diagnosis of inborn errors of metabolism - univerzita …che1.lf1.cuni.cz/html/6 pbch diagnosis of...
TRANSCRIPT

Viktor Kožich
Ústav dědičných metabolických poruch1.LF UK a VFN Praha
Diagnosis of inbornerrors of metabolism
Structure
Diagnosis in generalNewborn screeningSelective screening
clinical approachlaboratory tests

Inborn errors of metabolism
product
substrateusually AR, GR
clinicallyvariable
usually enzyme

Diagnosis ≈ hypothesis verification
http://farm1.static.flickr.com/21/100467846_832c312de1_o.gif
patient

Linear causality
http://students.ou.edu/Y/Jacob.R.Yandell-1/karma.png

Nonlinear causality
http://www.biomedcentral.com/content/figures/1471-2105-10-122-4-l.jpg
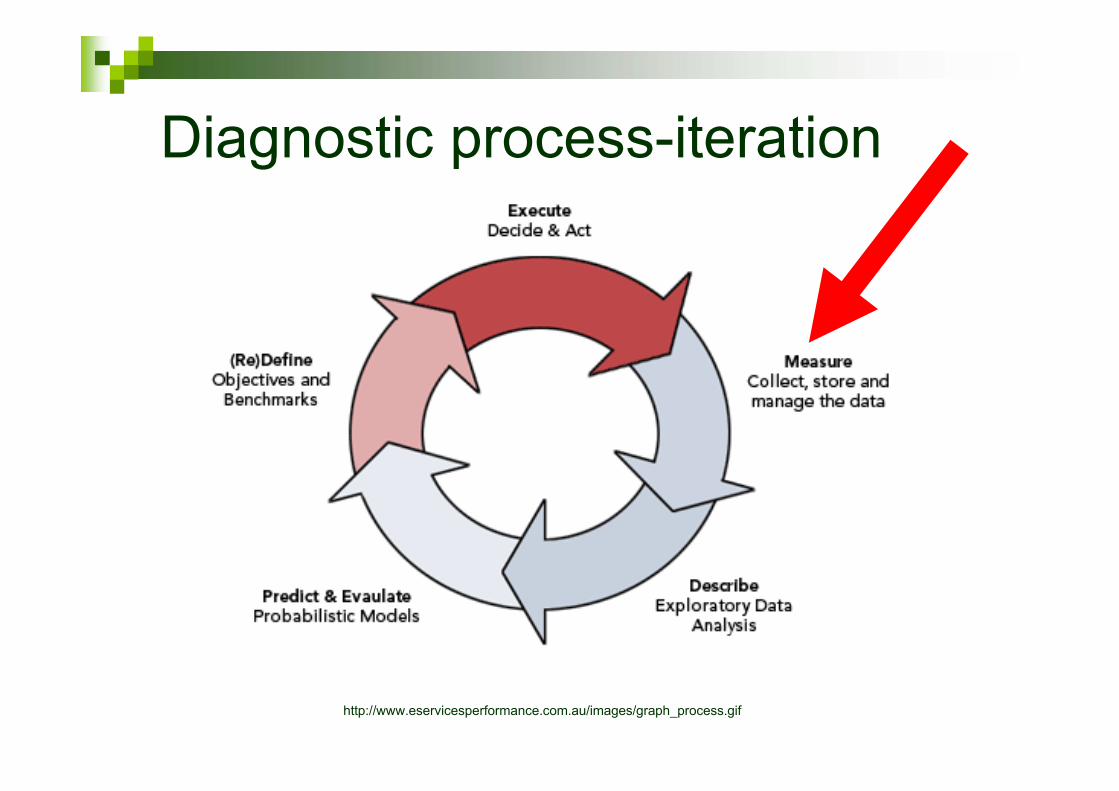
Diagnostic process-iteration
http://www.eservicesperformance.com.au/images/graph_process.gif
Successful diagnosis of IEM
+
3.bp.blogspot.com/.../s320/physicianatdesk.jpg
knowledgeable physician availability of appropriate test
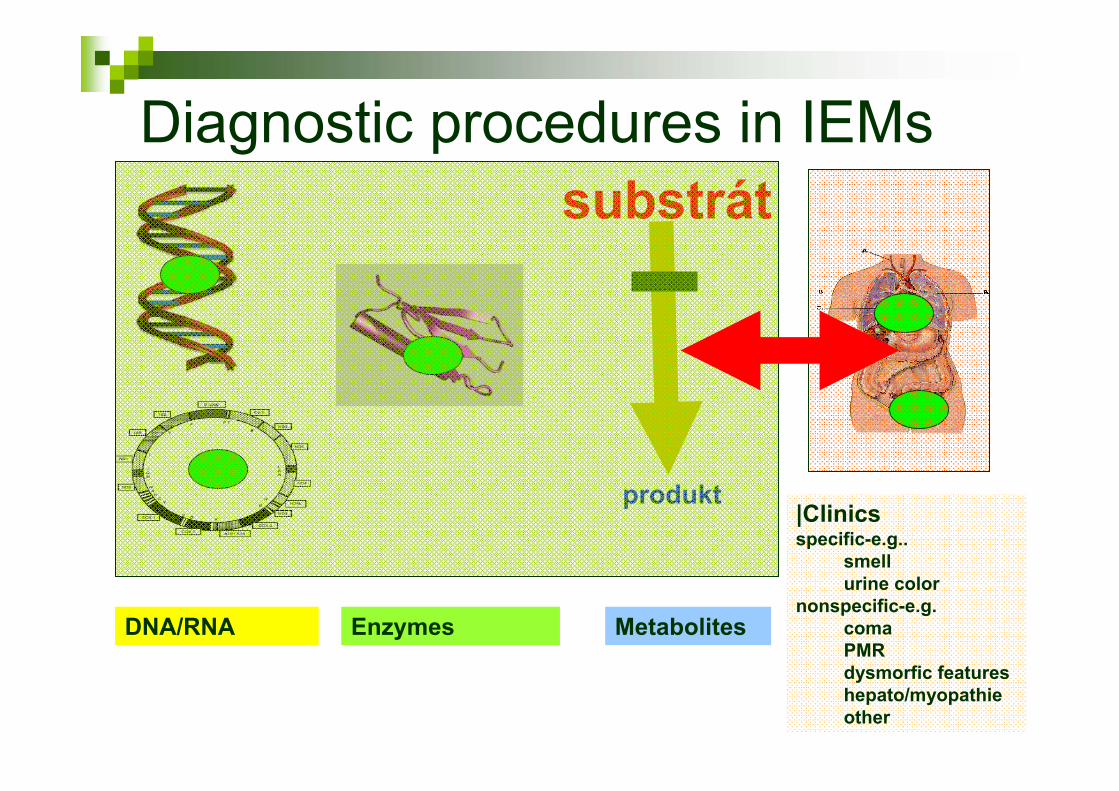
Diagnostic procedures in IEMs
produkt
substrát
DNA/RNA Enzymes Metabolites
|Clinicsspecific-e.g..
smellurine color
nonspecific-e.g.comaPMRdysmorfic featureshepato/myopathieother

