diabetes care - guidelines howto
DESCRIPTION
Guidelines for the Management of Diabetes including diagnosis criteria, treatment, monitoring, goals, and long-term care.TRANSCRIPT

Standards ofMedical Care inDiabetesd2013AMERICAN DIABETES ASSOCIATION
D iabetes mellitus is a chronic illnessthat requires continuing medical careand ongoing patient self-management
education and support to prevent acutecomplications and to reduce the risk oflong-term complications. Diabetes care iscomplex and requires multifactorial riskreduction strategies beyond glycemic con-trol. A large body of evidence exists thatsupports a range of interventions to improvediabetes outcomes.
These standards of care are intendedto provide clinicians, patients, researchers,payers, and other interested individualswith the components of diabetes care,general treatment goals, and tools to eval-uate the quality of care. Although individ-ual preferences, comorbidities, and otherpatient factors may require modification ofgoals, targets that are desirable for mostpatients with diabetes are provided. Spe-cifically titled sections of the standardsaddress children with diabetes, pregnantwomen, and people with prediabetes.These standards are not intended to pre-clude clinical judgment or more extensiveevaluation and management of the patientby other specialists as needed. For moredetailed information about management ofdiabetes, refer to references (1–3).
The recommendations included arescreening, diagnostic, and therapeuticactions that are known or believed tofavorably affect health outcomes of patientswith diabetes. A large number of theseinterventions have been shown to be cost-effective (4). A grading system (Table 1),developed by the American Diabetes Asso-ciation (ADA) and modeled after existingmethods, was utilized to clarify and codifythe evidence that forms the basis for therecommendations. The level of evidencethat supports each recommendation islisted after each recommendation usingthe letters A, B, C, or E.
These standards of care are revisedannually by the ADA’s multidisciplinaryProfessional Practice Committee, incor-porating new evidence. For the currentrevision, committee members systemati-cally searched Medline for human stud-ies related to each subsection andpublished since 1 January 2011. Recom-mendations (bulleted at the beginningof each subsection and also listed inthe “Executive Summary: Standards ofMedical Care in Diabetesd2013”) wererevised based on new evidence or, insome cases, to clarify the prior recom-mendation or match the strength of thewording to the strength of the evidence.A table linking the changes in recom-mendations to new evidence can be re-viewed at http://professional.diabetes.org/CPR. As is the case for all positionstatements, these standards of care werereviewed and approved by the ExecutiveCommittee of ADA’s Board of Directors,which includes health care professionals,scientists, and lay people.
Feedback from the larger clinicalcommunity was valuable for the 2013revision of the standards. Readers whowish to comment on the “Standards ofMedical Care in Diabetesd2013” areinvited to do so at http://professional.diabetes.org/CPR.
Members of the Professional PracticeCommittee disclose all potential finan-cial conflicts of interest with industry.These disclosures were discussed at theonset of the standards revision meeting.Members of the committee, their em-ployer, and their disclosed conflicts ofinterest are listed in the “ProfessionalPractice Committee for the 2013 ClinicalPractice Recommendations” table (seep. S109). The ADA funds developmentof the standards and all its position state-ments out of its general revenues and
does not use industry support for thesepurposes.
I. CLASSIFICATION ANDDIAGNOSIS
A. ClassificationThe classification of diabetes includesfour clinical classes:
c Type 1 diabetes (results from b-celldestruction, usually leading to absoluteinsulin deficiency)
c Type 2 diabetes (results from a pro-gressive insulin secretory defect on thebackground of insulin resistance)
c Other specific types of diabetes due toother causes, e.g., genetic defects inb-cell function, genetic defects in in-sulin action, diseases of the exocrinepancreas (such as cystic fibrosis), anddrug- or chemical-induced (such as inthe treatment of HIV/AIDS or after or-gan transplantation)
c Gestational diabetes mellitus (GDM)(diabetes diagnosed during pregnancythat is not clearly overt diabetes)
Some patients cannot be clearly clas-sified as type 1 or type 2 diabetic. Clinicalpresentation and disease progression varyconsiderably in both types of diabetes.Occasionally, patients who otherwisehave type 2 diabetes may present withketoacidosis. Similarly, patients with type1 diabetes may have a late onset and slow(but relentless) progression of diseasedespite having features of autoimmunedisease. Such difficulties in diagnosis mayoccur in children, adolescents, andadults. The true diagnosis may becomemore obvious over time.
B. Diagnosis of diabetesFor decades, the diagnosis of diabetes wasbased on plasma glucose criteria, eitherthe fasting plasma glucose (FPG) or the2-h value in the 75-g oral glucose toler-ance test (OGTT) (5).
In 2009, an International ExpertCommittee that included representativesof the ADA, the International Diabetes
c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c
Originally approved 1988. Most recent review/revision October 2012.DOI: 10.2337/dc13-S011© 2013 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and thework is not altered. See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S11
P O S I T I O N S T A T E M E N T
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Federation (IDF), and the EuropeanAssociation for the Study of Diabetes(EASD) recommended the use of the A1Ctest to diagnose diabetes, with a thresholdof $6.5% (6), and the ADA adopted thiscriterion in 2010 (5). The diagnostic testshould be performed using a method thatis certified by the NGSP and standardizedor traceable to the Diabetes Control andComplications Trial (DCCT) reference as-say. Although point-of-care (POC) A1C as-says may be NGSP certified, proficiencytesting is not mandated for performingthe test, so use of these assays for diagnosticpurposes could be problematic.
Epidemiological datasets show a sim-ilar relationship for A1C to the risk ofretinopathy as has been shown for thecorresponding FPG and 2-h PG thresh-olds. The A1C has several advantages tothe FPG and OGTT, including greaterconvenience (since fasting is not required),evidence to suggest greater preanalyticalstability, and less day-to-day perturbationsduring periods of stress and illness. Theseadvantages must be balanced by greatercost, the limited availability of A1C testingin certain regions of the developing world,and the incomplete correlation betweenA1C and average glucose in certain indi-viduals. In addition, HbA1c levels may varywith patients’ race/ethnicity (7,8). Some
have posited that glycation rates differ byrace (with, for example, African Americanshaving higher rates of glycation), but this iscontroversial. A recent epidemiologicalstudy found that, when matched for FPG,African Americans (with and without dia-betes) indeed had higher A1C than whites,but also had higher levels of fructosamineand glycated albumin and lower levels of1,5 anhydroglucitol, suggesting that theirglycemic burden (particularly postpran-dially) may be higher (9). Epidemiologicalstudies forming the framework for recom-mending use of the A1C to diagnose diabe-tes have all been in adult populations.Whether the cut point would be the sameto diagnose children or adolescents withtype 2 diabetes is an area of uncertainty(3,10). A1C inaccurately reflects glycemiawith certain anemias and hemoglobinopa-thies. For patients with an abnormal hemo-globin but normal red cell turnover, such assickle cell trait, an A1C assay without inter-ference fromabnormal hemoglobins shouldbe used (an updated list is available at www.ngsp.org/interf.asp). For conditions withabnormal red cell turnover, such as preg-nancy, recent blood loss or transfusion, orsome anemias, the diagnosis of diabetesmust employ glucose criteria exclusively.
The established glucose criteria forthe diagnosis of diabetes (FPG and 2-h
PG) remain valid as well (Table 2). Just asthere is less than 100% concordance be-tween the FPG and 2-h PG tests, there isno perfect concordance between A1C andeither glucose-based test. Analyses of theNational Health and Nutrition Examina-tion Survey (NHANES) data indicate that,assuming universal screening of the un-diagnosed, the A1C cut point of $6.5%identifies one-third fewer cases of undiag-nosed diabetes than a fasting glucose cutpoint of$126 mg/dL (7.0 mmol/L) (11),and numerous studies have confirmedthat at these cut points the 2-h OGTTvalue diagnoses more screened peoplewith diabetes (12). However, in practice, alarge portion of the diabetic population re-mains unaware of its condition. Thus, thelower sensitivity of A1C at the designatedcut point may well be offset by the test’sgreater practicality, and wider applicationof a more convenient test (A1C) may actu-ally increase the number of diagnosesmade.
As with most diagnostic tests, a testresult diagnostic of diabetes should berepeated to rule out laboratory error,unless the diagnosis is clear on clinicalgrounds, such as a patient with a hyper-glycemic crisis or classic symptoms ofhyperglycemia and a random plasmaglucose $200 mg/dL. It is preferablethat the same test be repeated for confir-mation, since there will be a greater likeli-hood of concurrence in this case. Forexample, if the A1C is 7.0% and a repeatresult is 6.8%, the diagnosis of diabetes isconfirmed. However, if two different tests(such as A1C and FPG) are both above thediagnostic thresholds, the diagnosis of di-abetes is also confirmed.
On the other hand, if two differenttests are available in an individual and theresults are discordant, the test whose resultis above the diagnostic cut point should berepeated, and the diagnosis is made basedon the confirmed test. That is, if a patientmeets the diabetes criterion of the A1C (tworesults$6.5%) but not the FPG (,126mg/dL or 7.0 mmol/L), or vice versa, that per-son should be considered to have diabetes.
Since there is preanalytical and ana-lytical variability of all the tests, it is alsopossible that when a test whose result wasabove the diagnostic threshold is re-peated, the second value will be belowthe diagnostic cut point. This is leastlikely for A1C, somewhat more likely forFPG, and most likely for the 2-h PG.Barring a laboratory error, such patientsare likely to have test results near themargins of the threshold for a diagnosis.The health care professional might opt to
Table 1dADA evidence grading system for clinical practice recommendations
Level ofevidence Description
A Clear evidence from well-conducted, generalizable RCTs that are adequatelypowered, including:c Evidence from a well-conducted multicenter trialc Evidence from a meta-analysis that incorporated quality ratings in theanalysis
Compelling nonexperimental evidence, i.e., “all or none” rule developed by theCentre for Evidence-Based Medicine at the University of Oxford
Supportive evidence from well-conducted RCTs that are adequately powered,including:c Evidence from a well-conducted trial at one or more institutionsc Evidence from ameta-analysis that incorporated quality ratings in the analysis
B Supportive evidence from well-conducted cohort studiesc Evidence from a well-conducted prospective cohort study or registryc Evidence from a well-conducted meta-analysis of cohort studies
Supportive evidence from a well-conducted case-control studyC Supportive evidence from poorly controlled or uncontrolled studies
c Evidence from randomized clinical trials with one or more major or three ormore minor methodological flaws that could invalidate the results
c Evidence from observational studies with high potential for bias (such as caseseries with comparison with historical controls)
c Evidence from case series or case reportsConflicting evidence with the weight of evidence supporting the recommendation
E Expert consensus or clinical experience
S12 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

follow the patient closely and repeat thetesting in 3–6 months.
The current diagnostic criteria fordiabetes are summarized in Table 2.
C. Categories of increased riskfor diabetes (prediabetes)In 1997 and 2003, the Expert Committeeon Diagnosis and Classification of Diabe-tes Mellitus (13,14) recognized an inter-mediate group of individuals whoseglucose levels, although not meeting cri-teria for diabetes, are nevertheless toohigh to be considered normal. These per-sons were defined as having impaired fast-ing glucose (IFG) (FPG levels 100 mg/dL[5.6 mmol/L] to 125 mg/dL [6.9 mmol/L])or impaired glucose tolerance (IGT) (2-hvalues in the OGTT of 140 mg/dL [7.8mmol/L] to 199 mg/dL [11.0 mmol/L]). Itshould be noted that the World HealthOrganization (WHO) and a number ofother diabetes organizations define the cut-off for IFG at 110 mg/dL (6.1 mmol/L).
Individuals with IFG and/or IGT havebeen referred to as having prediabetes,indicating the relatively high risk for thefuture development of diabetes. IFG andIGT should not be viewed as clinicalentities in their own right but rather riskfactors for diabetes aswell as cardiovasculardisease (CVD). IFG and IGT are associatedwith obesity (especially abdominal or vis-ceral obesity), dyslipidemia with high tri-glycerides and/or lowHDL cholesterol, andhypertension.
As is the case with the glucose mea-sures, several prospective studies that
used A1C to predict the progression todiabetes demonstrated a strong, continu-ous association between A1C and sub-sequent diabetes. In a systematic review of44,203 individuals from 16 cohort stud-ies with a follow-up interval averaging 5.6years (range 2.8–12 years), those with anA1C between 5.5 and 6.0% had a substan-tially increased risk of diabetes with 5-yearincidences ranging from 9 to 25%. An A1Crange of 6.0–6.5% had a 5-year risk of de-veloping diabetes between 25 to 50% andrelative risk (RR) 20 times higher comparedwith anA1Cof 5.0% (15). In a community-based study of black and white adultswithout diabetes, baseline A1C was astronger predictor of subsequent diabetesand cardiovascular events than was fast-ing glucose (16). Other analyses suggestthat an A1C of 5.7% is associated withdiabetes risk similar to that in the high-risk participants in the Diabetes PreventionProgram (DPP) (17).
Hence, it is reasonable to consider anA1C range of 5.7–6.4% as identifying in-dividuals with prediabetes. As is the casefor individuals found to have IFG andIGT, individuals with an A1C of 5.7–6.4%should be informed of their increased riskfor diabetes as well as CVD and counseledabout effective strategies to lower their risks(see Section IV). As with glucose measure-ments, the continuum of risk is curvilinear,so that as A1C rises, the risk of diabetes risesdisproportionately (15). Accordingly, inter-ventions should be most intensive andfollow-up particularly vigilant for thosewith A1Cs above 6.0%,who should be con-sidered to be at very high risk.
Table 3 summarizes the categories ofprediabetes.
II. TESTING FOR DIABETES INASYMPTOMATIC PATIENTS
Recommendationsc Testing to detect type 2 diabetes andprediabetes in asymptomatic peopleshould be considered in adults of anyage who are overweight or obese (BMI$25 kg/m2) and who have one or moreadditional risk factors for diabetes (Table4). In those without these risk factors,testing should begin at age 45. (B)
c If tests are normal, repeat testing at leastat 3-year intervals is reasonable. (E)
c To test for diabetes or prediabetes, theA1C, FPG, or 75-g 2-h OGTT are appro-priate. (B)
c In those identified with prediabetes,identify and, if appropriate, treat otherCVD risk factors. (B)
Formany illnesses, there is a major dis-tinction between screening and diagnostictesting. However, for diabetes, the sametests would be used for “screening” as fordiagnosis. Diabetes may be identified any-where along a spectrum of clinical scenar-ios ranging from a seemingly low-riskindividual who happens to have glucosetesting, to a higher-risk individual whomthe provider tests because of high suspicionof diabetes, to the symptomatic patient.The discussion herein is primarily framedas testing for diabetes in those withoutsymptoms. The same assays used for test-ing for diabetes will also detect individualswith prediabetes.
A. Testing for type 2 diabetes andrisk of future diabetes in adultsPrediabetes and diabetes meet establishedcriteria for conditions in which early de-tection is appropriate. Both conditions arecommon, increasing in prevalence, andimpose significant public health burdens.There is a long presymptomatic phasebefore the diagnosis of type 2 diabetes isusually made. Relatively simple tests areavailable to detect preclinical disease. Ad-ditionally, the duration of glycemic burdenis a strong predictor of adverse outcomes,and effective interventions exist to preventprogression of prediabetes to diabetes (seeSection IV) and to reduce risk of compli-cations of diabetes (see Section VI).
Type 2 diabetes is frequently not di-agnosed until complications appear, andapproximately one-fourth of all peoplewith diabetes in the U.S. may be undiag-nosed. The effectiveness of early identifica-tion of prediabetes and diabetes throughmass testing of asymptomatic individualshas not been proven definitively, andrigorous trials to provide such proof areunlikely to occur. In a large randomizedcontrolled trial (RCT) in Europe, generalpractice patients between the ages of 40–69 years were screened for diabetes and
Table 2dCriteria for the diagnosis ofdiabetes
A1C$6.5%. The test should be performed ina laboratory using a method that is NGSPcertified and standardized to the DCCTassay.*
ORFPG $126 mg/dL (7.0 mmol/L). Fasting isdefined as no caloric intake for at least 8 h.*
OR2-h plasma glucose$200mg/dL (11.1mmol/L)during an OGTT. The test should beperformed as described by the WHO, usinga glucose load containing the equivalent of75 g anhydrous glucose dissolved in water.*
ORIn a patient with classic symptoms ofhyperglycemia or hyperglycemic crisis,a random plasma glucose $200 mg/dL(11.1 mmol/L).
*In the absence of unequivocal hyperglycemia, re-sult should be confirmed by repeat testing.
Table 3dCategories of increased risk fordiabetes (prediabetes)*
FPG 100 mg/dL (5.6 mmol/L) to 125 mg/dL(6.9 mmol/L) (IFG)
OR2-h plasmaglucose in the 75-gOGTT140mg/dL(7.8 mmol/L) to 199 mg/dL (11.0 mmol/L)(IGT)
ORA1C 5.7–6.4%
*For all three tests, risk is continuous, extending be-low the lower limit of the range and becoming dis-proportionately greater at higher ends of the range.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S13
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

then randomly assigned by practice toroutine care of diabetes or intensive treat-ment of multiple risk factors. After 5.3years of follow-up, CVD risk factors weremodestly but significantly more improvedwith intensive treatment. Incidence of firstCVD event and mortality rates were notsignificantly different between groups(18). This study would seem to add sup-port for early treatment of screen-detecteddiabetes, as risk factor control was excel-lent even in the routine treatment armand both groups had lower event ratesthan predicted. The absence of a controlunscreened arm limits the ability to defi-nitely prove that screening impacts out-comes. Mathematical modeling studiessuggest that screening independent ofrisk factors beginning at age 30 yearsor age 45 years is highly cost-effective(,$11,000 per quality-adjusted life-year gained) (19).
Recommendations for testing for di-abetes in asymptomatic, undiagnosedadults are listed in Table 4. Testing shouldbe considered in adults of any age withBMI $25 kg/m2 and one or more of theknown risk factors for diabetes. In addi-tion to the listed risk factors, certain med-ications, such as glucocorticoids andantipsychotics (20), are known to in-crease the risk of type 2 diabetes. Thereis compelling evidence that lower BMI cutpoints suggest diabetes risk in some racialand ethnic groups. In a large multiethniccohort study, for an equivalent incidencerate of diabetes conferred by a BMI of 30kg/m2 in whites, the BMI cutoff value was
24 kg/m2 in South Asians, 25 kg/m2 inChinese, and 26 kg/m2 in African Ameri-cans (21). Disparities in screening rates,not explainable by insurance status, arehighlighted by evidence that despitemuch higher prevalence of type 2 diabe-tes, non-Caucasians in an insured popu-lation are no more likely than Caucasiansto be screened for diabetes (22). Becauseage is a major risk factor for diabetes, test-ing of those without other risk factorsshould begin no later than age 45 years.
The A1C, FPG, or the 2-h OGTT areappropriate for testing. It should be notedthat the tests do not necessarily detectdiabetes in the same individuals. Theefficacy of interventions for primary pre-vention of type 2 diabetes (23–29) hasprimarily been demonstrated among in-dividuals with IGT, not for individualswith isolated IFG or for individuals withspecific A1C levels.
The appropriate interval betweentests is not known (30). The rationalefor the 3-year interval is that false nega-tives will be repeated before substantialtime elapses, and there is little likelihoodthat an individual will develop significantcomplications of diabetes within 3 yearsof a negative test result. In the modelingstudy, repeat screening every 3 or 5 yearswas cost-effective (19).
Because of the need for follow-up anddiscussion of abnormal results, testingshould be carried out within the healthcare setting. Community screening outsidea health care setting is not recommendedbecause people with positive tests may not
seek, orhave access to, appropriate follow-uptesting and care. Conversely, there may befailure to ensure appropriate repeat testingfor individuals who test negative. Commu-nity screening may also be poorly targeted; i.e., it may fail to reach the groupsmost at riskand inappropriately test those at low risk (theworried well) or even those already diag-nosed.
B. Screening for type 2 diabetesin childrenRecommendationsc Testing to detect type 2 diabetes andprediabetes should be considered in chil-dren and adolescents who are overweightand who have two or more additionalrisk factors for diabetes (Table 5). (E)
The incidence of type 2 diabetes inadolescents has increased dramatically inthe last decade, especially in minoritypopulations (31), although the diseaseremains rare in the general pediatric pop-ulation (32). Consistent with recom-mendations for adults, children andyouth at increased risk for the presenceor the development of type 2 diabetesshould be tested within the health caresetting (33). The recommendations ofthe ADA consensus statement “Type 2Diabetes in Children and Adolescents,”with some modifications, are summa-rized in Table 5.
C. Screening for type 1 diabetesRecommendationsc Consider referring relatives of thosewith type 1 diabetes for antibody test-ing for risk assessment in the settingof a clinical research study. (E)
Generally, people with type 1 diabetespresent with acute symptoms of diabetesand markedly elevated blood glucoselevels, and some cases are diagnosed withlife-threatening ketoacidosis. Evidencefrom several studies suggests that mea-surement of islet autoantibodies in rela-tives of those with type 1 diabetesidentifies individuals who are at risk fordeveloping type 1 diabetes. Such testing,coupled with education about symptomsof diabetes and follow-up in an observa-tional clinical study, may allow earlieridentification of onset of type 1 diabetesand lessen presentation with ketoacidosisat time of diagnosis. This testing may beappropriate in those who have relativeswith type 1 diabetes, in the context of
Table 4dCriteria for testing for diabetes in asymptomatic adult individuals
1. Testing should be considered in all adults who are overweight (BMI $25 kg/m2*)and have additional risk factors:
c physical inactivityc first-degree relative with diabetesc high-risk race/ethnicity (e.g., African American, Latino, Native American, Asian
American, Pacific Islander)c women who delivered a baby weighing .9 lb or were diagnosed with GDMc hypertension ($140/90 mmHg or on therapy for hypertension)c HDL cholesterol level ,35 mg/dL (0.90 mmol/L) and/or a triglyceride
level .250 mg/dL (2.82 mmol/L)c women with polycystic ovary syndromec A1C $5.7%, IGT, or IFG on previous testingc other clinical conditions associated with insulin resistance (e.g., severe obesity,
acanthosis nigricans)c history of CVD
2. In the absence of the above criteria, testing for diabetes should begin at age 45 years.3. If results are normal, testing should be repeated at least at 3-year intervals, with
consideration of more frequent testing depending on initial results (e.g., those withprediabetes should be tested yearly) and risk status.
*At-risk BMI may be lower in some ethnic groups.
S14 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

clinical research studies (see, for example,http://www.diabetestrialnet.org). However,widespread clinical testing of asymptomaticlow-risk individuals cannot currently berecommended, as it would identify veryfew individuals in the general populationwho are at risk. Individuals who screenpositive should be counseled about theirrisk of developing diabetes and symptomsof diabetes, followed closely to prevent de-velopment of diabetic ketoacidosis, andinformed about clinical trials. Clinicalstudies are being conducted to test variousmethods of preventing type 1 diabetes inthose with evidence of autoimmunity.Some interventions have demonstratedmodest efficacy in slowing b-cell loss earlyin type 1 diabetes (34,35), and further re-search is needed to determine whetherthey may be effective in preventing type1 diabetes.
III. DETECTION ANDDIAGNOSIS OF GDM
Recommendationsc Screen for undiagnosed type 2 diabetesat the first prenatal visit in those withrisk factors, using standard diagnosticcriteria. (B)
c In pregnant women not previouslyknown to have diabetes, screen for
GDM at 24–28 weeks of gestation,using a 75-g 2-h OGTT and the di-agnostic cut points in Table 6. (B)
c Screen womenwith GDM for persistentdiabetes at 6–12 weeks postpartum,using the OGTT and nonpregnancydiagnostic criteria. (E)
c Women with a history of GDM shouldhave lifelong screening for the de-velopment of diabetes or prediabetes atleast every 3 years. (B)
c Women with a history of GDM foundto have prediabetes should receivelifestyle interventions or metformin toprevent diabetes. (A)
For many years, GDM was defined asany degree of glucose intolerance withonset or first recognition during preg-nancy (13), whether or not the conditionpersisted after pregnancy, and not ex-cluding the possibility that unrecognizedglucose intolerance may have antedatedor begun concomitantly with the preg-nancy. This definition facilitated a uniformstrategy for detection and classification ofGDM, but its limitations were recognizedfor many years. As the ongoing epidemicof obesity and diabetes has led to moretype 2 diabetes in women of childbearingage, the number of pregnant women withundiagnosed type 2 diabetes has increased(36). Because of this, it is reasonable to
screen women with risk factors for type2 diabetes (Table 4) for diabetes at theirinitial prenatal visit, using standard diag-nostic criteria (Table 2). Women with di-abetes found at this visit should receivea diagnosis of overt, not gestational,diabetes.
GDM carries risks for the mother andneonate. The Hyperglycemia and Ad-verse Pregnancy Outcome (HAPO) study(37), a large-scale (;25,000 pregnantwomen) multinational epidemiologicalstudy, demonstrated that risk of adversematernal, fetal, and neonatal outcomescontinuously increased as a function ofmaternal glycemia at 24–28 weeks, evenwithin ranges previously considered nor-mal for pregnancy. For most complica-tions, there was no threshold for risk.These results have led to careful recon-sideration of the diagnostic criteria forGDM. After deliberations in 2008–2009, the International Association ofDiabetes and Pregnancy Study Groups(IADPSG), an international consensusgroup with representatives frommultipleobstetrical and diabetes organizations,including ADA, developed revised rec-ommendations for diagnosing GDM.The group recommended that all womennot known to have prior diabetesundergo a 75-g OGTT at 24–28 weeksof gestation. Additionally, the group de-veloped diagnostic cut points for the fast-ing, 1-h, and 2-h plasma glucosemeasurements that conveyed an oddsratio for adverse outcomes of at least1.75 compared with women with themean glucose levels in the HAPO study.Current screening and diagnostic strate-gies, based on the IADPSG statement(38), are outlined in Table 6.
These new criteria will significantlyincrease the prevalence of GDM, primar-ily because only one abnormal value, nottwo, is sufficient to make the diagnosis.The ADA recognizes the anticipated sig-nificant increase in the incidence of GDMdiagnosed by these criteria and is sensitiveto concerns about the “medicalization” ofpregnancies previously categorized as nor-mal. These diagnostic criteria changes arebeing made in the context of worrisomeworldwide increases in obesity and diabe-tes rates, with the intent of optimizing ges-tational outcomes for women and theirbabies.
Admittedly, there are few data fromrandomized clinical trials regarding ther-apeutic interventions in women who willnow be diagnosed with GDM based ononly one blood glucose value above the
Table 5dTesting for type 2 diabetes in asymptomatic children*
Criteriac Overweight (BMI .85th percentile for age and sex, weight for height .85th percentile, orweight .120% of ideal for height)
Plus any two of the following risk factors:c Family history of type 2 diabetes in first- or second-degree relativec Race/ethnicity (Native American, African American, Latino, Asian American, PacificIslander)
c Signs of insulin resistance or conditions associated with insulin resistance (acanthosisnigricans, hypertension, dyslipidemia, polycystic ovary syndrome, or small-for-gestational-age birth weight)
c Maternal history of diabetes or GDM during the child’s gestationAge of initiation: age 10 years or at onset of puberty, if puberty occurs at a younger ageFrequency: every 3 years
*Persons aged 18 years and younger.
Table 6dScreening for and diagnosis of GDM
Perform a 75-g OGTT, with plasma glucose measurement fasting and at 1 and 2 h, at 24–28weeks of gestation in women not previously diagnosed with overt diabetes.
The OGTT should be performed in the morning after an overnight fast of at least 8 h.The diagnosis of GDM is made when any of the following plasma glucose values are exceeded:
c Fasting: $92 mg/dL (5.1 mmol/L)c 1 h: $180 mg/dL (10.0 mmol/L)c 2 h: $153 mg/dL (8.5 mmol/L)
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S15
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

specified cut points (in contrast to the oldercriteria that stipulated at least two abnor-mal values). However, there is emergingobservational and retrospective evidencethat women diagnosed with the newcriteria (even if they would not havebeen diagnosed with older criteria) haveincreased rates of poor pregnancy out-comes similar to those of women withGDM by prior criteria (39,40). Expectedbenefits to these pregnancies and offspringare inferred from intervention trials thatfocused on women with more mild hyper-glycemia than identified using older GDMdiagnostic criteria and that found modestbenefits (41,42). The frequency of follow-up and blood glucose monitoring for thesewomen is not yet clear, but likely to be lessintensive than for women diagnosed by theolder criteria. It is important to note that80–90% of women in both of the mildGDM studies (whose glucose values over-lapped with the thresholds recommendedherein) could be managed with lifestyletherapy alone.
The American College of Obstetri-cians and Gynecologists announced in2011 that they continue to recommenduse of prior diagnostic criteria for GDM(43). Several other countries haveadopted the new criteria, and a reportfrom the WHO on this topic is pendingat the time of publication of these stand-ards. The National Institutes of Health isplanning to hold a consensus develop-ment conference on this topic in 2013.
Because some cases of GDM mayrepresent pre-existing undiagnosed type2 diabetes, women with a history ofGDM should be screened for diabetes6–12 weeks postpartum, using nonpreg-nant OGTT criteria. Because of their pre-partum treatment for hyperglycemia, useof the A1C for diagnosis of persistent di-abetes at the postpartum visit is not rec-ommended (44). Women with a historyof GDM have a greatly increased subse-quent risk for diabetes (45) and shouldbe followed up with subsequent screen-ing for the development of diabetes orprediabetes, as outlined in Section II.Lifestyle interventions or metforminshould be offered to women with a his-tory of GDM who develop prediabetes,as discussed in Section IV. In the pro-spective Nurses’ Health Study II, risk ofsubsequent diabetes after a history ofGDM was significantly lower in womenwho followed healthy eating patterns.Adjusting for BMI moderately, but notcompletely, attenuated this association(46).
IV. PREVENTION/DELAYOF TYPE 2 DIABETES
Recommendationsc Patientswith IGT (A), IFG (E), or anA1Cof 5.7–6.4% (E) should be referred to aneffective ongoing support program tar-geting weight loss of 7% of body weightand increasing physical activity to at least150 min/week of moderate activity suchas walking.
c Follow-up counseling appears to beimportant for success. (B)
c Based on the cost-effectiveness of diabetesprevention, such programs should becovered by third-party payers. (B)
c Metformin therapy for prevention oftype 2 diabetes may be considered inthosewith IGT (A), IFG (E), or anA1Cof5.7–6.4% (E), especially for those withBMI .35 kg/m2, aged ,60 years, andwomen with prior GDM. (A)
c At least annual monitoring for the de-velopment of diabetes in those withprediabetes is suggested. (E)
c Screening for and treatment of modifi-able risk factors for CVD is suggested. (B)
RCTs have shown that individuals athigh risk for developing type 2 diabetes(those with IFG, IGT, or both) can signif-icantly decrease the rate of onset of diabeteswith particular interventions (23–29).These include intensive lifestyle modifica-tion programs that have been shown to bevery effective (;58% reduction after 3years) and use of the pharmacologicalagents metformin, a-glucosidase inhibi-tors, orlistat, and thiazolidinediones, eachof which has been shown to decrease inci-dent diabetes to various degrees. Follow-upof all three large studies of lifestyle interven-tion has shown sustained reduction in therate of conversion to type 2 diabetes, with43% reduction at 20 years in the Da Qingstudy (47), 43% reduction at 7 years in theFinnish Diabetes Prevention Study (DPS)(48), and 34% reduction at 10 years inthe U.S. Diabetes Prevention ProgramOutcomes Study (DPPOS) (49). A cost-effectiveness model suggested that lifestyleinterventions as delivered in the DPP arecost-effective (50), and actual cost datafrom theDPP andDPPOS confirm that life-style interventions are highly cost-effective(51). Group delivery of the DPP interven-tion in community settings has the poten-tial to be significantly less expensive whilestill achieving similar weight loss (52).
Based on the results of clinical trialsand the known risks of progression ofprediabetes to diabetes, persons with an
A1C of 5.7–6.4%, IGT, or IFG should becounseled on lifestyle changes with goalssimilar to those of the DPP (7% weightloss and moderate physical activity of atleast 150 min/week). Regarding drugtherapy for diabetes prevention, metfor-min has a strong evidence base and dem-onstrated long-term safety (53). For otherdrugs, issues of cost, side effects, and lackof persistence of effect in some studies(54) require consideration. Metforminwas less effective than lifestyle modifica-tion in the DPP and DPPOS, but may becost-saving over a 10-year period (51). Itwas as effective as lifestyle modificationin participants with a BMI of at least 35kg/m2, but not significantly better thanplacebo than those over age 60 years(23). In women in the DPP with a historyof GDM,metformin and intensive lifestylemodification led to an equivalent 50% re-duction in the risk of diabetes (55). Met-formin therefore might reasonably berecommended for very high-risk individ-uals (those with a history of GDM, thevery obese, and/or those with more severeor progressive hyperglycemia).
People with prediabetes often haveother cardiovascular risk factors, such asobesity, hypertension, and dyslipidemia.Assessing and treating these risk factors isan important aspect of reducing cardio-metabolic risk. In the DPP and DPPOS,cardiovascular event rates have been verylow, perhaps due to appropriate manage-ment of cardiovascular risk factors in allarms of the study (56).
V. DIABETES CARE
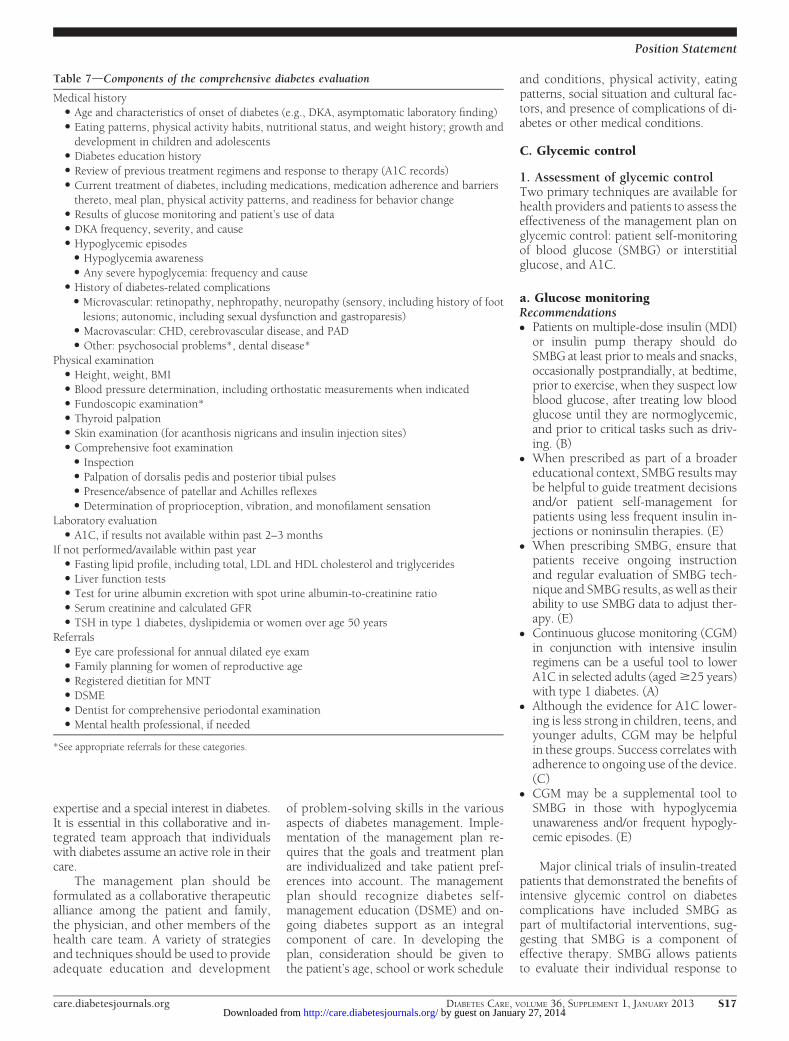
A. Initial evaluationA complete medical evaluation should beperformed to classify the diabetes, detectthe presence of diabetes complications,review previous treatment and risk factorcontrol in patients with established diabe-tes, assist in formulating a managementplan, and provide a basis for continuingcare. Laboratory tests appropriate to theevaluation of each patient’s medical condi-tion should be performed. A focus on thecomponents of comprehensive care (Table7) will assist the health care team to ensureoptimal management of the patient withdiabetes.
B. ManagementPeople with diabetes should receive med-ical care from a team that may includephysicians, nurse practitioners, physician’sassistants, nurses, dietitians, pharmacists,and mental health professionals with
S16 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
expertise and a special interest in diabetes.It is essential in this collaborative and in-tegrated team approach that individualswith diabetes assume an active role in theircare.
The management plan should beformulated as a collaborative therapeuticalliance among the patient and family,the physician, and other members of thehealth care team. A variety of strategiesand techniques should be used to provideadequate education and development
of problem-solving skills in the variousaspects of diabetes management. Imple-mentation of the management plan re-quires that the goals and treatment planare individualized and take patient pref-erences into account. The managementplan should recognize diabetes self-management education (DSME) and on-going diabetes support as an integralcomponent of care. In developing theplan, consideration should be given tothe patient’s age, school or work schedule
and conditions, physical activity, eatingpatterns, social situation and cultural fac-tors, and presence of complications of di-abetes or other medical conditions.
C. Glycemic control
1. Assessment of glycemic controlTwo primary techniques are available forhealth providers and patients to assess theeffectiveness of the management plan onglycemic control: patient self-monitoringof blood glucose (SMBG) or interstitialglucose, and A1C.
a. Glucose monitoringRecommendationsc Patients on multiple-dose insulin (MDI)or insulin pump therapy should doSMBG at least prior to meals and snacks,occasionally postprandially, at bedtime,prior to exercise, when they suspect lowblood glucose, after treating low bloodglucose until they are normoglycemic,and prior to critical tasks such as driv-ing. (B)
c When prescribed as part of a broadereducational context, SMBG results maybe helpful to guide treatment decisionsand/or patient self-management forpatients using less frequent insulin in-jections or noninsulin therapies. (E)
c When prescribing SMBG, ensure thatpatients receive ongoing instructionand regular evaluation of SMBG tech-nique and SMBG results, as well as theirability to use SMBG data to adjust ther-apy. (E)
c Continuous glucose monitoring (CGM)in conjunction with intensive insulinregimens can be a useful tool to lowerA1C in selected adults (aged$25 years)with type 1 diabetes. (A)
c Although the evidence for A1C lower-ing is less strong in children, teens, andyounger adults, CGM may be helpfulin these groups. Success correlates withadherence to ongoing use of the device.(C)
c CGM may be a supplemental tool toSMBG in those with hypoglycemiaunawareness and/or frequent hypogly-cemic episodes. (E)
Major clinical trials of insulin-treatedpatients that demonstrated the benefits ofintensive glycemic control on diabetescomplications have included SMBG aspart of multifactorial interventions, sug-gesting that SMBG is a component ofeffective therapy. SMBG allows patientsto evaluate their individual response to
Table 7dComponents of the comprehensive diabetes evaluation
Medical historyc Age and characteristics of onset of diabetes (e.g., DKA, asymptomatic laboratory finding)c Eating patterns, physical activity habits, nutritional status, and weight history; growth anddevelopment in children and adolescents
c Diabetes education historyc Review of previous treatment regimens and response to therapy (A1C records)c Current treatment of diabetes, including medications, medication adherence and barriersthereto, meal plan, physical activity patterns, and readiness for behavior change
c Results of glucose monitoring and patient’s use of datac DKA frequency, severity, and causec Hypoglycemic episodes
c Hypoglycemia awarenessc Any severe hypoglycemia: frequency and cause
c History of diabetes-related complicationsc Microvascular: retinopathy, nephropathy, neuropathy (sensory, including history of footlesions; autonomic, including sexual dysfunction and gastroparesis)
c Macrovascular: CHD, cerebrovascular disease, and PADc Other: psychosocial problems*, dental disease*
Physical examinationc Height, weight, BMIc Blood pressure determination, including orthostatic measurements when indicatedc Fundoscopic examination*c Thyroid palpationc Skin examination (for acanthosis nigricans and insulin injection sites)c Comprehensive foot examination
c Inspectionc Palpation of dorsalis pedis and posterior tibial pulsesc Presence/absence of patellar and Achilles reflexesc Determination of proprioception, vibration, and monofilament sensation
Laboratory evaluationc A1C, if results not available within past 2–3 months
If not performed/available within past yearc Fasting lipid profile, including total, LDL and HDL cholesterol and triglyceridesc Liver function testsc Test for urine albumin excretion with spot urine albumin-to-creatinine ratioc Serum creatinine and calculated GFRc TSH in type 1 diabetes, dyslipidemia or women over age 50 years
Referralsc Eye care professional for annual dilated eye examc Family planning for women of reproductive agec Registered dietitian for MNTc DSMEc Dentist for comprehensive periodontal examinationc Mental health professional, if needed
*See appropriate referrals for these categories.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S17
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

therapy and assess whether glycemic tar-gets are being achieved. Results of SMBGcan be useful in preventing hypoglycemiaand adjusting medications (particularlyprandial insulin doses), medical nutritiontherapy (MNT), and physical activity.
The frequency and timing of SMBGshould be dictated by the particular needsand goals of the patient. SMBG is espe-cially important for patients treated withinsulin tomonitor for and prevent asymp-tomatic hypoglycemia and hyperglyce-mia. Most patients with type 1 diabetesand others on intensive insulin regimens(MDI or insulin pump therapy) should doSMBG at least prior to meals and snacks,occasionally postprandially, at bedtime,prior to exercise, when they suspect lowblood glucose, after treating low bloodglucose until they are normoglycemic,and prior to critical tasks such as driving.For many patients, this will require test-ing 6–8 times daily, although individualneeds may be greater. Although there arefew rigorous studies, a database study ofalmost 27,000 children and adolescentswith type 1 diabetes showed that, afteradjustment for multiple confounders, in-creased daily frequency of SMBG was sig-nificantly associated with lower A1C(20.2% per additional test per day, level-ing off at five tests per day) and with feweracute complications (57). The optimalfrequency of SMBG for patients on non-intensive regimens, such as those withtype 2 diabetes on basal insulin, is notknown, although a number of studieshave used fasting SMBG for patient or pro-vider titration of the basal insulin dose.
The evidence base for SMBG forpatientswith type 2 diabetes on noninsulin therapyis somewhat mixed. Several randomizedtrials have called into question the clinicalutility and cost-effectiveness of routineSMBG in non–insulin-treated patients(58–60). A recent meta-analysis suggestedthat SMBG reduced A1C by 0.25% at 6months (61), while a Cochrane review con-cluded that the overall effect of SMBG insuch patients is small up to 6 months afterinitiation and subsides after 12months (62).
Because the accuracy of SMBG isinstrument and user dependent (63), itis important to evaluate each patient’smonitoring technique, both initially andat regular intervals thereafter. Optimaluse of SMBG requires proper review andinterpretation of the data, both by the pa-tient and provider. Among patients whochecked their blood glucose at least oncedaily, many reported taking no actionwhen results were high or low (64). In
one study of insulin-naïve patients withsuboptimal initial glycemic control, useof structured SMBG (a paper tool to col-lect and interpret 7-point SMBG profilesover 3 days at least quarterly) reducedA1C by 0.3% more than in an active con-trol group (65). Patients should be taughthow to use SMBG data to adjust food in-take, exercise, or pharmacological therapyto achieve specific goals, and the ongoingneed for and frequency of SMBG should bere-evaluated at each routine visit.
Real-time CGM through the measure-ment of interstitial glucose (which corre-lates well with plasma glucose) is available.These sensors require calibration withSMBG, and the latter are still recommendedfor making acute treatment decisions.CGM devices have alarms for hypo- andhyperglycemic excursions. A 26-week ran-domized trial of 322 type 1 diabetic pa-tients showed that adults aged $25 yearsusing intensive insulin therapy and CGMexperienced a 0.5% reduction in A1C(from;7.6 to 7.1%) compared with usualintensive insulin therapy with SMBG (66).Sensor use in children, teens, and adults toage 24 years did not result in significantA1C lowering, and there was no significantdifference in hypoglycemia in any group.Importantly, the greatest predictor of A1Clowering in this study for all age-groupswas frequency of sensor use, which waslower in younger age-groups. In a smallerRCT of 129 adults and children with base-line A1C ,7.0%, outcomes combiningA1C and hypoglycemia favored the grouputilizing CGM, suggesting that CGM is alsobeneficial for individuals with type 1 dia-betes who have already achieved excellentcontrol (67).
A trial comparing CGM plus insulinpump to SMBG plus multiple injectionsof insulin in adults and children with type1 diabetes showed significantly greaterimprovements in A1C with “sensor-augmented pump” therapy (68,69), butthis trial did not isolate the effect of CGMitself. Overall, meta-analyses suggest thatcompared with SMBG, CGM lowers A1Cby ;0.26% (70). Altogether, these datasuggest that, in appropriately selected pa-tients who are motivated to wear it most ofthe time, CGM reduces A1C. The technol-ogymay be particularly useful in thosewithhypoglycemia unawareness and/or fre-quent episodes of hypoglycemia, althoughstudies as yet have not shown significantreductions in severe hypoglycemia (70).CGM forms the underpinning for the de-velopment of pumps that suspend insulindelivery when hypoglycemia is developing
and for the burgeoning work on “artificialpancreas” systems.
b. A1CRecommendationsc Perform the A1C test at least twotimes a year in patients who are meet-ing treatment goals (and who havestable glycemic control). (E)
c Perform the A1C test quarterly in pa-tients whose therapy has changed orwho are not meeting glycemic goals. (E)
c Use of POC testing for A1C providesthe opportunity for more timely treat-ment changes. (E)
Because A1C is thought to reflect aver-age glycemia over several months (63) andhas strong predictive value for diabetescomplications (71,72), A1C testingshould be performed routinely in all pa-tients with diabetes, at initial assessmentand then as part of continuing care. Mea-surement approximately every 3 monthsdetermines whether patient’s glycemic tar-gets have been reached and maintained.For any individual patient, the frequencyof A1C testing should be dependent onthe clinical situation, the treatment regimenused, and the judgment of the clinician.Some patients with stable glycemia wellwithin target may do well with testingonly twice per year, while unstable orhighly intensively managed patients (e.g.,pregnant type 1 diabetic women) may betested more frequently than every 3months. The availability of the A1C resultat the time that the patient is seen (POCtesting) has been reported in small studiesto result in increased intensification of ther-apy and improvement in glycemic control(73,74). However, two recent systematicreviews andmeta-analyses found no signif-icant difference in A1C between POC andlaboratory A1C usage (75,76).
The A1C test is subject to certainlimitations. Conditions that affect eryth-rocyte turnover (hemolysis, blood loss)and hemoglobin variants must be consid-ered, particularly when the A1C resultdoes not correlate with the patient’s clin-ical situation (63). In addition, A1C doesnot provide a measure of glycemic vari-ability or hypoglycemia. For patientsprone to glycemic variability (especiallytype 1 diabetic patients or type 2 diabeticpatients with severe insulin deficiency),glycemic control is best judged by thecombination of results of self-monitoringand the A1C. The A1Cmay also serve as acheck on the accuracy of the patient’s me-ter (or the patient’s reported SMBG
S18 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

