diarrhea in child travelers
TRANSCRIPT
Diarrhea in Child Travelers
Eyal Leshem
Viral Gastroenteritis Team
CISTM14, Quebec City
National Center for Immunization & Respiratory Diseases
Division of Viral Diseases



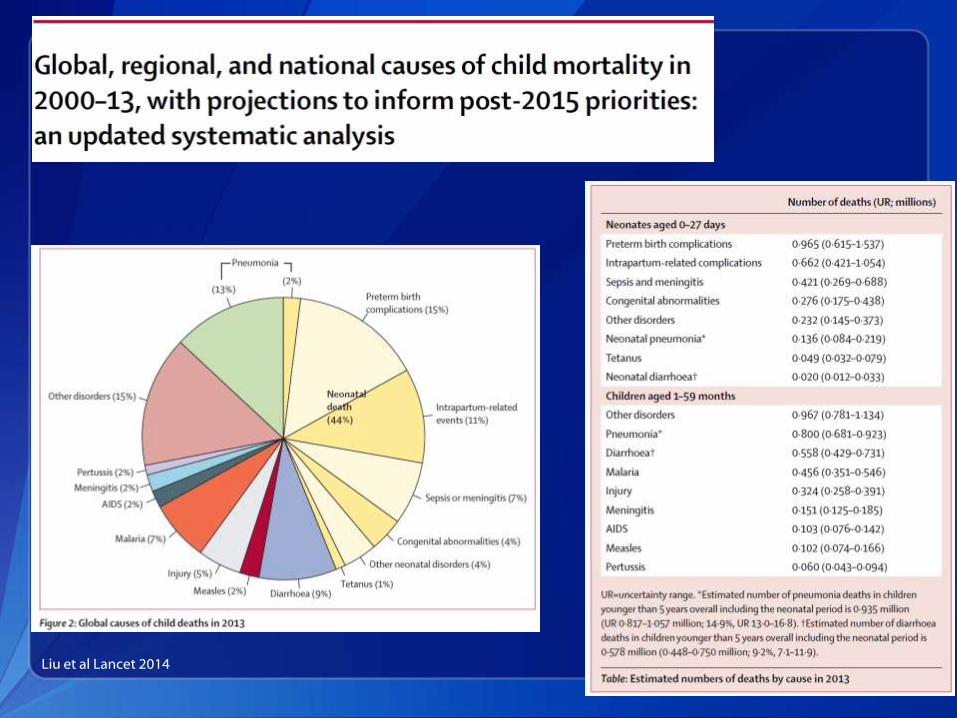
Liu et al Lancet 2014

Liu et al Lancet 2014

Kotloff et al Lancet 2013

Steffen et al JAMA 2015

Kendell et al CID 2012

Pediatric Traveler’s Diarrhea
We know what causes pediatric diarrhea in developing countries
We know what causes travelers diarrhea
Kean, Annals of Intern Med 1963
Pediatric Traveler’s Diarrhea
We know what causes pediatric diarrhea in developing countries
We know what causes travelers diarrhea
What do we know about pediatric travelers diarrhea??
Kean, Annals of Intern Med 1963
Regimen Thailand Mexico
A Rehydration, ORS only
B Fluids and loperamide
