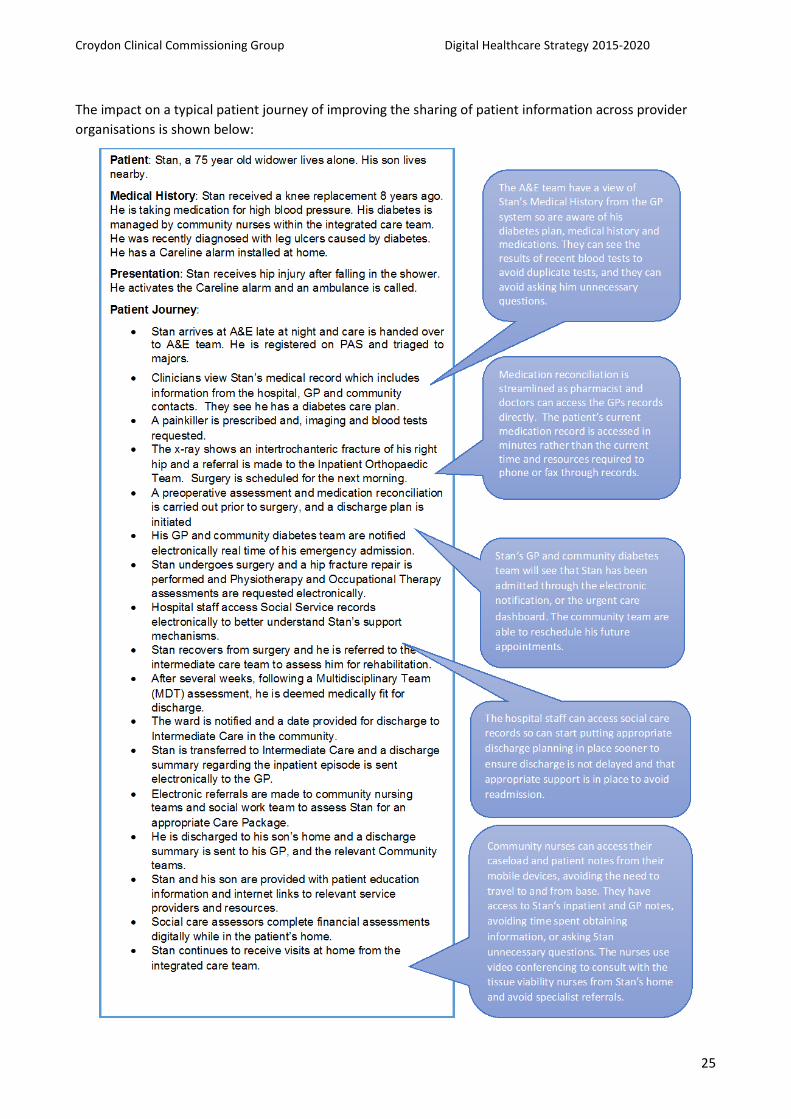
The impact on a typical patient journey of improving the sharing of patient information across provider
organisations is shown below:

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
26
6.2.3. Objective three - Technology to promote wellness and engage and empower the people of
Croydon
Self-management and prevention of illness is crucial to improvements in population based health
outcomes. Patients require access to information, their care records, decision support tools to self manage
their health. Intelligent data is required to understand and profile who is ill, or at risk of ill health, and
target with appropriate interventions. The relationship between population health management and
patient engagement is highlighted in the diagram below.
SW London Commissioning Collaborative aim to procure a holistic population health solution, and develop
patient engagement and telehealth/telecare strategies. These timeframes may not align with the CCG’s
commissioning goals as Croydon move to supporting Outcome Based Commissioning by the next financial
year.
It is recommended that the CCG remain engaged with the plans and activity of SW London to ensure
alignment and to avoid duplication, but take a lead on investigating a population health and patient
engagement solution in a timeframe that meets their needs.
The approach to achieving this objective over the next 6 to 24 months should include:
Optimising use of the CCGs existing risk stratification tools (for example, Sollis) to
understand population health needs.
