diabetes health disparities in the latino populationc.ymcdn.com/sites/ syndrome idf (international...
TRANSCRIPT

Diabetes Health Disparities in
the Latino Population The metabolic syndrome associated with
diabetes and the implications for clinical practice.
September 20, 2013
Portland, Oregon
Sponsored by: The CME Committee
OPSO
Richard B. Aguilar, MD Medical Director
Diabetes Nation, LLC Private Practice: Downey, California

Dr. Aguilar is a member of the Advisory Board and/or Speakers Bureau for:
- Boehringer Ingelheim Pharmaceuticals, Inc. - Eli Lilly & Company - Janssen Pharmaceuticals, Inc. - Novo Nordisk A/S - Takeda Pharmaceuticals of America
• In several instances, the branded names of certain medications may be
used (i.e. Humalog®, Humulin®, Novolog®, etc.) in addition to their non-branded names (Lispro, Regular, Aspart, etc). This may done in an attempt to minimize confusion that often exists when citing numerous medications and to improve the correct identification of the products being cited.
• All efforts were made to maintain fair balance.
• This will be done as little as possible and does not reflect any financial associations Dr. Aguilar has with the pharmaceutical industry.

Educational Objectives: • Understand the definitions of Metabolic Syndrome (MS)
• Understand the current diagnostic targets for diabetes as well as treatment goals for A1c, FPG and PPG in the context of individualization of care- (ADA/EASD Position Statement)
• Discuss the basic physiology surrounding the use of many of the agents used for the treatment of T2DM.
• Be familiar with the unique ethnic/Latino, cultural, genetic and environmental factors that may impact the development of diabetes and its management.
• Be familiar with Data from several large clinical trials which studied diabetes in Latinos.
• Review some culturally tailored practices that may be suitable to the primary care setting.

Diabetes and the “Latino”
The ethnic terms Latino and Hispanic are sometimes used interchangeably
Latino*: Persons of any race who trace their origin to Mexico, Puerto Rico, Cuba, Central and South America, or other Spanish cultures.*
* Standards for the Classification of Federal Data on race and Ethnicity. Federal Register Notice. October 30, 1997 http://www.whitehouse.gov/omb/fedreg_1997 standards/

The Metabolic Syndrome
Metabolic Syndrome: Synomyms* • Hypertension-hyperglycemia-hyperuricemia syndrome • Syndrome X • Dysmetabolic syndrome X • Insulin resistance syndrome • Metabolic dyslipidemia • The Deadly Quartet (upper-body obesity, glucose intolerance, hypertriglyceridemia, and hypertension) • Civilization syndrome
* https://www.clinicalkey.com/topics/internal-medicine/metabolic-syndrome.html

The Metabolic Syndrome Metabolic Syndrome: web definition* (Insulin resistance syndrome, Syndrome X) MS is a name for a group of risk factors that occur together and increase the risk for coronary artery disease, stroke, and T2DM.
* http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0004546/#adam_007290.disease.causes

The Metabolic Syndrome
Metabolic Syndrome*: (Insulin resistance syndrome, Syndrome X) The two most important risk factors for MS are: • Extra weight around the middle and upper parts of the body (central obesity). The “apple-shaped”. • Insulin Resistance.
* http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0004546/#adam_007290.disease.causes

The Metabolic Syndrome
Metabolic Syndrome*:
* http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0004546/#adam_007290.disease.causes
Other risk factors include: 1. Aging 2. Genetic influences 3. Hormone changes 4. Lack of exercise Patients who have MS often have 2 other problems that can either cause the condition or make it worse: 1. Excess blood clotting 2. Abnormal levels of inflammation markers

Metabolic Syndrome IDF (International Diabetes Federation)
WHO
WHO Consultation. Definition, diagnosis and classification of diabetes mellitus and its complications. Geneva: World Health Organization, 1999:31-33. http://www.idf.org/metabolic-syndrome Executive Summary of the Third Report of the NCEP expert panel (ATPIII), JAMA June, 2001; 285;2486-2497.
• A quarter of the world’s adults have metabolic syndrome
• People with metabolic syndrome are: 1. Twice as likely to die from CHD 2. Three times as likely to have a heart attack or stroke compared with people without the syndrome

