digestive trac • spring 2013, issue 6
DESCRIPTION
COLONOSCOPY, COLORECTAL CANCER DIAGNOSIS & TREATMENT This issue of Digestive Trac discuses steps to achieve good colon prep and other aspects of colon disease diagnosis and management. Article Topics: Multidisciplinary Team Provides Seamless Continuum of Care Accurate Colonoscopy Results Begin with Good Colon Prep Adenoma Detection is a Key Measure of Colonoscopy Effectiveness Minimally Invasive Procedures Result in Less Pain and Faster Recovery Medical and Radiation Oncology and Pathology Play Key Roles in Cancer Management Social Work and Spiritual Care Resources Provide Added Support After-Treatment Surveillance Helps Minimize Threat of RecurrenceTRANSCRIPT

DigestiveTracDIGESTIVE DISEASES • SPRING 2013
Issue 6
INSIDE THIS ISSUE:
Multidisciplinary Team Provides Seamless Continuum of Care
Accurate Colonoscopy Results Begin with Good Colon Prep
Adenoma Detection is a Key Measure of Colonoscopy Effectiveness
Minimally Invasive Procedures Result in Less Pain and Faster Recovery
Medical and Radiation Oncology and Pathology Play Key Roles in Cancer Management
Social Work and SpiritualCare Resources Provide Added Support
After-Treatment Surveillance Helps Minimize Threat of Recurrence
Scott L. Baker, MD, FACS, FASCRS Steven Condron, MD, MHES, FACPColorectal Surgery Gastroenterology and HepatologySurgical Institute of South Dakota Avera Medical Group GastroenterologySurgical Director of Avera Digestive Disease Institute Medical Director of Avera Digestive Disease Institute
Dear Colleagues,
March is National Colorectal Awareness Month. Nationwide, approximately 150,000 new cases of colorectal cancer are diagnosed each year, and 52,000 people die of the disease. Of cancers affecting both men and women, colorectal cancer is the second leading cause of cancer deaths.
The good news is that thanks to screening and early detection, colorectal cancer is one of the most preventable and treatable cancers – if caught in its early stages. Studies show that people who are screened have a 90 percent reduced risk of developing colon cancer. Yet nationwide, only about 50 percent of people who are eligible for regular recommended screenings take advantage of it. We at the Avera Digestive Disease Institute are taking all the steps we can to ensure screening colonoscopy is accessible to everyone. Primary care providers can also help to change this troubling statistic by encouraging patients to undergo screening colonoscopy beginning at age 50, and providing education on this important cancer-prevention tool.
Through regular recommended colonoscopy screenings, it is our primary goal to prevent colorectal cancer from ever happening, which is entirely possible by finding and removing precancerous adenomatous polyps before they have the opportunity to develop into cancer.
A quality colonoscopy requires the expertise of an experienced team, but it begins with the patient’s willingness to take the necessary steps to achieve good colon prep. We address this issue and other aspects of colon disease diagnosis and management in this edition of Digestive Trac.
When malignancies do occur, we want to provide an accurate diagnosis and begin treatment at the earliest stage possible, for the best possible outcomes.
Dedicated to providing the highest quality care, our multidisciplinary team offers a full range of treatment options – including surgery, medical and radiation oncology, genetic testing, support services and follow-up care and surveillance. We invite you to take time to read about these specific aspects of our program in this issue.
As always, it is our privilege to work closely with primary care physicians for our patients’ best interest and continuity of care. This includes patients with colorectal cancer, polyps, or other malignant and non-malignant disease of the digestive tract. Please feel free to contact us at 605-322-7797 with questions or for more information.
Sincerely,
1
Avera Makes the Grade!Avera McKennan Hospital & University Health Center Achieves
Top Rankings in Gastrointestinal and General Surgical Care
Healthgrades has ranked Avera McKennan the No. 1 Hospital in South Dakota
for GI Services and GI Medical Treatment in 2013.
Healthgrades Awards for GI care:
n Top 5% in the Nation for Overall GI Services
n Top 5% in the Nation for GI Medical Treatment
n Top 5% in the Nation for General Surgery
n Ranked No. 1 in S.D. for General Surgery
n Ranked No. 1 in S.D. for GI Services and GI Medical Treatment n Five-Star Recipient for GI Procedures and Surgeries, Treatment of GI Bleed,
and Treatment of Bowel Obstruction
A v e r a D i g e s t i v e D i s e a s e . o r g 2

Multidisciplinary Team ProvidesSeamless Continuum of Care
From screening to diagnosis to treatment and follow-up care, a multidisciplinary team of physicians and other medical professionals at Avera Digestive Disease Institute are committed to helping patients experience a seamless continuum of care, compassionate services and the best possible outcomes.
