diet and eating disorders health psychology chapter 7 october 8-10, 2007 classes #20-21
TRANSCRIPT
Diet and Eating Disorders
Health PsychologyChapter 7
October 8-10, 2007Classes #20-21

Nutrition
46 nutrients are required
- Water is most important
- Others: protein, fats, carbohydrates, minerals, and vitamins
Glycemic Index
Ranks carbohydrates on how quickly your body converts them to sugar glucose
- Index ranges from 0-100
- Higher ranges for those foods that cause the most rapid rise in blood sugar
- For example: pure glucose has GI = 100
Our bodies perform best when blood sugar is relatively constant
History of the GI
The GI was initially developed to “standardize” the body’s glycemic response after eating a carbohydrate-rich food
Today the GI is being touted as a dietary planning tool to promote weight loss, prevent obesity, and reduce the risk for chronic diseases
- despite a lack of scientific evidence to support such claims

Definitions of GI
Often used (but inaccurate) definitions:
- Rate of digestion and absorption of a carbohydrate-rich food
- Blood glucose response to a carbohydrate rich food
Accurate definition of GI is much more complicated:
- The incremental area under the blood glucose response curve of a 50g portion of available carbohydrate of a test food expressed as a percentage of the response to the same amount of the reference food (i.e., white bread or glucose)

Measuring GI
Standardized methodology for measuring GI
- Subjects:
- Typical sample size is 10-12 subjects
- Subjects in a given sample must be matched for glucose tolerance (i.e., all subjects must be diabetic or glucose intolerant, or “normal”)
- Protocol:
- Subjects come into a laboratory after an overnight fast
- Subjects consume, in random order, 50g of carbohydrate of the test food (e.g., red potatoes ) or reference food (e.g.,glucose) and come back another day to test the alternate food.

Measuring GI- Protocol (cont.)
- Blood glucose is measured every 15-30 minutes for at least 2 hours and values are plotted on a graph.
- Area under the curve (AUC) is calculated and GI is determined:- GI = [AUC of test food (e.g., red potatoes) ÷ AUC of reference food (e.g.,
glucose] ÷ 100
0
1
2
3
4
5
6
7
8
9
0 30 60 90 120
redpotatoesglucose
Minutes
Pla
sma
gluc
ose
(mm
ol/L
)

GI Classification
Category Glucose Reference White Bread Reference
Low < 55 < 60
Medium 55-70 60-85
High > 70 > 85
Brand-Miller. The New Glucose Revolution. 1996
Note: There was no research conducted to establish the cut-off values for the GI.
Limitations of the GI
Many factors affect the GI of a carbohydrate-rich food, limiting its practicality and applicability
1. Processing/preparation
2. Ripeness
3. Variety or origin
4. Inclusion of other foods or condiments
5. Variability in the measurement
– Time of day
– Between subject variation
– Within subject variation

Limitations of the GI1. Processing/preparation- Alteration of food form
- Changing the physical form or particle size by mashing, grinding, rolling, even thoroughly chewing can increase the GI of a food
- Heating and cooling certain carbohydrates can result in the formation of resistant starch and produce a lower GI
- Example: Heating and cooling potatoes results in a significantly lower GI
- Cooking method and duration

Limitations of GI
2. Ripeness- Ripening generally decreases GI
- Example: the GI of a green banana would be higher than that for a ripe banana
3. Origin/Variety- Variable GIs of similar foods from different countries
- Russet Potato (Canada): 56
- Russet Potato (USA): 76
- Russet Potato (Australia): 85
- Variable GIs for different varieties of similar food
- Long-grain instant white rice: 75
- Long-grain wild rice: 54

Limitations of the GI
4. Addition of other macronutrients
- Protein
- Lowers the GI but increases insulin response
- Fat
- Lowers the GI, but increases the calorie content
- Fiber
- Impact of fiber on GI is controversial
- Soluble vs insoluble
- Experimental vs practical applications
brown rice: 55 vs white rice: 64
whole wheat bread: 71 vs white bread: 70
wheat spaghetti: 37 vs white spaghetti: 42

Limitations of the GI
4. Addition of other macronutrients (cont.)
- Single foods vs mixed meals
- Usefulness of GI in the context of mixed meals is controversial
- GI of a single food much less important than overall GI of a given meal or snack

