diagnosis and treatment of multiligament knee injury...
TRANSCRIPT

State of the Art
To cite: Moatshe G, Chahla J, LaPrade RF, et al. J ISAKOS Published Online First: [please include Day Month Year]. doi:10.1136/jisakos-2016-000072
1Oslo University Hospital and University of Oslo, Oslo, Norway2Steadman Philippon Research Institute, Vail, Colorado, USA3OSTRC, The Norwegian School of Sports Sciences, Oslo, Norway4Hospital Britanico de Buenos Aires, Buenos Aires, Argentina5The Steadman Clinic, Vail, Colorado, USA
Correspondence toDr Robert F LaPrade, The Steadman Philippon Research 13 Institute, 181 West Meadow Drive, Suite 1000, Vail, CO 81657, USA; drlaprade@ sprivail. org
Received 9 November 2016Revised 8 January 2017Accepted 15 January 2017
Diagnosis and treatment of multiligament knee injury: state of the artGilbert Moatshe,1,2,3 Jorge Chahla,2,4 Robert F LaPrade,2,5 Lars Engebretsen1,3
AbSTrACTMultiligament knee injuries constitute a complex and challenging entity, not only because of the diagnosis and reconstruction procedure itself, but also because of the rehabilitation programme after the index procedure. A high level of suspicion and a comprehensive clinical and radiographic examination are required to identify all injured structures. Concomitant meniscal, chondral and nerve injuries are common in multiligament injuries necessitating a detailed evaluation. Stress radiographs are valuable in evaluating patients preoperatively and postoperatively. The current literature supports surgical management of multiligament injuries, and reconstructions are recommended because repair of ligaments has higher failure rates. Reconstruction of all injured ligaments in one stage is advocated (if possible) in order to achieve early mobilisation and to avoid joint stiffness. Using biomechanically and clinically validated anatomic ligament reconstructions improves outcomes. In the setting of multiligament knee reconstructions, several technical aspects that require consideration are vital, such as the graft choice, the sequence of ligaments reconstruction, tunnel position and orientation to avoid tunnel interference and graft tensioning order. This review article discusses the use of stress radiographs in diagnosing ligament injuries and evaluating postoperative stability. Tunnel convergence and tensioning sequence are potential problems, and guidelines to address these are also discussed. Recovery after a multiligament reconstruction surgery typically requires 9 to 12 months of rehabilitation prior to returning to full activities. The purpose of this article is to review the specific principles of multiligament injuries, classification, diagnosis, treatment options and rehabilitation guidelines for addressing these complex injuries.
InTroduCTIonThe definition of a multiligament knee injury is commonly recognised as a tear of at least two of the four major knee ligament structures: the anterior cruciate ligament (ACL), the posterior cruciate liga-ment (PCL), the posteromedial corner (PMC) and the posterolateral corner (PLC).1 2 The terms knee dislocation and multiligament knee injuries are often used interchangeably. Knee dislocations often result in multiligament knee injuries, but some multiliga-ment knee injuries are not knee dislocations. A knee dislocation is typically characterised by rupture of both cruciate ligaments, with or without an asso-ciated grade III medial or lateral-sided injury.2 3 However, knee dislocations with one of the cruciate ligaments intact have been reported.4 5 Multiliga-ment injuries are heterogeneous, and a thorough
diagnostic workup and treatment plan is mandatory when dealing with these injuries. The purpose of this article is to review specific focused principles of multiligament knee injuries, classification, diag-nosis, treatment options and rehabilitation guide-lines for addressing these complex injuries. Key information and articles on these injuries can be found in box 1 and box 2 respectively.
ClassificationSchenck described the most widely used classifica-tion system for the dislocated knee in 1994, which is based on the anatomical patterns of the torn liga-ments (table 1).3 6 The advantage of this classifica-tion is that it allows for identification of the torn ligaments and planning of treatment. In addition, it makes it possible to compare the different studies in the literature using the same classification system of knee dislocations.
AetiologyMultiligament knee injuries can be caused by both high-energy trauma,7 such as motor vehicle accidents and fall from heights, and low-energy trauma,8 including sporting activities. In a cohort of 85 patients with knee dislocations, Engebretsen et al reported that 51% were high-energy injuries, and 47% were sports-related injuries.9 In a review of 303 patients with knee dislocations, Moatshe et al10 reported equivalent rates of high- and low-energy trauma, with 50.3% and 49.7%, respectively. Miller et al reported on multiligament knee injuries in obese individuals as a result of ultra-low velocity trauma.11
EvaluationMultiligament knee injuries are not uncommon. Only 28% of PLC injuries occur in isolation.12 The clinician should have a high level of suspi-cion, and a detailed knee examination should be performed including assessment of the limb’s neurovascular status. PLC injuries are associated with both common peroneal nerve injuries and vascular injuries (Moatshe et al,10). When both cruciate ligaments are torn, the risk of vascular and neurological injuries is very high and vascular assessment is often needed.2 Magnetic resonance imaging (MRI) is performed to evaluate all the injured structures (figure 1). For both acute and chronic injuries, stress radiographs are essential, but can be difficult to carry out in the acute phase (tables 2 and 3, figures 2 and 3).13–15
Acute multiligament knee injuriesFor high-energy injuries, Advanced Trauma Life Support principles apply. Foot pulses and skin
State of the Art
1Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072. Copyright © 2017 ISAKOS
Journal of ISAKOS: Joint Disorders & Orthopaedic Sports Medicine Publish Ahead of Print, published on March 8, 2017 as doi:10.1136/jisakos-2016-000072
Copyright 2017 by International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine.
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
colour should be monitored and compared with the uninjured side. An ankle–brachial index (ABI) <0.9 warrants an angi-ography (figure 4).16 17 Knee dislocations are associated with injuries to the popliteal artery (23%–32%).7 18 Injury to the common peroneal nerve occurs in 14%–40% of knee dislo-cations.19 20 Ultra-low velocity knee dislocations in the obese patients are associated both with nerve and vascular injuries, and also with higher complication rates after surgical treat-ment.11 21
ABI is useful as an adjunct to physical examination to assess for vascular injuries. Physical examination with the presence of a normal vascular examination (normal and symmetrical pulses, capillary refill, normal neurological examination) is reported to be reliable to screen patients with knee dislocations for ‘selec-tive’ arteriography.22 Some protocols recommend an ABI cut-off of <0.8,23 and others recommend <0.9 to perform arteriog-raphy.22 24 Stannard et al developed a protocol for monitoring vascular injuries in knee dislocations.25 Patients with vascular injuries are treated with acute revascularisation, and the knee is protected in an external fixator to protect the revascularisation graft and to maintain knee reduction.23 26 The external fixator is usually removed at 2–6 weeks and the knee is placed in a hinged brace to avoid pin infections and joint stiffness.
