development of new treatment modalities oncolytic viruses ...€¦ · oncolytic viruses and...
TRANSCRIPT

By
Professor Kjell Öberg, M.D., Ph.D.
Dept. of Endocrine Oncology , University Hospital , Uppsala, Sweden
Nashville Oct. 2011
Development of
New Treatment
Modalities –
Oncolytic Viruses
and Nano-
technique

Hallmarks of GEP-NETs
Initially diffuse symptoms (Doctors and
patient delay of 3-4 years!)
More than 60% present metastatic
disease at diagnosis
Variable growth rate
Expression of specific receptors
(SSTR, DA, GF)
Highly vascular

Therapeutic Options NETs
Surgery
– Curative (rarely), Ablative (very often)
Debulking
– Radiofrequency ablation (RFA)
– Embolization/chemoembolization/radioembolization
(Spherex®)
Medical therapy
– Chemotherapy
– Biological treatment:
• Somatostatin analogs
• α-interferon
• m-TOR inhibitors
• VEGF R inhibitors
• Other TKI’s
Irradiation
– External (bone, brain-mets)
– Tumor targeted, radioactive therapy (MIBG, Y90-DOTATOC,
Lu177 -DOTATATE)

177Lu-DOTA-octreotate therapy The Uppsala experience
Results: CR 1 (1%)
PR 57 (31%) 43%
MR 20 (11%)
SD 99 (54%)
PD 8 (4%)
32 patients who responded or had SD later progressed
• 229 patients 96 (midgut), 13 (lung), 17 (rectal), 44 (non-functioning
pNET), 9 (gastrinoma), 6 (glucagonoma), 7 (paraganglioma/
pheochromocytoma)
• No. treatments: 842
• Follow-up (n=185): Mean 13 mo (range 2–57 mo)

Chemotherapy
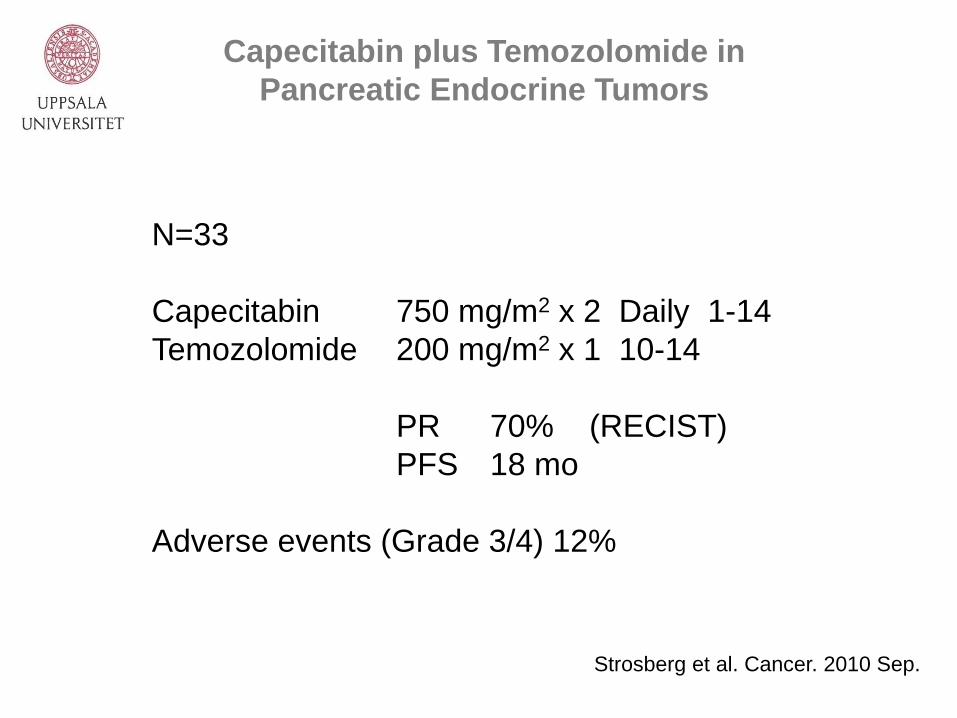
Capecitabin plus Temozolomide in
Pancreatic Endocrine Tumors
N=33
Capecitabin 750 mg/m2 x 2 Daily 1-14
Temozolomide 200 mg/m2 x 1 10-14
PR 70% (RECIST)
PFS 18 mo
Adverse events (Grade 3/4) 12%
Strosberg et al. Cancer. 2010 Sep.