Structure
Diagnosis in general
Newborn screeningSelective screening
clinical approachlaboratory tests

Presymptomatic diagnosis
produkt
substrát
at risk relatives
screening of population segment
newborn screening
single disease or groupof diseases

Newborn screening (NBS)
• active search for disease in the entire population
• presymptomatic diagnosis
• sensu stricto- laboratory analyses of diseases usingdry blood spots
NBS

Founder
Prof. Robert Guthrie 1916-1995
University of Buffalo, NY
PKU- bacterial inhibition test

JMG Wilson and G Jungner: Principles and Practice of Screening for Disease, WHO 1968

Classical criteria for NBS
Diseases freqeuncy and severityAsymptomatic latent phaseDisease mechanisms are knownReliable testTest is acceptable by the populationProgram is a continuous processAcceptable treatmetnConditions for dx and rx establishedConsensus on whom and how to treatCost-benefit ratio acceptable by the system

Quality Adjuste Life Yearsusual accepted limit 50.000 USD
QALY for MS-MS (30 IEMs): 6.000-15.000 USD, newborn screening of CF: 13.728 USD
QALY for other situationsdefibrilators in aircrafts/malls 50.000-70.000 USDprostatic ca screening 9.000-23.000 USDmammography 2.000-20.000 (but 232.000 USD under 50 y)MRI screening of breast ca in carriers of BRCA1/2 mutations: 45.000-700.000 USDACE inhibitors in hypertension 5.600 USD

http://www.bioethics.gov/images/new_born_screening.gif
81 diseases
29 diseases

3434
4444
4444 4545
50
5353
3535
51
50
3232
41414747
4646
3737
2929
2929
41414848
4040
DC
51 1331
4545
3535
33
36
2929
50
4141
4848
31
4545
33 4545
4848
52
31
31
3535
54 4949
3232
504949
2424
31
314646
49
51
52
32
5252
31
30
NBS USA-2009

NBS Europe-2009


Disorders screened in ČR 10/2009
~1:4 000
~1:2 900
~1:4 000
Total 1:1 200

Congenital hypothyroidism
1:4000etiology heterogeneous-peripheral diseaseTSH measurement (also T4) Aim: early substitution with thyroxinprevents irreversible CNS damage(+detection of associated congenitalanomalies)