results) and the adequacy of the SMBGtesting schedule.
Table 8 contains the correlation be-tween A1C levels and mean plasma glu-cose levels based on data from theinternational A1C-Derived Average Glu-cose (ADAG) trial utilizing frequentSMBG and CGM in 507 adults (83% Cau-casian) with type 1, type 2, and no diabe-tes (77). The ADA and the AmericanAssociation for Clinical Chemistry havedetermined that the correlation (r 50.92) is strong enough to justify reportingboth an A1C result and an estimated av-erage glucose (eAG) result when a clini-cian orders the A1C test. The table in pre-2009 versions of the “Standards of Medi-cal Care in Diabetes” describing the cor-relation between A1C and mean glucosewas derived from relatively sparse data(one 7-point profile over 1 day per A1Creading) in the primarily Caucasian type 1diabetic participants in the DCCT (78).Clinicians should note that the numbersin the table are now different, as they arebased on;2,800 readings per A1C in theADAG trial.
In the ADAG trial, there were no sig-nificant differences among racial and eth-nic groups in the regression lines betweenA1C and mean glucose, although therewas a trend toward a difference betweenAfrican/African American participantsand Caucasian ones. A small study com-paring A1C to CGM data in type 1 di-abetic children found a highly statisticallysignificant correlation between A1C andmean blood glucose, although the corre-lation (r 5 0.7) was significantly lowerthan in the ADAG trial (79). Whether
there are significant differences in howA1C relates to average glucose in childrenor in African American patients is an areafor further study. For the time being, thequestion has not led to different recom-mendations about testing A1C or to dif-ferent interpretations of the clinicalmeaning of given levels of A1C in thosepopulations.
For patients in whom A1C/eAG andmeasured blood glucose appear discrep-ant, clinicians should consider the possi-bilities of hemoglobinopathy or alteredred cell turnover, and the options of morefrequent and/or different timing of SMBGor use of CGM.Othermeasures of chronicglycemia such as fructosamine are avail-able, but their linkage to average glucoseand their prognostic significance are notas clear as is the case for A1C.
2. Glycemic goals in adultsRecommendationsc Lowering A1C to below or around 7%has been shown to reduce microvas-cular complications of diabetes and ifimplemented soon after the diagnosisof diabetes is associated with long-termreduction in macrovascular disease.Therefore, a reasonable A1C goal formany nonpregnant adults is ,7%. (B)
c Providers might reasonably suggestmore stringent A1C goals (such as,6.5%) for selected individual pa-tients, if this can be achieved withoutsignificant hypoglycemia or other ad-verse effects of treatment. Appropriatepatients might include those with shortduration of diabetes, long life expec-tancy, and no significant CVD. (C)
c Less stringent A1C goals (such as,8%) may be appropriate for patientswith a history of severe hypoglycemia,limited life expectancy, advanced mi-crovascular or macrovascular complica-tions, extensive comorbid conditions,and those with long-standing diabetes inwhom the general goal is difficult to at-tain despite DSME, appropriate glucosemonitoring, and effective doses of mul-tiple glucose-lowering agents includinginsulin. (B)
Hyperglycemia defines diabetes, andglycemic control is fundamental to themanagement of diabetes. The DCCT(71), a prospective RCT of intensive ver-sus standard glycemic control in patientswith relatively recently diagnosed type 1diabetes, showed definitively thatimproved glycemic control is associ-ated with significantly decreased rates of
microvascular (retinopathy and nephro-pathy) and neuropathic complications.Follow-up of the DCCT cohorts in the Ep-idemiology of Diabetes Interventions andComplications (EDIC) study (80,81) dem-onstrated persistence of these microvascu-lar benefits in previously intensively treatedsubjects, even though their glycemic con-trol approximated that of previous stan-dard arm subjects during follow-up.
The Kumamoto Study (82) and UKProspective Diabetes Study (UKPDS)(83,84) confirmed that intensive glycemiccontrol was associated with significantlydecreased rates of microvascular and neu-ropathic complications in patients withtype 2 diabetes. Long-term follow-up ofthe UKPDS cohorts showed persistence ofthe effect of early glycemic control onmost microvascular complications (85).
Subsequent trials in patients withmore long-standing type 2 diabetes, de-signed primarily to look at the role ofintensive glycemic control on cardiovas-cular outcomes, also confirmed a benefit,although more modest, on onset or pro-gression of microvascular complications.The Veterans Affairs Diabetes Trial(VADT) showed significant reductionsin albuminuria with intensive (achievedmedian A1C 6.9%) compared with stan-dard glycemic control, but no differencein retinopathy and neuropathy (86,87).The Action in Diabetes and Vascular Dis-ease: Preterax and Diamicron MR Con-trolled Evaluation (ADVANCE) study ofintensive versus standard glycemic con-trol in type 2 diabetes found a statisticallysignificant reduction in albuminuria, butnot in neuropathy or retinopathy, with anA1C target of ,6.5% (achieved medianA1C 6.3%) compared with standard ther-apy achieving amedian A1C of 7.0% (88).Analyses from the Action to Control Car-diovascular Risk in Diabetes (ACCORD)trial have shown lower rates of onset orprogression of early-stage microvascularcomplications in the intensive glycemiccontrol arm compared with the standardarm (89,90).
Epidemiological analyses of the DCCTand UKPDS (71,72) demonstrate a curvi-linear relationship between A1C and mi-crovascular complications. Such analysessuggest that, on a population level, thegreatest number of complications will beaverted by taking patients from very poorcontrol to fair or good control. These anal-yses also suggest that further lowering ofA1C from7 to 6% is associatedwith furtherreduction in the risk of microvascularcomplications, albeit the absolute risk
Table 8dCorrelation of A1C with averageglucose
A1C (%)
Mean plasma glucose
mg/dL mmol/L
6 126 7.07 154 8.68 183 10.29 212 11.810 240 13.411 269 14.912 298 16.5
These estimates are based on ADAG data of;2,700glucose measurements over 3 months per A1Cmeasurement in 507 adults with type 1, type 2, andno diabetes. The correlation between A1C and av-erage glucose was 0.92 (ref. 77). A calculator forconverting A1C results into eAG, in either mg/dL ormmol/L, is available at http://professional.diabetes.org/eAG.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S19
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

reductions become much smaller. Giventhe substantially increased risk of hypogly-cemia (particularly in those with type 1 di-abetes, but also in the recent type 2 diabetestrials), the concerning mortality findings inthe ACCORD trial (91), and the relativelymuch greater effort required to achievenear-normoglycemia, the risks of lower gly-cemic targets may outweigh the potentialbenefits on microvascular complicationson a population level. However, selectedindividual patients, especially those withlittle comorbidity and long life expectancy(who may reap the benefits of further low-ering of glycemia below 7%), may, basedon provider judgment and patient prefer-ences, adopt more intensive glycemic tar-gets (e.g., an A1C target,6.5%) as long assignificant hypoglycemia does not becomea barrier.
CVD, a more common cause of deathin populations with diabetes than micro-vascular complications, is less clearlyimpacted by levels of hyperglycemia orthe intensity of glycemic control. In theDCCT, there was a trend toward lowerrisk of CVD events with intensive control,and in 9-year post-DCCT follow-up of theEDIC cohort participants previously ran-domized to the intensive arm had a sig-nificant 57% reduction in the risk ofnonfatalmyocardial infarction (MI), stroke,or CVD death compared with those pre-viously in the standard arm (92). The ben-efit of intensive glycemic control in thistype 1 diabetic cohort has recently beenshown to persist for several decades (93).
In type 2 diabetes, there is evidencethat more intensive treatment of glycemiain newly diagnosed patients may reducelong-term CVD rates. During the UKPDStrial, there was a 16% reduction in car-diovascular events (combined fatal ornonfatal MI and sudden death) in theintensive glycemic control arm that didnot reach statistical significance (P 50.052), and there was no suggestion ofbenefit on other CVD outcomes such asstroke. However, after 10 years of follow-up, those originally randomized to inten-sive glycemic control had significantlong-term reductions in MI (15% withsulfonylurea or insulin as initial pharma-cotherapy, 33% with metformin as initialpharmacotherapy) and in all-cause mor-tality (13% and 27%, respectively) (85).
Three more recent large trials(ACCORD, ADVANCE, and VADT) sug-gested no significant reduction in CVDoutcomes with intensive glycemic controlin participants who had more advancedtype 2 diabetes than UKPDS participants.
All three of these trials were conducted inparticipants with more long-standing di-abetes (mean duration 8–11 years) andeither known CVD or multiple cardiovas-cular risk factors. Details of these threestudies are reviewed extensively in anADA position statement (94).
The ACCORD study enrolled partici-pants with either known CVD or two ormore major cardiovascular risk factorsand randomized them to intensive glyce-mic control (goal A1C,6%) or standardglycemic control (goal A1C 7–8%). Theglycemic control comparison was haltedearly due to the finding of an increasedrate of mortality in the intensive arm com-pared with the standard arm (1.41% vs.1.14% per year; HR 1.22; 95% CI 1.01–1.46), with a similar increase in cardiovas-cular deaths. This increase in mortality inthe intensive glycemic control arm wasseen in all prespecified patient subgroups.The primary outcome of ACCORD (non-fatal MI, nonfatal stroke, or cardiovascu-lar death) was nonsignificantly lower inthe intensive glycemic control groupdue to a reduction in nonfatal MI, bothwhen the glycemic control comparisonwas halted and all participants transi-tioned to the standard glycemic controlintervention (91), and at completion ofthe planned follow-up (95).
Exploratory analyses of the mortalityfindings of ACCORD (evaluating vari-ables including weight gain, use of anyspecific drug or drug combination, andhypoglycemia) were reportedly unable toidentify a clear explanation for the excessmortality in the intensive arm (91). TheACCORD investigators subsequentlypublished additional epidemiologicalanalyses showing no increase in mortalityin the intensive arm participants whoachieved A1C levels below 7% nor inthose who lowered their A1C quickly af-ter trial enrollment. In fact, although therewas no A1C level at which intensive armparticipants had significantly lower mor-tality than standard arm participants, thehighest risk for mortality was observed inintensive arm participants with the high-est A1C levels (96).
The role of hypoglycemia in the ex-cess mortality findings was also complex.Severe hypoglycemia was significantlymore likely in participants randomizedto the intensive glycemic control arm.However, excess mortality in the inten-sive versus standard arms was only sig-nificant for participants with no severehypoglycemia, and not for those with oneor more episodes. Severe hypoglycemia
was associated with excess mortality ineither arm, but the association was stron-ger in those randomized to the standardglycemic control arm (97). Unlike thecase with the DCCT trial, where lowerachieved A1C levels were related to sig-nificantly increased rates of severe hypo-glycemia, in ACCORD every 1% declinein A1C from baseline to 4 months into thetrial was associated with a significant de-crease in the rate of severe hypoglycemiain both arms (96).
The primary outcome of ADVANCEwas a combination of microvascularevents (nephropathy and retinopathy)and major adverse cardiovascular events(MI, stroke, and cardiovascular death).Intensive glycemic control (to a goal A1C,6.5% vs. treatment to local standards)significantly reduced the primary endpoint. However, this was due to a significantreduction in themicrovascular outcome, pri-marily development of macroalbuminuria,with no significant reduction in the macro-vascular outcome. There was no differencein overall or cardiovascular mortality be-tween the intensive compared with thestandard glycemic control arms (88).
The VADT randomized participantswith type 2 diabetes uncontrolled oninsulin or maximal-dose oral agents (me-dian entry A1C 9.4%) to a strategy ofintensive glycemic control (goal A1C,6.0%) or standard glycemic control,with a planned A1C separation of at least1.5%. The primary outcome of the VADTwas a composite of CVD events. The cu-mulative primary outcome was nonsig-nificantly lower in the intensive arm(86). An ancillary study of the VADTdemonstrated that intensive glycemiccontrol significantly reduced the primaryCVD outcome in individuals with lessatherosclerosis at baseline (assessed bycoronary calcium) but not in personswith more extensive baseline atheroscle-rosis (98). A post hoc analysis showed acomplex relationship between durationof diabetes before glycemic intensifica-tion and mortality: mortality in the inten-sive vs. standard glycemic control armwas inversely related to duration of dia-betes at the time of study enrollment.Those with diabetes duration less than15 years had a mortality benefit in the in-tensive arm, while those with duration of20 years or more had higher mortality inthe intensive arm (99).
The evidence for a cardiovascular ben-efit of intensive glycemic control primarilyrests on long-term follow-up of studycohorts treated early in the course of type
S20 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

1 and type 2 diabetes and subset analyses ofACCORD, ADVANCE, and VADT. Agroup-level meta-analysis of the latter threetrials suggests that glucose lowering has amodest (9%) but statistically significantreduction in major CVD outcomes, pri-marily nonfatal MI, with no significanteffect onmortality.However, heterogeneityof the mortality effects across studies wasnoted, precluding firm summary measuresof the mortality effects. A prespecified sub-group analysis suggested that major CVDoutcome reduction occurred in patientswithout known CVD at baseline (HR 0.84,95% CI 0.74–0.94) (100). Conversely, themortality findings in ACCORD and sub-group analyses of the VADT suggest thatthe potential risks of intensive glycemiccontrol may outweigh its benefits in somepatients, such as those with very long du-ration of diabetes, known history of severehypoglycemia, advanced atherosclerosis,and advanced age/frailty. Certainly, provid-ers should be vigilant in preventing severehypoglycemia in patients with advanceddisease and should not aggressively at-tempt to achieve near-normal A1C levelsin patients in whom such a target cannotbe safely and reasonably easily achieved.Severe or frequent hypoglycemia is an ab-solute indication for the modification oftreatment regimens, including settinghigher glycemic goals. Many factors, in-cluding patient preferences, should betaken into account when developing a pa-tient’s individualized goals (101).
Recommended glycemic goals formany nonpregnant adults are shown inTable 9. The recommendations are basedon those for A1C values, with listed bloodglucose levels that appear to correlatewith achievement of an A1C of ,7%.
The issue of pre- versus postprandialSMBG targets is complex (102). Elevatedpostchallenge (2-h OGTT) glucose valueshave been associated with increased car-diovascular risk independent of FPG insome epidemiological studies. In diabeticsubjects, some surrogate measures ofvascular pathology, such as endothelialdysfunction, are negatively affected bypostprandial hyperglycemia (103). It isclear that postprandial hyperglycemia,like preprandial hyperglycemia, contrib-utes to elevated A1C levels, with its rela-tive contribution being higher at A1Clevels that are closer to 7%. However,outcome studies have clearly shownA1C to be the primary predictor of com-plications, and landmark glycemic con-trol trials such as the DCCT and UKPDSrelied overwhelmingly on preprandialSMBG. Additionally, an RCT in patientswith known CVD found no CVD benefitof insulin regimens targeting postpran-dial glucose compared with thosetargeting preprandial glucose (104). Areasonable recommendation for post-prandial testing and targets is that for in-dividuals who have premeal glucosevalues within target but have A1C valuesabove target, monitoring postprandialplasma glucose (PPG) 1–2 h after the startof themeal and treatment aimed at reduc-ing PPG values to,180 mg/dL may helplower A1C.
Glycemic goals for children are pro-vided in Section VIII.A.1.a. As regards goalsfor glycemic control for women withGDM, recommendations from the FifthInternational Workshop-Conference onGestational Diabetes Mellitus (105) wereto target maternal capillary glucose con-centrations of:
c preprandial:#95mg/dL (5.3 mmol/L),and either:
c 1-h postmeal:#140mg/dL (7.8mmol/L)or
c 2-h postmeal:#120mg/dL (6.7mmol/L)
For women with pre-existing type 1or type 2 diabetes who become pregnant, arecent consensus statement (106) recom-mended the following as optimal glycemicgoals, if they can be achieved without ex-cessive hypoglycemia:
c premeal, bedtime, and overnight glu-cose 60–99 mg/dL (3.3–5.4 mmol/L)
c peak postprandial glucose 100–129mg/dL (5.4–7.1 mmol/L)
c A1C ,6.0%
D. Pharmacological and overallapproaches to treatment
1. Insulin therapy for type 1 diabetesRecommendationsc Most people with type 1 diabetes shouldbe treated with MDI injections (threeto four injections per day of basal andprandial insulin) or continuous sub-cutaneous insulin infusion (CSII). (A)
c Most people with type 1 diabetesshould be educated in how to matchprandial insulin dose to carbohydrateintake, premeal blood glucose, andanticipated activity. (E)
c Most people with type 1 diabetesshould use insulin analogs to reducehypoglycemia risk. (A)
c Consider screening those with type 1diabetes for other autoimmune dis-eases (thyroid, vitamin B12 deficiency,celiac) as appropriate. (B)
The DCCT clearly showed that inten-sive insulin therapy (three or more in-jections per day of insulin, CSII, or insulinpump therapy) was a key part of im-proved glycemia and better outcomes(71,92). At the time of the study, therapywas carried out with short- and intermedi-ate-acting human insulins. Despite bettermicrovascular outcomes, intensive insulintherapy was associated with a high rate insevere hypoglycemia (62 episodes per 100patient-years of therapy). Since the time ofthe DCCT, a number of rapid-acting andlong-acting insulin analogs have been de-veloped. These analogs are associated withless hypoglycemia with equal A1C lower-ing in type 1 diabetes (107,108).
Recommended therapy for type 1 di-abetes consists of the following components:
Table 9dSummary of glycemic recommendations for many nonpregnant adults with diabetes
A1C ,7.0%*Preprandial capillary plasma glucose 70–130mg/dL* (3.9–7.2 mmol/L)Peak postprandial capillary plasma glucose† ,180 mg/dL* (,10.0 mmol/L)
c*Goals should be individualized based on:c duration of diabetesc age/life expectancyc comorbid conditionsc known CVD or advanced microvascular complicationsc hypoglycemia unawarenessc individual patient considerations
c More or less stringent glycemic goals may be appropriatefor individual patients
c Postprandial glucose may be targeted if A1C goals arenot met despite reaching preprandial glucose goals
†Postprandial glucose measurements should be made 1–2 h after the beginning of the meal, generally peaklevels in patients with diabetes.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S21
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

1) use of MDI injections (three to four in-jections per day of basal and prandial in-sulin) or CSII therapy; 2) matching ofprandial insulin to carbohydrate intake,premeal blood glucose, and anticipatedactivity; and 3) for most patients (espe-cially if hypoglycemia is a problem), useof insulin analogs. There are excellent re-views available that guide the initiationand management of insulin therapyto achieve desired glycemic goals(107,109,110). Although most studies ofMDI versus pump therapy have been smalland of short duration, a systematic reviewand meta-analysis concluded that therewere no systematic differences in A1C orrates of severe hypoglycemia in childrenand adults between the two forms of inten-sive insulin therapy (70).
Because of the increased frequencyof other autoimmune diseases in type 1diabetes, screening for thyroid dysfunc-tion, vitamin B12 deficiency, or celiacdisease should be considered based onsigns and symptoms. Periodic screeningin absence of symptoms has been recom-mended, but the effectiveness and opti-mal frequency are unclear.
2. Pharmacological therapy for hyper-glycemia in type 2 diabetesRecommendationsc Metformin, if not contraindicated and iftolerated, is the preferred initial pharma-cological agent for type 2 diabetes. (A)
c In newly diagnosed type 2 diabeticpatients with markedly symptomaticand/or elevated blood glucose levels orA1C, consider insulin therapy, with orwithout additional agents, from theoutset. (E)
c If noninsulin monotherapy at maximaltolerated dose does not achieve or main-tain the A1C target over 3–6 months,add a second oral agent, a glucagon-likepeptide-1 (GLP-1) receptor agonist, orinsulin. (A)
c A patient-centered approach should beused to guide choice of pharmacologicalagents. Considerations include efficacy,cost, potential side effects, effects onweight, comorbidities, hypoglycemiarisk, and patient preferences. (E)
c Due to the progressive nature of type 2diabetes, insulin therapy is eventuallyindicated for many patients with type 2diabetes. (B)
The ADA and EASD have recentlypartnered on guidance for individualiza-tion of use of medication classes andcombinations in patients with type 2
diabetes (111). This 2012 position state-ment is less prescriptive than prior algo-rithms and discusses advantages anddisadvantages of the available medicationclasses and considerations for their use. Apatient-centered approach is stressed,taking into account patient preferences,cost and potential side effects of eachclass, effects on body weight, and hypo-glycemia risk. The position statement re-affirms metformin as the preferred initialagent, barring contraindication or intoler-ance, either in addition to lifestyle coun-seling and support for weight loss andexercise, or when lifestyle efforts alonehave not achieved ormaintained glycemicgoals. Metformin has a long-standingevidence base for efficacy and safety, isinexpensive, and may reduce risk of car-diovascular events (85). When metforminfails to achieve or maintain glycemic goals,another agent should be added. Althoughthere are a number of trials comparingdual therapy to metformin alone, few di-rectly compare drugs as add-on therapy.Comparative effectiveness meta-analyses(112) suggest that overall each new classof noninsulin agents added to initial ther-apy lowers A1C around 0.9–1.1%.
Many patients with type 2 diabeteseventually benefit from insulin therapy.The progressive nature of type 2 diabetesand its therapies should regularly beexplained in a matter-of-fact manner topatients, avoiding using insulin as a threator describing it as a failure or punishment.Providing patients with an algorithm forself-titration of insulin doses based onSMBG results improves glycemic controlin type 2 diabetic patients initiatinginsulin (113). For more details on phar-macotherapy for hyperglycemia in type2 diabetes, including a table of informa-tion about currently approved classesof medications for treating hyperglyce-mia in type 2 diabetes, readers are referredto the ADA-EASD position statement(111).
E. MNTGeneral recommendationsc Individuals who have prediabetes ordiabetes should receive individualizedMNT as needed to achieve treatmentgoals, preferably provided by a regis-tered dietitian familiar with the com-ponents of diabetes MNT. (A)
c Because MNT can result in cost-savingsand improved outcomes (B), MNTshould be adequately covered by in-surance and other payers. (E)
Energy balance, overweight, and obesityc Weight loss is recommended for alloverweight or obese individuals whohave or are at risk for diabetes. (A)
c For weight loss, either low-carbohydrate,low-fat calorie-restricted, or Mediterra-nean diets may be effective in the short-term (up to 2 years). (A)
c For patients on low-carbohydrate diets,monitor lipid profiles, renal function,and protein intake (in those with ne-phropathy) and adjust hypoglycemictherapy as needed. (E)
c Physical activity and behavior modifi-cation are important components ofweight loss programs and are mosthelpful in maintenance of weightloss. (B)
Recommendations for primaryprevention of type 2 diabetesc Among individuals at high risk for de-veloping type 2 diabetes, structuredprograms that emphasize lifestylechanges that include moderate weightloss (7% body weight) and regularphysical activity (150 min/week), withdietary strategies including reducedcalories and reduced intake of dietaryfat, can reduce the risk for developingdiabetes and are therefore recom-mended. (A)
c Individuals at risk for type 2 diabetesshould be encouraged to achieve theU.S. Department of Agriculture (USDA)recommendation for dietary fiber (14 gfiber/1,000 kcal) and foods containingwhole grains (one-half of grain intake).(B)
c Individuals at risk for type 2 diabetesshould be encouraged to limit theirintake of sugar-sweetened beverages(SSBs). (B)
Recommendations for managementof diabetesMacronutrients in diabetes managementc The mix of carbohydrate, protein, andfat may be adjusted to meet the meta-bolic goals and individual preferencesof the person with diabetes. (C)
c Monitoring carbohydrate, whether bycarbohydrate counting, choices, or ex-perience-based estimation, remains a keystrategy in achieving glycemic control. (B)
c Saturated fat intake should be ,7% oftotal calories. (B)
c Reducing intake of trans fat lowers LDLcholesterol and increases HDL choles-terol (A); therefore, intake of trans fatshould be minimized. (E)
S22 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Other nutrition recommendationsc If adults with diabetes choose to usealcohol, they should limit intake to amoderate amount (one drink per day orless for adult women and two drinksper day or less for adultmen) and shouldtake extra precautions to prevent hypo-glycemia. (E)
c Routine supplementation with anti-oxidants, such as vitamins E and C andcarotene, is not advised because of lackof evidence of efficacy and concern re-lated to long-term safety. (A)
c It is recommended that individualizedmeal planning include optimization offood choices to meet recommended di-etary allowance (RDA)/dietary referenceintake (DRI) for all micronutrients. (E)
MNT is an integral component of di-abetes prevention, management, and self-management education. In addition to itsrole in preventing and controlling diabetes,the ADA recognizes the importance ofnutrition as an essential component of anoverall healthy lifestyle. A full review of theevidence regarding nutrition in preventingand controlling diabetes and its complica-tions and additional nutrition-related rec-ommendations can be found in the ADAposition statement “Nutrition Recommen-dations and Interventions for Diabetes”(114), which is being updated as of 2013.Achieving nutrition-related goals requires acoordinated team effort that includes the ac-tive involvement of the person with predia-betes or diabetes. Because of the complexityof nutrition issues, it is recommended that aregistered dietitian who is knowledgeableand skilled in implementing nutritiontherapy into diabetes management andeducation be the team member who pro-vides MNT.
Clinical trials/outcome studies ofMNT have reported decreases in A1C at3–6 months ranging from 0.25 to 2.9%with higher reductions seen in type 2diabetes of shorter duration. Multiplestudies have demonstrated sustained im-provements in A1C at 12months and lon-ger when a registered dietitian providedfollow-up visits ranging from monthly to3 sessions per year (115–122). Studies innondiabetic individuals suggest thatMNT reduces LDL cholesterol by 15–25mg/dL up to 16% (123) and support arole for lifestyle modification in treatinghypertension (123,124).
Although the importance of weight lossfor overweight and obese individuals is welldocumented, an optimal macronutrientdistribution and dietary pattern of weight
loss diets has not been established. Asystematic review of 80 weight loss studiesof $1-year duration demonstrated thatmoderate weight loss achieved throughdiet alone, diet and exercise, and meal re-placements can be achieved and main-tained (4.8–8% weight loss at 12 months)(125). Both low-fat low-carbohydrate andMediterranean style eating patterns havebeen shown to promote weight loss withsimilar results after 1 to 2 years of follow-up (126–129). A meta-analysis showedthat at 6 months, low-carbohydrate dietswere associated with greater improvementsin triglyceride andHDLcholesterol concen-trations than low-fat diets; however, LDLcholesterol was significantly higher on thelow-carbohydrate diets (130).
Because of the effects of obesity oninsulin resistance, weight loss is an im-portant therapeutic objective for over-weight or obese individuals who are atrisk for diabetes (131). The multifactorialintensive lifestyle intervention used in theDPP, which included reduced intake of fatand calories, led to weight loss averaging7% at 6 months and maintenance of 5%weight loss at 3 years, associated with a58% reduction in incidence of type 2 di-abetes (23). An RCT looking at high-riskindividuals in Spain showed that theMediterranean dietary pattern reducedthe incidence of diabetes in the absenceof weight loss by 52% compared with thelow-fat control group (132).
Although our society abounds withexamples of high-calorie nutrient-poorfoods, large increases in the consumptionof SSBs have coincided with the epidemicsof obesity and type 2 diabetes. In a meta-analysis of eight prospective cohort stud-ies (n5 310,819), a diet high in consump-tion of SSBs was associated with thedevelopment of type 2 diabetes (n 515,043). Individuals in the highest versuslowest quantile of SSB intake had a 26%greater risk of developing diabetes (133).
For individuals with type 2 diabetes,studies have demonstrated that moderateweight loss (5% of body weight) is associ-ated with decreased insulin resistance, im-proved measures of glycemia and lipemia,and reduced blood pressure (134); longer-term studies ($52 weeks) showed mixedeffects onA1C in adultswith type 2diabetes(135–137), and in some studies resultswere confounded by pharmacologicalweight loss therapy. Look AHEAD (Actionfor Health in Diabetes) is a large clinical trialdesigned to determine whether long-termweight loss will improve glycemia and pre-vent cardiovascular events in subjects with
type 2 diabetes. One-year results of the in-tensive lifestyle intervention in this trialshow an average 8.6% weight loss, signifi-cant reduction of A1C, and reduction inseveral CVD risk factors (138), with benefitssustained at 4 years (139). At the time thisarticle was going to press, the LookAHEADtrial was halted early, after 11 years of fol-low-up, because there was no significantdifference in the primary cardiovascularoutcome between the weight loss and stan-dard care group (http://www.nih.gov/news/health/oct2012/niddk-19.htm). Multiplecardiovascular risk factors were improvedwith weight loss, and those participantson average were on fewer medications toachieve these improvements.
Although numerous studies have at-tempted to identify the optimal mix ofmacronutrients for meal plans of peoplewith diabetes, a recent systematic review(140) confirms that there is nomost effec-tive mix that applies broadly, and thatmacronutrient proportions should be indi-vidualized. It must be clearly recognizedthat regardless of the macronutrient mix,total caloric intake must be appropriate toweight management goal. Further, individ-ualization of the macronutrient composi-tion will depend on the metabolic statusof the patient (e.g., lipid profile, renal func-tion) and/or food preferences. A variety ofdietary meal patterns are likely effective inmanaging diabetes including Mediterra-nean-style, plant-based (vegan or vegetar-ian), low-fat and lower-carbohydrate eatingpatterns (127,141–143).
It should be noted that the RDA fordigestible carbohydrate is 130 g/day and isbased on providing adequate glucose as therequired fuel for the central nervous systemwithout reliance on glucose productionfrom ingested protein or fat. Althoughbrain fuel needs can be met on lowercarbohydrate diets, long-term metaboliceffects of very low-carbohydrate diets areunclear and such diets eliminate manyfoods that are important sources of energy,fiber, vitamins, and minerals and are im-portant in dietary palatability (144).
Saturated and trans fatty acids are theprincipal dietary determinants of plasmaLDL cholesterol. There is a lack of evi-dence on the effects of specific fatty acidson people with diabetes, so the recom-mended goals are consistent with thosefor individuals with CVD (123,145).
Reimbursement for MNTMNT, when delivered by a registereddietitian according to nutrition practiceguidelines, is reimbursed as part of the
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S23
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Medicare program as overseen by theCenters for Medicare and Medicaid Serv-ices (CMS), as well as many health in-surance plans.
F. Diabetes self-managementeducation and supportRecommendationsc People with diabetes should receiveDSME and diabetes self-managementsupport (DSMS) according to NationalStandards for Diabetes Self-Manage-ment Education and Support whentheir diabetes is diagnosed and asneeded thereafter. (B)
c Effective self-management and qualityof life are the key outcomes of DSMEand DSMS and should be measuredand monitored as part of care. (C)
c DSME and DSMS should addresspsychosocial issues, since emotionalwell-being is associated with positivediabetes outcomes. (C)
c DSME and DSMS programs are appro-priate venues for people with prediabetesto receive education and support to de-velop and maintain behaviors that canprevent or delay the onset of diabetes. (C)
c Because DSME and DSMS can result incost-savings and improved outcomes (B),DSME and DSMS should be adequatelyreimbursed by third-party payers. (E)
DSME and DSMS are essential ele-ments of diabetes care (146–151), and re-cently updated National Standards forDiabetes Self-Management Education andSupport (152) are based on evidence for itsbenefits. Education helps people with dia-betes initiate effective self-management andcope with diabetes when they are first di-agnosed. Ongoing DSME and DSMS alsohelp people with diabetes maintain effec-tive self-management throughout a lifetimeof diabetes as they face new challenges andtreatment advances become available.DSME helps patients optimize metaboliccontrol, prevent and manage complica-tions, and maximize quality of life in acost-effective manner (153).
DSME and DSMS are the ongoingprocesses of facilitating the knowledge,skill, and ability necessary for diabetesself-care. This process incorporates theneeds, goals, and life experiences of theperson with diabetes. The overall objec-tives of DSME and DSMS are to supportinformed decisionmaking, self-care behav-iors, problem-solving, and active collabo-ration with the health care team to improveclinical outcomes, health status, and qual-ity of life in a cost-effective manner (152).
Current best practice of DSME is askill-based approach that focuses onhelping those with diabetes make in-formed self-management choices. DSMEhas changed from a didactic approachfocusing on providing information tomore theoretically based empowermentmodels that focus on helping those withdiabetes make informed self-managementdecisions. Care of diabetes has shifted toan approach that is more patient centeredand places the person with diabetesand his or her family at the center of thecare model working in collaborationwith health care professionals. Patient-centered care is respectful of and respon-sive to individual patient preferences,needs, and values and ensures that patientvalues guide all decision making (154).
Evidence for the benefits of DSME andDSMSMultiple studies have found that DSME isassociated with improved diabetes knowl-edge and improved self-care behavior(146), improved clinical outcomes suchas lower A1C (147,148,150,151,155–158), lower self-reported weight (146), im-proved quality of life (149,156,159),healthy coping (160), and lower costs(161). Better outcomes were reported forDSME interventions that were longer andincluded follow-up support (DSMS)(146,162–165), that were culturally(166,167) and age appropriate (168,169)and were tailored to individual needs andpreferences, and that addressed psychoso-cial issues and incorporated behavioralstrategies (146,150,170,171). Both indi-vidual and group approaches have beenfound effective (172,173). There is growingevidence for the role of community healthworkers and peer (174–180) and lay lead-ers (181) in delivering DSME and DSMS inconjunction with the core team (182).
Diabetes education is associated withincreased use of primary and preventiveservices (161,183) and lower use of acute,inpatient hospital services (161). Patientswho participate in diabetes education aremore likely to follow best practice treat-ment recommendations, particularlyamong the Medicare population, andhave lower Medicare and commercialclaim costs (184,185).
The National Standards for DiabetesSelf-Management Education andSupportThe National Standards for Diabetes Self-Management Education and Support aredesigned to define quality DSME and
DSMS and to assist diabetes educatorsin a variety of settings to provide evidence-based education and self-managementsupport (152). The standards, recently up-dated, are reviewed and updated every 5years by a task force representing key or-ganizations involved in the field of diabeteseducation and care.
DSME and DSMS providers and peo-ple with prediabetesThe new standards for DSME and DSMSalso apply to the education and support ofpeople with prediabetes. Currently, thereare significant barriers to the provision ofeducation and support to those with pre-diabetes. However, the strategies for sup-porting successful behavior change andthe healthy behaviors recommended forpeople with prediabetes are largely iden-tical to those for people with diabetes. Asbarriers to care are overcome, providers ofDSME and DSMS, given their training andexperience, are particularly well equippedto assist people with prediabetes in de-veloping and maintaining behaviors thatcan prevent or delay the onset of diabetes(152,186).
Reimbursement for DSME and DSMSDSME, when provided by a program thatmeets national standards for DSME and isrecognized by the ADA or other approvalbodies, is reimbursed as part of theMedicareprogram as overseen by the CMS. DSMEis also covered by most health insuranceplans. Although DSMS has been shown tobe instrumental for improving outcomes, asdescribed in the “Evidence for the benefits ofDSME and DSMS,” and can be provided informats such as phone calls and via tele-health, it currently has limited reimburse-ment as face-to-face visits included asfollow-up to DSME.
G. Physical activityRecommendationsc Adults with diabetes should be advisedto perform at least 150 min/week ofmoderate-intensity aerobic physicalactivity (50–70% of maximum heartrate), spread over at least 3 days/weekwith no more than two consecutivedays without exercise. (A)
c In the absence of contraindications,adults with type 2 diabetes should beencouraged to perform resistance train-ing at least twice per week. (A)
Exercise is an important part of thediabetes management plan. Regular exer-cise has been shown to improve blood
S24 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

glucose control, reduce cardiovascular riskfactors, contribute to weight loss, andimprove well-being. Furthermore, regularexercise may prevent type 2 diabetes inhigh-risk individuals (23–25). Structuredexercise interventions of at least 8 weeks’duration have been shown to lower A1C byan average of 0.66% in people with type2 diabetes, even with no significant changein BMI (187). Higher levels of exercise in-tensity are associated with greater improve-ments in A1C and in fitness (188). A jointposition statement of the ADA and theAmerican College of Sports Medicine(ACSM) summarizes the evidence for thebenefits of exercise in people with type 2diabetes (189).
Frequency and type of exerciseThe U.S. Department of Health and HumanServices’ Physical Activity Guidelines forAmericans (190) suggest that adults overage 18 years do 150 min/week of moder-ate-intensity, or 75 min/week of vigorousaerobic physical activity, or an equivalentcombination of the two. In addition, theguidelines suggest that adults also domuscle-strengthening activities that in-volve all major muscle groups $2 days/week. The guidelines suggest that adultsover age 65 years, or those with disabili-ties, follow the adult guidelines if possibleor (if this is not possible) be as physicallyactive as they are able. Studies included inthe meta-analysis of effects of exercise in-terventions on glycemic control (187)had a mean number of sessions perweek of 3.4, with a mean of 49 min persession. The DPP lifestyle intervention,which included 150 min/week of moder-ate-intensity exercise, had a beneficialeffect on glycemia in those with predia-betes. Therefore, it seems reasonable torecommend that people with diabetestry to follow the physical activity guide-lines for the general population.
Progressive resistance exercise im-proves insulin sensitivity in older menwith type 2 diabetes to the same or even agreater extent as aerobic exercise (191).Clinical trials have provided strong evidencefor the A1C lowering value of resistancetraining in older adults with type 2 dia-betes (192,193) and for an additive ben-efit of combined aerobic and resistanceexercise in adults with type 2 diabetes(194,195). In the absence of contraindi-cations, patients with type 2 diabetesshould be encouraged to do at least twoweekly sessions of resistance exercise (ex-ercise with free weights or weight ma-chines), with each session consisting of
at least one set of five or more differentresistance exercises involving the largemuscle groups (189).
Evaluation of the diabetic patient beforerecommending an exercise programPrior guidelines suggested that beforerecommending a program of physical activ-ity, the provider should assess patients withmultiple cardiovascular risk factors for cor-onary artery disease (CAD). As discussedmore fully in Section VI.A.5, the area ofscreening asymptomatic diabetic patientsfor CAD remains unclear, and a recent ADAconsensus statement on this issue con-cluded that routine screening is not recom-mended (196). Providers should use clinicaljudgment in this area. Certainly, high-riskpatients should be encouraged to start withshort periods of low-intensity exercise andincrease the intensity and duration slowly.
Providers should assess patients forconditions that might contraindicate cer-tain types of exercise or predispose toinjury, such as uncontrolled hyperten-sion, severe autonomic neuropathy, se-vere peripheral neuropathy or history offoot lesions, and unstable proliferativeretinopathy. The patient’s age and pre-vious physical activity level should beconsidered.
Exercise in the presence of nonoptimalglycemic controlHyperglycemia. When people with type1 diabetes are deprived of insulin for 12–48 h and are ketotic, exercise can worsenhyperglycemia and ketosis (197); there-fore, vigorous activity should be avoidedin the presence of ketosis. However, it isnot necessary to postpone exercise basedsimply on hyperglycemia, provided thepatient feels well and urine and/or bloodketones are negative.Hypoglycemia. In individuals taking in-sulin and/or insulin secretagogues, phys-ical activity can cause hypoglycemia ifmedication dose or carbohydrate con-sumption is not altered. For individualson these therapies, added carbohydrateshould be ingested if pre-exercise glucoselevels are,100 mg/dL (5.6 mmol/L). Hy-poglycemia is rare in diabetic individualswho are not treated with insulin or insulinsecretagogues, and no preventive mea-sures for hypoglycemia are usually ad-vised in these cases.
Exercise in the presence of specificlong-term complications of diabetesRetinopathy. In the presence of prolifer-ative diabetic retinopathy (PDR) or severe
non-PDR (NPDR), vigorous aerobic orresistance exercise may be contraindi-cated because of the risk of triggeringvitreous hemorrhage or retinal detach-ment (198).Peripheral neuropathy. Decreased painsensation in the extremities results inincreased risk of skin breakdown andinfection and of Charcot joint destruc-tion. Prior recommendations have ad-vised non–weight-bearing exercise forpatients with severe peripheral neuropa-thy. However, studies have shown thatmoderate-intensity walking may notlead to increased risk of foot ulcers orreulceration in those with peripheralneuropathy (199). All individuals withperipheral neuropathy should wearproper footwear and examine their feetdaily to detect lesions early. Anyonewith a foot injury or open sore shouldbe restricted to non–weight-bearing ac-tivities.Autonomic neuropathy. Autonomic neu-ropathy can increase the risk of exercise-induced injury or adverse event throughdecreased cardiac responsiveness to exer-cise, postural hypotension, impaired ther-moregulation, impaired night vision due toimpaired papillary reaction, and unpredict-able carbohydrate delivery from gastropa-resis predisposing to hypoglycemia (200).Autonomic neuropathy is also strongly as-sociated with CVD in people with diabetes(201,202). People with diabetic autonomicneuropathy should undergo cardiac inves-tigation before beginning physical activitymore intense than that to which they areaccustomed.Albuminuria and nephropathy. Physicalactivity can acutely increase urinary pro-tein excretion. However, there is no evi-dence that vigorous exercise increases therate of progression of diabetic kidneydisease, and there is likely no need forany specific exercise restrictions for peo-ple with diabetic kidney disease (203).
H. Psychosocial assessment and careRecommendationsc It is reasonable to include assessment ofthe patient’s psychological and socialsituation as an ongoing part of themedical management of diabetes. (E)
c Psychosocial screening and follow-upmay include, but is not limited to, at-titudes about the illness, expectationsfor medical management and out-comes, affect/mood, general and di-abetes-related quality of life, resources(financial, social, and emotional), andpsychiatric history. (E)
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S25
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