Chronic multiligament knee injuriesSome multiligament knee injuries are missed in the acute phase, or concurrent ligament injuries are not acknowledged, in a multi-trauma patient. A thorough patient history, clinical examination supplemented with stress radiography and MRI are mandatory to identify all injured structures. Concomitant cartilage and meniscal injuries should be diagnosed and treated concurrently. In addition, long axis radiographs of the lower extremity should be obtained to assess alignment, especially for chronic multi-ligament knee injuries. Varus malalignment is defined as being
box 1 Key information
► Multiligament injuries are complex and challenging. ► Detailed evaluation with physical examination, MRI, stress
radiographs and angiography if ankle–brachial index <0.9 ► Concomitant injuries including meniscal, chondral, nerve and
vascular injuries are common. ► Surgical treatment of all injured structures in the same
setting is recommended. ► A well-crafted rehabilitation protocol is important to ensure
good functional outcomes. ► Good functional outcomes can be achieved with surgical
treatment.
box 2 Key articles
Levy BA, Dajani KA, Whelan DB, et al. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthros-copy. 2009;25:430–438.Levy BA, Fanelli GC, Whelan DB, et al. Controversies in the treatment of knee dislocations and multiligament reconstruction. J Am Acad Orthop Surg. 2009;17:197–206.James EW, Williams BT, LaPrade RF. Stress radiography for the diagnosis of knee ligament injuries: a systematic review. Clin Orthop Relat Res. 2014;472:2644–2657.Richter M, Bosch U, Wippermann B, Hofmann A, Krettek C. Comparison of surgical repair or reconstruction of the cruciate ligaments versus nonsurgical treatment in patients with traumatic knee dislocations. Am J Sports Med. 2002;30:718–727.Medina O, Arom GA, Yeranosian MG, Petrigliano FA, McAllister DR. Vascular and nerve injury after knee dislocation: a systematic review. Clin Orthop Relat Res. 2014;472:2621–2629.Schenck R. Classification of knee dislocations. Operative Techniques in Sports Medicine. 2003;11:193–198.Peskun CJ, Whelan DB. Outcomes of operative and nonoperative treatment of multiligament knee injuries: an evidence-based review. Sports Med Arthrosc. 2011;19:167–173.Engebretsen L, Risberg MA, Robertson B, Ludvigsen TC, Johansen S. Outcome after knee dislocations: a 2–9 years follow-up of 85 consecu-tive patients. Knee Surg Sports Traumatol Arthrosc. 2009;17:1013–1026.Dedmond BT, Almekinders LC. Operative versus nonoperative treatment of knee dislocations: a meta-analysis. Am J Knee Surg. 2001;14:33–38.Spiridonov SI, Slinkard NJ, LaPrade RF. Isolated and combined grade-III posterior cruciate ligament tears treated with double-bundle recon-struction with use of endoscopically placed femoral tunnels and grafts: operative technique and clinical outcomes. J Bone Joint Surg Am. 2011;93:1773–1780.
Figure 1 MRI showing a PCL tear on the sagittal plane (A) and a sMCL injury seen in the coronal plane (B). A detailed evaluation of the patient; and the images are mandatory to diagnose all the injured structures. PCL, posterior cruciate ligament; sMCL, superficial medial collateral ligament.
2 Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
Table 1 Explaining Schenck’s knee dislocation classification
Kd I Injury to single cruciate + collaterals
KD II Injury to ACL and PCL with intact collaterals
KD III M Injury to ACL, PCL, MCL
KD III L Injury to ACL, PCL, FCL
KD IV Injury to ACL, PCL, MCL, FCL
KD V Dislocation + fracture
Additional caps of “C” and “N” are utilized for associated injuries. “C” indicates an arterial injury. “N” indicates a neural injury, such as the tibial or, more commonly, the peroneal nerve. ACL, anterior cruciate ligament; FCL, fibular collateral ligament; KD, Knee Dislocation Classification I–V; MCL, media collateral ligament.
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
present when a line from the centre of the femoral head to the centre of the ankle joint (the mechanical axis) falls medial to the apex of the medial tibial eminence on a long-leg alignment radiograph (figure 5). When varus mal-alignment is present in a patient with a chronic PLC injury, a corrective osteotomy should be considered prior to reconstruction. Reconstruction grafts in the PLC do not tolerate varus mal-alignment, and this will potentially lead to graft stretching and reconstruction failure. Arthur et al reported on 21 patients with chronic combined PLC
injuries, 38% had sufficient improvement after proximal tibia osteotomy that subsequent PLC reconstruction was not neces-sary.27
Concomitant injuriesHigh incidences of meniscal and focal cartilage injuries are reported in multiligament knee injuries. In a review of 303 patients at a level I trauma centre (Moatshe et al,10), reported meniscal injuries were found in 37.3% of the patients and carti-lage injuries in 28.3%. Richter et al reported lower incidence (15%) of meniscal injuries in association with knee disloca-tions;28 however, Krych et al reported higher rates of meniscal and chondral lesions associated with knee dislocation in 121 patients (122 knees) with 76% of overall patients having a meniscal or chondral injury; 55% presented with meniscal tears while 48% presented with a chondral injury.29 Common pero-neal nerve injuries are frequently associated with lateral-sided injuries. Moatshe et al.10 reported common peroneal nerve inju-ries and vascular injuries in 19% and 5% of the 303 patients with knee dislocations, respectively. Medina et al19 reported a frequency of 25% and 18% for nerve and vascular injuries in knee dislocations, respectively, in a recent systematic review.
Table 2 Evaluation of posterior knee instability
Grade Clinical finding with posterior drawer test
Kneeling stress radiographs
I 0–5 mm PTT 0–7 mm PTT → normal or partial tear
II 5–10 mm PTT 8–11 mm PTT → Complete PCL tear
III >10 mm PTT → posterior sag ≥ 12 mm PTT → Combined ligament injury
Clinical test findings and the corresponding stress radiograph values in evaluating posterior knee instability. PCL, posterior cruciate ligament; PTT, posterior tibial translation.
Table 3 Evaluation of varus and valgus instability using stress radiographs
Varus stress test Valgus stress test
<2.7 mm → Normal or partial tear <3.2 mm → Normal or partial tear
2.7 mm → Isolated FCL tear 3.2 mm → Complete sMCL tear
≥4 mm: → Complete PLC injury ≥9.8 mm → Complete tear of all medial structures
Side-to-side differences between the injured and the noninjured knee using stress radiograph to evaluate varus and valgus knee instability.FCL, fibular collateral ligament; PLC, posterolateral corner; sMCL, superficial medial collateral ligament.