Temozolomide-Based Chemotherapy
in Progressing PDECs After First-Line
Chemotherapy
N=25 (GI-NETS)
Treatment Tem alone N=5
Tem + Cap N=13
Tem + Cap + bev N=7
Responses
CR n=1 (4%) (48 mo)
PR n=7 (29%) (median 19 mo)
SP n=9 (38%) (median 18 mo)
Median PFS 6 mo (95%) CI 4-14 mo)
Median OS 22 mo (95% CI 8-27 mo)
Toxicity 1 Grade 3 hematol.tox
(Grade 3-4) 1 Grade 3 liver tox
1 patient developed diabetes
Welin S et al. Cancer 2011

Agent (s)
Target (s) N Tumour ORR Outcomes Comments
Bevacizumab +
octreotide VEGF 22 Carcinoid 18% 16.5 mo (PFS) -
Sunitinib VEGFR,
PDGFR, RET,
FLT3
41
66
Carcinoid
PNETs
2%
17%
10.5 mo (TTP)
7.7 mo (TTP)
-
Sorafenib VEGFR, PDGF,
Raf
51
42
Carcinoid
PNETs
7%
17%
7.8 mo (PFS)
11.9 mo (PFS)
-
Vatalanib
VEGFR, PDGFR 11 GEPNET 0% NR Ongoing
Pazopanib VEGFR,
PDGFR,
30
30
Carcinoid
PNET
-
-
-
-
Ongoing
Motesanib VEGFR,
PDGFR, RET
44 LGNET - - Ongoing
Atiprimod
Unclear 25 LGNET 0% 76% at 6 mo (TTP) Ongoing
Bevacizumab +
2-methoxyestradiol VEGF 31 Carcinoid 0 Median PFS not
reached at 8.9 mo
Ongoing
Angiogenesis inhibitors
Adapted from Phan and Yao, Oncology 2008
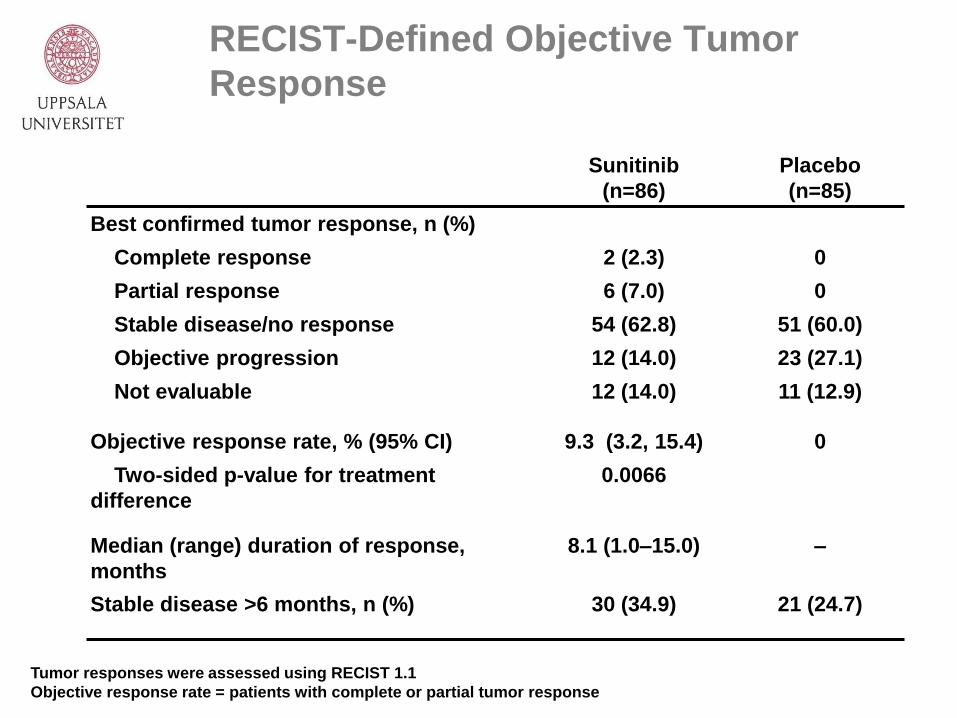
RECIST-Defined Objective Tumor
Response
Sunitinib
(n=86)
Placebo
(n=85)
Best confirmed tumor response, n (%)
Complete response
Partial response
Stable disease/no response
Objective progression
Not evaluable
2 (2.3)
6 (7.0)
54 (62.8)
12 (14.0)
12 (14.0)
0
0
51 (60.0)
23 (27.1)
11 (12.9)
Objective response rate, % (95% CI)
Two-sided p-value for treatment
difference
9.3 (3.2, 15.4)
0.0066
0
Median (range) duration of response,
months
8.1 (1.0–15.0) –
Stable disease >6 months, n (%) 30 (34.9) 21 (24.7)
Tumor responses were assessed using RECIST 1.1
Objective response rate = patients with complete or partial tumor response