c Screen for psychosocial problems suchas depression and diabetes-relateddistress, anxiety, eating disorders,and cognitive impairment when self-management is poor. (B)
It is important to establish that emotionalwell-being is part of diabetes care and self-management. Psychological and socialproblems can impair the individual’s(204–207) or family’s ability to carry outdiabetes care tasks and therefore compro-mise health status. There are opportuni-ties for the clinician to assess psychosocialstatus in a timely and efficient manner sothat referral for appropriate services canbe accomplished. A systematic review andmeta-analysis showed that psychosocialinterventions modestly but significantlyimproved A1C (standardizedmean differ-ence 20.29%) and mental health out-comes. However, there was a limitedassociation between the effects on A1Cand mental health, and no interventioncharacteristics predicted benefit on bothoutcomes (208).
Key opportunities for screening ofpsychosocial status occur at diagnosis,during regularly scheduled managementvisits, during hospitalizations, at discov-ery of complications, or when problemswith glucose control, quality of life, oradherence are identified. Patients arelikely to exhibit psychological vulnerabil-ity at diagnosis and when their medicalstatus changes (e.g., the end of the hon-eymoon period), when the need for in-tensified treatment is evident, and whencomplications are discovered (206).
Depression affects about 20–25% ofpeople with diabetes (207) and increasesthe risk forMI and post-MI (209,210) andall-cause (211) mortality. Other issuesknown to impact self-management andhealth outcomes include but are not limitedto attitudes about the illness, expectationsfor medical management and outcomes,affect/mood, general and diabetes-relatedquality of life, diabetes-related distress(212,213), resources (financial, social,and emotional) (214), and psychiatric his-tory (215–217). Screening tools are avail-able for a number of these areas (170).Indications for referral to a mental healthspecialist familiar with diabetes manage-ment may include gross disregard for themedical regimen (by self or others) (217),depression, possibility of self-harm, debil-itating anxiety (alone or with depression),indications of an eating disorder (218), orcognitive functioning that significantlyimpairs judgment. It is preferable to
incorporate psychological assessmentand treatment into routine care ratherthan waiting for identification of a specificproblem or deterioration in psychologicalstatus (170). Although the clinician maynot feel qualified to treat psychologicalproblems (219), utilizing the patient-provider relationship as a foundationcan increase the likelihood that the pa-tient will accept referral for other services.Collaborative care interventions andusing a team approach have demon-strated efficacy in diabetes and depres-sion (220,221).
I. When treatment goals are not metFor a variety of reasons, some people withdiabetes and their health care providersdo not achieve the desired goals of treat-ment (Table 9). Rethinking the treatmentregimen may require assessment of barri-ers including income, health literacy,diabetes distress, depression, and com-peting demands, including those relatedto family responsibilities and dynamics.Other strategies may include culturallyappropriate and enhanced DSME andDSMS, co-management with a diabetesteam, referral to a medical social workerfor assistance with insurance coverage, orchange in pharmacological therapy. Initi-ation of or increase in SMBG, utilizationof CGM, frequent contact with the pa-tient, or referral to a mental health pro-fessional or physician with specialexpertise in diabetes may be useful.
J. Intercurrent illnessThe stress of illness, trauma, and/or sur-gery frequently aggravates glycemic con-trol and may precipitate diabeticketoacidosis (DKA) or nonketotic hyper-osmolar statedlife-threatening conditionsthat require immediate medical care to pre-vent complications and death. Any condi-tion leading to deterioration in glycemiccontrol necessitatesmore frequentmonitor-ing of blood glucose and (in ketosis-pronepatients) urine or blood ketones. Markedhyperglycemia requires temporary adjust-ment of the treatment program and, if ac-companied by ketosis, vomiting, oralteration in level of consciousness, imme-diate interaction with the diabetes careteam. The patient treated with noninsulintherapies or MNT alone may temporarilyrequire insulin. Adequate fluid and caloricintake must be assured. Infection or dehy-dration is more likely to necessitate hospi-talization of the person with diabetes thanthe person without diabetes.
The hospitalized patient should betreated by a physician with expertise inthe management of diabetes. For furtherinformation on management of patientswith hyperglycemia in the hospital, seeSection IX.A. For further informationon management of DKA or hyperglycemicnonketotic hyperosmolar state, refer to theADA statement on hyperglycemic crises(222).
K. HypoglycemiaRecommendationsc Individuals at risk for hypoglycemiashould be asked about symptomaticand asymptomatic hypoglycemia ateach encounter. (C)
c Glucose (15–20 g) is the preferredtreatment for the conscious individualwith hypoglycemia, although any formof carbohydrate that contains glucosemay be used. If SMBG 15 min aftertreatment shows continued hypogly-cemia, the treatment should be re-peated. Once SMBG glucose returns tonormal, the individual should consume ameal or snack to prevent recurrence ofhypoglycemia. (E)
c Glucagon should be prescribed for allindividuals at significant risk of severehypoglycemia, and caregivers or familymembers of these individuals shouldbe instructed on its administration.Glucagon administration is not limitedto health care professionals. (E)
c Hypoglycemia unawareness or one ormore episodes of severe hypoglycemiashould trigger re-evaluation of thetreatment regimen. (E)
c Insulin-treated patients with hypogly-cemia unawareness or an episode ofsevere hypoglycemia should be advisedto raise their glycemic targets to strictlyavoid further hypoglycemia for at leastseveral weeks, to partially reverse hy-poglycemia unawareness, and to re-duce risk of future episodes. (A)
c Ongoing assessment of cognitive func-tion is suggestedwith increased vigilancefor hypoglycemia by the clinician, pa-tient, and caregivers if low cognitionand/or declining cognition is found. (B)
Hypoglycemia is the leading limitingfactor in the glycemic management of type1 and insulin-treated type 2 diabetes (223).Mild hypoglycemia may be inconvenientor frightening to patients with diabetes,and more severe hypoglycemia can causeacute harm to the person with diabetes orothers, if it causes falls, motor vehicle
S26 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

accidents, or other injury. A large cohortstudy suggested that among older adultswith type 2 diabetes, a history of severehypoglycemia was associated with greaterrisk of dementia (224). Conversely, in asubstudy of the ACCORD trial, cognitiveimpairment at baseline or decline in cog-nitive function during the trial was signif-icantly associated with subsequentepisodes of severe hypoglycemia (225).Evidence from the DCCT/EDIC trial,which involved younger adults and ado-lescents with type 1 diabetes, suggested noassociation of frequency of severe hypo-glycemia with cognitive decline (226). Asdiscussed in the Section VIII.A.1.a, a fewstudies have suggested that severe hypo-glycemia in very young children is associ-ated with mild impairments in cognitivefunction.
As described in the Section V.b.2,severe hypoglycemia was associated withmortality in participants in both the stan-dard and intensive glycemia arms of theACCORD trial, but the relationships withachieved A1C and treatment intensitywere not straightforward. An associationof severe hypoglycemia with mortalitywas also found in the ADVANCE trial(227), but its association with other out-comes such as pulmonary and skin disor-ders raises the question of whether severehypoglycemia is a marker for a sicker pa-tient, rather than a cause of mortality. Anassociation of self-reported severe hypo-glycemia with 5-year mortality has alsobeen reported in clinical practice (228).At the time this statement went to press,the ADA and The Endocrine Society werefinalizing a Hypoglycemia Work Groupreport, where the causes of and associa-tions with hypoglycemia are discussed indepth.
Treatment of hypoglycemia (plasmaglucose,70 mg/dL) requires ingestion ofglucose- or carbohydrate-containingfoods. The acute glycemic response cor-relates better with the glucose contentthan with the carbohydrate content ofthe food. Although pure glucose is thepreferred treatment, any form of carbohy-drate that contains glucose will raiseblood glucose. Added fat may retard andthen prolong the acute glycemic response.Ongoing activity of insulin or insulin sec-retagoguesmay lead to recurrence of hypo-glycemia unless further food is ingestedafter recovery.
Severe hypoglycemia (where the in-dividual requires the assistance of an-other person and cannot be treated withoral carbohydrate due to confusion or
unconsciousness) should be treated usingemergency glucagon kits, which require aprescription. Those in close contact with,or having custodial care of, people withhypoglycemia-prone diabetes (familymembers, roommates, school personnel,child care providers, correctional institu-tion staff, or coworkers) should be in-structed in use of such kits. An individualdoes not need to be a health care pro-fessional to safely administer glucagon.Care should be taken to ensure that un-expired glucagon kits are available.
Prevention of hypoglycemia is a crit-ical component of diabetes management.Particularly for insulin-treated patients,SMBG and, for some patients, CGM todetect incipient hypoglycemia and assessadequacy of treatment are a key compo-nent of safe therapy. Patients should un-derstand situations that increase their riskof hypoglycemia, such as when fasting fortests or procedures, during or after in-tense exercise, and during sleep and thatincrease the risk of harm to self or othersfrom hypoglycemia, such as with driving.Teaching people with diabetes to balanceinsulin use, carbohydrate intake, andexercise is a necessary but not alwayssufficient strategy for prevention. In type1 diabetes and severely insulin-deficienttype 2 diabetes, the syndrome of hypo-glycemia unawareness, or hypoglycemia-associated autonomic failure, can severelycompromise stringent diabetes controland quality of life. The deficient counter-regulatory hormone release and autonomicresponses in this syndrome are both riskfactors for, and caused by, hypoglycemia. Acorollary to this “vicious cycle” is that sev-eral weeks of avoidance of hypoglycemiahas been demonstrated to improvecounter-regulation and awareness to someextent in many patients (229). Hence,patients with one or more episodes ofsevere hypoglycemia may benefit fromat least short-term relaxation of glycemictargets.
L. Bariatric surgeryRecommendationsc Bariatric surgery may be considered foradults with BMI$35 kg/m2 and type 2diabetes, especially if the diabetes orassociated comorbidities are difficult tocontrol with lifestyle and pharmaco-logical therapy. (B)
c Patients with type 2 diabetes who haveundergone bariatric surgery need life-long lifestyle support and medicalmonitoring. (B)
c Although small trials have shown gly-cemic benefit of bariatric surgery inpatients with type 2 diabetes and BMI30–35 kg/m2, there is currently in-sufficient evidence to generally rec-ommend surgery in patients with BMI,35 kg/m2 outside of a research pro-tocol. (E)
c The long-termbenefits, cost-effectiveness,and risks of bariatric surgery in indivi-duals with type 2 diabetes should bestudied in well-designed controlled trialswith optimalmedical and lifestyle therapyas the comparator. (E)
Gastric reduction surgery, either gas-tric banding or procedures that involvebypassing, transposing, or resecting sec-tions of the small intestine, when part of acomprehensive team approach, can be aneffective weight loss treatment for severeobesity, and national guidelines supportits consideration for people with type2 diabetes who have BMI of 35 kg/m2
or greater. Bariatric surgery has beenshown to lead to near- or complete nor-malization of glycemia in ;40–95% ofpatients with type 2 diabetes, dependingon the study and the surgical procedure(230–232). A meta-analysis of studies ofbariatric surgery involving 3,188 patientswith diabetes reported that 78% had re-mission of diabetes (normalization ofblood glucose levels in the absence ofmedications) and that the remission rateswere sustained in studies that had follow-up exceeding 2 years (233). Remissionrates tend to be lower with proceduresthat only constrict the stomach andhigher with those that bypass portionsof the small intestine. Additionally, thereis a suggestion that intestinal bypass pro-ceduresmay have glycemic effects that areindependent of their effects on weight,perhaps involving the incretin axis.
There is also evidence for diabetesremission in subjects who are less obese.One randomized trial compared adjust-able gastric banding to “best available”medical and lifestyle therapy in subjectswith type 2 diabetes and BMI 30–40 kg/m2
(234). Overall, 73% of surgically treatedpatients achieved “remission” of their di-abetes compared with 13% of those trea-ted medically. The latter group lost only1.7% of body weight, suggesting thattheir therapy was not optimal. Overallthe trial had 60 subjects, and only 13had a BMI under 35 kg/m2, making it dif-ficult to generalize these results widely todiabetic patients who are less severelyobese or with longer duration of diabetes.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S27
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

In a recent nonrandomized study of 66people with BMI of 30–35 kg/m2, 88%of participants had remission of theirtype 2 diabetes up to 6 years after surgery(235).
Bariatric surgery is costly in the short-term and has some risks. Rates of mor-bidity andmortality directly related to thesurgery have been reduced considerablyin recent years, with 30-day mortalityrates now 0.28%, similar to those oflaparoscopic cholecystectomy (236).Longer-term concerns include vitaminand mineral deficiencies, osteoporosis,and rare but often severe hypoglycemiafrom insulin hypersecretion. Cohortstudies attempting to match subjectssuggest that the procedure may reducelonger-term mortality rates (237). Recentretrospective analyses and modelingstudies suggest that these proceduresmay be cost-effective, when one considersreduction in subsequent health care costs(238–240).
Some caution about the benefits ofbariatric surgery might come from recentstudies. Propensity score–adjusted anal-yses of older severely obese patients withhigh baseline mortality in Veterans Af-fairs Medical Centers found that the useof bariatric surgery was not associatedwith decreased mortality compared withusual care during a mean 6.7 years offollow-up (241). A study that followedpatients who had undergone laparo-scopic adjustable gastric banding(LAGB) for 12 years found that 60%were satisfied with the procedure. Nearlyone out of three patients experiencedband erosion, and almost half requiredremoval of their bands. The authors’ con-clusion was that “LAGB appears to resultin relatively poor long-term outcomes”(242). Studies of the mechanisms of gly-cemic improvement and long-term bene-fits and risks of bariatric surgery inindividuals with type 2 diabetes, espe-cially those who are not severely obese,will require well-designed clinical trials,with optimal medical and lifestyle ther-apy of diabetes and cardiovascular riskfactors as the comparator.
M. ImmunizationRecommendationsc Annually provide an influenza vaccineto all diabetic patients $6 months ofage. (C)
c Administer pneumococcal polysaccharidevaccine to all diabetic patients $2 yearsof age. A one-time revaccination is rec-ommended for individuals.64 years of
age previously immunized when theywere ,65 years of age if the vaccinewas administered.5 years ago. Otherindications for repeat vaccination in-clude nephrotic syndrome, chronicrenal disease, and other immunocom-promised states, such as after trans-plantation. (C)
c Administer hepatitis B vaccination tounvaccinated adults with diabetes whoare aged 19 through 59 years. (C)
c Consider administering hepatitis B vac-cination to unvaccinated adults withdiabetes who are aged$60 years. (C)
Influenza and pneumonia are common,preventable infectious diseases associatedwith high mortality and morbidity in theelderly and in people with chronic dis-eases. Though there are limited studiesreporting the morbidity and mortality ofinfluenza and pneumococcal pneumoniaspecifically in people with diabetes, ob-servational studies of patients with a va-riety of chronic illnesses, includingdiabetes, show that these conditions areassociated with an increase in hospital-izations for influenza and its complica-tions. People with diabetes may be atincreased risk of the bacteremic form ofpneumococcal infection and have beenreported to have a high risk of nosocomialbacteremia, which has a mortality rate ashigh as 50% (243).
Safe and effective vaccines are avail-able that can greatly reduce the risk ofserious complications from these diseases(244,245). In a case-control series, influ-enza vaccine was shown to reduce dia-betes-related hospital admission by asmuch as 79% during flu epidemics(244). There is sufficient evidence to sup-port that people with diabetes haveappropriate serological and clinical re-sponses to these vaccinations. The Cen-ters for Disease Control and Prevention(CDC) Advisory Committee on Immuni-zation Practices recommends influenzaand pneumococcal vaccines for all indi-viduals with diabetes (http://www.cdc.gov/vaccines/recs/).
Late in 2012, the Advisory Commit-tee on Immunization Practices of the CDCrecommended that all previously unvac-cinated adults with diabetes aged 19through 59 years be vaccinated againsthepatitis B virus (HBV) as soon as possibleafter a diagnosis of diabetes is made andthat vaccination be considered for thoseaged $60 years, after assessing risk andlikelihood of an adequate immune re-sponse (246). At least 29 outbreaks of
HBV in long-term care facilities and hos-pitals have been reported to the CDC,with the majority involving adults withdiabetes receiving “assisted blood glucosemonitoring,” in which such monitoring isdone by a health care professional withresponsibility for more than one patient.HBV is highly transmissible and stable forlong periods of time on surfaces such aslancing devices and blood glucose meters,even when no blood is visible. Blood suf-ficient to transmit the virus has also beenfound in the reservoirs of insulin pens,resulting in warnings against sharingsuch devices between patients.
The CDC analyses suggest that, ex-cluding persons with HBV-related riskbehaviors, acute HBV infection is abouttwice as high among adults with diabetesaged $23 years compared with adultswithout diabetes. Seroprevalence of anti-body toHBV core antigen, suggesting pastor current infection, is 60% higher amongadults with diabetes than those without,and there is some evidence that diabetesimparts a higher HBV case fatality rate.The age differentiation in the recommen-dations stems from CDC economic mod-els suggesting that vaccination of adultswith diabetes who were aged 20–59 yearswould cost an estimated $75,000 perquality-adjusted life-year saved, whilecost per quality-adjusted life-year savedincreased significantly at higher ages. Inaddition to competing causes of mortalityin older adults, the immune response tothe vaccine declines with age (246).
These new recommendations regard-ing HBV vaccinations serve as a reminderto clinicians that children and adults withdiabetes need a number of vaccinations,both those specifically indicated becauseof diabetes as well as those recommendedfor the general population (http://www.cdc.gov/vaccines/recs/).
VI. PREVENTION ANDMANAGEMENT OF DIABETESCOMPLICATIONS
A. CVDCVD is the major cause of morbidity andmortality for individuals with diabetesand the largest contributor to the directand indirect costs of diabetes. The commonconditions coexisting with type 2 diabetes(e.g., hypertension and dyslipidemia) areclear risk factors for CVD, and diabetesitself confers independent risk. Numerousstudies have shown the efficacy of con-trolling individual cardiovascular riskfactors in preventing or slowing CVD in
S28 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

people with diabetes. Large benefits areseen when multiple risk factors are ad-dressed globally (247,248). There is evi-dence that measures of 10-year coronaryheart disease (CHD) risk among U.S.adults with diabetes have improved signif-icantly over the past decade (249).
1. Hypertension/blood pressurecontrolRecommendationsScreening and diagnosisc Blood pressure should be measured atevery routine visit. Patients found tohave elevated blood pressure shouldhave blood pressure confirmed on aseparate day. (B)
Goalsc People with diabetes and hypertensionshould be treated to a systolic bloodpressure goal of ,140 mmHg. (B)
c Lower systolic targets, such as ,130mmHg, may be appropriate for certainindividuals, such as younger patients,if it can be achieved without unduetreatment burden. (C)
c Patients with diabetes should be treatedto a diastolic blood pressure,80mmHg.(B)
Treatmentc Patients with a blood pressure .120/80 mmHg should be advised on life-style changes to reduce blood pressure.(B)
c Patients with confirmed blood pressure$140/80 mmHg should, in addition tolifestyle therapy, have prompt initia-tion and timely subsequent titration ofpharmacological therapy to achieveblood pressure goals. (B)
c Lifestyle therapy for elevated bloodpressure consists of weight loss, ifoverweight; Dietary Approaches toStop Hypertension (DASH)-style di-etary pattern including reducing so-dium and increasing potassium intake;moderation of alcohol intake; and in-creased physical activity. (B)
c Pharmacological therapy for patientswith diabetes and hypertension shouldbe with a regimen that includes eitheran ACE inhibitor or an angiotensinreceptor blocker (ARB). If one class isnot tolerated, the other should be sub-stituted. (C)
c Multiple-drug therapy (two or moreagents at maximal doses) is generallyrequired to achieve blood pressuretargets. (B)
c Administer one or more antihyperten-sive medications at bedtime. (A)
c If ACE inhibitors, ARBs, or diuretics areused, serum creatinine/estimated glo-merular filtration rate (eGFR) and serumpotassium levels should be monitored.(E)
c In pregnant patients with diabetes andchronic hypertension, blood pressuretarget goals of 110–129/65–79 mmHgare suggested in the interest of long-term maternal health and minimizingimpaired fetal growth. ACE inhibitorsand ARBs are contraindicated duringpregnancy. (E)
Hypertension is a common comor-bidity of diabetes, affecting themajority ofpatients, with prevalence depending ontype of diabetes, age, obesity, and ethnic-ity. Hypertension is a major risk factor forboth CVD and microvascular complica-tions. In type 1 diabetes, hypertension isoften the result of underlying nephropa-thy, while in type 2 diabetes it usuallycoexists with other cardiometabolic riskfactors.
Screening and diagnosisMeasurement of blood pressure in theoffice should be done by a trained in-dividual and follow the guidelines es-tablished for nondiabetic individuals:measurement in the seated position,with feet on the floor and arm supportedat heart level, after 5 min of rest. Cuff sizeshould be appropriate for the upper armcircumference. Elevated values should beconfirmed on a separate day.
Home blood pressure self-monitoringand 24-h ambulatory blood pressuremonitoring may provide additional evi-dence of “white coat” and masked hyper-tension and other discrepancies betweenoffice and “true” blood pressure. Studiesin nondiabetic populations found thathome measurements may better correlatewith CVD risk than office measurements(250,251). However, the preponderanceof the evidence of benefits of treatment ofhypertension in people with diabetes isbased on office measurements.
Treatment goalsEpidemiological analyses show that bloodpressure .115/75 mmHg is associatedwith increased cardiovascular event ratesand mortality in individuals with diabetes(252–254) and that systolic blood pres-sure above 120mmHg predicts long-termend-stage renal disease (ESRD). Random-ized clinical trials have demonstrated thebenefit (reduction of CHD events, stroke,and nephropathy) of lowering blood
pressure to ,140 mmHg systolic and,80 mmHg diastolic in individuals withdiabetes (252,255–257). The evidence forbenefits from lower systolic blood pres-sure targets is, however, limited.
The ACCORD trial examinedwhether blood pressure lowering to sys-tolic blood pressure ,120 mmHg pro-vides greater cardiovascular protectionthan a systolic blood pressure level of130–140 mmHg in patients with type 2diabetes at high risk for CVD (258). Theblood pressure achieved in the intensivegroup was 119/64 mmHg and in the stan-dard group 133/70mmHg; the goals wereattained with an average of 3.4 medica-tions per participant in the intensivegroup and 2.1 in the standard therapygroup. The hazard ratio for the primaryend point (nonfatal MI, nonfatal stroke,and CVD death) in the intensive groupwas 0.88 (95% CI 0.73–1.06, P 5 0.20).Of the prespecified secondary end points,only stroke and nonfatal stroke were sta-tistically significantly reduced by inten-sive blood pressure treatment, with ahazard ratio of 0.59 (95% CI 0.39–0.89,P 5 0.01) and 0.63 (95% CI 0.41–0.96,P 5 0.03), respectively. Absolute strokeevent rates were low; the number neededto treat to prevent one stroke over thecourse of 5 years with intensive bloodpressure management is 89. Serious ad-verse event rates (including syncope andhyperkalemia) were higher with intensivetargets (3.3% vs. 1.3%, P5 0.001). Ratesof albuminuria were reduced with moreintensive blood pressure goals, but therewere no differences in renal function inthis 5-year trial (and in fact more adverseevents related to reduced eGFRwithmoreintensive goals) nor in other microvascu-lar complications.
Other recent randomized trial datainclude those of the ADVANCE trial inwhich treatment with an ACE inhibitorand a thiazide-type diuretic reduced therate of death but not the compositemacrovascular outcome. However, theADVANCE trial had no specified targetsfor the randomized comparison, and themean systolic blood pressure in the in-tensive group (135mmHg)was not as lowas the mean systolic blood pressure evenin the ACCORD standard-therapy group(259). Post hoc analysis of achieved bloodpressure in several hypertension treat-ment trials has suggested no benefit oflower achieved systolic blood pressure.As an example, among 6,400 patientswith diabetes and CAD enrolled in onetrial, “tight control” (achieved systolic
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S29
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

blood pressure,130 mmHg) was not as-sociated with improved cardiovascularoutcomes compared with “usual care”(achieved systolic blood pressure 130–140 mmHg) (260). Similar findingemerged from an analysis of another trial,but additionally those with achieved sys-tolic blood pressure (,115 mmHg) hadincreased rates of CVD events (thoughlower rates of stroke) (261).
Observational data, including thosederived from clinical trials, may be in-appropriate to use for defining bloodpressure targets since sicker patientsmay have low blood pressure or, con-versely, healthier or more adherent pa-tients may achieve goals more readily. Arecent meta-analysis of randomized trialsof adults with type 2 diabetes comparingprespecified blood pressure targets foundno significant reduction in mortality ornonfatal MI. There was a statisticallysignificant 35% relative reduction instroke, but the absolute risk reductionwas only 1% (262). Other outcomes, suchas indicators of microvascular complica-tions, were not examined. Anothermeta-analysis that included both trialscomparing blood pressure goals and trialscomparing treatment strategies con-cluded that a systolic treatment goal of130–135 mmHg was acceptable. Withgoals,130 mmHg, there were greater re-ductions in stroke, a 10% reduction inmortality, but no reduction of otherCVD events and increased rates of seriousadverse events. Systolic blood pressure,130 mmHg was associated with re-duced onset and progression of albumin-uria. However, there was heterogeneity inthemeasure, rates of more advanced renaldisease outcomes were not affected, andthere were no significant changes in reti-nopathy or neuropathy (263).
This change in the “default” systolicblood pressure target is not meant todownplay the importance of treating hy-pertension in patients with diabetes or toimply that lower targets than ,140mmHg are generally inappropriate. Theclear body of evidence that systolic bloodpressure over 140 mmHg is harmful sug-gests that clinicians should promptly ini-tiate and titrate therapy in an ongoingfashion to achieve and maintain systolicblood pressure below 140 mmHg in vir-tually all patients. Additionally, patientswith long life expectancy (in whom theremay be renal benefits from long-termstricter blood pressure control) or thosein whom stroke risk is a concern might,as part of shared decision making,
appropriately have lower systolic targetssuch as ,130 mmHg. This would espe-cially be the case if this can be achievedwith few drugs and without side effects oftherapy.
Treatment strategiesAlthough there are no well-controlledstudies of diet and exercise in the treat-ment of elevated blood pressure or hy-pertension in individuals with diabetes,the DASH study in nondiabetic individu-als has shown antihypertensive effectssimilar to pharmacological monotherapy.Lifestyle therapy consists of reducingsodium intake (to below 1,500 mg/day)and excess body weight; increasing con-sumption of fruits, vegetables (8–10 serv-ings per day), and low-fat dairy products(2–3 servings per day); avoiding excessivealcohol consumption (no more than twoservings per day for men and no morethan one serving per day for women)(264); and increasing activity levels(252). These nonpharmacological strate-gies may also positively affect glycemiaand lipid control and as a result shouldbe encouraged in those with even mildlyelevated blood pressure. Their effects oncardiovascular events have not been es-tablished. Nonpharmacological therapyis reasonable in diabetic individuals withmildly elevated blood pressure (systolicblood pressure .120 mmHg or diastolicblood pressure.80 mmHg). If the bloodpressure is confirmed to be$140 mmHgsystolic and/or $80 mmHg diastolic,pharmacological therapy should be initi-ated along with nonpharmacologicaltherapy (252).
Lowering of blood pressure with regi-mens based on a variety of antihypertensivedrugs, including ACE inhibitors, ARBs,b-blockers, diuretics, and calcium channelblockers, has been shown to be effective inreducing cardiovascular events. Severalstudies suggested that ACE inhibitors maybe superior to dihydropyridine calciumchannel blockers in reducing cardiovascu-lar events (265–267). However, a variety ofother studies have shown no specific ad-vantage to ACE inhibitors as initial treat-ment of hypertension in the generalhypertensive population, but rather an ad-vantage on cardiovascular outcomes of ini-tial therapy with low-dose thiazide diuretics(252,268,269).
In people with diabetes, inhibitors ofthe renin-angiotensin system (RAS) mayhave unique advantages for initial or earlytherapy of hypertension. In a nonhyper-tension trial of high-risk individuals,
including a large subset with diabetes,an ACE inhibitor reduced CVD outcomes(270). In patients with congestive heartfailure (CHF), including diabetic sub-groups, ARBs have been shown to reducemajor CVD outcomes (271–274), and intype 2 diabetic patients with significantnephropathy, ARBs were superior to cal-cium channel blockers for reducing heartfailure (275). Though evidence for dis-tinct advantages of RAS inhibitors onCVD outcomes in diabetes remains con-flicting (255,269), the high CVD risks as-sociated with diabetes, and the highprevalence of undiagnosed CVD,may stillfavor recommendations for their use asfirst-line hypertension therapy in peoplewith diabetes (252).
Recently, the blood pressure arm ofthe ADVANCE trial demonstrated thatroutine administration of a fixed combi-nation of the ACE inhibitor perindopriland the diuretic indapamide significantlyreduced combined microvascular andmacrovascular outcomes, as well as CVDand total mortality. The improved out-comes could also have been due tolower achieved blood pressure in theperindopril-indapamide arm (259). An-other trial showed a decrease inmorbidityand mortality in those receiving benaze-pril and amlodipine compared with bena-zepril and hydrochlorothiazide (HCTZ).The compelling benefits of RAS inhibitorsin diabetic patients with albuminuria orrenal insufficiency provide additional ra-tionale for use of these agents (see SectionVI.B). If needed to achieve blood pressuretargets, amlodipine, HCTZ, or chlorthali-done can be added. If eGFR is ,30 mL/min/m2, a loop diuretic rather than HCTZor chlorthalidone should be prescribed.Titration of and/or addition of furtherblood pressure medications should bemade in timely fashion to overcome clin-ical inertia in achieving blood pressuretargets.
Evidence is emerging that health in-formation technology can be used safelyand effectively as a tool to enable attain-ment of blood pressure goals. Usinga telemonitoring intervention to directtitrations of antihypertensive medicationsbetween medical office visits has beendemonstrated to have a profound impacton systolic blood pressure control (276).
An important caveat is that mostpatients with hypertension requiremultiple-drug therapy to reach treatmentgoals (252). Identifying and addressingbarriers to medication adherence (suchas cost and side effects) should routinely
S30 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

be done. If blood pressure is refractorydespite confirmed adherence to optimaldoses of at least three antihypertensiveagents of different classifications, one ofwhich should be a diuretic, cliniciansshould consider an evaluation for sec-ondary forms of hypertension. Growingevidence suggests that there is an associ-ation between increase in sleep-timeblood pressure and incidence of CVDevents. A recent RCT of 448 participantswith type 2 diabetes and hypertensiondemonstrated reduced cardiovascularevents and mortality with medianfollow-up of 5.4 years if at least one an-tihypertensive medication was given atbedtime (277).
During pregnancy in diabetic womenwith chronic hypertension, target bloodpressure goals of systolic blood pressure110–129mmHg and diastolic blood pres-sure 65–79 mmHg are reasonable, as theycontribute to long-term maternal health.Lower blood pressure levels may be asso-ciated with impaired fetal growth. Duringpregnancy, treatment with ACE inhibi-tors and ARBs is contraindicated becausethey can cause fetal damage. Antihyper-tensive drugs known to be effective andsafe in pregnancy include methyldopa,labetalol, diltiazem, clonidine, and pra-zosin. Chronic diuretic use during preg-nancy has been associated with restrictedmaternal plasma volume, which mightreduce uteroplacental perfusion (278).
2. Dyslipidemia/lipid managementRecommendationsScreeningc In most adult patients with diabetes,measure fasting lipid profile at leastannually. (B)
c In adults with low-risk lipid values(LDL cholesterol ,100 mg/dL, HDLcholesterol .50 mg/dL, and trigly-cerides,150 mg/dL), lipid assessmentsmay be repeated every 2 years. (E)
Treatment recommendations and goalsc Lifestyle modification focusing on thereduction of saturated fat, trans fat, andcholesterol intake; increase of n-3 fattyacids, viscous fiber, and plant stanols/sterols; weight loss (if indicated); andincreased physical activity should berecommended to improve the lipidprofile in patients with diabetes. (A)
c Statin therapy should be added to life-style therapy, regardless of baselinelipid levels, for diabetic patients:c with overt CVD (A)c without CVD who are over the age of40 years and have one or more other
CVD risk factors (family history ofCVD, hypertension, smoking, dysli-pidemia, or albuminuria) (A)
c For lower-risk patients than the above(e.g., without overt CVD and under theage of 40 years), statin therapy shouldbe considered in addition to lifestyletherapy if LDL cholesterol remainsabove 100 mg/dL or in those withmultiple CVD risk factors. (C)
c In individuals without overt CVD, thegoal is LDL cholesterol ,100 mg/dL(2.6 mmol/L). (B)
c In individuals with overt CVD, a lowerLDL cholesterol goal of ,70 mg/dL(1.8 mmol/L), using a high dose of astatin, is an option. (B)
c If drug-treated patients do not reachthe above targets on maximal toleratedstatin therapy, a reduction in LDLcholesterol of;30–40% from baselineis an alternative therapeutic goal. (B)
c Triglycerides levels ,150 mg/dL (1.7mmol/L) and HDL cholesterol .40mg/dL (1.0 mmol/L) in men and .50mg/dL (1.3 mmol/L) in women aredesirable (C). However, LDL cholesterol–targeted statin therapy remains thepreferred strategy. (A)
c Combination therapy has been shownnot to provide additional cardiovascu-lar benefit above statin therapy aloneand is not generally recommended. (A)
c Statin therapy is contraindicated inpregnancy. (B)
Evidence for benefits of lipid-loweringtherapyPatients with type 2 diabetes have anincreased prevalence of lipid abnormali-ties, contributing to their high risk ofCVD. Multiple clinical trials demon-strated significant effects of pharmacolog-ical (primarily statin) therapy on CVDoutcomes in subjects with CHD and forprimary CVD prevention (279,280). Sub-analyses of diabetic subgroups of largertrials (281–285) and trials specifically insubjects with diabetes (286,287) showedsignificant primary and secondary pre-vention of CVD events 1/2 CHD deathsin diabetic populations. Meta-analyses in-cluding data from over 18,000 patientswith diabetes from 14 randomized trialsof statin therapy, followed for a mean of4.3 years, demonstrate a 9% proportionalreduction in all-cause mortality and 13%reduction in vascular mortality, for eachmmol/L reduction in LDL cholesterol(288). As is the case in nondiabetic indi-viduals, absolute reductions in “hard”CVD outcomes (CHD death and nonfatal
MI) are greatest in people with high base-line CVD risk (known CVD and/or veryhigh LDL cholesterol levels), but overallthe benefits of statin therapy in peoplewith diabetes at moderate or high riskfor CVD are convincing.
There is an increased risk of incidentdiabetes with statin use (289,290), whichmay be limited to those with risk factorsfor diabetes. These patients may benefitadditionally from diabetes screeningwhen on statin therapy. In an analysis ofone of the initial studies suggesting thatstatins are linked to risk of diabetes, thecardiovascular event rate reduction withstatins outweighed the risk of incident di-abetes even for patients at highest risk fordiabetes. The absolute risk increase wassmall (over 5 years of follow-up, 1.2% ofparticipants on placebo developed diabe-tes and 1.5% on rosuvastatin) (291). Therelative risk-benefit ratio favoring statinsis further supported by meta-analysis ofindividual data of over 170,000 personsfrom 27 randomized trials. This demon-strated that individuals at low risk of vas-cular disease, including those undergoingprimary prevention, received benefitsfrom statins that included reductions inmajor vascular events and vascular deathwithout increase in incidence of cancer ordeaths from other causes (280).
Low levels of HDL cholesterol, oftenassociated with elevated triglyceride lev-els, are the most prevalent pattern ofdyslipidemia in persons with type 2 di-abetes. However, the evidence base fordrugs that target these lipid fractions issignificantly less robust than that forstatin therapy (292). Nicotinic acid hasbeen shown to reduce CVD outcomes(293), although the study was done in anondiabetic cohort. Gemfibrozil has beenshown to decrease rates of CVD events insubjects without diabetes (294,295) andin the diabetic subgroup of one of thelarger trials (294). However, in a large trialspecific to diabetic patients, fenofibratefailed to reduce overall cardiovascularoutcomes (296).
Combination therapy, with a statinand a fibrate or statin and niacin, may beefficacious for treatment for all three lipidfractions, but this combination is associ-ated with an increased risk for abnormaltransaminase levels, myositis, or rhabdo-myolysis. The risk of rhabdomyolysis ishigher with higher doses of statins andwith renal insufficiency and seems to belower when statins are combined withfenofibrate than gemfibrozil (297). In theACCORD study, the combination of
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S31
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

fenofibrate and simvastatin did not re-duce the rate of fatal cardiovascularevents, nonfatal MI, or nonfatal stroke,as compared with simvastatin alone, inpatients with type 2 diabetes who wereat high risk for CVD. Prespecified sub-group analyses suggested heterogeneityin treatment effects according to sex,with a benefit of combination therapyfor men and possible harm for women,and a possible benefit for patients withboth triglyceride level $204 mg/dL andHDL cholesterol level #34 mg/dL (298).The AIM-HIGH trial randomized over3,000 patients (about one-third with di-abetes) with established CVD, low levelsof HDL cholesterol, and triglyceride levelsof 150–400 mg/dL to statin therapy plusextended release niacin or matching pla-cebo. The trial was halted early due to lackof efficacy on the primary CVD outcomeand a possible increase in ischemic strokein those on combination therapy (299).Hence, combination lipid-lowering ther-apy cannot be broadly recommended.
Dyslipidemia treatment and targetlipid levelsFor most patients with diabetes, the firstpriority of dyslipidemia therapy (unlesssevere hypertriglyceridemia with risk ofpancreatitis is the immediate issue) is tolower LDL cholesterol to a target goal of,100 mg/dL (2.60 mmol/L) (300). Life-style intervention, including MNT, in-creased physical activity, weight loss,and smoking cessation, may allow somepatients to reach lipid goals. Nutrition in-tervention should be tailored according toeach patient’s age, type of diabetes, phar-macological treatment, lipid levels, andother medical conditions and should fo-cus on the reduction of saturated fat, cho-lesterol, and trans unsaturated fat intakeand increases in n-3 fatty acids, viscousfiber (such as in oats, legumes, citrus),and plant stanols/sterols. Glycemic con-trol can also beneficially modify plasmalipid levels, particularly in patients withvery high triglycerides and poor glycemiccontrol.
In those with clinical CVD or over age40 years with other CVD risk factors,pharmacological treatment should beadded to lifestyle therapy regardless ofbaseline lipid levels. Statins are the drugsof choice for LDL cholesterol loweringand cardioprotection. In patients otherthan those described above, statin treat-ment should be considered if there is aninadequate LDL cholesterol response tolifestyle modifications and improved
glucose control, or if the patient hasincreased cardiovascular risk (e.g., multi-ple cardiovascular risk factors or longduration of diabetes). Very little clinicaltrial evidence exists for type 2 diabeticpatients under the age 40 years, or fortype 1 diabetic patients of any age. In theHeart Protection Study (lower age limit40 years), the subgroup of;600 patientswith type 1 diabetes had a reduction inrisk proportionately similar to that of pa-tients with type 2 diabetes, although notstatistically significant (282). Althoughthe data are not definitive, considerationshould be given to similar lipid-loweringgoals in type 1 diabetic patients as in type2 diabetic patients, particularly if theyhave other cardiovascular risk factors.
Alternative lipoprotein goalsVirtually all trials of statins and CVDoutcome tested specific doses of statinsagainst placebo, other doses of statin, orother statins, rather than aiming for spe-cific LDL cholesterol goals (301). Placebo-controlled trials generally achieved LDLcholesterol reductions of 30–40% frombaseline. Hence, LDL cholesterol lower-ing of this magnitude is an acceptable out-come for patients who cannot reach LDLcholesterol goals due to severe baselineelevations in LDL cholesterol and/or in-tolerance of maximal, or any, statin doses.Additionally for those with baseline LDLcholesterol minimally above 100 mg/dL,prescribing statin therapy to lower LDLcholesterol about 30–40% from baselineis probably more effective than prescrib-ing just enough to get LDL cholesterolslightly below 100 mg/dL.
Clinical trials in high-risk patients,such as those with acute coronary syn-dromes or previous cardiovascular events(302–304), have demonstrated that moreaggressive therapy with high doses of sta-tins to achieve an LDL cholesterol of,70mg/dL led to a significant reduction infurther events. Therefore, a reduction inLDL cholesterol to a goal of,70 mg/dL isan option in very high-risk diabetic pa-tients with overt CVD (305). Some ex-perts recommend a greater focus onnon–HDL cholesterol, apolipoprotein B(apoB), or lipoprotein particle measure-ments to assess residual CVD risk instatin-treated patients who are likely tohave small LDL particles, such as peoplewith diabetes (306), but it is unclearwhether clinical management wouldchange with these measurements.
In individual patients, LDL choles-terol lowering with statins is highly
variable, and this variable response ispoorly understood (307). Reduction ofCVD events with statins correlates veryclosely with LDL cholesterol lowering(279). If initial attempts to prescribe astatin leads to side effects, cliniciansshould attempt to find a dose or alterna-tive statin that the patient can tolerate.There is evidence for significant LDLcholesterol lowering from even ex-tremely low, less than daily, statin doses(308). When maximally tolerated dosesof statins fail to significantly lower LDLcholesterol (,30% reduction from thepatient’s baseline), there is no strong ev-idence that combination therapy shouldbe used to achieve additional LDL cho-lesterol lowering. Niacin, fenofibrate,ezetimibe, and bile acid sequestrants alloffer additional LDL cholesterol loweringto statins alone, but without evidencethat such combination therapy for LDLcholesterol lowering provides a signifi-cant increment in CVD risk reductionover statin therapy alone.
Treatment of other lipoprotein frac-tions or targetsHypertriglyceridemia should be ad-dressed with dietary and lifestyle changes.Severe hypertriglyceridemia (.1,000mg/dL) may warrant immediate pharma-cological therapy (fibric acid derivative,niacin, or fish oil) to reduce the risk ofacute pancreatitis. In the absence of se-vere hypertriglyceridemia, therapy target-ing HDL cholesterol or triglycerides lacksthe strong evidence base of statin therapy.If the HDL cholesterol is,40 mg/dL andthe LDL cholesterol is between 100 and129 mg/dL, a fibrate or niacin might beused, especially if a patient is intolerant tostatins. Niacin is the most effective drugfor raising HDL cholesterol. It can signif-icantly increase blood glucose at high doses,but at modest doses (750–2,000 mg/day)significant improvements in LDL choles-terol, HDL cholesterol, and triglyceridelevels are accompanied by only modestchanges in glucose that are generally ame-nable to adjustment of diabetes therapy(299,309,310).
Table 10 summarizes common treat-ment goals for A1C, blood pressure, andLDL cholesterol.
3. Antiplatelet agentsRecommendationsc Consider aspirin therapy (75–162mg/day) as a primary prevention strategyin those with type 1 or type 2 diabetes
S32 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