Limitations of the GI
5. Variability in the measurement:
- Time of day
- Morning vs afternoon
- Between similar foods
- whole milk: 11-40 - ice cream: 36-68
- glucose: 85-111
- Between & within subjects:
Standard Coefficient of Deviation Variation(%)
Within-subject: 15.9 21
Between subject: 5.8 8

Limitations of the GI A low GI diet does not promote weight loss
Reference Duration Diets
(Isoenergetic)
Weight Loss Differences
Jenkins et al. 1985 4 weeks Low-GI vs Low Fat diet Low GI > High GI
Jenkins et al. 1987a 2 weeks Low-GI vs High-GI Not Significant (NS)
Jenkins et al. 1988 2 weeks Low GI vs. High-GI High GI > Low GI
Jenkins et al. 1987b 4 weeks Low-GI vs High-GI Low GI > High GI
Brand et al. 1991 12 weeks Low-GI vs High-GI NS
Fontvielle et al. 1992 5 weeks Low-GI vs High-GI foods NS
Frost et al. 1994 12 weeks Low-GI vs High-GI foods NS
Frost et al. 1998 3 weeks Low-GI vs High-GI foods NS
Luscombe et al. 1999 4 weeks Low-GI vs High-GI foods NS
Jarvi et al. 1999 24 days Low-GI vs High-GI diets NS
Tshillas et al. 2000 6 mo Low-GI vs High-GI breakfasts NS
Giacco et al. 2000 24 weeks Low-GI vs High-GI foods NS
Alfenas & Mattes 2004 8 days Low-GI vs High-GI diets NS
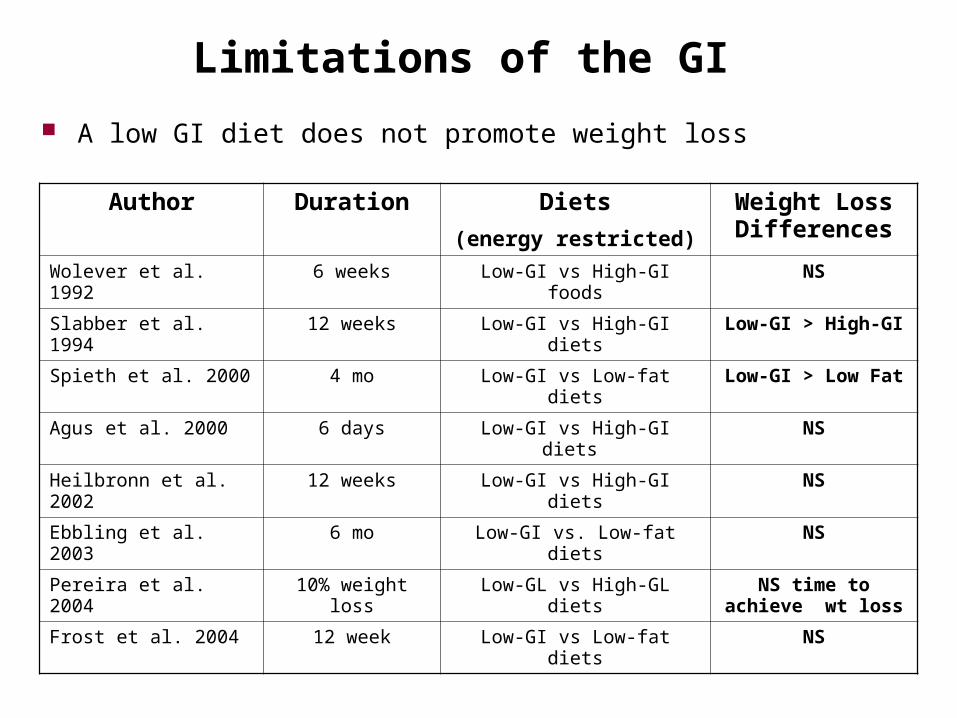
Limitations of the GI
A low GI diet does not promote weight loss
Author Duration Diets
(energy restricted)
Weight Loss Differences
Wolever et al. 1992 6 weeks Low-GI vs High-GI foods NS
Slabber et al. 1994 12 weeks Low-GI vs High-GI diets Low-GI > High-GI
Spieth et al. 2000 4 mo Low-GI vs Low-fat diets Low-GI > Low Fat
Agus et al. 2000 6 days Low-GI vs High-GI diets NS
Heilbronn et al. 2002 12 weeks Low-GI vs High-GI diets NS
Ebbling et al. 2003 6 mo Low-GI vs. Low-fat diets NS
Pereira et al. 2004 10% weight loss Low-GL vs High-GL diets NS time to achieve wt loss
Frost et al. 2004 12 week Low-GI vs Low-fat diets NS