C Fluids and bismuth subsalicylate
D Fluids and rifaximin
E Fluids and co-trimoxazole
F Fluids and ciprofloxacin
G Fluids and azithromycin
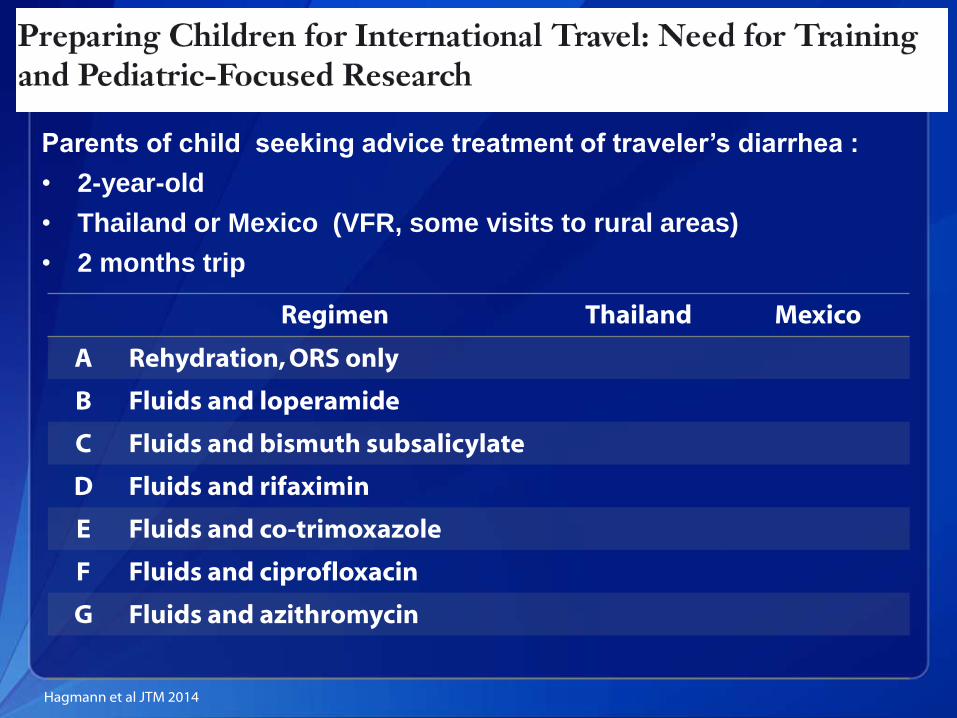
Hagmann et al JTM 2014
Parents of child seeking advice treatment of traveler’s diarrhea :
• 2-year-old
• Thailand or Mexico (VFR, some visits to rural areas)
• 2 months trip
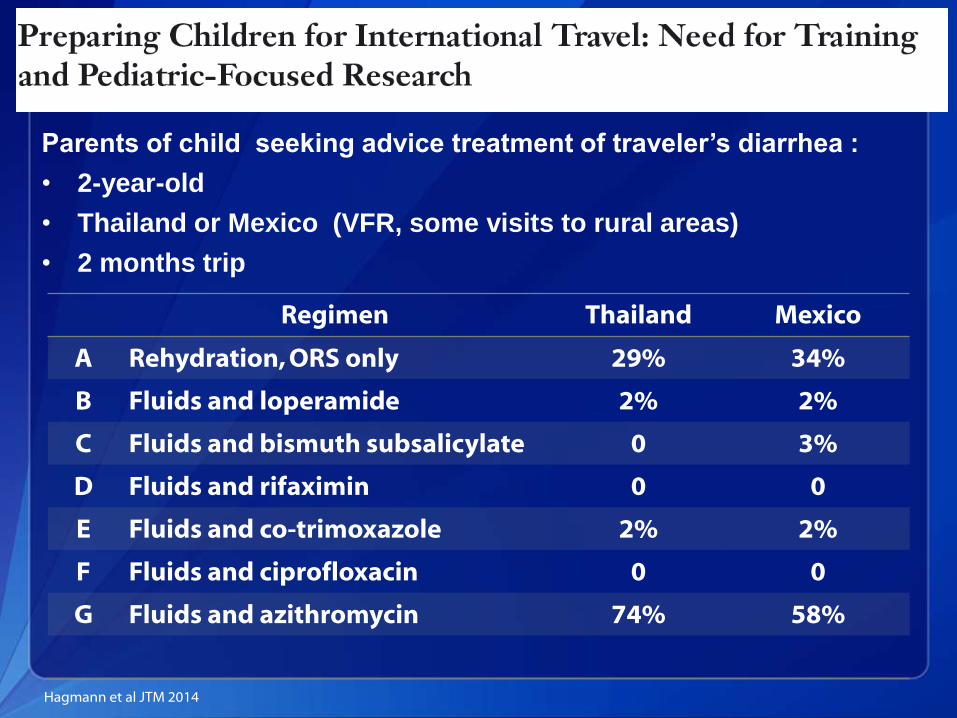
Regimen Thailand Mexico
A Rehydration, ORS only 29% 34%
B Fluids and loperamide 2% 2%
C Fluids and bismuth subsalicylate 0 3%
D Fluids and rifaximin 0 0
E Fluids and co-trimoxazole 2% 2%
F Fluids and ciprofloxacin 0 0
G Fluids and azithromycin 74% 58%
Hagmann et al JTM 2014
Parents of child seeking advice treatment of traveler’s diarrhea :
• 2-year-old
• Thailand or Mexico (VFR, some visits to rural areas)