Congenital Adrenal HyperplasiaDeficient activity of 21-hydroxylase- CYP21 gene mutationsAbnormala steroidogenesis in adrenal cortex –hypokortikalism, hypoaldosteronism andhyperandrogenismClassic (salt wasting or simple virilizing) and lateonset formsClassic form 1:10 000, LO up to 1:100. test: 17-hydroxyprogesteroneAim: early substitution prevents life-threateningcortical insufficency and premature puberty
IEMs of amino acids
accumulation of toxic products: chronic toxicity: e.g. Pheacute toxicity: BCKA, glutarate, isovalerate
clinical featureschronic toxicity: PMR, seizuresacute toxicity: encephalopathy with coma
therapy aim: decrease the load of affectedpathway + supplement other AA
Beta-oxidation defects
common mechanism: decreased production of ketone bodies upon fastingaccumulation of toxic acylCoAs
clinical features:common-hypoglycemia under fastingin some FAO defects-myopathy (especially after prolongedexercise), cardiomyopathy
treatment: prevention of hypoglycemia in catabolic situations, prevention of fasting

Cystic fibrosisAR inheritance1: 2500 – 4000 Mutations in CFTR gen
abnormal chloride channelabnormally thick mucus-bronchi, pancreas, male GU
Severe chronically debilitating disease leading to respiratory failureMedian survival in developed countries: 37yAim ot therapy: slowing down the progression by ATB treatment

Good sampling practice
http://cms.ich.ucl.ac.uk/website/imagebank/images/Neonatal_appendix.gif
correct drying3 hres, no direct heat

Why is correct sampling crucial?

Laboratory analysis of DBS
http://nl.ijs.si/et/talks/esslli02/metadata_files/Haystack-FINALb.jpg

Immunological metods
CH and CAH: hormonesCF: IRT

Tandem mass spectrometrymodern analytical methodprofile of analyteswide spectrum of compounds: amino acids, acylcarnitines, sugars......enzyme activitiesused for NBS since mid1990s

www.nature.com/.../v2/n2/fig_tab/nrd1011_F5.html

http://www.ch.cam.ac.uk/staff/pics/es1.jpg
Structuralinformation

http://cache.boston.com/resize/bonzai-fba/Globe_Photo/2008/01/22/1201060537_1951/300h.jpg
MS/MS- verygood identificationof analyteshigh sensitivityfast analysis of many metabolitesin a single assay

suchá krevní kapka
200 µl methanolu
se standardy
odstranění terčíku25 min extrakce
vyražení
3 mm terčíku
odpaření methanolu
butylace 30 min při 60 °Codpaření derivatizačního
činidla
analýza
1 vzorku 2,5 min
100µl
derivatizačního
činidla
NBS for IEMs by MS/MS
200 µl
1:1 acetonitril a voda + 0,02 % kys.
mravenčí

Optimal screening test
•http://www.connectseward.org/shs/da1/review07/Right%20Skewed.jpg
e.g. classical PKU and mild HPA
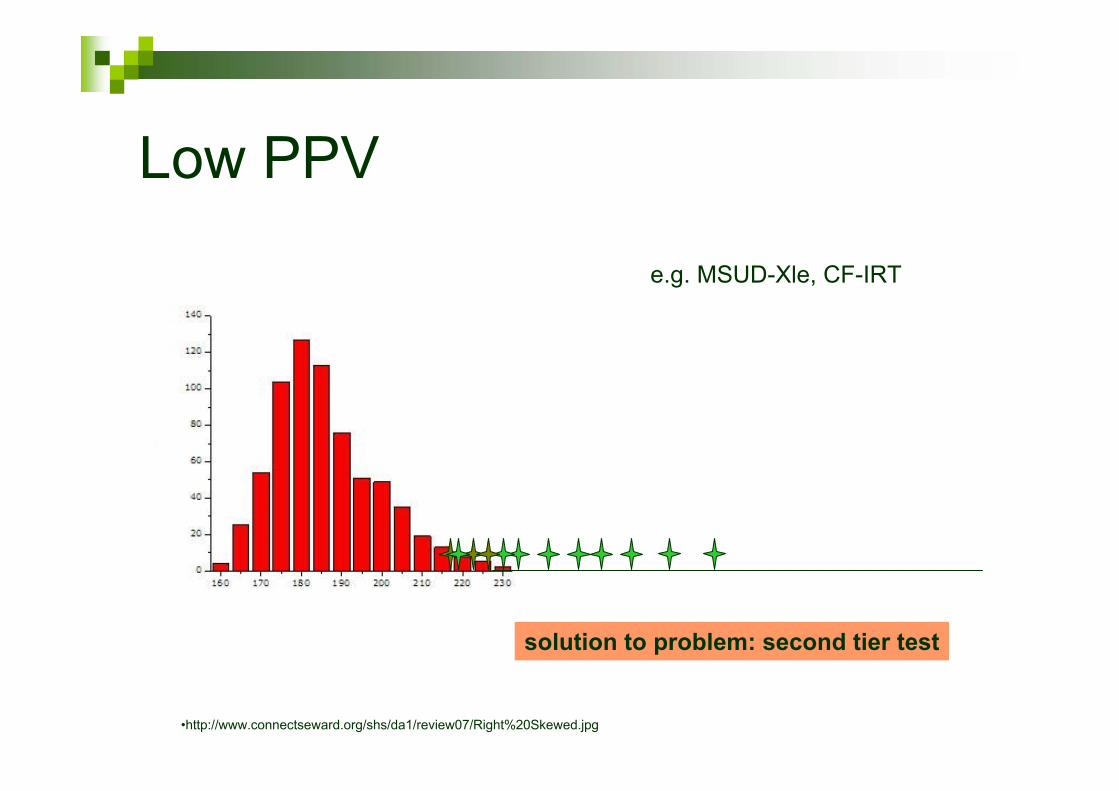
Low PPV
•http://www.connectseward.org/shs/da1/review07/Right%20Skewed.jpg
e.g. MSUD-Xle, CF-IRT
solution to problem: second tier test

