dh220 dental materials - erie community collegefacultypages.ecc.edu/lamannac/pdf lectures...
TRANSCRIPT
DH220 Dental Materials
Lecture #4
Prof. Lamanna RDH, MS

Restorative Dentistry:
Composite
Ivoclar 4 Seasons Composite System®
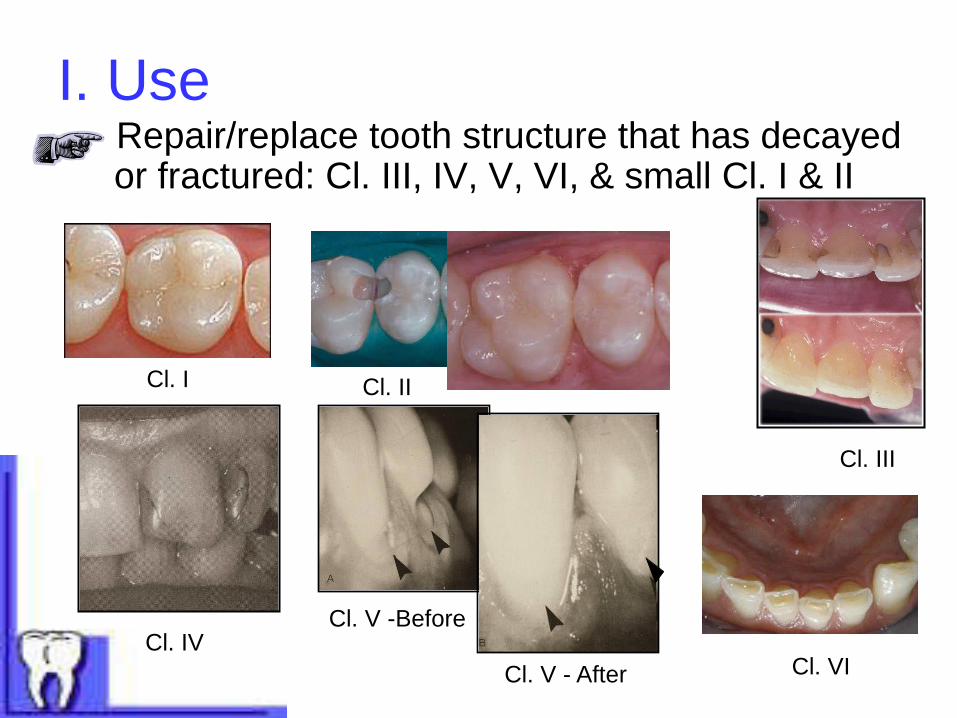
I. Use - Repair/replace tooth structure that has decayed
or fractured: Cl. III, IV, V, VI, & small Cl. I & II
Cl. V -Before
Cl. V - After
Cl. IV
Cl. I Cl. II
Cl. III
Cl. VI

- Enhance esthetic appearance of teeth: veneers, close diastemas, contour (reshape) teeth
Veneers
Diastemia closed
Recontour peg
laterals

- Cores for cast restorations
- Repairing fractured/chipped porcelain restorations

