dian: understanding ad in persons with causative genetic ... · dian clinical trials lthe 2007 rfa...
TRANSCRIPT

DIAN: Understanding AD in Persons with Causative Genetic
Mutations
John C. Morris, MDHarvey A. and Dorismae Hacker Friedman
Distinguished Professor of Neurology
24th Annual Southern California AD Research Conference

Disclosure Statement (2012-2013)l Sources of Research Support
1. National Institute on Aging (P50 AG05681; P01 AG03991; P01 AG026276; U19 AG032438)
2. Anonymous Foundation3. Alzheimer’s Association
l Consulting Relationships
1. Lilly USA
l Industry-Sponsored Trials
1. Janssen2. Pfizer3. Eli Lilly/Avid
Radiopharmaceuticals
� Fees > $10,000
None
� Stock Equity
None
� Speaker’s Bureaus
None
� Editorial Boards
Annals of Neurology

UCI MIND (Institute for Memory Impairments and Neurological Disorders)
l Founding Director, Carl W. Cotman, PhD, started the Institute in 1995; UCI Alzheimer’s Disease Research Center (ADRC) officially established in 2000 with Dr Cotman as Director
l Frank LaFerla, PhD, succeeded Dr Cotman as Director of the Institute and its ADRC in 2009
l Recognized for developing animal models of Alzheimer disease, exploring mechanisms (including exercise) to enhance successful aging, and establishing unique study populations (Down syndrome, the oldest old)
l Also notable because Dr LaFerla is known to prepare dinner for selected supporters!

Knight ADRC – Faculty and Staff (with gratitude to our participants and families!)
Knight ADRC – Faculty and Staff (with gratitude to our participants and families!)
David Holtzman, MD

Knight ADRC – Faculty and Staff (with gratitude to our participants and families!)
Randall Bateman, MD

My View of AD
l “Alzheimer disease” (AD) refers to the neurodegenerative brain disorder, regardless of clinical status, representing a continuous process of synaptic and neuronal deterioration
l AD has two major stages:– Preclinical (presymptomatic; asymptomatic), undetectable by current
clinical methods– Symptomatic (clinical)
l Symptomatic AD is defined by intraindividual cognitive decline, from subtle to severe, that interfers with daily function, and can be subclassified on symptom severity: – Incipient (prodromal; mild cognitive impairment)– Dementia
Morris JC, Arch Neurol 2012;69:700-708.

It is the best of times…l Most exciting research advances ever for AD
– Development of biomarkers for AD diagnosis and preclinical research
l Several promising therapeutic agents– Plans for secondary prevention trials
… it is the worst of timesl “Disease-modifying” drug trials all have failed
l Funding is critically needed, but in the US severe curtailment of NIH support for AD research

Failure of AD Candidate TherapeuticsAgent Target/Mechanism Outcome
Non-AβAtorvastatin; Simvastatin Cholesterol (HMG CoA reductase inhibitor) Negative
NSAIDs Inflammation Negative
Rosiglitazone Insulin (PPAR gamma agonist) Negative
Latrepirdine Mitochondrial function Negative
AβAN1792 Amyloid immunoRx Negative (AEs)
Tramiprosate Amyloid aggregation Negative
Tarenflurbil Gamma secretase Negative
Semagacestat; Avagacestat Gamma secretase Negative
Bapineuzumab Amyloid immunoRx Negative
Solanezumab Amyloid immunoRx Negative (+/-)
IVIG Nonselective immunoRx Negative
LY2886721 Beta secretase AEs
ACC-001 Amyloid immunoRx Negative

Preclinical and Symptomatic AD
Preclinical AD~20 y
No AD Symptomatic AD~7-10 y
Synaptic/Neuronal Integrity
↓ Hippocampal Volume
↑ CSF tau
+ Amyloid Imaging
↓ CSF Aβ42 TransitionPeriod
~5 y 0.5 à 1 à 2 à 3Cognitively Normal
↓ Cognition,↓ Metabolism,
and Other Potential
Indicators
Death
Tau
Microglia
Inflammation
Oxidative stress
Neuronal loss
CDR
Other