at increased cardiovascular risk (10-yearrisk .10%). This includes most menaged .50 years or women aged .60years who have at least one additionalmajor risk factor (family history of CVD,hypertension, smoking, dyslipidemia, oralbuminuria). (C)
c Aspirin should not be recommendedfor CVD prevention for adults withdiabetes at low CVD risk (10-year CVDrisk ,5%, such as in men aged ,50years and women aged,60 years withno major additional CVD risk factors),since the potential adverse effects frombleeding likely offset the potentialbenefits. (C)
c In patients in these age-groups withmultiple other risk factors (e.g., 10-year risk 5–10%), clinical judgment isrequired. (E)
c Use aspirin therapy (75–162 mg/day)as a secondary prevention strategy inthose with diabetes with a history ofCVD. (A)
c For patients with CVD and docu-mented aspirin allergy, clopidogrel (75mg/day) should be used. (B)
c Combination therapy with aspirin (75–162mg/day) and clopidogrel (75mg/day)is reasonable for up to a year after anacute coronary syndrome. (B)
Aspirin has been shown to be effectivein reducing cardiovascular morbidity andmortality in high-risk patients with pre-vious MI or stroke (secondary prevention).Its net benefit in primary preventionamong patients with no previous cardio-vascular events is more controversial, bothfor patients with and without a history ofdiabetes (311). Two recent RCTs of aspirinspecifically in patients with diabetes failedto show a significant reduction in CVD endpoints, raising further questions about theefficacy of aspirin for primary prevention inpeople with diabetes (312,313).
The Antithrombotic Trialists’ (ATT)collaborators recently published an indi-vidual patient-level meta-analysis of thesix large trials of aspirin for primary pre-vention in the general population. Thesetrials collectively enrolled over 95,000participants, including almost 4,000with diabetes. Overall, they found that as-pirin reduced the risk of vascular eventsby 12% (RR 0.88, 95% CI 0.82–0.94).The largest reduction was for nonfatalMI with little effect on CHD death (RR0.95, 95% CI 0.78–1.15) or total stroke.There was some evidence of a differencein aspirin effect by sex. Aspirin signifi-cantly reduced CHD events in men butnot in women. Conversely, aspirin hadno effect on stroke in men but signifi-cantly reduced stroke in women. Notably,sex differences in aspirin’s effects have notbeen observed in studies of secondaryprevention (311). In the six trials exam-ined by the ATT collaborators, the effectsof aspirin on major vascular events weresimilar for patients with or without diabe-tes: RR 0.88 (95%CI 0.67–1.15) and 0.87(95% CI 0.79–0.96), respectively. Theconfidence interval was wider for thosewith diabetes because of their smallernumber.
Based on the currently available evi-dence, aspirin appears to have a modesteffect on ischemic vascular events withthe absolute decrease in events depend-ing on the underlying CVD risk. Themain adverse effects appear to be anincreased risk of gastrointestinal bleed-ing. The excess risk may be as high as 1–5per 1,000 per year in real-world settings.In adults with CVD risk greater than 1%per year, the number of CVD events pre-vented will be similar to or greater thanthe number of episodes of bleeding in-duced, although these complications donot have equal effects on long-termhealth (314).
In 2010, a position statement of theADA, the American Heart Association(AHA), and the American College ofCardiology Foundation (ACCF) updatedprior joint recommendations for primaryprevention (315). Low-dose (75–162mg/day) aspirin use for primary preven-tion is reasonable for adults with diabetesand no previous history of vascular dis-ease who are at increased CVD risk (10-year risk of CVD events over 10%) andwho are not at increased risk for bleeding.This generally includes most men overage 50 years andwomen over age 60 yearswho also have one or more of the follow-ing major risk factors: 1) smoking, 2) hy-pertension, 3) dyslipidemia, 4) familyhistory of premature CVD, and 5) albu-minuria.
However, aspirin is no longer recom-mended for those at low CVD risk(women under age 60 years and menunder age 50 years with no major CVDrisk factors; 10-year CVD risk under 5%)as the low benefit is likely to be out-weighed by the risks of significant bleed-ing. Clinical judgment should be used forthose at intermediate risk (younger pa-tients with one or more risk factors, orolder patients with no risk factors; thosewith 10-year CVD risk of 5–10%) untilfurther research is available. Use of aspirinin patients under the age of 21 years iscontraindicated due to the associatedrisk of Reye syndrome.
Average daily dosages used in mostclinical trials involving patients with di-abetes ranged from 50 to 650 mg butwere mostly in the range of 100 to 325mg/day. There is little evidence to sup-port any specific dose, but using thelowest possible dosage may help reduceside effects (316). In the U.S., the mostcommon low dose tablet is 81 mg. Al-though platelets from patients with dia-betes have altered function, it is unclearwhat, if any, impact that finding has onthe required dose of aspirin for cardio-protective effects in the patient with di-abetes. Many alternate pathways forplatelet activation exist that are indepen-dent of thromboxane A2 and thus notsensitive to the effects of aspirin (317).Therefore, while “aspirin resistance” ap-pears higher in the diabetic patients whenmeasured by a variety of ex vivo and invitro methods (platelet aggregometry,measurement of thromboxane B2), theseobservations alone are insufficient to em-pirically recommend higher doses of as-pirin be used in the diabetic patient at thistime.
Table 10dSummary of recommendations for glycemic, blood pressure, and lipid control formost adults with diabetes
A1C ,7.0%*Blood pressure ,140/80 mmHg**LipidsLDL cholesterol ,100 mg/dL (,2.6 mmol/L)†
Statin therapy for those with history of MI or age over 401other risk factors
*More or less stringent glycemic goals may be appropriate for individual patients. Goals should be in-dividualized based on duration of diabetes, age/life expectancy, comorbid conditions, known CVD or ad-vanced microvascular complications, hypoglycemia unawareness, and individual patient considerations.**Based on patient characteristics and response to therapy, lower systolic blood pressure targets may beappropriate. †In individuals with overt CVD, a lower LDL cholesterol goal of,70mg/dL (1.8mmol/L), usinga high dose of a statin, is an option.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S33
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Clopidogrel has been demonstratedto reduce CVD events in diabetic individ-uals (318). It is recommended as adjunc-tive therapy in the first year after an acutecoronary syndrome or as alternative ther-apy in aspirin-intolerant patients.
4. Smoking cessationRecommendationsc Advise all patients not to smoke or usetobacco products. (A)
c Include smoking cessation counselingand other forms of treatment as a rou-tine component of diabetes care. (B)
A large body of evidence from epide-miological, case-control, and cohort stud-ies provides convincing documentationof the causal link between cigarette smok-ing and health risks. Much of the workdocumenting the impact of smoking onhealth did not separately discuss resultson subsets of individuals with diabetes,but suggests that the identified risks are atleast equivalent to those found in thegeneral population. Other studies of in-dividuals with diabetes consistently dem-onstrate that smokers have a heightenedrisk of CVD, premature death, and in-creased rate of microvascular complica-tions of diabetes. Smoking may have arole in the development of type 2 diabetes.One study in smokers with newly diag-nosed type 2 diabetes found that smokingcessation was associated with ameliorationofmetabolic parameters and reducedbloodpressure and albuminuria at 1 year (319).
The routine and thorough assessmentof tobacco use is important as a means ofpreventing smoking or encouraging ces-sation. A number of large randomizedclinical trials have demonstrated the effi-cacy and cost-effectiveness of brief coun-seling in smoking cessation, including theuse of quitlines, in the reduction oftobacco use. For the patient motivatedto quit, the addition of pharmacologicaltherapy to counseling is more effectivethan either treatment alone. Special con-siderations should include assessment oflevel of nicotine dependence, which isassociated with difficulty in quitting andrelapse (320).
5. CHD screening and treatmentRecommendationsScreeningc In asymptomatic patients, routinescreening for CAD is not recommended,as it does not improve outcomes as longas CVD risk factors are treated. (A)
Treatmentc In patients with known CVD, considerACE inhibitor therapy (C) and use as-pirin and statin therapy (A) (if notcontraindicated) to reduce the risk ofcardiovascular events. In patients with aprior MI, b-blockers should be contin-ued for at least 2 years after the event. (B)
c Avoid thiazolidinedione treatment inpatients with symptomatic heart fail-ure. (C)
c Metformin may be used in patientswith stable CHF if renal function isnormal. It should be avoided in unstableor hospitalized patients with CHF. (C)
Screening for CAD is reviewed in arecently updated consensus statement(196). To identify the presence of CADin diabetic patients without clear or sug-gestive symptoms, a risk factor–based ap-proach to the initial diagnostic evaluationand subsequent follow-up has intuitiveappeal. However, recent studies con-cluded that using this approach fails toidentify which patients with type 2 diabe-tes will have silent ischemia on screeningtests (201,321).
Candidates for cardiac testing includethose with 1) typical or atypical cardiacsymptoms and 2) an abnormal restingECG. The screening of asymptomatic pa-tients remains controversial. Intensivemedical therapy that would be indicatedanyway for diabetic patients at high riskfor CVD seems to provide equal outcomesto invasive revascularization (322,323).There is also some evidence that silentmyocardial ischemia may reverse overtime, adding to the controversy concern-ing aggressive screening strategies (324).Finally, a recent randomized observa-tional trial demonstrated no clinical ben-efit to routine screening of asymptomaticpatients with type 2 diabetes and normalECGs (325). Despite abnormal myocar-dial perfusion imaging in more than onein five patients, cardiac outcomes wereessentially equal (and very low) inscreened compared with unscreened pa-tients. Accordingly, the overall effective-ness, especially the cost-effectiveness, ofsuch an indiscriminate screening strategyis now questioned.
Newer noninvasive CAD screeningmethods, such as computed tomography(CT) and CT angiography have gained inpopularity. These tests infer the presenceof coronary atherosclerosis by measuringthe amount of calcium in coronary arter-ies and, in some circumstances, bydirect visualization of luminal stenoses.
Although asymptomatic diabetic patientsfound to have a higher coronary diseaseburden have more future cardiac events(326–328), the role of these tests beyondrisk stratification is not clear. Their rou-tine use leads to radiation exposure andmay result in unnecessary invasive testingsuch as coronary angiography and revas-cularization procedures. The ultimatebalance of benefit, cost, and risks ofsuch an approach in asymptomatic pa-tients remains controversial, particularlyin the modern setting of aggressive CVDrisk factor control.
In all patients with diabetes, cardio-vascular risk factors should be assessedat least annually. These risk factorsinclude dyslipidemia, hypertension,smoking, a positive family history ofpremature coronary disease, and thepresence of micro- or macroalbu-minuria. Abnormal risk factors shouldbe treated as described elsewhere inthese guidelines. Patients at increasedCHD risk should receive aspirin and astatin, and ACE inhibitor or ARB therapyif hypertensive, unless there are contra-indications to a particular drug class.Although clear benefit exists for ACEinhibitor and ARB therapy in patientswith nephropathy or hypertension, thebenefits in patients with CVD in theabsence of these conditions are less clear,especially when LDL cholesterol is con-comitantly controlled (329,330).
B. Nephropathy screening andtreatmentRecommendationsGeneral recommendationsc To reduce the risk or slow the progres-sion of nephropathy, optimize glucosecontrol. (A)
c To reduce the risk or slow the pro-gression of nephropathy, optimizeblood pressure control. (A)
Screeningc Perform an annual test to assess urinealbumin excretion in type 1 diabeticpatients with diabetes duration of $5years and in all type 2 diabetic patientsstarting at diagnosis. (B)
c Measure serumcreatinine at least annuallyin all adults with diabetes regardless of thedegree of urine albumin excretion. Theserum creatinine should be used to esti-mate GFR and stage the level of chronickidney disease (CKD), if present. (E)
Treatmentc In the treatment of the nonpregnantpatient with modestly elevated (30–299
S34 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

mg/day) (C) or higher levels ($300mg/day) of urinary albumin excretion(A), either ACE inhibitors or ARBs arerecommended.
c Reduction of protein intake to 0.8–1.0g/kg body wt per day in individualswith diabetes and the earlier stages ofCKD and to 0.8 g/kg body wt per day inthe later stages of CKD may improvemeasures of renal function (urine al-bumin excretion rate, GFR) and isrecommended. (C)
c When ACE inhibitors, ARBs, or diu-retics are used, monitor serum creati-nine and potassium levels for thedevelopment of increased creatinine orchanges in potassium. (E)
c Continued monitoring of urine albu-min excretion to assess both responseto therapy and progression of disease isreasonable. (E)
c When eGFR ,60 mL/min/1.73 m2,evaluate and manage potential com-plications of CKD. (E)
c Consider referral to a physician expe-rienced in the care of kidney disease foruncertainty about the etiology of kid-ney disease, difficult management is-sues, or advanced kidney disease. (B)
Diabetic nephropathy occurs in 20–40%of patients with diabetes and is the singleleading cause of ESRD. Persistent albu-minuria in the range of 30–299 mg/24 h(historically called microalbuminuria)has been shown to be the earliest stageof diabetic nephropathy in type 1 diabetesand a marker for development of nephrop-athy in type 2 diabetes. It is also a well-established marker of increased CVD risk(331,332). Patients with microalbuminuriawho progress to more significant levels($300 mg/24 h, historically called mac-roalbuminuria) are likely to progress toESRD (333,334). However, a number ofinterventions have been demonstrated toreduce the risk and slow the progressionof renal disease.
Intensive diabetes management withthe goal of achieving near-normoglycemiahas been shown in large prospective ran-domized studies to delay the onset andprogression of increased urinary albuminexcretion in patients with type 1(335,336) and type 2 (83,84,88,89) dia-betes. The UKPDS provided strong evi-dence that control of blood pressure canreduce the development of nephropathy(255). In addition, large prospective ran-domized studies in patients with type 1diabetes have demonstrated that achieve-ment of lower levels of systolic blood
pressure (,140 mmHg) resulting fromtreatment using ACE inhibitors provides aselective benefit over other antihyperten-sive drug classes in delaying the progres-sion of increased urinary albumin excretionand can slow the decline in GFR in patientswith higher levels of albuminuria (337–339). In type 2 diabetes with hypertensionand normoalbuminuria, RAS inhibitionhas been demonstrated to delay onset ofmicroalbuminuria (340,341). In the latterstudy, there was an unexpected higher rateof fatal cardiovascular events with olmesar-tan among patients with preexisting CHD.
ACE inhibitors have been shown toreduce major CVD outcomes (i.e., MI,stroke, death) in patients with diabetes(270), thus further supporting the use ofthese agents in patients with albuminuria, aCVD risk factor. ARBs do not prevent onsetof albuminuria in normotensive patientswith type 1 or type 2 diabetes (342,343);however, ARBs have been shown to reducethe rate of progression from micro- to mac-roalbuminuria as well as ESRD in patientswith type 2 diabetes (344–346). Some ev-idence suggests that ARBs have a smallermagnitude of rise in potassium comparedwith ACE inhibitors in people with ne-phropathy (347,348). Combinations ofdrugs that block the renin-angiotensin-aldosterone system (e.g., an ACE inhibitorplus an ARB, a mineralocorticoid antago-nist, or a direct renin inhibitor) provideadditional lowering of albuminuria (349–352). However, such combinations havebeen found to provide no additional car-diovascular benefit and have higher ad-verse event rates (353), and their effectson major renal outcomes have not yetbeen proven.
Other drugs, such as diuretics, cal-cium channel blockers, and b-blockers,should be used as additional therapy tofurther lower blood pressure in patientsalready treated with ACE inhibitors orARBs (275), or as alternate therapy inthe rare individual unable to tolerateACE inhibitors or ARBs.
Studies in patients with varying stagesof nephropathy have shown that proteinrestriction of dietary protein helps slowthe progression of albuminuria, GFR de-cline, and occurrence of ESRD (354–357), although more recent studies haveprovided conflicting results (140). Die-tary protein restriction might be consid-ered particularly in patients whosenephropathy seems to be progressing de-spite optimal glucose and blood pressurecontrol and use of ACE inhibitor and/orARBs (357).
Assessment of albuminuria status andrenal functionScreening for increased urinary albuminexcretion can be performed by measure-ment of the albumin-to-creatinine ratioin a random spot collection; 24-h ortimed collections are more burdensomeand add little to prediction or accuracy(358,359). Measurement of a spot urinefor albumin only, whether by immunoas-say or by using a dipstick test specific formicroalbumin, without simultaneouslymeasuring urine creatinine, is somewhatless expensive but susceptible to false-negative and false-positive determina-tions as a result of variation in urineconcentration due to hydration and otherfactors.
Abnormalities of albumin excretionand the linkage between albumin-to-creatinine ratio and 24-h albumin excre-tion are defined in Table 11. Because ofvariability in urinary albumin excretion,two of three specimens collected within a3- to 6-month period should be abnormalbefore considering a patient to have de-veloped increased urinary albumin excre-tion or had a progression in albuminuria.Exercise within 24 h, infection, fever,CHF, marked hyperglycemia, andmarked hypertension may elevate urinaryalbumin excretion over baseline values.
Information on presence of abnormalurine albumin excretion in addition tolevel of GFR may be used to stage CKD.The National Kidney Foundation classifi-cation (Table 12) is primarily based onGFR levels and therefore differs fromother systems, in which staging is basedprimarily on urinary albumin excretion(360). Studies have found decreasedGFR in the absence of increased urine al-bumin excretion in a substantial percent-age of adults with diabetes (361). Serumcreatinine should therefore be measuredat least annually in all adults with
Table 11dDefinitions of abnormalities inalbumin excretion
CategorySpot collection
(mg/mg creatinine)
Normal ,30Increased urinaryalbumin excretion* $30
*Historically, ratios between 30 and 299 have beencalled microalbuminuria and those 300 or greaterhave been called macroalbuminuria (or clinical al-buminuria).
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S35
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

diabetes, regardless of the degree of urinealbumin excretion.
Serum creatinine should be used toestimate GFR and to stage the level ofCKD, if present. eGFR is commonlycoreported by laboratories or can beestimated using formulae such as theModification of Diet in Renal Disease(MDRD) study equation (362). Recent re-ports have indicated that the MDRD ismore accurate for the diagnosis and strat-ification of CKD in patients with diabetesthan the Cockcroft-Gault formula (363).GFR calculators are available at http://www.nkdep.nih.gov.
The role of continued annual quanti-tative assessment of albumin excretionafter diagnosis of albuminuria and insti-tution of ACE inhibitor or ARB therapyand blood pressure control is unclear.Continued surveillance can assess bothresponse to therapy and progression ofdisease. Some suggest that reducing al-buminuria to the normal (,30 mg/g) ornear-normal range may improve renaland cardiovascular prognosis, but this ap-proach has not been formally evaluated inprospective trials.
Complications of kidney disease cor-relate with level of kidney function.Whenthe eGFR is,60 mL/min/1.73 m2, screen-ing for complications of CKD is indicated(Table 13). Early vaccination against hepa-titis B is indicated in patients likely to prog-ress to end-stage kidney disease.
Consider referral to a physician expe-rienced in the care of kidney disease whenthere is uncertainty about the etiology ofkidney disease (heavy proteinuria, activeurine sediment, absence of retinopathy,rapid decline in GFR, resistant hyperten-sion). Other triggers for referral may in-clude difficult management issues (anemia,secondary hyperparathyroidism,metabolicbone disease, or electrolyte disturbance) oradvanced kidney disease. The threshold forreferral may vary depending on the fre-quency with which a provider encountersdiabetic patients with significant kidney
disease. Consultation with a nephrologistwhen stage 4CKDdevelops has been foundto reduce cost, improve quality of care, andkeep people off dialysis longer (364). How-ever, nonrenal specialists should not delayeducating their patients about the progres-sive nature of diabetic kidney disease; therenal preservation benefits of aggressivetreatment of blood pressure, blood glucose,and hyperlipidemia; and the potential needfor renal replacement therapy.
C. Retinopathy screening andtreatmentRecommendationsGeneral recommendationsc To reduce the risk or slow the pro-gression of retinopathy, optimize gly-cemic control. (A)
c To reduce the risk or slow the pro-gression of retinopathy, optimize bloodpressure control. (A)
Screeningc Adults and children aged $10 yearswith type 1 diabetes should have aninitial dilated and comprehensive eyeexamination by an ophthalmologist oroptometrist within 5 years after theonset of diabetes. (B)
c Patients with type 2 diabetes shouldhave an initial dilated and compre-hensive eye examination by an oph-thalmologist or optometrist shortlyafter the diagnosis of diabetes. (B)
c Subsequent examinations for type 1and type 2 diabetic patients should berepeated annually by an ophthalmologistor optometrist. Less frequent exams(every 2–3 years) may be consideredfollowing one ormore normal eye exams.Examinations will be required more fre-quently if retinopathy is progressing. (B)
c High-quality fundus photographs candetect most clinically significant di-abetic retinopathy. Interpretation ofthe images should be performed by atrained eye care provider. While retinalphotography may serve as a screeningtool for retinopathy, it is not a substitute
for a comprehensive eye exam, whichshould be performed at least initiallyand at intervals thereafter as recom-mended by an eye care professional. (E)
c Womenwith pre-existing diabetes whoare planning pregnancy or who havebecome pregnant should have a com-prehensive eye examination and becounseled on the risk of developmentand/or progression of diabetic reti-nopathy. Eye examination should oc-cur in the first trimester with closefollow-up throughout pregnancy andfor 1 year postpartum. (B)
Treatmentc Promptly refer patients with any levelof macular edema, severe NPDR, or anyPDR to an ophthalmologist who isknowledgeable and experienced in themanagement and treatment of diabeticretinopathy. (A)
c Laser photocoagulation therapy is in-dicated to reduce the risk of vision lossin patients with high-risk PDR, clini-cally significant macular edema, and insome cases of severe NPDR. (A)
c Anti–vascular endothelial growth fac-tor (VEGF) therapy is indicated for di-abetic macular edema. (A)
c The presence of retinopathy is not acontraindication to aspirin therapy forcardioprotection, as this therapy doesnot increase the risk of retinal hemor-rhage. (A)
Diabetic retinopathy is a highly specificvascular complication of both type 1 andtype 2 diabetes, with prevalence stronglyrelated to the duration of diabetes. Di-abetic retinopathy is the most frequentcause of new cases of blindness amongadults aged 20–74 years. Glaucoma, cata-racts, and other disorders of the eye occurearlier and more frequently in people withdiabetes.
In addition to duration of diabetes,other factors that increase the risk of, orare associated with, retinopathy includechronic hyperglycemia (365), nephrop-athy (366), and hypertension (367). In-tensive diabetes management with thegoal of achieving near-normoglycemiahas been shown in large prospective ran-domized studies to prevent and/or delaythe onset and progression of diabetic ret-inopathy (71,83,84,90). Lowering bloodpressure has been shown to decrease theprogression of retinopathy (255), al-though tight targets (systolic ,120mmHg) do not impart additional benefit(90). Several case series and a controlledprospective study suggest that pregnancy
Table 12dStages of CKD
Stage DescriptionGFR (mL/min/1.73 m2
body surface area)
1 Kidney damage* with normal or increased GFR $902 Kidney damage* with mildly decreased GFR 60–893 Moderately decreased GFR 30–594 Severely decreased GFR 15–295 Kidney failure ,15 or dialysis
*Kidney damage defined as abnormalities on pathological, urine, blood, or imaging tests. Adapted from ref.359.
S36 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

in type 1 diabetic patients may aggravateretinopathy (368,369); laser photocoa-gulation surgery can minimize this risk(369).
One of the main motivations forscreening for diabetic retinopathy is thelong-established efficacy of laser photo-coagulation surgery in preventing visualloss. Two large trials, the Diabetic Reti-nopathy Study (DRS) in patients withPDR and the Early Treatment DiabeticRetinopathy Study (ETDRS) in patientswith macular edema, provide the stron-gest support for the therapeutic benefitsof photocoagulation surgery. The DRS(370) showed that panretinal photocoag-ulation surgery reduced the risk of severevision loss from PDR from 15.9% in un-treated eyes to 6.4% in treated eyes, withgreatest risk-benefit ratio in those withbaseline disease (disc neovascularizationor vitreous hemorrhage).
The ETDRS (371) established thebenefit of focal laser photocoagulationsurgery in eyes with macular edema, par-ticularly those with clinically significantmacular edema, with reduction of dou-bling of the visual angle (e.g., 20/50 to20/100) from 20% in untreated eyes to8% in treated eyes. The ETDRS also veri-fied the benefits of panretinal photocoag-ulation for high-risk PDR and in older-onset patients with severe NPDR or less-than-high-risk PDR.
Laser photocoagulation surgery inboth trials was beneficial in reducing therisk of further visual loss, but generally notbeneficial in reversing already diminished
acuity. Recombinant monoclonal neutral-izing antibody to VEGF is a newly ap-proved therapy that improves vision andreduces the need for laser photocoa-gulation in patients with macular edema(372). Other emerging therapies for reti-nopathy include sustained intravitreal de-livery of fluocinolone (373) and thepossibility of prevention with fenofibrate(374,375).
The preventive effects of therapy andthe fact that patients with PDR or macularedema may be asymptomatic providestrong support for a screening programto detect diabetic retinopathy. As retinop-athy is estimated to take at least 5 years todevelop after the onset of hyperglycemia,patients with type 1 diabetes should havean initial dilated and comprehensive eyeexamination within 5 years after the onsetof diabetes. Patients with type 2 diabetes,who generally have had years of undiag-nosed diabetes and who have a significantrisk of prevalent diabetic retinopathy attime of diabetes diagnosis, should have aninitial dilated and comprehensive eye exam-ination soon after diagnosis. Examinationsshould be performed by an ophthalmologistor optometrist who is knowledgeable andexperienced in diagnosing the presence ofdiabetic retinopathy and is aware of itsmanagement. Subsequent examinationsfor type 1 and type 2 diabetic patients aregenerally repeated annually. Less frequentexams (every 2–3 years) may be cost effec-tive after one or more normal eye exams,and in a population with well-controlledtype 2 diabetes there was essentially no
risk of development of significant retinop-athy with a 3-year interval after a normalexamination (376). Examinations will berequired more frequently if retinopathy isprogressing (377).
The use of retinal photography withremote reading by experts has great po-tential in areas where qualified eye careprofessionals are not available and mayalso enhance efficiency and reduce costswhen the expertise of ophthalmologistscan be utilized for more complex exami-nations and for therapy (378). In-personexams are still necessary when the photosare unacceptable and for follow-up of ab-normalities detected. Photos are not asubstitute for a comprehensive eyeexam, which should be performed at leastinitially and at intervals thereafter as rec-ommended by an eye care professional.Results of eye examinations should bedocumented and transmitted to the refer-ring health care professional.
D. Neuropathy screening andtreatmentRecommendationsc All patients should be screened for distalsymmetric polyneuropathy (DPN) start-ing at diagnosis of type 2 diabetes and 5years after the diagnosis of type 1 diabetesand at least annually thereafter, usingsimple clinical tests. (B)
c Electrophysiological testing is rarelyneeded, except in situations where theclinical features are atypical. (E)
c Screening for signs and symptoms ofcardiovascular autonomic neuropathy(CAN) should be instituted at diagnosisof type 2 diabetes and 5 years after thediagnosis of type 1 diabetes. Specialtesting is rarely needed and may notaffect management or outcomes. (E)
c Medications for the relief of specificsymptoms related to painful DPN andautonomic neuropathy are recom-mended, as they improve the quality oflife of the patient. (E)
The diabetic neuropathies are hetero-geneous with diverse clinical manifesta-tions. They may be focal or diffuse. Mostcommon among the neuropathies arechronic sensorimotor DPN and autonomicneuropathy. Although DPN is a diagnosisof exclusion, complex investigations toexclude other conditions are rarely needed.
The early recognition and appropri-ate management of neuropathy in thepatient with diabetes is important for anumber of reasons: 1) nondiabetic
Table 13dManagement of CKD in diabetes
GFR Recommended
All patients Yearly measurement of creatinine, urinary albumin excretion, potassium45–60 Referral to nephrology if possibility for nondiabetic kidney disease exists
(duration of type 1 diabetes ,10 years, heavy proteinuria, abnormalfindings on renal ultrasound, resistant hypertension, rapid fall in GFR,or active urinary sediment on ultrasound)
Consider need for dose adjustment of medicationsMonitor eGFR every 6 monthsMonitor electrolytes, bicarbonate, hemoglobin, calcium, phosphorus,parathyroid hormone at least yearly
Assure vitamin D sufficiencyConsider bone density testingReferral for dietary counseling
30–44 Monitor eGFR every 3 monthsMonitor electrolytes, bicarbonate, calcium, phosphorus, parathyroidhormone, hemoglobin, albumin, weight every 3–6 months
Consider need for dose adjustment of medications,30 Referral to nephrologist
Adapted from http://www.kidney.org/professionals/KDOQI/guideline_diabetes/.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S37
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

neuropathies may be present in patientswith diabetes and may be treatable; 2) anumber of treatment options exist forsymptomatic diabetic neuropathy; 3) upto 50% of DPNmay be asymptomatic andpatients are at risk for insensate injury totheir feet; and 4) autonomic neuropathy,and particularly CAN, is associated withsubstantial morbidity and even mortality.Specific treatment for the underlyingnerve damage is currently not available,other than improved glycemic control,which may modestly slow progression(89) but not reverse neuronal loss. Effec-tive symptomatic treatments are availablefor somemanifestations of DPN (379) andautonomic neuropathy.
Diagnosis of neuropathyDPN. Patients with diabetes should bescreened annually for DPN using testssuch as pinprick sensation, vibration per-ception (using a 128-Hz tuning fork), 10-gmonofilament pressure sensation at thedistal plantar aspect of both great toes andmetatarsal joints, and assessment of anklereflexes. Combinations of more than onetest have .87% sensitivity in detectingDPN. Loss of 10-g monofilament percep-tion and reduced vibration perceptionpredict foot ulcers (380). Importantly, inpatients with neuropathy, particularlywhen severe, causes other than diabetesshould always be considered, such as neu-rotoxic medications, heavy metal poison-ing, alcohol abuse, vitamin B12 deficiency(especially in those taking metformin forprolonged periods (381), renal disease,chronic inflammatory demyelinating neu-ropathy, inherited neuropathies, and vas-culitis (382).Diabetic autonomic neuropathy. Thesymptoms and signs of autonomic dys-function should be elicited carefully dur-ing the history and physical examination.Major clinical manifestations of diabeticautonomic neuropathy include restingtachycardia, exercise intolerance, ortho-static hypotension, constipation, gastro-paresis, erectile dysfunction, sudomotordysfunction, impaired neurovascular func-tion, and, potentially, autonomic failure inresponse to hypoglycemia (383).
CAN, a CVD risk factor (93), is themost studied and clinically importantform of diabetic autonomic neuropathy.CAN may be indicated by resting tachy-cardia (.100 bpm), orthostasis (a fall insystolic blood pressure.20 mmHg uponstanding without an appropriate heartrate response); it is also associated withincreased cardiac event rates. Although
some societies have developed guidelinesfor screening for CAN, the benefits of so-phisticated testing beyond risk stratifica-tion are not clear (384).
Gastrointestinal neuropathies (e.g.,esophageal enteropathy, gastroparesis,constipation, diarrhea, fecal inconti-nence) are common, and any section ofthe gastrointestinal tract may be affected.Gastroparesis should be suspected in in-dividuals with erratic glucose control orwith upper gastrointestinal symptomswithout other identified cause. Evalua-tion of solid-phase gastric emptying usingdouble-isotope scintigraphy may be doneif symptoms are suggestive, but test re-sults often correlate poorly with symp-toms. Constipation is the most commonlower-gastrointestinal symptom but canalternate with episodes of diarrhea.
Diabetic autonomic neuropathy isalso associated with genitourinary tractdisturbances. In men, diabetic autonomicneuropathy may cause erectile dysfunc-tion and/or retrograde ejaculation. Eval-uation of bladder dysfunction should beperformed for individuals with diabeteswho have recurrent urinary tract infec-tions, pyelonephritis, incontinence, or apalpable bladder.
Symptomatic treatmentsDPN. The first step in management ofpatients with DPN should be to aim forstable and optimal glycemic control. Al-though controlled trial evidence is lack-ing, several observational studies suggestthat neuropathic symptoms improve notonly with optimization of control, butalso with the avoidance of extreme bloodglucose fluctuations. Patients with painfulDPN may benefit from pharmacologicaltreatment of their symptoms: manyagents have confirmed or probable effi-cacy confirmed in systematic reviews ofRCTs (379), with several U.S. Food andDrug Administration (FDA)-approved forthe management of painful DPN.Treatment of autonomic neuropathy.Gastroparesis symptoms may improvewith dietary changes and prokineticagents such as metoclopramide or eryth-romycin. Treatments for erectile dysfunc-tion may include phosphodiesterase type5 inhibitors, intracorporeal or intraure-thral prostaglandins, vacuum devices, orpenile prostheses. Interventions for othermanifestations of autonomic neuropathyare described in the ADA statement onneuropathy (380). As with DPN treat-ments, these interventions do not changethe underlying pathology and natural
history of the disease process, but mayhave a positive impact on the quality oflife of the patient.
E. Foot careRecommendationsc For all patients with diabetes, performan annual comprehensive foot exami-nation to identify risk factors predictiveof ulcers and amputations. The footexamination should include inspection,assessment of foot pulses, and testing forloss of protective sensation (LOPS) (10-gmonofilament plus testing any one ofthe following: vibration using 128-Hztuning fork, pinprick sensation, anklereflexes, or vibration perception thresh-old). (B)
c Provide general foot self-care educationto all patients with diabetes. (B)
c A multidisciplinary approach is rec-ommended for individuals with footulcers and high-risk feet, especiallythose with a history of prior ulcer oramputation. (B)
c Refer patients who smoke, have LOPSand structural abnormalities, or havehistory of prior lower-extremity com-plications to foot care specialists forongoing preventive care and lifelongsurveillance. (C)
c Initial screening for peripheral arterialdisease (PAD) should include a historyfor claudication and an assessment ofthe pedal pulses. Consider obtainingan ankle-brachial index (ABI), as manypatients with PAD are asymptom-atic. (C)
c Refer patients with significant claudi-cation or a positive ABI for furthervascular assessment and consider ex-ercise, medications, and surgical op-tions. (C)
Amputation and foot ulceration, con-sequences of diabetic neuropathy and/orPAD, are common and major causes ofmorbidity and disability in people withdiabetes. Early recognition and manage-ment of risk factors can prevent or delayadverse outcomes.
The risk of ulcers or amputations isincreased in people who have the follow-ing risk factors:
c Previous amputationc Past foot ulcer historyc Peripheral neuropathyc Foot deformityc Peripheral vascular diseasec Visual impairment
S38 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

c Diabetic nephropathy (especially pa-tients on dialysis)
c Poor glycemic controlc Cigarette smoking
Many studies have been publishedproposing a range of tests that mightusefully identify patients at risk for footulceration, creating confusion amongpractitioners as to which screening testsshould be adopted in clinical practice. AnADA task force was therefore assembledin 2008 to concisely summarize recentliterature in this area and then recommendwhat should be included in the compre-hensive foot exam for adult patients withdiabetes. Their recommendations are sum-marized below, but clinicians should referto the task force report (385) for furtherdetails and practical descriptions of howto perform components of the comprehen-sive foot examination.
At least annually, all adults with di-abetes should undergo a comprehensivefoot examination to identify high-riskconditions. Clinicians should ask abouthistory of previous foot ulceration oramputation, neuropathic or peripheralvascular symptoms, impaired vision, to-bacco use, and foot care practices. Ageneral inspection of skin integrity andmusculoskeletal deformities should bedone in a well-lit room. Vascular assess-ment would include inspection and as-sessment of pedal pulses.
The neurologic exam recommendedis designed to identify LOPS rather thanearly neuropathy. The clinical examina-tion to identify LOPS is simple andrequires no expensive equipment. Fivesimple clinical tests (use of a 10-g mono-filament, vibration testing using a 128-Hztuning fork, tests of pinprick sensation,ankle reflex assessment, and testing vi-bration perception threshold with a bio-thesiometer), each with evidence fromwell-conducted prospective clinical co-hort studies, are considered useful in thediagnosis of LOPS in the diabetic foot.The task force agrees that any of the fivetests listed could be used by clinicians toidentify LOPS, although ideally two ofthese should be regularly performed dur-ing the screening examdnormally the10-g monofilament and one other test.One or more abnormal tests would sug-gest LOPS, while at least two normal tests(and no abnormal test) would rule outLOPS. The last test listed, vibration as-sessment using a biothesiometer or simi-lar instrument, is widely used in the U.S.;
however, identification of the patient withLOPS can easily be carried out withoutthis or other expensive equipment.
Initial screening for PAD shouldinclude a history for claudication and anassessment of the pedal pulses. A diag-nostic ABI should be performed in anypatient with symptoms of PAD. Due tothe high estimated prevalence of PAD inpatients with diabetes and the fact thatmany patients with PAD are asymptom-atic, an ADA consensus statement on PAD(386) suggested that a screening ABI beperformed in patients over 50 years of ageand be considered in patients under 50years of age who have other PAD risk fac-tors (e.g., smoking, hypertension, hyper-lipidemia, or duration of diabetes .10years). Refer patients with significantsymptoms or a positive ABI for furthervascular assessment and consider exer-cise, medications, and surgical options(386).
Patients with diabetes and high-riskfoot conditions should be educated re-garding their risk factors and appropriatemanagement. Patients at risk should un-derstand the implications of the loss ofprotective sensation, the importance offoot monitoring on a daily basis, theproper care of the foot, including nailand skin care, and the selection of appro-priate footwear. Patients with LOPSshould be educated on ways to substituteother sensory modalities (hand palpation,visual inspection) for surveillance of earlyfoot problems. The patients’ understand-ing of these issues and their physical abil-ity to conduct proper foot surveillanceand care should be assessed. Patientswith visual difficulties, physical con-straints preventing movement, or cogni-tive problems that impair their ability toassess the condition of the foot and to in-stitute appropriate responses will needother people, such as family members,to assist in their care.
People with neuropathy or evidenceof increased plantar pressure (e.g., ery-thema, warmth, callus, or measuredpressure) may be adequately managedwith well-fitted walking shoes or athleticshoes that cushion the feet and redistrib-ute pressure. Callus can be debridedwith a scalpel by a foot care specialistor other health professional with experi-ence and training in foot care. Peoplewith bony deformities (e.g., hammer-toes, prominent metatarsal heads, bun-ions) may need extra-wide or -depthshoes. People with extreme bonydeformities (e.g., Charcot foot) who
cannot be accommodated with commercialtherapeutic footwear may need custom-molded shoes.
Foot ulcers and wound care mayrequire care by a podiatrist, orthopedicor vascular surgeon, or rehabilitationspecialist experienced in the managementof individuals with diabetes. Guidelinesfor treatment of diabetic foot ulcers haverecently been updated (387).
VII. ASSESSMENT OFCOMMON COMORBIDCONDITIONS
Recommendationsc For patients with risk factors, signs orsymptoms, consider assessment andtreatment for common diabetes-asso-ciated conditions (see Table 14). (B)
In addition to the commonly appre-ciated comorbidities of obesity, hyperten-sion, and dyslipidemia, diabetes is alsoassociated with other diseases or condi-tions at rates higher than those of age-matched people without diabetes. A fewof the more common comorbidities aredescribed herein and listed in Table 14.
Hearing impairmentHearing impairment, both high frequencyand low/mid frequency, is more commonin people with diabetes, perhaps due toneuropathy and/or vascular disease. In anNHANES analysis, hearing impairmentwas about twice as great in people withdiabetes compared with those without,after adjusting for age and other riskfactors for hearing impairment (388).Controlling for age, race, and other demo-graphic factors, high frequency loss inthose with diabetes was significantly asso-ciated with history of CHD and with pe-ripheral neuropathy, while low/midfrequency loss was associated with lowHDL cholesterol and with poor reportedhealth status (389).
Table 14dCommon comorbidities for whichincreased risk is associated with diabetes
Hearing impairmentObstructive sleep apneaFatty liver diseaseLow testosterone in menPeriodontal diseaseCertain cancersFracturesCognitive impairmentDepression
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S39
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Obstructive sleep apneaAge-adjusted rates of obstructive sleepapnea, a risk factor for CVD, are signifi-cantly higher (4- to 10-fold) with obesity,especially with central obesity, in menand women (390). The prevalence in gen-eral populations with type 2 diabetes maybe up to 23% (391), and in obese partic-ipants enrolled in the Look AHEAD trialexceeded 80% (392). Treatment of sleepapnea significantly improves quality oflife and blood pressure control. The evi-dence for a treatment effect on glycemiccontrol is mixed (393).
Fatty liver diseaseUnexplained elevation of hepatic trans-aminase concentrations is significantlyassociated with higher BMI, waist circum-ference, triglycerides, and fasting insulin,and with lower HDL cholesterol. Type 2diabetes and hypertension are indepen-dently associated with transaminase ele-vations in women (394). In a prospectiveanalysis, diabetes was significantly associ-ated with incident nonalcoholic chronicliver disease and with hepatocellular car-cinoma (395). Interventions that improvemetabolic abnormalities in patients withdiabetes (weight loss, glycemic control,treatment with specific drugs for hyper-glycemia or dyslipidemia) are also benefi-cial for fatty liver disease (396).
Low testosterone in menMean levels of testosterone are lower inmen with diabetes compared with age-matched men without diabetes, butobesity is a major confounder (397). Theissue of treatment in asymptomatic men iscontroversial. The evidence for effects of tes-tosterone replacement on outcomes ismixed, and recent guidelines suggest thatscreening and treatment of men withoutsymptoms are not recommended (398).
Periodontal diseasePeriodontal disease is more severe, butnot necessarily more prevalent, in pa-tients with diabetes than those without(399). Numerous studies have suggestedassociations with poor glycemic control,nephropathy, and CVD, but most studiesare highly confounded. A comprehensiveassessment, and treatment of identifieddisease, is indicated in patients with dia-betes, but the evidence that periodontaldisease treatment improves glycemic con-trol is mixed. A meta-analysis reported asignificant 0.47% improvement in A1C,but notedmultiple problemswith the qual-ity of the published studies included in the
analysis (400). Several high-quality RCTshave not shown a significant effect (401).
CancerDiabetes (possibly only type 2 diabetes) isassociated with increased risk of cancersof the liver, pancreas, endometrium, co-lon/rectum, breast, and bladder (402).The association may result from sharedrisk factors between type 2 diabetes andcancer (obesity, age, and physical inactiv-ity) but may also be due to hyperinsuline-mia or hyperglycemia (401,403). Patientswith diabetes should be encouragedto undergo recommended age- and sex-appropriate cancer screenings and to re-duce their modifiable cancer risk factors(obesity, smoking, and physical inactivity).
FracturesAge-matched hip fracture risk is signifi-cantly increased in both type 1 (summaryRR 6.3) and type 2 diabetes (summary RR1.7) in both sexes (404). Type 1 diabetesis associated with osteoporosis, but intype 2 diabetes an increased risk of hipfracture is seen despite higher bone min-eral density (BMD) (405). One studyshowed that prevalent vertebral fractureswere significantly more common in menand women with type 2 diabetes, butwere not associated with BMD (406). Inthree large observational studies of olderadults, femoral neck BMD T-score andthe WHO fracture risk algorithm(FRAX) score were associated with hipand nonspine fracture, although fracturerisk was higher in diabetic participantscompared with participants without dia-betes for a given T-score and age or for agiven FRAX score risk (407). It is appro-priate to assess fracture history and riskfactors in older patients with diabetes andrecommend BMD testing if appropriatefor the patient’s age and sex. For at-riskpatients, it is reasonable to consider stan-dard primary or secondary preventionstrategies (reduce risk factors for falls, en-sure adequate calcium and vitamin D in-take, avoid use of medications that lowerBMD, such as glucocorticoids), and to con-sider pharmacotherapy for high-risk pa-tients. For patients with type 2 diabeteswith fracture risk factors, avoiding use ofthiazolidinediones is warranted.
Cognitive impairmentDiabetes is associated with significantlyincreased risk of cognitive decline, agreater rate of cognitive decline, andincreased risk of dementia (408,409).In a 15-year prospective study of a
community-dwelling people over theage of 60 years, the presence of diabetesat baseline significantly increased the age-and sex-adjusted incidence of all-causedementia, Alzheimer disease, and vascu-lar dementia compared with rates in thosewith normal glucose tolerance (410). In asubstudy of the ACCORD study, therewere no differences in cognitive outcomesbetween intensive and standard glycemiccontrol, although there was significantlyless of a decrement in total brain volumeby magnetic resonance imaging in partic-ipants in the intensive arm (411). The ef-fects of hyperglycemia and insulin on thebrain are areas of intense research interest.
DepressionAs discussed in Section V.H, depression ishighly prevalent in people with diabetesand is associated with worse outcomes.
VIII. DIABETES CARE INSPECIFIC POPULATIONS
A. Children and adolescentsRecommendationsc As is the case for all children, childrenwith diabetes or prediabetes should beencouraged to engage in at least 60 minof physical activity each day. (B)
1. Type 1 diabetesThree-quarters of all cases of type 1 di-abetes are diagnosed in individuals ,18years of age. It is appropriate to considerthe unique aspects of care and manage-ment of children and adolescents withtype 1 diabetes. Children with diabetesdiffer from adults in many respects, in-cluding changes in insulin sensitivity re-lated to sexual maturity and physicalgrowth, ability to provide self-care, super-vision in child care and school, andunique neurologic vulnerability to hypo-glycemia and DKA. Attention to such is-sues as family dynamics, developmentalstages, and physiological differences re-lated to sexual maturity are all essentialin developing and implementing an opti-mal diabetes regimen. Although recom-mendations for children and adolescentsare less likely to be based on clinical trialevidence, expert opinion and a review ofavailable and relevant experimental dataare summarized in the ADA statement oncare of children and adolescents with type1 diabetes (412).
Ideally, the care of a child or adoles-cent with type 1 diabetes should be pro-vided by a multidisciplinary team ofspecialists trained in the care of children
S40 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