• 2 months trip
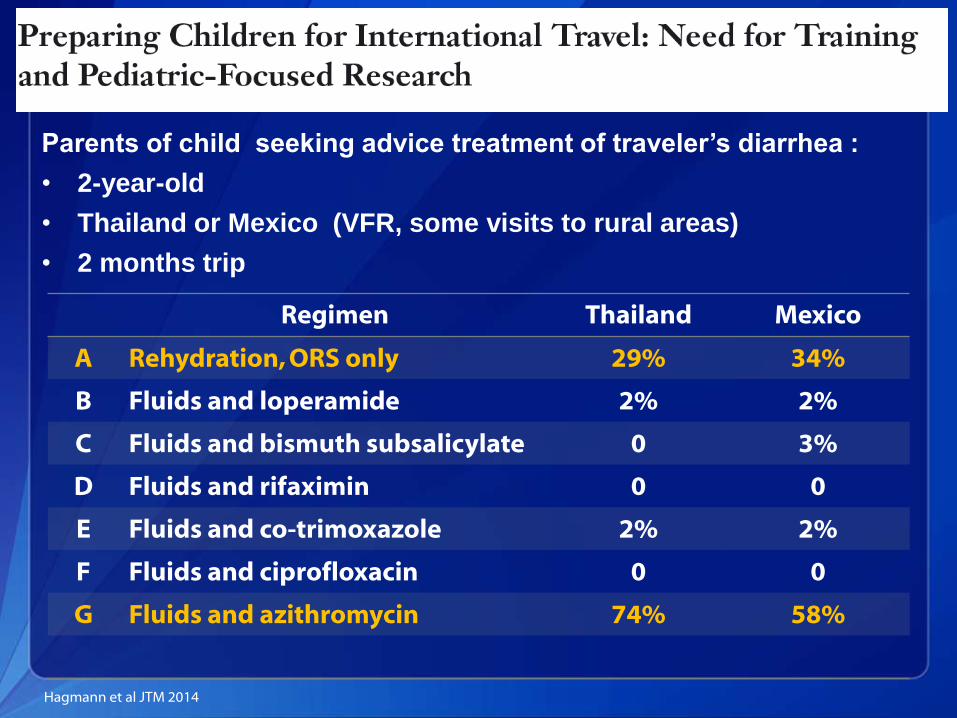
Regimen Thailand Mexico
A Rehydration, ORS only 29% 34%
B Fluids and loperamide 2% 2%
C Fluids and bismuth subsalicylate 0 3%
D Fluids and rifaximin 0 0
E Fluids and co-trimoxazole 2% 2%
F Fluids and ciprofloxacin 0 0
G Fluids and azithromycin 74% 58%
Hagmann et al JTM 2014
Parents of child seeking advice treatment of traveler’s diarrhea :
• 2-year-old
• Thailand or Mexico (VFR, some visits to rural areas)
• 2 months trip
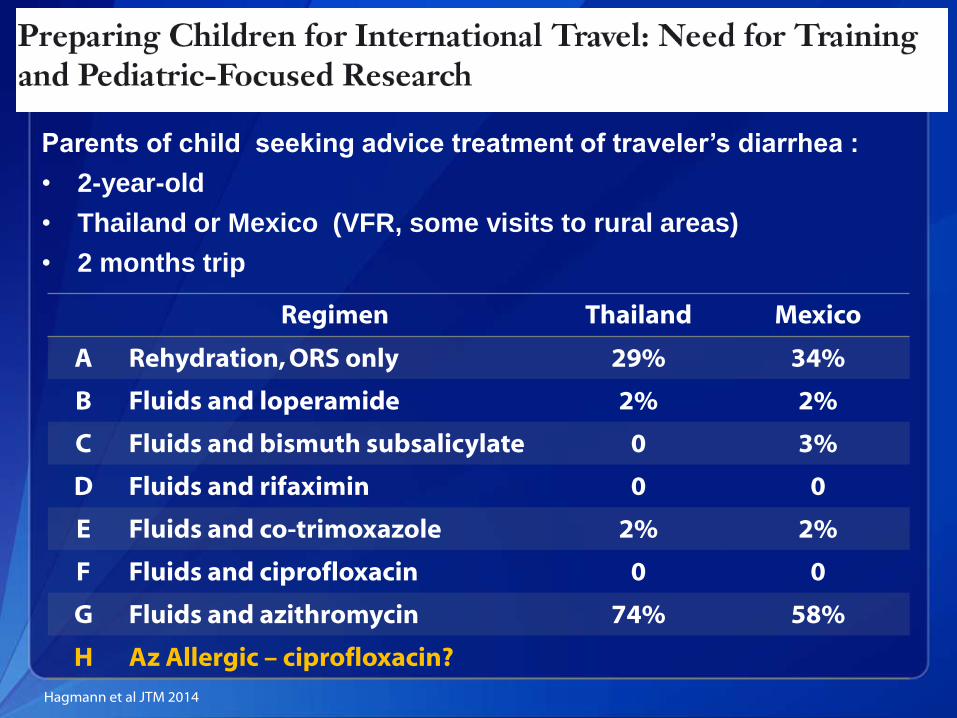
Regimen Thailand Mexico
A Rehydration, ORS only 29% 34%
B Fluids and loperamide 2% 2%
C Fluids and bismuth subsalicylate 0 3%
D Fluids and rifaximin 0 0
E Fluids and co-trimoxazole 2% 2%
F Fluids and ciprofloxacin 0 0
G Fluids and azithromycin 74% 58%
H Az Allergic – ciprofloxacin?
Hagmann et al JTM 2014