Bottom Line
GI is NOT practical
- A complex physiological measure
- Laboratory assessment does not readily translate to how we normally eat
- GI is not an inherent property of a food
- Readily altered by variety, origin, cooking, processing, and the addition of other nutrients and foods
- Limitations of GI are numerous
GI has not been shown to be associated with:
- Satiety or satiation
- Weight loss
- Nutrient density
Basal Metabolic Rate
Basal metabolic rate (BMR) is the amount of energy expended while at rest in a neutrally temperate environment, in the post-absorptive state (meaning that the digestive system is inactive, which requires about twelve hours of fasting in humans). If you've noticed that every year, it becomes harder to
eat whatever you want and stay slim, you've also learnt that your BMR decreases as you age. Likewise, depriving yourself of food in hopes of losing weight also decreases your BMR, a foil to your intentions.
M > W (more muscle) Exercise increases BMR
Set Point Theory
Set point is the weight that your body wants to be… It is a self-regulatory system that maintains your
body weight If you starve yourself the hypothalamus
activates compensatory mechanisms, your metabolism slows so that energy stores are used more sparingly and the amount of insulin that is produced increases so that more of the food that you take in remains as fat (this makes it possible to maintain weight on a meager diet)
Obesity
Weight which is 20-40% above the normal standard for a person’s height (BMI over 30 kg/m2) Rates of obesity are climbing and have risen from
12 to 20 percent of the population since 1991. An ominous statistic which indicates that the
epidemic of obesity may get even worse is that the percentage of children and adolescents who are obese has doubled in the last 20 years
Why is this happening?
Obesity
Why do some people become seriously overweight? Emotional problems
Depression Anxiety
Sedentary lifestyle Too much TV and not
enough exercise Genetics
Higher set point

What factors help prevent obesity? Preventing obesity must begin in
childhood Breastfed children less obesity Encouraging children to exercise
and eat healthy foods don’t use “special food” as a
reward – Stanek et al. (1990) children tend to be more
interested in a “forbidden food” –– Mennella et al. (2001)
Limiting television watching Problem with adult modeling,
increase consumption of snacks low in nutrients and watching TV during meals increase consumption of salty snacks and pop and less fruit and vegetables – Goldberg et al. (2001)
Many ads have low-nutrient beverages and sweets – Story and Faulkner (1990)

How is obesity treated?
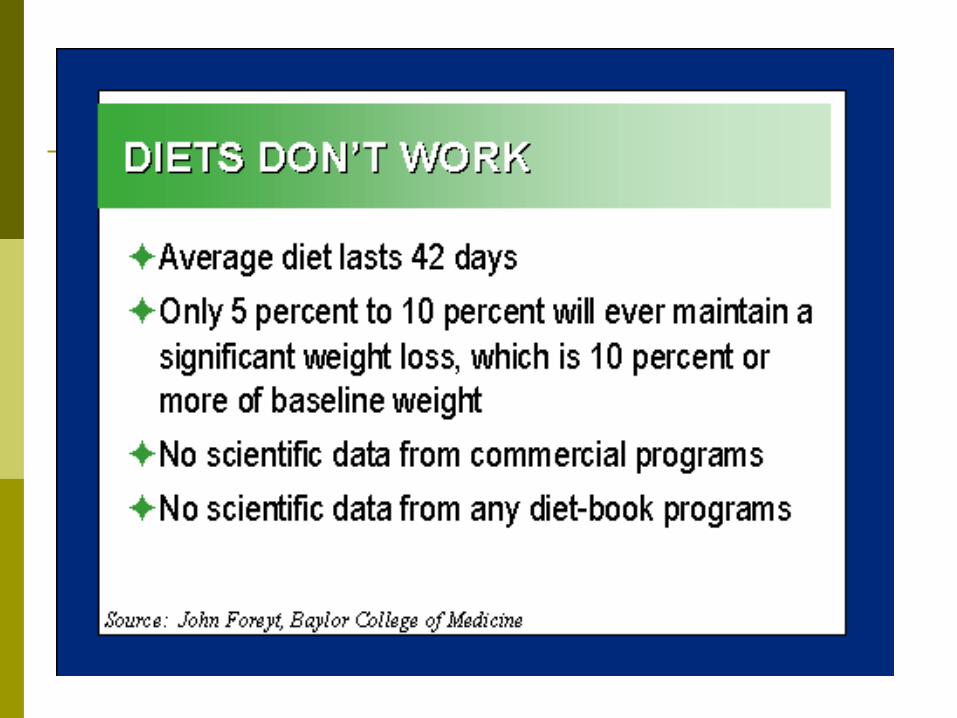
Fad Diets Exaggerated claims based on false
theories Potentially harmful
Weight Cycling Set point theory? Psychological ramification