Through Digestive Disease, referring physicians and their patients have access to:• Themostadvancedtreatmentoptionsavailable
offered by a multidisciplinary team, including colorectal surgery and GI surgery, gastroenterology, genetics, solid organ transplant, medical oncology, pathology, radiation oncology, and radiology
• State-of-the-artendoscopysuites• Personalattentiontoindividualneedsthrough
partnership with a Digestive Disease navigator• Continuingeducationandsupport
A key component of the program is the Digestive Disease Conference, in which a comprehensive array of dedicated professionals meets weekly to discuss individual cases and unique treatment plans for the patients involved.
When patients are diagnosed with cancer or complex disease of the digestive tract, their treatment may involve surgery, chemotherapy, radiation, medication or other modes of therapy. The Digestive Disease Conference brings all these pieces together in an individualized plan of care specific for each patient. A multidisciplinary team of specialists represents the following specialty areas:
• Colorectalsurgery •Radiationoncology• Gastroenterology •Radiology• Genetics •Surgery• Transplant •Chaplaincy• Medicaloncology • Pathology• Socialworkers
As this team reviews details of patient history, pathology reports and diagnostic images, members collaborate in making the best treatment recommendations for each individual case. This approach helps patients get the most effective treatment at the earliest point possible in their disease for the best possible outcomes.
A v e r a D i g e s t i v e D i s e a s e . o r g3

“Our approach is bringing high-level specialists to the table – physicians who specialize in GI care, cancer treatment, pancreatic disease, colorectal surgery and more. It creates a tertiary care environment in which each specialty is represented,” said Dr. Scott Baker, fellowship-trained colorectal surgeon.
Physicians may refer their patients to be presented at the conference by working with Digestive Disease navigator, Liz Harden. In advance, radiologists and pathologists review the case and bring pertinent information such as photos of laboratory slides, as well as diagnostic images. After a case synopsis is presented, the multidisciplinary team develops a recommended plan of care.
For patients, it’s like getting a second, third and fourth professional opinion from the best specialists available, all at the same time. The GI navigator is key to this program. She communicates with patients and their family or support persons, guiding them through all phases of treatment and survivorship. This concept is designed to make the transition between different treatment modalities very smooth, and to ensure that patients are getting all available services at each juncture of their treatment.
Referringphysiciansarewelcometoattendtheconference when their patient’s case is presented either in person or via teleconference.
The conference follows treatment, disease management, follow-up and surveillance guidelines set by the National Comprehensive Cancer Network (NCCN), a national alliance dedicated to improving the quality and effectiveness of cancer care.
For example, NCCN guidelines provide algorithms of care for patients depending on whether or not the disease is resectable or nonresectable, and based on findings of surgery. These guidelines are considered best practices and followed by the Digestive Disease Institute team in making care recommendations.
A v e r a D i g e s t i v e D i s e a s e . o r g 4
Patients benefit from shared medical knowledge including opportunities to enroll in clinical trials. “Having multiple specialists in the room allows every angle to be considered, and places patients where they deserve to be – at the center of our attention,” Dr. Baker said.
As Digestive Disease navigator, Liz Harden, CNP, is present at the conference and ensures that patients are scheduled for any additional tests or procedures recommended. Each patient diagnosed with colorectal cancer is connected with the navigator, who comes alongside patients and their families to help guide them through the process of diagnosis, treatment and survivorship.
Harden helps patients navigate the health care system as they see different physicians and go through the various aspects of care outlined in their treatment plan, and serves as an access point for patients and families. She is available to answer questions, help resolve concerns, and make sure that tests or procedures are done in a timely manner. She provides education to patients and families about their particular diagnosis and connects them with resources like Integrative Medicine.
“Having multiple specialists in the room allows every angle to be considered, and places patients where they deserve to be – at the center of our attention,” Dr. Baker said.

Dr. Cristina Hill Jensen performingan endoscopy
A v e r a D i g e s t i v e D i s e a s e . o r g5
The navigator may enter the picture as early as the diagnostic phase. After a diagnosis is confirmed, Harden is there for patients as they go through all modes of treatment. She also sees them through to survivorship care. This includes a complete assessment of the patient’s diagnosis and treatment, recommendations for future care, and referrals to support groups or other survivorship resources.
“Patients appreciate having someone who can spend time with them, talk with them, and answer all their questions. They appreciate having one contact person. When patients are seeing several different physicians, they may not know who to call for the specific problem they’re having,” Harden says. Or, for those traveling from out of town, she helps organize care so patients can get as much done as possible on one trip, rather than having to travel back and forth for multiple appointments. When their patient is seeing multiple specialists, primary care physicians also appreciate having one contact person with whom to consult.
“Our approach is bringing high-level specialists to the table – physicians who specialize in GI care, cancer treatment, pancreatic disease, colorectal surgery and more. It creates a tertiary care environment in which each specialty is represented,” said Dr. Scott Baker, fellowship-trained colorectal surgeon.

AccurateColonoscopyResultsBegin with Good Colon Prep
Although it’s proven to save lives, colonoscopy is one screening exam that many adults tend to put off. In fact, research shows that up to 60 percent of South Dakotans over age 50 have never received the recommended colon screenings.