Parents of child seeking advice treatment of traveler’s diarrhea :
• 2-year-old
• Thailand or Mexico (VFR, some visits to rural areas)
• 2 months trip
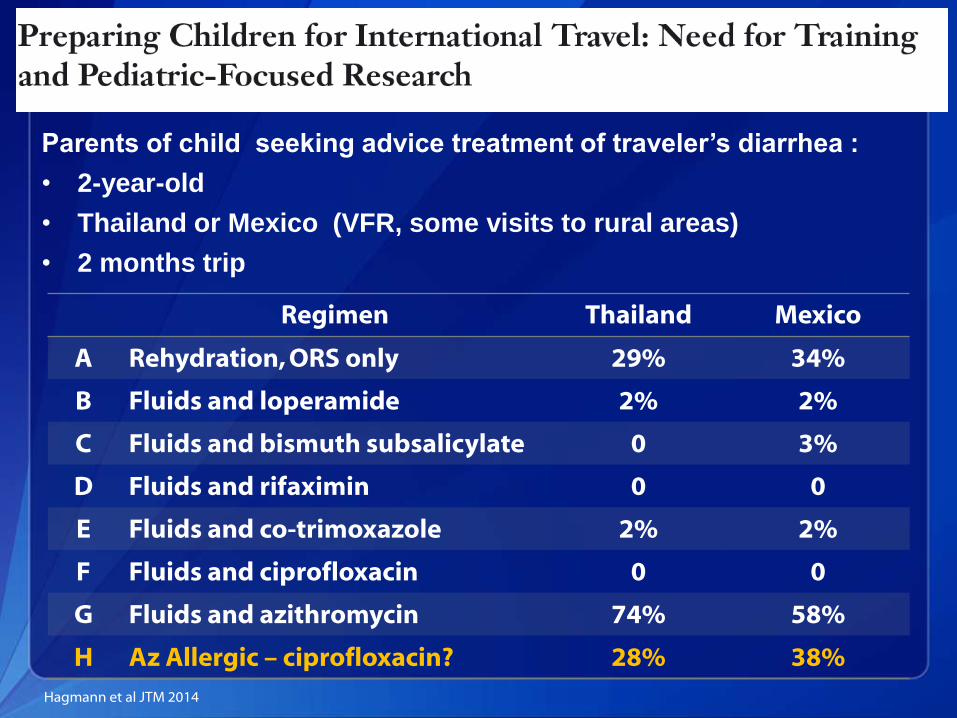
Regimen Thailand Mexico
A Rehydration, ORS only 29% 34%
B Fluids and loperamide 2% 2%
C Fluids and bismuth subsalicylate 0 3%
D Fluids and rifaximin 0 0
E Fluids and co-trimoxazole 2% 2%
F Fluids and ciprofloxacin 0 0
G Fluids and azithromycin 74% 58%
H Az Allergic – ciprofloxacin? 28% 38%
Hagmann et al JTM 2014
Parents of child seeking advice treatment of traveler’s diarrhea :
• 2-year-old
• Thailand or Mexico (VFR, some visits to rural areas)
• 2 months trip
Objectives
To present what we know about the epidemiology of diarrhea in child travelers
To discuss treatment options and the role of empiric antibiotic use

