development of kidneys and its anamolies
TRANSCRIPT

DEVELOPMENT OF KIDNEYS AND ITS
ANAMOLIES
1

• "It is not birth, marriage, or death, but gastrulation which is truly the most important time in your life."
– Prof Lewis Wolpert
2

• Gastrulation begins between days 14 and 16 of human development.
• Gastrulation results in formation of the 3 germ layers:
• Mesoderm(e.g. muscle, bone, kidneys)
• Endoderm (e.g. gut) and
• Ectoderm (e.g. nervoussystem/epidermis)
3
Zygote
Blastocyst
Three germ layers:1) Mesoderm
2) Endoderm
3) Ectoderm

INTRODUCTION
• The embryonic structures that play an important role in development of GUS are:
1. Intermediate Mesoderm
2. Cloaca
4

INTERMEDIATE MESODERM
Intra-embryonic mesoderm is subdivided into
• Paraxial mesoderm
• Intermediate mesoderm
• Lateral mesoderm
5

6
Kidney Development
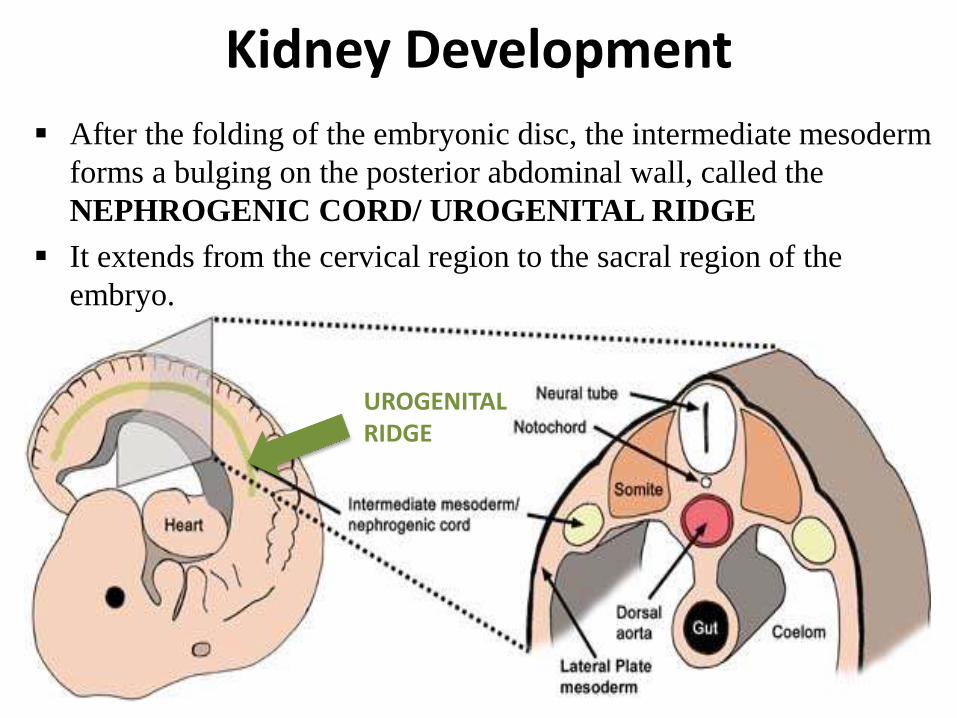
After the folding of the embryonic disc, the intermediate mesoderm
forms a bulging on the posterior abdominal wall, called the
NEPHROGENIC CORD/ UROGENITAL RIDGE
It extends from the cervical region to the sacral region of the
embryo.
UROGENITAL RIDGE

8

CLOACA
• Primitive urogenital sinus
1) Vesico-urethral canal
2) Definative urogenital sinus
- Pelvic part
- Phallic part
9