Results from NBS programsNormal
cave!!!!- atypical form of screened disease is not excluded
Borderlineusually non-specificrecall needed-MS/MS on a new sample
Positivevarying PPV (5-100%)diagnostic workup initiated

Structure
Diagnosis in generalNewborn screening
Selective screeninglaboratory testsclinical approach

Diagnostic procedures in IEMs
produkt
substrát
DNA/RNA Enzymes Metabolites
|Clinicsspecific-e.g..
smellurine color
nonspecific-e.g.comaPMRdysmorfic featureshepato/myopathieother

IEM- metabolite analysis
produkt
Substrát

Metabolite analysis- IEMs
specialized testsusually not available in routinely labsmostly profile analysesmostly chromatographic techniques, expensiveequipment neededlaborious methods, lack of kits and controlmaterialcomplex interpretation (e.g. organic acids) by specialist

Small molecules in biochemicalgenetics
definition: < 1500 Dagases, inorganic ionsamino acidsorganic acidssaccharidespolyolssimple lipidspurines, pyrimidinesvitaminsoligomers: peptides up to 5-10 AA, oligosaccharides
cytosol, mitochondrial stromablood, urine

Complex molecules in biochemicalgenetics
definition: > 1500 Daglykolipidssphingolipidsplasmalogensneutral polysaccharides (glycogen)mucopolysaccharides(other polymers: proteins, nucleic acids...)
usually associated with membranesconcentrations in blood/urine rather low, exceptions exist ( x MS/MS technologie)
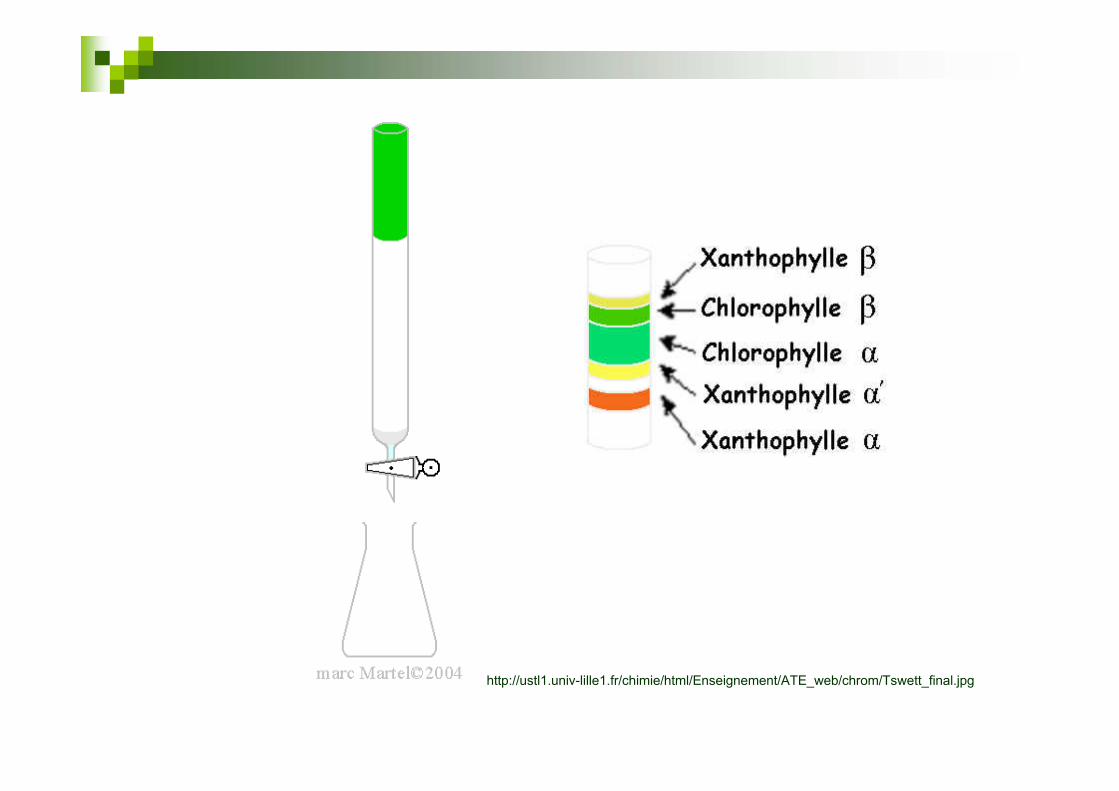
http://ustl1.univ-lille1.fr/chimie/html/Enseignement/ATE_web/chrom/Tswett_final.jpg