Reasonsmayincludefearofpainorembarrassment,soit’s important for primary care physicians to encourage this testing, and accurately inform patients of what to expect.
Colon prep is important in order to gain a full and clear view of the entire lining of the colon. For many patients, this screening is only done once every 10 years, so it’s important to make the best possible use of this screening opportunity. More than the actual colonoscopy, the aspect patients report disliking the most is colon prep. High-volume preps are the standard because a high volume of liquid needs to be ingested in order to purge bowel content. Yet patients report that they dislike the volume of fluid and the taste. New options in colon prep are helping to minimize these two issues.
Traditionally, patients have been asked to drink up to 4 liters of a cleansing solution the day before the test. Newer preparations have been reduced to 2 liters, and there are also preps that are 2 cups in volume. Laxative pills are an option if patients cannot tolerate the liquid preps, but this involves not taking just one pill, but 32.
Generally, a large volume of liquid is necessary to move all solid matter out and irrigate the colon. Otherwise, pieces of solid material still in the bowel can hide small polyps and interfere with endoscopy equipment. In the worst case, a colonoscopy must be rescheduled, and the patient has to go through colon prep again.
One current example of a lower volume colon prep is a combination of Miralax, Gatorade and Senokot, which has a more tolerable taste. Some physicians allow taking half of the solution the evening before the test, and the other half the morning of the test.
If patients are from rural areas, it is usually advised to take the full prep the night before so the patient doesn’t have to worry about finding a restroom while en route. Generally if patients begin the prep by 5 or 6 p.m., they are finished moving their stools by midnight the night before.
A v e r a D i g e s t i v e D i s e a s e . o r g 6
“We have a staff that does this
routinely. Bowel prep instructions
are very clearly explained to the
patient, and we ensure that we
update the patient’s medical history,”
said Dr. Cristina Hill Jensen,
gastroenterologist with Avera
Medical Group Gastroenterology.
Patients are asked to eat no solid food the day before the exam. This reduces the likelihood of undigested food remaining in the colon. This means that patients should not eat anything they can’t “see through.” Among options are clear broth and gelatin (with the exception of red or purple colored gelatin). If patients get extremely hungry, they may be able to supplement the clear liquid diet with a product like Boost or Ensure that contains protein but not fiber.
In addition, patients should not eat or drink anything at least four hours before the test. They should take their important medications, such as blood pressure medication, with sips of water. If the patient has a special condition affecting diet such as diabetes, consultation should take place between the primary care physician and endoscopist regarding oral medications or insulin.
Because patients will have frequent stools after taking the prep, they should plan to spend the evening at home, and take the day of the test off work. The prep is designed so that most patients only have to take one day off work.
“We have a staff that does this routinely. Bowel prep instructions are very clearly explained to the patient, and we ensure that we update the patient’s medical history,” said Dr. Cristina Hill Jensen, gastroenterologist with Avera Medical Group Gastroenterology. When a colonoscopy is scheduled, patients are given specific printed instructions.
Time at the clinic or outpatient hospital setting for the procedure typically is two and a half to three hours, and the actual procedure time is approximately 30 minutes.
Sedative medications make the procedure itself very comfortable. Many patients wake up after the procedure is over and don’t even realize it has already taken place. During colonoscopy, a gastroenterologist gently moves a long, lighted tube with a tiny camera through the entire colon, and watches a magnified view of the inside of the colon on a monitor. If polyps are found, the endoscopist removes the polyps immediately with a tool attached to
A v e r a D i g e s t i v e D i s e a s e . o r g7
Dr. Christopher Hurley performingan endoscopy
the colonosope. If a suspicious lesion is found, a biopsy can be taken during the same procedure.