NIA-AA Diagnostic Guidelines for Dementia Due to AD (McKhann G et al, Alzheimer’s & Dementia 2011; 7: 263-269)
l Enhance diagnostic confidence for AD– Molecular biomarkers of AD
» Low levels of CSF Aβ42
» Elevated levels of CSF tau and phospho-tau» Amyloid imaging (PET tracers: 11C PIB, 18F Florbetapir, others)
– “Downstream” indicators of neurodegeneration» Reduced temporoparietal metabolism with FDG-PET» Whole brain and/or regional atrophy on MRI» (Disrupted connectivity on fMRI)
– Causative gene mutation (PSEN1, PSEN2, APP)» APOE4 insufficiently specific to be a diagnostic biomarker

Presymptomatic Detection of AD:Biomarkers (PIB Imaging)
Cognitively normal
Amyloid –
Cognitively normal
Amyloid +
Alzheimer dementia
Amyloid +
Courtesy of Mark A. Mintun and John C. Morris. Reprinted with permission. Copyright 2010 Washington University, St. Louis Missouri. All Rights Reserved
3 years later,Alzheimer dementia

0%
5%
10%
15%
20%
25%
30%
35%
50 55 60 65 70 75 80 85 90
Perc
ent w
ith A
myl
oid
Plaq
ues
Age
Percent of Cognitively Normal Participants with Amyloid Plaques
Courtesy of Mark Mintun, MD, and Andrei Vlasenko, PhD
Cross-sectional data Longitudinal data

Preclinical AD Stages and Symptomatic AD
Vos et al., Lancet Neurology 2013

Progression to CDR ≥0.5 DAT by Preclinical AD Stage
Vos et al., Lancet Neurology 2013

The Dawn of Clinical Amyloid Imaging Is Here
l Amyvid® (Florbetapir)– 18F tracer; FDA approved (2012) – commercially viable,
and may also replace 11C PIB in research
l Other 18F tracers in development, including by GE (Flutemetamol), Bayer (Florbetaben), and Navidea (NAV4694)
l Jan 2013: Medicare advisory panel voted to not cover costs of Amyvid®
– Insufficient evidence that it changes outcomes– July 2013: Original decision upheld; final decision
expected in October 2013
l Tau imaging– 18F-T807 and 18F-T808 recently acquired by Eli Lilly
from Siemens– Three 18F tracers in development by N Okamura
(Tohoku Univ, Sendai, Japan) in collaboration with V Villemagne (Univ Melbourne, Australia)
l Inflammation– PK11195, DPA-714, others
l Synuclein– Consortium to Develop an Alpha-Synuclein Imaging
Agent funded by the Michael J. Fox Foundation
Developing Molecular Imaging for Non-Amyloid Pathologies

Preclinical Alzheimer Diseasel ~30% of cognitively normal older adults have biomarker
evidence of preclinical AD
l Biomarker-positive CN persons are at increased risk of developing symptomatic AD compared with biomarker-negative CN older adults
l However, individual level prediction not currently possible– Is symptomatic AD inevitable?– If so, when will it develop?
l Asymptomatic AD mutation carriers are destined to develop symptomatic AD, and at about the same age as their affected parent

Introduction to Autosomal Dominant ADMeasure Autosomal
Dominant ADSporadic AD
Clinical presentation Amnestic Amnestic
Course
Gradual cognitive and functional decline, plus motor signs and seizures
Gradual cognitive and functional decline
MRI Hippocampal and whole brain atrophy
Hippocampal and whole brain atrophy
PIB PET Cortex plus basalganglia Cortex
FDG PET Parietal hypometabolism
Parietalhypometabolism
CSF Aβ 42 Decreased by 50% Decreased by 50%
CSF tau Increased by 2-fold Increased by 2-fold

Original DIAN Aims
l Determine WHEN the pathobiology of AD begins in asymptomatic mutation carriers in relation to parental age of onset of dementia
l Determine the SEQUENCE and RATE of the pathobiological changes
l Compare the clinical and pathological phenotypes of dominantly inherited AD with late onset AD
l Enroll and study longitudinally with a uniform protocol 400 persons (~200 MCs, ~200 NCs) from families with a known pathogenic mutation for AD