II. Characteristics
• ↓ thermal conductivity
• ↑ thermal expansion (percolation)
• Polymerization shrinkage
• ↑ sorption
• Color stability (staining due to surface roughness,
internal change)
• Strength: tensile similar to amalgam; ↓ compressive
• ↓abrasion resistance
• Retention mechanism:
chemical
Mechanical
retention
Chemical
retention
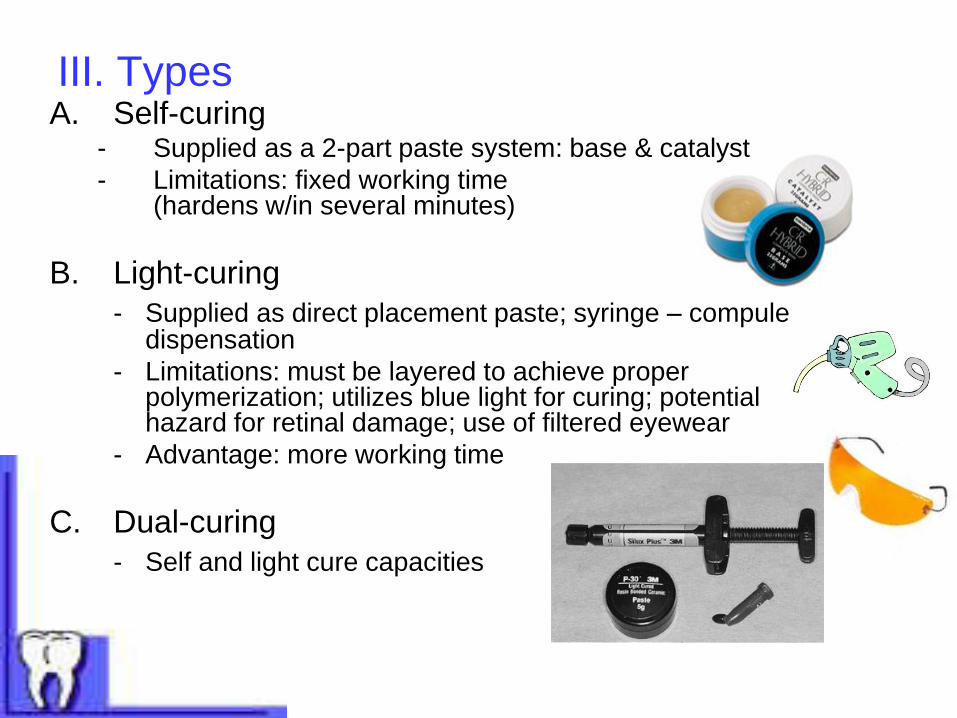
III. Types A. Self-curing
- Supplied as a 2-part paste system: base & catalyst
- Limitations: fixed working time (hardens w/in several minutes)
B. Light-curing
- Supplied as direct placement paste; syringe – compule dispensation
- Limitations: must be layered to achieve proper polymerization; utilizes blue light for curing; potential hazard for retinal damage; use of filtered eyewear
- Advantage: more working time
C. Dual-curing
- Self and light cure capacities
IV. Composition A. Polymer (resin) matrix
1. BIS-GMA (bisphenol-A glycidal methacrylate)
2. Triethylene glycol dimethacrylate
B. Glass particles (fillers)
1. Ground quartz, glasses, silica particles
*Always coated with a coupling agent: silane. WHY? Enhances adherence of matrix (resin) to the filler particles.
2. Particle size
a. Macrofills – 10-25 µ - ↑ strength
- ↓ polishability
- ↓ wear resistence (KHN – 55)
- quartz
- primarily used for orthodontics (luting brackets) and cores

b. Microfils – 0.04 µ
- ↓ strength
- ↑ polishability
- silica
c. Small particle – 1 – 5 µ
- strength, but not as strong as macro
- polishable, but not as smooth as micro
- glasses
d. Hybrids (micro + small particle)
- ↑strength
- ↑polishability
- glasses
- radiopaque
Composite surface
Magnified particles
p. 59
C. Chemicals – promotes polymerization
1. Self-curing system:
a. benzoyl peroxide
b. amine
2. Light-curing system:
a. camphoroquinone
b. amine
D. Pigments – provide different shades to match existing teeth
● inorganic oxides
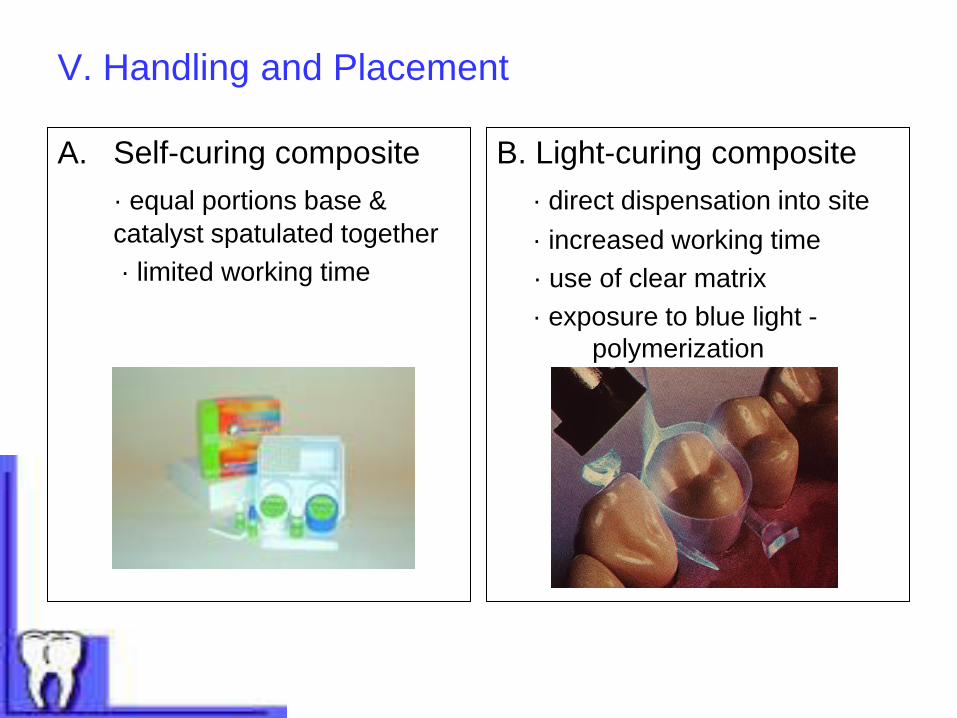
V. Handling and Placement
A. Self-curing composite
· equal portions base &
catalyst spatulated together
· limited working time
B. Light-curing composite
· direct dispensation into site
· increased working time
· use of clear matrix
· exposure to blue light -
polymerization