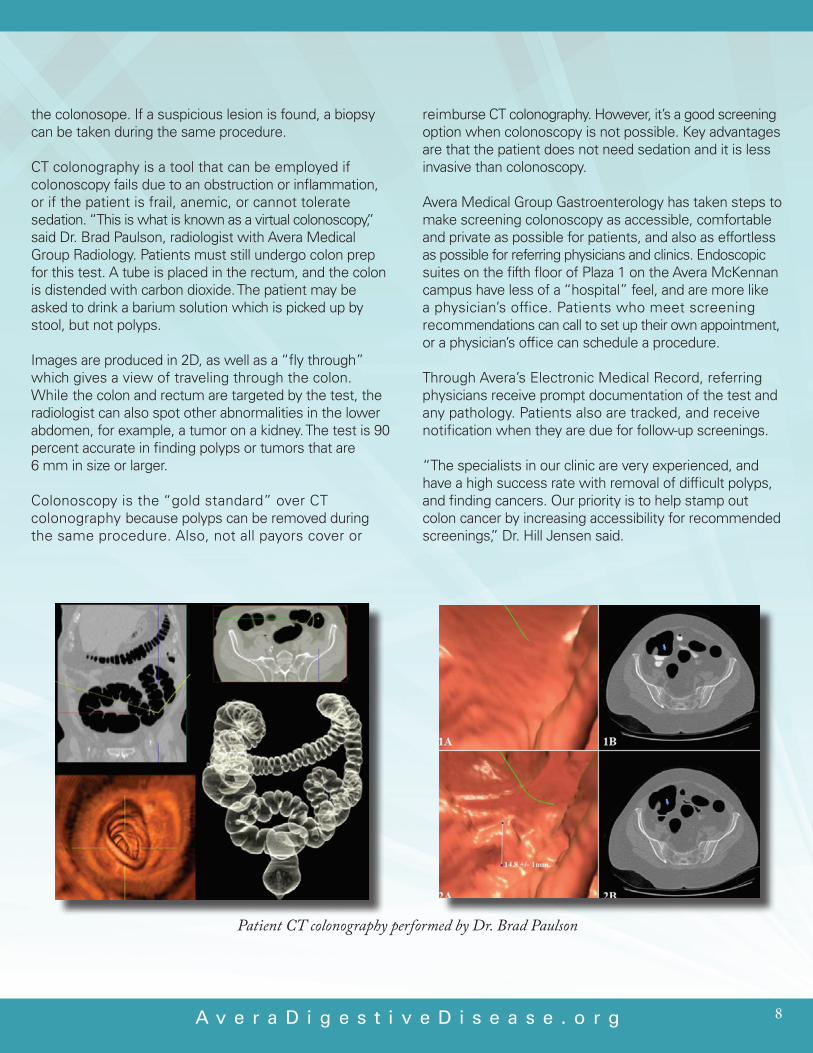
CT colonography is a tool that can be employed if colonoscopy fails due to an obstruction or inflammation, or if the patient is frail, anemic, or cannot tolerate sedation. “This is what is known as a virtual colonoscopy,” said Dr. Brad Paulson, radiologist with Avera Medical GroupRadiology.Patientsmuststillundergocolonprepfor this test. A tube is placed in the rectum, and the colon is distended with carbon dioxide. The patient may be asked to drink a barium solution which is picked up by stool, but not polyps.
Images are produced in 2D, as well as a “fly through” which gives a view of traveling through the colon. While the colon and rectum are targeted by the test, the radiologist can also spot other abnormalities in the lower abdomen, for example, a tumor on a kidney. The test is 90 percent accurate in finding polyps or tumors that are 6 mm in size or larger.
Colonoscopy is the “gold standard” over CT colonography because polyps can be removed during the same procedure. Also, not all payors cover or
reimburse CT colonography. However, it’s a good screening option when colonoscopy is not possible. Key advantages are that the patient does not need sedation and it is less invasive than colonoscopy.
Avera Medical Group Gastroenterology has taken steps to make screening colonoscopy as accessible, comfortable and private as possible for patients, and also as effortless as possible for referring physicians and clinics. Endoscopic suites on the fifth floor of Plaza 1 on the Avera McKennan campus have less of a “hospital” feel, and are more like a physician’s office. Patients who meet screening recommendations can call to set up their own appointment, or a physician’s office can schedule a procedure.
ThroughAvera’sElectronicMedicalRecord,referringphysicians receive prompt documentation of the test and any pathology. Patients also are tracked, and receive notification when they are due for follow-up screenings.
“The specialists in our clinic are very experienced, and have a high success rate with removal of difficult polyps, and finding cancers. Our priority is to help stamp out colon cancer by increasing accessibility for recommended screenings,” Dr. Hill Jensen said.
A v e r a D i g e s t i v e D i s e a s e . o r g 8
Patient CT colonography performed by Dr. Brad Paulson
A v e r a D i g e s t i v e D i s e a s e . o r g
Adenoma Detection is a Key Measure of Colonoscopy Effectiveness
March is National Colorectal Cancer Awareness Month, a key time for primary care physicians to remind their patients to schedule a screening colonoscopy.
Studies show that people who are screened have a 90 percent reduced risk of developing colon cancer. Yet nationwide, only about 50 percent of people who are eligible for regular recommended screenings take advantage of it.
Colonoscopy is recommended beginning at age 50, and should be repeated every 10 years and every two to five years if polyps are detected. For African Americans, who are at higher risk for colorectal cancer, screening should begin at age 45. The incidence of colorectal cancer peaks at age 60. Colon cancer evolves slowly over time from polyps, so beginning screenings at age 50 gives physicians a chance to catch precancerous polyps in the 10-year window between age 50 and 60.
Colon cancer is distinguished from among many other cancer types in that it is largely preventable. Most colon cancers grow from adenomatous polyps which develop into cancer over a period of10to15years.Removingprecancerouspolypsduring that window of time virtually eliminates the potential for cancer.
Colonoscopy is most sensitive test for detecting colon polyps, because it examines the entire colon and gives the best visibility of any abnormalities. At the same time, the endoscopist can remove any precancerous polyps or biopsy suspicious lesions. Colonoscopy has the potential to stop the process of colon cancer development, and prevent future surgery and chemotherapy, making colonoscopy the most cost-effective screening tool.