Weight Cycling
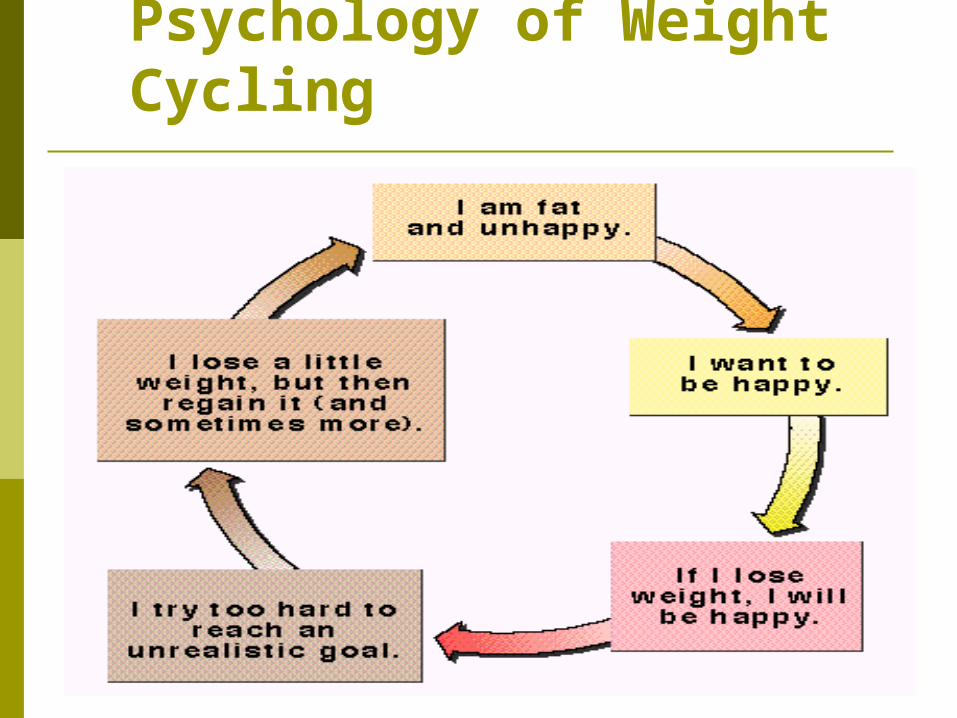
Psychology of Weight Cycling

Pills, Procedures and other Possibilities Diuretics - rapid loss of water and minerals Amphetamines (speed)
historical use, not approved by FDA, Addictive, ineffective
Prescription drugs interfere with fat absorption, suppress appetite
dexfenfluramine increased serotonin (neurotransmitter) psychological problems Heart problems
Over-the-Counter Drugs taste suppressants

Pills, Procedures and other Possibilities Very-Low-Calorie Diets (VLCD)
promote rapid weight loss physician supervised 800 kcal, 1 gram protein/kg body weight little or no fat little CHO (not enough to spare protein) starvation Potential cardiovascular and respiratory
problems Not very successful in keeping weight off (long
term)

Pills, Procedures and other Possibilities Weight
management approaches gastric stapling,
intestinal bypass, gastric balloons, wiring jaw closed (liquid diet)

How is obesity treated? Eating less Realistic energy intake
rapid weight loss is protein and water loss rule of thumb: 10 kcal/pound promotes weight loss
Nutritional Adequacy/Nutrient Dense Foods difficult to achieve on less than 1200 kcal food guide pyramid principles adequate water - sense of fullness

How is obesity treated?
Physical Activity - Increasing exercise Activity and BMR- activity increases BMR Activity and appetite control
energy released from stores (plasma glucose normal) digestive functions are suppressed
Physical Activity setting short-term goals reminders or prompts making behavior fit into daily schedule/ routine