Figure 2 Kneeling stress radiographs for evaluation posterior laxity are an important part of the evaluation. In this patient, there was a 10 mm increase in posterior tibial translation on the left compared with the right knee. To compare the posterior tibial translation, a point is identified along the posterior tibial cortex 15 cm distal to the joint line. A line is then drawn from this point parallel to the posterior cortex, through the femoral condyles. The most posterior point of Blumensaat’s line is marked. A perpendicular line is drawn from the most posterior point of the Blumensaat´s line to intersect the first line drawn parallel to the tibial cortex. This distance is compared with the contralateral side to give a side-to-side difference. A posterior translation side-to-side difference of 0 to 6 mm are usually due to partial PCL tear or in patients who are too sore to put sufficient weight on the knee; an 8 mm to 11 mm side-to-side difference is associated with a complete isolated PCL tear; ≥12 mm is usually observed in patients with complete PCL tear with another ligament injury, usually the PLC or PMC, but can also be seen in patients with decreased sagittal plane tibial slope. PCL, posterior cruciate ligament; PLC, posterolateral corner; PMC, posteromedial corner.
Figure 3 Valgus stress radiographs to evaluate the medial and posteromedial side of the knee are important and should be incorporated in the evaluation, especially in chronic cases. In this case there is a 3.4 mm increase in medial compartment gapping on the right (A) compared with the left (B) knee, indication a complete sMCL tear. Overall, a 3.2 mm side to side difference of gapping represents a complete sMCL tear, and a 9.8 mm difference represents injury to all medial structures. sMCL, superficial medial collateral ligament.
Figure 4 A photograph demonstrating measurement of systolic blood pressure on the injured limb (ankle) using a Doppler probe (A) and systolic blood pressure on the uninjured upper limb (brachial) (B). The ankle brachial index (ABI) is calculated by taking the ratio of the Doppler systolic blood pressure in the injured limb (ankle) to the systolic arterial blood pressure in the uninjured upper limb (brachial). ABI = Doppler systolic blood pressure in the injured limb/systolic blood pressure in the uninjured upper limb.
3Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
Becker et al reported peroneal nerve injury in 25% of knees and arterial injury in 21% in a series of 106 patients.30 Moatshe et al10 reported that the odds of having a peroneal nerve injury were 42 times higher among patients with injury than those without, while the odds of having a popliteal artery injury were 9.2 times higher in patients with a posterolateral corner injury (figure 6).
Medial-sided injuries are usually the most common injuries in multiligament knee injury patterns. Moatshe et al10 reported that medial-sided injuries constituted 52% of the injuries in 303 patients with multiligament knee injuries. In their series, lateral-sided injuries constituted 28% and bicruciate injuries constituted only 5%. In a review by Robertson et al,31 medi-al-sided and lateral-sided injuries were reported in 41% and 28%, respectively. In contrast, Becker et al reported that later-al-sided injuries were the most common (43%) in a series of 106 patients.30
Surgical versus nonsurgical managementSurgical treatment of the torn ligaments in multiligament injured knees improves patient-reported outcomes.28 32 33 In a meta-anal-ysis including 132 knees treated surgically and 74 treated nonsur-gically, Dedmond et al reported improved motion and Lysholm scores in the surgical treatment group.32 The surgical group had significantly better range of motion (123° in the surgical group vs 108° in the nonsurgical group) and Lysholm scores (85.2 in the surgical group vs 66.5 in the nonsurgical group). Richter et al27 reported on 89 patients with traumatic knee dislocations with a mean follow-up of 8.2 years. Sixty-three patients were treated with surgical repair or reconstruction, while 26 patients were treated nonsurgically. The authors reported significantly improved outcomes in the surgical group compared with the nonsurgical group. Functional rehabilitation after surgery was reported to be the most important positive prognostic factor. In addition, patients who were 40 years of age or younger and who had low velocity sports injuries had better scores.28 In a liter-ature review by Peskun and Whelan,33 evaluating outcomes in 855 patients from 31 studies treated surgically, and 61 patients from four studies treated nonsurgically, functional outcomes, contracture, instability, and return to activity favoured surgical treatment. In summary, the literature supports surgical treat-ment, and postoperative functional rehabilitation of multiliga-ment knee injuries. It is in rare occasions such as advanced age, immobility and comorbidities that nonsurgical treatment can be considered.
repair versus reconstructionEarlier studies have reported poor outcomes after repair of isolated ACL injuries.34–36 Mariani et al evaluated outcomes in a cohort of patients with multiligament injuries; 52 patients treated with repair of the ligaments versus 28 treated with reconstructions.37 All patients had bicruciate ligament injuries, and they were divided into three groups; direct ACL/PCL repair (group 1), ACL reconstruction and PCL repair (group 2) and ACL and PCL reconstruction (group 3). Patients with repair of cruciate ligaments had higher rates of flexion deficit >6°, higher rates of posterior instability and lower rates of return to prein-jury activity levels. High reoperation rates have been reported in patients with posterolateral injuries treated with repair.38 39 Anatomic reconstruction of the injured structures using biome-chanically validated techniques has been reported to yield improved outcomes (figure 7).40–42 In the setting of multiligament injuries, reconstruction of the torn ligaments is recommended.
Figure 5 In chronic cases, long-leg radiographs are recommended to evaluate alignment. Patients with chronic PLC injuries and varus malalignment should be treated with an osteotomy to correct mal-alignment prior to PLC reconstruction. Untreated mal-alignment will likely cause the grafts to stretch over time and fail. PLC: posterolateral corner.
Figure 6 Image showing a left knee with multiligament knee injury involving the posterolateral corner. There is increased risk of common peroneal nerve injury with posterolateral corner injuries. CPN: common peroneal nerve.
4 Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
Repair of the collaterals is usually reserved for bony avulsion injuries.43
Timing of surgeryTiming of surgery during multiligament injuries is a topic of debate. In addition, there is still no consensus on the point of demarcation between acute and chronic. Some authors have used 3 weeks as the critical time to better identify and treat the struc-tures before scarring and tissue necrosis affect outcomes.9 37 44 45 This is also particularly important in the case of bony avulsion injuries. However, some authors have used 6 weeks to demarcate between acute and chronic.40 Better outcomes are reported in acute compared with chronic treatment in studies that directly compared timing of treatment. Levy et al reported no difference in range of motion after acute and chronic surgery in a system-atic review of literature that included five studies46 Moatshe et al. (unpublished data, 2016) reported on 303 patients with knee dislocations, and the percentage of patients developing arthro-fibrosis was 15.2% and 3.8% in the acutely treated and the chronic injuries, respectively. The authors preferred acute treat-ment of the injured structures to facilitate early rehabilitation.40 In addition, staging the reconstruction can potentially alter joint kinematics, and increase the risk of graft failure.47–49 In high energy trauma, surgery may be delayed because of injuries to the soft tissue about the knee and concomitant injuries to other vital organs. However, stiffness in these patients may be easier to treat than recurrent instability.