In order to make a difference in preventing colorectal cancer, colonoscopies must not only be scheduled regularly, the procedure must be performed effectively.
Because of the high link between adenomatous polyps and colorectal cancer, adenoma detection rate(ADR)hasbeencalledthemostimportantquality indicator for lower bowel endoscopy. The minimum national benchmark is 25 percent for men and 15 percent for women. Determining factors include a good, clean bowel prep and a thorough, high quality colon exam.
A quality colonoscopy begins with the patient with colon prep. Experience and formal training of the endoscopist is important. Endoscopists need this specialized training to detect polyps or lesions that are as small as 1 mm in size, which even though small can be aggressive, and also to find polyps
9
“Our goals at the Avera Digestive Disease Institute are to get a greater number of patients in for their screening colonoscopy, and detect a high number of adenomas for the maximum benefit in cancer prevention. Future reimbursement is only a small part of the issue – the most important consideration is saving lives,” added Dr. Steven Condron, gastroenterologist with Avera Medical Group Gastroenterology.
A v e r a D i g e s t i v e D i s e a s e . o r g 10
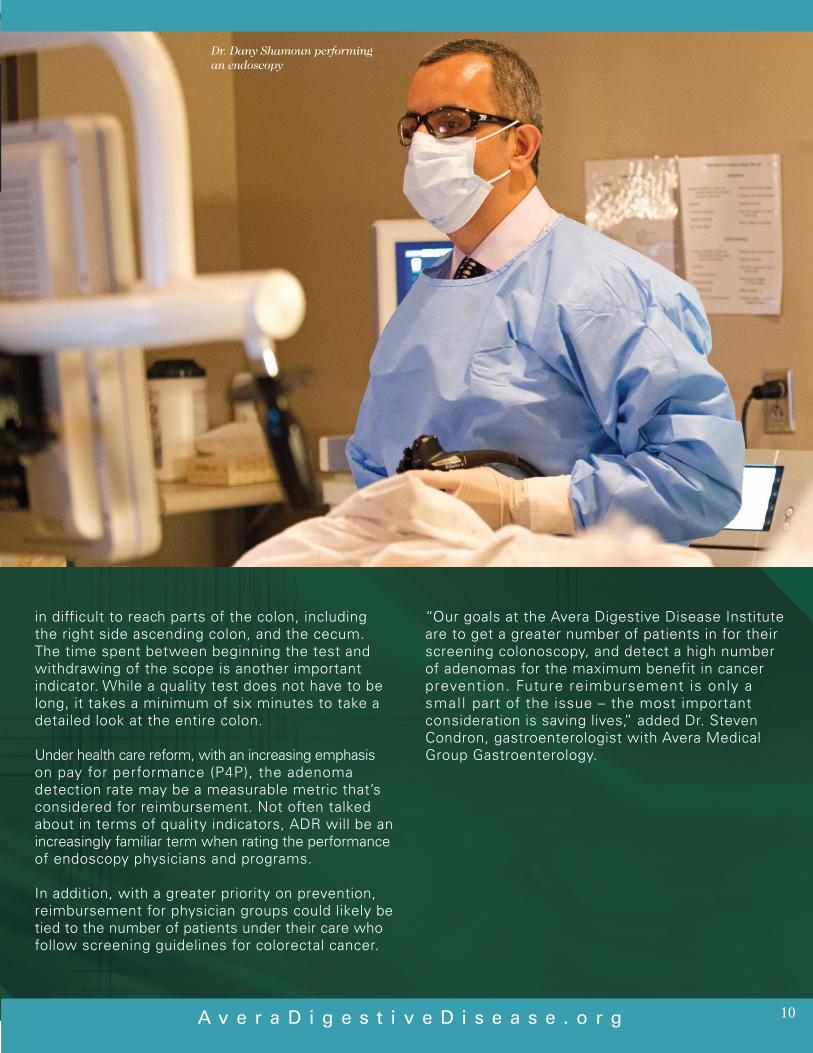
in difficult to reach parts of the colon, including the right side ascending colon, and the cecum. The time spent between beginning the test and withdrawing of the scope is another important indicator. While a quality test does not have to be long, it takes a minimum of six minutes to take a detailed look at the entire colon.
Under health care reform, with an increasing emphasis on pay for performance (P4P), the adenoma detection rate may be a measurable metric that’s considered for reimbursement. Not often talked aboutintermsofqualityindicators,ADRwillbeanincreasingly familiar term when rating the performance of endoscopy physicians and programs.
In addition, with a greater priority on prevention, reimbursement for physician groups could likely be tied to the number of patients under their care who follow screening guidelines for colorectal cancer.
“Our goals at the Avera Digestive Disease Institute are to get a greater number of patients in for their screening colonoscopy, and detect a high number of adenomas for the maximum benefit in cancer prevention. Future reimbursement is only a smal l part of the issue – the most important consideration is saving lives,” added Dr. Steven Condron, gastroenterologist with Avera Medical Group Gastroenterology.