How is obesity treated? Operant conditioning approaches
Make small changes to behavior Having the support of family members, and
friends – social support Other self-control approaches Behavior and Attitude stimuli behavior consequence Awareness of behavior
why do I eat, when, where
Eating Eating DisordersDisorders

Eating Disorders: An Overview
Two Major Types of DSM-IV Eating Disorders Anorexia nervosa and bulimia nervosa Both involve severe disruptions in eating behavior Both involve extreme fear and apprehension about
gaining weight Both have strong sociocultural origins –Westernized views
Other Subtypes of DSM-IV Eating Disorders Binge-eating disorder Rumination disorder Pica Feeding disorder

Anorexia Nervosa
Anorexia Nervosa Self-starvation and severe weight loss Usually starts as an innocent diet that went out
of control They eat less and exercise more Often they come from high-achieving or over-
protective families At first, self-esteem was raised – “you look
great”

Symptoms Of Inadequate Energy Intake
Amenorrhea Cold hands/feet Constipation Dry skin/hair loss Headaches Fainting/dizziness Lethargy Anorexia
Concentration Decisions Irritability Depression Social withdrawal Obsessiveness
(food)
Physical health Mental health

Anorexia Nervosa
Complications Hypothermia may result
Results when the body’s natural isolation fat stores become non-existent and the victim becomes cold all the time
Some must be tube-fed to prevent death Some will die from heart failure
Anorexia Nervosa
Prognosis With individual, group, and family therapy there is
a good chance for improvement and hopefully recovery
Anti-depressants are often combined with these therapies
It is a life-long process though

Anorexia Nervosa (pursuit of thinness) Successful Weight Loss – Hallmark of Anorexia
Defined as 15% below expected weight Intense fear of obesity and losing control over eating Anorexics show a relentless pursuit of thinness, often
beginning with dieting DSM-IV Subtypes of Anorexia
Restricting subtype – Limit caloric intake via diet and fasting
Binge-eating-purging subtype – About 50% of anorexics Associated Features
Most show marked disturbance in body image Most are comorbid for other psychological disorders Methods of weight loss can have severe life threatening
medical consequences

Anorexia: Facts and Statistics
0.5-5% 15-19 year old females Majority are female (90-95%) and white (>
95%), from middle-to-upper middle class families
Usually develops around age 13 or early adolescence
Tends to be more chronic and resistant to treatment than bulimia
3rd most common chronic illness in adolescents


Major Systems Affected Metabolic
Hypometabolism/Refeeding Syndrome
Cardiovascular Arrhythmias
Musculoskeletal Osteoporosis
Reproductive Amenorrhea

Bulimia Nervosa (avoidance of obesity) Associated Features
Most are within 10% of target body weight
Most are over concerned with body shape, fear gaining weight
Most are comorbid for other psychological disorders
Purging methods can result in severe medical problems

Bulimia Nervosa
Disorder characterized by repeated binge-purge episodes of overeating followed by vomiting or using a laxative
Again, mostly women in their early teens These individuals can be thin, average in
weight or even overweight – so this one is more likely to go unnoticed by family or friends

Bulimia Nervosa
Symptoms of Bulimia Eating binges Purging Sore throat Mouth and throat ulcers Swollen salivary glands Destruction of tooth enamel Depression, obsessive-compulsive symptoms
Bulimia Nervosa
Prognosis With the long-term psychotherapy combined with
group and family therapy the patient will likely improve
Often, anti-depressants are combined with therapy
Again, this is a life-long process
Bulimia: Facts and Statistics
Bulimia Majority are
female, with onset around 16 to 19 years of age
Lifetime prevalence is about 1.1% for females, 0.1% for males
5-10% of college women suffer from bulimia
Tends to be chronic if left untreated

Signs And Symptoms Of Vomiting Or Laxative Abuse
Weight loss Electrolyte
disturbance K CO2
Dental enamel erosion
Hypovolemia Knuckle calluses
Guilt Depression Anxiety Confusion
Physical health Mental health

At-Risk Groups for both AN and BN Adolescent females
with low self-esteem
Gymnasts
Dancers (ballet)
Wrestlers
Runners
When thinness is
related to success
AN & BN: Engaging Parents in Treatment Developmental framework (child adult)
Discuss blame, fault, guilt openly
Realignment of roles in family
Positive framing of family attributes
Future orientation
Authority to treat, and empowerment of, professionals comes from parents