Surgical principlesAvoiding tunnel convergenceReconstructing several reconstruction tunnels in the distal femur and proximal tibia pose a risk of tunnel convergence because of limited bone mass in these areas. Tunnel convergence increases the risk of reconstruction graft failure because of the potential damage to reconstruction grafts, fixation devices and not having
sufficient bone stock between the grafts for fixation and graft incorporation. Few studies have evaluated the risk of tunnel convergence and optimal angulation of the tunnels. Moatshe et al reported a 66.7% tunnel convergence rate between the posterior oblique ligament (POL) tunnel and the PCL tunnel in the tibia when the POL tunnel was aimed at Gerdy´s tubercle. They recommended that the POL tunnels be aimed to a point 15 mm medial to Gerdy´s tubercle to reduce risk of convergence with the PCL, and that the superficial medial collateral ligament (sMCL) tunnel be aimed 30° distally to avoid convergence with the PCL.50
On the lateral femoral side, Moatshe et al (in press, 2016) performed a 3D imaging study varying the angles of the FCL and popliteus tunnels. A 35°–40° angulation in the axial plane and 0° in the coronal plane were safe and avoided tunnel convergence. On the medial side, aiming the sMCL tunnel 40° in the axial and coronal planes and the POL tunnel 20° in the axial and coronal planes was safe to avoid convergence with the double-bundle PCL tunnels (figure 8). In a laboratory study, Carmada et al reported a high risk of tunnel convergence between the ACL and the FCL (69%–75% depending on the length of the tunnel) and recommended aiming the FCL tunnel 0° in the coronal plane and 20° - 40° in the axial plane.51 Gelber et al evaluated tunnel convergence and optimal angulation of the tunnels on the medial femur condyle. They found that angulations of 30° in the axial plane and coronal plane reduced the risk of convergence with the PCL tunnels.52 However, the diameter of their PCL tunnels were smaller than those used by Moatshe et al.
Tensioning sequenceThe tensioning sequence in multiligament injuries is a topic of debate. Different tensioning sequences have been reported in the literature. Some authors advocate for starting with the PCL to restore the central pivot and tibial step-off, followed by the ACL in extension to ensure the knee can be fully extended, postero-lateral corner and the posteromedial corner last.53 54 A biome-chanical study by Wentorf et al reported that in a posterolateral corner deficient knee, tension during fixation of the ACL graft increased external tibial rotation of the tibia.49 Therefore, there
Figure 7 An intraoperative arthroscopy image showing double-bundle PCL reconstruction. Anatomic reconstruction of all the torn ligaments using biomechanically and clinically validated techniques is recommended. ALB, anterolateral bundle; PMB, posteromedial bundle; MFC, medial femoral condyle.
Figure 8 Reconstruction of the sMCL on a right knee. The AT is an important landmark to locate the adductor tubercle which is just distal to the adductor tendon insertion. The attachment site of the MCL is 12 mm distal and 8 mm anterior to the adductor tubercle. To avoid convergence with the PCL tunnels, the sMCL and popliteus tunnels should be aimed anteriorly and proximally. AT, adductor tendon; PCL, posterior cruciate ligament; sMCL, superficial medial collateral ligament.
5Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
are authors that advocate for fixing the posterolateral corner prior to the ACL to avoid external tibial rotation. Markolf et al reported in a biomechanical study that the PCL should be fixed prior to the ACL to best restore graft forces.55 Kim et al retro-spectively reviewed 25 patients with multiligament injuries, 14 with the PCL tensioned first and 11 with simultaneous tension and fixing the ACL first. Posterior stress radiographs, Lysholm score, International Knee Documentation Committee (IKDC) scores favoured fixing the ACL first.56 The optimal tensioning sequence can be best evaluated with well-designed biome-chanical studies.57 The authors preferred tensioning sequence which fixes the anterolateral bundle of the PCL at 90° to restore the normal tibial step-off, the posteromedial bundle of the PCL in extension, the FCL at 20°−30° of knee flexion and a slight valgus force, followed by the rest of the PLC structures at 60° of flexion and neutral rotation, the ACL near full extension and finally the posteromedial corner.
Surgical techniqueA thorough preoperative assessment to aid patient selection and planning of treatment is important (box 3). The surgical technique uses both allografts and autografts depending on the ligaments injured. Anatomic ligament reconstructions that are biomechanically and clinically validated are performed. An open surgical approach is performed prior to arthroscopy to allow for improved soft tissue visualisation and to limit fluid extravasa-tion into the surgical site. On the medial side, a skin incision is performed proximally between the adductor tubercle and the patella and extended 8 cm distally from the joint line to the medial part of the tibia. The semitendinosus and gracilis tendons are harvested and fixed at the superficial MCL attachment site, 6 cm distal to the joint line with two suture anchors.58 A femoral reconstruction tunnel is reamed at the anatomic attachment of the MCL, and the grafts are passed under the sartorius fascia and the graft ends are whipstitched so that 30 mm will fit into the femoral tunnel (figure 9).59 On the posterolateral side, a technique described by LaPrade et al60 is performed using a split Achilles graft (figure 10). The fibular, tibial and femoral tunnels are reamed and passing sutures are placed. After drilling the tunnels for the collateral ligament reconstruction grafts, attention is turned to the intra-articular injuries. An anatomic double-bundle PCL41 61 and single-bundle ACL reconstructions are performed. The concomitant meniscal and chondral lesions are addressed prior to graft fixation and tensioning. Graft tensioning is performed as described above. Tips and tricks, and some potential pitfalls when performing this type of surgery can be found in box 4 and box 5 respectively.
rehabilitationMultiligament knee injuries are complex and challenging pathol-ogies to rehabilitate due to the extensive soft tissue damage and the different injury patterns that can occur. An appropriate
diagnosis and treatment of all the damaged structures is vital for a successful outcome. Reconstruction of all injured liga-ments and repair of soft tissue structures such as the meniscus or cartilage are recommended to aid in early mobilisation and to avoid joint stiffness or graft failure. Postoperative recovery after a multiligament reconstruction procedure typically requires 9–12 months of rehabilitation prior to returning to full activities. This allows proper time for the grafts to incorporate and to heal in order to prevent reconstruction graft failure. A well-crafted rehabilitation plan after a multiligament reconstruction should focus on graft protection and functional outcomes including regaining motion, strength and function. A dynamic PCL brace
Figure 9 A diagram of a left knee illustrating the superficial medial collateral: ligament (sMCL) and posterior oblique ligament (POL) reconstruction grafts. ME: medial epicondyle. Reprinted with permission of SAGE Publications, Inc, from Coobs BR, Wijdicks CA, Armitage BM, Spiridonov SI, Westerhaus BD, Johansen S, Engebretsen L, LaPrade RF. An in vitro analysis of an anatomic medial knee reconstruction. Am J Sports Med. 2010;38:339–347
box 3 Key issues of patient selection
► Injury to>1 major knee ligament (ACL, PCL, MCL, FCL or PCL) ► Active patients without major comorbidities ► Detailed assessment of all injuries ► Aim for surgical treatment of all injured structures in the
acute setting ► Obese patients have higher complication rates ► Delay ligament surgery in patients with vascular injuries
Figure 10 An illustration of the right knee demonstrating the posterolateral knee reconstruction procedure. A, posterior view; B, lateral view. PLT, popliteus tendon; FCL, fibular collateral ligament; PFL, popliteofibular ligament. Reprinted with permission of SAGE Publications, Inc, from LaPrade RF, Johansen S, Wentorf FA, Engebretsen L, Esterberg JL, Tso A. An Analysis of an Anatomical Posterolateral Knee Reconstruction: An In Vitro Biomechanical Study and Development of a Surgical Technique. Am J Sports Med. 2004;32:1405–1414.