The Relationship Between Obesity, Insulin Resistance and Dyslipidemia
Adapted from Brunzell JD, et al. Diabetes Care. 1999(suppl 3) C210-C13
NCEP: Clinical Identification of the Metabolic Syndrome*
*Adapted from Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
ATP III Third Report of the Expert Panel on
Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults
(Adult Treatment Panel III)
Circulation January 27, 2004 vol. 109 no. 3433-438

NCEP: Clinical Identification of the Metabolic Syndrome*
Risk Factor Defining Measures
*Adapted from Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
• Abdominal obesity Waist circumference Men >40 in (>102 cm) Women >35 in (>88 cm)
• TG ³150 mg/dL
• HDL-C Men <40 mg/dL Women < 50 mg/dL
• Blood pressure ³130/³85 mm Hg
• Fasting glucose ³110 mg/dL

AACE Clinical Criteria for Diagnosis of the Insulin Resistance Syndrome*
Additional Defining Measures
*Circulation January 27, 2004 vol. 109 no. 3433-438 http://circ.ahajournals.org/content/109/3/433/T3.expansion.html
Other risk factors
Family history of T2DM, hypertension or CVD
Polycystic ovary syndrome
Sedentary lifestyle
Advancing age
Ethnic groups having high risk for T2DM or CVD
*Diagnosis depends on clinical judgment based on risk factors.

Metabolic Syndrome International Diabetes Federation, 2006
http://www.idf.org/webdata/docs/IDF_Meta_def_final.pdf
Raised triglycerides ≥ 150 mg/dL (1.7 mmol/L) or specific treatment for this lipid abnormality Reduced HDL cholesterol < 40 mg/dL (1.03 mmol/L) in males < 50 mg/dL (1.29 mmol/L) in females or specific treatment for this lipid abnormality Raised blood pressure systolic BP ≥ 130 or diastolic BP ≥ 85 mm Hg or treatment of previously diagnosed hypertension Raised fasting plasma glucose (FPG) ≥ 100 mg/dL (5.6 mmol/L), or previously diagnosed type 2 diabetes
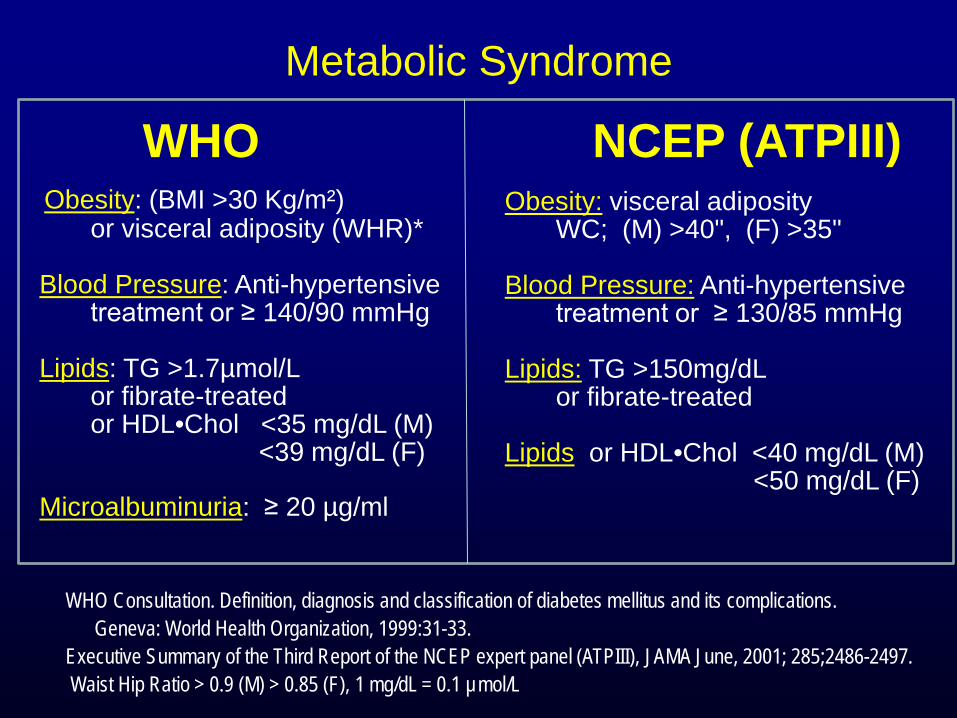
Metabolic Syndrome
WHO NCEP (ATPIII)
WHO Consultation. Definition, diagnosis and classification of diabetes mellitus and its complications. Geneva: World Health Organization, 1999:31-33. Executive Summary of the Third Report of the NCEP expert panel (ATPIII), JAMA June, 2001; 285;2486-2497. Waist Hip Ratio > 0.9 (M) > 0.85 (F), 1 mg/dL = 0.1 µmol/L
Obesity: (BMI >30 Kg/m²) or visceral adiposity (WHR)* Blood Pressure: Anti-hypertensive treatment or ≥ 140/90 mmHg Lipids: TG >1.7µmol/L or fibrate-treated or HDL•Chol <35 mg/dL (M) <39 mg/dL (F) Microalbuminuria: ≥ 20 µg/ml
Obesity: visceral adiposity WC; (M) >40", (F) >35" Blood Pressure: Anti-hypertensive treatment or ≥ 130/85 mmHg Lipids: TG >150mg/dL or fibrate-treated Lipids: or HDL•Chol <40 mg/dL (M) <50 mg/dL (F)