Problems Addressed In Mental Health Treatment
Low Self-esteem Distorted body-image Dysfunctional coping
behaviors and habits Depression
SSRIs for BN and weight recovered AN
Ineffective communication
Conflict resolution Lack of assertiveness Post-trauma recovery
(sexual abuse, etc)

Indications for Hospitalization
Severe malnutrition: Weight for height <75%
Dehydration Electrolyte disturbances Cardiac dysrhythmia Physiologic instability
Severe bradycardia or hypotension Hypothermia Orthostatic pulse changes
http://www.adolescenthealth.org/html/eating_disorders.html

Indications for Hospitalization
Arrested growth and development
Failure of outpatient treatment
Acute food refusal Uncontrollable bingeing
and purging Acute medical
complication of malnutrition
Acute psychiatric emergencies
Comorbid diagnosis interfering with treatment
(Fisher et al: JAH 1995;16:420-437)

Eating Disorder, Not Otherwise Specified All criteria for AN, except still menstruating All criteria for AN, except normal weight All criteria for BN, except frequency or
duration Compensatory weight control after small
amounts of food Chewing/spitting out, but not swallowing,
large amounts of food Binge eating disorder

Binge-Eating Disorder Binge-Eating Disorder – Appendix of DSM-
IV Experimental diagnostic category Engage in food binges, but do not
engage in compensatory behaviors Associated Features
Many persons with binge-eating disorder are obese
Most are older than bulimics and anorexics
Show more psychopathology than obese people who do not binge
Share similar concerns as anorexics and bulimics regarding shape and weight

Signs And Symptoms Of Binge Eating
Weight gain Bloating Fullness Lethargy Salivary gland
enlargement
Guilt Depression Anxiety
Physical health Mental health

How do biological factors lead to eating disorders?
Women who have close relative with an eating disorder are 2-3 times more likely to suffer from one
More likely to occur in both identical twins than fraternal twins (higher concordance)
Anorexa sufferers have higher levels of serotonin
Bulimia sufferers are less sensitive to serotonin

What psychological factors lead to eating disorders? Cultural norms
Thinness norm is portrayed in media
Brazilian model Ana Carolina Reston…this 21-year-old anorexic model reportedly weighed just 88 pounds

What psychological factors lead to eating disorders? Family dynamics
Families of women with eating disorders are particularly focused on weight and shape
Families of anorexics have potentially dysfunctional dynamics
Families of bulimics have more conflict, and less nurturance

What psychological factors lead to eating disorders? Personality
The “perfect child” expectation in families Anorexics: rigid, anxious, perfectionists, and
obsessed with order and cleanliness Bulimics: depressed, anxious, lack clear sense
of self-identity, have negative self-views

What approaches help prevent eating disorders? Interventions specifically targeting women
with poor body images can be effective
Weight Gain
Rate 1 lb/week, Target weight >85% average, if low...
70% of weight gain is lean body mass (muscle)
Must eat adequately to gain lean body mass
Lean body mass will result in Higher metabolism More energy Fewer symptoms
Cognitive-behavioral therapy is used to design programs for weight gain

“But, I’m Not Hungry”
Body burns calories throughout life
Appetite need to eat Eating Disorder Appetite If only respond to appetite,
will not get enough energy If eat on regular schedule,
more likely to get energy Higher energy fuel ensures
greater likelihood of getting enough energy
Even if you’re not hungry, your body burns calories
Appetite car’s gas gauge Eating Disorder broken
gas gauge If drive car with broken gas
gauge can run out of gas Fill car with gas based on
miles driven & gas mileage Fat has more energy than
carbohydrate or protein and is a necessary body fuel
Physiologic Fact Reframing for patient

Lingering issues…
Is obesity really unhealthy? “upper-body fat” is particularly bad
Can eating disorder prevention programs have dangerous effects? Eating disorder prevention programs can sometimes lead
to an increase in disordered behavior Nova film, “Dying to be Thin” - emaciated women are
triggering girls who want to be thin. Instead… Show the videos: “Body Talk”, or “Killing Us
Softly”. Shows being able to express their body image and resist media messages.

Credits Slides 2-17 primarily prepared by:
http://www.healthypotato.com/downloads/Glycemic_Index_8-8-05.ppt
http://www2.una.edu/psychology/health/ch08%20obesity2.ppt#1