DIANCoordinating
CenterCore A: Administration
Morris
Core B: ClinicalBateman
Core D: Neuropath
Cairns
Core E: Biomarker
Fagan
Core C: Biostatistics
Xiong
Core F: GeneticsGoate
Core G: Imaging
Benzinger
Core H: Informatics
Marcus
External AdvisoryCommittee
Steering Committee(Core & Site Leaders,
FDA, Ethicist, Family Members, NIA, Other Key Personnel)
Clinical Coordinating
CenterAisenADCS
Wash.Univ
St. LouisBateman
UCLALos Angeles
Ringman
IndianaUniv
IndianapolisGhetti
ColumbiaUniv
New YorkMayeux
B&W; MGH
BostonSperling
Univ of MelbourneMelbourneMasters
Univ of New South Wales
SydneySchofield
NationalCell
RepositoryFor ADForoud
(NCRAD)
MRI Pre-Processing
MayoJack
(ADNI)
PET Pre-Processing
U MichKoeppe(ADNI)
Sub-Committees• Imaging Core Executive Committee• Resource Allocation Review
Univ of PittsburghPittsburghMcDade
Inst of Neurology
Univ CollegeLondonRossor
Edith Cowan UnivPerth
Martins
Butler Hosp Brown UnivProvidenceSalloway
Mayo-Jacksonville
Graff-Radford
University of Tübingen
JuckerDZNE
Ludwig-Maximilians-Universität
DanekDZNE
Dominantly Inherited Alzheimer Network (DIAN)*
*U19 AG032438 (JC Morris, PI)

Procedure Initial Visit
Follow-up Visit*
Study explanation XConsent XBlood for Genetic Analysis XBlood for Biochemical biomarkers X XInclusion and Exclusion Criteria XDemographics, Family History, Medical History, Physical Exam, Neurological Exam, UPDRS
X X
Clinical Evaluation – CDR, GDS, NPI, FAQ (Lifestyle),Hollingshead, Hachinski, Exercise questionnaire
X X
Psychometric Battery – MMSE, Logical Memory Test IA & IIA, Digit Span Test (forward and backward), Category Fluency Test, Trail Making Test (Parts A & B), Boston Naming Test, Letter Fluency, WAIS-R Digit Symbol, Word List Immediate and Delayed Recall, IPIP, Computerized Cognitive Battery
X X
MRI-3T X XFDG-PET X XPIB-PET X XLumbar Puncture for Cerebrospinal Fluid X X* Participants and collateral sources not seen annually have a yearly telephone interview
DIAN Assessments

DIAN Enrollment ReportOver Years 01-06, sites will recruit, enroll and follow these individuals to reach a sample size of 400 participants
Initial Visits Actual
Follow-up Visits
In-Person
Follow-up Visits
RemoteYear One (9/2008-6/2009) 11 0 0
Year Two (7/2009-6/2010) 76 0 5
Year Three (7/2010-6/2011) 103 26 39
Year Four (7/2011-6/2012) 79 57 92
Year Five (7/2012-6/15/2013) 67 75 103
YTD TOTALS 336 158 239

Participant Entry CharacteristicsAsymptomatic
244 (72.6%) Symptomatic
92 (27.4%)N = 336* (Target 80% Asymptomatic, 20% Symptomatic) (*Table based on 310 participants. 14 Mutations in Process- Missing)
MUT: 233 (72.4%) MUT: 89 (27.6%)
113 (NC-) 120 (MC+) 8 (NC-) 81 (MC+)
Age 39.1(SD 10.2)
35.2 (SD 9.1)
50.3(SD 12.4)
45.3(SD 9.7)
Gender (% Female) 58.2% 54.9% 75.0% 55.7%
Parental Age of Onset46.6
(SD 6.9)47.1
(SD 6.7)46.2
(SD 7.2)45.0
(SD 8.3)
Education14.7
(SD 2.6)14.6
(SD 2.8)12.5
(SD 3.4)13.5
(SD 2.6)
MMSE29.1
(SD 1.2)29.0
(SD 1.2)28.4
(SD 1.6)23.6
(SD 10.8)ApoE4+ 1 E4
2 E432 32 0 201 2 0 5
MC = Mutation Carrier; NC = Non-carrier*Table statistics based on 322 participants with NCRAD confirmed mutation data available as of 15 JUN 2013