6 Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
(Ossur PCL Rebound brace, Foothill Ranch, CA, USA) or a Jack PCL brace (Albrecht GmbH, DE, USA) is used in the rehabili-tation period (9–12 months) to protect the reconstruction. It is also recommended to use a brace on the first year of returning to activities. Full range of motion is especially vital to long-term outcomes, and patients should aim to obtain 0–90° of knee flexion within the first 2 weeks after surgery. Once a muscular strength foundation with good dynamic neuromuscular control has been established, patients can progress to their functional sport specific exercises.
Initial management should focus on supportive measures such as pain control, inflammation/effusion control (cryotherapy, elevation and compression of the affected limb), range of motion re-establishment, patellar mobilisation, restoring appropriate muscle activation patterns and progressive gait training. Soft tissue healing involves a predictable series of phases (inflam-mation, proliferative and remodelling phases) that should be addressed at a proper time to promote physiological healing responses, minimise negative changes and facilitate the prolif-eration and alignment of collagen fibres.62 Patellar mobilisation should be a primary initial focus of the rehabilitation, as hypo-mobility of the proximal pole of the patella can interfere with the extensor mechanism leading to loss of range of motion and a quadricep lag.62 Conversely, flexion can be affected by a dimin-ished patellar inferior glide. With regards to weight bearing, to date there is no randomised clinical trial assessing the effective-ness of early weight bearing after a multiligament reconstruc-tion, and therefore protected weight bearing is carried out for the first 6 weeks after which partial weight bearing is allowed.
Periodisation is the division of a training or rehabilitation programme into smaller phases (periods) as a means of creating more manageable segments. In a multiligament knee reconstruc-tion rehabilitation programme, the phases are constituted by muscular endurance, strength and power and can be developed based on the patient’s expectations and return to activity time-line. The length of each phase depends on the time frame of the rehabilitation programme, but it should be no shorter than 6 weeks. With range of motion (ROM) restored, the treatment emphasis shifts to the development of a muscular endurance base. A transition in training emphasis to the development of muscular strength can then be made before muscular power is developed. Three to four sessions a week are appropriate while still providing adequate recovery between sessions.63
Given the numerous variables (age, BMI, sport, concurrent injuries, etc) that can interact in the decision to allow a patient to return to sport, the rehabilitation process and return to sport timeline should be tailored to each patient. A systematic review of 264 studies by Barber-Westin and Noyes reported that the return to play decision was based on subjective nonspecific criteria such as ‘regained full functional stability’, ‘normal knee function on clinical examination’, ‘satisfactory stability’ or ‘nearly full ROM and muscle strength’.64 Few studies described objective criteria such as time from surgery, muscle strength, ROM and effusion, which were the most frequently used.64
Subjective and objective outcomesPoor outcomes are reported for nonsurgical management of multiligament knee injuries, therefore this section will focus on outcomes after surgical management. Preoperative and post-operative stability and functional scores are usually compared to evaluate patient outcomes (box 6). Unfortunately, most studies on multiligament knee injuries have small cohorts and the follow-up is generally short. Good functional outcomes are reported in short to medium follow-up after surgical treatment
box 4 Tips and tricks
► Patient positioning: The patient should be positioned to allow full flexion and extension of the knee.
► Graft preparation: Ensure availability of grafts and correct graft length. Tightly spacing the whipstitch sutures protects the grafts from laceration when securing with an interfer-ence screw.
► Steps during surgery: Start with the collateral ligament injuries. Fluid extravasation from arthroscopy can impair visualisation and identification of structures.
► Tunnel positioning: All the tunnels should be placed at the anatomic footprint of the ligaments being reconstructed. All the tunnels’ positions and orientations should be planned in detail to avoid tunnel convergence. Aiming the femoral FCL and popliteus tunnels anteriorly reduces the risk of convergence with the ACL tunnel and the risk of violating the intercondylar notch. The centre of the popliteus tunnel is 18.5 mm anterior to the centre of the FCL tunnel, and there is an 8–9 mm bone bridge between the tunnels. The femoral tunnels for the posteromedial corner should be aimed anteriorly and proximally to avoid convergence with the PCL tunnels. The femoral PCL tunnels should be divergent.
► Acorn reamers: These reamers allow the surgeon to add fine adjustments to the tibial tunnel paths. The edges of the tunnels should be smooth to prevent the bone edges from damaging the grafts.
► Fixation: The sequence of graft fixation affects the tibiofem-oral orientation and the graft forces. The PCL is tensioned first, followed by the PLC, then the ACL and finally the PMC.
► Postoperative rehabilitation: Early protected range of motion is important. Periodisation, progressive weight bearing, quadriceps activation and patella mobility. Rehabilitation takes 9–12 months. Use brace during activities the first year of returning to activities.
box 5 Major pitfalls
► Patient positioning: Incorrect positioning of the patient may limit knee motion and the space available for the surgeon to work effectively.
► Graft preparation: Oversizing the grafts can complicate the passage of grafts in the tunnels. Care must be taken to ensure availability of graft for all torn ligaments.
► Tunnel convergence: With many tunnels being created in both the femur and tibia, the risk of tunnel convergence is high. Tunnel convergence will potentially damage the grafts, fixation devices, create too short tunnels or leave not enough bone stock for graft fixation and integration. The PCL femoral tunnels should be divergent.
► Meniscal root injuries: Malposition of the PCL tibial tunnel can potentially injure the posterior root of the medial meniscus. Malposition of the ACL tibial tunnels can poten-tially injure the anterior horn of the lateral meniscus.
► Neurovascular complications: There is increased risk of neurovascular injuries when creating tibial femoral tunnels. The guide pin should be visualised and advancement of the guide pin should be prevented during reaming.
► Fixation: The sequence of graft fixation can theoretically alter tibiofemoral orientation and thus knee kinematics, increasing the risk of graft failure and osteoarthritis.
7Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from
State of the Art
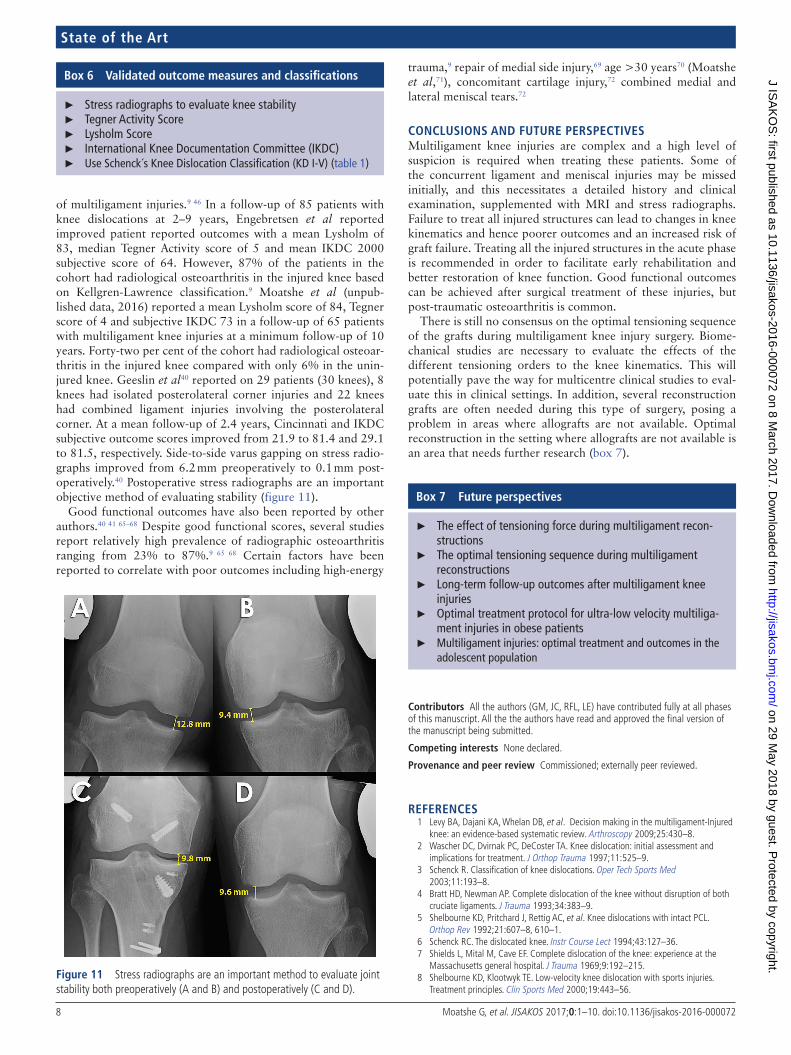
of multiligament injuries.9 46 In a follow-up of 85 patients with knee dislocations at 2–9 years, Engebretsen et al reported improved patient reported outcomes with a mean Lysholm of 83, median Tegner Activity score of 5 and mean IKDC 2000 subjective score of 64. However, 87% of the patients in the cohort had radiological osteoarthritis in the injured knee based on Kellgren-Lawrence classification.9 Moatshe et al (unpub-lished data, 2016) reported a mean Lysholm score of 84, Tegner score of 4 and subjective IKDC 73 in a follow-up of 65 patients with multiligament knee injuries at a minimum follow-up of 10 years. Forty-two per cent of the cohort had radiological osteoar-thritis in the injured knee compared with only 6% in the unin-jured knee. Geeslin et al40 reported on 29 patients (30 knees), 8 knees had isolated posterolateral corner injuries and 22 knees had combined ligament injuries involving the posterolateral corner. At a mean follow-up of 2.4 years, Cincinnati and IKDC subjective outcome scores improved from 21.9 to 81.4 and 29.1 to 81.5, respectively. Side-to-side varus gapping on stress radio-graphs improved from 6.2 mm preoperatively to 0.1 mm post-operatively.40 Postoperative stress radiographs are an important objective method of evaluating stability (figure 11).
Good functional outcomes have also been reported by other authors.40 41 65–68 Despite good functional scores, several studies report relatively high prevalence of radiographic osteoarthritis ranging from 23% to 87%.9 65 68 Certain factors have been reported to correlate with poor outcomes including high-energy
trauma,9 repair of medial side injury,69 age >30 years70 (Moatshe et al,71), concomitant cartilage injury,72 combined medial and lateral meniscal tears.72
ConCluSIonS And FuTurE pErSpECTIVESMultiligament knee injuries are complex and a high level of suspicion is required when treating these patients. Some of the concurrent ligament and meniscal injuries may be missed initially, and this necessitates a detailed history and clinical examination, supplemented with MRI and stress radiographs. Failure to treat all injured structures can lead to changes in knee kinematics and hence poorer outcomes and an increased risk of graft failure. Treating all the injured structures in the acute phase is recommended in order to facilitate early rehabilitation and better restoration of knee function. Good functional outcomes can be achieved after surgical treatment of these injuries, but post-traumatic osteoarthritis is common.
There is still no consensus on the optimal tensioning sequence of the grafts during multiligament knee injury surgery. Biome-chanical studies are necessary to evaluate the effects of the different tensioning orders to the knee kinematics. This will potentially pave the way for multicentre clinical studies to eval-uate this in clinical settings. In addition, several reconstruction grafts are often needed during this type of surgery, posing a problem in areas where allografts are not available. Optimal reconstruction in the setting where allografts are not available is an area that needs further research (box 7).
Contributors All the authors (GM, JC, RFL, LE) have contributed fully at all phases of this manuscript. All the the authors have read and approved the final version of the manuscript being submitted.
Competing interests None declared.
provenance and peer review Commissioned; externally peer reviewed.
RefeRences 1 Levy BA, Dajani KA, Whelan DB, et al. Decision making in the multiligament-Injured
knee: an evidence-based systematic review. Arthroscopy 2009;25:430–8. 2 Wascher DC, Dvirnak PC, DeCoster TA. Knee dislocation: initial assessment and
implications for treatment. J Orthop Trauma 1997;11:525–9. 3 Schenck R. Classification of knee dislocations. Oper Tech Sports Med
2003;11:193–8. 4 Bratt HD, Newman AP. Complete dislocation of the knee without disruption of both
cruciate ligaments. J Trauma 1993;34:383–9. 5 Shelbourne KD, Pritchard J, Rettig AC, et al. Knee dislocations with intact PCL.
Orthop Rev 1992;21:607–8, 610–1. 6 Schenck RC. The dislocated knee. Instr Course Lect 1994;43:127–36. 7 Shields L, Mital M, Cave EF. Complete dislocation of the knee: experience at the
Massachusetts general hospital. J Trauma 1969;9:192–215. 8 Shelbourne KD, Klootwyk TE. Low-velocity knee dislocation with sports injuries.