Marchesini, et al. Diabetes Med. April 2004:21; 383-387. n = 1569 consecutive subjects. • 65% of patients had A1c <8.0%, 58% on oral therapy and 3.8% on insulin
1569 Total patients 1113 71% Positive for both methods 183 12% Concordantly negative
Prevalence of the MS using two different proposals WHO vs. ATPIII
in Patients with T2DM

Metabolic Syndrome New IDF WORLDWIDE DEFINITION
OF THE METABOLIC SYNDROME: WHO
http://www.idf.org/metabolic-syndrome
• For a person to be defined as having the MS, the new definition Required they have central obesity, plus two of the following four additional factors: raised triglycerides (TG), reduced HDL-cholesterol, raised blood pressure or raised fasting plasma glucose level.
• Gender and, for the first time, ethnicity specific cut-off points for central obesity as measured by waist circumference were included.

1. For Japanese women and men the established cut points were changed:
>80cm in women (31.4 inches) >90cm in men (35.4 inches) 2. Waist Circumference: ATPIII >35 inches Female >40 inches Male
1. http://www.idf.org/metabolic-syndrome 2. Executive Summary of the Third Report of the NCEP expert panel (ATPIII), JAMA June, 2001; 285;2486-2497.
Metabolic Syndrome New IDF WORLDWIDE DEFINITION
OF THE METABOLIC SYNDROME: WHO

Age –Adjusted Prevalence of the Metabolic Syndrome by Race/Ethnicity Among US Adults
Adopted from Ford ES et al. JAMA. 2002;287:356-359.
20.3 21.623.8
31.9
0
5
10
15
20
25
30
35
Other A.A. White Mexican A.
% Prevalence