Procedure Completion Rates(as of August 31, 2013)
Initial Visit Procedures Completed
TotalsN= 352
Psychometrics 347 (98%)Genetics Blood 352 (100%)MRI 330 (94%)PET PIB 314 (89%)FDG PET 318 (90%)Lumbar Puncture 291 (83%)Fasted Serum and Plasma 342 (97%)

DIAN Mutation Distribution
Gene Frequency
PSEN1 72.2%
PSEN2 8.7%
APP 19.1%
2:975-984.
Bateman et al., NEJM 2012
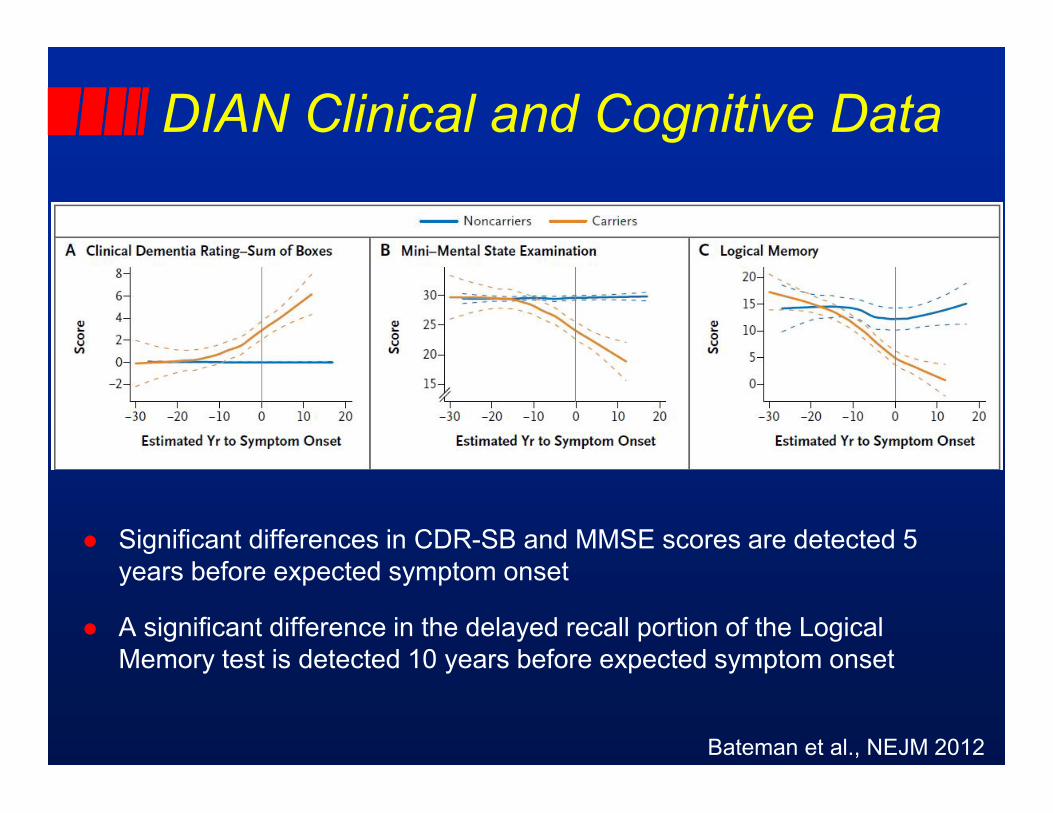
DIAN Clinical and Cognitive Data
l Significant differences in CDR-SB and MMSE scores are detected 5 years before expected symptom onset
l A significant difference in the delayed recall portion of the Logical Memory test is detected 10 years before expected symptom onset