DEVELOPMENT OF KIDNEYS
• The kidneys develop originally as a pair of structures located in the cervical and thoracic region of the developing embryo.
• They develop from intermediate mesoderm.
10
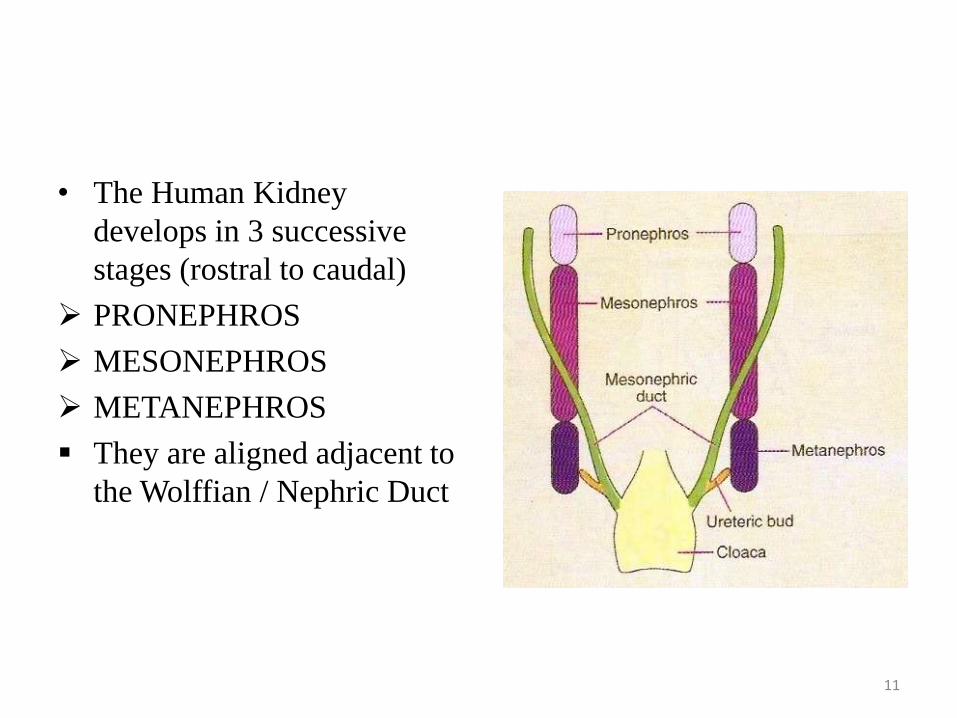
• The Human Kidney
develops in 3 successive
stages (rostral to caudal)
PRONEPHROS
MESONEPHROS
METANEPHROS
They are aligned adjacent to
the Wolffian / Nephric Duct
11

Development of Kidney• PRONEPHROS
– First to form, appears in the cervical region .
• MESONEPHROS
– Second to form, consist of a series of excretory tubules that develop in the thoracolumbarregion.
• METANEPHROS
– Final formation, in the sacral region

Ontogeny recapitulates phylogeny
13

Ernst Haeckel 1860
• Ontogeny is the development of the individual
• Phylogeny is the evolution of the species• So this is the idea that during
development an organism (or an organ) goes through the same stages as during their evolution.
• Consider the Frog– It development retraces the
evolution of vertebrates from fish to reptiles
– From the tadpole stage• Water breathing with tail and no
limbs (like a fish)• Rudimentary limbs• Reduction of tail• Development of lungs –
breathes air• Fully developed limbs, loss of tail
moves onto land– To the fully developed frog
14

15

Pronephros
The PRONEPHROS
develops from the cranial
most part of urogenital
ridge.
It is transitory, non
functional and regresses
completely by 5 weeks of
gestation.
Analogous to primitive
fish.

• The human pronephros are never functional and degenerates on 24th or 25th
day.
• A nephric duct is formed in relation to the pronephrosand ends into cloaca however persists.
• 7-10 solid or tubular arranged cell groups in the cervical region (head kidney)
17

Pronephric
tubule
Pronephros
Time:3rd week
Function:no
Destiny: degeneration in
the 5th week

Mesonephros
MESONEPHROS develops caudal to the Pronephros in thoracolumbar region.
It consists of a series of tubules that drain into the nephric duct, which can be called the Mesonephric duct.
Transistionary Excretory organ for embryo until metanephros takes over.

• The blind end of the duct grows towardsthe primitive cloaca and soon fuses to itabout 28th day.
By the 4th month of gestation-completely disappears.
Before its degeneration some of its cells migrate and ultimately form the
• Adrenal glands• Gonads
20

Time:end of 4th week
Function:
transient urinary
Destiny:
Most degeneration,
Small part form male
excurrent duct
Mesonephric duct
Mesonephric tubule

METANEPHROS, third
and final stage of Kidney
development
It results from Reciprocal
inductive signals between
the Metanephric
Mesenchyme (MM) and the
Ureteric Bud (UB) at the
caudal end of the
Urogenital bridge.
Ureteric bud is an
outgrowth at the distal end
of the Wolfian duct, first
visible at approx. 5 weeks
of gestation.
Metanephros

Time:begin at 5th week,
exist forever
Function:begin at 3th month,
urinary function
Position:rise gradually
Metanephros
Metanephros

Kidney Development
Development of the
NEPHRON
Development of the
COLLECTING SYSTEM Development
of the VASCULATURE

Development of Nephron
Upon invasion of UB in the
loose MM, signals from MM
cause UB to branch into a T -
tubule
Signals from UB induce the
MM to condense along the
surface of UB
The METANEPHRIC
MESENCHYME (MM)
becomes distinct from the
surrounding loose
mesenchymal cells and come
to lie adjacent to the
URETERIC BUD (UB).