with pediatric diabetes. At the very least,education of the child and family shouldbe provided by health care providerstrained and experienced in childhooddiabetes and sensitive to the challengesposed by diabetes in this age-group. It isessential that DSME, MNT, and psycho-social support be provided at the time ofdiagnosis and regularly thereafter by in-dividuals experiencedwith the educational,nutritional, behavioral, and emotional needsof the growing child and family. It isexpected that the balance between adultsupervision and self-care should be definedand that it will evolve with physical, psy-chological, and emotional maturity.
a. Glycemic controlRecommendationsc Consider age when setting glycemicgoals in children and adolescents withtype 1 diabetes. (E)
While current standards for diabetesmanagement reflect the need to lowerglucose as safely possible, special consid-eration should be given to the uniquerisks of hypoglycemia in young children.Glycemic goals may need to be modifiedto take into account the fact that mostchildren,6 or 7 years of age have a formof “hypoglycemic unawareness,” includ-ing immaturity and a relative inability torecognize and respond to hypoglycemicsymptoms, placing them at greater riskfor severe hypoglycemia and its sequelae.In addition, and unlike the case in type 1diabetic adults, young children below theage of 5 years may be at risk for perma-nent cognitive impairment after episodesof severe hypoglycemia (413–415). Fur-thermore, the DCCT demonstrated thatnear-normalization of blood glucose lev-els was more difficult to achieve in ado-lescents than adults. Nevertheless, theincreased frequency of use of basal-bolusregimens and insulin pumps in youthfrom infancy through adolescence hasbeen associated with more childrenreaching ADA blood glucose targets(416,417) in those families in whichboth parents and the child with diabetesparticipate jointly to perform the re-quired diabetes-related tasks. Further-more, recent studies documentingneurocognitive sequelae of hyperglyce-mia in children provide another compel-ling motivation for achieving glycemictargets (418,419).
In selecting glycemic goals, the bene-fits on long-term health outcomes ofachieving a lower A1C should be balanced
against the risks of hypoglycemia and thedevelopmental burdens of intensive regi-mens in children and youth. Age-specificglycemic and A1C goals are presented inTable 15.
b. Screening and managementof chronic complications inchildren and adolescentswith type 1 diabetes
i. NephropathyRecommendationsc Annual screening for microalbuminuria,with a random spot urine sample foralbumin-to-creatinine ratio, should beconsidered once the child is 10 years ofage and has had diabetes for 5 years. (B)
c Treatment with an ACE inhibitor, ti-trated to normalization of albumin ex-cretion, should be considered whenelevated albumin-to-creatinine ratio issubsequently confirmed on two addi-tional specimens from different days. (E)
ii. HypertensionRecommendationsc Blood pressure should be measured ateach routine visit. Children found tohave high-normal blood pressure orhypertension should have blood pres-sure confirmed on a separate day. (B)
c Initial treatment of high-normal bloodpressure (systolic or diastolic blood pres-sure consistently above the 90th percen-tile for age, sex, and height) includesdietary intervention and exercise, aimedat weight control and increased physicalactivity, if appropriate. If target bloodpressure is not reached with 3–6 monthsof lifestyle intervention, pharmacologicaltreatment should be considered. (E)
c Pharmacological treatment of hyperten-sion (systolic or diastolic blood pressureconsistently above the 95th percentile forage, sex, and height or consistently.130/80 mmHg, if 95% exceeds thatvalue) should be considered as soon asthe diagnosis is confirmed. (E)
c ACE inhibitors should be consideredfor the initial treatment of hypertension,following appropriate reproductivecounseling due to its potential terato-genic effects. (E)
c The goal of treatment is a blood pres-sure consistently ,130/80 or belowthe 90th percentile for age, sex, andheight, whichever is lower. (E)
It is important that blood pressuremeasurements are determined correctly,using the appropriate size cuff, and withthe child seated and relaxed. Hypertension
should be confirmed on at least threeseparate days. Normal blood pressurelevels for age, sex, and height and appro-priate methods for determinations areavailable online at www.nhlbi.nih.gov/health/prof/heart/hbp/hbp_ped.pdf.
iii. DyslipidemiaRecommendationsScreeningc If there is a family history of hypercho-lesterolemia or a cardiovascular eventbefore age 55 years, or if family history isunknown, then consider obtaining afasting lipid profile on children.2 yearsof age soon after diagnosis (after glucosecontrol has been established). If familyhistory is not of concern, then considerthe first lipid screening at puberty ($10years of age). For children diagnosedwith diabetes at or after puberty, con-sider obtaining a fasting lipid profilesoon after the diagnosis (after glucosecontrol has been established). (E)
c For both age-groups, if lipids are ab-normal, annual monitoring is reason-able. If LDL cholesterol values are withinthe accepted risk levels (,100 mg/dL[2.6 mmol/L]), a lipid profile repeatedevery 5 years is reasonable. (E)
Treatmentc Initial therapy may consist of optimi-zation of glucose control and MNTusing a Step 2 AHA diet aimed at adecrease in the amount of saturated fatin the diet. (E)
c After the age of 10 years, the additionof a statin in patients who, after MNTand lifestyle changes, have LDL choles-terol.160mg/dL (4.1mmol/L), or LDLcholesterol .130 mg/dL (3.4 mmol/L)and one or more CVD risk factors, isreasonable. (E)
c The goal of therapy is an LDL choles-terol value,100mg/dL (2.6mmol/L). (E)
People diagnosed with type 1 diabetesin childhood have a high risk of earlysubclinical (420–422) and clinical (423)CVD. Although intervention data arelacking, the AHA categorizes childrenwith type 1 diabetes in the highest tierfor cardiovascular risk and recommendsboth lifestyle and pharmacological treat-ment for those with elevated LDL choles-terol levels (424,425). Initial therapyshould be with a Step 2 AHA diet, whichrestricts saturated fat to 7% of total calo-ries and restricts dietary cholesterol to200 mg/day. Data from randomized clin-ical trials in children as young as 7monthsof age indicate that this diet is safe and
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S41
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

does not interfere with normal growthand development (426,427).
Neither long-term safety nor cardio-vascular outcome efficacy of statin therapyhas been established for children. How-ever, recent studies have shown short-termsafety equivalent to that seen in adults andefficacy in lowering LDL cholesterol levels,improving endothelial function and caus-ing regression of carotid intimal thickening(428–430). No statin is approved for useunder the age of 10 years, and statin treat-ment should generally not be used in chil-dren with type 1 diabetes prior to this age.For postpubertal girls, issues of pregnancyprevention are paramount, since statins arecategory X in pregnancy. See Section VIII.Bfor more information.
iv. RetinopathyRecommendationsc The first ophthalmologic examinationshould be obtained once the child is$10 years of age and has had diabetesfor 3–5 years. (B)
c After the initial examination, annualroutine follow-up is generally recom-mended. Less frequent examinationsmay be acceptable on the advice of aneye care professional. (E)
Although retinopathy (like albuminuria)most commonly occurs after the onset ofpuberty and after 5–10 years of diabetesduration (431), it has been reported inprepubertal children and with diabetesduration of only 1–2 years. Referrals
should be made to eye care professionalswith expertise in diabetic retinopathy, anunderstanding of the risk for retinopathyin the pediatric population, and experi-ence in counseling the pediatric patientand family on the importance of early pre-vention/intervention.
v. Celiac diseaseRecommendationsc Consider screening children with type1 diabetes for celiac disease by measuringtissue transglutaminase or antiendomysialantibodies, with documentation of nor-mal total serum IgA levels, soon after thediagnosis of diabetes. (E)
c Testing should be considered in chil-dren with growth failure, failure to gainweight, weight loss, diarrhea, flatulence,abdominal pain, or signs of malabsorp-tion or in children with frequent un-explained hypoglycemia or deteriorationin glycemic control. (E)
c Consider referral to a gastroenterolo-gist for evaluation with possible en-doscopy and biopsy for confirmation ofceliac disease in asymptomatic childrenwith positive antibodies. (E)
c Children with biopsy-confirmed celiacdisease should be placed on a gluten-free diet and have consultation with adietitian experienced in managing bothdiabetes and celiac disease. (B)
Celiac disease is an immune-mediated dis-order that occurs with increased frequencyin patients with type 1 diabetes (1–16% of
individuals compared with 0.3–1% in thegeneral population) (432,433). Symptomsof celiac disease include diarrhea, weightloss or poor weight gain, growth failure,abdominal pain, chronic fatigue, malnutri-tion due to malabsorption, and othergastrointestinal problems, and unexplainedhypoglycemia or erratic blood glucose con-centrations.
Screening for celiac disease includesmeasuring serum levels of tissue trans-glutaminase or antiendomysial antibodies,then small bowel biopsy in antibody-positive children. Recent European guide-lines on screening for celiac disease inchildren (not specific to children with type1 diabetes) suggested that biopsy mightnot be necessary in symptomatic childrenwith positive antibodies, as long as furthertesting such as genetic or HLA testing wassupportive, but that asymptomatic but at-risk children should have biopsies (434).One small study that included childrenwith and without type 1 diabetes sugges-ted that antibody-positive but biopsy-neg-ative children were similar clinically tothose who were biopsy positive and thatbiopsy-negative children had benefitsfrom a gluten-free diet but worsening on ausual diet (435). Because this study wassmall and because children with type 1 di-abetes already need to follow a careful diet,it is difficult to advocate for not confirmingthe diagnosis bybiopsy before recommend-ing a lifelong gluten-free diet, especially inasymptomatic children. In symptomaticchildren with type 1 diabetes and celiac
Table 15dPlasma blood glucose and A1C goals for type 1 diabetes by age-group
Values by age (years)
Plasma blood glucose goalrange (mg/dL)
A1C RationaleBeforemeals
Bedtime/overnight
Toddlers and preschoolers (0–6) 100–180 110–200 ,8.5% c Vulnerability to hypoglycemiac Insulin sensitivityc Unpredictability in dietary intake and physical activityc A lower goal (,8.0%) is reasonable if it can beachieved without excessive hypoglycemia
School age (6–12) 90–180 100–180 ,8% c Vulnerability of hypoglycemiac A lower goal (,7.5%) is reasonable if it can beachieved without excessive hypoglycemia
Adolescents and young adults (13–19) 90–130 90–150 ,7.5% c A lower goal (,7.0%) is reasonable if it can beachieved without excessive hypoglycemia
Key concepts in setting glycemic goals:c Goals should be individualized and lower goals may be reasonable based on benefit-risk assessment.c Blood glucose goals should be modified in children with frequent hypoglycemia or hypoglycemia unawareness.c Postprandial blood glucose values should be measured when there is a discrepancy between preprandial blood glucose values and A1Clevels and to help assess glycemia in those on basal/bolus regimens.
S42 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

disease, gluten-free diets reduce symptomsand rates of hypoglycemia (436).
vi. HypothyroidismRecommendationsc Consider screening children with type1 diabetes for thyroid peroxidase andthyroglobulin antibodies soon afterdiagnosis. (E)
c Measuring thyroid-stimulating hor-mone (TSH) concentrations soon afterdiagnosis of type 1 diabetes, after me-tabolic control has been established,is reasonable. If normal, consider re-checking every 1–2 years, especially ifthe patient develops symptoms of thy-roid dysfunction, thyromegaly, or anabnormal growth rate. (E)
Autoimmune thyroiddisease is themostcommon autoimmune disorder associ-ated with diabetes, occurring in 17–30%of patients with type 1 diabetes (437).About one-quarter of type 1 diabetic chil-dren have thyroid autoantibodies at thetime of diagnosis of their diabetes (438),and the presence of thyroid autoantibod-ies is predictive of thyroid dysfunction,generally hypothyroidism but less com-monly hyperthyroidism (439). Subclini-cal hypothyroidism may be associatedwith increased risk of symptomatic hypo-glycemia (440) and with reduced lineargrowth (441). Hyperthyroidism altersglucose metabolism, potentially resultingin deterioration of metabolic control.
c. Self-managementNo matter how sound the medical regi-men, it can only be as good as the abilityof the family and/or individual to imple-ment it. Family involvement in diabetesremains an important component of opti-mal diabetes management throughoutchildhood and adolescence. Health careproviders who care for children and adoles-cents, therefore, must be capable ofevaluating the educational, behavioral, emo-tional, and psychosocial factors that impactimplementation of a treatment plan andmust workwith the individual and family toovercome barriers or redefine goals as ap-propriate.
d. School and day careSince a sizable portion of a child’s day isspent in school, close communicationwith and cooperation of school or daycare personnel is essential for optimal di-abetes management, safety, and maximalacademic opportunities. See the ADA po-sition statement on diabetes care in the
school and day care setting (442) for fur-ther discussion.
e. Transition from pediatric to adultcareRecommendationsc As teens transition into emergingadulthood, health care providers andfamilies must recognize their manyvulnerabilities (B) and prepare the de-veloping teen, beginning in early tomid adolescence and at least 1 yearprior to the transition. (E)
c Both pediatricians and adult healthcare providers should assist in pro-viding support and links to resourcesfor the teen and emerging adult. (B)
Care and close supervision of diabetesmanagement is increasingly shifted fromparents and other older adults through-out childhood and adolescence. How-ever, the shift from pediatrics to adulthealth care providers often occurs veryabruptly as the older teen enters the nextdevelopmental stage referred to as emerg-ing adulthood (443), a critical period foryoung people who have diabetes; duringthis period of major life transitions, youthbegin to move out of their parents’ homeand must become more fully responsiblefor their diabetes care including the manyaspects of self management, making med-ical appointments, and financing healthcare once they are no longer covered un-der their parents’ health insurance(444,445). In addition to lapses in healthcare, this is also a period of deteriorationin glycemic control, increased occurrenceof acute complications, psycho-social-emotional-behavioral issues, and emergenceof chronic complications (444–447).
Though scientific evidence continuesto be limited, it is clear that early andongoing attention be given to compre-hensive and coordinated planning forseamless transition of all youth frompediatric to adult health care (444,445).A comprehensive discussion regardingthe challenges faced during this period,including specific recommendations, isfound in the ADA position statement “Di-abetes Care for Emerging Adults: Recom-mendations for Transition From Pediatricto Adult Diabetes Care Systems” (445).
The National Diabetes Education Pro-gram (NDEP) has materials available tofacilitate the transition process (http://ndep.nih.gov/transitions/), and The EndocrineSociety (in collaboration with the ADAand other organizations has developedtransition tools for clinicians and youth/
families (http://www.endo-society.org/clinicalpractice/transition_of_care.cfm).
2. Type 2 diabetesThe incidence of type 2 diabetes in ado-lescents is increasing, especially in ethnicminority populations (31). Distinctionbetween type 1 and type 2 diabetes inchildren can be difficult, since the preva-lence of overweight in children continuesto rise and since autoantigens and ketosismay be present in a substantial number ofpatients with features of type 2 diabetes(including obesity and acanthosis nigri-cans). Such a distinction at the time ofdiagnosis is critical because treatment reg-imens, educational approaches, and die-tary counsel will differ markedly betweenthe two diagnoses.
Type 2 diabetes has a significant in-cidence of comorbidities already presentat the time of diagnosis (448). It is recom-mended that blood pressure measurement,a fasting lipid profile, microalbuminuria as-sessment, and dilated eye examination beperformed at the time of diagnosis. There-after, screening guidelines and treatmentrecommendations for hypertension, dysli-pidemia, microalbuminuria, and retinopa-thy in youthwith type 2 diabetes are similarto those for youth with type 1 diabetes. Ad-ditional problems that may need to be ad-dressed include polycystic ovarian diseaseand the various comorbidities associatedwith pediatric obesity such as sleep apnea,hepatic steatosis, orthopedic complica-tions, and psychosocial concerns. TheADA consensus statement on this subject(33) provides guidance on the prevention,screening, and treatment of type 2 diabetesand its comorbidities in young people.
3. Monogenic diabetes syndromesMonogenic forms of diabetes (neonataldiabetes or maturity-onset diabetes of theyoung) represent a small fraction of chil-dren with diabetes (,5%), but the readyavailability of commercial genetic testingis now enabling a true genetic diagnosiswith increasing frequency. It is importantto correctly diagnose one of the mono-genic forms of diabetes, as these childrenmay be incorrectly diagnosed with type 1or type 2 diabetes, leading to nonoptimaltreatment regimens and delays in diag-nosing other family members.
The diagnosis of monogenic diabetesshould be considered in the followingsettings: diabetes diagnosed within thefirst 6 months of life; in children withstrong family history of diabetes but with-out typical features of type 2 diabetes
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S43
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

(nonobese, low-risk ethnic group); in chil-drenwithmild fasting hyperglycemia (100–150 mg/dL [5.5–8.5 mmol]), especially ifyoung and nonobese; and in children withdiabetes but with negative autoantibodieswithout signs of obesity or insulin resis-tance. A recent international consensusdocument discusses in further detail the di-agnosis and management of children withmonogenic forms of diabetes (449).
B. Preconception careRecommendationsc A1C levels should be as close to normalas possible (,7%) in an individual pa-tient before conception is attempted. (B)
c Starting at puberty, preconceptioncounseling should be incorporated inthe routine diabetes clinic visit for allwomen of childbearing potential. (C)
c Women with diabetes who are con-templating pregnancy should be eval-uated and, if indicated, treated fordiabetic retinopathy, nephropathy,neuropathy, and CVD. (B)
c Medications used by such womenshould be evaluated prior to conception,since drugs commonly used to treat di-abetes and its complications may becontraindicated or not recommended inpregnancy, including statins, ACE in-hibitors, ARBs, and most noninsulintherapies. (E)
c Since many pregnancies are unplanned,consider the potential risks and benefitsof medications that are contraindicatedin pregnancy in all women of child-bearing potential and counsel womenusing such medications accordingly. (E)
Major congenital malformations re-main the leading cause of mortality andserious morbidity in infants of motherswith type 1 and type 2 diabetes. Obser-vational studies indicate that the risk ofmalformations increases continuouslywith increasing maternal glycemia duringthe first 6–8weeks of gestation, as definedby first-trimester A1C concentrations.There is no threshold for A1C values be-low which risk disappears entirely. How-ever, malformation rates above the 1–2%background rate of nondiabetic pregnan-cies appear to be limited to pregnancies inwhich first-trimester A1C concentrationsare .1% above the normal range for anondiabetic pregnant woman.
Preconception care of diabetes ap-pears to reduce the risk of congenitalmalformations. Five nonrandomizedstudies compared rates of major malfor-mations in infants between women who
participated in preconception diabetescare programs and women who initiatedintensive diabetes management after theywere already pregnant. The preconcep-tion care programsweremultidisciplinaryand designed to train patients in diabetesself-management with diet, intensifiedinsulin therapy, and SMBG. Goals wereset to achieve normal blood glucose con-centrations, and .80% of subjects ach-ieved normal A1C concentrations beforethey became pregnant. In all five studies,the incidence of major congenital malfor-mations in women who participated inpreconception care (range 1.0–1.7% ofinfants) was much lower than the inci-dence in women who did not participate(range 1.4–10.9% of infants) (106). Onelimitation of these studies is that partici-pation in preconception care was self-selected rather than randomized. Thus,it is impossible to be certain that the lowermalformation rates resulted fully fromimproved diabetes care. Nonetheless,the evidence supports the concept thatmalformations can be reduced or preven-ted by careful management of diabetes be-fore pregnancy.
Planned pregnancies greatly facilitatepreconception diabetes care. Unfortu-nately, nearly two-thirds of pregnanciesin women with diabetes are unplanned,leading to a persistent excess of malfor-mations in infants of diabetic mothers. Tominimize the occurrence of these devas-tating malformations, standard care for allwomen with diabetes who have child-bearing potential, beginning at the onsetof puberty or at diagnosis, should include1) education about the risk of malforma-tions associated with unplanned pregnan-cies and poor metabolic control and 2)use of effective contraception at all times,unless the patient has good metaboliccontrol and is actively trying to conceive.
Women contemplating pregnancyneed to be seen frequently by a multidis-ciplinary team experienced in the man-agement of diabetes before and duringpregnancy. The goals of preconceptioncare are to 1) involve and empower thepatient in the management of her diabe-tes, 2) achieve the lowest A1C test resultspossible without excessive hypoglycemia,3) assure effective contraception until sta-ble and acceptable glycemia is achieved,and 4) identify, evaluate, and treat long-term diabetes complications such asretinopathy, nephropathy, neuropathy,hypertension, and CHD (106).
Among the drugs commonly used inthe treatment of patients with diabetes, a
number may be relatively or absolutelycontraindicated during pregnancy. Sta-tins are category X (contraindicated foruse in pregnancy) and should be discon-tinued before conception, as should ACEinhibitors (450). ARBs are category C(risk cannot be ruled out) in the first tri-mester but category D (positive evidenceof risk) in later pregnancy and shouldgenerally be discontinued before preg-nancy. Since many pregnancies are un-planned, health care professionals caringfor any woman of childbearing potentialshould consider the potential risks andbenefits of medications that are contrain-dicated in pregnancy.Women usingmed-ications such as statins or ACE inhibitorsneed ongoing family planning counsel-ing. Among the oral antidiabetic agents,metformin and acarbose are classified ascategory B (no evidence of risk in hu-mans) and all others as category C. Poten-tial risks and benefits of oral antidiabeticagents in the preconception period mustbe carefully weighed, recognizing thatdata are insufficient to establish the safetyof these agents in pregnancy.
For further discussion of preconcep-tion care, see the ADA’s consensus state-ment on pre-existing diabetes andpregnancy (106) and the position state-ment (451) on this subject.
C. Older adultsRecommendationsc Older adults who are functional, cog-nitively intact, and have significant lifeexpectancy should receive diabetescare with goals similar to those de-veloped for younger adults. (E)
c Glycemic goals for some older adultsmight reasonably be relaxed, using in-dividual criteria, but hyperglycemialeading to symptoms or risk of acutehyperglycemic complications shouldbe avoided in all patients. (E)
c Other cardiovascular risk factorsshould be treated in older adults withconsideration of the time frame ofbenefit and the individual patient.Treatment of hypertension is indicatedin virtually all older adults, and lipidand aspirin therapy may benefit thosewith life expectancy at least equal to thetime frame of primary or secondaryprevention trials. (E)
c Screening for diabetes complicationsshould be individualized in olderadults, but particular attention shouldbe paid to complications that wouldlead to functional impairment. (E)
S44 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Diabetes is an important health condi-tion for the aging population; at least 20%of patients over the age of 65 years havediabetes, and this number can be expectedto grow rapidly in the coming decades.Older individuals with diabetes havehigher rates of premature death, functionaldisability, and coexisting illnesses such ashypertension, CHD, and stroke than thosewithout diabetes. Older adults with diabe-tes are also at greater risk than other olderadults for several common geriatric syn-dromes, such as polypharmacy, depres-sion, cognitive impairment, urinaryincontinence, injurious falls, and persistentpain.
A consensus report on diabetes andolder adults (452) influenced the follow-ing discussion and recommendations.The care of older adults with diabetes iscomplicated by their clinical and func-tional heterogeneity. Some older individ-uals developed diabetes years earlier andmay have significant complications; oth-ers who are newly diagnosed may havehad years of undiagnosed diabetes withresultant complications or may have trulyrecent-onset disease and few or no com-plications. Some older adults with diabe-tes are frail and have other underlyingchronic conditions, substantial diabetes-related comorbidity, or limited physicalor cognitive functioning. Other older in-dividuals with diabetes have little comor-bidity and are active. Life expectancies arehighly variable for this population, butoften longer than clinicians realize. Pro-viders caring for older adults with diabe-tes must take this heterogeneity intoconsideration when setting and prioritiz-ing treatment goals.
There are few long-term studies inolder adults demonstrating the benefits ofintensive glycemic, blood pressure, andlipid control. Patients who can beexpected to live long enough to reap thebenefits of long-term intensive diabetesmanagement, who have good cognitiveand functional function, and who chooseto do so via shared decision making maybe treated using therapeutic interventionsand goals similar to those for youngeradults with diabetes. As with all patients,DSME and ongoing DSMS are vital com-ponents of diabetes care for older adultsand their caregivers.
For patients with advanced diabetescomplications, life-limiting comorbid ill-ness, or substantial cognitive or func-tional impairment, it is reasonable to setless intensive glycemic target goals. Thesepatients are less likely to benefit from
reducing the risk of microvascular com-plications and more likely to suffer seri-ous adverse effects from hypoglycemia.However, patients with poorly controlleddiabetes may be subject to acute compli-cations of diabetes, including dehydration,poor wound healing, and hyperglycemichyperosmolar coma. Glycemic goalsat a minimum should avoid these conse-quences.
Although control of hyperglycemiamay be important in older individualswith diabetes, greater reductions in mor-bidity and mortality may result fromcontrol of other cardiovascular risk fac-tors rather than from tight glycemic con-trol alone. There is strong evidence fromclinical trials of the value of treatinghypertension in the elderly (453,454).There is less evidence for lipid-loweringand aspirin therapy, although the benefitsof these interventions for primary andsecondary prevention are likely to applyto older adults whose life expectanciesequal or exceed the time frames seen inclinical trials.
Special care is required in prescribingand monitoring pharmacological therapyin older adults. Costs may be a significantfactor, especially since older adults tendto be on many medications. Metforminmay be contraindicated because of renalinsufficiency or significant heart failure.Thiazolidinediones, if used at all, shouldbe used very cautiously in those with, orat risk for, CHF and have also beenassociated with fractures. Sulfonylureas,other insulin secretagogues, and insulincan cause hypoglycemia. Insulin use re-quires that patients or caregivers have goodvisual and motor skills and cognitive abil-ity. Dipeptidyl peptidase 4 (DPP-4) inhib-itors have few side effects, but their costsmay be a barrier to some older patients; thelatter is also the case for GLP-1 agonists.
Screening for diabetes complicationsin older adults also should be individual-ized. Particular attention should be paidto complications that can develop overshort periods of time and/or that wouldsignificantly impair functional status,such as visual and lower-extremity com-plications.
D. Cystic fibrosis–related diabetesRecommendationsc Annual screening for cystic fibrosis–related diabetes (CFRD) with OGTTshould begin by age 10 years in all pa-tients with cystic fibrosis who do nothave CFRD (B). Use of A1C as a
screening test for CFRD is not recom-mended. (B)
c During a period of stable health, thediagnosis of CFRD can be made incystic fibrosis patients according tousual glucose criteria. (E)
c Patients with CFRD should be treatedwith insulin to attain individualizedglycemic goals. (A)
c Annual monitoring for complicationsof diabetes is recommended, beginning5 years after the diagnosis of CFRD. (E)
CFRD is the most common comorbidityin persons with cystic fibrosis, occurringin about 20% of adolescents and 40–50%of adults. The additional diagnosis of di-abetes in this population is associatedwith worse nutritional status, more severeinflammatory lung disease, and greatermortality from respiratory failure. Insulininsufficiency related to partial fibrotic de-struction of the islet mass is the primarydefect in CFRD. Genetically determinedfunction of the remaining b-cells and in-sulin resistance associated with infectionand inflammation may also play a role.Encouraging new data suggest that earlydetection and aggressive insulin therapyhave narrowed the gap in mortality be-tween cystic fibrosis patients with andwithout diabetes and have eliminatedthe sex difference in mortality (455).
Recommendations for the clinicalmanagement of CFRD can be found inthe recent ADA position statement on thistopic (456).
IX. DIABETES CARE INSPECIFIC SETTINGS
A. Diabetes care in the hospitalRecommendationsc All patients with diabetes admitted to thehospital shouldhave their diabetes clearlyidentified in the medical record. (E)
c All patients with diabetes should havean order for blood glucose monitoring,with results available to all members ofthe health care team. (E)
c Goals for blood glucose levels:c Critically ill patients: Insulin ther-apy should be initiated for treatmentof persistent hyperglycemia startingat a threshold of no greater than 180mg/dL (10 mmol/L). Once insulintherapy is started, a glucose range of140–180 mg/dL (7.8–10 mmol/L) isrecommended for the majority ofcritically ill patients. (A)
c More stringent goals, such as 110–140 mg/dL (6.1–7.8 mmol/L) may be
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S45
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

appropriate for selected patients, aslong as this can be achieved withoutsignificant hypoglycemia. (C)
c Critically ill patients require an intrave-nous insulin protocol that has demon-strated efficacy and safety in achievingthe desired glucose range without in-creasing risk for severe hypoglycemia. (E)
c Non–critically ill patients: There is noclear evidence for specific blood glucosegoals. If treated with insulin, the pre-meal blood glucose targets generally,140 mg/dL (7.8 mmol/L) with ran-domblood glucose,180mg/dL (10.0mmol/L) are reasonable, providedthese targets can be safely achieved.More stringent targets may be appro-priate in stable patients with previoustight glycemic control. Less stringenttargets may be appropriate in thosewith severe comorbidities. (E)
c Scheduled subcutaneous insulin withbasal, nutritional, and correction com-ponents is the preferred method forachieving and maintaining glucose con-trol in non–critically ill patients. (C)
c Glucose monitoring should be initiatedin any patient not known to be diabeticwho receives therapy associated withhigh risk for hyperglycemia, includinghigh-dose glucocorticoid therapy, initi-ation of enteral or parenteral nutrition,or other medications such as octreotideor immunosuppressive medications. (B)If hyperglycemia is documented andpersistent, consider treating such pa-tients to the same glycemic goals as pa-tients with known diabetes. (E)
c A hypoglycemia management protocolshould be adopted and implementedby each hospital or hospital system. Aplan for preventing and treating hypo-glycemia should be established for eachpatient. Episodes of hypoglycemia inthe hospital should be documented inthe medial record and tracked. (E)
c Consider obtaining an A1C on patientswith diabetes admitted to the hospital ifthe result of testing in the previous 2–3months is not available. (E)
c Consider obtaining an A1C in patientswith risk factors for undiagnosed di-abetes who exhibit hyperglycemia inthe hospital. (E)
c Patients with hyperglycemia in thehospital who do not have a prior di-agnosis of diabetes should have ap-propriate plans for follow-up testingand care documented at discharge. (E)
Hyperglycemia in the hospital can re-present previously known diabetes,
previously undiagnosed diabetes, or hos-pital-related hyperglycemia (fastingblood glucose $126 mg/dL or randomblood glucose $200 mg/dL occurringduring the hospitalization that reverts tonormal after hospital discharge). The dif-ficulty distinguishing between the secondand third categories during the hospitali-zation may be overcome by measuring anA1C in undiagnosed patients with hyper-glycemia, as long as conditions interferingwith A1C utility (hemolysis, blood trans-fusion) have not occurred. The manage-ment of hyperglycemia in the hospital hasoften been considered secondary in im-portance to the condition that promptedadmission (457). However, a body of lit-erature now supports targeted glucosecontrol in the hospital setting for poten-tial improved clinical outcomes. Hyper-glycemia in the hospital may result fromstress, decompensation of type 1 or type 2or other forms of diabetes, and/or may beiatrogenic due to withholding of antihy-perglycemic medications or administra-tion of hyperglycemia-provoking agentssuch as glucocorticoids or vasopressors.
There is substantial observational ev-idence linking hyperglycemia in hospital-ized patients (with or without diabetes) topoor outcomes. Cohort studies as wellas a few early RCTs suggested that in-tensive treatment of hyperglycemia im-proved hospital outcomes (457–459). Ingeneral, these studies were heterogeneousin terms of patient population, blood glu-cose targets and insulin protocols used,provision of nutritional support, and theproportion of patients receiving insulin,which limits the ability to make meaning-ful comparisons among them. Recent tri-als in critically ill patients have failed toshow a significant improvement in mor-tality with intensive glycemic control(460,461) or have even shown increasedmortality risk (462). Moreover, these re-cent RCTs have highlighted the risk ofsevere hypoglycemia resulting from suchefforts (460–465).
The largest study to date, NICE-SUGAR (Normoglycaemia in IntensiveCare Evaluation and Survival Using Glu-cose Algorithm Regulation), a multicen-ter, multinational RCT, compared theeffect of intensive glycemic control (target81–108 mg/dL, mean blood glucose at-tained 115 mg/dL) to standard glycemiccontrol (target 144–180 mg/dL, meanblood glucose attained 144 mg/dL) onoutcomes among 6,104 critically ill par-ticipants, almost all of whom required me-chanical ventilation (462). Ninety-day
mortality was significantly higher inthe intensive versus the conventionalgroup in both surgical and medical pa-tients, as was mortality from cardiovascu-lar causes. Severe hypoglycemia was alsomore common in the intensively treatedgroup (6.8% vs. 0.5%, P , 0.001). Theprecise reason for the increased mortalityin the tightly controlled group is un-known. The results of this study lie instark contrast to a famous 2001 single-center study that reported a 42% relativereduction in intensive care unit (ICU)mortality in critically ill surgical patientstreated to a target blood glucose of 80–110mg/dL (458). Importantly, the controlgroup in NICE-SUGAR had reasonablygood blood glucose management, main-tained at a mean glucose of 144 mg/dL,only 29 mg/dL above the intensively man-aged patients. Accordingly, this study’sfindings do not disprove the notion thatglycemic control in the ICU is important.However, they do strongly suggest that itmay not be necessary to target blood glu-cose values,140 mg/dL and that a highlystringent target of,110 mg/dL may actu-ally be dangerous.
In a recent meta-analysis of 26 trials(N5 13,567), which included the NICE-SUGAR data, the pooled RR of death withintensive insulin therapy was 0.93 ascompared with conventional therapy(95% CI 0.83–1.04) (465). Approxi-mately half of these trials reported hypo-glycemia, with a pooled RR of intensivetherapy of 6.0 (95% CI 4.5–8.0). Thespecific ICU setting influenced the find-ings, with patients in surgical ICUs ap-pearing to benefit from intensive insulintherapy (RR 0.63, 95% CI 0.44–0.91),whereas those in other medical andmixed critical care settings did not. Itwas concluded that, overall, intensive in-sulin therapy increased the risk of hypo-glycemia but provided no overall benefiton mortality in the critically ill,although a possible mortality benefit topatients admitted to the surgical ICU wassuggested.
1. Glycemic targets in hospitalizedpatients
Definition of glucose abnormalities inthe hospital settingHyperglycemia in the hospital has beendefined as any blood glucose.140 mg/dL(7.8 mmol/L). Levels that are significantlyand persistently above this may requiretreatment in hospitalized patients. A1Cvalues .6.5% suggest, in undiagnosed
S46 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

patients, that diabetes preceded hospitali-zation (466). Hypoglycemia has been de-fined as any blood glucose ,70 mg/dL(3.9 mmol/L). This is the standard defini-tion in outpatients and correlates with theinitial threshold for the release of counter-regulatory hormones. Severe hypoglyce-mia in hospitalized patients has been de-fined bymany as,40mg/dL (2.2mmol/L),although this is lower than the;50mg/dL(2.8 mmol/L) level at which cognitive im-pairment begins in normal individuals(467). As with hyperglycemia, hypoglyce-mia among inpatients is also associatedwith adverse short- and long-term out-comes. Early recognition and treatmentof mild to moderate hypoglycemia (40–69 mg/dL [2.2–3.8 mmol/L]) can preventdeterioration to a more severe episodewith potential adverse sequelae (468).
Critically ill patientsBased on the weight of the availableevidence, for the majority of critically illpatients in the ICU setting, insulin infusionshould be used to control hyperglycemia,with a starting threshold of no higher than180 mg/dL (10.0 mmol/L). Once intrave-nous insulin is started, the glucose levelshould be maintained between 140 and180mg/dL (7.8 and 10.0mmol/L). Greaterbenefit maybe realized at the lower end ofthis range. Although strong evidence islacking, somewhat lower glucose targetsmay be appropriate in selected patients.One small study suggested that medicalintensive care unit (MICU) patients treatedto targets of 120–140 mg/dL had less neg-ative nitrogen balance than those treated tohigher targets (469). However, targets,110 mg/dL (6.1 mmol/L) are not recom-mended. Use of insulin infusion protocolswith demonstrated safety and efficacy, re-sulting in low rates of hypoglycemia, arehighly recommended (468).
Non–critically ill patientsWith no prospective RCT data to informspecific glycemic targets in non–criticallyill patients, recommendations are basedon clinical experience and judgment(470). For the majority of non–criticallyill patients treated with insulin, premealglucose targets should generally be,140mg/dL (7.8 mmol/L) with random bloodglucose ,180 mg/dL (10.0 mmol/L), aslong as these targets can be safely achieved.To avoid hypoglycemia, considerationshould be given to reassessing the insulinregimen if blood glucose levels fall below100 mg/dL (5.6 mmol/L). Modification ofthe regimen is required when blood
glucose values are ,70 mg/dL (3.9mmol/L), unless the event is easily ex-plained by other factors (such as a missedmeal). There is some evidence that system-atic attention to hyperglycemia in theemergency room leads to better glycemiccontrol in the hospital for those subse-quently admitted (471).
Occasional patients with a prior his-tory of successful tight glycemic control inthe outpatient setting who are clinicallystable may be maintained with a glucoserange below the above cut points. Con-versely, higher glucose ranges may beacceptable in terminally ill patients or inpatients with severe comorbidities, as wellas in those in patient care settings wherefrequent glucose monitoring or closenursing supervision is not feasible.
Clinical judgment, combined withongoing assessment of the patient’s clini-cal status, including changes in the trajec-tory of glucose measures, the severity ofillness, nutritional status, or concurrentuse of medications that might affect glu-cose levels (e.g., steroids, octreotide),must be incorporated into the day-to-day decisions regarding insulin dosing(468).
2. Antihyperglycemic agents inhospitalized patientsIn the hospital setting, insulin therapy isthe preferred method of glycemic controlin majority of clinical situations (468). Inthe ICU, intravenous infusion is the pre-ferred route of insulin administration.When the patient is transitioned off intra-venous insulin to subcutaneous therapy,precautions should be taken to preventhyperglycemia escape (472,473). Outsideof critical care units, scheduled subcuta-neous insulin that delivers basal, nutri-tional, and correction (supplemental)components is preferred. Typical dosingschemes are based on body weight, withsome evidence that patients with renal in-sufficiency should be treated with lowerdoses (474). Prolonged therapy withsliding-scale insulin (SSI) as the soleregimen is ineffective in the majority ofpatients, increases risk of both hypogly-cemia and hyperglycemia, and has re-cently been shown in a randomized trialto be associated with adverse outcomes ingeneral surgery patients with type 2 diabe-tes (475). SSI is potentially dangerous intype 1 diabetes (468). The reader is referredto several recent publications and reviewsthat describe currently available insulinpreparations and protocols and provideguidance in use of insulin therapy in
specific clinical settings including paren-teral nutrition (476), enteral tube feedingsand with high dose glucocorticoid therapy(468).
There are no data on the safety andefficacy of oral agents and injectable non-insulin therapies such as GLP-1 analogsand pramlintide in the hospital. They aregenerally considered to have a limited rolein the management of hyperglycemia inconjunction with acute illness. Continu-ation of these agents may be appropriatein selected stable patients who areexpected to consume meals at regularintervals, and they may be initiated orresumed in anticipation of discharge oncethe patient is clinically stable. Specificcaution is required with metformin, dueto the possibility that a contraindicationmay develop during the hospitalization,such as renal insufficiency, unstable he-modynamic status, or need for an imagingstudy that requires a radio-contrast dye.
3. Preventing hypoglycemiaIn the hospital, multiple risk factors forhypoglycemia are present. Patients withor without diabetes may experience hy-poglycemia in the hospital in associationwith altered nutritional state, heart fail-ure, renal or liver disease, malignancy,infection, or sepsis. Additional triggeringevents leading to iatrogenic hypoglycemiainclude sudden reduction of corticoste-roid dose, altered ability of the patient toreport symptoms, reduction of oral in-take, emesis, new NPO status, inappro-priate timing of short- or rapid-actinginsulin in relation to meals, reduction ofrate of administration of intravenous dex-trose, and unexpected interruption ofenteral feedings or parenteral nutrition.
Despite the preventable nature ofmanyinpatient episodes of hypoglycemia, insti-tutions are more likely to have nursingprotocols for the treatment of hypoglyce-mia than for its prevention. Tracking suchepisodes and analyzing their causes areimportant quality-improvement activities(468).
4. Diabetes care providers in thehospitalInpatient diabetes management may beeffectively championed and/or providedby primary care physicians, endocrinolo-gists, intensivists, or hospitalists. Involve-ment of appropriately trained specialistsor specialty teams may reduce length ofstay, improve glycemic control, and im-prove outcomes (468). In the care of di-abetes, implementation of standardized
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S47
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

order sets for scheduled and correction-dose insulin may reduce reliance onsliding-scale management. As hospitalsmove to comply with “meaningful use”regulations for electronic health records,as mandated by the Health InformationTechnology Act, efforts should be madeto assure that all components of struc-tured insulin order sets are incorporatedinto electronic insulin order sets (477,478).
A team approach is needed to estab-lish hospital pathways. To achieve glyce-mic targets associated with improvedhospital outcomes, hospitals will needmultidisciplinary support to develop in-sulin management protocols that effec-tively and safely enable achievement ofglycemic targets (479).
5. Self-management in the hospitalSelf-management of diabetes in the hos-pital may be appropriate for competentadult patients who have a stable level ofconsciousness, have reasonably stabledaily insulin requirements, successfullyconduct self-management of diabetes athome, have physical skills needed tosuccessfully self-administer insulin andperform SMBG, have adequate oral in-take, and are proficient in carbohydratecounting, use of multiple daily insulininjections or insulin pump therapy, andsick-day management. The patient andphysician, in consultation with nursingstaff, must agree that patient self-management is appropriate under theconditions of hospitalization.
Patients who use CSII pump therapyin the outpatient setting can be candidatesfor diabetes self-management in the hos-pital, provided that they have the mentaland physical capacity to do so (468). Ahospital policy and procedures delineat-ing inpatient guidelines for CSII therapyare advisable, and availability of hospitalpersonnel with expertise in CSII therapyis essential. It is important that nursingpersonnel document basal rates and bolusdoses taken on a regular basis (at leastdaily).
6. MNT in the hospitalThe goals of MNT are to optimize glyce-mic control, to provide adequate caloriesto meet metabolic demands, and tocreate a discharge plan for follow-upcare (457,480). The ADA does not en-dorse any single meal plan or specifiedpercentages of macronutrients, and theterm “ADA diet” should no longer beused. Current nutrition recommenda-tions advise individualization based on
treatment goals, physiological parame-ters, and medication usage. Consistentcarbohydrate meal plans are preferredby many hospitals because they facilitatematching the prandial insulin dose to theamount of carbohydrate consumed (481).Because of the complexity of nutrition is-sues in the hospital, a registered dietitian,knowledgeable and skilled in MNT,should serve as an inpatient team mem-ber. The dietitian is responsible for inte-grating information about the patient’sclinical condition, eating, and lifestylehabits and for establishing treatmentgoals in order to determine a realisticplan for nutrition therapy (482,483).
7. Bedside blood glucose monitoringPOC blood glucose monitoring per-formed at the bedside is used to guideinsulin dosing. In the patient who isreceiving nutrition, the timing of glucosemonitoring should match carbohydrateexposure. In the patient who is not re-ceiving nutrition, glucose monitoring isperformed every 4 to 6 h (484,485). Morefrequent blood glucose testing rangingfrom every 30 min to every 2 h is requiredfor patients on intravenous insulin infusions.
Safety standards should be estab-lished for blood glucose monitoring pro-hibiting sharing of finger-stick lancingdevices, lancets, needles, and meters toreduce the risk of transmission of bloodborne diseases. Shared lancing devices carryessentially the same risk as is conferred fromsharing of syringes and needles (486).
Accuracy of blood glucose measure-ments using POC meters has limitationsthat must be considered. Although theFDA allows a 1/2 20% error for bloodglucose meters, questions about the ap-propriateness of these criteria have beenraised (388). Glucose measures differ sig-nificantly between plasma and wholeblood, terms that are often used inter-changeably and can lead to misinterpre-tation. Most commercially availablecapillary blood glucose meters introduce acorrection factor of ;1.12 to report a“plasma-adjusted” value (487).
Significant discrepancies betweencapillary, venous, and arterial plasmasamples have been observed in patientswith low or high hemoglobin concentra-tions, hypoperfusion, and the presence ofinterfering substances particularlymaltose, as contained in immunoglobu-lins (488). Analytical variability has beendescribed with several POCmeters (489).Increasingly newer generation POC bloodglucose meters correct for variation in
hematocrit and for interfering substances.Any glucose result that does not correlatewith the patient’s status should be con-firmed through conventional laboratorysampling of plasma glucose. The FDAhas become increasingly concerned aboutthe use of POC blood glucose meters inthe hospital and is presently reviewingmatters related to their use.
8. Discharge planning and DSMETransition from the acute care setting is ahigh-risk time for all patients, not just thosewith diabetes or new hyperglycemia. Al-though there is an extensive literatureconcerning safe transition within andfrom the hospital, little of it is specific todiabetes (490). It is important to rememberthat diabetes discharge planning is not aseparate entity, but is part of an overall dis-charge plan. As such, discharge planningbegins at admission to the hospital and isupdated as projected patient needs change.
Inpatients may be discharged to var-ied settings, including home (with orwithout visiting nurse services), assistedliving, rehabilitation, or skilled nursingfacilities. The latter two sites are generallystaffed by health professionals, so diabe-tes discharge planning will be limited tocommunication of medication and dietorders. For the patient who is dischargedto assisted living or to home, the optimalprogram will need to consider the typeand severity of diabetes, the effects of thepatient’s illness on blood glucose levels,and the capacities and desires of the pa-tient. Smooth transition to outpatient careshould be ensured. The Agency for Health-care Research and Quality (AHRQ) recom-mends that at a minimum, discharge plansinclude the following:
c Medication reconciliation: The pa-tient’s medications must be cross-checked to ensure that no chronicmedications were stopped and to en-sure the safety of new prescriptions.
c Whenever possible, prescriptions fornew or changed medication should befilled and reviewedwith the patient andfamily at or before discharge.
c Structured discharge communication:Information on medication changes,pending tests and studies, and follow-upneeds must be accurately and promptlycommunicated to outpatient physicians.
c Discharge summaries should be trans-mitted to the primary physician as soonas possible after discharge.
c Appointment keeping behavior isenhanced when the inpatient team
S48 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