Chemical Retention ● Step #1 – Acid etchant
– 10-37% phosphoric acid; removes smear
layer on dentin
- applied, rinsed, dried
● Step #2 – Primer
- wetting agent- ↑ penetration into
dentinal tubules
- applied, not rinsed, dried sparingly
● Step #3 – Adhesive (resin material)
- interlocking with dentin to achieve chemical retention –
referred to as “hybrid zone”
- applied, light-cured
Chelating agent
Smear layer
Dentin
Enamel
Process of decalcifying &
removing tooth structure by
chemical means.
Return
Ground dentin & cytoplasmic
cells that are mixed together as
the tooth is prepped. It is sticky
and adheres to the tooth
surface; “smeared” inside the
tooth prep. Return
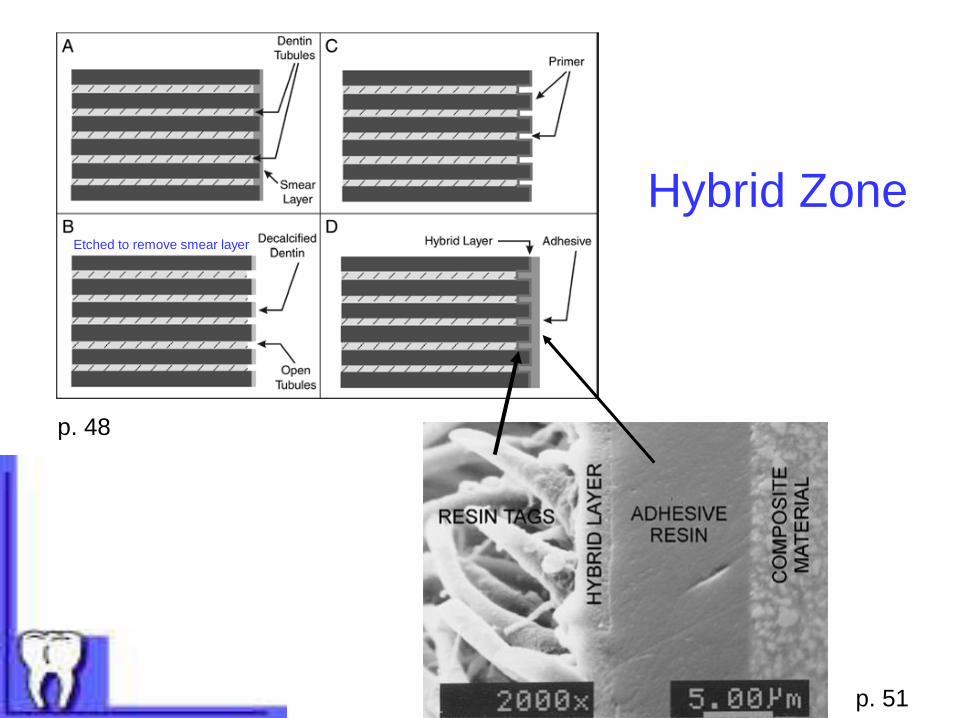
Hybrid Zone Etched to remove smear layer
p. 48
p. 51