After condensation a subset of the MM
aggregates inferior and adjacent to the
tips of the branching ureterIc bud,
forming the PERITUBULAR
AGREGATES.
These undergo mesenchyme – to –
epithelial transformation and form the
RENAL VESICLE
The Renal vesicle ultimately forms the
• Glomerulus
• Proximal Convoluted tubule
• Loop of Henle
• Distal Convoluted tubule
Renal Vesicle

Renal Vesicle in contact with the
epithelium of the ureteric bud forms
the ‘COMMA SHAPE’
Glomerulus develops from the most
proximal end of the Renal Vesicle,
farthest from UB tip.
These cells develop into Podocytes.
Vascular cleft develops between
podocyte layes and the more
proximal cells – ‘S SHAPE’
Endothelial cells migrate into the
vascular cleft
Mesangial cell ingrowth follows the
endothelial cells into the vascular
cleft.


29

• In principle, all nephrons are formed in the same way and can be classified into fairly well-defined developmental stages (Larsson et al, 1983).
- Stage I
- Stage II
- Stage III
- Stage IV
30

Development of the Collecting
System The collecting ducts are all derived from the Ureteric Bud.
The ureteric bud initially penetrates the metanephric mesoderm to form an ampulla,
and then undergoes repeated branching to form the ureters, renal pelvis, major calyces,
minor calyces, and collecting ducts.
This branching is highly patterned

• By the 6th week, the ureteric bud has bifurcated at least four times, yielding approximately 16 branches.
• These branches then coalesce to form two to four major calyces extending from the renal pelvis.
• By the 7th week, the next four generations of branches also fuse, forming the minor calyces.
• By the 32nd week, approximately 11 additional generations of bifurcation have resulted in approximately 1 million to 3 million branches, which become the collecting duct tubules
32

After the first few rounds of branching of the UB derivatives and
the concomitant induction of nephrons, the kidney begins to
become divided into an outer CORTICAL region (where
nephrons are being induced) and an inner MEDULLARY region
where the collecting system forms.
As growth continues successive groups of nephrons are induced
at the peripheral regions of the kidney, known as the
NEPHROGENIC ZONE.

Schematic representation of progressive nephron
differentiation.• Older, more
differentiated nephrons are located in the inner part of the kidney near the juxtamedullaryregion.
• Newer, less differentiated nephrons are found at the periphery.
34

Development of Vasculature
• Angiogenic Hypothesis- derived from branches off aorta and other pre-existing extrarenalvessels.
• Vasculogenic Hypothesis-originate in situ from vascular progenitor cells (VEGF).

Ascent of Kidneys
• During the fifth and sixth weeks of development, the maturekidneys lie in the pelvis with their hila pointed anteriorly.
• As the pelvis and abdomen grow, the kidneys slowly moveupward.
• By the seventh week, the hilum points medially and thekidneys are located in the abdomen.
• As the embryo continues to grow in a caudal direction, thekidneys are left behind and eventually come to lie in aretroperitoneal position at the level of L1 by the ninth weekof development.
• In the meantime, the kidneys have completed rotation andthe hila now face anteromedially.

• The metanephric ducts elongate and become the ureters.
• As the kidney ascends it receives new segmental arteries from the aorta and loses those vessels below (“climbing a ladder”). Thus sometimes there is more than one renal artery.
• Sometimes one kidney fails to ascend => pelvic kidney
• Sometimes the left and right kidneys become attached in the pelvis then the horseshoe kidney can’t ascend above the inferior mesenteric artery
37



Molecular mechanism of ureteral bud outgrowth
GDNF-(glial cell line- derived neurotrophic factor) ret Signaling in Kidney Development
Ret is a tyrosine kinase receptor
Ret is expressed in the Wolfian duct and the ureteric bud.
For stimulation of ureteric bud branching
By the time the bud has branched several times, expression is restricted to the tips of the
branches.

• In particular, several lines ofexperimental evidence have revealeda crucial role of the RET-GDNF-GFRα1pathway in ureteric bud outgrowth.
41

Timeline of Kidney Embryology
• Week 4 : appearance of Wolffian or Mesonephric Duct
• Day 28 : formation of Ureteric Bud (UB)
• Week 4-8 : Initial MM induction and UB branching
• Week 8 : First nephrons are formed
• Week 6-8 : kidneys ascend from pelvis to lumbar location
• Week 8-15 : Period of UB branching with stochastic formation of UB ampulla and nephron units
• Week 10 : filtration begins
• Week 32-36: End of Nephrogenesis

CONGENITAL ANOMALIES
1. Anomalies of number
2. Anomalies of ascent
3. Anomalies of form and fusion
4. Anomalies of rotation
5. Anomalies of the collecting system
6. Anomalies of renal vasculature
43