Review and evaluate Population Health Management, Patient Engagement and
telehealth/telecare solutions and strategies solutions available to the UK market in
collaboration with the SW London Collaboration.
Utilise and build upon the CCGs Prevention, Self-care And Shared Decision Making Strategy.
Collaborating with Healthwatch to understand the wants and needs of the people of
Croydon taking into consideration the unique characteristics of the diverse Croydon
population.
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
27
In order to achieve Outcome Based Commissioning goals the CCG should be planning now to support the
procurement within the next 6-18 months of a Population Health Management solution and within 18-36
months the procurement of a Patient Engagement solution for Croydon.
6.2.4. Objective four – Business Intelligence to understand population needs, and manage
contracts
Business intelligence is critical to the CCGs and primary care business for:
managing quality standards and benchmarking;
risk stratification and understanding the health needs of the population;
monitoring quality and outcomes of service provision;
managing contracts; and
providing clinical and executive decision support tools (for example, dashboards).
Business Intelligence will become increasingly important to CCGs as its role of understanding population
needs, and measuring outcomes, and monitoring care quality becomes a greater focus of its core business.
However, the CCG are currently not receiving optimal benefit with the current arrangements in place for
provision of BI services, and in particular the ‘additional service’ commissioned from the CSU.
The CCG also need to address the barriers to accessing centralised primary care records for the purpose of
identifying population need, risk stratification and cohorts of patients, and the barriers to providing greater
GP access to data and BI tools.
To address the gaps identified in the current provision of BI the CCG will over the next 12 months need to:
Review current procedures for prioritising and requesting data analysis to ensure that
priorities and requirements are clear to both the CCG and the BI team. This should include
agreed standard tools and processes for specifying requirements, and prioritising projects.
It is recommended BI team provide regular updates of work in progress, and pipeline to
ensure transparency and awareness of priorities and workload.
Review the ‘additional service’ arrangements to determine how this cost could be spent
more effectively to support BI in other ways.
Review breadth and quality of datasets available for analysis to identify where gaps exist in
meeting the CCG’s care quality and health outcome goals (for example, mental health,
community data, outcome capture). Address these gaps within the established intra-
borough IM&T structures and forums.
Understand and address barriers to accessing centralised primary care data for purposes of
population need, risk stratification and cohort identification. This may be addressed
through GP network arrangement with the Croydon GP Collaborative, or better
restructuring of user access to align with IG policies. It is also believed that moving to a
single GP system across the borough will improve access to centralised GP data.
Education for CCG staff to improve understanding of BI, analytics and self-service tools
available such as Data Cubes. This goal aims to increase the number of data requests which
are accessed via self-service, and improve the quality of data request specifications.
Improve GP awareness and access to existing analytical tools within practices including
EMIS Clinical Utilities and Sollis, and work with software suppliers to establish training
resources.
Over the next 12 to 24 months:
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
28
Robust data and BI will become an increasingly vital asset to the CCG and they must
consider providing in-house business and data analysts to support the BI function. These
resources will act as expert customer from within the organisation and ensure that the
data requirements underpinning the success of the CCGs commissioning goals are met.
The CCG must work with the CSU to ensure the most effective tools are in place to provide
data analytics to support clinical and business decision support such as real-time
dashboards. As Croydon become data rich with increased data collection, data sharing and
improved data quality, the CSU will be able to provide an increasingly more agile and
inspiring approach to BI development.
6.2.5. Objective five – Provision of robust infrastructure and IM&T support
The CCG is committed to outsourced support and want to achieve a successful technology partnership with
its contracted Clinical Support Unit. There are a number of factors which have contributed to a level of
dissatisfaction with the CSU including:
misalignment of CCG and CSU expectations;
no expert customer within CCG to define requirements and measure performance;
underutilisation of CSU services;
variable quality of service delivery; and
lack of some skills required by the CCG (for example, project management and healthcare IM&T
strategy).