schedules outpatient medical follow-up prior to discharge. Ideally the in-patient care providers or case managers/discharge planners will schedule fol-low-up visit(s) with the appropriateprofessionals, including the primarycare provider, endocrinologist, and di-abetes educator (491).
Teaching diabetes self-management topatients in hospitals is a challenging task.Patients are ill, under increased stress relatedto their hospitalization and diagnosis, andin an environment not conducive to learn-ing. Ideally, people with diabetes should betaught at a time and place conducive tolearning: as an outpatient in a recognizedprogram of diabetes education. For thehospitalized patient, diabetes “survivalskills” education is generally a feasible ap-proach to provide sufficient informationand training to enable safe care at home.Patients hospitalized because of a crisis re-lated to diabetes management or poor careat home need education to prevent subse-quent episodes of hospitalization. An as-sessment of the need for a home healthreferral or referral to an outpatient diabeteseducation program should be part of dis-charge planning for all patients.
DSME cannot wait until discharge,especially in those new to insulin ther-apy or in whom the diabetes regimen hasbeen substantially altered during thehospitalization.
It is recommended that the followingareas of knowledge be reviewed andaddressed prior to hospital discharge:
c Identification of health care providerwho will provide diabetes care afterdischarge
c Level of understanding related to thediagnosis of diabetes, SMBG, and ex-planation of home blood glucose goals
c Definition, recognition, treatment, andprevention of hyperglycemia and hy-poglycemia
c Information on consistent eatingpatterns
c When and how to take blood glucose–loweringmedications including insulinadministration (if going home on in-sulin)
c Sick-day managementc Proper use and disposal of needles andsyringes
It is important that patients be pro-vided with appropriate durable medicalequipment, medication, supplies, andprescriptions at the time of discharge in
order to avoid a potentially dangeroushiatus in care. These supplies/prescrip-tions should include the following:
c Insulin (vials or pens) if neededc Syringes or pen needles (if needed)c Oral medications (if needed)c Blood glucose meter and stripsc Lancets and lancing devicec Urine ketone strips (type 1)c Glucagon emergency kit (insulin-treated)c Medical alert application/charm
More expanded diabetes education canbe arranged in the community. An out-patient follow-up visit with the primarycare provider, endocrinologist, or diabeteseducator within 1 month of discharge isadvised for all patients having hyperglyce-mia in the hospital. Clear communicationwith outpatient providers either directly orvia hospital discharge summaries facilitatessafe transitions to outpatient care. Provid-ing information regarding the cause or theplan for determining the cause of hyper-glycemia, related complications and co-morbidities, and recommended treatmentscan assist outpatient providers as theyassume ongoing care.
B. Diabetes and employmentAny person with diabetes, whether in-sulin treated or noninsulin treated,should be eligible for any employmentfor which he/she is otherwise qualified.Employment decisions should never bebased on generalizations or stereotypesregarding the effects of diabetes. Whenquestions arise about the medical fitnessof a person with diabetes for a particularjob, a health care professional with ex-pertise in treating diabetes should per-form an individualized assessment. Seethe ADA position statement on diabetesand employment (492).
C. Diabetes and drivingA large percentage of people with diabetesin the U.S. and elsewhere seek a license todrive, either for personal or employmentpurposes. There has been considerable de-bate whether, and the extent to which,diabetes may be a relevant factor in de-termining the driver ability and eligibilityfor a license.
People with diabetes are subject to agreat variety of licensing requirements ap-plied by both state and federal jurisdic-tions, which may lead to loss ofemployment or significant restrictionson a person’s license. Presence of a medicalcondition that can lead to significantly
impaired consciousness or cognition maylead to drivers being evaluated for fitness todrive. For diabetes, this typically ariseswhen the person has had a hypoglycemicepisode behind the wheel, even if this didnot lead to a motor vehicle accident.
Epidemiological and simulator datasuggest that people with insulin-treateddiabetes have a small increase in risk ofmotor vehicle accidents, primarily due tohypoglycemia and decreased awarenessof hypoglycemia. This increase (RR 1.12–1.19) is much smaller than the risks asso-ciated with teenage male drivers (RR 42),driving at night (RR 142), driving on ruralroads compared with urban roads (RR9.2), and obstructive sleep apnea (RR2.4), all of which are accepted for unre-stricted licensure.
The ADA position statement on di-abetes and driving (493) recommendsagainst blanket restrictions based on thediagnosis of diabetes and urges individualassessment by a health care professionalknowledgeable in diabetes if restrictionson licensure are being considered. Pa-tients should be evaluated for decreasedawareness of hypoglycemia, hypoglyce-mia episodes while driving, or severe hy-poglycemia. Patients with retinopathy orperipheral neuropathy require assess-ment to determine if those complicationsinterfere with operation of a motor vehi-cle. Health care professionals should becognizant of the potential risk of drivingwith diabetes and counsel their patientsabout detecting and avoiding hypoglyce-mia while driving.
D. Diabetes management incorrectional institutionsPeople with diabetes in correctional facil-ities should receive care that meets na-tional standards. Because it is estimatedthat nearly 80,000 inmates have diabetes,correctional institutions should havewritten policies and procedures for themanagement of diabetes and for trainingof medical and correctional staff in di-abetes care practices. See the ADA posi-tion statement on diabetes managementin correctional institutions (494) for fur-ther discussion.
X. STRATEGIES FORIMPROVING DIABETES CARE
Recommendationsc Care should be aligned with compo-nents of the Chronic Care Model(CCM) to ensure productive inter-actions between a prepared proactive
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S49
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

practice team and an informed acti-vated patient. (A)
c When feasible, care systems shouldsupport team-based care, communityinvolvement, patient registries, andembedded decision support tools tomeet patient needs. (B)
c Treatment decisions should be timelyand based on evidence-based guide-lines that are tailored to individualpatient preferences, prognoses, andcomorbidities. (B)
c A patient-centered communicationstyle should be employed that in-corporates patient preferences, assessesliteracy and numeracy, and addressescultural barriers to care. (B)
There has been steady improvement in theproportion of diabetic patients achievingrecommended levels of A1C, blood pres-sure, and LDL cholesterol in the last 10years, both in primary care settings and inendocrinology practices. Mean A1C na-tionally has declined from 7.82% in 1999–2000 to 7.18% in 2004 based onNHANESdata (495). This has been accompanied byimprovements in lipids and blood pressurecontrol and led to substantial reductions inend-stage microvascular complications inthose with diabetes. Nevertheless in somestudies only 57.1% of adults with diag-nosed diabetes achieved an A1C of ,7%,only 45.5% had a blood pressure,130/80mmHg, and just 46.5% had a total choles-terol ,200 mg/dL, with only 12.2% ofpeople with diabetes achieving all threetreatment goals (496). Evidence also sug-gests that progress in risk factor controlmay be slowing (497). Certain patientgroups, such as patients with complex co-morbidities, financial or other social hard-ships, and/or limited English proficiency,may present particular challenges to goal-based care (498,499). Persistent variationin quality of diabetes care across providersand across practice settings even after ad-justing for patient factors indicates thatthere remains potential for substantial fur-ther improvements in diabetes care.
Although numerous interventions toimprove adherence to the recommendedstandards have been implemented, a ma-jor barrier to optimal care is a deliverysystem that too often is fragmented, lacksclinical information capabilities, oftenduplicates services, and is poorly de-signed for the coordinated delivery ofchronic care. The CCM has been shownin numerous studies to be an effectiveframework for improving the quality ofdiabetes care (500). The CCM includes
six core elements for the provision of op-timal care of patients with chronic dis-ease: 1) delivery system design (movingfrom a reactive to a proactive care deliverysystem where planned visits are coordi-nated through a team based approach),2) self-management support, 3) decisionsupport (basing care on evidence-based,effective care guidelines), 4) clinical infor-mation systems (using registries that canprovide patient-specific and population-based support to the care team), 5)community resources and policies (iden-tifying or developing resources to supporthealthy lifestyles), and 6) health systems(to create a quality-oriented culture). Re-definition of the roles of the clinic staffand promoting self-management on thepart of the patient are fundamental tothe successful implementation of theCCM (501). Collaborative, multidisci-plinary teams are best suited to providesuch care for people with chronicconditions such as diabetes and to facili-tate patients’ performance of appropriateself-management (163,165,220,502).
NDEP maintains an online resource(www.betterdiabetescare.nih.gov) to helphealth care professionals design and im-plement more effective health care deliv-ery systems for those with diabetes. Threespecific objectives, with references to lit-erature that outlines practical strategies toachieve each, are outlined below.
Objective 1: Optimize provider andteam behaviorThe care team should prioritize timely andappropriate intensification of lifestyle and/or pharmaceutical therapy of patients whohave not achieved beneficial levels of bloodpressure, lipid, or glucose control (503).Strategies such as explicit goal settingwith patients (504); identifying and ad-dressing language, numeracy, or culturalbarriers to care (505–508); integrating evi-dence-based guidelines and clinical infor-mation tools into the process of care(509–511); and incorporating caremanage-ment teams including nurses, pharmacists,and other providers (512–515) have eachbeen shown to optimize provider and teambehavior and thereby catalyze reduction inA1C, blood pressure, and LDL cholesterol.
Objective 2: Support patient behaviorchangeSuccessful diabetes care requires a sys-tematic approach to supporting patients’behavior change efforts, including a)healthy lifestyle changes (physical activ-ity, healthy eating, nonuse of tobacco,
weight management, effective coping),b) disease self-management (medicationtaking and management; self-monitoringof glucose and blood pressure when clin-ically appropriate), and c) prevention ofdiabetes complications (self-monitoringof foot health; active participation inscreening for eye, foot, and renal compli-cations; immunizations). High-qualityDSME has been shown to improve patientself-management, satisfaction, and glu-cose control (184,516), as has deliveryof ongoing DSMS so that gains achievedduringDSME are sustained (134,135,152).National DSME standards call for anintegrated approach that includes clinicalcontent and skills, behavioral strategies(goal-setting, problem solving), and ad-dressing emotional concerns in eachneeded curriculum content area.
Objective 3: Change the systemof careThe most successful practices have an in-stitutional priority for providing high qual-ity of care (517). Changes that have beenshown to increase quality of diabetes careinclude basing care on evidence-basedguidelines (518), expanding the role ofteams and staff (501,519), redesigning theprocesses of care (520), implementing elec-tronic health record tools (521,522), acti-vating and educating patients (523,524),and identifying and/or developing and en-gaging community resources and publicpolicy that support healthy lifestyles(525). Recent initiatives such as thePatient-Centered Medical Home showpromise to improve outcomes through co-ordinated primary care and offer new op-portunities for team-based chronic diseasecare (526). Alterations in reimbursementthat reward the provision of appropriateand high-quality care rather than visit-based billing (527) and that can accommo-date the need to personalize care goals mayprovide additional incentives to improvediabetes care (528).
It is clear that optimal diabetes man-agement requires an organized, system-atic approach and involvement of acoordinated team of dedicated healthcare professionals working in an environ-ment where patient-centered high-qualitycare is a priority.
References1. American Diabetes Association. Medical
Management of Type 1 Diabetes. Alexandria,VA, American Diabetes Association, 2012
2. American Diabetes Association. MedicalManagement of Type 2 Diabetes.
S50 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Alexandria, VA, American Diabetes As-sociation, 2012
3. American Diabetes Association. Therapyfor Diabetes Mellitus and Related Dis-orders. Alexandria, VA, American Di-abetes Association, 2009
4. Li R, Zhang P, Barker LE, ChowdhuryFM, Zhang X. Cost-effectiveness of in-terventions to prevent and control di-abetes mellitus: a systematic review.Diabetes Care 2010;33:1872–1894
5. American Diabetes Association. Diagnosisand classification of diabetes mellitus.Diabetes Care 2010;33(Suppl. 1):S62–S69
6. International Expert Committee. In-ternational Expert Committee report onthe role of the A1C assay in the diagnosisof diabetes. Diabetes Care 2009;32:1327–1334
7. Ziemer DC, Kolm P, Weintraub WS,et al. Glucose-independent, black-whitedifferences in hemoglobin A1c levels:a cross-sectional analysis of 2 studies.Ann Intern Med 2010;152:770–777
8. Kumar PR, Bhansali A, RavikiranM, et al.Utility of glycated hemoglobin in di-agnosing type 2 diabetes mellitus:a community-based study. J Clin Endo-crinol Metab 2010;95:2832–2835
9. Selvin E, Steffes MW, Ballantyne CM,Hoogeveen RC, Coresh J, Brancati FL.Racial differences in glycemic markers:a cross-sectional analysis of community-based data. Ann Intern Med 2011;154:303–309
10. Nowicka P, Santoro N, Liu H, et al.Utility of hemoglobin A(1c) for di-agnosing prediabetes and diabetes inobese children and adolescents. DiabetesCare 2011;34:1306–1311
11. Cowie CC, Rust KF, Byrd-Holt DD, et al.Prevalence of diabetes and high risk fordiabetes using A1C criteria in the U.S.population in 1988-2006. Diabetes Care2010;33:562–568
12. Picón MJ, Murri M, Muñoz A,Fern�andez-Garc�ıa JC, Gomez-Huelgas R,Tinahones FJ. Hemoglobin A1c versusoral glucose tolerance test in postpartumdiabetes screening. Diabetes Care 2012;35:1648–1653
13. Expert Committee on the Diagnosis andClassification of Diabetes Mellitus. Re-port of the Expert Committee on theDiagnosis and Classification of DiabetesMellitus. Diabetes Care 1997;20:1183–1197
14. Genuth S, Alberti KG, Bennett P, et al.;Expert Committee on the Diagnosisand Classification of Diabetes Mellitus.Follow-up report on the diagnosis ofdiabetes mellitus. Diabetes Care 2003;26:3160–3167
15. Zhang X, Gregg EW, Williamson DF,et al. A1C level and future risk of di-abetes: a systematic review. DiabetesCare 2010;33:1665–1673
16. Selvin E, Steffes MW, Zhu H, et al. Gly-cated hemoglobin, diabetes, and car-diovascular risk in nondiabetic adults.N Engl J Med 2010;362:800–811
17. Ackermann RT, Cheng YJ, WilliamsonDF, Gregg EW. Identifying adults at highrisk for diabetes and cardiovascular dis-ease using hemoglobin A1c NationalHealth and Nutrition Examination Sur-vey 2005-2006. Am J PrevMed 2011;40:11–17
18. Griffin SJ, Borch-Johnsen K, Davies MJ,et al. Effect of early intensive multifac-torial therapy on 5-year cardiovascularoutcomes in individuals with type 2 di-abetes detected by screening (ADDI-TION-Europe): a cluster-randomisedtrial. Lancet 2011;378:156–167
19. Kahn R, Alperin P, Eddy D, et al. Ageat initiation and frequency of screen-ing to detect type 2 diabetes: a cost-effectiveness analysis. Lancet 2010;375:1365–1374
20. Erickson SC, Le L, Zakharyan A, et al.New-onset treatment-dependent di-abetes mellitus and hyperlipidemia as-sociated with atypical antipsychotic usein older adults without schizophrenia orbipolar disorder. J Am Geriatr Soc 2012;60:474–479
21. Chiu M, Austin PC, Manuel DG, ShahBR, Tu JV. Deriving ethnic-specific BMIcutoff points for assessing diabetes risk.Diabetes Care 2011;34:1741–1748
22. Sheehy A, Pandhi N, Coursin DB, et al.Minority status and diabetes screening inan ambulatory population. DiabetesCare 2011;34:1289–1294
23. Knowler WC, Barrett-Connor E, FowlerSE, et al.; Diabetes Prevention ProgramResearch Group. Reduction in the in-cidence of type 2 diabetes with lifestyleintervention or metformin. N Engl J Med2002;346:393–403
24. Tuomilehto J, Lindström J, Eriksson JG,et al.; Finnish Diabetes Prevention StudyGroup. Prevention of type 2 diabetesmellitus by changes in lifestyle amongsubjects with impaired glucose tolerance.N Engl J Med 2001;344:1343–1350
25. Pan XR, Li GW, Hu YH, et al. Effects ofdiet and exercise in preventing NIDDMin people with impaired glucose toler-ance. The Da Qing IGT and DiabetesStudy. Diabetes Care 1997;20:537–544
26. Buchanan TA, Xiang AH, Peters RK, et al.Preservation of pancreatic beta-cellfunction and prevention of type 2 di-abetes by pharmacological treatment ofinsulin resistance in high-risk Hispanicwomen. Diabetes 2002;51:2796–2803
27. Chiasson JL, Josse RG, Gomis R,HanefeldM, Karasik A, LaaksoM; STOP-NIDDM Trial Research Group. Acarbosefor prevention of type 2 diabetes melli-tus: the STOP-NIDDM randomised trial.Lancet 2002;359:2072–2077
28. Gerstein HC, Yusuf S, Bosch J, et al.;DREAM (Diabetes REduction Assess-ment with ramipril and rosiglitazoneMedication) Trial Investigators. Effect ofrosiglitazone on the frequency of di-abetes in patients with impaired glucosetolerance or impaired fasting glucose:a randomised controlled trial. Lancet2006;368:1096–1105
29. Ramachandran A, Snehalatha C, Mary S,Mukesh B, Bhaskar AD, Vijay V; IndianDiabetes Prevention Programme (IDPP).The Indian Diabetes Prevention Pro-gramme shows that lifestyle modifica-tion and metformin prevent type 2diabetes in Asian Indian subjects withimpaired glucose tolerance (IDPP-1).Diabetologia 2006;49:289–297
30. Johnson SL, Tabaei BP, Herman WH.The efficacy and cost of alternativestrategies for systematic screening fortype 2 diabetes in the U.S. population45-74 years of age. Diabetes Care 2005;28:307–311
31. Dabelea D, D’Agostino RB Jr, Mayer-Davis EJ, et al.; SEARCH for Diabetes inYouth Study Group. Testing the accel-erator hypothesis: body size, beta-cellfunction, and age at onset of type 1(autoimmune) diabetes. Diabetes Care2006;29:290–294
32. Liese AD, D’Agostino RB Jr, HammanRF, et al.; SEARCH for Diabetes in YouthStudy Group. The burden of diabetesmellitus among US youth: prevalenceestimates from the SEARCH for Diabetesin Youth Study. Pediatrics 2006;118:1510–1518
33. American Diabetes Association. Type 2diabetes in children and adolescents.Diabetes Care 2000;23:381–389
34. Pescovitz MD, Greenbaum CJ, Krause-Steinrauf H, et al.; Type 1 DiabetesTrialNet Anti-CD20 Study Group. Rit-uximab, B-lymphocyte depletion, andpreservation of beta-cell function. NEngl J Med 2009;361:2143–2152
35. Orban T, Bundy B, Becker DJ, et al.;Type 1 Diabetes TrialNet AbataceptStudy Group. Co-stimulation modulationwith abatacept in patients with recent-onset type 1 diabetes: a randomised,double-blind, placebo-controlled trial.Lancet 2011;378:412–419
36. Lawrence JM, Contreras R, Chen W,Sacks DA. Trends in the prevalence ofpreexisting diabetes and gestationaldiabetes mellitus among a racially/ethnically diverse population of preg-nant women, 1999-2005. Diabetes Care2008;31:899–904
37. Metzger BE, Lowe LP, Dyer AR, et al.;HAPO Study Cooperative ResearchGroup. Hyperglycemia and adversepregnancy outcomes. N Engl J Med2008;358:1991–2002
38. Metzger BE, Gabbe SG, Persson B, et al.;International Association of Diabetes
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S51
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

and Pregnancy Study Groups ConsensusPanel. International association of di-abetes and pregnancy study groups rec-ommendations on the diagnosis andclassification of hyperglycemia in preg-nancy. Diabetes Care 2010;33:676–682
39. O’Sullivan EP, Avalos G, O’Reilly M,Dennedy MC, Gaffney G, Dunne F; At-lantic DIP collaborators. Atlantic Diabetesin Pregnancy (DIP): the prevalence andoutcomes of gestational diabetes mellitususing newdiagnostic criteria. Diabetologia2011;54:1670–1675
40. Lapolla A, Dalfrà MG, Ragazzi E, De CataAP, Fedele D. New International Asso-ciation of the Diabetes and PregnancyStudy Groups (IADPSG) recommen-dations for diagnosing gestational di-abetes compared with former criteria:a retrospective study on pregnancy out-come. Diabet Med 2011;28:1074–1077
41. Landon MB, Spong CY, Thom E, et al.;Eunice Kennedy Shriver National In-stitute of Child Health and Human De-velopment Maternal-Fetal MedicineUnits Network. A multicenter, random-ized trial of treatment for mild gesta-tional diabetes. N Engl J Med 2009;361:1339–1348
42. Crowther CA, Hiller JE, Moss JR,McPhee AJ, Jeffries WS, Robinson JS;Australian Carbohydrate IntoleranceStudy in Pregnant Women (ACHOIS)Trial Group. Effect of treatment of ges-tational diabetes mellitus on pregnancyoutcomes. N Engl J Med 2005;352:2477–2486
43. Committee on Obstetric Practice. Com-mittee opinion no. 504: screening anddiagnosis of gestational diabetes melli-tus. Obstet Gynecol 2011;118:751–753
44. Kim C, Herman WH, Cheung NW,Gunderson EP, Richardson C. Compar-ison of hemoglobin A1c with fastingplasma glucose and 2-h postchallengeglucose for risk stratification amongwomen with recent gestational diabetesmellitus. Diabetes Care 2011;34:1949–1951
45. Kim C, Newton KM, Knopp RH. Gesta-tional diabetes and the incidence of type2 diabetes: a systematic review. DiabetesCare 2002;25:1862–1868
46. Tobias DK, Hu FB, Chavarro J, Rosner B,Mozaffarian D, Zhang C. Healthful di-etary patterns and type 2 diabetes mel-litus risk among women with a history ofgestational diabetesmellitus. Arch InternMed 2012;172:1566–1572
47. Li G, Zhang P,Wang J, et al. The long-termeffect of lifestyle interventions to preventdiabetes in the China Da Qing DiabetesPrevention Study: a 20-year follow-upstudy. Lancet 2008;371:1783–1789
48. Lindström J, Ilanne-Parikka P, PeltonenM, et al.; Finnish Diabetes PreventionStudy Group. Sustained reduction in theincidence of type 2 diabetes by lifestyle
intervention: follow-up of the FinnishDiabetes Prevention Study. Lancet 2006;368:1673–1679
49. Knowler WC, Fowler SE, Hamman RF,et al.; Diabetes Prevention Program Re-search Group. 10-year follow-up of di-abetes incidence and weight loss in theDiabetes Prevention Program OutcomesStudy. Lancet 2009;374:1677–1686
50. Herman WH, Hoerger TJ, Brandle M,et al.; Diabetes Prevention Program Re-search Group. The cost-effectiveness oflifestyle modification or metformin inpreventing type 2 diabetes in adults withimpaired glucose tolerance. Ann InternMed 2005;142:323–332
51. Diabetes Prevention Program ResearchGroup. The 10-year cost-effectiveness oflifestyle intervention or metformin fordiabetes prevention: an intent-to-treatanalysis of the DPP/DPPOS. DiabetesCare 2012;35:723–730
52. Ackermann RT, Finch EA, Brizendine E,Zhou H, Marrero DG. Translating theDiabetes Prevention Program into thecommunity. The DEPLOY Pilot Study.Am J Prev Med 2008;35:357–363
53. Diabetes Prevention Program ResearchGroup. Long-term safety, tolerability,and weight loss associated with metfor-min in the Diabetes Prevention ProgramOutcomes Study. Diabetes Care 2012;35:731–737
54. DREAM Trial Investigators. Incidence ofdiabetes following ramipril or rosiglita-zone withdrawal. Diabetes Care 2011;34:1265–1269
55. Ratner RE, Christophi CA, Metzger BE,et al.; Diabetes Prevention Program Re-search Group. Prevention of diabetes inwomen with a history of gestational di-abetes: effects of metformin and lifestyleinterventions. J Clin Endocrinol Metab2008;93:4774–4779
56. Orchard TJ, Temprosa M, Barrett-Connor E, et al.; The Diabetes Pre-vention Program Outcomes StudyResearch Group; prepared on behalf ofthe DPPOS Research Group. Long-termeffects of the Diabetes Prevention Pro-gram interventions on cardiovascularrisk factors: a report from the DPP Out-comes Study. Diabet Med. 19 July 2012[Epub ahead of print]
57. Ziegler R, Heidtmann B, Hilgard D,Hofer S, Rosenbauer J, Holl R; DPV-Wiss-Initiative. Frequency of SMBGcorrelates with HbA1c and acute com-plications in children and adolescentswith type 1 diabetes. Pediatr Diabetes2011;12:11–17
58. Farmer A, Wade A, Goyder E, et al. Im-pact of self monitoring of blood glucosein the management of patients with non-insulin treated diabetes: open parallelgroup randomised trial. BMJ 2007;335:132
59. O’Kane MJ, Bunting B, Copeland M,Coates VE; ESMON Study Group. Effi-cacy of self monitoring of blood glucosein patients with newly diagnosed type 2diabetes (ESMON study): randomisedcontrolled trial. BMJ 2008;336:1174–1177
60. Simon J, Gray A, Clarke P, Wade A, NeilA, Farmer A; Diabetes Glycaemic Edu-cation and Monitoring Trial Group. Costeffectiveness of self monitoring of bloodglucose in patients with non-insulintreated type 2 diabetes: economic eval-uation of data from the DiGEM trial. BMJ2008;336:1177–1180
61. Farmer AJ, Perera R, Ward A, et al. Meta-analysis of individual patient data inrandomised trials of self monitoring ofblood glucose in people with non-insulin treated type 2 diabetes. BMJ2012;344:e486
62. Malanda UL, Welschen LMC, RiphagenII, Dekker JM, Nijpels G, Bot SD. Self-monitoring of blood glucose in patientswith type 2 diabetes mellitus who are notusing insulin. Cochrane Database SystRev 2012;2012(Issue 1):CD005060
63. Sacks DB, Arnold M, Bakris GL, et al.;National Academy of Clinical Bio-chemistry. Position statement executivesummary: guidelines and recommenda-tions for laboratory analysis in the di-agnosis and management of diabetesmellitus. Diabetes Care 2011;34:1419–1423
64. Wang J, Zgibor J, Matthews JT, Charron-Prochownik D, Sereika SM, Siminerio L.Self-monitoring of blood glucose is as-sociated with problem-solving skills inhyperglycemia and hypoglycemia. Di-abetes Educ 2012;38:207–218
65. Polonsky WH, Fisher L, Schikman CH,et al. Structured self-monitoring of bloodglucose significantly reduces A1C levelsin poorly controlled, noninsulin-treatedtype 2 diabetes: results from the Struc-tured Testing Program study. DiabetesCare 2011;34:262–267
66. Tamborlane WV, Beck RW, Bode BW,et al.; Juvenile Diabetes Research Foun-dation Continuous Glucose Monitor-ing Study Group. Continuous glucosemonitoring and intensive treatment oftype 1 diabetes. N Engl J Med 2008;359:1464–1476
67. Beck RW, Hirsch IB, Laffel L, et al.; Ju-venile Diabetes Research FoundationContinuous Glucose Monitoring StudyGroup. The effect of continuous glucosemonitoring in well-controlled type 1diabetes. Diabetes Care 2009;32:1378–1383
68. Bergenstal RM, Tamborlane WV,Ahmann A, et al.; STAR 3 Study Group.Effectiveness of sensor-augmented in-sulin-pump therapy in type 1 diabetes. NEngl J Med 2010;363:311–320
S52 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
69. Slover RH, Welsh JB, Criego A, et al.Effectiveness of sensor-augmented pumptherapy in children and adolescents withtype 1 diabetes in the STAR 3 study. Pe-diatr Diabetes 2012;13:6–11
70. Yeh HC, Brown TT, Maruthur N, et al.Comparative effectiveness and safety ofmethods of insulin delivery and glucosemonitoring for diabetes mellitus: a sys-tematic review and meta-analysis. AnnIntern Med 2012;157:336–347
71. The Diabetes Control and ComplicationsTrial Research Group. The effect of in-tensive treatment of diabetes on the de-velopment and progression of long-termcomplications in insulin-dependent di-abetes mellitus. N Engl J Med 1993;329:977–986
72. Stratton IM, Adler AI, Neil HA, et al.Association of glycaemia with macro-vascular and microvascular complica-tions of type 2 diabetes (UKPDS 35):prospective observational study. BMJ2000;321:405–412
73. Cagliero E, Levina EV, Nathan DM. Im-mediate feedback of HbA1c levels im-proves glycemic control in type 1 andinsulin-treated type 2 diabetic patients.Diabetes Care 1999;22:1785–1789
74. Miller CD, Barnes CS, Phillips LS, et al.Rapid A1c availability improves clinicaldecision-making in an urban primarycare clinic. Diabetes Care 2003;26:1158–1163
75. Al-Ansary L, Farmer A, Hirst J, et al.Point-of-care testing for Hb A1c in themanagement of diabetes: a systematicreview and metaanalysis. Clin Chem2011;57:568–576
76. Gialamas A, St John A, Laurence CO,Bubner TK; PoCT Management Com-mittee. Point-of-care testing for patientswith diabetes, hyperlipidaemia or co-agulation disorders in the general prac-tice setting: a systematic review. FamPract 2010;27:17–24
77. Nathan DM, Kuenen J, Borg R, Zheng H,Schoenfeld D, Heine RJ; A1C-DerivedAverage Glucose Study Group. Trans-lating the A1C assay into estimated av-erage glucose values. Diabetes Care2008;31:1473–1478
78. Rohlfing CL, Wiedmeyer HM, Little RR,England JD, Tennill A, Goldstein DE.Defining the relationship betweenplasma glucose and HbA(1c): analysis ofglucose profiles and HbA(1c) in the Di-abetes Control and Complications Trial.Diabetes Care 2002;25:275–278
79. Wilson DM, Kollman; Diabetes Researchin Children Network (DirecNet) StudyGroup. Relationship of A1C to glucoseconcentrations in children with type 1diabetes: assessments by high-frequencyglucose determinations by sensors. Di-abetes Care 2008;31:381–385
80. The Diabetes Control and Complica-tions Trial/Epidemiology of Diabetes
Interventions and Complications Re-search Group. Retinopathy and ne-phropathy in patients with type 1diabetes four years after a trial of in-tensive therapy. N Engl J Med 2000;342:381–389
81. Martin CL, Albers J, Herman WH, et al.;DCCT/EDIC Research Group. Neurop-athy among the diabetes control andcomplications trial cohort 8 years aftertrial completion. Diabetes Care 2006;29:340–344
82. Ohkubo Y, Kishikawa H, Araki E, et al.Intensive insulin therapy prevents theprogression of diabetic microvascularcomplications in Japanese patients withnon-insulin-dependent diabetes melli-tus: a randomized prospective 6-yearstudy. Diabetes Res Clin Pract 1995;28:103–117
83. UK Prospective Diabetes Study (UKPDS)Group. Effect of intensive blood-glucosecontrol with metformin on complica-tions in overweight patients with type 2diabetes (UKPDS 34). Lancet 1998;352:854–865
84. UK Prospective Diabetes Study (UKPDS)Group. Intensive blood-glucose controlwith sulphonylureas or insulin com-pared with conventional treatment andrisk of complications in patients withtype 2 diabetes (UKPDS 33). Lancet1998;352:837–853
85. Holman RR, Paul SK, Bethel MA,Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2diabetes. N Engl J Med 2008;359:1577–1589
86. Duckworth W, Abraira C, Moritz T,et al.; VADT Investigators. Glucosecontrol and vascular complications inveterans with type 2 diabetes. N Engl JMed 2009;360:129–139
87. Moritz T, Duckworth W, Abraira C. Vet-erans Affairs Diabetes Trialdcorrections.N Engl J Med 2009;361:1024–1025
88. Patel A, MacMahon S, Chalmers J, et al.;ADVANCE Collaborative Group. In-tensive blood glucose control and vas-cular outcomes in patients with type 2diabetes. N Engl J Med 2008;358:2560–2572
89. Ismail-Beigi F, Craven T, Banerji MA,et al.; ACCORD Trial Group. Effect ofintensive treatment of hyperglycaemiaon microvascular outcomes in type 2diabetes: an analysis of the ACCORDrandomised trial. Lancet 2010;376:419–430
90. Chew EY, Ambrosius WT, Davis MD,et al.; ACCORD Study Group; ACCORDEye Study Group. Effects of medicaltherapies on retinopathy progression intype 2 diabetes. N Engl J Med 2010;363:233–244
91. Gerstein HC, Miller ME, Byington RP,et al.; Action to Control CardiovascularRisk in Diabetes Study Group. Effects of
intensive glucose lowering in type 2 di-abetes. N Engl J Med 2008;358:2545–2559
92. Nathan DM, Cleary PA, Backlund JY,et al.; Diabetes Control and Compli-cations Trial/Epidemiology of DiabetesInterventions and Complications (DCCT/EDIC) Study Research Group. Intensivediabetes treatment and cardiovasculardisease in patients with type 1 diabetes.N Engl J Med 2005;353:2643–2653
93. Nathan DM, Zinman B, Cleary PA, et al.;Diabetes Control and ComplicationsTrial/Epidemiology of Diabetes Inter-ventions and Complications (DCCT/EDIC) Research Group. Modern-dayclinical course of type 1 diabetes mellitusafter 30 years’ duration: the Diabetes Con-trol and Complications Trial/Epidemiologyof Diabetes Interventions and Complica-tions and Pittsburgh Epidemiology ofDiabetes Complications experience (1983-2005). Arch Intern Med 2009;169:1307–1316
94. Skyler JS, Bergenstal R, Bonow RO, et al.;American Diabetes Association; Ameri-can College of Cardiology Foundation;American Heart Association. Intensiveglycemic control and the prevention ofcardiovascular events: implications ofthe ACCORD, ADVANCE, and VA Di-abetes Trials: a position statement of theAmerican Diabetes Association and ascientific statement of the AmericanCollege of Cardiology Foundation andthe American Heart Association. Di-abetes Care 2009;32:187–192
95. Gerstein HC, Miller ME, Genuth S, et al.;ACCORD Study Group. Long-term ef-fects of intensive glucose lowering oncardiovascular outcomes. N Engl J Med2011;364:818–828
96. Riddle MC, Ambrosius WT, Brillon DJ,et al.; Action to Control CardiovascularRisk in Diabetes Investigators. Epidemi-ologic relationships between A1C andall-cause mortality during a median 3.4-year follow-up of glycemic treatment inthe ACCORD trial. Diabetes Care 2010;33:983–990
97. Bonds DE, Miller ME, Bergenstal RM,et al. The association between symp-tomatic, severe hypoglycaemia andmortality in type 2 diabetes: retrospec-tive epidemiological analysis of the AC-CORD study. BMJ 2010;340:b4909
98. Reaven PD, Moritz TE, Schwenke DC,et al. Intensive glucose-lowering therapyreduces cardiovascular disease events inVeterans Affairs Diabetes Trial participantswith lower calcified coronary atheroscle-rosis. Diabetes 2009;58:2642–2648
99. Duckworth WC, Abraira C, Moritz TE,et al.; Investigators of the VADT. Theduration of diabetes affects the responseto intensive glucose control in type2 subjects: the VA Diabetes Trial.
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S53
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

J Diabetes Complications 2011;25:355–361
100. Turnbull FM, Abraira C, Anderson RJ,et al.; Control Group. Intensive glucosecontrol and macrovascular outcomes intype 2 diabetes. Diabetologia 2009;52:2288–2298
101. Ismail-Beigi F, Moghissi E, Tiktin M,Hirsch IB, Inzucchi SE, Genuth S. In-dividualizing glycemic targets in type 2diabetes mellitus: implications of recentclinical trials. Ann InternMed 2011;154:554–559
102. American Diabetes Association. Post-prandial blood glucose. Diabetes Care2001;24:775–778
103. Ceriello A, Taboga C, Tonutti L, et al.Evidence for an independent and cu-mulative effect of postprandial hyper-triglyceridemia and hyperglycemia onendothelial dysfunction and oxidativestress generation: effects of short- andlong-term simvastatin treatment. Circu-lation 2002;106:1211–1218
104. Raz I,Wilson PW, Strojek K, et al. Effectsof prandial versus fasting glycemia oncardiovascular outcomes in type 2 di-abetes: the HEART2D trial. DiabetesCare 2009;32:381–386
105. Metzger BE, Buchanan TA, Coustan DR,et al. Summary and recommendationsof the Fifth International Workshop-Conference on Gestational DiabetesMellitus. Diabetes Care 2007;30(Suppl.2):S251–S260
106. Kitzmiller JL, Block JM, Brown FM, et al.Managing preexisting diabetes for pr-egnancy: summary of evidence andconsensus recommendations for care.Diabetes Care 2008;31:1060–1079
107. DeWitt DE, Hirsch IB. Outpatient in-sulin therapy in type 1 and type 2 di-abetes mellitus: scientific review. JAMA2003;289:2254–2264
108. Rosenstock J, Dailey G, Massi-BenedettiM, Fritsche A, Lin Z, Salzman A. Re-duced hypoglycemia risk with insulinglargine: a meta-analysis comparing in-sulin glargine with human NPH insulinin type 2 diabetes. Diabetes Care 2005;28:950–955
109. American Diabetes Association. IntensiveDiabetes Management. Alexandria, VA,American Diabetes Association, 2009
110. Mooradian AD, BernbaumM, Albert SG.Narrative review: a rational approach tostarting insulin therapy. Ann Intern Med2006;145:125–134
111. Inzucchi SE, Bergenstal RM, Buse JB,et al.; American Diabetes Association(ADA); European Association for theStudy of Diabetes (EASD). Managementof hyperglycemia in type 2 diabetes:a patient-centered approach. PositionStatement of the American Diabetes As-sociation (ADA) and the European As-sociation for the Study of Diabetes
(EASD). Diabetes Care 2012;35:1364–1379
112. Bennett WL, Maruthur NM, Singh S,et al. Comparative effectiveness andsafety of medications for type 2 diabetes:an update including new drugs and 2-drug combinations. Ann Intern Med2011;154:602–613
113. Blonde L,MerilainenM, Karwe V, RaskinP; TITRATE Study Group. Patient-di-rected titration for achieving glycaemicgoals using a once-daily basal insulinanalogue: an assessment of two differentfasting plasma glucose targets–theTITRATE study. Diabetes Obes Metab2009;11:623–631
114. Bantle JP, Wylie-Rosett J, Albright AL,et al.; American Diabetes Association.Nutrition recommendations and inter-ventions for diabetes: a position statementof the American Diabetes Association.Diabetes Care 2008;31(Suppl. 1):S61–S78
115. DAFNE Study Group. Training in flexi-ble, intensive insulin management toenable dietary freedom in people withtype 1 diabetes: dose adjustment fornormal eating (DAFNE) randomisedcontrolled trial. BMJ 2002;325:746
116. Franz MJ, Monk A, Barry B, et al. Effec-tiveness of medical nutrition therapyprovided by dietitians in the manage-ment of non-insulin-dependent diabetesmellitus: a randomized, controlled clinicaltrial. J Am Diet Assoc 1995;95:1009–1017
117. Goldhaber-Fiebert JD, Goldhaber-FiebertSN, Trist�anML,NathanDM. Randomizedcontrolled community-based nutritionand exercise intervention improves gly-cemia and cardiovascular risk factors intype 2 diabetic patients in ruralCosta Rica.Diabetes Care 2003;26:24–29
118. Lemon CC, Lacey K, Lohse B, HubacherDO, Klawitter B, Palta M. Outcomesmonitoring of health, behavior, andquality of life after nutrition interventionin adults with type 2 diabetes. J Am DietAssoc 2004;104:1805–1815
119. Miller CK, Edwards L, Kissling G,Sanville L. Nutrition education improvesmetabolic outcomes among older adultswith diabetes mellitus: results from arandomized controlled trial. Prev Med2002;34:252–259
120. Wilson C, Brown T, Acton K, Gilliland S.Effects of clinical nutrition educationand educator discipline on glycemiccontrol outcomes in the Indian HealthService. Diabetes Care 2003;26:2500–2504
121. Graber AL, Elasy TA, Quinn D, Wolff K,Brown A. Improving glycemic control inadults with diabetes mellitus: shared re-sponsibility in primary care practices.South Med J 2002;95:684–690
122. Gaetke LM, Stuart MA, Truszczynska H.A single nutrition counseling session
with a registered dietitian improvesshort-term clinical outcomes for ruralKentucky patients with chronic diseases.J Am Diet Assoc 2006;106:109–112
123. Van Horn L, McCoin M, Kris-EthertonPM, et al. The evidence for dietary pre-vention and treatment of cardiovasculardisease. J Am Diet Assoc 2008;108:287–331
124. Appel LJ, Moore TJ, Obarzanek E, et al.;DASH Collaborative Research Group. Aclinical trial of the effects of dietary pat-terns on blood pressure. N Engl J Med1997;336:1117–1124
125. FranzMJ, VanWormer JJ, Crain AL, et al.Weight-loss outcomes: a systematic reviewand meta-analysis of weight-loss clinicaltrials with a minimum 1-year follow-up. JAm Diet Assoc 2007;107:1755–1767
126. Foster GD, Wyatt HR, Hill JO, et al. Arandomized trial of a low-carbohydratediet for obesity. N Engl J Med 2003;348:2082–2090
127. Stern L, Iqbal N, Seshadri P, et al. Theeffects of low-carbohydrate versus con-ventional weight loss diets in severelyobese adults: one-year follow-up of arandomized trial. Ann Intern Med 2004;140:778–785
128. Foster GD, Wyatt HR, Hill JO, et al.Weight and metabolic outcomes after 2years on a low-carbohydrate versus low-fat diet: a randomized trial. Ann InternMed 2010;153:147–157
129. Shai I, Schwarzfuchs D, Henkin Y, et al.;Dietary Intervention Randomized Con-trolled Trial (DIRECT) Group. Weightloss with a low-carbohydrate, Mediter-ranean, or low-fat diet. N Engl J Med2008;359:229–241
130. Nordmann AJ, Nordmann A, Briel M,et al. Effects of low-carbohydrate vs low-fat diets on weight loss and cardiovas-cular risk factors: a meta-analysis ofrandomized controlled trials. Arch In-tern Med 2006;166:285–293
131. Norris SL, Zhang X, Avenell A, et al.Long-term effectiveness of weight-lossinterventions in adults with pre-diabetes: a review. Am J Prev Med 2005;28:126–139
132. Salas-Salvado J, Bullo M, Babio N, et al.Reduction in the incidence of type 2 di-abetes with the Mediterranean diet: re-sults of the PREDIMED-Reus nutritionintervention randomized trial. DiabetesCare 2011;34:14–19
133. Malik VS, Popkin BM, Bray GA, DesprésJP, Willett WC, Hu FB. Sugar-sweetenedbeverages and risk of metabolic syn-drome and type 2 diabetes: a meta-analysis. Diabetes Care 2010;33:2477–2483
134. Klein S, Sheard NF, Pi-Sunyer X, et al.;American Diabetes Association; NorthAmerican Association for the Study ofObesity; American Society for ClinicalNutrition. Weight management through
S54 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
lifestyle modification for the preventionand management of type 2 diabetes: ra-tionale and strategies. A statement ofthe American Diabetes Association, theNorth American Association for theStudy of Obesity, and the American So-ciety for Clinical Nutrition. DiabetesCare 2004;27:2067–2073
135. Norris SL, Zhang X, Avenell A, et al. Ef-ficacy of pharmacotherapy for weightloss in adults with type 2 diabetes mel-litus: a meta-analysis. Arch Intern Med2004;164:1395–1404
136. Wolf AM, Conaway MR, Crowther JQ,et al.; Translating lifestyle intervention topractice in obese patients with type 2diabetes: Improving Control with Ac-tivity and Nutrition (ICAN) study. Di-abetes Care 2004;27:1570–1576
137. Manning RM, Jung RT, Leese GP,Newton RW. The comparison of fourweight reduction strategies aimed atoverweight patients with diabetes melli-tus: four-year follow-up. Diabet Med1998;15:497–502
138. Pi-Sunyer X, Blackburn G, Brancati FL,et al.; Look AHEAD Research Group.Reduction in weight and cardiovasculardisease risk factors in individuals withtype 2 diabetes: one-year results of thelook AHEAD trial. Diabetes Care 2007;30:1374–1383
139. Wing RR; Look AHEAD ResearchGroup. Long-term effects of a lifestyleintervention on weight and cardiovas-cular risk factors in individuals with type2 diabetes mellitus: four-year results ofthe Look AHEAD trial. Arch Intern Med2010;170:1566–1575
140. Wheeler ML, Dunbar SA, Jaacks LM,et al. Macronutrients, food groups, andeating patterns in the management ofdiabetes: a systematic review of the lit-erature, 2010. Diabetes Care 2012;35:434–445
141. Esposito K, Maiorino MI, Ciotola M,et al. Effects of aMediterranean-style dieton the need for antihyperglycemic drugtherapy in patients with newly di-agnosed type 2 diabetes: a randomizedtrial. Ann Intern Med 2009;151:306–314
142. Barnard ND, Cohen J, Jenkins DJ, et al. Alow-fat vegan diet improves glycemiccontrol and cardiovascular risk factorsin a randomized clinical trial in in-dividuals with type 2 diabetes. DiabetesCare 2006;29:1777–1783
143. Turner-McGrievy GM, Barnard ND,Cohen J, Jenkins DJ, Gloede L, GreenAA. Changes in nutrient intake and di-etary quality among participants withtype 2 diabetes following a low-fat vegandiet or a conventional diabetes diet for22 weeks. J Am Diet Assoc 2008;108:1636–1645
144. Institute of Medicine. Dietary ReferenceIntakes: Energy, Carbohydrate, Fiber, Fat,
Fatty Acids, Cholesterol, Protein, andAmino Acids. Washington, DC, NationalAcademies Press, 2002
145. Franz MJ, Bantle JP, Beebe CA, et al.Evidence-based nutrition principles andrecommendations for the treatment andprevention of diabetes and related com-plications. Diabetes Care 2002;25:148–198
146. Norris SL, Engelgau MM, Narayan KM.Effectiveness of self-management train-ing in type 2 diabetes: a systematic re-view of randomized controlled trials.Diabetes Care 2001;24:561–587
147. Norris SL, Lau J, Smith SJ, Schmid CH,Engelgau MM. Self-management educa-tion for adults with type 2 diabetes: ameta-analysis of the effect on glycemic control.Diabetes Care 2002;25:1159–1171
148. Gary TL, Genkinger JM, Guallar E,Peyrot M, Brancati FL. Meta-analysis ofrandomized educational and behavioralinterventions in type 2 diabetes. DiabetesEduc 2003;29:488–501
149. Steed L, CookeD,Newman S. A systematicreview of psychosocial outcomes followingeducation, self-management and psycho-logical interventions in diabetes mellitus.Patient Educ Couns 2003;51:5–15
150. Ellis SE, Speroff T, Dittus RS, Brown A,Pichert JW, Elasy TA. Diabetes patienteducation: a meta-analysis and meta-regression. Patient Educ Couns 2004;52:97–105
151. Warsi A,Wang PS, LaValleyMP, Avorn J,Solomon DH. Self-management educa-tion programs in chronic disease: a sys-tematic review and methodologicalcritique of the literature. Arch InternMed 2004;164:1641–1649
152. Haas L, Maryniuk M, Beck J, et al.; onbehalf of the 2012 Standards RevisionTask Force. National Standards for Di-abetes Self-Management Education andSupport. Diabetes Care 2012;35:2393–2401
153. Mulcahy K, Maryniuk M, Peeples M,et al. Diabetes self-management educa-tion core outcomes measures. DiabetesEduc 2003;29:768–803
154. Glasgow RE, Peeples M, Skovlund SE.Where is the patient in diabetes perfor-mance measures? The case for includingpatient-centered and self-managementmeasures. Diabetes Care 2008;31:1046–1050
155. Barker JM, Goehrig SH, Barriga K, et al.;DAISY study. Clinical characteristics ofchildren diagnosed with type 1 diabetesthrough intensive screening and follow-up. Diabetes Care 2004;27:1399–1404
156. Heinrich E, Schaper NC, de Vries NK.Self-management interventions for type2 diabetes: a systematic review. Eur Di-abetes Nurs 2010;7:71–76
157. Frosch DL, Uy V, Ochoa S, MangioneCM. Evaluation of a behavior supportintervention for patients with poorly
controlled diabetes. Arch Intern Med2011;171:2011–2017
158. McGowan P. The efficacy of diabetespatient education and self-managementeducation in type 2 diabetes. Can J Di-abetes 2011;35:46–53
159. Cochran J, Conn VS. Meta-analysis ofquality of life outcomes following di-abetes self-management training. Di-abetes Educ 2008;34:815–823
160. Fisher EB, Thorpe CT, Devellis BM,Devellis RF. Healthy coping, negativeemotions, and diabetes management:a systematic review and appraisal. Di-abetes Educ 2007;33:1080–1103; dis-cussion 1104–1106
161. Robbins JM, Thatcher GE, Webb DA,Valdmanis VG. Nutritionist visits, di-abetes classes, and hospitalization ratesand charges: the Urban Diabetes Study.Diabetes Care 2008;31:655–660
162. Polonsky WH, Earles J, Smith S, et al.Integrating medical management withdiabetes self-management training: a ran-domized control trial of the DiabetesOutpatient Intensive Treatment program.Diabetes Care 2003;26:3048–3053
163. Piatt GA, Anderson RM, Brooks MM,et al. 3-year follow-up of clinical andbehavioral improvements following amultifaceted diabetes care intervention:results of a randomized controlled trial.Diabetes Educ 2010;36:301–309
164. Tang TS, Funnell MM, Brown MB,Kurlander JE. Self-management supportin “real-world” settings: an empower-ment-based intervention. Patient EducCouns 2010;79:178–184
165. Renders CM, Valk GD, Griffin S, WagnerEH, Eijk JT, Assendelft WJ. Interventionsto improve the management of diabetesmellitus in primary care, outpatient andcommunity settings. Cochrane DatabaseSyst Rev 2001;(1):CD001481
166. Glazier RH, Bajcar J, Kennie NR,WillsonK. A systematic review of interventionsto improve diabetes care in socially dis-advantaged populations. Diabetes Care2006;29:1675–1688
167. Hawthorne K, Robles Y, Cannings-JohnR, Edwards AG. Culturally appropriatehealth education for type 2 diabetesmellitus in ethnic minority groups. Co-chrane Database Syst Rev 2008;(3):CD006424
168. Sarkisian CA, Brown AF, Norris KC,Wintz RL, Mangione CM. A systematicreview of diabetes self-care interventionsfor older, African American, or Latinoadults. Diabetes Educ 2003;29:467–479
169. Chodosh J, Morton SC, Mojica W, et al.Meta-analysis: chronic disease self-management programs for older adults.Ann Intern Med 2005;143:427–438
170. Peyrot M, Rubin RR. Behavioral andpsychosocial interventions in diabetes:
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S55
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