Agent (s)
Target (s) N Tumour ORR Outcomes Comments
Everolimus+Octreotide
(MDACC)
mTOR 30
30
Carcinoid
PNETs
17
27
14.6 mo (PFS)
11.6 mo (PFS)
-
Everolimus
Everolimus+octreotide
(RADIANT-1)
mTOR 115
45
PNET
PNET
8
4
9.3 mo (PFS)
12.9 mo (PFS)
Patients with
PD at entry
Tensirolimus mTOR 21
15
Carcinoid
PNETs
5
7
6.0 mo (TTP)
10.6 mo (TTP)
Patients with
PD at entry
Everolimus + bevacizumab mTOR, VEGF 36 NET - - Ongoing
Everolimus + pasireotide mTOR, SMS Phase
1
NET - - Ongoing
Everolimus +
temozolomide
mTOR, chemo Phase
1/2
NET - - Ongoing
mTOR inhibitors
Adapted from Phan and Yao, Oncology 2008

Oncolytic Viruses as Anticancer
Agents
Replicating viruses as anticancer agents has three
major advantages over conventional therapy
i. A virus can kill drug-resistant cancer stem cells
ii. A virus propagates inside tumor cells before
lysing them lytic cell death leads to release of
large amount of progeny viruses which can infect
neighboring cells
iii. Presence of immunogenic virus within a tumor
can alter the otherwise immunosuppressive
milieu in favor of an anti-tumor immune
response. Stimulate dendritic cells to produce
IFN-α and IL-12 with induction of cytotoxic T-cell

Oncolytic Viruses
RNA viruses New Castle disease virus
(Phase 1-12 trials) Seneca Valley virus
Reovirus
DNA-viruses Adenovirus
Herpes simplex (HSP-2)
Vaccinia virus
Genetically modified
viruses ONYX-015 H101

Structure of Adenovirus

The Life Cycle of Adenovirus

Transcription map of the Adenovirus Genome
The adenovirus genome is organized in early (red),
intermediate (blue) and late (green) transcriptional units

Adenovirus Gene Products and
Their Functions

The Biogenesis and Functions of Micro RNAs
(miRNAs) and Other Small Interfering RNAs (siRNAs)

Neuroendocrine cells support E1A expression after Ad[CgA-
E1A] transduction
Leja J et al. Clin Cancer Res 2007;13:2455-2462
©2007 by American Association for Cancer Research

Selective replication of Ad[CgA-E1A] in cells of
neuroendocrine origin
Leja J et al. Clin Cancer Res 2007;13:2455-2462
©2007 by American Association for Cancer Research

Specific cytotoxicity of Ad[CgA-E1A] on cells of
neuroendocrine origin
Leja J et al. Clin Cancer Res 2007;13:2455-2462
©2007 by American Association for Cancer Research

Ad[CgA-E1A] suppresses carcinoid tumor growth in vivo
Leja J et al. Clin Cancer Res 2007;13:2455-2462
©2007 by American Association for Cancer Research

Freshly isolated hepatocytes do not express CgA
Leja J et al. Clin Cancer Res 2007;13:2455-2462
©2007 by American Association for Cancer Research

CgA RNA is highly expressed in midgut carcinoid cells and
barely detectable in freshly isolated hepatocytes
Leja J et al. Clin Cancer Res 2007;13:2455-2462
©2007 by American Association for Cancer Research