The CCG is working with the CSU to resolve these issues. It sees the partnership as an opportunity to
provide an exemplar healthcare IM&T environment and support the CCGs progressive IM&T goals. In order
to achieve this the CCG will need to ensure the following structures are in place:
In the next 6 months
Firstly and foremost, the CCG must ensure that an ‘expert customer’ role exists within the
organisation with the knowledge and expertise to define what is required from the CSU and hold
them to account. This role will be fundamental to the successful delivery of this Digital Healthcare
Strategy, and delivery of Croydon and SW London’s digital roadmaps. This will enable the CSU to
better understand the strategic direction and needs of its customer, and better match services to
requirements. It is recommended that the CCG construct a job description/person specification for
this role identify the funding for the post and consider options for filling this role in the short and
long term. This may include using an independent contractor on a short-term basis.
Use the newly appointed to ‘expert customer’ to change the relationship around IT and
Information with the CSU from reactive to proactive. This will increase the value of the service the
CSU provides to the CCG because they will no longer be focussed into the position of instructing the
CSU. Instead the CSU will understand and appreciate the CCGs business issues and offer evaluated
solutions to these issues.
As part of the Windows 7 roll out a primary care IT asset register has been created by the CSU for
Croydon. The CCG must work with the CSU to create a budget and plan to replace and refresh
primary care hardware and infrastructure as it comes to the end of its effective life. This budget
and plan will be used to inform the Project Initiation Document (PID) and central funding request
for 2016/17.
Work with the recently appointed GP IT Facilitator on improving IM&T efficiencies, optimising
solutions and working with practice managers to develop individual practice IM&T plans. Define a
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
29
set of critical success factors to review the effectiveness of this individual. Share these CSF with the
CSU.
In the next 12 months
Review the work of the GP IT Facilitator and assess if one individual is sufficient to cover the 57
practices within Croydon. If required build a business case for additional facilitator resources.
6.2.6. Objective six – Optimise, standardise and integrate GP software to support clinical
knowledge and decision making
General Practice software is key to improving quality of primary care, clinical decision support, variance and
medication optimisation, and for achieving the vision of paperless working. The CCG and practices have
invested in a number of clinical tools which have not been utilised to their full extent, including DXS, Sollis,
clinical dashboards and analytic tools. This situation has arisen for a number of reasons including historical
lack of IM&T strategy and structure to underpin purchasing decisions and business case development, and
lack of transparency or awareness surrounding software purchasing decision making
Where software has been adopted variation in workflow, utilisation rates and quality of data (for example,
coding) still exists. For example, some practices have strong usage of Docman, while others report a low
usage rate. One reason for variation across practices is the use of two different Primary Care Systems. This
is seen as a barrier to standardising data, improving quality, and reducing costs. Standardised data,
workflow and architecture will provide considerable benefits to achieving the data sharing goals that
underpin the IM&T strategy.
There are a number of strategies the CCG can implement to achieve better standardisation and utilisation:
In the next 6 – 12 months
The CCG in conjunction with the CSU firstly, will produce an audit of software licenses and usage
levels across all practices to understand the current state. Once this is achieved the CCG can work
with practices understand why tools are not being utilised successfully, and produce a software
strategy which aligns with this Digital Healthcare Strategy.
Structures will be developed to support clinical software purchasing and decision making, to ensure
that decision fully support the CCGs IM&T and software strategy, and have user buy-in.
Neighbouring CCGs also have success stories for use of software such as Sollis and DXS, and lessons
will be learnt from these organisations.
In the next 6 – 18 months
The CCG will work with software suppliers and leading CCGs to understand how to optimise use of
software. Suppliers such as EMIS should be approached to provide the CCG with resources and
tools to improve user experience and utilisation of their software. For example, the EMIS User
Forum, and Clinical Utilities appear to be underutilised tools.
It is recommended the CCG produce a Target Operating Model for General Practice which
promotes standardised workflows, and optimises utilisation and access to software. In order to
achieve this the CCG may consider the following strategies:
o Create an exemplar practice which follows a Target Operating Model to demonstrate what
good looks like, and the benefits derived.