a conceptual review. Diabetes Care2007;30:2433–2440
171. Anderson DR, Christison-Legay J,Proctor-Gray E. Self-Management goalsetting in a community health center: theimpact of goal attainment on diabetesoutcomes. Diabetes Spectrum 2010;23:97–106
172. Deakin T, McShane CE, Cade JE,Williams RD. Group based training forself-management strategies in peoplewith type 2 diabetes mellitus. CochraneDatabase Syst Rev 2005;(2):CD003417
173. Duke SA, Colagiuri S, Colagiuri R. In-dividual patient education for peoplewith type 2 diabetes mellitus. CochraneDatabase Syst Rev 2009;(1):CD005268
174. Heisler M, Vijan S, Makki F, Piette JD.Diabetes control with reciprocal peersupport versus nurse care management:a randomized trial. Ann Intern Med2010;153:507–515
175. Heisler M. Different models to mobilizepeer support to improve diabetes self-management and clinical outcomes:evidence, logistics, evaluation consid-erations and needs for future research.Fam Pract 2010;27(Suppl. 1):i23–i32
176. Long JA, Jahnle EC, Richardson DM,Loewenstein G, Volpp KG. Peermentoring and financial incentives toimprove glucose control in AfricanAmerican veterans: a randomized trial.Ann Intern Med 2012;156:416–424
177. Tang TS, Funnell MM, Gillard M,Nwankwo R,HeislerM. The developmentof a pilot training program for peer leadersin diabetes: process and content. DiabetesEduc 2011;37:67–77
178. Tang T, Ayala GX, Cherrington A, RanaG. A review of volunteer-based peersupport interventions in diabetes. Di-abetes Spectrum 2011;24:85–98
179. Tang TS, Nwankwo R, Whiten Y, OneyC. Training peers to deliver a church-based diabetes prevention program. Di-abetes Educ 2012;38:519–525
180. Dale JR,Williams SM, Bowyer V.What isthe effect of peer support on diabetesoutcomes in adults? A systematic review.Diabet Med 2012;29:1361–1377
181. Foster G, Taylor SJ, Eldridge SE, RamsayJ, Griffiths CJ. Self-management educa-tion programmes by lay leaders forpeople with chronic conditions. Co-chrane Database Syst Rev 2007;(4):CD005108
182. Norris SL, Chowdhury FM, Van Le K,et al. Effectiveness of community healthworkers in the care of persons with di-abetes. Diabet Med 2006;23:544–556
183. Johnson TM, Murray MR, Huang Y. As-sociations between self-managementeducation and comprehensive diabetesclinical care. Diabetes Spectrum 2010;23:41–46
184. Duncan I, Birkmeyer C, Coughlin S, LiQE, Sherr D, Boren S. Assessing the
value of diabetes education. DiabetesEduc 2009;35:752–760
185. Duncan I, Ahmed T, Li QE, et al. As-sessing the value of the diabetes educa-tor. Diabetes Educ 2011;37:638–657
186. Kramer MK, McWilliams JR, Chen HY,Siminerio LM. A community-based di-abetes prevention program: evaluationof the group lifestyle balance programdelivered by diabetes educators. Di-abetes Educ 2011;37:659–668
187. Boulé NG, Haddad E, Kenny GP, WellsGA, Sigal RJ. Effects of exercise on gly-cemic control and body mass in type 2diabetes mellitus: a meta-analysis ofcontrolled clinical trials. JAMA 2001;286:1218–1227
188. Boulé NG, Kenny GP, Haddad E, WellsGA, Sigal RJ. Meta-analysis of the effectof structured exercise training on cardio-respiratory fitness in Type 2 diabetes mel-litus. Diabetologia 2003;46:1071–1081
189. Colberg SR, Sigal RJ, Fernhall B, et al.Exercise and type 2 diabetes. TheAmerican College of Sports Medicineand the American Diabetes Association:joint position statement. Diabetes Care2010;33:2692–2696
190. U.S. Department of Health and HumanServices. 2008 Physical Activity Guide-lines for Americans [article online],2008. Available from http://www.health.gov/paguidelines/guidelines/default.aspx. Accessed October 2012
191. Cauza E, Hanusch-Enserer U, Strasser B,et al. The relative benefits of enduranceand strength training on the metabolicfactors and muscle function of peoplewith type 2 diabetes mellitus. Arch PhysMed Rehabil 2005;86:1527–1533
192. Dunstan DW, Daly RM, Owen N, et al.High-intensity resistance training im-proves glycemic control in older patientswith type 2 diabetes. Diabetes Care2002;25:1729–1736
193. Castaneda C, Layne JE, Munoz-Orians L,et al. A randomized controlled trial ofresistance exercise training to improveglycemic control in older adults withtype 2 diabetes. Diabetes Care 2002;25:2335–2341
194. Sigal RJ, Kenny GP, Wasserman DH,Castaneda-Sceppa C. Physical activity/exercise and type 2 diabetes. DiabetesCare 2004;27:2518–2539
195. Church TS, Blair SN, Cocreham S, et al.Effects of aerobic and resistance trainingon hemoglobin A1c levels in patientswith type 2 diabetes: a randomizedcontrolled trial. JAMA 2010;304:2253–2262
196. Bax JJ, Young LH, Frye RL, Bonow RO,Steinberg HO, Barrett EJ. Screening forcoronary artery disease in patients withdiabetes. Diabetes Care 2007;30:2729–2736
197. Berger M, Berchtold P, C€uppers HJ, et al.Metabolic and hormonal effects of
muscular exercise in juvenile type dia-betics. Diabetologia 1977;13:355–365
198. Aiello LP, Wong J, Cavallerano J, BursellSE, Aiello LM. Retinopathy. In Handbookof Exercise in Diabetes. 2nd ed. RudermanN, Devlin JT, Kriska A, Eds. Alexandria,VA, American Diabetes Association,2002, p. 401–413
199. Lemaster JW, Reiber GE, Smith DG,Heagerty PJ, Wallace C. Daily weight-bearing activity does not increase the riskof diabetic foot ulcers. Med Sci SportsExerc 2003;35:1093–1099
200. Vinik A, Erbas T. Neuropathy. InHandbook of Exercise in Diabetes. 2nd ed.Ruderman N, Devlin JT, Kriska A, Eds.Alexandria, VA, American Diabetes As-sociation, 2002, p. 463–496
201. Wackers FJ, Young LH, Inzucchi SE,et al.; Detection of Ischemia in Asymp-tomatic Diabetics Investigators. De-tection of silent myocardial ischemia inasymptomatic diabetic subjects: theDIAD study. Diabetes Care 2004;27:1954–1961
202. Valensi P, Sachs RN, Harfouche B, et al.Predictive value of cardiac autonomicneuropathy in diabetic patients with orwithout silent myocardial ischemia. Di-abetes Care 2001;24:339–343
203. Mogensen CE. Nephropathy. In Hand-book of Exercise in Diabetes. 2nd ed.Ruderman N, Devlin JT, Kriska A, Eds.Alexandria, VA, American Diabetes As-sociation, 2002, p. 433–449
204. Anderson RJ, Grigsby AB, Freedland KE,et al. Anxiety and poor glycemic control:a meta-analytic review of the literature.Int J Psychiatry Med 2002;32:235–247
205. Delahanty LM, Grant RW,Wittenberg E,et al. Association of diabetes-relatedemotional distress with diabetes treat-ment in primary care patients with Type2 diabetes. Diabet Med 2007;24:48–54
206. American Diabetes Association. Psycho-social factors affecting adherence, qualityof life, and well-being: helping patientscope. In Medical Management of Type 1Diabetes. 5 ed. Kaufman FR, Ed. Alex-andria, VA, American Diabetes Associa-tion, 2008, p. 173–193
207. Anderson RJ, Freedland KE, Clouse RE,Lustman PJ. The prevalence of comorbiddepression in adults with diabetes:a meta-analysis. Diabetes Care 2001;24:1069–1078
208. Harkness E, Macdonald W, Valderas J,Coventry P, Gask L, Bower P. Identifyingpsychosocial interventions that improveboth physical and mental health in pa-tients with diabetes: a systematic reviewand meta-analysis. Diabetes Care 2010;33:926–930
209. Scherrer JF, Garfield LD, Chrusciel T,et al. Increased risk of myocardial in-farction in depressed patients with type 2diabetes. Diabetes Care 2011;34:1729–1734
S56 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

210. Bot M, Pouwer F, Zuidersma M, vanMelle JP, de Jonge P. Association of co-existing diabetes and depression withmortality after myocardial infarction.Diabetes Care 2012;35:503–509
211. Sullivan MD, O’Connor P, Feeney P,et al. Depression predicts all-cause mor-tality: epidemiological evaluation from theACCORDHRQL substudy. Diabetes Care2012;35:1708–1715
212. Fisher L, Skaff MM, Mullan JT, et al.Clinical depression versus distress amongpatients with type 2 diabetes: not just aquestion of semantics. Diabetes Care2007;30:542–548
213. Fisher L, Glasgow RE, Strycker LA. Therelationship between diabetes distressand clinical depression with glycemiccontrol among patients with type 2 di-abetes. Diabetes Care 2010;33:1034–1036
214. Gary TL, Safford MM, Gerzoff RB, et al.Perception of neighborhood problems,health behaviors, and diabetes outcomesamong adults with diabetes in managedcare: the Translating Research Into Ac-tion for Diabetes (TRIAD) study. Di-abetes Care 2008;31:273–278
215. Katon W, Fan MY, Un€utzer J, Taylor J,Pincus H, Schoenbaum M. Depressionand diabetes: a potentially lethal com-bination. J Gen Intern Med 2008;23:1571–1575
216. Zhang X, Norris SL, Gregg EW, ChengYJ, Beckles G, Kahn HS. Depressivesymptoms and mortality among personswith and without diabetes. Am J Epi-demiol 2005;161:652–660
217. Rubin RR, Peyrot M. Psychological is-sues and treatments for people with di-abetes. J Clin Psychol 2001;57:457–478
218. Young-Hyman DL, Davis CL. Disor-dered eating behavior in individuals withdiabetes: importance of context, evalua-tion, and classification. Diabetes Care2010;33:683–689
219. Beverly EA, Hultgren BA, Brooks KM,Ritholz MD, Abrahamson MJ, WeingerK. Understanding physicians’ challengeswhen treating type 2 diabetic patients’social and emotional difficulties: a quali-tative study. Diabetes Care 2011;34:1086–1088
220. Katon WJ, Lin EH, Von Korff M, et al.Collaborative care for patients with de-pression and chronic illnesses. N Engl JMed 2010;363:2611–2620
221. Ciechanowski P. An integrated modelfor understanding the experience of in-dividuals with co-occuring diabetes anddepression. Clin Diabetes 2011;29:43–50
222. Kitabchi AE, Umpierrez GE, Miles JM,Fisher JN. Hyperglycemic crises in adultpatients with diabetes. Diabetes Care2009;32:1335–1343
223. Cryer PE. Hypoglycaemia: the limitingfactor in the glycaemic management of
Type I and Type II diabetes. Diabetologia2002;45:937–948
224. Whitmer RA, Karter AJ, Yaffe K,Quesenberry CP Jr, Selby JV. Hypogly-cemic episodes and risk of dementia inolder patients with type 2 diabetes mel-litus. JAMA 2009;301:1565–1572
225. Punthakee Z,Miller ME, Launer LJ, et al.;ACCORD Group of Investigators;ACCORD-MIND Investigators. Poorcognitive function and risk of severehypoglycemia in type 2 diabetes: posthoc epidemiologic analysis of theACCORD trial. Diabetes Care 2012;35:787–793
226. Jacobson AM, Musen G, Ryan CM, et al.;Diabetes Control and ComplicationsTrial/Epidemiology of Diabetes Inter-ventions and Complications StudyResearch Group. Long-term effect of di-abetes and its treatment on cognitivefunction. N Engl J Med 2007;356:1842–1852
227. Zoungas S, Patel A, Chalmers J, et al.;ADVANCE Collaborative Group. Severehypoglycemia and risks of vascularevents and death. N Engl J Med 2010;363:1410–1418
228. McCoy RG, Van Houten HK, ZiegenfussJY, Shah ND, Wermers RA, Smith SA.Increased mortality of patients with di-abetes reporting severe hypoglycemia.Diabetes Care 2012;35:1897–1901
229. Cryer PE. Diverse causes of hypoglycemia-associated autonomic failure in diabetes.N Engl J Med 2004;350:2272–2279
230. Schauer PR, Kashyap SR, Wolski K, et al.Bariatric surgery versus intensive medi-cal therapy in obese patients with diabetes.N Engl J Med 2012;366:1567–1576
231. Mingrone G, Panunzi S, De Gaetano A,et al. Bariatric surgery versus conven-tional medical therapy for type 2 diabetes.N Engl J Med 2012;366:1577–1585
232. Dorman RB, Serrot FJ, Miller CJ, et al.Case-matched outcomes in bariatricsurgery for treatment of type 2 diabetesin the morbidly obese patient. Ann Surg2012;255:287–293
233. Buchwald H, Estok R, Fahrbach K, et al.Weight and type 2 diabetes after bariatricsurgery: systematic review and meta-analysis. Am J Med 2009;122:248–256,e5
234. Dixon JB, O’Brien PE, Playfair J, et al.Adjustable gastric banding and conven-tional therapy for type 2 diabetes: a ran-domized controlled trial. JAMA 2008;299:316–323
235. Cohen RV, Pinheiro JC, Schiavon CA,Salles JE, Wajchenberg BL, CummingsDE. Effects of gastric bypass surgery inpatients with type 2 diabetes and onlymild obesity. Diabetes Care 2012;35:1420–1428
236. Buchwald H, Estok R, Fahrbach K, BanelD, Sledge I. Trends in mortality in bari-atric surgery: a systematic review and
meta-analysis. Surgery 2007;142:621–632; discussion 632–635
237. Sjöström L, Narbro K, Sjöström CD,et al.; Swedish Obese Subjects Study.Effects of bariatric surgery on mortalityin Swedish obese subjects. N Engl J Med2007;357:741–752
238. Hoerger TJ, Zhang P, Segel JE, Kahn HS,Barker LE, Couper S. Cost-effectivenessof bariatric surgery for severely obeseadults with diabetes. Diabetes Care2010;33:1933–1939
239. Makary MA, Clark JM, Shore AD, et al.Medication utilization and annual healthcare costs in patients with type 2 diabetesmellitus before and after bariatric sur-gery. Arch Surg 2010;145:726–731
240. Keating CL, Dixon JB, Moodie ML,Peeters A, Playfair J, O’Brien PE. Cost-efficacy of surgically induced weight lossfor the management of type 2 diabetes:a randomized controlled trial. DiabetesCare 2009;32:580–584
241. Maciejewski ML, Livingston EH, SmithVA, et al. Survival among high-risk pa-tients after bariatric surgery. JAMA 2011;305:2419–2426
242. Himpens J, Cadière GB, Bazi M, VoucheM, Cadière B, Dapri G. Long-term out-comes of laparoscopic adjustable gastricbanding. Arch Surg 2011;146:802–807
243. Smith SA, Poland GA. Use of influenzaand pneumococcal vaccines in peoplewith diabetes. Diabetes Care 2000;23:95–108
244. Colquhoun AJ, Nicholson KG, Botha JL,Raymond NT. Effectiveness of influenzavaccine in reducing hospital admissionsin people with diabetes. Epidemiol Infect1997;119:335–341
245. Bridges CB, Fukuda K, Uyeki TM, CoxNJ, Singleton JA; Centers for DiseaseControl and Prevention, AdvisoryCommittee on Immunization Practices.Prevention and control of influenza.Recommendations of the AdvisoryCommittee on Immunization Practices(ACIP). MMWR Recomm Rep 2002;51(RR-3):1–31
246. Centers for Disease Control and Pre-vention. Use of hepatitis B vaccinationfor adults with diabetes mellitus: rec-ommendations of the Advisory Com-mittee on Immunization Practices(ACIP). MMWR 2012;60:1709–1711
247. Buse JB, Ginsberg HN, Bakris GL, et al.;American Heart Association; AmericanDiabetes Association. Primary pre-vention of cardiovascular diseases inpeople with diabetes mellitus: a scientificstatement from the American Heart As-sociation and the American DiabetesAssociation. Diabetes Care 2007;30:162–172
248. Gaede P, Lund-Andersen H, ParvingHH, Pedersen O. Effect of a multifacto-rial intervention on mortality in type 2
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S57
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
diabetes. N Engl J Med 2008;358:580–591
249. Ford ES. Trends in the risk for coronaryheart disease among adults with di-agnosed diabetes in the U.S.: findingsfrom the National Health and NutritionExamination Survey, 1999-2008. Di-abetes Care 2011;34:1337–1343
250. Bobrie G, Genès N, Vaur L, et al. Is“isolated home” hypertension as op-posed to “isolated office” hypertension asign of greater cardiovascular risk? ArchIntern Med 2001;161:2205–2211
251. Sega R, Facchetti R, Bombelli M, et al.Prognostic value of ambulatory andhome blood pressures compared withoffice blood pressure in the generalpopulation: follow-up results from thePressioni Arteriose Monitorate e LoroAssociazioni (PAMELA) study. Circula-tion 2005;111:1777–1783
252. Chobanian AV, Bakris GL, Black HR,et al.; National Heart, Lung, and BloodInstitute Joint National Committee onPrevention, Detection, Evaluation, andTreatment of High Blood Pressure; Na-tional High Blood Pressure EducationProgram Coordinating Committee. TheSeventh Report of the Joint NationalCommittee on Prevention, Detection,Evaluation, and Treatment of HighBlood Pressure: the JNC 7 report. JAMA2003;289:2560–2572
253. Lewington S, Clarke R, Qizilbash N, PetoR, Collins R; Prospective Studies Col-laboration. Age-specific relevance ofusual blood pressure to vascular mor-tality: a meta-analysis of individualdata for one million adults in 61 pro-spective studies. Lancet 2002;360:1903–1913
254. Stamler J, Vaccaro O, Neaton JD,Wentworth D. Diabetes, other risk fac-tors, and 12-yr cardiovascular mortalityfor men screened in the Multiple RiskFactor Intervention Trial. Diabetes Care1993;16:434–444
255. UK Prospective Diabetes Study Group.Tight blood pressure control and risk ofmacrovascular and microvascular com-plications in type 2 diabetes: UKPDS 38.BMJ 1998;317:703–713
256. Hansson L, Zanchetti A, Carruthers SG,et al.; HOT Study Group. Effects of in-tensive blood-pressure lowering andlow-dose aspirin in patients with hy-pertension: principal results of the Hy-pertension Optimal Treatment (HOT)randomised trial. Lancet 1998;351:1755–1762
257. Adler AI, Stratton IM, Neil HA, et al.Association of systolic blood pressurewith macrovascular and microvascularcomplications of type 2 diabetes(UKPDS 36): prospective observationalstudy. BMJ 2000;321:412–419
258. Cushman WC, Evans GW, Byington RP,et al.; ACCORD Study Group. Effects
of intensive blood-pressure control intype 2 diabetes mellitus. N Engl J Med2010;362:1575–1585
259. Patel A, MacMahon S, Chalmers J, et al.;ADVANCE Collaborative Group. Effectsof a fixed combination of perindopriland indapamide on macrovascular andmicrovascular outcomes in patients withtype 2 diabetes mellitus (the ADVANCEtrial): a randomised controlled trial.Lancet 2007;370:829–840
260. Cooper-DeHoff RM, Gong Y, HandbergEM, et al. Tight blood pressure controland cardiovascular outcomes amonghypertensive patients with diabetes andcoronary artery disease. JAMA 2010;304:61–68
261. Sleight P, Redon J, Verdecchia P, et al.;ONTARGET investigators. Prognosticvalue of blood pressure in patients withhigh vascular risk in the Ongoing Tel-misartan Alone and in combination withRamipril Global Endpoint Trial study. JHypertens 2009;27:1360–1369
262. McBrien K, Rabi DM, Campbell N, et al.Intensive and standard blood pressuretargets in patients with type 2 diabetesmellitus: systematic review and meta-analysis. Arch Intern Med 2012;172:1296–1303
263. Bangalore S, Kumar S, Lobach I, MesserliFH. Blood pressure targets in subjectswith type 2 diabetes mellitus/impairedfasting glucose: observations from tra-ditional and bayesian random-effectsmeta-analyses of randomized trials. Cir-culation 2011;123:2799–2810
264. Sacks FM, Svetkey LP, Vollmer WM,et al.; DASH-Sodium Collaborative Re-search Group. Effects on blood pressureof reduced dietary sodium and the Di-etary Approaches to Stop Hypertension(DASH) diet. N Engl J Med 2001;344:3–10
265. Tatti P, Pahor M, Byington RP, et al.Outcome results of the Fosinopril VersusAmlodipine Cardiovascular EventsRandomized Trial (FACET) in patientswith hypertension and NIDDM. DiabetesCare 1998;21:597–603
266. Estacio RO, Jeffers BW, Hiatt WR,Biggerstaff SL, Gifford N, Schrier RW.The effect of nisoldipine as comparedwith enalapril on cardiovascular out-comes in patients with non-insulin-de-pendent diabetes and hypertension. NEngl J Med 1998;338:645–652
267. Schrier RW, Estacio RO, Mehler PS,Hiatt WR. Appropriate blood pressurecontrol in hypertensive and normoten-sive type 2 diabetes mellitus: a summaryof the ABCD trial. Nat Clin Pract Nephrol2007;3:428–438
268. ALLHAT Officers and Coordinators forthe ALLHAT Collaborative ResearchGroup. The Antihypertensive andLipid-Lowering Treatment to PreventHeart Attack Trial. Major outcomes in
high-risk hypertensive patients ran-domized to angiotensin-converting en-zyme inhibitor or calcium channelblocker vs diuretic: The Antihyperten-sive and Lipid-Lowering Treatment toPrevent Heart Attack Trial (ALLHAT).JAMA 2002;288:2981–2997
269. Psaty BM, Smith NL, Siscovick DS, et al.Health outcomes associated with anti-hypertensive therapies used as first-lineagents. A systematic review and meta-analysis. JAMA 1997;277:739–745
270. Heart Outcomes Prevention EvaluationStudy Investigators. Effects of ramiprilon cardiovascular and microvascularoutcomes in people with diabetes mel-litus: results of the HOPE study andMICRO-HOPE substudy. Lancet 2000;355:253–259
271. McMurray JJ, Ostergren J, Swedberg K,et al.; CHARM Investigators and Com-mittees. Effects of candesartan in pa-tients with chronic heart failure andreduced left-ventricular systolic functiontaking angiotensin-converting-enzymeinhibitors: the CHARM-Added trial.Lancet 2003;362:767–771
272. Pfeffer MA, Swedberg K, Granger CB,et al.; CHARM Investigators and Com-mittees. Effects of candesartan on mor-tality and morbidity in patients withchronic heart failure: the CHARM-Overall programme. Lancet 2003;362:759–766
273. Granger CB, McMurray JJ, Yusuf S, et al.;CHARM Investigators and Committees.Effects of candesartan in patients withchronic heart failure and reduced left-ventricular systolic function intolerantto angiotensin-converting-enzyme in-hibitors: the CHARM-Alternative trial.Lancet 2003;362:772–776
274. Lindholm LH, Ibsen H, Dahlöf B, et al.;LIFE Study Group. Cardiovascularmorbidity and mortality in patients withdiabetes in the Losartan Intervention ForEndpoint reduction in hypertensionstudy (LIFE): a randomised trial againstatenolol. Lancet 2002;359:1004–1010
275. Berl T, Hunsicker LG, Lewis JB, et al.;Irbesartan Diabetic Nephropathy Trial.Collaborative Study Group. Cardiovas-cular outcomes in the Irbesartan Di-abetic Nephropathy Trial of patients withtype 2 diabetes and overt nephropathy.Ann Intern Med 2003;138:542–549
276. McManus RJ, Mant J, Bray EP, et al.Telemonitoring and self-management inthe control of hypertension (TASMINH2):a randomised controlled trial. Lancet 2010;376:163–172
277. Hermida RC, Ayala DE, Mojón A,Fern�andez JR. Influence of time of day ofblood pressure-lowering treatment oncardiovascular risk in hypertensive pa-tients with type 2 diabetes. Diabetes Care2011;34:1270–1276
S58 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
278. Sibai BM. Treatment of hypertension inpregnant women. N Engl J Med 1996;335:257–265
279. Baigent C, Keech A, Kearney PM, et al.;Cholesterol Treatment Trialists’ (CTT)Collaborators. Efficacy and safety of cho-lesterol-lowering treatment: prospectivemeta-analysis of data from 90,056 partic-ipants in 14 randomised trials of statins.Lancet 2005;366:1267–1278
280. Mihaylova B, Emberson J, Blackwell L,et al.; Cholesterol Treatment Trialists’(CTT) Collaborators. The effects oflowering LDL cholesterol with statintherapy in people at low risk of vasculardisease: meta-analysis of individual datafrom 27 randomised trials. Lancet 2012;380:581–590
281. Py�orälä K, Pedersen TR, Kjekshus J,Faergeman O, Olsson AG, ThorgeirssonG. Cholesterol lowering with simvastatinimproves prognosis of diabetic patientswith coronary heart disease. A subgroupanalysis of the Scandinavian SimvastatinSurvival Study (4S). Diabetes Care 1997;20:614–620
282. Collins R, Armitage J, Parish S, Sleigh P,Peto R; Heart Protection Study Collabo-rative Group. MRC/BHF Heart ProtectionStudy of cholesterol-lowering with sim-vastatin in 5963 people with diabetes:a randomised placebo-controlled trial.Lancet 2003;361:2005–2016
283. Goldberg RB, Mellies MJ, Sacks FM,et al.; the Care Investigators. Cardiovas-cular events and their reduction withpravastatin in diabetic and glucose-in-tolerant myocardial infarction survivorswith average cholesterol levels: sub-group analyses in the cholesterol andrecurrent events (CARE) trial. Circula-tion 1998;98:2513–2519
284. Shepherd J, Barter P, Carmena R, et al.Effect of lowering LDL cholesterol sub-stantially below currently recommendedlevels in patients with coronary heartdisease and diabetes: the Treating toNew Targets (TNT) study. Diabetes Care2006;29:1220–1226
285. Sever PS, Poulter NR, Dahlöf B, et al.Reduction in cardiovascular events withatorvastatin in 2,532 patients with type 2diabetes: Anglo-Scandinavian CardiacOutcomes Trialdlipid-lowering arm(ASCOT-LLA). Diabetes Care 2005;28:1151–1157
286. Knopp RH, d’Emden M, Smilde JG,Pocock SJ. Efficacy and safety of ator-vastatin in the prevention of cardiovas-cular end points in subjects with type 2diabetes: the Atorvastatin Study for Pre-vention of Coronary Heart DiseaseEndpoints in non-insulin-dependentdiabetes mellitus (ASPEN). DiabetesCare 2006;29:1478–1485
287. Colhoun HM, Betteridge DJ, DurringtonPN, et al.; CARDS investigators. Primaryprevention of cardiovascular disease
with atorvastatin in type 2 diabetes inthe Collaborative Atorvastatin DiabetesStudy (CARDS): multicentre rando-mised placebo-controlled trial. Lancet2004;364:685–696
288. Kearney PM, Blackwell L, Collins R,et al.; Cholesterol Treatment Trialists’(CTT) Collaborators. Efficacy of choles-terol-lowering therapy in 18,686 peoplewith diabetes in 14 randomised trials ofstatins: a meta-analysis. Lancet 2008;371:117–125
289. Rajpathak SN, Kumbhani DJ, Crandall J,Barzilai N, Alderman M, Ridker PM.Statin therapy and risk of developingtype 2 diabetes: ameta-analysis. DiabetesCare 2009;32:1924–1929
290. Sattar N, Preiss D, Murray HM, et al.Statins and risk of incident diabetes:a collaborative meta-analysis of rando-mised statin trials. Lancet 2010;375:735–742
291. Ridker PM, Pradhan A, MacFadyen JG,Libby P, Glynn RJ. Cardiovascular ben-efits and diabetes risks of statin therapyin primary prevention: an analysis fromthe JUPITER trial. Lancet 2012;380:565–571
292. Singh IM, Shishehbor MH, Ansell BJ.High-density lipoprotein as a therapeu-tic target: a systematic review. JAMA2007;298:786–798
293. Canner PL, Berge KG, Wenger NK, et al.Fifteen year mortality in Coronary DrugProject patients: long-term benefit withniacin. J Am Coll Cardiol 1986;8:1245–1255
294. Rubins HB, Robins SJ, Collins D, et al.;Veterans Affairs High-Density Lipopro-tein Cholesterol Intervention Trial StudyGroup. Gemfibrozil for the secondaryprevention of coronary heart disease inmen with low levels of high-density li-poprotein cholesterol. N Engl J Med1999;341:410–418
295. FrickMH, Elo O, Haapa K, et al. HelsinkiHeart Study: primary-prevention trialwith gemfibrozil in middle-aged menwith dyslipidemia. Safety of treatment,changes in risk factors, and incidence ofcoronary heart disease. N Engl J Med1987;317:1237–1245
296. Keech A, Simes RJ, Barter P, et al.; FIELDStudy Investigators. Effects of long-termfenofibrate therapy on cardiovascularevents in 9795 people with type 2 di-abetes mellitus (the FIELD study):randomised controlled trial. Lancet2005;366:1849–1861
297. Jones PH, Davidson MH. Reporting rateof rhabdomyolysis with fenofibrate 1statin versus gemfibrozil 1 any statin.Am J Cardiol 2005;95:120–122
298. Ginsberg HN, Elam MB, Lovato LC,et al.; ACCORD Study Group. Effects ofcombination lipid therapy in type 2 di-abetes mellitus. N Engl J Med 2010;362:1563–1574
299. Boden WE, Probstfield JL, Anderson T,et al.; AIM-HIGH Investigators. Niacinin patients with low HDL cholesterollevels receiving intensive statin the-rapy. N Engl J Med 2011;365:2255–2267
300. Expert Panel on Detection, Evaluation,and Treatment of High Blood Choles-terol in Adults. Executive Summary ofthe Third Report of the National Cho-lesterol Education Program (NCEP) Ex-pert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol inAdults (Adult Treatment Panel III).JAMA 2001;285:2486–2497
301. Hayward RA, Hofer TP, Vijan S. Narra-tive review: lack of evidence forrecommended low-density lipoproteintreatment targets: a solvable problem.Ann Intern Med 2006;145:520–530
302. Cannon CP, Braunwald E, McCabe CH,et al.; Pravastatin or Atorvastatin Evalua-tion and Infection Therapy-Thrombolysisin Myocardial Infarction 22 Investigators.Intensive versus moderate lipid loweringwith statins after acute coronary syn-dromes. N Engl J Med 2004;350:1495–1504
303. de Lemos JA, Blazing MA, Wiviott SD,et al.; A to Z Investigators. Early intensivevs a delayed conservative simvastatinstrategy in patients with acute coronarysyndromes: phase Z of the A to Z trial.JAMA 2004;292:1307–1316
304. Nissen SE, Tuzcu EM, Schoenhagen P,et al.; REVERSAL Investigators. Effect ofintensive compared with moderate lipid-lowering therapy on progression of cor-onary atherosclerosis: a randomizedcontrolled trial. JAMA 2004;291:1071–1080
305. Grundy SM, Cleeman JI, Merz CN, et al.;National Heart, Lung, and Blood In-stitute; American College of CardiologyFoundation; American Heart Associa-tion. Implications of recent clinical trialsfor the National Cholesterol EducationProgram Adult Treatment Panel IIIguidelines. Circulation 2004;110:227–239
306. Brunzell JD, Davidson M, Furberg CD,et al.; American Diabetes Association;American College of Cardiology Foun-dation. Lipoprotein management inpatients with cardiometabolic risk: con-sensus statement from the AmericanDiabetes Association and the AmericanCollege of Cardiology Foundation. Di-abetes Care 2008;31:811–822
307. Chasman DI, Posada D, SubrahmanyanL, Cook NR, Stanton VP Jr, Ridker PM.Pharmacogenetic study of statin therapyand cholesterol reduction. JAMA 2004;291:2821–2827
308. Meek C, Wierzbicki AS, Jewkes C, et al.Daily and intermittent rosuvastatin 5 mgtherapy in statin intolerant patients: an
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S59
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
observational study. Curr Med Res Opin2012;28:371–378
309. Elam MB, Hunninghake DB, Davis KB,et al. Effect of niacin on lipid and lipo-protein levels and glycemic control inpatients with diabetes and peripheralarterial disease. The ADMIT Study:a randomized trial. JAMA 2000;284:1263–1270
310. Grundy SM, Vega GL, McGovern ME,et al.; Diabetes Multicenter ResearchGroup. Efficacy, safety, and tolerabilityof once-daily niacin for the treatment ofdyslipidemia associated with type 2 di-abetes: results of the assessment of di-abetes control and evaluation of theefficacy of niaspan trial. Arch Intern Med2002;162:1568–1576
311. Baigent C, Blackwell L, Collins R, et al.;Antithrombotic Trialists’ (ATT) Collab-oration. Aspirin in the primary and sec-ondary prevention of vascular disease:collaborative meta-analysis of individualparticipant data from randomised trials.Lancet 2009;373:1849–1860
312. Ogawa H, Nakayama M, Morimoto T,et al.; Japanese Primary Prevention ofAtherosclerosis with Aspirin for Diabetes(JPAD) Trial Investigators. Low-doseaspirin for primary prevention of ath-erosclerotic events in patients with type2 diabetes: a randomized controlled trial.JAMA 2008;300:2134–2141
313. Belch J, MacCuish A, Campbell I, et al.The prevention of progression of arterialdisease and diabetes (POPADAD) trial:factorial randomised placebo controlledtrial of aspirin and antioxidants in pa-tients with diabetes and asymptomaticperipheral arterial disease. BMJ 2008;337:a1840
314. Pignone M, Earnshaw S, Tice JA,Pletcher MJ. Aspirin, statins, or bothdrugs for the primary prevention ofcoronary heart disease events in men:a cost-utility analysis. Ann Intern Med2006;144:326–336
315. PignoneM, Alberts MJ, Colwell JA, et al.;American Diabetes Association; Ameri-can Heart Association; American Collegeof Cardiology Foundation. Aspirin forprimary prevention of cardiovascularevents in people with diabetes: a positionstatement of the American DiabetesAssociation, a scientific statement of theAmerican Heart Association, and an ex-pert consensus document of the Ameri-can College of Cardiology Foundation.Diabetes Care 2010;33:1395–1402
316. Campbell CL, Smyth S, Montalescot G,Steinhubl SR. Aspirin dose for the pre-vention of cardiovascular disease: a system-atic review. JAMA 2007;297:2018–2024
317. Davì G, Patrono C. Platelet activationand atherothrombosis. N Engl J Med2007;357:2482–2494
318. Bhatt DL, Marso SP, Hirsch AT, RinglebPA, Hacke W, Topol EJ. Amplified
benefit of clopidogrel versus aspirin inpatients with diabetes mellitus. Am JCardiol 2002;90:625–628
319. Voulgari C, Katsilambros N, TentolourisN. Smoking cessation predicts ameliora-tion of microalbuminuria in newly di-agnosed type 2 diabetes mellitus: a 1-yearprospective study. Metabolism 2011;60:1456–1464
320. Ranney L, Melvin C, Lux L, McClain E,Lohr KN. Systematic review: smokingcessation intervention strategies foradults and adults in special populations.Ann Intern Med 2006;145:845–856
321. Scognamiglio R, Negut C, Ramondo A,Tiengo A, Avogaro A. Detection of cor-onary artery disease in asymptomaticpatients with type 2 diabetes mellitus. JAm Coll Cardiol 2006;47:65–71
322. Boden WE, O’Rourke RA, Teo KK, et al.;COURAGE Trial Research Group. Opti-mal medical therapy with or without PCIfor stable coronary disease. N Engl J Med2007;356:1503–1516
323. Frye RL, August P, Brooks MM, et al.;BARI 2D Study Group. A randomizedtrial of therapies for type 2 diabetes andcoronary artery disease. N Engl J Med2009;360:2503–2515
324. Wackers FJ, ChyunDA, Young LH, et al.;Detection of Ischemia in AsymptomaticDiabetics (DIAD) Investigators. Resolu-tion of asymptomatic myocardial ische-mia in patients with type 2 diabetes inthe Detection of Ischemia in Asymp-tomatic Diabetics (DIAD) study. Di-abetes Care 2007;30:2892–2898
325. Young LH,Wackers FJ, ChyunDA, et al.;DIAD Investigators. Cardiac outcomesafter screening for asymptomatic coro-nary artery disease in patients with type 2diabetes: the DIAD study: a randomizedcontrolled trial. JAMA 2009;301:1547–1555
326. Hadamitzky M, Hein F, Meyer T, et al.Prognostic value of coronary computedtomographic angiography in diabeticpatients without known coronary arterydisease. Diabetes Care 2010;33:1358–1363
327. Elkeles RS, Godsland IF, Feher MD,et al.; PREDICT Study Group. Coronarycalcium measurement improves predic-tion of cardiovascular events in asymp-tomatic patients with type 2 diabetes: thePREDICT study. Eur Heart J 2008;29:2244–2251
328. Choi EK, Chun EJ, Choi SI, et al. As-sessment of subclinical coronary ath-erosclerosis in asymptomatic patientswith type 2 diabetes mellitus with singlephoton emission computed tomographyand coronary computed tomographyangiography. Am J Cardiol 2009;104:890–896
329. Braunwald E, Domanski MJ, Fowler SE,et al.; PEACE Trial Investigators. An-giotensin-converting-enzyme inhibition
in stable coronary artery disease. N Engl JMed 2004;351:2058–2068
330. Yusuf S, Teo K, Anderson C, et al.; Tel-misartan Randomised AssessmeNt Studyin ACE iNtolerant subjects with cardio-vascular Disease (TRANSCEND) Inves-tigators. Effects of the angiotensin-receptorblocker telmisartan on cardiovascular ev-ents in high-risk patients intolerant to an-giotensin-converting enzyme inhibitors:a randomised controlled trial. Lancet 2008;372:1174–1183
331. Garg JP, Bakris GL. Microalbuminuria:marker of vascular dysfunction, risk fa-ctor for cardiovascular disease. VascMed2002;7:35–43
332. Klausen K, Borch-Johnsen K, Feldt-Rasmussen B, et al. Very low levels ofmicroalbuminuria are associated withincreased risk of coronary heart diseaseand death independently of renal func-tion, hypertension, and diabetes. Circu-lation 2004;110:32–35
333. Gall MA, Hougaard P, Borch-Johnsen K,Parving HH. Risk factors for develo-pment of incipient and overt diabeticnephropathy in patients with non-insulindependent diabetes mellitus: prospective,observational study. BMJ 1997;314:783–788
334. Ravid M, Lang R, Rachmani R, LishnerM. Long-term renoprotective effect ofangiotensin-converting enzyme inhibitionin non-insulin-dependent diabetes melli-tus. A 7-year follow-up study. Arch InternMed 1996;156:286–289
335. Reichard P, Nilsson BY, Rosenqvist U.The effect of long-term intensified in-sulin treatment on the development ofmicrovascular complications of diabetesmellitus. N Engl J Med 1993;329:304–309
336. The Diabetes Control and Complica-tions (DCCT) Research Group. Effect ofintensive therapy on the developmentand progression of diabetic nephropathyin the Diabetes Control and Complica-tions Trial. Kidney Int 1995;47:1703–1720
337. Lewis EJ, Hunsicker LG, Bain RP, RohdeRD; The Collaborative Study Group. Theeffect of angiotensin-converting-enzymeinhibition on diabetic nephropathy.N Engl J Med 1993;329:1456–1462
338. Laffel LM, McGill JB, Gans DJ; NorthAmerican Microalbuminuria StudyGroup. The beneficial effect of angio-tensin-converting enzyme inhibitionwith captopril on diabetic nephropathyin normotensive IDDM patients withmicroalbuminuria. Am J Med 1995;99:497–504
339. Bakris GL,WilliamsM, Dworkin L, et al.;National Kidney Foundation Hyperten-sion and Diabetes Executive CommitteesWorking Group. Preserving renal func-tion in adults with hypertension and
S60 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
diabetes: a consensus approach. Am JKidney Dis 2000;36:646–661
340. Remuzzi G, Macia M, Ruggenenti P.Prevention and treatment of diabetic re-nal disease in type 2 diabetes: theBENEDICT study. J Am Soc Nephrol2006;17(Suppl. 2):S90–S97
341. HallerH, Ito S, Izzo JL Jr, et al.; ROADMAPTrial Investigators. Olmesartan for thedelay or prevention of microalbuminuriain type 2 diabetes.NEngl JMed2011;364:907–917
342. Bilous R, Chaturvedi N, Sjølie AK, et al.Effect of candesartan on microalbu-minuria and albumin excretion rate indiabetes: three randomized trials. AnnIntern Med 2009;151:11–20
343. Mauer M, Zinman B, Gardiner R, et al.Renal and retinal effects of enalapril andlosartan in type 1 diabetes. N Engl J Med2009;361:40–51
344. Lewis EJ, Hunsicker LG, Clarke WR,et al.; Collaborative Study Group. Re-noprotective effect of the angiotensin-receptor antagonist irbesartan in patientswith nephropathy due to type 2 diabetes.N Engl J Med 2001;345:851–860
345. Brenner BM, Cooper ME, de Zeeuw D,et al.; RENAAL Study Investigators. Ef-fects of losartan on renal and cardiovas-cular outcomes in patients with type 2diabetes and nephropathy. N Engl J Med2001;345:861–869
346. Parving HH, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S,Arner P; Irbesartan in Patients with Type2 Diabetes and Microalbuminuria StudyGroup. The effect of irbesartan on thedevelopment of diabetic nephropathy inpatients with type 2 diabetes. N Engl JMed 2001;345:870–878
347. Pepine CJ, Handberg EM, Cooper-DeHoff RM, et al.; INVEST Investigators.A calcium antagonist vs a non-calciumantagonist hypertension treatment stra-tegy for patients with coronary arterydisease. The International Verapamil-Trandolapril Study (INVEST): a ran-domized controlled trial. JAMA 2003;290:2805–2816
348. Bakris GL, Siomos M, Richardson D,et al.; VAL-K Study Group. ACE in-hibition or angiotensin receptor block-ade: impact on potassium in renalfailure. Kidney Int 2000;58:2084–2092
349. Mogensen CE, Neldam S, Tikkanen I,et al. Randomised controlled trial of dualblockade of renin-angiotensin system inpatients with hypertension, micro-albuminuria, and non-insulin dependentdiabetes: the candesartan and lisinoprilmicroalbuminuria (CALM) study. BMJ2000;321:1440–1444
350. Schjoedt KJ, Jacobsen P, Rossing K,Boomsma F, Parving HH. Dual blockadeof the renin-angiotensin-aldosteronesystem in diabetic nephropathy: the role
of aldosterone. HormMetab Res 2005;37(Suppl. 1):4–8
351. Schjoedt KJ, Rossing K, Juhl TR, et al.Beneficial impact of spironolactone indiabetic nephropathy. Kidney Int 2005;68:2829–2836
352. Parving HH, Persson F, Lewis JB, LewisEJ, Hollenberg NK; AVOID Study In-vestigators. Aliskiren combined withlosartan in type 2 diabetes and ne-phropathy. N Engl J Med 2008;358:2433–2446
353. Yusuf S, Teo KK, Pogue J, et al.;ONTARGET Investigators. Telmisartan,ramipril, or both in patients at high riskfor vascular events. N Engl J Med 2008;358:1547–1559
354. Pijls LT, de Vries H, Donker AJ, van EijkJT. The effect of protein restriction onalbuminuria in patients with type 2 di-abetes mellitus: a randomized trial.Nephrol Dial Transplant 1999;14:1445–1453
355. Pedrini MT, Levey AS, Lau J, ChalmersTC, Wang PH. The effect of dietaryprotein restriction on the progression ofdiabetic and nondiabetic renal diseases:a meta-analysis. Ann Intern Med 1996;124:627–632
356. Hansen HP, Tauber-Lassen E, Jensen BR,Parving HH. Effect of dietary proteinrestriction on prognosis in patients withdiabetic nephropathy. Kidney Int 2002;62:220–228
357. Kasiske BL, Lakatua JD, Ma JZ, Louis TA.A meta-analysis of the effects of dietaryprotein restriction on the rate of declinein renal function. Am J Kidney Dis 1998;31:954–961
358. Eknoyan G, Hostetter T, Bakris GL, et al.Proteinuria and other markers of chronickidney disease: a position statement ofthe National Kidney Foundation (NKF)and the National Institute of Diabetesand Digestive and Kidney Diseases(NIDDK). Am J Kidney Dis 2003;42:617–622
359. Levey AS, Coresh J, Balk E, et al.; Na-tional Kidney Foundation. NationalKidney Foundation practice guidelinesfor chronic kidney disease: evaluation,classification, and stratification. Ann In-tern Med 2003;139:137–147
360. Kramer H, Molitch ME. Screening forkidney disease in adults with diabetes.Diabetes Care 2005;28:1813–1816
361. Kramer HJ, Nguyen QD, Curhan G, HsuCY. Renal insufficiency in the absence ofalbuminuria and retinopathy amongadults with type 2 diabetes mellitus.JAMA 2003;289:3273–3277
362. Levey AS, Bosch JP, Lewis JB, Greene T,Rogers N, Roth D; Modification of Dietin Renal Disease Study Group. A moreaccurate method to estimate glomerularfiltration rate from serum creatinine:a new prediction equation. Ann InternMed 1999;130:461–470
363. Rigalleau V, Lasseur C, Perlemoine C,et al. Estimation of glomerular filtrationrate in diabetic subjects: Cockcroft for-mula or Modification of Diet in RenalDisease study equation? Diabetes Care2005;28:838–843
364. Levinsky NG. Specialist evaluation inchronic kidney disease: too little, toolate. Ann InternMed 2002;137:542–543
365. Klein R. Hyperglycemia and microvas-cular and macrovascular disease in di-abetes. Diabetes Care 1995;18:258–268
366. Estacio RO, McFarling E, Biggerstaff S,Jeffers BW, Johnson D, Schrier RW.Overt albuminuria predicts diabetic ret-inopathy in Hispanics with NIDDM. AmJ Kidney Dis 1998;31:947–953
367. Leske MC, Wu SY, Hennis A, et al.;Barbados Eye Study Group. Hypergly-cemia, blood pressure, and the 9-yearincidence of diabetic retinopathy: theBarbados Eye Studies. Ophthalmology2005;112:799–805
368. Fong DS, Aiello LP, Ferris FL 3rd, KleinR. Diabetic retinopathy. Diabetes Care2004;27:2540–2553
369. Diabetes Control and ComplicationsTrial Research Group. Effect of preg-nancy on microvascular complicationsin the Diabetes Control and Complica-tions Trial. Diabetes Care 2000;23:1084–1091
370. The Diabetic Retinopathy Study Re-search Group. Preliminary report on ef-fects of photocoagulation therapy. Am JOphthalmol 1976;81:383–396
371. Early Treatment Diabetic RetinopathyStudy Research Group. Photocoagula-tion for diabetic macular edema. EarlyTreatment Diabetic Retinopathy Studyreport number 1. Arch Ophthalmol1985;103:1796–1806
372. Nguyen QD, Brown DM, Marcus DM,et al.; RISE and RIDE Research Group.Ranibizumab for diabetic macularedema: results from 2 phase III ran-domized trials: RISE and RIDE. Oph-thalmology 2012;119:789–801
373. Pearson PA, Comstock TL, Ip M, et al.Fluocinolone acetonide intravitreal im-plant for diabetic macular edema: a 3-year multicenter, randomized, controlledclinical trial. Ophthalmology 2011;118:1580–1587
374. Chew EY, Ambrosius WT. Update of theACCORD Eye Study. N Engl J Med2011;364:188–189
375. Keech AC, Mitchell P, Summanen PA,et al.; FIELD Study Investigators. Effectof fenofibrate on the need for lasertreatment for diabetic retinopathy(FIELD study): a randomised controlledtrial. Lancet 2007;370:1687–1697
376. Agardh E, Tababat-Khani P. Adopting3-year screening intervals for sight-threatening retinal vascular lesionsin type 2 diabetic subjects without
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S61
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
retinopathy. Diabetes Care 2011;34:1318–1319
377. Fong DS, Aiello L, Gardner TW, et al.;American Diabetes Association. Reti-nopathy in diabetes. Diabetes Care 2004;27(Suppl. 1):S84–S87
378. Ahmed J, Ward TP, Bursell SE, AielloLM, Cavallerano JD, Vigersky RA. Thesensitivity and specificity of nonmy-driatic digital stereoscopic retinal imag-ing in detecting diabetic retinopathy.Diabetes Care 2006;29:2205–2209
379. Bril V, England J, Franklin GM, et al.;American Academy of Neurology;American Association of Neuromuscularand Electrodiagnostic Medicine; Ameri-can Academy of Physical Medicine andRehabilitation. Evidence-based guideline:treatment of painful diabetic neuropathy:report of the American Academy ofNeurology, the American Association ofNeuromuscular and ElectrodiagnosticMedicine, and the American Academy ofPhysical Medicine and Rehabilitation.Neurology 2011;76:1758–1765
380. Boulton AJ, Vinik AI, Arezzo JC, et al.;American Diabetes Association. Diabeticneuropathies: a statement by the Amer-ican Diabetes Association. Diabetes Care2005;28:956–962
381. Wile DJ, Toth C. Association of metfor-min, elevated homocysteine, and meth-ylmalonic acid levels and clinicallyworsened diabetic peripheral neuropa-thy. Diabetes Care 2010;33:156–161
382. Freeman R. Not all neuropathy in di-abetes is of diabetic etiology: differentialdiagnosis of diabetic neuropathy. CurrDiab Rep 2009;9:423–431
383. Vinik AI, Maser RE, Mitchell BD, FreemanR. Diabetic autonomic neuropathy. Di-abetes Care 2003;26:1553–1579
384. Spallone V, Bellavere F, Scionti L, et al.;Diabetic Neuropathy Study Group of theItalian Society of Diabetology. Recom-mendations for the use of cardiovasculartests in diagnosing diabetic autonomicneuropathy. Nutr Metab Cardiovasc Dis2011;21:69–78
385. Boulton AJ, Armstrong DG, Albert SF,et al. Comprehensive foot examinationand risk assessment: a report of the TaskForce of the Foot Care Interest Group ofthe American Diabetes Association, withendorsement by the American Associa-tion of Clinical Endocrinologists. Di-abetes Care 2008;31:1679–1685
386. American Diabetes Association. Peri-pheral arterial disease in people withdiabetes. Diabetes Care 2003;26:3333–3341
387. Lipsky BA, Berendt AR, Cornia PB, et al.;Infectious Diseases Society of America.2012 Infectious Diseases Society ofAmerica clinical practice guideline forthe diagnosis and treatment of diabeticfoot infections. Clin Infect Dis 2012;54:e132–e173
388. Bainbridge KE, Hoffman HJ, Cowie CC.Diabetes and hearing impairment in theUnited States: audiometric evidencefrom the National Health and NutritionExamination Survey, 1999 to 2004. AnnIntern Med 2008;149:1–10
389. Bainbridge KE, Hoffman HJ, Cowie CC.Risk factors for hearing impairmentamong U.S. adults with diabetes: Na-tional Health and Nutrition ExaminationSurvey 1999-2004. Diabetes Care 2011;34:1540–1545
390. Li C, Ford ES, Zhao G, Croft JB, BalluzLS, Mokdad AH. Prevalence of self-reported clinically diagnosed sleep ap-nea according to obesity status in menand women: National Health and Nu-trition Examination Survey, 2005-2006.Prev Med 2010;51:18–23
391. West SD, Nicoll DJ, Stradling JR. Preva-lence of obstructive sleep apnoea in menwith type 2 diabetes. Thorax 2006;61:945–950
392. Foster GD, Sanders MH, Millman R,et al.; Sleep AHEAD Research Group.Obstructive sleep apnea among obesepatients with type 2 diabetes. DiabetesCare 2009;32:1017–1019
393. Shaw JE, Punjabi NM, Wilding JP,Alberti KG, Zimmet PZ. Sleep-disorderedbreathing and type 2 diabetes: a reportfrom the International Diabetes Federa-tion Taskforce on Epidemiology and Pre-vention. Diabetes Res Clin Pract 2008;81:2–12
394. Clark JM, Brancati FL, Diehl AM. Theprevalence and etiology of elevatedaminotransferase levels in the UnitedStates. Am J Gastroenterol 2003;98:960–967
395. El-Serag HB, Tran T, Everhart JE. Di-abetes increases the risk of chronic liverdisease and hepatocellular carcinoma.Gastroenterology 2004;126:460–468
396. American Gastroenterological Associa-tion. American Gastroenterological As-sociation medical position statement:nonalcoholic fatty liver disease. Gastro-enterology 2002;123:1702–1704
397. Dhindsa S, Miller MG, McWhirter CL,et al. Testosterone concentrations in di-abetic and nondiabetic obese men. Di-abetes Care 2010;33:1186–1192
398. Bhasin S, Cunningham GR, Hayes FJ,et al. Testosterone therapy in men withandrogen deficiency syndromes: an En-docrine Society clinical practice guide-line. J Clin Endocrinol Metab 2010;95:2536–2559
399. Khader YS, Dauod AS, El-Qaderi SS,Alkafajei A, Batayha WQ. Periodontalstatus of diabetics compared with non-diabetics: a meta-analysis. J DiabetesComplications 2006;20:59–68
400. Darré L, Vergnes JN, Gourdy P, Sixou M.Efficacy of periodontal treatment onglycaemic control in diabetic patients:
a meta-analysis of interventional studies.Diabetes Metab 2008;34:497–506
401. International Diabetes Federation. OralHealth for People with Diabetes. Brussels,International Diabetes Federation,2009
402. Suh S, Kim KW. Diabetes and cancer: isdiabetes causally related to cancer? Di-abetes Metab J 2011;35:193–198
403. Giovannucci E, Harlan DM, Archer MC,et al. Diabetes and cancer: a consensusreport. Diabetes Care 2010;33:1674–1685
404. Janghorbani M, Van Dam RM, WillettWC, Hu FB. Systematic review of type 1and type 2 diabetes mellitus and risk offracture. Am J Epidemiol 2007;166:495–505
405. Vestergaard P. Discrepancies in bonemineral density and fracture risk in pa-tients with type 1 and type 2 diabetesdameta-analysis. Osteoporos Int 2007;18:427–444
406. Yamamoto M, Yamaguchi T, YamauchiM, Kaji H, Sugimoto T. Diabetic patientshave an increased risk of vertebral frac-tures independent of BMD or diabeticcomplications. J Bone Miner Res 2009;24:702–709
407. Schwartz AV, Vittinghoff E, Bauer DC,et al.; Study of Osteoporotic Fractures(SOF) Research Group; OsteoporoticFractures inMen (MrOS) ResearchGroup;Health, Aging, and Body Composition(Health ABC) Research Group. Associa-tion of BMD and FRAX score with risk offracture in older adults with type 2 di-abetes. JAMA 2011;305:2184–2192
408. Cukierman T, Gerstein HC, WilliamsonJD. Cognitive decline and dementia indiabetesdsystematic overview of pro-spective observational studies. Dia-betologia 2005;48:2460–2469
409. Biessels GJ, Staekenborg S, Brunner E,Brayne C, Scheltens P. Risk of dementiain diabetes mellitus: a systematic review.Lancet Neurol 2006;5:64–74
410. Ohara T, Doi Y, Ninomiya T, et al. Glu-cose tolerance status and risk of de-mentia in the community: the Hisayamastudy. Neurology 2011;77:1126–1134
411. Launer LJ, Miller ME, Williamson JD,et al.; ACCORD MIND Investigators.Effects of intensive glucose lowering onbrain structure and function in peoplewith type 2 diabetes (ACCORD MIND):a randomised open-label substudy.Lancet Neurol 2011;10:969–977
412. Silverstein J, Klingensmith G, CopelandKC, et al.; American Diabetes Associa-tion. Care of children and adolescentswith type 1 diabetes: a statement of theAmerican Diabetes Association. DiabetesCare 2005;28:186–212
413. Northam EA, Anderson PJ, Werther GA,Warne GL, Adler RG, Andrewes D.Neuropsychological complications of
S62 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