Insulin Resistance Syndrome in African Americans*
Additional Defining Measures
1. Ethn Dis. 2003 Fall;13(4):414-28.The Metabolic Syndrome in African Americans: 2. Ethn Dis. 2009 Spring;19(2 Suppl 2):S2-1-7.
Other risk factors
1. African-American women and Hispanic men and women have the highest prevalence of the Metabolic Syndrome.
2. The lower reported rates of metabolic syndrome in Blacks can be partly ascribed to the lower prevalent rates of some major components of metabolic syndrome, TG and HDL cholesterol levels.
The higher prevalence of HTN and CKD in Blacks suggests that the current classification, definition, and criteria for metabolic syndrome in Blacks needed to be reconsidered.
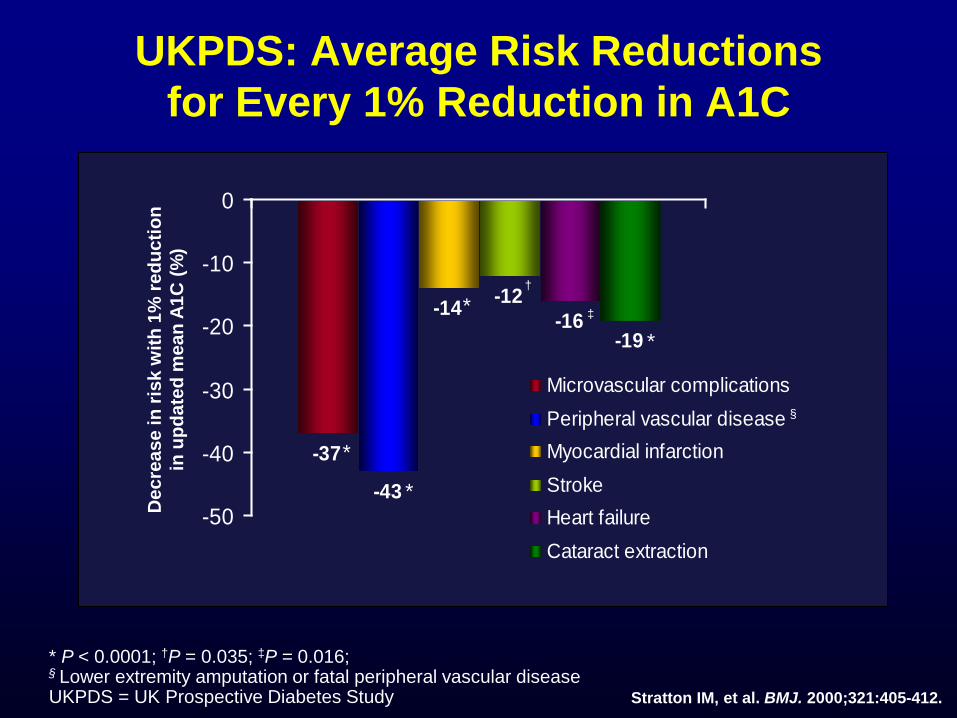
Stratton IM, et al. BMJ. 2000;321:405-412.
* P < 0.0001; †P = 0.035; ‡P = 0.016; § Lower extremity amputation or fatal peripheral vascular disease UKPDS = UK Prospective Diabetes Study
-37
-43
-14 -12-16
-19
-50
-40
-30
-20
-10
0
Microvascular complicationsPeripheral vascular diseaseMyocardial infarctionStrokeHeart failureCataract extraction
Dec
reas
e in
risk
with
1%
red
uctio
n
in u
pdat
ed m
ean
A1C
(%)
‡
§
†
*
*
*
*
UKPDS: Average Risk Reductions for Every 1% Reduction in A1C

Management of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Approach
Position Statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ANTI-HYPERGLYCEMIC THERAPY
• Glycemic targets - HbA1c < 7.0% (mean PG ~150-160 mg/dl [8.3-8.9
mmol/l]) - Pre-prandial PG <130 mg/dl (7.2 mmol/l) - Post-prandial PG <180 mg/dl (10.0 mmol/l) - Individualization is key: Ø Tighter targets (6.0 - 6.5%) - younger, healthier Ø Looser targets (7.5 - 8.0%+) - older, comorbidities,
hypoglycemia prone, etc. - Avoidance of hypoglycemia

Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]