Traveler’s Diarrhea Definition
Adults ≥3 unformed stools / day
Children ≥2 fold increase in the frequency of unformed stools
NIH consensus report 1985

EPIDEMIOLOGY
What is the incidence of travelers diarrhea in children aged <2 years
A. 10%
B. 20%
C. 30%
D. 40%
What is the incidence of travelers diarrhea in children aged <2 years
A. 10%
B. 20%
C. 30%
D. 40%

Incidence of Traveler’s Diarrhea - Children
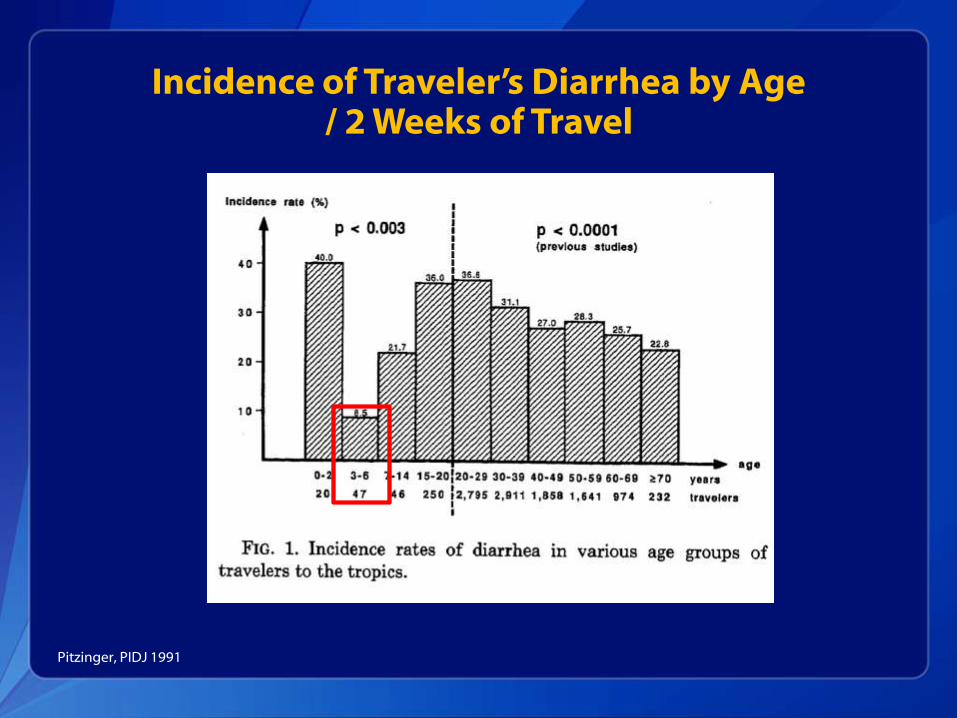
Pitzinger 1991
Zurich University Vaccination Center Retrospective survey
Pretravel visitors of vaccine center
Questionnaire 2 weeks after return
Age 0-20 years old
N=363 Travelers
Pitzinger, PIDJ 1991
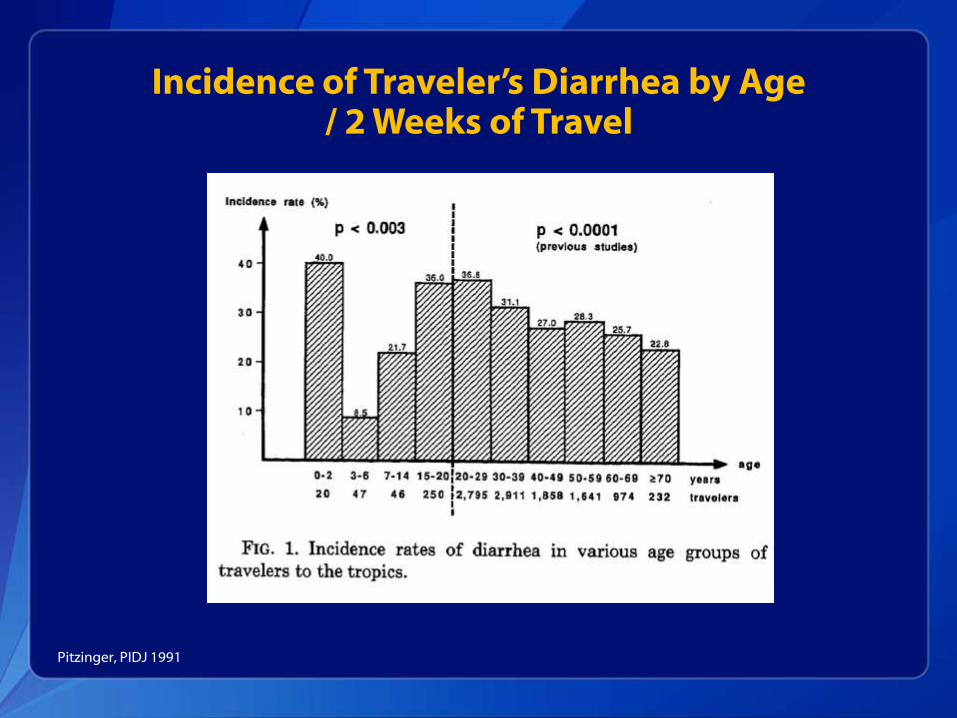
Incidence of Traveler’s Diarrhea by Age / 2 Weeks of Travel
Pitzinger, PIDJ 1991

Incidence of Traveler’s Diarrhea by Age / 2 Weeks of Travel
Pitzinger, PIDJ 1991
Incidence of Traveler’s Diarrhea by Age / 2 Weeks of Travel
Pitzinger, PIDJ 1991
Are children at higher risk than adults accompanying them?
A. Yes
B. No

Newman-Klee, AJTMH 2007
7 episodes / 100 person weeks

ETIOLOGY

Etiology of Traveler’s Diarrhea - Children
University of Bern, Switzerland Children aged 5 weeks – 15 years
Admitted due to acute diarrhea
History of stay in hot climate, poorly industrialized country during the last 10 days prior to disease onset
Essers, Clin Infect Dis 2000
Etiology of Traveler’s Diarrhea - Children
In children hospitalized due to diarrhea
Rotavirus most common cause of diarrhea (24%)
Bacterial causes Salmonella spp.
Campylobacter spp.
Aeromonas spp.
Essers, Clin Infect Dis 2000

Etiology of Traveler’s Diarrhea - Children
Travel history by etiology of diarrhea
Essers, Clin Infect Dis 2000
Recent travel to hot climate country
Shigella spp. and ETEC 60%
Other bacterial causes 16-29%
Rotavirus 4%

CLINICAL FEATURES AND SEVERITY

What is the median duration of travelers diarrhea in children aged<2 yeas
A. 1 day
B. 3 days
C. 5 days
D. >7 days

Duration of Traveler’s Diarrhea by Age Group
Age (years) Mean Duration (days)
Median Duration (days)
0-2 29 17
3-6 8 4
7-14 3 3
15-20 5 5
Total 11 3
Pitzinger, PIDJ 1991