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
30
o Formalise a Chief Clinical Information Officer CCIO role to champion the Target Operating
Model, provide Primary Care Clinical input into purchasing decisions and proposed changes
to information flows/integration points between organisations.
o It is recommended the CCG promote use of a single General Practice solution.
Approximately 90% of practices are currently using EMIS. The CCG and provider partners
will benefit from the standardisation and economy of scale that a single primary care
system can bring. The CCG may not wish to mandate use of a single system, however, it
might want to highlight the benefits of using a single solution, the dis-benefits for non-EMIS
sites, and look at options for encouraging practices to migrate where they wish to. It is
recommended that the Croydon GP Collaboration is involved in agreeing and formulating
options to meet this goal.
6.2.7. Objective seven - Improving the satisfaction and productivity of the workforce through
information and digital technology
Technology, information and flexible working arrangements can create a motivated and satisfied
workforce, improving productivity, and staffing levels. Efficiencies can also be gained through use of
business technologies to improve communication and knowledge sharing.
Stakeholder interviews found that CCG staff and GP satisfaction and productivity could be improved with
technology that enables more flexible working conditions. Staff are currently working in a ‘hot-desking’
environment which is not satisfactory, and remote working is only available to very few, at a high cost.
The following strategies will address workplace satisfaction and productivity:
In the next 6 months
Intranet and content management solutions were identified as a major gap and will need to be
addressed over the short term. It is recommended that the CCG work with the CSU to scope and
implement a replacement Intranet for the CCG. Whilst scoping this project the CCG should
consider the purpose of the intranet, it relationship with DXS, how existing content will be
reviewed and uploaded to the new site, how the site will be kept current, how new content will be
uploaded, how much CCG staff can do themselves and how much will need the involvement of the
CSU. These factors will help determine whether they require a solution to manage and present
content or to solution to enable collaboration and the on-going service they require from the CSU.
In the next 12-24 months
Provide the flexibility for CCG staff to work anywhere in the office, from home or whilst travelling.
There are a number of different technical options and strategies that can be used or combined to
achieve this flexibility. The major choice is between providing staff with laptops, or implementing
desktop virtualisation. These choices are explore in more detail below:
o In a laptop environment the user carries their own device and uses it where they land in
the office. When working from home the user would use their laptop and connect to the
CCG’s network via the Internet (probably via their home Wi-Fi) and using a three-factor
authentication method (e.g. a SecureID token) establish an encrypted data linked to the
CCGs network and server. The user would be able to work as if they were in the office.
o In a virtualised infrastructure (VDI) environment all the applications and data remain on the
centralised server with only display, keyboard and mouse information communicated with
the local client device, which may be a conventional PC/Laptop, a thin client device, a
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
31
tablet or even a smartphone. A user in the office would be able to work immediately from
any desk without having to download their remote profile, because there is no data saved
locally. A user working at home would be able to use their home PC or tablet to log onto
the CCGs VDI using a three-factor authentication method (e.g. a SecureID token). The link
between the home device would be encrypted and the user would be able to work as if
they were at their desk.
o The main advantages of VDI over laptops is that it is more secure (no data is stored locally),
is easier to maintain centrally – so is less expensive to set up and run, is more resilient
because there are no moving parts in a desktop thin client and naturally supports Bring
Your Own Device (BYOD)1. Although the costs of providing desktop devices is significantly
reduced (a thin client the third the cost of a PC) more money has to be invested in the
central servers so overall the costs are probably neutral.
Consider upgrading to the latest versions of office automation products such Microsoft Office 365.
This product is licenced on a subscription basis and may prove more cost effective than the former
perpetual licences. It would also give the CCG access to licences for Microsoft Office Apps, which
would allow Word, Excel and PowerPoint Documents to be edited natively on OS devices like an
iPad.
The CCG should work with its staff and the CSU to identify other modern business technology and
tools to help improve productivity and staff satisfaction.