§ ↑ Insulin Release
§ ↓ Gluconeogenesis & “IR”
§ Insulin Sensitizers
§ Delay glucose absorption
§ β-cell and non β-cell effects
§ Inhibit DPP IV = ↑ Native GLP-1
§ Suppress glucagon/+satiety
Pharmacologic Effect on Glycemic Control: Reduction in A1c
(Data Based On Clinical Trials/PI information)
Drug Class Mode of Action
§ Sulfonylureas/Meglitinides
§ Metformin
§ Thiazolidinediones
§ Alpha-glucosidase inhibitors
§ Incretin Mimetics
§ DPP IV Inhibitors
§ Amylin analog

§ Bind bile acids ¯ Hepatic glucose production § ↑ Glucose loss in the urine (↓ Blood pressure) (↓ Weight)
Pharmacologic Effect on Glycemic Control: Reduction in A1c
(Data Based On Clinical Trials/PI information)
Drug Class Mode of Action
§ Bile acid sequestrans
§ SGLT-2 Antagonist “Glucuretics”

Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
OTHER CONSIDERATIONS • Sex/ethnic/racial/genetic differences
- MODY & other monogenic forms of diabetes - Latinos: more insulin resistance - East Asians: more beta cell dysfunction - Gender may drive concerns about adverse effects
(e.g., bone loss from TZDs)

Projected Increase in the US Population with Diagnosed Diabetes by 2020 by Ethnicity
Projected Increase (%)
Adapted from American Diabetes Association. Diabetes Care. 2003;26:917-932.
0
20
40
60
80
100
120
Non Latino Whites Non Latino Blacks Latinos

• US healthcare system, costs of diabetes treatment increased from $174 billion in 2007 to $245 billion in 2012.¹
• Projected increase to $333 billion by 2034.²
• Hispanic/Latino population is the largest and fastest growing minority group in the US, with an annual national growth rate of 3.2%.
• By 2050, Latinos may constitute up to 30% of the US population.³
Diabetes Health Disparities in the Latino Population
1. Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008;31:569-615,
http://www.diabetes.org/advocate/resources/cost-of-diabetes.html (70% increase in 5 years 2007 to 2012) 2. Huang ES, et al. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care
2009;32:2225-9
3. US Census Bureau. Facts for Features – Hispanic Heritage Month 2009. CB09-FF17 Updated Sept 14, 2009. Available at: http://www.censusgov/newsroom/releases/archives/facts_for_features_special_editions/cb09-ff17html

Total per-capita health care expenditures are: 1. Lower among Hispanics ($5,930) 2. Higher among non-Hispanic blacks ($9,540) 3. vs. Non-Hispanic whites ($8,101). Non-Hispanic blacks also have 75% more emergency department visits than the population with diabetes as a whole.
Diabetes Health Disparities in the Ethnic Populations¹
1. http://www.diabetes.org/advocate/resources/cost-of-diabetes.html (70% increase in 5 years 2007 to 2012) March 6,
2013 press release.

Compared to non-Hispanic whites: 1. Per capita hospital inpatient costs are 41.3% higher among non-Hispanic blacks 2. 25.8% lower among Hispanics.
Diabetes Health Disparities in the Ethnic Populations¹
1. http://www.diabetes.org/advocate/resources/cost-of-diabetes.html (70% increase in 5 years 2007 to 2012) March 6,
2013 press release.

• Are at increased risk for obesity and T2DM compared with Whites.¹
• Develop diabetes at younger ages and with lower BMI.¹
• Age-adjusted prevalence of diabetes in 2006 was 16% in Mexican American adults compared with 9% in non-Latino Whites.²
• Higher prevalence of metabolic syndrome and adolescent diabetes.³
Diabetes Health Disparities in the Latino Population
1. Sanchez-Castillo CP, et al. Anthropometric cutoff points for predicting chronic diseases in the Mexican National Health
Survey 2000. Obes Res 2003;11:442-451 2. Huang ES, et al. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care
2009;32:2225-9
3. Lawrence JM, et al. Diabetes in Hispanic American youth: prevalence, incidence, demographics, and clinical characteristics: the SEARCH for Diabetes in Youth Study. Diabetes Care 2009;32(Suppl.2)s123-32