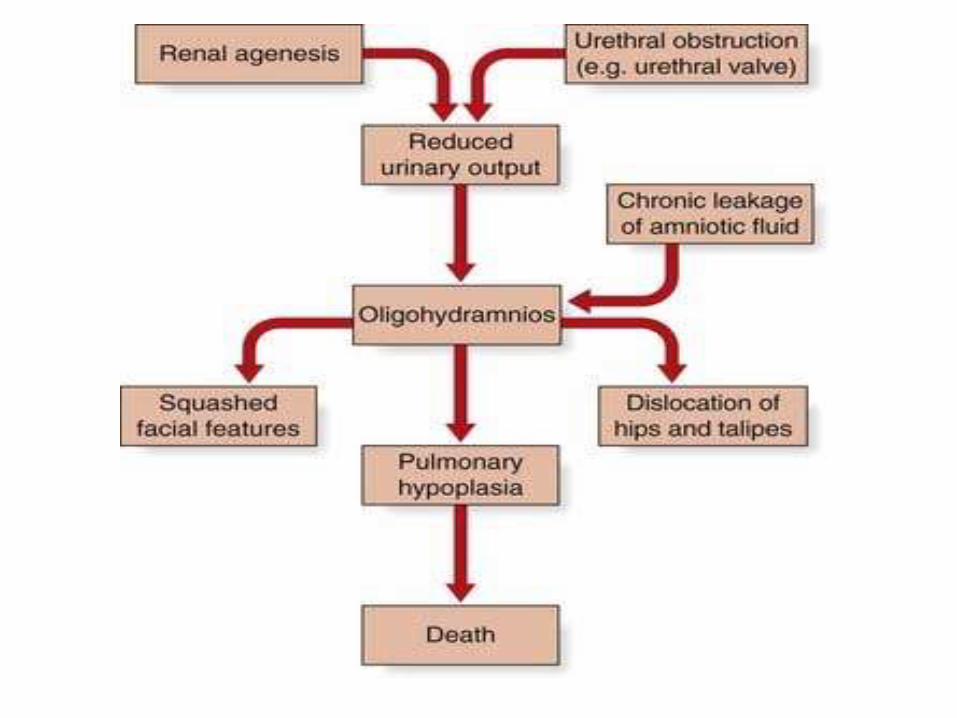
ANOMALIES OF NUMBER1. Bilateral renal agenesis (BRA) -
• First recognized 1671 by Wolfstrigel.
• Quite rare.
• 500 cases have been cited in the literature.
• Significant Males predominance.
• Increase maternal age.
44
45
Cause : The absence of a nephrogenic ridge on the dorsolateral aspect of the coelomic cavity or the failure of a ureteral bud to develop from the mesonephric duct will lead to agenesis of the kidney.
• Besides the absence of functioning kidneys, each ureter may be either wholly or partially absent.
• Complete ureteral atresia is observed in 50%.
46

• 40% of the affected infants are stillborn.
• Most of the children who are born alive do not survive beyond 48 hours because of respiratory distress associated with pulmonary hypoplasia.
47
48

Associated anomalies seen are
1. Low birth weight – 1000-2000 g.
2. IUGR.
3. Potters facial appearance.
4. Legs often bowed and clubbed.
5. Skin excessively dry.
6. Hands are relatively large and clawlike.49

7. Pulmonary hypoplasia - anephric fetus fails to produce proline, which is needed for collagen formation in the bronchiolar tree.
8. In males, rarely hypospadias and undescended testis.
9. In females, ovaries are hypoplastic or absent. Uterus is usually rudementary or bicornuate with vagina short, blind or completely absent.
50

• Diagnosis – characteristic potter facies, presence of oligohydraminos and presence of amnion nodusum - small white, keratinized nodules found on the surface of the amniotic sac—may also suggest this anomaly.
• Anuria after the first 24 hours without distention of the bladder should suggest renal agenesis.
51

• Renal ultrasonography is probably the easiest way to identify the kidneys and bladder to confirm the presence or absence of urine within these structures.
• Doppler ultrasonography to diagnose renal agenesis when renal arteries are not detectable has been highly accurate, even in fetuses with oligohydramnios.
52
2. Unilateral renal agenesis (URA) –
• More commonly than BRA.
• Occurs once in 1100 births.
• Males predominant 8:1.
• More frequently on left side.
53

Cause :
• Fault lies most probably with the ureteral bud.
• Complete absence of a bud or aborted ureteral development prevents maturation of the metanephric blastema into adult kidney tissue.
• It is unlikely that the metanephros is responsible, because the ipsilateral gonad is rarely absent, malpositioned, or nonfunctioning.
• Occurs no later than 4th or 5th week of gestation.54

• Magee and coworkers (1979) proposed an embryologic classification based on the timing of the faulty differentiation-
• Type I – before 4th week.
unilateral agenesis of GUS.
55

• Type II – early 4th week.
- affects both mesonephric duct and ureteral buds.
- didelphys uterus with obstructive ipsilateral horn and vagina.
• Type III – after 4th week.
- mesonephric duct devlopsnormally only ureteral bud or metanephric blastema affected.
56

Associated anomalies –
1. The ipsilateral ureter is completely absent in slightly more than half of the patients.
2. Ipsilateral adrenal agenesis -rare
3. Genital anomalies are much more frequently observed. Despite the predominance in males(10% to 15%), reproductive organ abnormalities seem to occur more in females (25% to 50%).
57