Dr. Dany Shamoun performingan endoscopy

A v e r a D i g e s t i v e D i s e a s e . o r g11
Traditionally, colorectal surgery has involved a large incision and an open procedure, accompanied by a long hospital stay. Nationwide, approximately 40 to 50 percent of colon resections are laparoscopic, compared with about 70 to 80 percent at the Avera Digestive Disease Institute.
Whether a colon resection will be open, laparoscopic or robotic, there are several key principles that must be followed that constitute a high-quality procedure. “As long as these same principles are followed, we experience the same results with no change in outcomes or survival,” said Dr. Scott Baker, fellowship-trained colorectal surgeon. With minimally invasive techniques, patients see advantages such as less time in the hospital, less post-operative pain and an earlier return to work.
Quality surgical management begins at diagnosis, when gastroenterologists place an ink tattoo at the site of the tumor or lesion so the surgeon knows exactly where the tumor is located.
Patients first should be educated before surgery about their diagnosis and the surgical procedure that is best for their particular case. Preoperative testing includes a CT scan to rule out metastasis to distant sites such as the lung or liver, and a baseline CEA (carcinoembryonic antigen) level blood test. CEA is a protein normally found in the tissue of a developing fetus. Levels of this protein disappear or become very low after birth. In adults, an abnormal amount of CEA may signal cancer.
Also preoperatively, most patients undergo a bowel prep which is less extensive than the prep for colonoscopy. Patients are also treated with a preoperative antibiotic to prevent infection and DVT prophylaxis to prevent blood clots.
In most cases, tumors spread no further than 2 to 3 cm from the original site, so surgeons plan to remove a section of colon with 5 cm margins on each side of the tumor. Unless there are multiple adhesions or a very large tumor, most colon resection cases can be performed laparoscopically by an experienced surgeon. Single incision laparoscopy surgery (SILS) is a further evolution of laparoscopy. This procedure involves one small incision in the navel, with all instruments being placed through this central port
Harvesting at least 12 lymph nodes that drain from the affected area is necessary to ensure the cancer has not spread to the lymph nodes. Analyzing fewer than 12 nodes for cancer cells is not enough evidence to ensure that cancer has not spread. High ligation of the supplying vessels close to their origin helps ensure maximal lymph node harvest.
MinimallyInvasiveProceduresResultinLessPainandFasterRecovery
“Colorectal cancer is one of the curable cancers, if we catch it early enough. This requires regular screening as opposed to the patient presenting with symptoms, because by the time symptoms are present, the disease is usually fairly advanced,” Dr. Baker added.

Because some tumors grow from the inside of the colon out into other structures such as the bladder, small bowel or abdominal wall, all cancerous tissue needs to be removed through an en-bloc resection.
If there is widespread metastasis, colon resection is not scheduled, as it does not provide a greater survival benefit. However, if colorectal cancer has spread to the liver with one or two lesions in a part of a liver that can be removed, the patient reaps a huge benefit from resection. The same is true for an isolated metastatic lesion in the lung.
A v e r a D i g e s t i v e D i s e a s e . o r g 12
Whenever possible, the goal is to reattach the remaining colon, so the patient does not require a colostomy.
“Colorectal cancer is one of the curable cancers, if we catch it early enough. This requires regular screening as opposed to the patient presenting with symptoms, because by the time symptoms are present, the disease is usually fairly advanced,” Dr. Baker added.
Dr. Scott Bakerperforming surgery
Green lines indicate length of incisions which have dramatically decreased over time.
Evolution of Surgical Management of Colon Cancer
1 2 3 4
Open Procedure Hand Assist Laparoscopy SILS
MedicalandRadiationOncologyandPathologyPlayKeyRolesinCancerManagement
Depending on specific aspects of each particular case of colorectal cancer, medical and radiation oncology may play a key role in curative therapy, prevention of a recurrence, or palliative treatment.
Most stage 1 and 2 cancers that are surgically resectable do not need further treatment. Adjuvant chemotherapy is recommended as part of the treatment regimen for patientswithstage3and4cancers.Radiationoncologymay be recommended if the size or location of the tumor warrants.
Chemotherapy helps prevent recurrence by killing any remaining cancer cells. “Chemotherapy with stage 2 cancer remains a field of study,” said Dr. Addison Tolentino, medical oncologist with Avera Medical Group Oncology & Hematology. Most stage 2 patients will not have a recurrence, although there is a subgroup with a certain type of cancer at higher risk for recurrence, and genotyping is used to identify which cancers are more aggressive.
At stage 3, there is a definite indication for undergoing chemotherapy. At stage 3, the cancer has spread to as many as three lymph nodes, and/or to nearby tissues, and according to the literature, treating patients at stage 3 with chemotherapy will reduce recurrence by at least one-third.