Ad[CgA-E1A] provides weak E1A expression in hepatocytes
Leja J et al. Clin Cancer Res 2007;13:2455-2462
©2007 by American Association for Cancer Research
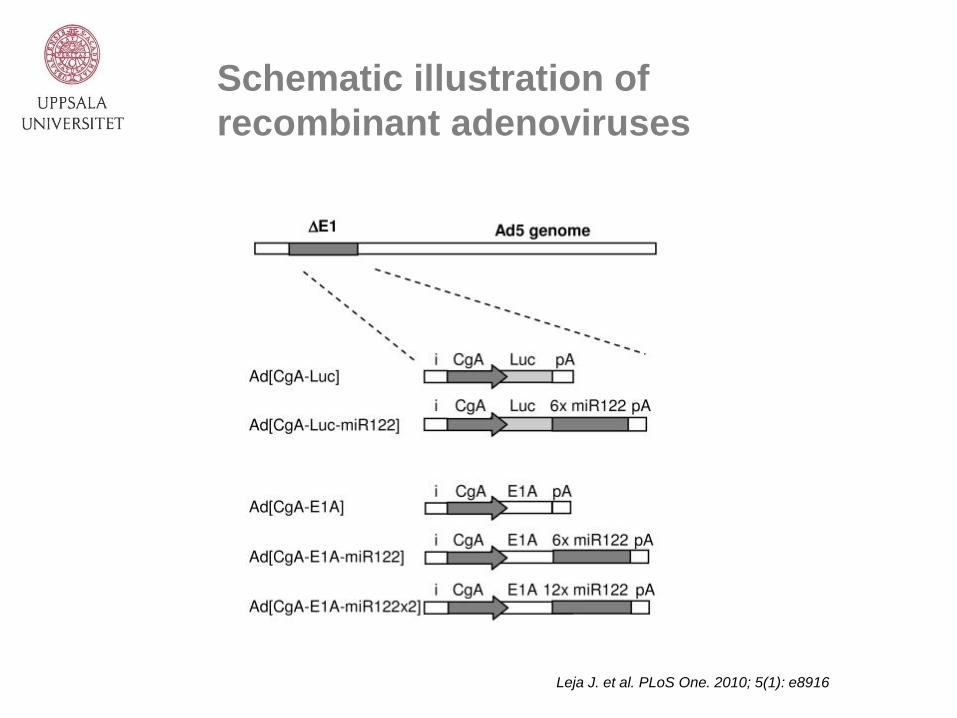
Schematic illustration of
recombinant adenoviruses
Leja J. et al. PLoS One. 2010; 5(1): e8916

Leja J. et al. PLoS One. 2010; 5(1): e8916
Specific silencing
of luciferase
expression in liver
cells by miR122 in
vitro and in vivo

Leja J. et al. PLoS One. 2010; 5(1): e8916
miR122-mediated
suppression of
adenoviral
protein
expression in
hepatic cells

Leja J. et al. PLoS One. 2010; 5(1): e8916
Replication arrest
and reduced
cytolytic activity
in hepatic cells
for adenoviruses
carrying miR122
target sites

Leja J. et al. PLoS One. 2010; 5(1): e8916
Lack of hepatotoxicity in mice injected
with Ad [CgA-E1A-miR122]

Leja J. et al. PLoS One. 2010; 5(1): e8916
Stronger reduction of
cytolytic ability in
hepatic cells by double-
targeted than single-
targeted adenovirus

Leja J, et al. Gene
Therapy 2011

Leja J, et al. Gene
Therapy 2011

Virus Delivery
Co-administration of immunosuppressive
agents
Coat the virus with PEG
Hide the virus within T-cells with specificity
for a tumor-associated antigen
Incorporation of transgenes to increase cell
penetration
Local delivery
Combination with cytotoxic or targeted small
molecules


Nanoparticles
communication for
amplified tumor
targeting
von Maltzahn G, et al. Nature
Materials. Vol 10, july 2011

Amplified tumor therapy with
communicating NPs
von Maltzahn G, et al. Nature
Materials. Vol 10, july 2011

Novel nanosystems for targeting
and diagnostics
Nanotubes
Dispersed lc
Bicelles
Nanogels/microgels
Nanodiscs Coated microgels
Malmsten, M.,“Surfactants and Polymers in Drug Delivery”,
Marcel Dekker, 2003.



111In-octreotide “uptake”
125I-somatostatin “uptake”

1) Vaso-expressing BON cells
2) Vector control
pSecTag2A vector
Materials and Methods

IFN-a signaling
A
WT Vector
IFN-α
Vector IFN-α
Control Vector
IFN-α
Vector
IFN-α
Inhibition of angiogenesis
Adhesion and invasion Morphology
Results IFN-α sinaling
Cell
proliferation

Conclusions
There is an unmet need for more
effective antitumor therapy in
metastatic NETs
Cytotoxic viruses demonstrates
potential for cure in metastatic NET
Combinations of cytotoxic viruses and
cytotoxic agents as well as targeting
small molecules might be the future
therapy for NETs
Nanoparticles for diagnosis and
therapy seems promising for
“targeting” therapy

Thank you!
Centre of Excellence Endocrine
Tumors, Uppsala University
http://www.endocrinetumors.org/
E n d o c r i n e T u m o r s C e n t r e o f E x c e l l e n c e
endocrinetumors.org