• The diagnosis should be suspected during a physical examination when the vas deferens or body and tail of the epididymis is missing or when an absent, septate, or hypoplastic vagina is associated with a unicornuate or bicornuate uterus.
• Cystoscopy - reveals an asymmetrical trigone
either partial or complete ureteral atresia
58

59

3. Supernumerary kidney –
• Is truly an accessory organ with its own collecting system, blood supply, and encapsulated parenchymalmass.
• Only 100 cases reported.
• Left side.
• Affects equally men and women.
60

Cause :
• The sequence of interdependent events involved in ureteralbud formation and metanephric blastema development, which is required for the maturation of the normal kidney, probably also allows for the occurrence of a supernumerary kidney.
• It is postulated that a deviation involving both of these processes must take place to create the anomaly.
61

• A second ureteral outpouching off the wolffian duct or a branching from the initial ureteral bud appears as a necessary first step.
• Next, the nephrogenic anlage may divide into two metanephric tails, which separate entirely when induced to differentiate by the separate or bifid ureteral buds.
• The twin metanephros develop only when the bifid or separate ureteral buds enter them.
62

• The supernumerary kidney is a distinct parenchymatous mass that may be either completely separate or only loosely attached to the major kidney on the ipsilateral side.
• In general, it is located somewhat caudal to the dominant kidney, which is in its correct position in the renal fossa.
• Occasionally, the supernumerary kidney lies either posterior or craniad to the main kidney, or it may even be a midline structure anterior to the great vessels and loosely attached to each of the other two kidneys
63

• A to H, Various patterns of urinary drainage when ureters form a common stem.
• All kidney positions are relative only and are depicted on the left side for ease of interpretation.
• Dashed lines indicate that detail was not defined
64

• The ureteral interrelationships on the side of the supernumerary kidney are quite variable.
• Convergence of the ipsilateral ureters distally to form a common stem and a single ureteral orifice occurs in 50% of the cases.
• Two completely independent ureters, each with its own entrance into the bladder, are seen in the other 50% of cases.
65

• It may not produce symptoms until early adulthood.
• Average age at diagnosis 30 to 36 years.
• A supernumerary kidney may become symptomatic from hydronephrosis or even stone formation.
• Cystoscopy reveals one or two ureteral orifices on the ipsilateral side.
66

ANOMALIES OF ASCENT1. Simple renal ectopic –
• Fails to reach its normal location in renal fossa.
• Found in – pelvis, iliac, abdomen, thorax and crossed.
• 1 in 900.
• Left side is more common.
67

• The classification of ectopia is based on the position of the kidney within the retroperitoneum:
• the pelvic kidney is opposite the sacrum and below the aortic bifurcation;
• the lumbar kidney rests near the sacral promontory in the iliac fossa and anterior to the iliac vessels;
• the abdominal kidney is so named when it is above the iliac crest and adjacent to the second lumbar vertebra.
68

• Factors that may prevent the orderly movement of kidneys include
- ureteral bud maldevelopment,
- defective metanephric tissue that by itself fails to induce ascent,
- genetic abnormalities, and
- maternal illnesses or teratogenic causes.
• Genital anomalies are more commonly associated with it.
69

• The renal pelvis is usually anterior because the kidney has incompletely rotated.
• As a result, 56% of ectopic kidneys have a hydronephroticcollecting system.
• Half of these cases result from obstruction at either the ureteropelvic or the ureterovesical junction (70% and 30%, respectively); 25% from reflux grade 3.
70

Associated anomalies :
• In females - bicornuate or unicornuate uterus with atresia of one horn, rudimentary or absent uterus and proximal and/or distal vagina.
• In males - undescended testes, duplication of the urethra, and hypospadias.
• Rarely adrenal glands are absent or abnormally positioned.
71

• Clinically asymptomatic.
• Vague abdominal complaints or frank ureteral colic secondary to obstructing stone is the most frequent symptoms leading to discovery of the misplaced kidney.
• The abnormal position of the kidney results in a pattern of direct and referred pain that is atypical for colic and may be misdiagnosed as acute appendicitis or as pelvic organ inflammatory disease in female patients.
72

2. Thoracic kidney –
• partial or a complete protrusion of the kidney above the level of the diaphragm into the posterior mediastinum.
• 200 cases have been reported.
• The renal counter and collecting system are usually normal.
73

74

Cause :
• Kidney reaches to its normal location by end of 8th week.
• Delayed closure of diaphramatic anlage which allows renal ascent above the level of future diaphragm or
• The kidney overshoot because of accelerated renal ascent before diaphragmatic closure.
75

• Associated anomalies : elongated ureter.
• Majority are asymptomatic.
• Diagnosis is most commonly made after a routine chest radiograph in which the affected hemidiaphragm is found to be elevated slightly.
76