Bateman et al., NEJM 2012
DIAN Imaging Data
l Significant differences in hippocampal volume and PET-PIB measures of precuneus Aβ deposition are detected 15 years before expected symptom onset
l A significant difference in FDG-PET measures of precuneus glucose metabolism is detected 10 years before expected symptom onset
Bateman et al., NEJM 2012
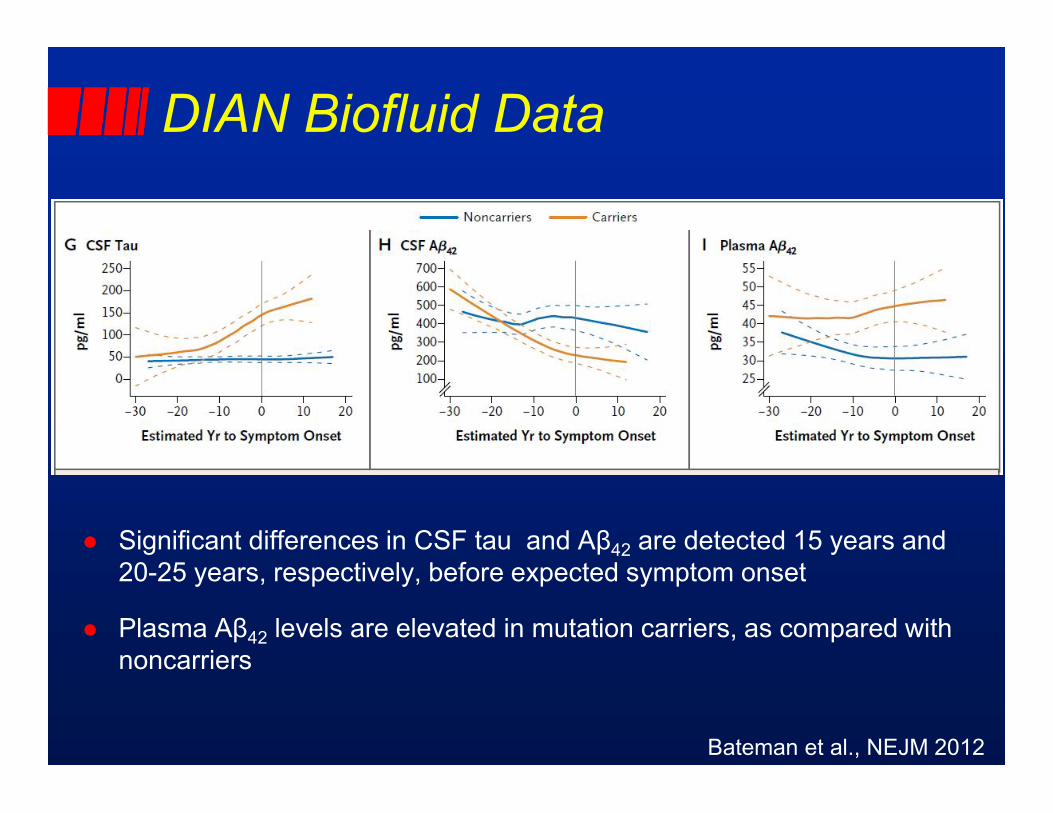
DIAN Biofluid Data
l Significant differences in CSF tau and Aβ42 are detected 15 years and 20-25 years, respectively, before expected symptom onset
l Plasma Aβ42 levels are elevated in mutation carriers, as compared with noncarriers

Alzheimer Biomarker Pathochronology in Autosomal Dominant AD
Morris et al., Clin Invest 2012; 2:975-984

DIAN Clinical Trials
l The 2007 RFA provided no funds for trials, but emphasized that the DIAN cohort “could serve as a population (for)… clinical trials funded by other mechanisms”
l The DIAN Clinical Trials Committee (CTC) formed in 2009 under the leadership of Randy Bateman– Members included DIAN investigators, a DIAN family member,
representatives from ADCS, NIA, and FDA
l In 2011, the DIAN CTC transitioned to the DIAN Trials Unit (TU), also led by Randy Bateman– Mission: design and manage interventional trials in DIAN
participants