Treatment principles. Clin Sports Med 2000;19:443–56.Figure 11 Stress radiographs are an important method to evaluate joint stability both preoperatively (A and B) and postoperatively (C and D).
box 6 Validated outcome measures and classifications
► Stress radiographs to evaluate knee stability ► Tegner Activity Score ► Lysholm Score ► International Knee Documentation Committee (IKDC) ► Use Schenck´s Knee Dislocation Classification (KD I-V) (table 1)
box 7 Future perspectives
► The effect of tensioning force during multiligament recon-structions
► The optimal tensioning sequence during multiligament reconstructions
► Long-term follow-up outcomes after multiligament knee injuries
► Optimal treatment protocol for ultra-low velocity multiliga-ment injuries in obese patients
► Multiligament injuries: optimal treatment and outcomes in the adolescent population
8 Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
9 Engebretsen L, Risberg MA, Robertson B, et al. Outcome after knee dislocations: a 2-9 years follow-up of 85 consecutive patients. Knee Surg Sports Traumatol Arthrosc 2009;17:1013–26.
10 Moatshe G, Dornan GJ, Løken S, et al. Knee dislocations demographics and associated injuries: a prospective review of 303 patients. Orthop J Sports Med 2017, In Press.
11 Werner BC, Gwathmey FW, Higgins ST, Jr, et al. Ultra-low velocity knee dislocations: patient characteristics, complications, and outcomes. Am J Sports Med 2014;42:358–63.
12 Geeslin AG, LaPrade RF. Location of bone bruises and other osseous injuries associated with acute grade III isolated and combined posterolateral knee injuries. Am J Sports Med 2010;38:2502–8.
13 Jackman T, LaPrade RF, Pontinen T, et al. Intraobserver and interobserver reliability of the kneeling technique of stress radiography for the evaluation of posterior knee laxity. Am J Sports Med 2008;36:1571–6.
14 Tsai AG, Wijdicks CA, Walsh MP, et al. Comparative kinematic evaluation of all-inside single-bundle and double-bundle anterior cruciate ligament reconstruction: a biomechanical study. Am J Sports Med 2010;38:263–72.
15 James EW, Williams BT, LaPrade RF. Stress radiography for the diagnosis of knee ligament injuries: a systematic review. Clin Orthop Relat Res 2014;472:2644–57.
16 Mills WJ, Barei DP, McNair P. The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: a prospective study. J Trauma 2004;56:1261–5.
17 Levy BA, Fanelli GC, Whelan DB, et al. Controversies in the treatment of knee dislocations and multiligament reconstruction. J Am Acad Orthop Surg 2009;17:197–206.
18 Wascher DC. High-velocity knee dislocation with vascular injury. treatment principles. Clin Sports Med 2000;19:457–77.
19 Medina O, Arom GA, Yeranosian MG, et al. Vascular and nerve injury after knee dislocation: a systematic review. Clin Orthop Relat Res 2014;472:2621–9.
20 Molund M, Engebretsen L, Hvaal K, et al. Posterior tibial tendon transfer improves function for foot drop after knee dislocation. Clin Orthop Relat Res 2014;472:2637–43.
21 Carr JB, Werner BC, Miller MD, et al. Knee dislocation in the morbidly obese patient. J Knee Surg 2016;29:278–86.
22 Kendall RW, Taylor DC, Salvian AJ, et al. The role of arteriography in assessing vascular injuries associated with dislocations of the knee. J Trauma 1993;35:875–8.
23 Klineberg EO, Crites BM, Flinn WR, et al. The role of arteriography in assessing popliteal artery injury in knee dislocations. J Trauma 2004;56:786–90.
24 Levy BA, Fanelli GC, Whelan DB, et al; Knee Dislocation Study Group. Controversies in the treatment of knee dislocations and multiligament reconstruction. J Am Acad Orthop Surg 2009;17:197–206.
25 Stannard JP, Sheils TM, Lopez-Ben RR, et al. Vascular injuries in knee dislocations: the role of physical examination in determining the need for arteriography. J Bone Joint Surg Am 2004;86-A:910–5.
26 Stuart MJ. Evaluation and treatment principlesof knee dislocations. Operative Techniques in Sports Medicine 2001;9:91–5.
27 Arthur A, LaPrade RF, Agel J. Proximal tibial opening wedge osteotomy as the initial treatment for chronic posterolateral corner deficiency in the varus knee: a prospective clinical study. Am J Sports Med 2007;35:1844–50.
28 Richter M, Bosch U, Wippermann B, et al. Comparison of surgical repair or reconstruction of the cruciate ligaments versus nonsurgical treatment in patients with traumatic knee dislocations. Am J Sports Med 2002;30:718–27.
29 Krych AJ, Sousa PL, King AH, et al. Meniscal tears and articular cartilage damage in the dislocated knee. Knee Surg Sports Traumatol Arthrosc 2015;23:3019–25.
30 Becker EH, Watson JD, Dreese JC. Investigation of multiligamentous knee injury patterns with associated injuries presenting at a level I trauma center. J Orthop Trauma 2013;27:226–31.
31 Robertson A, Nutton RW, Keating JF. Dislocation of the knee. J Bone Joint Surg Br 2006;88:706–11.
32 Dedmond BT, Almekinders LC. Operative versus nonoperative treatment of knee dislocations: a meta-analysis. Am J Knee Surg 2001;14:33–8.
33 Peskun CJ, Whelan DB. Outcomes of operative and nonoperative treatment of multiligament knee injuries: an evidence-based review. Sports Med Arthrosc 2011;19:167–73.
34 Feagin JA, Curl WW. Isolated tear of the anterior cruciate ligament: 5-year follow-up study. Am J Sports Med 1976;4:95–100.
35 Taylor DC, Posner M, Curl WW, et al. Isolated tears of the anterior cruciate ligament: over 30-year follow-up of patients treated with arthrotomy and primary repair. Am J Sports Med 2009;37:65–71.
36 Engebretsen L, Svenningsen S, Benum P. Poor results of anterior cruciate ligament repair in adolescence. Acta Orthop Scand 1988;59:684–6.
37 Mariani PP, Santoriello P, Iannone S, et al. Comparison of surgical treatments for knee dislocation. Am J Knee Surg 1999;12:214–21.
38 Levy BA, Dajani KA, Morgan JA, et al. Repair versus reconstruction of the fibular collateral ligament and posterolateral corner in the multiligament-injured knee. Am J Sports Med 2010;38:804–9.
39 Stannard JP, Brown SL, Farris RC, et al. The posterolateral corner of the knee: repair versus reconstruction. Am J Sports Med 2005;33:881–8.
40 Geeslin AG, LaPrade RF. Outcomes of treatment of acute grade-III isolated and combined posterolateral knee injuries: a prospective case series and surgical technique. J Bone Joint Surg Am 2011;93:1672–83.
41 Spiridonov SI, Slinkard NJ, LaPrade RF. Isolated and combined grade-III posterior cruciate ligament tears treated with double-bundle reconstruction with use of endoscopically placed femoral tunnels and grafts: operative technique and clinical outcomes. J Bone Joint Surg Am 2011;93:1773–80.