Diabetes Related complications: Cultural or genetic factors may contribute to an increased risk of developing diabetic complications.*
1. KPNC: despite insurance coverage the incidence of ESRD was significantly higher in Latinos.*
2. Latinos: less active lifestyle and higher proportion of dietary fat.¹ ² ׳
3. Greater propensity for IR.³
Diabetes Health Disparities in the Latino Population
*Karter AJ, et al. Ethnic disparities in diabetic complications in an insured population. JAMA 2002;287:2517-27 (KPNC
62K pts w DM) 1. Crespo CJ, et al. Acculturation and leisure-time physical inactivity in Mexican American adults: results from NHANES III,
1988-1994. Am J Pub Health 2001;91:1254-7
2. Unger JB, et al. Acculturation, physical activity, and fast-food consumption among Asian-American and Hispanic adolescents. J Community Health 2004;29:467-81
3. Haffner SM, et al. Increased insulin resistance and insulin secretion in nondiabetic African-Americans and Hispanics
compared with non-Hispanic whites. The Insulin Resistance Atherosclerosis Study. Diabetes 1996;45:742-8

Diabetes Health Disparities in the Latino Population The Insulin Resistance Atherosclerosis Study (IRAS)
Bond DE, et al. Diabetes Care. 2003; 26(4);1040-1046.
• Purpose - The healthcare treatment of non-Latino whites was compared with healthcare treatment of Latinos and African-Americans with T2DM and its complications • Population - Data from the IRAS study (1993-1998), N=452 • Results - Latinos and AA were as likely to receive treatment for their diabetes HTN, hyperlipidemia, albuminuria, and CAD as non-Latino whites. - Latinos and AA were more likely to have poorly controlled diabetes and HTN compared to non-Latino whites

Trends in T2DM Prevalence in High-Risk Populations:
Retrospective Analysis of >2000 patients
Prevalence of Diabetes
11% NHW
21% AA
29% Hispanic
Ness. et. al.Coron Artery Dis.1999,July;10(5):343-346 #2769 Mount Sinai School of Medicine, New York Academic hospital based geriatric practice mean age 80 ±8 years. NHW= non-Hispanic white, AA= African-American
19% NHW 33% AA 66% Hispanic
A1c >7%

• Meta-analysis reported HbA1c values for Latinos 0.5% higher than non-Latinos Whites.¹
• Data from NHANES reported a higher proportion of Latinos with “severely elevated” HbA1c levels. ² Latinos: >10% had an HbA1c >11% Whites: 1.7% had an HbA1c >11%
• Data from NHANES showed that roughly 62% of Latinos with diabetes were above the ADA target of <7% HbA1c
Diabetes Health Disparities in the Latino Population
1. Kirk Jk, et al. Disparities in A1C levels between Hispanic and non-Hispanic white adults with diabetes: a meta-analysis.
Diabetes Care 2008;31:240-6 2. Boltri JM, et al. Hemoglobin A1c levels in diagnosed and undiagnosed black, Hispanic, and white persons with diabetes:
results from NHANES 1999-2000. Ethn Dis 2005;15:562-7

• Despite the higher prevalence of obesity and risk factors for CV disease in the Latino population, Latinos have a LOWER risk of CV-related mortality. “Hispanic Paradox”¹ ³ ־
• Not all studies report similar findings of reduced CV mortality risk (Diabetes Care, Obesity and Am J Epidemiol)
• ↑ Retinopathy
• ↑ Amputation
• Higher incidence of failed Lower extremity bypass surgery leading to amputations despite NO difference in PVD
Diabetes Health Disparities in the Latino Population
1. Howard G, et al. Ethnic differences in stroke mortality between non-Hispanic whites, Hispanic whites, and blacks. The
National Longitudinal Mortality Study. Stroke 1994;25:2120-5 2. Wild SH, et al. Mortality from coronary heart disease and stroke for six ethnic groups in California. 1985 to 1990. Ann
Epidemiol 1995;5:432-9
3. Liao Y, et al. Mortality from coronary heart disease and cardiovascular disease among adult U.S. Hispanics. Findings from the National Health Inteview Survery(1986 to 1994). J Am Coll Cardiol 1997; 3-:1200-5

