diabetes susceptibility in sardinia
TRANSCRIPT
65
neurological disease. Since HTLV-II infection has been found tobe more prevalent than previously thought6 it is important toestablish the aetiological role of the virus in disease.
Department of Neurology,Kyushu University,Fukuoka 812, Japan;Department of Microbiology,Tokyo Medical and Dental University,and Ube Research Laboratory, Fujirebio Inc
JUN-ICHI KIRAYOSHIO KOYANAGITOSHINARI HAMAKADOYASUTO ITOYAMANAOKI YAMAMOTOIKUO GOTO
1. Roman GC, Osame M. Identity of HTLV-I-associated tropical spastic paraparesisand HTLV-I-associated myelopathy. Lancet 1988; i: 651.
2. Osame M, Janssen R, Kubota H, et al. Nationwide survey of HTLV-I-associatedmyelopathy in Japan: association with blood transfusion. Ann Neurol 1990; 28:50-56.
3. Hamakado T, Matsumoto T, Koyanagi Y, et al. Development of a supersensitivepolymerase chain reaction method for human T lymphotropic virus type II(HTLV-II) and detection of HTLV-II proviral DNA from blood donors in Japan.Virus Gene (in press).
4. Kira J, Koyanagi Y, Yamada T, et al. Increased HTLV-I proviral DNA inHTLV-I-associated myelopathy: a quantitative polymerase chain reaction study.Ann Neurol 1991; 29: 194-201.
5 Yoshida M, Osame M, Usuku K, et al. Viruses detected in HTLV-I-associated
myelopathy and adult T-cell leukaemia are identical in DNA blotting. Lancet 1987;i: 1085-86.
6. Lairmore MD, Jacobson S, Gracia F, et al. Isolation of human T-cell lymphotropicvirus type 2 from Guaymi Indians in Panama. Proc Natl Acad Sci 1990; 87:8840-44.
7 Greenberg SJ, Ehrlich GD, Abbott MA, et al. Detection of sequences homologous tohuman retroviral DNA in multiple sclerosis by gene amplification. Proc Natl AcadSci USA 1989; 233: 1076-78.
Diabetes susceptibility in Sardinia
SIR,-Dr Songini and Dr Muntoni (April 27, p 1047) stress thatthe high incidence of type-I diabetes in Sardinia contradicts thegeneral trend of a north-to-south gradient in Europe, the highestvalue being in Finland. They suggest that this high incidence can beexplained by genetic peculiarities in Sardinia but provide no specificdata on genetic susceptibility to insulin-dependent diabetes mellitus(IDDM) in this population. In Sardinia about 50% of the
population has the phenotype HLA-DR3 and 25% have the entireextended haplotype A30, Cw5, B18, 3F130, DR3, DQw2,’ adiabetogenic haplotype; the frequency of DR4 is about 30% andthat of DR2 is 40 %; 75 % of DR2 alleles in the Sardinian populationis represented by the DQB 1 *0502 allele,2 which is not protective forIDDM; and 36% of Sardinians have the IDDM susceptibilityphenotype HLA-DQ beta 57 non-Asp-non Asp.3Medical Genetics Department,Institute of Medical Clinics,University of Cagliari,09124 Cagliari, Italy
L. CONTUC. CARCASSI
Department of Pediatrics,University of Pittsburgh,Children’s Hospital,Pittsburgh, Pennsylvania, USA M. TRUCCO
1 Contu L, Carcassi C, Dausset J The "Sardinian" HLA-A30, B18, DR3, DQw2haplotype constantly lacks the 21-OH A and C4 B genes: is it an ancestral haplotypewithout duplication? Immunogenetics 1989; 30: 13-17.
2. Carcassi C, Trucco G, Trucco M, Contu L. A new HLA-DR2 extended haplotype isinvolved in IDDM susceptibility. Hum Immunol (in press).
3. La Nasa G, Carcassi C, Cirillo R, et al. Serological and molecular studies of HLA ininsulin-dependent diabetis mellitus in Sardinia. Dis Markers (in press).