3. Cephalad renal ectopia –
• Kidney is positioned more cranially than normal.
• H/o – Omphalocele.
• When liver herniates into omphalocele sac with the intesitinethe kidney continues to ascend till they are stopped by diaphragm at 10th thoracic vertebra.
• Ureter are excessively long.
77
Anomalies of form and fusion
1. Crossed renal ectopia with or without fusion –
• When a kidney is located on the side opposite from which its ureter inserts into the bladder, the condition is known as crossed ectopia.
• Ninety percent of crossed ectopic kidneys are fused.
78

• McDonald and McClellen classified :
79

Six forms of crossed renalectopia with fusion.
80

• First reported in 1654.
• 62 patients with crossed ectopia without fusion been reported.
• Solitary crossed ectopia has been reported in 34 patients.
• Crossed ectopic with fusion seen in 1 in 1000 live birth.
• Unilaterally fused kidney with inferior ectopia is the most common variety, whereas fusion with superior ectopia is the least common.
81

Cause :
• The reason of crossed ectopia are uncertain.
• Wilmer (1938) suggested that crossover occurs as a result of pressure from abnormally placed umbilical arteries that prevent cephalad migration of the renal unit, which then follows the path of least resistance to the opposite side.
82

• Potter (1952) and Alexander and coworkers (1950) theorized that crossed ectopia is strictly a ureteral phenomenon, with the developing ureteral bud wandering to the opposite side and inducing differentiation of the contralateral nephrogenicanlage.
• Fusion of the metanephric masses may occur when the renal anlagen are still in the true pelvis before or at the start of cephalad migration, or it may occur during the latter stages of ascent.
83

• It is the superior pole of the ectopic kidney that usually joins with the inferior aspect of the normal kidney.
• Ascent continues until either the uncrossed kidney reaches its normal location or one of the retroperitoneal structures prevents further migration of the fused mass.
• The final shape of the fused kidneys depends on the time and extent of fusion and the degree of renal rotation that has occurred.
84

• When the kidney not fused, the uncrossed kidney usually resides in its normal dorsolumbar location while the ectopic kidney is inferior and in either a diagonal or a horizontal position with an anteriorly placed renal pelvis.
• Solitary crossed ectopia, the kidney is usually located somewhat low but in the opposite renal fossa at the level of L1-L3 and is oriented anteriorly, having incompletely rotated on its vertical axis
85

Associated anomalies :
• In all the types of fusion anomalies, the ureter from each kidney usually is not ectopic. Except for solitary crossed ectopia, in which there may be a hemitrigone or a poorly developed trigone with a rudimentary or absent ureter on the side of the ectopic kidney.
• Vesicoureteral reflux is noted in 20% of crossed ectopia.
86

• The highest incidence of associated anomalies occurs in children with solitary renal ectopia and involves both the skeletal system and genital organs.
• Males - cryptorchidism or absence of the vas deferens;
• Female - vaginal atresia or a unilateral uterine abnormality.
• Imperforate anus has also been observed in 20% of the patients.
87

• As crossed ectopic anomalies have no symptoms. The defects are often discovered incidentally at autopsy, during routine perinatal ultrasound screening, or after bone scanning.
• Cystoscopy and retrograde pyelography were useful in mapping out the collecting system and pattern of drainage.
88

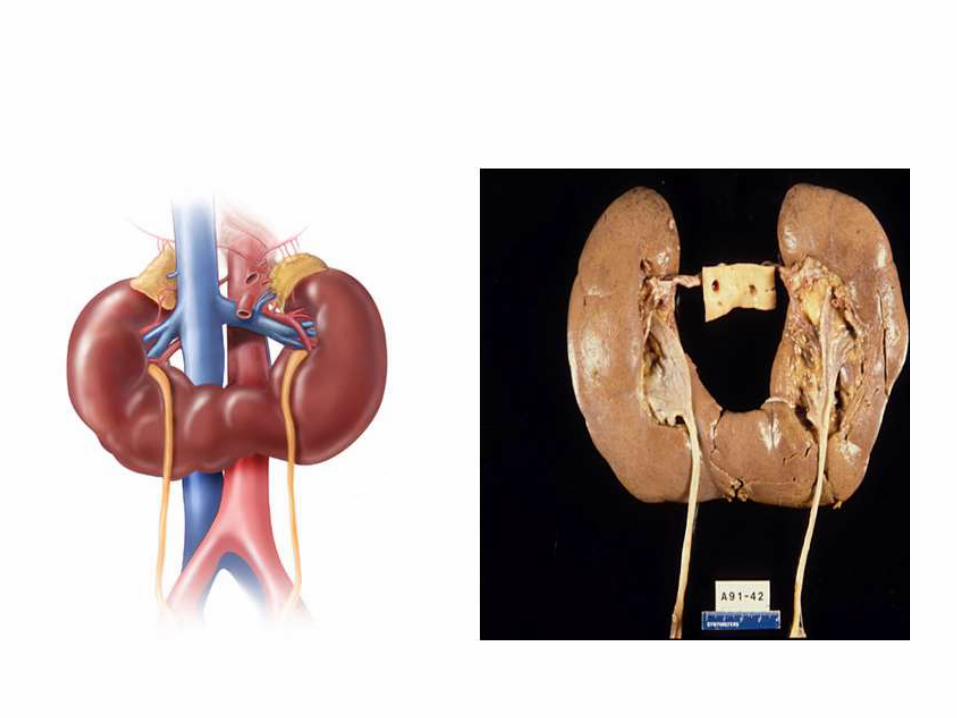
2. Horseshoe Kidney –
• Most common of all renal fusion anomalies.
• The anomaly consists of two distinct renal masses lying vertically on either side of the midline and connected at their respective lower poles by a parenchymatous or fibrous isthmus that crosses the midplane of the body.
• 1 in 500 births.
• 7% seen in Turners syndrome baby.
• 2 to 8 times more likely to have wilms tumor.
89
90