IDDM in children 2 years after diseaseonset. Diabetes Care 1998;21:379–384
414. Rovet J, Alvarez M. Attentional func-tioning in children and adolescents withIDDM. Diabetes Care 1997;20:803–810
415. Bjørgaas M, Gimse R, Vik T, Sand T.Cognitive function in type 1 diabeticchildren with and without episodes ofsevere hypoglycaemia. Acta Paediatr1997;86:148–153
416. Nimri R, Weintrob N, Benzaquen H,Ofan R, Fayman G, Phillip M. Insulinpump therapy in youth with type 1 di-abetes: a retrospective paired study. Pe-diatrics 2006;117:2126–2131
417. Doyle EA, Weinzimer SA, Steffen AT,Ahern JA, Vincent M, Tamborlane WV.A randomized, prospective trial com-paring the efficacy of continuous sub-cutaneous insulin infusion with multipledaily injections using insulin glargine.Diabetes Care 2004;27:1554–1558
418. Perantie DC, Wu J, Koller JM, et al. Re-gional brain volume differences associ-ated with hyperglycemia and severehypoglycemia in youth with type 1 di-abetes. Diabetes Care 2007;30:2331–2337
419. Mäkimattila S, Malmberg-Cèder K,Häkkinen AM, et al. Brain metabolic al-terations in patients with type 1 diabetes-hyperglycemia-induced injury. J CerebBlood Flow Metab 2004;24:1393–1399
420. Krantz JS, Mack WJ, Hodis HN, Liu CR,Liu CH, Kaufman FR. Early onset ofsubclinical atherosclerosis in youngpersons with type 1 diabetes. J Pediatr2004;145:452–457
421. Järvisalo MJ, Putto-Laurila A, Jartti L,et al. Carotid artery intima-media thick-ness in children with type 1 diabetes.Diabetes 2002;51:493–498
422. Haller MJ, Samyn M, Nichols WW, et al.Radial artery tonometry demonstratesarterial stiffness in children with type 1diabetes. Diabetes Care 2004;27:2911–2917
423. Orchard TJ, Forrest KY, Kuller LH,Becker DJ; Pittsburgh Epidemiology ofDiabetes Complications Study. Lipidand blood pressure treatment goals fortype 1 diabetes: 10-year incidence datafrom the Pittsburgh Epidemiology ofDiabetes Complications Study. DiabetesCare 2001;24:1053–1059
424. Kavey RE, Allada V, Daniels SR, et al.Cardiovascular risk reduction in high-risk pediatric patients: a scientificstatement from the American Heart As-sociation Expert Panel on Populationand Prevention Science; the Councils onCardiovascular Disease in the Young,Epidemiology and Prevention, Nutri-tion, Physical Activity and Metabolism,High Blood Pressure Research, Cardio-vascular Nursing, and the Kidney inHeart Disease; and the InterdisciplinaryWorking Group on Quality of Care and
Outcomes Research: endorsed by theAmerican Academy of Pediatrics. Circu-lation 2006;114:2710–2738
425. McCrindle BW, Urbina EM, DennisonBA, et al. Drug therapy of high-risk lipidabnormalities in children and adoles-cents: a scientific statement from theAmerican Heart Association Atheroscle-rosis, Hypertension, and Obesity inYouth Committee, Council of Cardio-vascular Disease in the Young, with theCouncil on Cardiovascular Nursing.Circulation 2007;115:1948–1967
426. Salo P, Viikari J, Hämäläinen M, et al.Serum cholesterol ester fatty acids in7- and 13-month-old children in a pro-spective randomized trial of a low-saturated fat, low-cholesterol diet: theSTRIP baby project. Special Turku cor-onary Risk factor Intervention Projectfor children. Acta Paediatr 1999;88:505–512
427. The Dietary Intervention Study in Chil-dren (DISC). The Writing Group for theDISC Collaborative Research Group.Efficacy and safety of lowering dietaryintake of fat and cholesterol in childrenwith elevated low-density lipoproteincholesterol. JAMA 1995;273:1429–1435
428. McCrindle BW, Ose L, Marais AD. Effi-cacy and safety of atorvastatin in childrenand adolescents with familial hypercho-lesterolemia or severe hyperlipidemia:a multicenter, randomized, placebo-controlled trial. J Pediatr 2003;143:74–80
429. de Jongh S, Lilien MR, op’t Roodt J,Stroes ES, Bakker HD, Kastelein JJ. Earlystatin therapy restores endothelial func-tion in children with familial hypercho-lesterolemia. J Am Coll Cardiol 2002;40:2117–2121
430. Wiegman A,Hutten BA, de Groot E, et al.Efficacy and safety of statin therapy inchildren with familial hypercholesterol-emia: a randomized controlled trial.JAMA 2004;292:331–337
431. Cho YH, Craig ME, Hing S, et al. Mi-crovascular complications assessment inadolescents with 2- to 5-yr duration oftype 1 diabetes from 1990 to 2006. Pe-diatr Diabetes 2011;12:682–689
432. Holmes GK. Screening for coeliac dis-ease in type 1 diabetes. Arch Dis Child2002;87:495–498
433. Rewers M, Liu E, Simmons J, RedondoMJ, Hoffenberg EJ. Celiac disease asso-ciated with type 1 diabetes mellitus.Endocrinol Metab Clin North Am 2004;33:197–214, xi
434. Husby S, Koletzko S, Korponay-SzabóIR, et al.; ESPGHANWorking Group onCoeliac Disease Diagnosis; ESPGHANGastroenterology Committee; EuropeanSociety for Pediatric Gastroenterology,Hepatology, and Nutrition. EuropeanSociety for Pediatric Gastroenterology,Hepatology, and Nutrition guidelines for
the diagnosis of coeliac disease. J PediatrGastroenterol Nutr 2012;54:136–160
435. Kurppa K, Ashorn M, Iltanen S, et al.Celiac disease without villous atrophy inchildren: a prospective study. J Pediatr2010;157:373–380
436. Abid N, McGlone O, Cardwell C,McCallion W, Carson D. Clinical andmetabolic effects of gluten free diet inchildren with type 1 diabetes and coeliacdisease. Pediatr Diabetes 2011;12:322–325
437. Rold�an MB, Alonso M, Barrio R. Thyroidautoimmunity in children and adoles-cents with Type 1 diabetes mellitus. Di-abetes Nutr Metab 1999;12:27–31
438. Triolo TM, Armstrong TK, McFann K,et al. Additional autoimmune diseasefound in 33% of patients at type 1 di-abetes onset. Diabetes Care 2011;34:1211–1213
439. Kordonouri O, Deiss D, Danne T, DorowA, Bassir C, Gr€uters-Kieslich A. Pre-dictivity of thyroid autoantibodiesfor the development of thyroid disor-ders in children and adolescents withType 1 diabetes. Diabet Med 2002;19:518–521
440. Mohn A, Di Michele S, Di Luzio R,Tumini S, Chiarelli F. The effect of sub-clinical hypothyroidism on metaboliccontrol in children and adolescents withType 1 diabetes mellitus. Diabet Med2002;19:70–73
441. Chase HP, Garg SK, Cockerham RS,Wilcox WD, Walravens PA. Thyroidhormone replacement and growth ofchildren with subclinical hypothyroid-ism and diabetes. Diabet Med 1990;7:299–303
442. American Diabetes Association. Diabetescare in the school and day care setting.Diabetes Care 2010;33(Suppl. 1):S70–S74
443. Arnett JJ. Emerging adulthood. A theoryof development from the late teensthrough the twenties. Am Psychol 2000;55:469–480
444. Weissberg-Benchell J, Wolpert H,Anderson BJ. Transitioning from pedi-atric to adult care: a new approach to thepost-adolescent young person with type1 diabetes. Diabetes Care 2007;30:2441–2446
445. Peters A, Laffel L, the American DiabetesAssociation TransitionsWorking Group.Diabetes care for emerging adults: rec-ommendations for transition from pe-diatric to adult diabetes care systems:a position statement of the AmericanDiabetes Association, with representa-tion by the American College of Osteo-pathic Family Physicians, the AmericanAcademy of Pediatrics, the AmericanAssociation of Clinical Endocrinologists,the American Osteopathic Association,the Centers for Disease Control andPrevention, Children with Diabetes, The
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S63
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

Endocrine Society, the InternationalSociety for Pediatric and AdolescentDiabetes, Juvenile Diabetes ResearchFoundation International, the NationalDiabetes Education Program, and thePediatric Endocrine Society (formerlyLawson Wilkins Pediatric EndocrineSociety). Diabetes Care 2011;34:2477–2485
446. Bryden KS, Peveler RC, Stein A, Neil A,Mayou RA, Dunger DB. Clinical andpsychological course of diabetes fromadolescence to young adulthood: a lon-gitudinal cohort study. Diabetes Care2001;24:1536–1540
447. Laing SP, Jones ME, Swerdlow AJ,Burden AC, GatlingW. Psychosocial andsocioeconomic risk factors for prematuredeath in young people with type 1 di-abetes.DiabetesCare 2005;28:1618–1623
448. Eppens MC, Craig ME, Cusumano J,et al. Prevalence of diabetes complica-tions in adolescents with type 2 com-pared with type 1 diabetes. DiabetesCare 2006;29:1300–1306
449. Hattersley A, Bruining J, Shield J,Njolstad P, Donaghue KC. The diagnosisand management of monogenic diabetesin children and adolescents. Pediatr Di-abetes 2009;10(Suppl. 12):33–42
450. Cooper WO, Hernandez-Diaz S,Arbogast PG, et al. Major congenitalmalformations after first-trimester expo-sure to ACE inhibitors. N Engl J Med2006;354:2443–2451
451. American Diabetes Association. Pre-conception care of womenwith diabetes.Diabetes Care 2004;27(Suppl. 1):S76–S78
452. Kirkman M, Briscoe VJ, Clark N, et al.Diabetes in older adults. Diabetes Care2012;35:2650–2664
453. Curb JD, Pressel SL, Cutler JA, et al.;Systolic Hypertension in the ElderlyProgram Cooperative Research Group.Effect of diuretic-based antihypertensivetreatment on cardiovascular disease riskin older diabetic patients with isolatedsystolic hypertension. JAMA 1996;276:1886–1892
454. Beckett NS, Peters R, Fletcher AE, et al.;HYVET Study Group. Treatment of hy-pertension in patients 80 years of age orolder. N Engl J Med 2008;358:1887–1898
455. Moran A, Dunitz J, Nathan B, Saeed A,Holme B, Thomas W. Cystic fibrosis-related diabetes: current trends inprevalence, incidence, and mortality.Diabetes Care 2009;32:1626–1631
456. Moran A, Brunzell C, Cohen RC, et al.;CFRD Guidelines Committee. Clinicalcare guidelines for cystic fibrosis-relateddiabetes: a position statement of theAmerican Diabetes Association and aclinical practice guideline of the CysticFibrosis Foundation, endorsed by the
Pediatric Endocrine Society. DiabetesCare 2010;33:2697–2708
457. Clement S, Braithwaite SS, Magee MF,et al.; American Diabetes AssociationDiabetes in Hospitals Writing Commit-tee. Management of diabetes and hy-perglycemia in hospitals. Diabetes Care2004;27:553–591
458. van den Berghe G, Wouters P, WeekersF, et al. Intensive insulin therapy incritically ill patients. N Engl J Med 2001;345:1359–1367
459. Malmberg K, Norhammar A, Wedel H,Rydén L. Glycometabolic state at ad-mission: important risk marker of mor-tality in conventionally treated patientswith diabetes mellitus and acute myo-cardial infarction: long-term results fromthe Diabetes and Insulin-Glucose In-fusion in Acute Myocardial Infarction(DIGAMI) study. Circulation 1999;99:2626–2632
460. Wiener RS, Wiener DC, Larson RJ.Benefits and risks of tight glucose controlin critically ill adults: a meta-analysis.JAMA 2008;300:933–944
461. Brunkhorst FM, Engel C, Bloos F, et al.;German Competence Network Sepsis(SepNet). Intensive insulin therapy andpentastarch resuscitation in severe sep-sis. N Engl J Med 2008;358:125–139
462. Finfer S, Chittock DR, Su SY, et al.;NICE-SUGAR Study Investigators. In-tensive versus conventional glucosecontrol in critically ill patients. N Engl JMed 2009;360:1283–1297
463. Krinsley JS, Grover A. Severe hypogly-cemia in critically ill patients: risk factorsand outcomes. Crit Care Med 2007;35:2262–2267
464. Van den Berghe G, Wilmer A, HermansG, et al. Intensive insulin therapy in themedical ICU. N Engl J Med 2006;354:449–461
465. Griesdale DE, de Souza RJ, van Dam RM,et al. Intensive insulin therapy andmortality among critically ill patients:a meta-analysis including NICE-SUGARstudy data. CMAJ 2009;180:821–827
466. Saudek CD, Herman WH, Sacks DB,Bergenstal RM, Edelman D, DavidsonMB. A new look at screening and di-agnosing diabetes mellitus. J Clin En-docrinol Metab 2008;93:2447–2453
467. Cryer PE, Davis SN, Shamoon H. Hy-poglycemia in diabetes. Diabetes Care2003;26:1902–1912
468. Moghissi ES, Korytkowski MT, DiNardoM, et al.; American Association of Clin-ical Endocrinologists; American DiabetesAssociation. American Association ofClinical Endocrinologists and AmericanDiabetes Association consensus statementon inpatient glycemic control. DiabetesCare 2009;32:1119–1131
469. Hsu CW, Sun SF, Lin SL, Huang HH,Wong KF. Moderate glucose control re-sults in less negative nitrogen balances in
medical intensive care unit patients:a randomized, controlled study. CritCare 2012;16:R56
470. Umpierrez GE, Hellman R, KorytkowskiMT, et al.; Endocrine Society. Manage-ment of hyperglycemia in hospitalizedpatients in non-critical care setting: anEndocrine Society clinical practiceguideline. J Clin Endocrinol Metab2012;97:16–38
471. Bernard JB, Munoz C, Harper J, MurielloM, Rico E, Baldwin D. Treatment of in-patient hyperglycemia beginning in theemergency department: a randomizedtrial using insulins aspart and detemircompared with usual care. J Hosp Med2011;6:279–284
472. Czosnowski QA, Swanson JM, Lobo BL,Broyles JE, Deaton PR, Finch CK. Eval-uation of glycemic control followingdiscontinuation of an intensive insulinprotocol. J Hosp Med 2009;4:28–34
473. Shomali MI, Herr DL, Hill PC,Pehlivanova M, Sharretts JM, Magee MF.Conversion from intravenous insulin tosubcutaneous insulin after cardiovascu-lar surgery: Transition to Target study.Diabetes Technol Ther 2011;13:121–126
474. Baldwin D, Zander J, Munoz C, et al. Arandomized trial of two weight-baseddoses of insulin glargine and glulisinein hospitalized subjects with type 2 di-abetes and renal insufficiency. DiabetesCare 2012;35:1970–1974
475. Umpierrez GE, Smiley D, Jacobs S, et al.Randomized study of basal-bolusinsulin therapy in the inpatient man-agement of patients with type 2 diabetesundergoing general surgery (RABBIT 2surgery). Diabetes Care 2011;34:256–261
476. Pasquel FJ, Spiegelman R, McCauley M,et al.Hyperglycemia during total parenteralnutrition: an important marker of pooroutcome and mortality in hospitalized pa-tients. Diabetes Care 2010;33:739–741
477. Schnipper JL, Liang CL, Ndumele CD,Pendergrass ML. Effects of a comput-erized order set on the inpatientmanagement of hyperglycemia: a cluster-randomized controlled trial. Endocr Pract2010;16:209–218
478. Wexler DJ, Shrader P, Burns SM,Cagliero E. Effectiveness of a computer-ized insulin order template in generalmedical inpatients with type 2 diabetes:a cluster randomized trial. Diabetes Care2010;33:2181–2183
479. Furnary AP, Braithwaite SS. Effects ofoutcome on in-hospital transition fromintravenous insulin infusion to sub-cutaneous therapy. Am J Cardiol 2006;98:557–564
480. Schafer RG, Bohannon B, Franz MJ,et al.; American Diabetes Association.Diabetes nutrition recommendations for
S64 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from
health care institutions. Diabetes Care2004;27(Suppl. 1):S55–S57
481. Curll M, Dinardo M, Noschese M,Korytkowski MT. Menu selection, gly-caemic control and satisfaction withstandard and patient-controlled consis-tent carbohydrate meal plans in hospi-talised patients with diabetes. Qual SafHealth Care 2010;19:355–359
482. Modic MB, Kozak A, Siedlecki SL, et al.Do we know what our patients with di-abetes are eating in the hospital? Di-abetes Spectrum 2011;24:100–106
483. Boucher JL, Swift CS, Franz MJ, et al.Inpatient management of diabetes andhyperglycemia: implications for nutri-tion practice and the food and nutritionprofessional. J Am Diet Assoc 2007;107:105–111
484. Korytkowski MT, Salata RJ, Koerbel GL,et al. Insulin therapy and glycemic con-trol in hospitalized patients with di-abetes during enteral nutrition therapy:a randomized controlled clinical trial.Diabetes Care 2009;32:594–596
485. Umpierrez GE. Basal versus sliding-scaleregular insulin in hospitalized patientswith hyperglycemia during enteral nu-trition therapy. Diabetes Care 2009;32:751–753
486. Klonoff DC, Perz JF. Assistedmonitoringof blood glucose: special safety needsfor a new paradigm in testing glucose.J Diabetes Sci Tech 2010;4:1027–1031
487. D’Orazio P, Burnett RW, Fogh-AndersenN, et al.; International Federation ofClinical Chemistry Scientific DivisionWorking Group on Selective Electrodesand Point of Care Testing. ApprovedIFCC recommendation on reporting re-sults for blood glucose (abbreviated).Clin Chem 2005;51:1573–1576
488. Dungan K, Chapman J, Braithwaite SS,Buse J. Glucose measurement: confound-ing issues in setting targets for inpatientmanagement. Diabetes Care 2007;30:403–409
489. Boyd JC, Bruns DE. Quality specifica-tions for glucose meters: assessment bysimulation modeling of errors in insulindose. Clin Chem 2001;47:209–214
490. Shepperd S, McClaran J, Phillips CO,et al. Discharge planning from hospitalto home. Cochrane Database Syst Rev2010;(1):CD000313
491. Agency for Healthcare Research andQuality. Adverse events after hospitaldischarge [article online]. Available fromhttp://psnet.ahrq.gov/primer.aspx?pri-merID511. Accessed 25 August 2012
492. American Diabetes Association. Diabetesand employment. Diabetes Care 2011;34(Suppl. 1):S82–S86
493. American Diabetes Association. Diabetesand driving. Diabetes Care 2012;35(Suppl. 1):S81–S86
494. American Diabetes Association. Diabetesmanagement in correctional institutions.Diabetes Care 2011;34(Suppl. 1):S75–S81
495. Hoerger TJ, Segel JE, Gregg EW,Saaddine JB. Is glycemic control im-proving in U.S. adults? Diabetes Care2008;31:81–86
496. Cheung BM, Ong KL, Cherny SS, ShamPC, Tso AW, Lam KS. Diabetes preva-lence and therapeutic target achievementin the United States, 1999 to 2006. Am JMed 2009;122:443–453
497. Wang J, Geiss LS, Cheng YJ, et al. Long-term and recent progress in blood pres-sure levels among U.S. adults withdiagnosed diabetes, 1988-2008. Dia-betes Care 2011;34:1579–1581
498. Kerr EA, Heisler M, Krein SL, et al. Be-yond comorbidity counts: how do co-morbidity type and severity influencediabetes patients’ treatment prioritiesand self-management? J Gen Intern Med2007;22:1635–1640
499. Fernandez A, Schillinger D, Warton EM,et al. Language barriers, physician-patient language concordance, and gly-cemic control among insured Latinoswith diabetes: the Diabetes Study ofNorthern California (DISTANCE). J GenIntern Med 2011;26:170–176
500. The Robert Wood Johnson Founda-tion. Evidence for better care: diabetes.Available at http://www.improvingchroniccare.org/index.php?p=Diabetes&s=86.Accessed 26 November 2012
501. Coleman K, Austin BT, Brach C, WagnerEH. Evidence on the Chronic CareModel in the newmillennium. Health Aff(Millwood) 2009;28:75–85
502. Parchman ML, Zeber JE, Romero RR,Pugh JA. Risk of coronary artery diseasein type 2 diabetes and the delivery of careconsistent with the chronic care modelin primary care settings: a STARNetstudy. Med Care 2007;45:1129–1134
503. Davidson MB. How our current medicalcare system fails people with diabetes:lack of timely, appropriate clinical deci-sions. Diabetes Care 2009;32:370–372
504. Grant RW, Pabon-Nau L, Ross KM,Youatt EJ, Pandiscio JC, Park ER. Di-abetes oral medication initiation andintensification: patient views comparedwith current treatment guidelines. Di-abetes Educ 2011;37:78–84
505. Schillinger D, Piette J, Grumbach K, et al.Closing the loop: physician communi-cation with diabetic patients who havelow health literacy. Arch Intern Med2003;163:83–90
506. Rosal MC, Ockene IS, Restrepo A, et al.Randomized trial of a literacy-sensitive,culturally tailored diabetes self-management intervention for low-income Latinos: Latinos en Control.Diabetes Care 2011;34:838–844
507. Osborn CY, Cavanaugh K, Wallston KA,et al. Health literacy explains racial
disparities in diabetes medication ad-herence. J Health Commun 2011;16(Suppl. 3):268–278
508. Rothman R, Malone R, Bryant B, HorlenC, DeWalt D, Pignone M. The relation-ship between literacy and glycemic controlin a diabetes disease-management pro-gram. Diabetes Educ 2004;30:263–273
509. O’Connor PJ, Sperl-Hillen JM, RushWA,et al. Impact of electronic health recordclinical decision support on diabetescare: a randomized trial. Ann Fam Med2011;9:12–21
510. Garg AX, Adhikari NK,McDonaldH, et al.Effects of computerized clinical decisionsupport systems on practitioner perfor-mance and patient outcomes: a systematicreview. JAMA 2005;293:1223–1238
511. Smith SA, Shah ND, Bryant SC, et al.;Evidens Research Group. Chronic caremodel and shared care in diabetes: ran-domized trial of an electronic decisionsupport system. Mayo Clin Proc 2008;83:747–757
512. McLean DL, McAlister FA, Johnson JA,et al.; SCRIP-HTN Investigators. A ran-domized trial of the effect of communitypharmacist and nurse care on improvingblood pressure management in patientswith diabetes mellitus: Study of Cardio-vascular Risk Intervention by Pharma-cists–Hypertension (SCRIP-HTN). ArchIntern Med 2008;168:2355–2361
513. Wubben DP, Vivian EM. Effects of phar-macist outpatient interventions on adultswith diabetes mellitus: a systematic review.Pharmacotherapy 2008;28:421–436
514. Davidson MB, Ansari A, Karlan VJ. Effectof a nurse-directed diabetes diseasemanagement program on urgent care/emergency room visits and hospital-izations in a minority population. Di-abetes Care 2007;30:224–227
515. Stone RA, Rao RH, Sevick MA, et al.Active care management supported byhome telemonitoring in veterans withtype 2 diabetes: the DiaTel randomizedcontrolled trial. Diabetes Care 2010;33:478–484
516. Berikai P, Meyer PM, Kazlauskaite R,Savoy B, Kozik K, Fogelfeld L. Gain inpatients’ knowledge of diabetes man-agement targets is associated with betterglycemic control. Diabetes Care 2007;30:1587–1589
517. Tricco AC, Ivers NM, Grimshaw JM,et al. Effectiveness of quality improve-ment strategies on the management ofdiabetes: a systematic review and meta-analysis. Lancet 2012;379:2252–2261
518. O’Connor PJ, Bodkin NL, Fradkin J,et al. Diabetes performance measures:current status and future directions. Di-abetes Care 2011;34:1651–1659
519. Peikes D, Chen A, Schore J, Brown R.Effects of care coordination on hospi-talization, quality of care, and healthcare expenditures among Medicare
care.diabetesjournals.org DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 S65
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from

beneficiaries: 15 randomized trials.JAMA 2009;301:603–618
520. Feifer C, Nemeth L, Nietert PJ, et al. Dif-ferent paths to high-quality care: threearchetypes of top-performing practicesites. Ann Fam Med 2007;5:233–241
521. Cebul RD, Love TE, Jain AK, Hebert CJ.Electronic health records and quality ofdiabetes care. N Engl J Med 2011;365:825–833
522. Ralston JD, Hirsch IB, Hoath J, MullenM, Cheadle A, Goldberg HI. Web-basedcollaborative care for type 2 diabetes:a pilot randomized trial. Diabetes Care2009;32:234–239
523. Battersby M, Von Korff M, Schaefer J,et al. Twelve evidence-based principlesfor implementing self-managementsupport in primary care. Jt Comm J QualPatient Saf 2010;36:561–570
524. Grant RW, Wald JS, Schnipper JL, et al.Practice-linked online personal healthrecords for type 2 diabetes mellitus:a randomized controlled trial. Arch In-tern Med 2008;168:1776–1782
525. Pullen-Smith B, Carter-Edwards L,Leathers KH. Community health am-bassadors: a model for engaging com-munity leaders to promote better health
in North Carolina. J Public HealthManag Pract 2008;14(Suppl.):S73–S81
526. Bojadzievski T, Gabbay RA. Patient-centered medical home and diabetes.Diabetes Care 2011;34:1047–1053
527. Rosenthal MB, Cutler DM, Feder J. TheACO rulesdstriking the balance be-tween participation and transformativepotential. N Engl J Med 2011;365:e6
528. Washington AE, Lipstein SH. The Pa-tient-Centered Outcomes Research In-stitutedpromoting better information,decisions, and health. N Engl J Med2011;365:e31
S66 DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY 2013 care.diabetesjournals.org
Position Statement
by guest on January 27, 2014http://care.diabetesjournals.org/Downloaded from