Education and Lifestyle Changes The Home and Cultural Environments may pose challenges that are unique for Latinos.¹
• Reluctance to part with traditional foods • Intolerance to foods • Feeling pressure from family/friends to eat during family events or holidays • Lack of facilities for exercise, sidewalks in certain neighborhoods.
Diabetes Health Disparities in the Latino Population What can be done?
1. Brown SA, et al. Culturally competent diabetes self-management education for Mexican Americans; the Starr County
border health initiative. Diabetes Care 2002;25:259-68

The Practitioner: • Minority patients don’t care about their health. • Biomedicine is right. • Science is the only basis for practice. • Traditional beliefs should be changed rather than built upon. • People will follow directions given by health practitioners. • Adherence failure is the patient’s problem.
Diabetes Health Disparities in the Latino Population What can be done?
Cultural Barriers and Opportunities¹
1. Adapted from Tripp-Reimer T, et al. Diabetes Spectrum 14; 13-22, 2001

• Ethnic differences in appointment keeping may be an important factor in poor health outcomes among Latino and African American patients with diabetes
• Survey of data and medical records for nearly 13,000 participants in the NIH-funded Diabetes Study of Northern California (DISTANCE) found that some minorities missed scheduled appointment with their primary care providers twice as often as others
• Latinos and African-Americans had the lowest rates
Diabetes Health Disparities in the Latino Population What can be done?
Cultural Barriers and Opportunities, the office visit¹
1. Health Services Research Health Behavior News Service 1. http://www.cfah.org/hbns/archives/getDocument.cfm?documentID=22448

The Actions, Attitudes and Beliefs of the Healthcare Team Can Strongly Influence Treatment
“The success of culturally tailored aspects of care, such as inclusion of peer educators and communications in Spanish, are … important in the physician-patient Relationship.” *
* Gonzalez, AB, et al. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Curr
Med Research & Opinion.27;5:969-79 1. Brown, SA, et al. Culturally competent diabetes education for Mexican Americans: the Star County Study, The Diabetes
Educator 1999;25:226-36
2. Metghalchi S, et al. Improved clinical outcomes using a culturally sensitive diabetes education program in a Hispanic population. Diabetes Educ 200;34:698-706
• Culturally sensitive health education programs have proven beneficial for Latinos with diabetes, particularly when community health workers are included and when meetings are conducted in Spanish. ¹ ² ׳

Culturally Competent Management The Centers for Disease Control Racial and Ethnic Approaches to Community Health (REACH) program. ¹
• Designed to eliminate racial and ethnic health disparities in 8 disease states including diabetes.
• Utilized trained community residents to deliver 5 monthly 2-hr group meetings on healthy lifestyle modifications
• Demonstrated efficacy of community-based programs that provide culturally sensitive care to Latino patients.
•
•
Diabetes Health Disparities in the Latino Population
1. Racial and Ethnic Approaches to Community Health. Available at http://www.cdc.gov/reach/index .htm (last accessed
May 6 2012 2. Gilmer TP, et al. Outcomes of Project Dulce: a culturally specific diabetes management program. Ann Pharmacother
2005;39:817-22

Culturally Competent Management Verbal and nonverbal communication and personal interaction may play an important role in how Latino patients respond to healthcare professionals.¹
• Respect, sympathy in interpersonal relationships between Latinos and HCPs have demonstrated reductions in HbA1c of up to 0.8% (Project Dulce).²
Diabetes Health Disparities in the Latino Population
1. Flores G. Culture and the patient-physician relationship: achieving cultural competency in health care. J Pediatr
2002;134:14-23 2. Gilmer TP, et al. Outcomes of Project Dulce: a culturally specific diabetes management program. Ann Pharmacother
2005;39:817-22