Duration of Traveler’s Diarrhea by Age Group
Age (years) Mean Duration (days)
Median Duration (days)
0-2 29 17
3-6 8 4
7-14 3 3
15-20 5 5
Total 11 3
Pitzinger, PIDJ 1991
What proportion of children aged <10 years will need medical care for traveler’s diarrhea
A. 5%
B. 10%
C. 25%
D. >35%
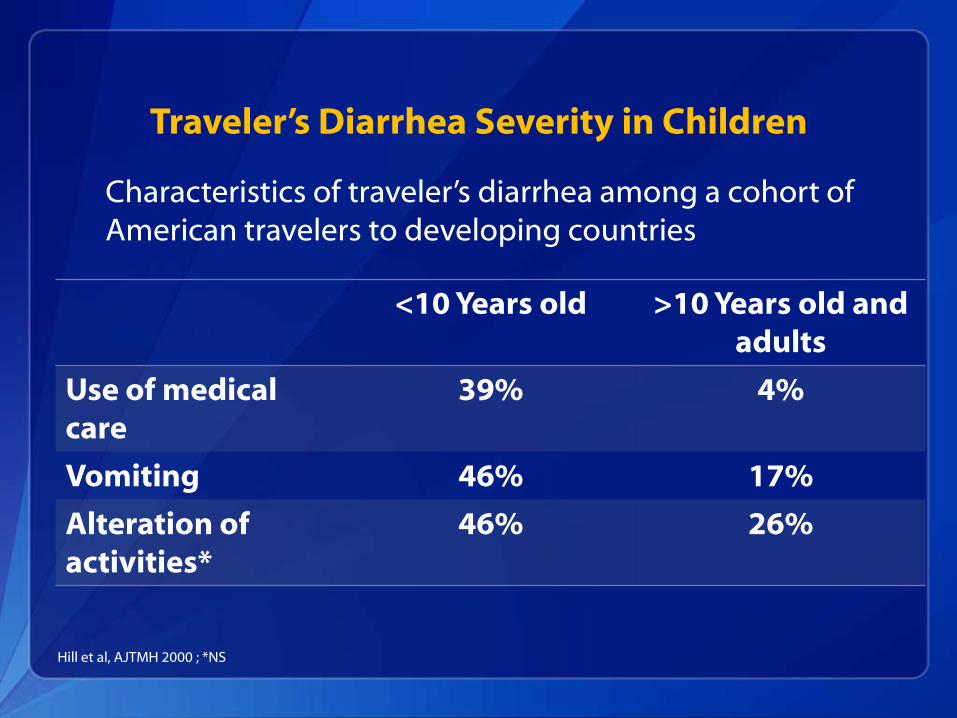
Traveler’s Diarrhea Severity in Children
Characteristics of traveler’s diarrhea among a cohort of American travelers to developing countries
Hill et al, AJTMH 2000 ; *NS
<10 Years old >10 Years old and adults
Use of medical care
39% 4%
Vomiting 46% 17%
Alteration of activities*
46% 26%
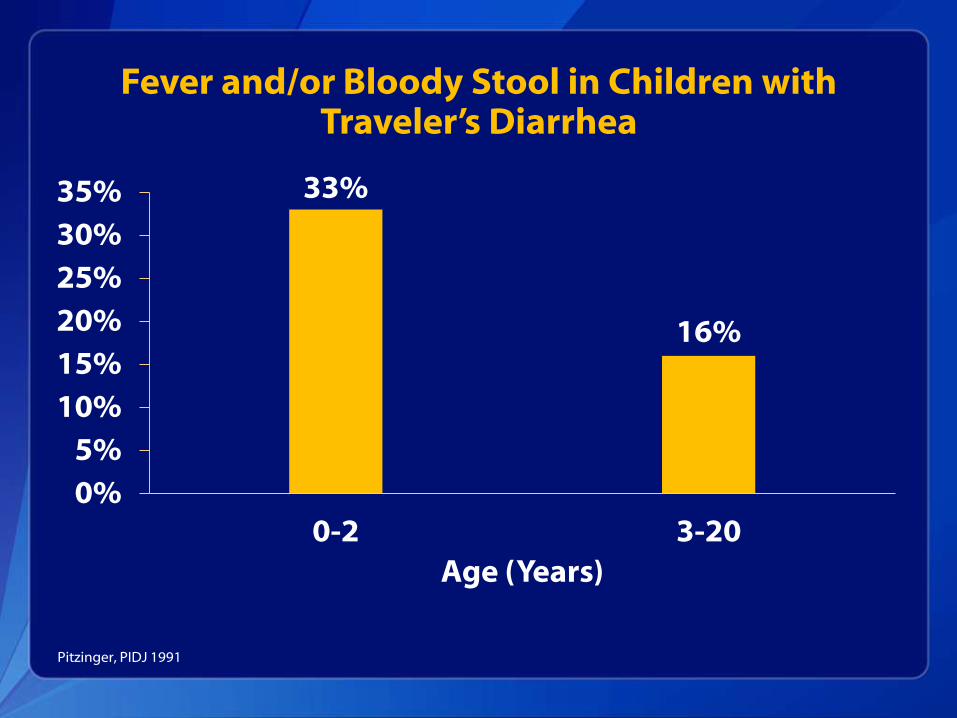
Fever and/or Bloody Stool in Children with Traveler’s Diarrhea
33%
16%
0%
5%
10%
15%
20%
25%
30%
35%
0-2 3-20
Age (Years)
Pitzinger, PIDJ 1991
Why is Acute Gastroenteritis a Severe Disease in Young Children?
Severe dehydration Hypovolemic shock
Replacement with fluids lacking electrolytes Normovolemic hyponatremia
Severe dysentery Intestinal perforation
Sepsis
Are There Severe Outcomes of Traveler’s Diarrhea in Children??
Literature review No reports of child deaths due to traveler’s diarrhea
Travel medicine professionals (Leshem, personal survey) Not aware of a single case