• The abnormality occurs between the 4th and 6th week of gestation.
• The intermediate mesoderm that gives rise to the metanephric blastema fails to separate.
• As the ureteric bud grows cranially, they come into contact with the fused nephrogenic cords and nephrogenesisproceeds.
• With growth of the embryo, the ascent of the kidney is arrested as the isthmus of the kidney makes contact with the inferior mesenteric artery.
91

• Normal posterior rotation of the kidney is prevented by the fusion resulting in the renal pelves becoming orientated anteriorly.
• Fusion usually occurs at the lower poles. Upper and midpole fusion is rare.
92
• Two theories of embryogenesis have been proposed –
- The classic theory involves mechanical fusion of two kidneys during organogenesis. The inferior poles of kidneys touch and fuse in the lower midline during the migration through the narrow fork of umbilical arteries.
- An alternative theory proposes that there is abnormal migration of posterior nephrogenic cells, which then coalesce to form the parenchymal isthmus.
93

• In 95% of patients, the kidneys join at the lower pole; in a small number, an isthmus connects both upper poles instead.
• Generally, the isthmus is bulky and consists of parenchymatous tissue with its own blood supply.
• The horseshoe kidney even though it produces no symptoms, is frequently found in association with other congenital anomalies like :
94
1. vesicoureteral reflux (50%),
2. duplication of ureters (10%),
3. hypospadias
4. undescended testis (4%),
5. bicornuate or septate uterus (7%).
6. Horseshoe kidney is also frequently found in association with other congenital anomalies. Most commonly affected organs are cardiovascular, skeletal, and central nervous systems.
95
• 50% of patients are asymptomatic.
• In most the anomaly is incidental finding at autopsy.
• When symptoms are present they are related to hydronephrosis, infection or calculus formation with vague abdominal pain.
• Sometimes abdominal lump.
• Ultrasonography is detected.
96
ANOMALIES OF ROTATION
• The kidney, as it assumes its final position in the “renal” fossa, orients itself so that the calyces point laterally and the pelvis faces medially. When this alignment is not exact, the condition is known as malrotation.
• Most often, is found with another renal anomaly, such as ectopia with or without fusion or horseshoe kidney.
• It is frequently observed in patients with Turner's syndrome.
97

• Medial rotation of the collecting system occurs simultaneously with renal migration.
• The kidney starts to turn during the 6th week, just when it is leaving the true pelvis, and it completes this process, having rotated 90 degrees toward the midline, by the time ascent is complete, at the end of the 9th week of gestation
98
• That rotation is actually the result of unequal branching of successive orders of the budding ureteral tree, with two branches extending ventrally and one dorsally during each generation or division.
• More parenchyma develops ventrally than dorsally, and the pelvis seems to rotate medially.
99

• Rotation of the kidney during its ascent from the pelvis. The left kidney with its renal artery and the aorta are viewed in transverse section to show normal and abnormal rotation during its ascent to the adult site.
• A, Primitive embryonic position; hilusfaces ventrad (anterior).
• B, Normal adult position; hilus faces mediad.
• C, Incomplete rotation. • D, Hyperrotation; hilus faces dorsad
(posterior). • E, Hyper-rotation; hilus faces laterad. • F, Reverse rotation; hilus faces
laterad.
100

• Rotational anomalies do not produce any symptoms, but if excessive rotation takes place can cause obstruction to outflow leading to hydronephrosis.
• The diagnosis may be done when a renal calculus is detected in an abnormal location, but confirmation should be obtained only from a renal ultrasound, excretory urogram, or retrograde pyelogram.
101

ANOMALIES OF THE COLLECTING SYSTEM
1. Megacalycosis –
• Defined as nonobstructive enlargement of calyces resulting from malformation of the renal papillae.
• It was first described by Puigvert in 1963.
• Most likely congenital and diagnosed prenatally.
• Males in a ratio of 6:1 and has been found only in white patients.
• Bilateral disease has been seen almost exclusively in males, whereas segmental unilateral involvement occurs only in females.
102