DIAN Pharma ConsortiumDIAN-TU Director: Randy Bateman DIAN -TU Team: Virginia Buckles, Matt Carril, Dave Clifford, Angela Fuqua, Denise Levitch, JackiMallmann, Susan Mills, Angela Oliver, Anna Santacruz, Wendy Sigurdson, Christy Stewart, Joy Snider

DIAN Pharma Consortium
l Pharma companies collaborate with DIAN-TU and its academic institutions to advise on DIAN trials, nominate candidate drugs to be considered for DIAN trials, and support the DIAN-TU
l Currently, 10 companies comprise the PharmaConsortium (inaugural meeting July 2011)
l To date, 15 drugs have been nominated to DIAN-TU– DIAN-TU Therapy Evaluation Committee– Review criteria: safety data available (Phase II/III), engage
appropriate target, pipeline-ready

Randomization of MCs in DIAN Trials
DIAN Participants: 290Trial Eligible: 130
Additional Identified Potential Participants: 2,972
Randomization #1[to Arm A, B, or C; 1:1:1]
Total N = 240MC = 160NC = 80
Randomization #2[to drug or placebo; 3:1]
Drug BMC = 40
Drug CMC = 40
Drug AMC = 40
Pooled PlaceboMC = 40NC = 80
MC = 13NC = 27
Drug C ArmTotal N = 80
MC = 54NC = 26
Drug A ArmTotal N = 80
MC = 53NC = 27
Drug B ArmTotal N = 80
MC = 53NC = 27
MC = 14NC = 26
MC = 13NC = 27

DRUG TYPEBM
OUTCOME (TARGET)
BM OUTCOME (DOWNSTREAM)
Solanezumab(LILLY)
Anti-Aβantibody (soluble
Aβ)
CSF Aβ40, Aβ42
CSF tau, ptau181, PET
PIB, vMRI
Gantenerumab(ROCHE)
Anti-Aβantibody (fibrillar
Aβ)
PET PIBCSF Aβ40, Aβ42,
tau, ptau181, vMRI
LY2886721(LILLY)
BACE Inhibitor
CSF Aβ40, Aβ42
CSF tau, ptau181, PET
PIB, vMRI
• 2 yr treatment to BM outcome + 3 yr cognitive outcome for promising drug(s)• ADAD from DIAN and DIAN Expanded Registry, N=240 (mixed mutations)• N = 240 (160 MC, 3 drug arms + pooled placebo, 40 each; ~80 NC, placebo)• Age = -15 to +10 years compared to parental age of symptom onset
First Three Drugs in the DIAN Trial
On Hold

DIAN TU: “First Time Ever…”l Pharma companies collaborating to provide competing
investigational products in a single trial
l Two companies and WU agree on a single protocol, AND contracts completed between companies and WU in <1 year
l FDA approval for first ever anti-amyloid trial to prevent symptomatic AD with no protocol changes
l WU IRB approval on first submission (with no contingencies)
l Within 3 months from announcement of the trial drugs, the initial participant consented 12/31/12 and was randomized to treatment arm on 3/18/13 – first patient in!
l First ever trial in autosomal dominant AD has begun!!!– 9 participants now randomized– US/Canada Investigators Meeting held August 2013

DIAN Websitesl DIAN: www.dian-info.org
l DIAN Expanded Registry: www.DianXR.org(or 800-747-2979 toll free)

Knight ADRC – Faculty and Staff (with gratitude to our participants and families!)
Anne Fagan, PhD

Molecular Biomarkers Detect Symptomatic and Preclinical AD
l CSF signature of AD– Reduced Aβ42, elevated tau and p-tau
l Amyloid imaging – Pittsburgh Compound B (PIB), Amyvid (florbetapir)
l Strong inverse relationship between CSF Aβ42and PIB amyloid burden
l PIB amyloid burden increases as a function of the two known risk factors for AD: age and APOE4
Fagan et al., Ann Neurol 2006; Fagan et al., Arch Neurol 2007; Fagan et al., Ann Neurol 2009; Morris et al., Ann Neurol 2010