PREVENTION

Prevention of Travelers Diarrhea in Children
Breastfeeding in very young children Alternatively use of formula + safe
water
Adherence to food and water precautions:
Newman-Klee, AJTMH 2007 ,Steffen JAMA 2015
Prevention of Travelers Diarrhea in Children
Breastfeeding in very young children Alternatively use of formula + safe
water
Adherence to food and water precautions: 32% in children
17% in accompanying adults
Newman-Klee, AJTMH 2007 ,Steffen JAMA 2015

Prevention of Travelers Diarrhea in Children
Antibiotic chemoprophylaxis Rarely used
Consider use in high-risk
Immune compromised
IgA deficiency
Rotavirus vaccines
Steffen JAMA 2015

TREATMENT
Treatment of Child Traveler's Diarrhea
Prevention of dehydration Oral rehydration salts (ORS)
Initiated immediately with recognition of diarrhea by parents
Use a teaspoon / syringe
Give 5mL every 2-4 minutes Do not stop if child vomits
Continue breastfeeding / resume regular diet

Antibiotic Treatment of Child Diarrhea
ISTM Pediatric interest group survey ORS only 29-34%

Antibiotic Treatment of Child Diarrhea
ISTM Pediatric interest group survey ORS only 29-34%
Why are travel health professionals hesitant about prescribing empiric antibiotics for traveler’s diarrhea in children?
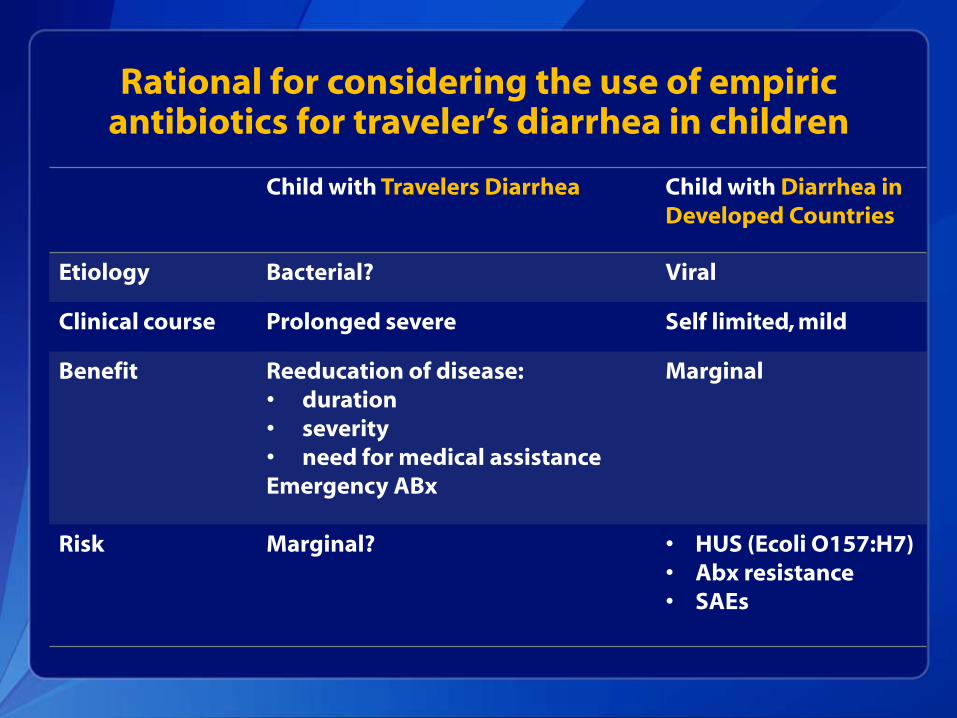
Rational for considering the use of empiric antibiotics for traveler’s diarrhea in children
Child with Travelers Diarrhea Child with Diarrhea in Developed Countries
Etiology Bacterial? Viral
Clinical course Prolonged severe Self limited, mild
Benefit Reeducation of disease: • duration • severity • need for medical assistance Emergency ABx
Marginal
Risk Marginal? • HUS (Ecoli O157:H7) • Abx resistance • SAEs
When Should Antibiotics be Started
Judgment call:
Any case of diarrhea Initiate ORS
Consider antibiotics
Consider use antibiotics Younger age
Remoteness / limited availability of healthcare
Signs of dehydration
Any signs of severe disease (fever, vomiting, dysentery)

Antibiotic Treatment of Child Traveler's Diarrhea
Azithromycin
Dose: 10mg/kg QD up to 3 days
Travel >2 weeks Unreconstituted powder – mix with water
Recommended for SE Asia (FQ resistance)

Regimen Thailand Mexico
A Rehydration, ORS only 29% 34%
B Fluids and loperamide 2% 2%
C Fluids and bismuth subsalicylate 0 3%
D Fluids and rifaximin 0 0
E Fluids and co-trimoxazole 2% 2%
F Fluids and ciprofloxacin 0 0
G Fluids and azithromycin 74% 58%
H Az Allergic – ciprofloxacin? 28% 38%
Hagmann et al JTM 2014
Parents of child seeking advice treatment of traveler’s diarrhea :
• 2-year-old
• Thailand or Mexico (VFR, some visits to rural areas)
• 2 months trip