HLA typing by double ARMSSIR,-DR typing within the class II human leucocyte antigens
(HLA) is conventionally done serologically in a mixed lymphocytereaction. The advent of the polymerase chain reaction (PCR) andoligotyping technology has allowed the accurate genotyping ofdifferent class II alleles.’ Oligotyping is typically done byhybridising sequence-specific oligonucleotides to dot blots of PCRproducts.2 The oligonucleotides are usually radiolabelled, whichmay limit application in a routine laboratory. The amplificationrefractory mutation system (ARMS)3 allows allele-specific DNAamplification to be used for HLA typing.4 However, because of thecomplexity of the HLA system, a single ARMS primer is often not
Fig 1-Relative locations of ARMS primers.DB3=5’ GACCACGTTTCTTGGAGCT 3’P-a=5’ CTCCTGGTTATGGAAGTATCTGTCCACGT 3’P-b=5’ GTCCTTCTGGCTGTTCCAGTACTCGGAAT 3’P-c =5’ CTCCCCCACGTCGCTGTCGAAGCGCACGG 3’AAT-1 =5’ CCCACCTTCCCCTCTCTCCAGGCAAATGGG 3’AAT-2-5’ GGGCCTCAGTCCCAACATGGCTAAGAGGTG 3’
sufficiently discriminatory for HLA typing to be done following asingle allele-specific amplification. Frequently, ARMS has to befollowed by oligotyping.1 Furthermore, the large number of HLAalleles necessitates an impracticable number of ARMS reactions.We have therefore devised a double ARMS method for HLA
typing that overcomes these limitations.This approach was developed for direct haplotype determination
in the &bgr;-globin cluster.s Two allele-specific ARMS primers areused simultaneously in a PCR to elucidate the relation between twopolymorphic sites on the same chromosome. Many HLA alleles arecharacterised by unique combinations of polymorphic sites that bythemselves may not be specific. Double ARMS offers much greaterdiscriminatory power. Furthermore, by designing ARMS primerssuch that different HLA alleles yield PCR products of differentlengths, a single PCR using a mixture of different primers issufficient to type many different alleles.As a model test system we used double ARMS to type the alleles
at the DRB3 locus, responsible for antigens HLA DRw52a,DRw52b, and DRw52c. An accurate system for typing DRB3alleles is clinically important because of the lack of discriminatoryserological reagents for these specificities and the recently reportedassociation with one DRw52 subtype and primary sclerosingcholangitis.6
Primers DB3, P-a, P-b, and P-c were ARMS primers and weredesigned from published sequences (see legend to fig 1). Deliberatemismatches near the 3’-end were introduced in P-a, P-b, and P-c toincrease specificity. AAT-1 and AAT-2 were as described byNewton et al.8 Primer DB3 is DRB3 specific and will not primeamplification from the other DRB loci. Primers P-a, P-b, and P-cdistinguish between the alleles coding for DRw52a (DRB3*0101),DRw52b (DRB3*0201 and DRB3*0202), and DRw52c
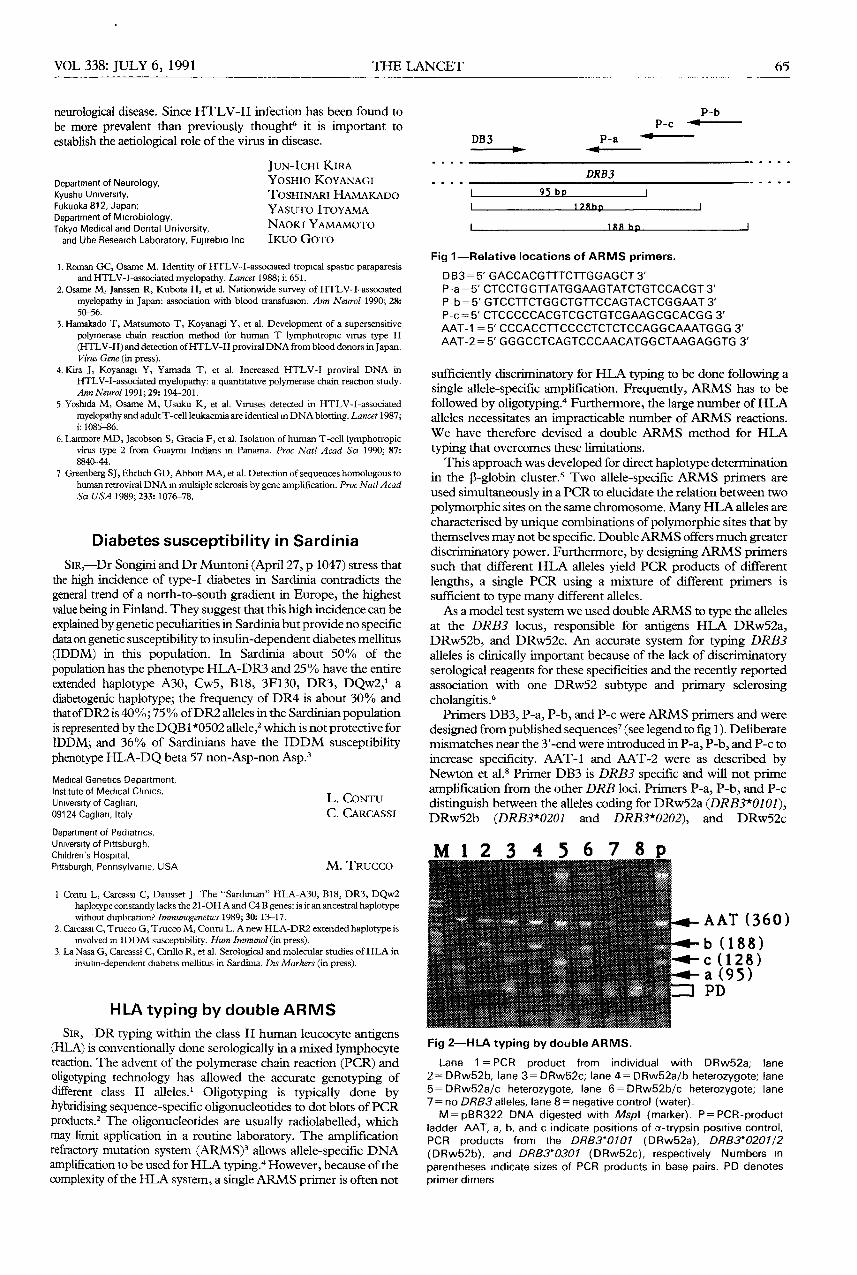
Fig 2-HLA typing by double ARMS.
Lane 1=PCR product from individual with DRw52a; lane
2=DRw52b, lane 3= DRw52c; lane 4= DRw52a/b heterozygote; lane5=DRw52a/c heterozygote, lane 6=DRw52b/c heterozygote; lane7 = no DRB3 alleles, lane 8 = negative control (water).M=pBR322 DNA digested with Mspl (marker). P=PCR-product
ladder AAT, a, b, and c indicate positions of a-trypsin positive control,PCR products from the DRB3*0101 (DRw52a), DRB3*0201/2(DRw52b), and DRB3*0301 (DRw52c), respectively Numbers in
parentheses indicate sizes of PCR products in base pairs. PD denotesprimer dimers