Stage 4 is a subgroup that will not be cured, yet is treated with chemotherapy to decrease the chances of early death from cancer. Palliative chemotherapy is an option to provide relief from symptoms when cancer has already spread to other organs, or the cancer is considered incurable at the time of initial diagnosis or surgery. In such cases, chemotherapy, including molecular agents, may shrink the tumor and slow its growth.
Because colorectal cancer is a less aggressive type, chemotherapy treatments can be drawn out to make them easier to tolerate. Common side effects are diarrhea, mouth sores, neuropathy, sensitivity to cold, fatigue and low blood count.
Treatment options are individualized based on the tumor size, location and stage of the cancer.
Radiationtherapycanalsoplayapalliativeroleifcancerhas metastasized, or provide local control of cancer to slow its growth. While not as common, radiation oncology may be used in the upper colon when the affected segment of the colon is attached to the abdominal walls. It may also be used to treat residual disease after surgery. AveraMedicalGroupRadiologyofferstwomatchedARTISTE™linearaccelerators.CombinedwithadedicatedBrachytherapy Suite, this provides a comprehensive portfolio of advanced treatment delivery tools. Three-dimensional conformal radiation therapy is an advanced technology involving the use of CT scanners and computers to map the tumor in three-dimensional form, and then matchorconformbeamstothecancer’sshape.IMRT,intensity modulated radiation therapy, is an advanced type of three-dimensional radiation that conforms to the shape of a tumor. It uses hundreds of small radiation beams of varying intensities to precisely irradiate a tumor. The radiation intensity of each beam is controlled, and the beam shape changes hundreds of times during each treatment. As a result, the radiation beam conforms
A v e r a D i g e s t i v e D i s e a s e . o r g13
Dr. Addison Tolentino, medical oncologist with Avera Medical Group Oncology & Hematology

A v e r a D i g e s t i v e D i s e a s e . o r g 14
around healthy tissues in a way that delivers a more accurate distribution of dose to the tumor, and less dose to surrounding normal tissues.
Pathologists participate in the multidisciplinary approach to colorectal cancer care. In addition to the stage of the disease, the treatment approach depends on the type of tumor, determined through pathological study. In addition to diagnosing malignancy and type of malignancy, pathology offers molecular screening.
For example, approximately 15 percent of colorectal cancers can be attributed to instability in microsatellites, which are sequences of DNA. When criteria indicate, Avera pathologists can perform microsatellite instability (MSI) screening to determine if a tumor, biopsy or other specimen contains genetic mutations. Molecular test-ing can help physicians know how to better treat certain types of cancer. Testing also gives further insight on
prognosis. For patients, genetic testing can indicate the need for more frequent cancer screening to watch for specific types of cancer. Also, children and other relatives who may also carry the genetic risk can take measures to prevent future cases of cancer, for example, colonoscopy beginning at an earlier age than the recommended age of 50.
The most common hereditary syndromes include Lynch syndrome, which increases the risk of colon and other cancers, and familial adenomatous polyposis (FAP), which results in the formation of hundreds or thousands of precancerous polyps at an early age.
“Identifying patients and families with conditions like Lynch syndrome allows appropriate medical management and preventative services to be in place to reduce hereditary cancer risk and improve outcomes,” said Dr. RaedSulaiman,AveraMcKennanpathologist.
Dr. Raed Sulaiman,Avera McKennan pathologist

A v e r a D i g e s t i v e D i s e a s e . o r g
Cancer is a life-changing diagnosis, so the Avera Cancer Institute offers resources to help patients and their families cope.
Social workers consult with patients and families through all phases of the cancer journey, with services based on need throughout the entire continuum of care, whether that’s at diagnosis, treatment, survivorship, or end-of-life care and grief and loss.
Social workers help patients and families by:• Accessinginformationabouttheirdiagnosisand proposed treatment• Helpingtofindwaystocopewiththediagnosis• Stagingfamilymeetingsorcounseling• Referringtocommunityresourcesforpatientswho
live at a distance from Sioux Falls• Helpingpatientsaccesstherightteammemberfor
a particular concern, whether it’s a need for patient advocacy, financial counseling, spiritual care, a dietary consultation, home care or hospice
• Helpingpatientssetupadvancedirectives,durablepower of attorney for health care or a living will
• Workingwithpatientsaftertreatmenttodeterminewhat’s next, whether it’s going back to work, applying for disability assistance or clarifying insurance
concerns• Connectingfamilieswithtransportationorlodging assistance• Referringorinvitingpatientstovarioussupportgroups
and programs, including “A Time to Heal,” a survivorship support program for people who have completed cancer treatment for all diagnoses
“We help people identify what their needs are and what’s available. Many patients don’t think they need a ‘social worker,’ but it’s nice to have some additional support outside of one’s typical circle,” said Lynne Hunter, oncology social worker.