Antibiotic Treatment of Child Traveler's Diarrhea
Ciprofloxacin
Dose: 20mg/kg/day divided BID for 3 days
Not approved by many countries for use in children “To date no child treated with FQs has developed physician drug
attributed bone or joint toxicity. This is based on experience with extensive use of ciprofloxacin and levofloxacin in children and adolescents.” (Red book 2012)
Not for SE Asia (FQ resistance)
Antibiotic Treatment of Child Traveler's Diarrhea
Second line antibiotics Furazolidone
Nalidixic acid
Cefixime
Rifaximin (non-invasive disease, pt. age>12 years)
No place for use of TMP / SMX Widespread resistance
Treatment of Child Traveler's Diarrhea
Bismuth subsalicylate Not recommended by AAP
Concerns regarding salicylate intoxication
Loperamide Not recommended by AAP
Concerns severe adverse events
Extrapyramidal adverse events
Conclusions

Conclusions
Thank You
For more information please contact Centers for Disease Control and Prevention
1600 Clifton Road NE, Atlanta, GA 30333
Telephone: 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348
E-mail: [email protected] Web: http://www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
National Center for Immunization & Respiratory Diseases
Division of Viral Diseases

Photo Title – Myriad Pro, Bold, Shadow, 20pt
Caption for photo, references, citations, or credits – Myriad Pro, 14pt

FUTURE RESEARCH

Antibiotic Treatment of Child Diarrhea
Use of antibiotic for treatment of children with diarrhea is discouraged Antibiotic resistance
Risk of hemolytic uremic syndrome (E. coli 0157:H7)
Allergic reactions
Adverse events

Evidence Based Child Traveler’s Diarrhea
Burden of child traveler’s diarrhea Risk for severe disease
Mortality?
Etiology
Prevention Targeting high risk populations (VFRs, travel to remote
destinations)
Treatment Effectiveness
Safety
ISTM Pediatric Interest Group Survey (PO23.01)

Incidence of Traveler’s Diarrhea - Children
Pitzinger 1991
Zurich University Vaccination Center Retrospective survey
Pretravel visitors of vaccine center
Questionnaire 2 weeks after return
Age 0-20 years old
N=363 Travelers
Pitzinger, PIDJ 1991
Incidence of Traveler’s Diarrhea - Children
Newman-Klee 2007 Pretravel clinic University hospital in Lausanne
Retrospective survey of traveling families
Post travel questionnaire of common travel related symptoms
Age 0-16 years
157 Child – adult pairs
Incidence of diarrhea was similar in adults and children 7 episodes / 100 person weeks
Newman-Klee, AJTMH 2007
SECTION HEADER MYRIAD PRO, BOLD, SHADOW, 34PT
Subhead for Section – Myriad Pro, 20pt

Basic Content Headline Myriad Pro, Bold, Shadow, 26pt
First Level Bullet – Myriad Pro, Bold, 24pt Second Level Bullet – Myriad Pro, 20pt
• Third Level Bullet – Myriad Pro, 18pt
o Fourth Level Bullet – Myriad Pro, 18pt
• Fifth Level Bullet – Myriad Pro, 18pt
* Citations, references, and credits – Myriad Pro, 11pt

Content With Caption Myriad Pro, Bold, Shadow, 20pt
First Level Bullet – Myriad Pro, Bold, 24pt Second Level Bullet – Myriad Pro, 20pt
• Third Level Bullet – Myriad Pro, 18pt
o Fourth Level Bullet – Myriad Pro, 18pt
• Fifth Level Bullet – Myriad Pro, 18pt
Paragraph of Type – Myriad Pro, 14pt
“Lorem ipsum dolor sit amet, consectetur adipiscing elit. Morbi commodo velit id libero venenatis vestibulum. In hac habitasse platea dictumst. Quisque sit amet sapien eget turpis rutrum suscipit sit amet a nulla. Duis tempus magna sed nunc auctor auctor. Ut est urna, viverra ut sodales ac, placerat nec purus. Nulla consectetur massa tellus. Curabitur nec nunc vitae neque lacinia congue. “
* Citations, references, and credits – Myriad Pro, 11pt

Closing – Myriad Pro, Bold, 28pt
For more information please contact Centers for Disease Control and Prevention
1600 Clifton Road NE, Atlanta, GA 30333
Telephone: 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348
E-mail: [email protected] Web: http://www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
National Center for Immunization & Respiratory Diseases

Epidemiology of Child Traveler’s Diarrhea
Diarrhea occurred on average on the 8th day
28% had a second episode Adventurous travel style

Antibiotic Treatment of Child Traveler's Diarrhea
Rational for use of empiric antibiotics for traveler’s diarrhea in children:
Etiology – predominantly bacterial
Clinical course – prolonged, severe
In adults, antibiotics reduce duration and severity of diarrhea

Etiology of Traveler’s Diarrhea - Adults
Adult travelers etiology identified 60-80% of cases
Mostly bacterial (50-80%)
Viruses
Parasites