Technology to support flexible working is also required for Primary Care GPs and clinicians to fully
support their role when working remotely (for example, from home or within the community
setting). This is a key enabler to achieving population health outcomes.
o It is recommended the CSU will with the Croydon GP Collaboration to provide a standard
mobile device strategy across all practices and which will meet the needs of the clinicians.
o It is also recommended the CSU work with software suppliers to address gaps (for example,
ability to use Docman on iPADs), and understand their software roadmap to ensure that any
hardware purchases, and mobile device policies are compatible with the software
development. They should also collaborate with suppliers to address any anticipated gaps.
6.3. What will 2020 look like….
The improvements, which will be achieved when the CCG’s Digital Strategy has been implemented, are
summarised in the table below
Theme Today What 2020 looks like…
Utilising IM&T to
improve integration
and quality of care
across the health
economy
Low level of integration
Low level of collaborative IM&T
processes across commissioners and
providers
Robust established collaborative
structures and processes in place to
deliver fully integrated care
Data captured as a by-product of care
to measure and verify improved
1 BYOD refers to the policy of permitting employees to bring personally owned mobile devices (laptops, tablets, and
smart phones) to their workplace, and to use those devices to access privileged company information and applications. The phenomenon is commonly referred to as IT consumerisation.
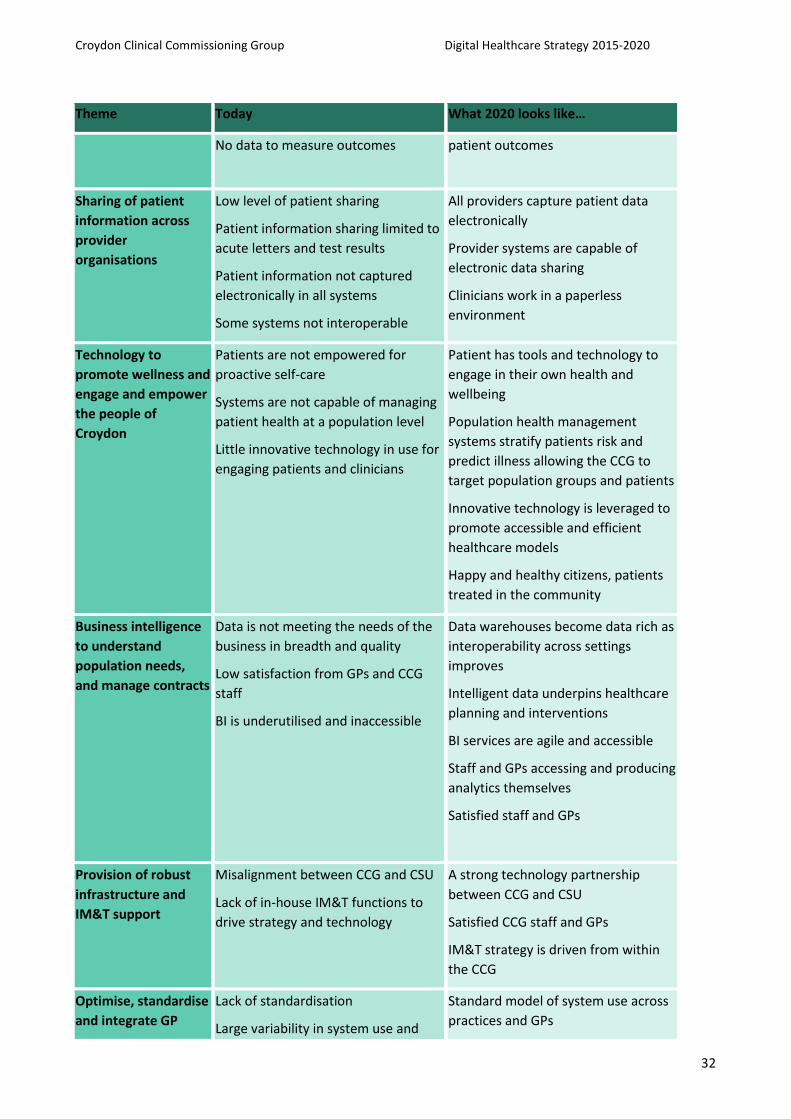
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
32
Theme Today What 2020 looks like…
No data to measure outcomes patient outcomes
Sharing of patient
information across
provider
organisations
Low level of patient sharing
Patient information sharing limited to
acute letters and test results
Patient information not captured
electronically in all systems
Some systems not interoperable
All providers capture patient data
electronically
Provider systems are capable of
electronic data sharing
Clinicians work in a paperless
environment
Technology to
promote wellness and
engage and empower
the people of
Croydon
Patients are not empowered for