Sensitivity
Alkaptonuria: 1-5 g homogentisate /dCystinuria: 1-5 g cystine /d
PKU: 0.1 g Phe /l blood
MCAD: C8 acylcarnitin 0.0001 g / l bloodDBS punch 0.003 ml blood
0.2 – 1 ml serum
urine- liters

HPTLC- oligosaccharides in urine
courtesy Dr.Ledvinová

α L- iduronidase deficiency
(excretion of dermatan sulphate/DS and heparan sulphate/HS )
courtesy Dr.Ledvinová

AA- citrullinemia
patient
control

GC-MS: methylmalonic aciduria
0,0 2,5 5,0 7,5 10,0 12,5 15,0 17,5 20,0Time [min.]
25
50
75
100
125
150
175
200Vo
ltage
[mV]
3,26
5,54
5,86
6,61
6,64
7,21 7,
77
10,3
610
,63
11,5
112
,08
12,2
8
13,7
213
,80
14,0
0
14,7
014
,81
18,3
90,0 2,5 5,0 7,5 10,0 12,5 15,0 17,5 20,0
Time [min.]
50
100
150
200
250
300
350
Vol
tage
[mV
]
3,57
4,24
5,07
5,93
6,63
10,6
4
12,0
812
,29
13,4
713
,72
13,8
1
14,7
014
,80
14,9
6
17,8
0
18,4
0