Health Perspectives of Some Latino Persons With Diabetes
¹Lipton RB,et al. Diabetes Educ. 1998;24(1):67-71
²Caballero AE. Curr Diab Rep. 2005;5(3):217-225
• Patients may not take their diabetes seriously until they develop complications.¹ (Machismo²)
• Patients may feel that treating diabetes is hopeless, or that their diabetes is an act of God.¹ (Fatalismo²)
• Language difficulty is more of a barrier that economics.¹
• Alternative treatments are often used-but the clinician won’t know unless he/she asks.¹
• Stories/recommendations from family and friends strongly influence patient behavior.¹ (Familismo/Comadre²)

The Perspectives of Some Latino Persons with Diabetes
Strong family dynamics • Positive - Families often come as a group to the office visit
- Enhances adherence to regimen
- Family provides valuable emotional support • Challenges - Women with diabetes may have family obligations which may hinder self-care
- The belief that the woman’s needs are secondary to the good of her family (fatalismo)
- Costs of medications and supplies were considered less important than the family needs.
Lipton RB. et al. Diabetes Educ. 1998;24(1);67-71

The Attitudes and Beliefs of Physicians and the Healthcare Team Can Strongly Influence Treatment
Recommendations
- Personalize the relationship • Ask questions • Respect your patient’s needs • Create an alliance with the patient and family
- Consider employing Spanish-speaking staff
- Obtain bilingual diabetes educational materials
- Prescribe diabetes education when possible • (CDE certified nurses and dietitians)

Management with Education and Lifestyle Changes The DPP evaluated lifestyle intervention on lowering the risk of developing DM which included 16% Latinos.
• Latino men and women lost a mean of 7.8% and 7.1% of body weight, respectively in the intensive lifestyle modification group Similar finding of weight loss were reported in other studies, (Look AHEAD trial).²
Diabetes Health Disparities in the Latino Population
1. West DS, et al. Weight loss of black, white and Hispanic men and women in the Diabetes Prevention Project Program.
Obesity 2008;16:1413-20 2. Wadden TA, et al. One-year weight losses in the Look AHEAD study; factors associated with success. Obesity
2009;17:713-22

Diabetes Health Disparities When dealing with the elderly Latino, remember-
“Respeto”*
• In dress and demeanor
• Address in respectful manner
• Do not ignore elder
• Explain without appearing condescending
*Espino, David, Oakes, Lilliana,” Health care for the Hispanic elder patient” ,Caring for Hispanic Patients,2004.

Diabetes Health Disparities When dealing with the elderly Latino, remember-
“Familia” (family)
• Allow for family members or friends to be present during the office visit
• Be sensitive to family dynamic but allow the patient to express themselves
*Espino, David, Oakes, Lilliana,” Health care for the Hispanic elder patient” ,Caring for Hispanic Patients,2004.

Summary: Metabolic Syndrome, Diabetes and the impact on ethnic populations.
• There are various and differing criteria for MS but they include obesity plus several clinical risk factors including BP, Lipids, glycemia and ethnic components. • Some Ethnic populations have a higher prevalence of MS
• Ethnic populations reflect higher (non-Hispanic blacks ) as well as lower (Hispanic) costs for US health care expenditure per capita compared to Non Hispanic whites. (2013 ADA) • There are number of different classes of medications to treat T2DM, two classes (TZD’s and Metformin) specifically address Insulin Resistance

Summary: Metabolic Syndrome, Diabetes and the impact on ethnic populations.
• Glycemic targets & BG-lowering therapies must be individualized.
• Cultural and/or genetic factors may contribute to an increased risk of developing diabetic and its complications
• There are unique cultural challenges in treating the Latino patient with diabetes.
• Culturally sensitive health education programs have proven beneficial for Latinos with diabetes.

Thank you
Questions…