proactive self-care
Systems are not capable of managing
patient health at a population level
Little innovative technology in use for
engaging patients and clinicians
Patient has tools and technology to
engage in their own health and
wellbeing
Population health management
systems stratify patients risk and
predict illness allowing the CCG to
target population groups and patients
Innovative technology is leveraged to
promote accessible and efficient
healthcare models
Happy and healthy citizens, patients
treated in the community
Business intelligence
to understand
population needs,
and manage contracts
Data is not meeting the needs of the
business in breadth and quality
Low satisfaction from GPs and CCG
staff
BI is underutilised and inaccessible
Data warehouses become data rich as
interoperability across settings
improves
Intelligent data underpins healthcare
planning and interventions
BI services are agile and accessible
Staff and GPs accessing and producing
analytics themselves
Satisfied staff and GPs
Provision of robust
infrastructure and
IM&T support
Misalignment between CCG and CSU
Lack of in-house IM&T functions to
drive strategy and technology
A strong technology partnership
between CCG and CSU
Satisfied CCG staff and GPs
IM&T strategy is driven from within
the CCG
Optimise, standardise
and integrate GP
Lack of standardisation
Large variability in system use and
Standard model of system use across
practices and GPs
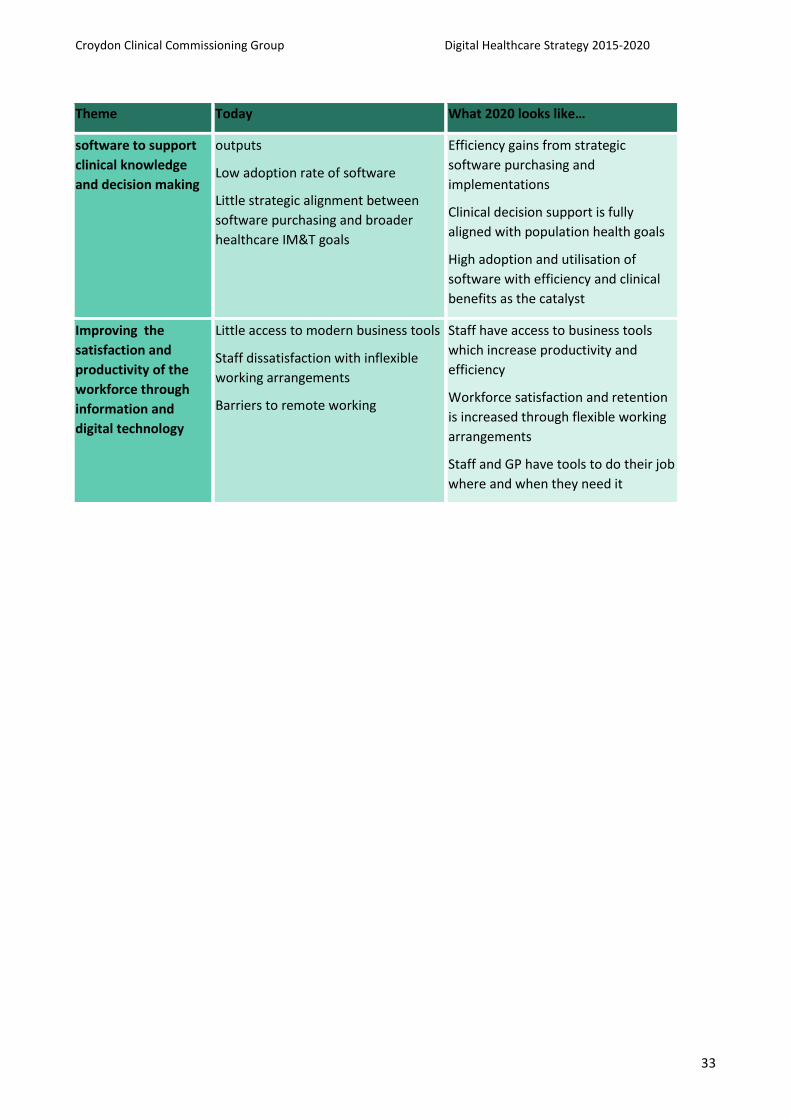
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
33
Theme Today What 2020 looks like…
software to support
clinical knowledge
and decision making
outputs
Low adoption rate of software
Little strategic alignment between
software purchasing and broader
healthcare IM&T goals
Efficiency gains from strategic
software purchasing and
implementations
Clinical decision support is fully
aligned with population health goals
High adoption and utilisation of
software with efficiency and clinical
benefits as the catalyst
Improving the
satisfaction and
productivity of the
workforce through
information and
digital technology
Little access to modern business tools
Staff dissatisfaction with inflexible
working arrangements
Barriers to remote working
Staff have access to business tools
which increase productivity and
efficiency