GC-MS: methylmalonic aciduria
http://biochemgenetics.stanford.edu/images/Fig%204%20(MMA).jpg
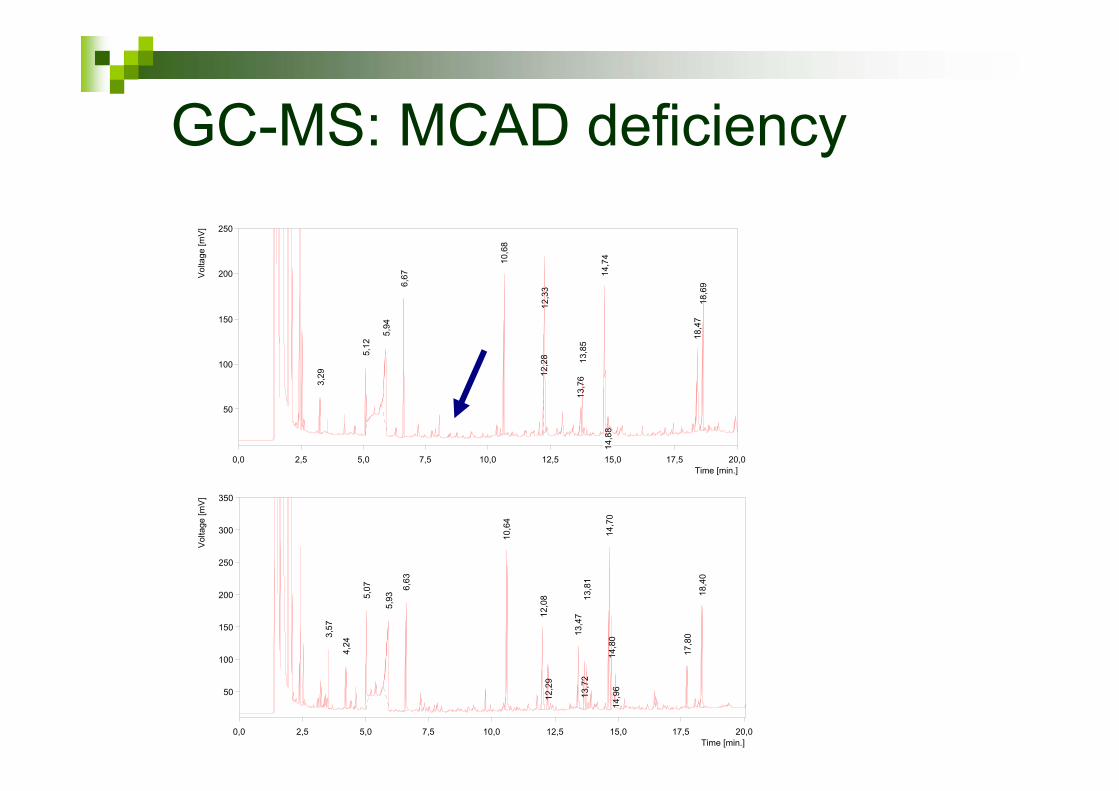
GC-MS: MCAD deficiency
0,0 2,5 5,0 7,5 10,0 12,5 15,0 17,5 20,0Time [min.]
50
100
150
200
250
Vol
tage
[mV
]
3,29
5,12
5,94
6,67
10,6
8
12,2
812
,33
13,7
613
,85
14,7
414
,88
18,4
718
,69
0,0 2,5 5,0 7,5 10,0 12,5 15,0 17,5 20,0Time [min.]
50
100
150
200
250
300
350
Vol
tage
[mV
]
3,57
4,24
5,07
5,93
6,63
10,6
4
12,0
812
,29
13,4
713
,72
13,8
1
14,7
014
,80
14,9
6
17,8
0
18,4
0

before treatment
after treatment
In vivo metabolite measurement
brain creatine deficiency

Metabolite analysis- IEMs
usually not available in routinely labsmostly profile analyses by chromatographic techniquecomplex interpretation (e.g. organic acids)

Diagnosis of IEM
produkt
Substrát
enzym

Principles of enzyme assays
substrate* product*
cofactor altered cofactor
•separation of substrate from product•quentitation of change
•quentitation of change

Enzyme assays in IEM diagnosisCells are usually needed
leukocytes, fibroblastschorion, amniocytes
Fluorimetry and radiometry (photometry)Measured variable:
substrate/product concentration changecofactor concentration change
ÚDMP: 46 enzyme assays
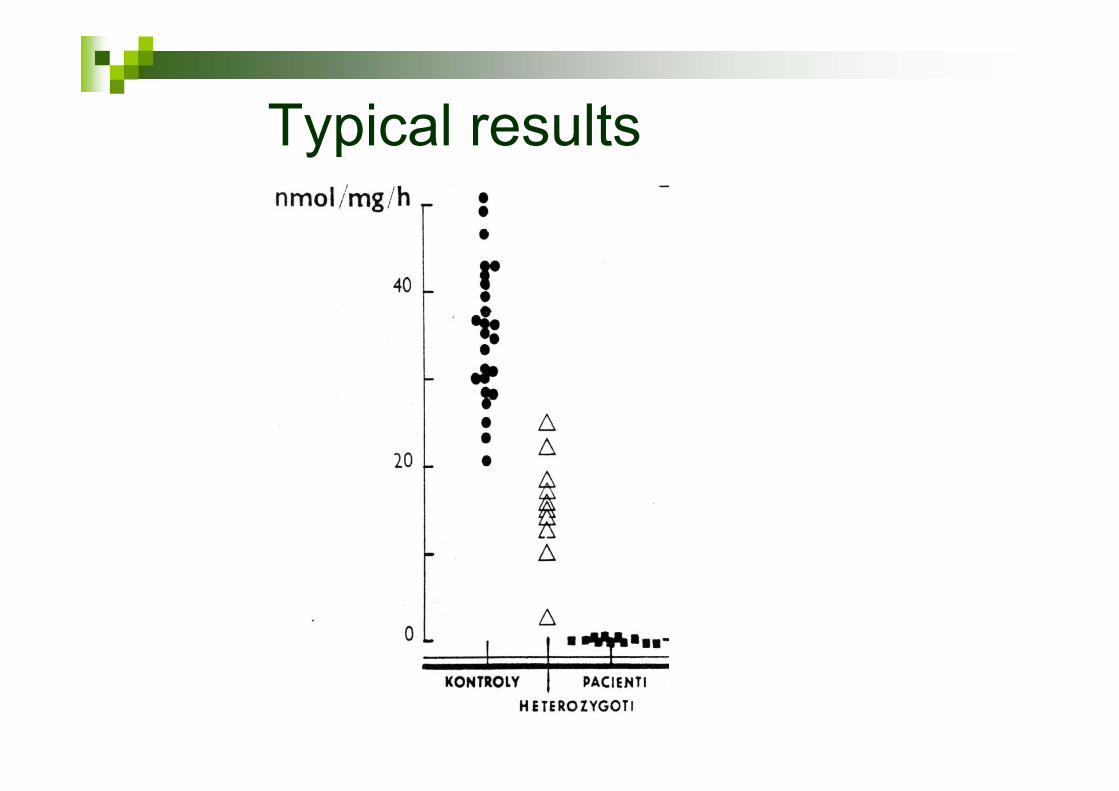
Typical results