• The calyces are generally dilated and malformed and may be increased in number.
• The renal pelvis is not dilated, nor is its wall thickened, and the UPJ is normally funneled without evidence of obstruction.
• The cortical tissue around the abnormal calyx is normal in thickness.
103

Cause :
• There is transient delay in the recanalization of the upper ureter after the branches of the ureteral bud hook up with the metanephric blastema.
• This produces a short-lived episode of obstruction when the embryonic glomeruli start producing urine.
• The fetal calyces may dilate and then retain their obstructed appearance.
104

105
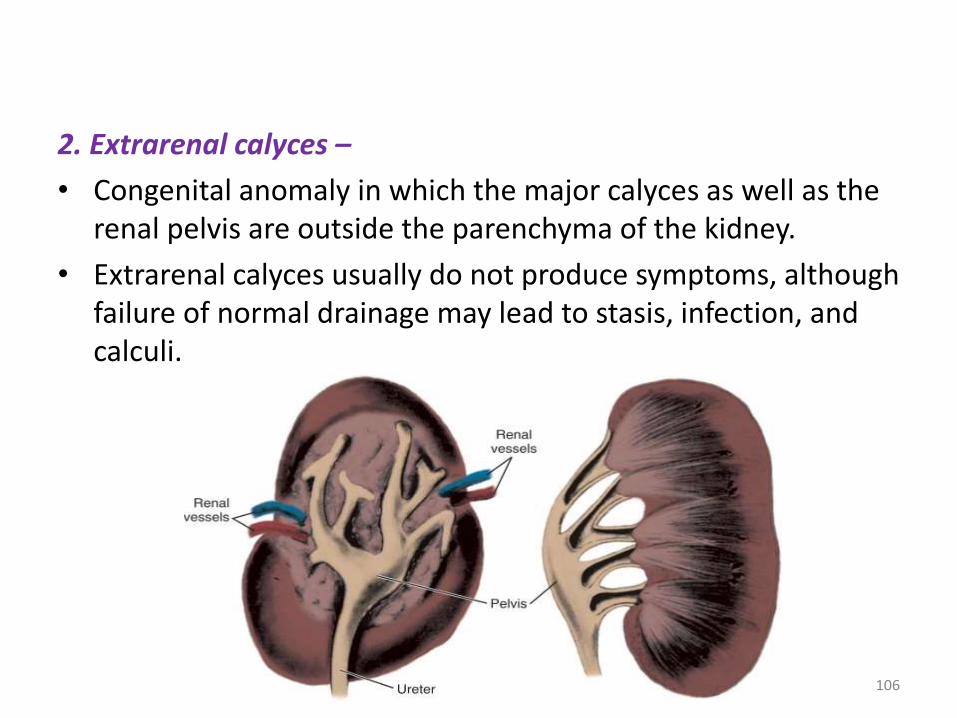
2. Extrarenal calyces –
• Congenital anomaly in which the major calyces as well as the renal pelvis are outside the parenchyma of the kidney.
• Extrarenal calyces usually do not produce symptoms, although failure of normal drainage may lead to stasis, infection, and calculi.
106

107

ANOMALIES OF RENAL VASCULATURE
Aberrant, Accessory, or Multiple Vessels
• Multiple renal arteries is the correct term to describe any kidney supplied by more than one vessel.
• The term aberrant vessels should be reserved for those arteries that originate from vessels other than the aorta or main renal artery.
• The term accessory vessels denotes two or more arterial branches supplying the same renal segment.
108

Accessory renal artey Multiple renal arteries
109

• The renal arterial tree is derived from three groups of primitive vascular channels-
• The cranial group consists of two pairs of arteries dorsal to the suprarenal gland that shift dorsally to form the phrenic artery.
• The middle group is made up of three pairs of vessels that pass through the suprarenal area. They retain the same lateral position and become the adrenal artery.
• The caudal group has four pairs of arteries that cross ventral to the suprarenal area and become the main renal artery.
110

• The kidney may receive its blood supply partially or entirely from arteries arising at an abnormal level.
• In the case of non ascent or of incomplete ascent the aberrant arteries may constitute the only supply.
• It may press upon the ureter and cause obstruction leading to hydronephrosis.
111

Renal artery aneurysm
• The overall incidence has been calculated to be between 0.1% and 0.3%.
• Most renal artery aneurysms are silent, especially in children.
• The diagnosis may be suspected with a pulsatile mass in the region of the renal hilum or when an abdominal bruit is heard.
112

113

• A wreathlike calcification in the area of the renal artery or its branches (30%) is highly suggestive.
• Many asymptomatic renal artery aneurysms come to light after the discovery and workup of hypertension.
114

Thank you• “Now an embryo may seem
like some scientific or laboratory term, but in fact the embryo contains the unique information that defines a person. All you add is food and climate control, and some time, and the embryo becomes you or me.”
-
Todd Akin
115