VI. Polymerization A. Two major considerations -
1. Polymerization shrinkage
a. overall volume shrinks
b. creates marginal gaps – breaks chemical seal
Result – sensitivity, 2º decay
2. Extent & depth of curing
a. exposure time –
☼ quantity of light shone on material – do not under cure; impossible to over cure
☼ quality of light of shone on material – bulb should be checked regularly on meter
b. Composite depth – built-up in thin (1.5-2 mm) layers to ensure proper curing; aids in polymerization shrinkage outcome
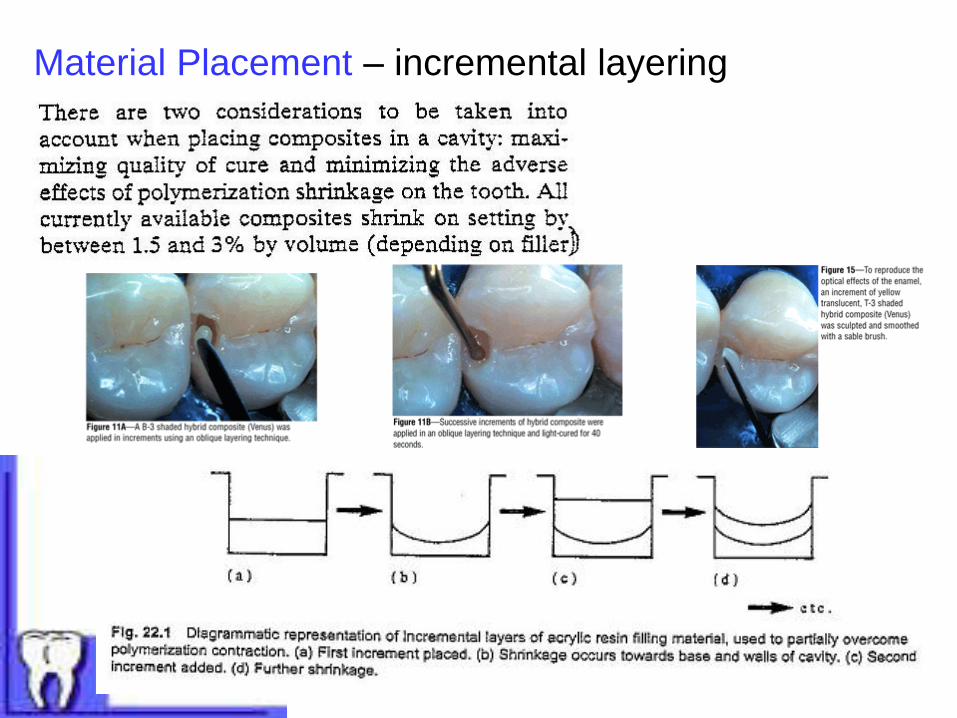
Material Placement – incremental layering

Vll. Finishing A. Can be finished & polished after placement
B. Wet field, carbide burs, diamonds, discs with varying
grades of abrasiveness
C. Polishing – aluminum oxide or diamond pastes;
composite polishing kits (lab)