Diagnosis of IEM
produkt
SubstrátDNA

http://www.biostudio.com/images/anim_freeman_dna_sequencing.gif
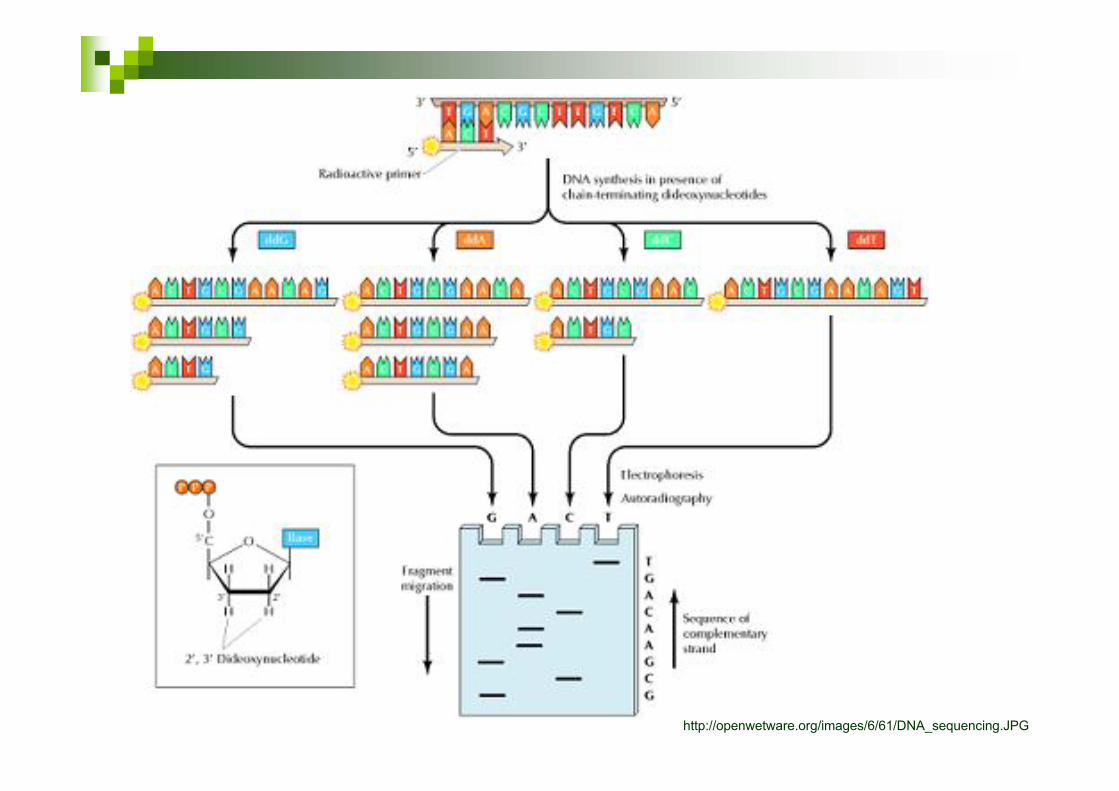
http://openwetware.org/images/6/61/DNA_sequencing.JPG

http://www.mun.ca/biology/scarr/fluorescent_dideoxy_sequencing.jpg

TCGGACCTCGGT/CGAAAAAGA
OTC: Mutation c. 829 C>T (R277W)

A GC T T CCAG G G CAC T T C T A T T T G T T T T T G T G G AA A G A CT G G CBases5 10 15 20 25 30 35 40
A GC TT CC AG G G C AC T T CT WT C T R T T T KT KT t GTG AWR G AC WG R C
Bases10 15 20 25 30 35 40 45 50
Heterozygous deletion
Wild type sequence

http://www.nature.com/nbt/journal/v26/n10/images/nbt1486-F1.gif
Structure
Diagnosis in generalNewborn screening
Selective screeninglaboratory tests
clinical approach