42 Laprade RF, Griffith CJ, Coobs BR, et al. Improving outcomes for posterolateral knee injuries. J Orthop Res 2014;32:485–91.
43 Geeslin AG, Moulton SG, LaPrade RF. A systematic review of the outcomes of posterolateral corner knee injuries, Part 1: Surgical Treatment of Acute Injuries. Am J Sports Med 2016;44;.
44 Fanelli GC, Giannotti BF, Edson CJ. Arthroscopically assisted combined posterior cruciate ligament/posterior lateral complex reconstruction. Arthroscopy 1996;12:521–30.
45 Harner CD, Waltrip RL, Bennett CH, et al. Surgical management of knee dislocations. J Bone Joint Surg Am 2004;86-A:262–73.
46 Levy BA, Dajani KA, Whelan DB, et al. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy 2009;25:430–8.
47 LaPrade RF, Muench C, Wentorf F, et al. The effect of injury to the posterolateral structures of the knee on force in a posterior cruciate ligament graft: a biomechanical study. Am J Sports Med 2002;30:233–8.
48 LaPrade RF, Resig S, Wentorf F, et al. The effects of grade III posterolateral knee complex injuries on anterior cruciate ligament graft force. A biomechanical analysis. Am J Sports Med 1999;27:469–75.
49 Wentorf FA, LaPrade RF, Lewis JL, et al. The influence of the integrity of posterolateral structures on tibiofemoral orientation when an anterior cruciate ligament graft is tensioned. Am J Sports Med 2002;30:796–9.
50 Moatshe G, Slette EL, Engebretsen L LaPrade RF. Intertunnel relationships in the tibia during reconstruction of multiple knee ligaments: how to avoid tunnel convergence. Am J Sports Med 2016;44:2864–9.
51 Camarda L, D’Arienzo M, Patera GP, et al. Avoiding tunnel collisions between fibular collateral ligament and ACL posterolateral bundle reconstruction. Knee Surg Sports Traumatol Arthrosc 2011;19:598–603.
52 Gelber PE, Masferrer-Pino À, Erquicia JI, et al. Femoral tunnel drilling angles for posteromedial corner reconstructions of the knee. Arthroscopy 2015;31:1764–71.
53 Fanelli GC, Edson CJ. Surgical treatment of combined PCL-ACL medial and lateral side injuries (global laxity): surgical technique and 2- to 18-year results. J Knee Surg 2012;25:307–16.
54 Levy BA, Boyd JL, Stuart MJ. Surgical treatment of acute and chronic anterior and posterior cruciate ligament and lateral side injuries of the knee. Sports Med Arthrosc 2011;19:110–9.
55 Markolf KL, O’Neill G, Jackson SR, et al. Reconstruction of knees with combined cruciate deficiencies: a biomechanical study. J Bone Joint Surg Am 2003;85-A:1768–74.
56 Kim SJ, Kim SH, Jung M, et al. Does sequence of graft tensioning affect outcomes in combined anterior and posterior cruciate ligament reconstructions? Clin Orthop Relat Res 2015;473:235–43.
57 Levy BA. CORR Insights®: Does sequence of graft tensioning affect outcomes in combined anterior and posterior cruciate ligament reconstructions? Clin Orthop Relat Res 2015;473:244–5.
58 Wijdicks CA, Griffith CJ, Johansen S, et al. Injuries to the medial collateral ligament and associated medial structures of the knee. J Bone Joint Surg Am 2010;92:1266–80.
59 Wijdicks CA, Michalski MP, Rasmussen MT, et al. Superficial medial collateral ligament anatomic augmented repair versus anatomic reconstruction: an in vitro biomechanical analysis. Am J Sports Med 2013;41:2858–66.
60 LaPrade RF, Johansen S, Wentorf FA, et al. An analysis of an anatomical posterolateral knee reconstruction: an in vitro biomechanical study and development of a surgical technique. Am J Sports Med 2004;32:1405–14.
61 Kennedy NI, LaPrade RF, Goldsmith MT, et al. Posterior cruciate ligament graft fixation angles, part 2: biomechanical evaluation for anatomic double-bundle reconstruction. Am J Sports Med 2014;42:2346–55.
62 Romeyn RL, Jennings J, Davies GJ. Surgical treatment and rehabilitation of combined complex ligament injuries. N Am J Sports Phys Ther 2008;3:212–25.
63 Lorenz DS, Reiman MP, Walker JC. Periodization: current review and suggested implementation for athletic rehabilitation. Sports Health 2010;2:509–18.
64 Barber-Westin SD, Noyes FR. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy 2011;27:1697–705.
65 Hirschmann MT, Zimmermann N, Rychen T, et al. Clinical and radiological outcomes after management of traumatic knee dislocation by open single stage complete reconstruction/repair. BMC Musculoskelet Disord 2010;11:102.
66 Fanelli GC, Edson CJ. Arthroscopically assisted combined anterior and posterior cruciate ligament reconstruction in the multiple ligament injured knee: 2- to 10-year follow-up. Arthroscopy 2002;18:703–14.
9Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from

State of the Art
67 Fanelli GC, Edson CJ. Surgical treatment of conbined PCL-ACL medial and lateral side injuries (Global Laxity): Surgical Technique and 2- to 18-Year Results. J Knee Surg 2012;25:307–16.
68 Fanelli GC, Sousa PL, Edson CJ. Long-term followup of surgically treated knee dislocations: stability restored, but arthritis is common. Clin Orthop Relat Res 2014;472:2712–7.
69 King AH, Krych AJ, Prince MR, et al. Surgical Outcomes of medial versus lateral Multiligament-Injured, Dislocated Knees. Arthroscopy 2016;32: 1814–9.
70 Levy NM, Krych AJ, Hevesi M, et al. Does age predict outcome after multiligament knee reconstruction for the dislocated knee? 2- to 22-year follow-up. Knee Surg Sports Traumatol Arthrosc 2015;23:3003–7.
71 Moatshe G, Dornan GJ, Ludvigsen TC, et al. High prevalence of knee osteoarthritis at a minimum 10-year follow-up after knee dislocation surgery. Knee Surg Sports Traumatol Arthrosc 2017, In Press.
72 King AH, Krych AJ, Prince MR, et al. Are meniscal tears and articular cartilage injury predictive of inferior patient outcome after surgical reconstruction for the dislocated knee? Knee Surg Sports Traumatol Arthrosc 2015;23:3008–11.
10 Moatshe G, et al. JISAKOS 2017;0:1–10. doi:10.1136/jisakos-2016-000072
on 29 May 2018 by guest. P
rotected by copyright.http://jisakos.bm
j.com/
J ISA
KO
S: first published as 10.1136/jisakos-2016-000072 on 8 M
arch 2017. Dow
nloaded from