Dental Charting – Paper Chart Black’s Classification I – VI Know them!!
Dental charting on a paper chart – hand-out #2
24
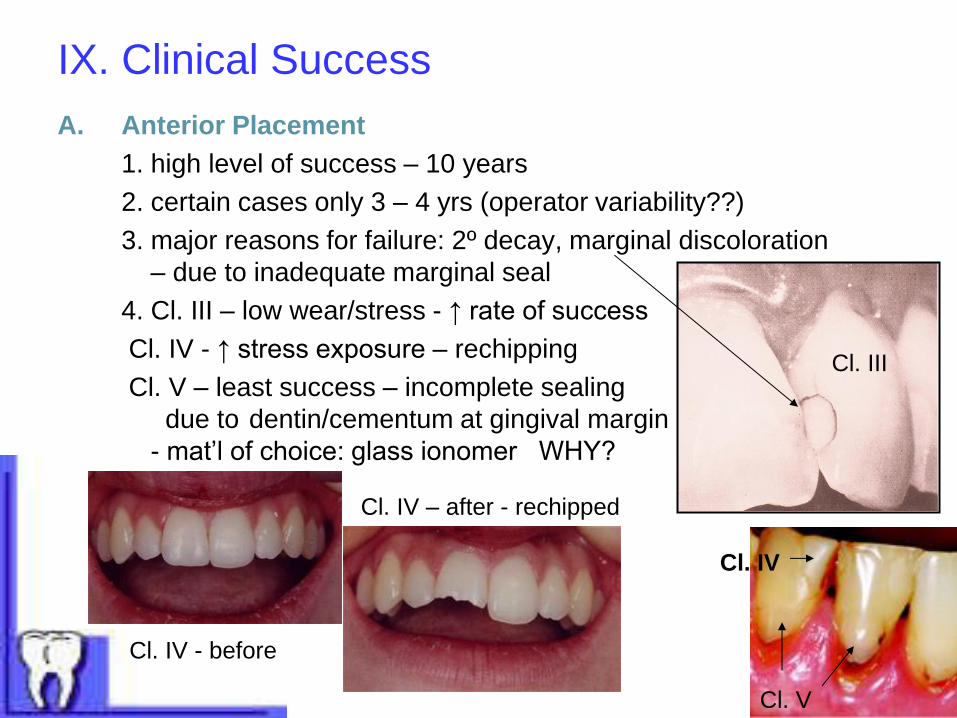
IX. Clinical Success
A. Anterior Placement
1. high level of success – 10 years
2. certain cases only 3 – 4 yrs (operator variability??)
3. major reasons for failure: 2º decay, marginal discoloration
– due to inadequate marginal seal
4. Cl. III – low wear/stress - ↑ rate of success
Cl. IV - ↑ stress exposure – rechipping
Cl. V – least success – incomplete sealing
due to dentin/cementum at gingival margin
- mat’l of choice: glass ionomer WHY?
Cl. III
Cl. V
Cl. IV - before
Cl. IV – after - rechipped
Cl. IV
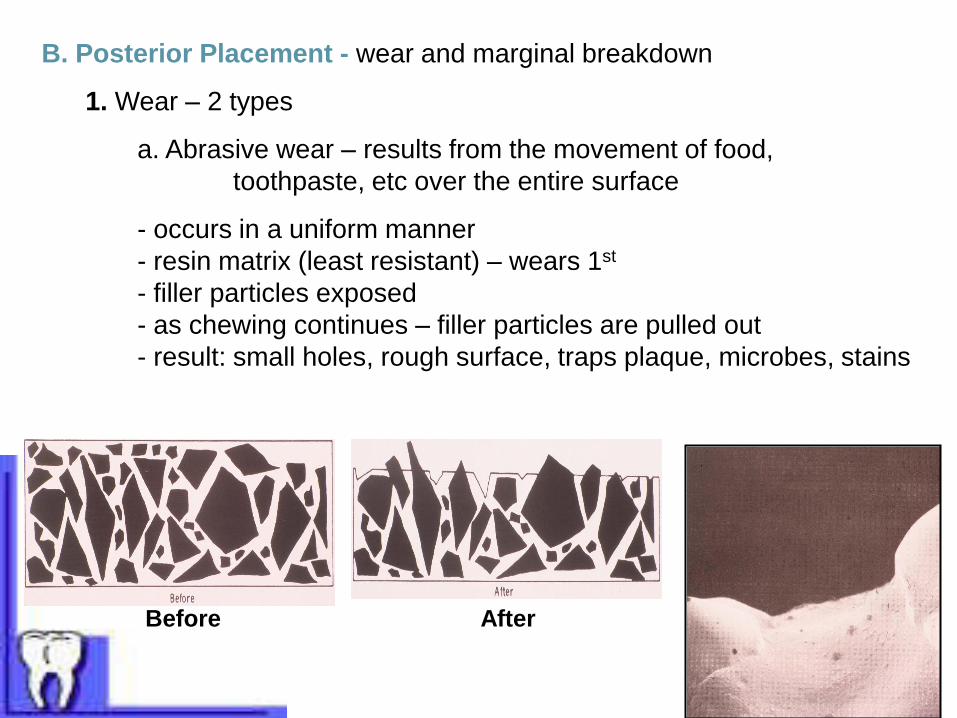
B. Posterior Placement - wear and marginal breakdown
1. Wear – 2 types
a. Abrasive wear – results from the movement of food,
toothpaste, etc over the entire surface
- occurs in a uniform manner
- resin matrix (least resistant) – wears 1st
- filler particles exposed
- as chewing continues – filler particles are pulled out
- result: small holes, rough surface, traps plaque, microbes, stains
Before After
b. Contact/Attrition wear – results from direct contact with opposing dentition
- 3 - 4 times more extensive damage then abrasive wear
KHN: enamel = 350
amalgam = 165
composite = 40 – 80
- Studies have shown that composites last 7-10 years, which is comparable
to amalgam except in very large restorations, where amalgam lasts much
longer than composites.
2. Premolars – less wear than molar placement due to less force during mastication
3. Contraindication to placement: bruxism, grinding
4. No “self sealing” mechanism
5. Exposed filler particles could abrade opposing enamel
6. RDH clinical management –
a. OHI –
b. Instrument choices -
c. Fluoride choices -
Any Questions??