Workforce satisfaction and retention
is increased through flexible working
arrangements
Staff and GP have tools to do their job
where and when they need it
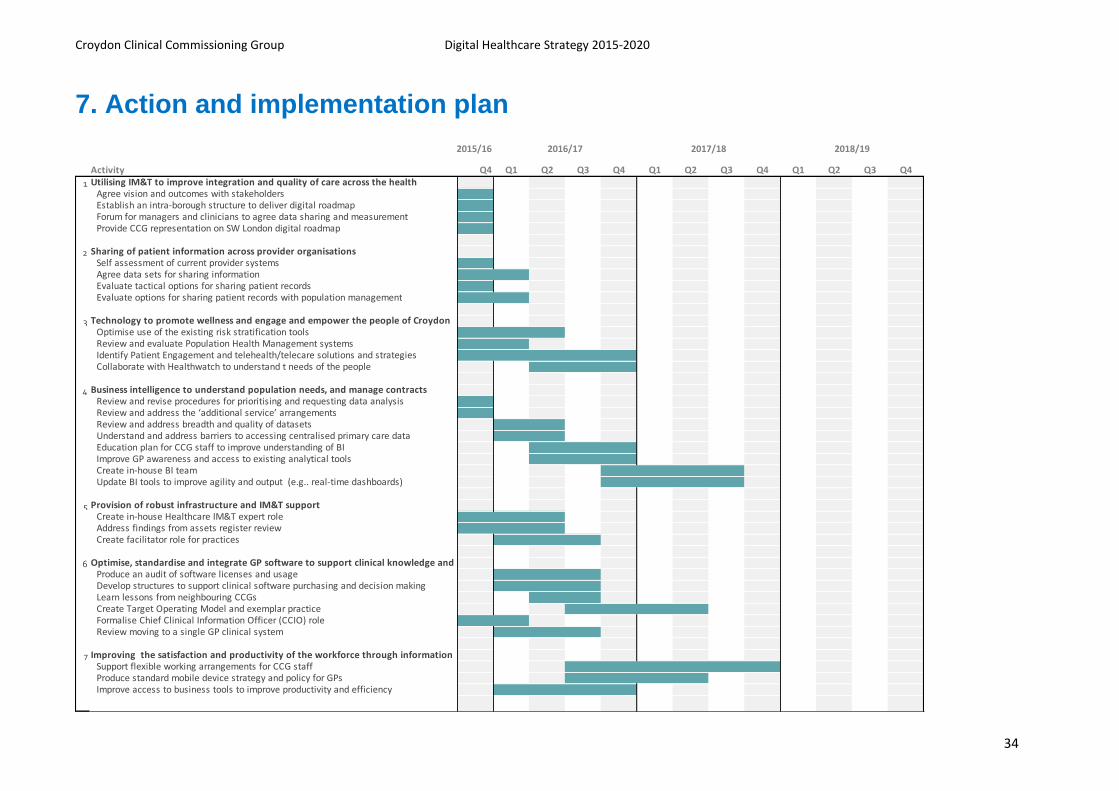
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
34
7. Action and implementation plan
Activity Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
1 Utilising IM&T to improve integration and quality of care across the health Agree vision and outcomes with stakeholdersEstablish an intra-borough structure to deliver digital roadmapForum for managers and clinicians to agree data sharing and measurementProvide CCG representation on SW London digital roadmap
2 Sharing of patient information across provider organisations Self assessment of current provider systems Agree data sets for sharing information Evaluate tactical options for sharing patient records Evaluate options for sharing patient records with population management
3 Technology to promote wellness and engage and empower the people of CroydonOptimise use of the existing risk stratification tools Review and evaluate Population Health Management systemsIdentify Patient Engagement and telehealth/telecare solutions and strategiesCollaborate with Healthwatch to understand t needs of the people
4 Business intelligence to understand population needs, and manage contractsReview and revise procedures for prioritising and requesting data analysis Review and address the ‘additional service’ arrangements Review and address breadth and quality of datasets Understand and address barriers to accessing centralised primary care data Education plan for CCG staff to improve understanding of BIImprove GP awareness and access to existing analytical tools Create in-house BI teamUpdate BI tools to improve agility and output (e.g.. real-time dashboards)
5 Provision of robust infrastructure and IM&T support Create in-house Healthcare IM&T expert roleAddress findings from assets register reviewCreate facilitator role for practices
6 Optimise, standardise and integrate GP software to support clinical knowledge and Produce an audit of software licenses and usage Develop structures to support clinical software purchasing and decision makingLearn lessons from neighbouring CCGsCreate Target Operating Model and exemplar practiceFormalise Chief Clinical Information Officer (CCIO) role Review moving to a single GP clinical system