Patophysiology IEM
product
vedl.produkt
substrate<1500 Da
>1500 Da
1 32

Clinical features of IEMs-age
http://markandrich.googlepages.com/Old-woman.jpg/Old-woman-full.jpg
http://www.hrr.co.uk/acatalog/crocodile_toddler.jpghttp://www.co.shasta.ca.us/html/DSS/images/FosterParentingAdopt/infant.jpg

Clinical features-multisystemicinvolvement
http://www.istockphoto.com/file_thumbview_approve/5982111/2/istockphoto_5982111-human-internal-organs.jpg

Clinical features of IEMs-organs
http://universe-review.ca/I10-82-organs.jpg

endogenousexogenousOrigin
N YAcute toxicity
inefficiousefficiousRx-diet, vitamins
tissues (U)blood,urineDx
YNImpact on structure
membranescytosol, ECTLocalization
Y±Chronic progression
> 1500 Da< 1500 Da

Isovaleric aciduria
FTT, vomiting, Kussmaulbreathingconsciousness: comawithin 24-48 h after onsetof symptomsmetabolic acidosis, ketonuriasweaty feet syndrome
http://images.google.com/imgres?imgurl=http://upload.wikimedia.org/wikipedia/commons/8/8b/Isovaleric_acid_structure.png

Diseases of small molecules
usually dependent on exogenous supplymanifestation: (repeated) acute toxicity, usuallywith encephalopathy/comahepatopathy commoncommon disturbances in routine labs-ammonia, Astrup, ketone bodies, glycemia, uric acid...symptoms develop due to specific type of food, fasting, catabolismchronic course possible (if toxicity low)usually good therapeutic response to diet and/orvitamins

Food and IEMs (small molecules)
(sub)acute toxicitymilk (lactose)-hepatopathysaccharose/fructose/sorbitol- hepatopathyand hypoglycemiaexcess protein- vomiting, lethargy, coma(urea cycle disorders, organic acidurias)

Fasting and IEMs
hypoglycemia in GSDhypoglycemia with decreased production of ketone bodies (beta-oxidation defects)acidosis, ketonuria and metabolicencephalopathy in prolonged fasting (organicacidurias)respiratory alkalosis and encephalopathy (urea cycle disorders)

Organic acidurias
several dozens of diseasescommon feature: excretion of carboxylic acids(test-organic acids in urine) orginin usually from carbon skeleton degradationof AAs (or saccharides or lipids)usually acute presentation- „intoxication type“metabolic acidosis common (combination withhyperammonemia frequent)

Mukopolysaccharidosis type I
http://deti.msk.ru/plaxin_egor.jpg
http://myweb.lsbu.ac.uk/dirt/museum/margaret/438-1811-2640151.jpg
http://eyepathologist.com/images/KL1771.jpg

Diseases of complex moleculesdisease progresses usually regardless of anyexogenous sources from foodtypical course is progressive (± symptom-freeperiod)dysmorphy at birth possiblefrequent involvement of nervous system andmusculatureorganomegaly due to storage in lysosomalstorage disordersusually untreatable by diet or vitamins

Clinical features: (non)specific signs
http://img.medscape.com/pi/emed/ckb/pediatrics_genetics/941088-943343-507.jpg
http://gatsome.com/images/iq.gifhttp://www.saratogaschools.org/AcademicServices/MiddleSchool
specific non-specific
e.g. NH3, uric acid
Abnormal urinary smell and colorsmell (small volatile molecules):
sweaty feet-isovaleratemaple syrup-branched ketoacidsboiled cabbage-methionine oxidfish-trimethylamineblackcurrant- organic acidsmouse-phenylacetate
colororange-urateblack upon oxidation-homogentisateblue-indoxyl derivatiesgreen-4-OH-butyrate

Common labs in IEMs
BloodglycemiacholesterolTGuric acidMAchyperammonemia, RAlkALT,ASTCKanemia/pancytopenia
Urineketone bodiesuric acidcrystaluriamyoglobinuria

Selected common situations withhigh risk of IEM
Small moleculesacutelly ill newborn(repeated) atack of long-term uncosciousnessfailure to thrive
Complex moleculesprogressive CNS and musculature involvementfacial dysmorphyorganomegaly (liver, spleen, heart)

Successful diagnosis of IEM
+
3.bp.blogspot.com/.../s320/physicianatdesk.jpg
knowledgeable physician availability of appropriate test