When a patient or family’s need is spiritual care, Mary Guth is available for one-on-one visits or family meetings. She’s available for people who may have anxiety about their diagnosis, or a spiritual concern, for example, at end of life or in reconciling a relationship. Spiritual Care includes:• Emotionalsupportforcaregivers• Socialsupportforthepatient• Contactforthepatientwithhisorherpastororchurch• Counselforethicalormoraldilemmas• Counselinsearchingformeaninginlife• Grieforbereavementsupport• Supportforcarestaff
Guth also makes rounds in infusion centers. A spiritual need may arise at that time, leading to ongoing support. Families and caregivers are offered this support as well, throughout a loved one’s illness as well as time of bereavement.
“We want to provide hope, empower people to express their feelings, and help them find the strength to move forward and experience inner peace,” Guth said. Cancer patients and their families often have a need to feel connected. “We want them to know they are part of a community at the Avera Cancer Institute, and we want to be supportive and helpful in any way we can.”
Social Work and Spiritual CareResourcesProvideAddedSupport
Lynne Hunter, oncology social worker
15
A v e r a D i g e s t i v e D i s e a s e . o r g 16
After treatment of colon cancer, patients of the Avera Digestive Disease Institute receive follow-up care and surveillance in order to monitor their health and any sign of recurrence, based on guidelines set by the National Comprehensive Cancer Network (NCCN).
A summary of these guidelines is as follows:• Patientsdiagnosedwithstage1and2tumorsdonot
need to receive adjuvant therapy; a colonoscopy is recommended after one year. If an advanced adenoma is found, a colonoscopy should be repeated again after a year, there is no advanced adenoma, the patient should receive a repeat colonoscopy in three years and then every five years.
• Patientsdiagnosedatstage3and4arefollowed up with a clinical trial, observation, or, adjuvant chemotherapy, depending on risk of recurrence.
Follow-up for patients at all stages of colorectal cancer:• AphysicalexamandhistoryandCEA(carcinoembryonic
antigen) test every three to six months then every six months for five years
• Colonoscopyafteroneyear;ifanadvancedadenomais found, a colonoscopy should be repeated again after
a year, there is no advanced adenoma, the patient should receive a repeat colonoscopy in three years and then every five years.
• Colonoscopyafterthreetosixmonthsiftherewasanobstructive lesion preventing a preoperative colonoscopy.
Additional follow-up for patients at stages 3 and 4:• Chest/abdominal/pelvicCTannuallyforuptofiveyears
for patients at high risk for recurrence
Statistics reveal that colorectal cancer metastasizes to distant sites in approximately 15-20 percent of cases. If cancer does metastasize, 90 percent of the time this happens within three years.
“It’s important for patients and primary care physicians to understand that if it does spread and we find it early, treatment can be effective for a cure or increased survival. The danger is when patients fall out of the post-cancer screening. Once symptoms appear, it is often too late,” said Dr. Michael Person, surgeon with Surgical Institute of South Dakota. “We want to manage this disease as a chronic illness – not as an acute illness that is life-threatening to the patient.”
After-Treatment Surveillance HelpsMinimizeThreatofRecurrence

Colorectal Surgery:Scott L. Baker, MD, FACS, FASCRS
Gastroenterology andHepatology:Steven Condron, MD, MHES, FACPCristina Hill Jensen, MDChristopher Hurley, MDLarry W. Schafer, MD, FACPDany Shamoun, MD
General Surgery:Scott L. Baker, MD, FACS, FASCRSMichael Bauer, MD, FACSWade E. Dosch, MD, FACSDavid Flanagan, MDThomas E. Fullerton, MDMichael Person, MD, FACSDavid A. Strand, MD, FACSBradley C. Thaemert, MD, FACSDonald J. Wingert, MD, FACS
Genetics: Nicole Mattila, CGC, MS
Hepatology:Hesham Elgouhari, MD, FACPMumtaz Niazi, MD
Multidisciplinary Team Includes the Following Areas of Specialty:
Medical Oncology:David Elson, MDMark R. Huber, MDMichael McHale, MDHeidi McKean, MDAddison R. Tolentino, MD
Pathology: Steven P. Olson, MD Bruce R. Prouse, MDRaed A. Sulaiman, MD
Radiation Oncology: Barbara Schlager, MDKathleen L. Schneekloth, MDJames Simon, MD
Radiology:Sabina Choudhry, MDBrad A. Paulson, MD
Research (Cancer clinical trials)
Transplant Surgery:Christopher Auvenshine, DOTariq N. Khan, MD
Urogynecology: Matthew A. Barker, MD, FACOG
w w w . A v e r a D i g e s t i v e D i s e a s e . o r g
If you have any questions or would like to make a referral to theAvera Digestive Disease Institute, call 605-322-7797.
17

To learn more, visit our website atAveraDigestiveDisease.org
Go Online to Learn More!
18

Hours: 8 a.m. - 5 p.m. • 605-322-7797
To learn more, visit our website atAveraDigestiveDisease.org
1325 S. Cliff AvenueSioux Falls, SD 57105
ADDI-26704-REVJA2313