7 Improving the satisfaction and productivity of the workforce through information Support flexible working arrangements for CCG staff Produce standard mobile device strategy and policy for GPsImprove access to business tools to improve productivity and efficiency
2018/192015/16 2016/17 2017/18
Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
35
8. Conclusion
An assessment of the CCGs current IM&T environment has identified there are significant digital challenges
and opportunities to come in meeting the CCG’s ambitious integrated care and commissioning goals. This
strategy aims to ensure that CCG has the appropriate structures in place as they embark on a progressive
health and wellbeing programme. The objectives required to achieve the population health goals of
Croydon align with the goals of local, regional and national imperatives.
The importance of communication, intelligent data, and digital technology to support these collaborative
goals cannot be understated. The strategy strongly recommends that the CCG invests in additional
structures and roles to support their vision including:
a dedicated Healthcare IM&T role within the CCG’s management structure to support delivery of
this Digital Healthcare Strategy, and Croydon’s Digital Roadmap;
a small in-house Business Intelligence analytics team; and
the formalisation of a Chief Clinical Information Officer (CCIO) role.
It is recommended that the CCG, in their role of co-ordinators of Croydon’s Digital Roadmap, drive forward:
an intra-borough structure comprising all commissioner and provider organisations for supporting
delivery of IM&T across the borough;
a target operating model to get the most of the existing investment in primary care systems; and
the delivery of a Population Health Management solution in timescales that meet their OBC goals.
Any initiatives from this Strategy requiring funding will require a business case to be developed for the
appropriate approval channels.
It is also recommended that the strategy is refreshed on annual basis over the next five years to reflect the
fast changing pace of technology and healthcare.

Croydon Clinical Commissioning Group Digital Healthcare Strategy 2015-2020
36
Appendix A – Governance
(to be included)